Vitamins, Minerals & Supplements for Pain & Healing
Critical analysis of most popular “nutraceuticals” — food-like pseudo-medicines taken for medicinal purposes, especially glucosamine and creatine, mostly as they relate to pain, arthritis, and recovery from exercise and injury

Arthritis is not caused by a lack of glucosamine. And it isn’t treated by them either. If you think they’re helping you, that’s the placebo talking.
People take many nutritional supplements because they are supposed to be “good for” muscles and joints, aches and pains, arthritis, and recovery from exercise and injury. These vitamins, minerals, and other assorted nutrients aren’t considered pain-killers — like ibuprofen — but people take them for pain anyway. They aren’t performance-enhancing “drugs,” but athletes and bodybuilders take them almost like drugs to enhance their performance… and people hope that anything that might enhance performance will also help the body with anything that ails it.
There is some good news here and there, but supplement science is almost entirely discouraging, not “promising,” and there are major concerns about contamination and side effects in any case.
This article covers creatine, vitamin D, chondroitin sulfate, magnesium, glucosamine, whey, collagen, glutamine, BCAAs, curcumin, bromelain, caffeine, Protandim, and fish oil. Hot takes and table of contents below.
Supplement science from 10,000 feet: the big picture in a paragraph
All the best-selling supplements have been studied and tested thoroughly over the years, and the results have been almost perfectly discouraging, particularly for the average healthy person with no particular problem to solve.1 New science is showing that even basic vitamin supplementation with staples like calcium may have more risks2 and fewer benefits3 than anyone suspected. Americans who use supplements don’t live any longer.4 They have been shown to be healthier by some measures, but likely just because people with healthier lifestyles tend to take supplements.5 And that was the basis for this excellent advice:
Be the kind of person who takes supplements — then skip the supplements.
Michael Pollan, Food Rules: An Eater’s Manual
None of this is surprising, because supplementation has never really been a plausible upgrade from good nutrition. The inevitable words “good for” betray a suspicious lack of biological specificity that plagues the topic: it is usually unclear just how supplements are supposed to be “good for” anything, and the more specific claims we see often just don’t make much sense. Many of them boil down to a shamefully simplistic more-is-better rationale.
And for pain, the focus of this article? Alas, in a whole world full of supplements, there isn’t compelling evidence that any supplement is helpful for any kind of significant chronic pain or rehab challenge. In twenty years of study, I have never encountered an important exception. That doesn’t mean that there’s literally nothing worth trying — there are interesting possibilities, like vitamin D deficiency. But there’s not a single proven pain-fighter in the entire supplement armamentarium.
Warning: contaminated supplements are common!
Contaminated supplements are a thing.6 The problem is so serious that it’s responsible for a huge rise in supplement-related calls to poison centers.7 In 2018 the Clean Label Project found 64 percent of a popular supplement category had detectable levels of arsenic, a third tested positive for lead, 17% had cadmium, and more and worse.
One major pharmacy is now testing products themselves to protect their customers (and reputation). A huge and totally unregulated industry is selling to legions of credulous people who are knee-jerk cynical about Big Pharma but never question the scruples of supplement sellers. What could possibly go wrong? Poisoning — that’s what!
Adulteration is another major concern: shady supplement makers spike their products with actual drugs to win fans… in shocking numbers.8910 Who needs placebo when your customers can “swear by” your product because it has actual pharmaceutical effects?
Dr William Osler once said, “One of the first duties of the physician is to educate the masses not to take medicine.” This sage advice coupled with the adage “first, do no harm” seems appropriate when discussing the use of dietary supplements with our patients and athletes due to their limited efficacy and known safety risks.
Supplement science highlights (and table of contents)
A 👍 appears with any supplement that has some kind of legitimate, significant good news about it — something about it that probably does actually help some people. And for the ones that are particularly dubious or problematic? 😠 Each item has a link to Examine.com (which has lots of science about most of these), or another key source.
- 👍 Fish oil (omega-3 fatty acids) — Fish is a fine source of omega-3 fatty acids, which seem to be linked to healthiness, a little, maybe, but it’s just not as clear as everyone seems to think. Actual fish is likely better than fish oil pills, and perhaps slightly anti-inflammatory — though probably just because it’s not poor nutrition (which is inflammatory). Examine.com
- 😠 Glucosamine and chondroitin sulfate — Both similar and known for being good for cartilage. Glucosamine is a building block of proteins and fats, especially in cell walls. Benefits for osteoarthritis possibly real but definitely trivial. Possibly toxic to pancreas. Chondroitin sulfate is a component of cartilage, taken for arthritis, largely ineffectively, and fairly safe — but with multiple rare and minor side effects. Examine.com
- 👍 Creatine — A form of stored energy for muscles, primarily used by athletes and bodybuilders. The most legitimate sports supplement with some verified benefits, but largely irrelevant to pain/recovery. Quite safe; may cause insomnia. Examine.com
- Whey protein — Prized by athletes as a convenient protein source to aid in building muscle, which does work, plus some wild speculation that it also has anti-inflammatory properties, all unproven. Numerous side effects and safety concerns, surprisingly. Examine.com
- Glutamine & Arginine — Amino acids (protein building blocks), mainly stored in muscle, taken by athletes to aid recovery from intense exertion and injury, also given to seriously sick/injured people. More drug-like and broadly plausible benefits for performance and recovery, but barely studied. Long lists of possible side effects and numerous safety concerns! Examine.com
- 😠 Collagen — Extremely abundant proteinaceous connective tissue ingredient (we are never “deficient” in it), popular for arthritis and touted as anti-inflammatory. Implausible. With scanty mixed evidence of any benefit. Probably very safe, though, so at least there’s that! Examine.com
- 👍 Curcumin — Curcumin is the biologically active part of turmeric with many claimed health benefits, but mainly anti-inflammatory. Mildly promising evidence for some kinds of pain, but even if it works your mileage may vary due to very complex bioavailability issues. Possibly safe, minor digestive side effects most likely. Examine.com
- 😠 Bromelain — A pineapple enzyme, better known as a meat tenderizer, that may also have anti-inflammatory properties — just an experimental drug that’s never been properly tested. Safety profile basically unknown; minor digestive side effects most likely. Examine.com
- 👍 Caffeine — The most popular drug in the world is a proven mild pain-killer and performance booster, but caffeine abuse — which is common, of course — is a plausible risk factor for chronic pain. Examine.com
- 😠 Protandim — Patented “blend of phytonutrients” from a multi-level marketing company that touts anti-aging and anti-inflammatory effects, classic too-good-to-be-true stuff. Barely studied, and no human studies related to pain at all. Safety? That’s a blank slate. ScienceBasedMedicine.org
- Tart cherry juice — A source of antioxidants and believed to be good for recovery from intense exercise, slightly supported by a couple small trials only. Possible sleep aid, oddly. Likely quite safe, of course — it’s just fruit juice. Examine.com
- 👍 Vitamin D — Vitamin D deficiency is probably more common than once suspected and may cause or aggravate chronic pain. While evidence that supplementation can correct it is scanty, it’s probably a worthwhile experimental medicine for chronic pain patients, because it’s cheap. But don’t “mega”-dose, that’s nonsense. And its ability to prevent muscle or bone loss in healthy older people is very much in doubt. Examine.com
- 👍 Magnesium — Magnesium is one of the essential minerals, widely used in biology, so deficiency has many possible effects, but most notably it makes nerves a wee bit trigger happy. Despite its importance, deficiencies may be both common and related to pain — but also probably better fixed with diet. For chronic pain patients, it isn’t a ridiculous supplementation option. Examine.com
- Branched-chain amino acids — The BCAAs are three of the essential amino acids, and yet another alleged recovery aid, better than the other amino acids at promoting protein synthesis. Preliminary evidence was promising (isn’t it always?), but hasn’t been replicated (is it ever?). Several known side effects: disorientation (!) and substantial indigestion. Examine.com
- Coenzyme Q10 (CoQ10) [MEMBERS] — An obscure nutrient and antioxidant (with all that implies), but also famed for relieving the muscle aching side effect of the statins (the cholesterol drugs). The science is sketchy, however: it’s not clear that CoQ10 can solve the problem … or even that there is a problem to solve.
- Probiotics [MEMBERS] — We do now know that gut health affects entire bodies. But do probiotics actually make guts healthier? And solve real health problems? Perhaps, but we are also clearly meddling with forces we do not yet understand, and meanwhile the supplements industry is cashing in on the hope. Probiotics for pain patients are still almost perfectly experimental.
The last two sections are visible to logged-in PainSci members only. Members can login to get all the details and with citations. You are a logged in member, so you can see them.
Some other topics:
- Do supplements show promise for pain patients in general?
- Anti-inflammatory nutrition vs. supplements
- Ergo-what? Performance, fatigue, and pain
- But it worked for me! The role of anecdotes and testimonials
- Big Suppla: Large supplement corporations are not only just as bad or worse than the pharmaceutical ones, many of them are the same corporations
- The Multi-Level Marketing Connection: Supplements and Fraud
- “Big Suppla” is now evidence-based debunking
- What about cannabis? Almost a “supplement,” but not quite. See Marijuana for Pain
- What about DMSO? Although marketed as a supplement, and sometimes combined with them, dimethyl sulfoxide is very much a chemical — a potent industrial solvent, alien to human biology, with peculiar properties of unclear medical value or safety. See DMSO for Pain.
- And how about just nutrition itself? I discuss the idea of “anti-inflammatory nutrition” below, and also in an article dedicated to inflammation: Chronic, Subtle, Systemic Inflammation.
Arthritis and exercise soreness are the focus of a great deal of supplement research
The more you read on this page, the more you might notice a pattern: again and again, the research is about arthritis or exercise soreness. They are good proxies for lots of other kinds of pain. They are very common, and anything good for those things might be useful for other kinds of pain, too.
You can only take that so far, though. There are many causes of pain, more than most people realize, and pain is weird — volatile, complex, and deeply baked into our biology. A “broad spectrum” pain-killer is impossible in principle: anything that works for one kind of pain is always likely to fail with a bunch of others. A basic truth about pain is that the only way to treat it is to take the person out of the equation — anaesthesia. As long as you are still conscious, there are still ways that you can hurt, no matter what you eat (or don’t).
Do supplements show promise for pain patients in general? More detail now
No, they do not. Many of the supplements above make little or no sense even in principle: regardless of whether or not we need a substance, it is often impossible to get more simply by eating it.11 And nearly all of them have been failing a basic credibility test for years: a lack of good evidence of efficacy, and not for lack of trying in the case of the popular ones. Only one of them (creatine) is a clear winner. Not one other is definitely helpful.
If any of the others truly had significant therapeutic effects, it shouldn’t be hard to prove it, should it? There should be studies that don’t just “kinda” show some benefit … maybe … . There should be studies that leave no doubt there is something there.
There’s a lot of seemingly conflicting evidence about nutraceuticals. However, there’s a pattern of much ado about nothing. Even the most generous interpretations of the most positive-seeming results are still kind of underwhelming.
And that squares nicely with the anecdotal evidence, which is hardly impressive either, despite great commercial success and lots of enthusiasm.12
Instead mostly we just have a mess of weak, confusing evidence, and it probably won’t get any better. It’s rare for anything particularly good to finally emerge from that kind of mess. The history of medicine shows us clearly that most popular remedies lacking good scientific support usually turn out to be popular because they are popular (and aggressively marketed) — not because they ever actually worked.
Survey says most people don’t care what the science says: most people won’t quit taking supplements no matter what
In 2013, Blendon et al. found that only about a quarter of surveyed supplement users would quit taking a supplement if it was shown to be ineffective.13 Faith in supplements is a freight train that probably cannot be stopped in anything less than a generation. When you consider what the evidence is up against — people’s hopes and fears — perhaps it’s remarkable and even encouraging that as many as 25% of people said they would lay off a supplement if it was proven to be useless. And presumably some percentage could be swayed by enough of the right kind of evidence and rhetoric, which hopefully means there is some damned point to our blogging!
You can’t reason people out of anything they didn’t reason themselves into. They’re taking supplements not because it makes sense, but because life — even for the healthy and wealthy — is often tiresome and difficult and discouraging and maybe, just maybe, supplements will make it all a little easier. Unless you can offer something that actually can, you’re not going to convince people to stop spending a little of their discretionary income on that gamble.
Anti-inflammatory nutrition versus supplements
Many supplements are touted to be “anti-inflammatory,” but loose usage has rendered this concept almost as meaningless as “detoxification.” Inflammation is synonymous with immune system activity, and “immunology is where intuition goes to die.”14 Inflammation is not one thing, but a huge family of overlapping and interacting processes. It’s not that we want less inflammation in our lives — it’s that we want a dynamical and dazzlingly complex balance of just the right types of inflammation in the right places, times, and amounts… all of which is a constantly moving target, as it strongly interacts with variables like your gut microbiome.
Based on the complexity alone, anti-inflammatory claims are broadly implausible. Any one substance is less likely to “fix” an inflammation problem than any one wrench is going to fix a broken down car.
There’s a lot of overlap between the idea of anti-inflammatory supplements and an anti-inflammatory diet. I think most people imagine that an inflammatory diet contains special foods — “super” foods, even — that have anti-inflammatory properties. And to whatever degree you accept that, then why not just eat whatever makes those foods special? Why bother with the food?
Because there mostly is no such thing as special anti-inflammatory ingredients — either as part of food, or isolated as a nutritional supplement. An anti-inflammatory diet is just a diet that avoids foods that are pro-inflammatory… which is mostly just an obviously unhealthy diet, because being unfit is inflammatory. So what’s an anti-inflammatory diet? Just a diet that isn’t terrible.
A few foods do seem to have some anti-inflammatory properties, but it’s quite rare, and they seem to be hard to extract and isolate. The main example of this is fish…
Omega-3 fatty acids, and fish versus fish oil pills
Fish is the best dietary source of omega-3 fatty acids, which might be a valuable class of nutrients. The conventional wisdom for years is that they are “heart healthy” and more, and maybe it’s even true, though Heaven help you if you try to actually find “proof” of that. Perhaps they are useful for athletic performance and recovery, but that’s seriously uncertain. And maybe omega-3 fatty acids are valuable on their own (fish oil in a pill), and maybe they aren’t. Some details…
Fish oil has perhaps shown some potential to aid with recovery from exercise.15 A 2020 review of more evidence like that is clearly bullish: the authors “identified evidence” that fish oil can improve performance: “enhanced endurance, markers of functional response to exercise, enhanced recovery or neuroprotection.”16 They also emphasized that the data is mixed and mediocre, and it all could so easily just be a cherry-picking expedition (seriously, anyone can “identify evidence” supporting anything these days). There’s no way to know if their optimism is trustworthy without more and better data and backup from other experts, but more data almost always leeds to more contradictions. Case in point…
Extracting and isolating omega-3 fatty acids and putting them in a pill might undermine their power to protect us from disease, but there’s no way to be sure. This body of evidence is much more substantial — dozens of studies, including some huge ones — and yet still extremely complex and inconsistent, with major trials and reviews pointing each way: some show that fish is better than fish pills,17 while others show that they are both protective against disease.18 But good luck finding a study that shows that supplements are better than fish! And the uncertainty only punctuates that fish oil on its own isn’t exactly guaranteed to do the job. Trying to actually prove that either fish or fish oil protects from disease is nearly impossible — the variables are nearly infinite. Wake me up in fifty years when science has sorted it all out.
Meanwhile, I suggest erring on the side of fish. This is an important general principle. Food is probably the best source of nutrients. Not extracted and purified molecules. No one’s actually surprised by that, right? Right?
Glucosamine — leading by example?
Glucosamine has long been the king of the supplement hill, and so you’d hope it was also the best — if any supplements work, it had better be this one. It is known as being “good for cartilage,” and is mostly used to treat osteoarthritis (especially hips and knees) via alleged anti-inflammatory and other happy effects on cartilage. It doesn’t really, and neither does its cousin chondroitin sulfate — not enough that even the largest trials can produce an uncontroversial result anyway. But let’s look at them earnestly a bit anyway, starting with some chemistry:
- Glucosamine is an abundant monosaccharide — and amino sugar — and a building block of proteins and fats, especially in cell walls. It is made commercially by extracting it from crustacean exoskeletons. Shrimp shell!
- Chondroitin sulfate is major component of cartilage, and it has much in common with glucosamine (they are often sold together). It is chemically complex, and it’s almost impossible to know what you’re really getting.
Both of these substances are “building block” supplements, which are all based on the idea that consuming the ingredients of a given tissue will enable the body to repair that tissue more effectively. But arthritis isn’t caused by a deficiency of the molecules it is made from. Even if it was, a deficiency is unlikely without a pathological cause: these are extremely abundant molecules in the human body, which our biology churns out by the billions from other more basic ingredients.19
Glucosamine supplementation has been mostly bashed by science continuously for at least twenty years now.2021 It bombed two particularly good tests in 2010,2223 showing benefits for osteoarthritis that are possibly real but barely clinically significant, like “taking a car from 40mpg to 42mpg” (Examine.com editor Sol Orwell’s analogy). Plus another flunk from a huge 2010 meta-analysis of 3800 patients.24 A major 2015 report on knee osteoarthritis treatments declared it to be particularly useless (along with chondroitin sulfate).25 A 2018 meta-analyses (pooled data study) in Rheumatology International was decisively negative.26 JAMA’s big 2018 meta-analysis took a more nuanced approach, focusing on long-term results (arguably the only results that matter for arthritis), and concluding that — despite mountains of data from forty-seven randomized controlled trials, including more than 22,000 patients — there was still “uncertainty” around the size of any benefit and the conclusion was an eye-roll inducing “we need more data.”27
Do we really, though? If you can’t find a signal in that much data, there isn’t anything interesting to find. If these substances were even remotely useful, don’t you think it would be just a teensy bit more obvious? If glucosamine were a student, its parents would get called in for a conference about little glucosamine’s poor performance. Perhaps there’s something going on at home?
In July 2010, Dr. Harriet Hall reviewed the evidence of absence of any glucosamine benefits at ScienceBasedMedicine.org and concluded that glucosamine proponents
… can always complain that maybe it works for knees but not for hips, or that a different dosage might have worked better, or that it works for some small sub-set of patients. There will always be “one more study” to do. … This new study confirms my opinion that we shouldn’t spend any more research dollars doing “one more study” on glucosamine.
Are there technically positive studies? Of course! It’s the 21st Century — you can’t swing a dead cat without hitting a positive study about practically anything. In this case, most are based on ideas like “maybe specific kinds of patients” or “maybe a specific type of glucosamine.” Some of these trials have yielded what appear to be “promising” results — that no one else ever seems to be able to confirm, and which have little relevance to the consumer. Let’s just say for the sake of argument that there actually is a particular combination of patient and chemistry where it works. Literally no one knows if they are that person, or how to know that they are getting that product. For the average consumer, it’s a meaningless signal, completely lost in the noise of science and marketing.
Not that any of the evidence will actually stop people from “believing” in glucosamine and buying it in bulk! Glucosamine bottlers really appreciate everyone’s continued gullibility.
P.S. on chondroitin sulfate
The science is basically identical, and indeed there’s a bunch of overlap in the research. All scientific papers about chondroitin sulfate are good examples of no clear good news. A good example is an experiment by Gabay et al., who somewhat absurdly concluded that chondroitin sulfate “improves hand pain” — which was technically true, but the improvement was rather trivial.28 In the context of the body of evidence, it’s really quite silly to write a summary that sounds so positive. Although it’s an aging reference, it was and remains perfectly cromulent: the New England Journal of Medicine slammed chondroitin sulfate hard back in 2006.29
Ergo-what? Performance, fatigue, and pain
Ergogenic aids improve physical or mental performance: stronger, faster, better in some way. Comic books are full of super-soldier serums, the ultimate fictional example. In real life, anabolic steroids are the most classic way to effectively cheat at sports — nothing else delivers an unfair advantage quite like that. Most ergogenic aids are less impressive, but the hope is that anything that can enhance performance is also a kind of medicine — that improvement is improvement, whether you’re starting from a healthy state or a messed up one.30
From stimulants like caffeine and cocaine to nutritional fuels like creatine, performance can be boosted — but usually not much, and often with a price. There ain’t no such thing as a free lunch, and better lunches usually cost more. They should be used with caution.31
What about pain? Can a proven performance booster help pain? Perhaps. We know that perception can change both pain and power.32 But what we all really want something that we can swallow — a pain-killer from the supplement store.
All the supplements that allegedly boost performance also have a bit of a reputation of being good for pain, and precious little evidence. But a link remains plausible in special cases. The largest subcategory of performance boosting is improved fatigue resistance and recovery, which in turn may overlap with healing — much of which is just recovery from the effects of acute physical stress.33 And that in turn may have some relevance to pain, because that which makes us tired may also make us hurt.34 Ever have a hard time telling the difference between pain and fatigue? They might have some biology in common.
But if any ergogenic aid can treat pain, it has yet to be proven. Creatine is probably the best hope there is.
Creatine: the most evidence-based common supplement
Creatine is the standard bearer for supplements that aid exercise recovery, reduces fatigue, and might by extension have other health benefits including less pain. It is by far the most popular supplement that actually does what it says on the tin: creatine really does fight muscle fatigue, a benefit that is mainly of interest to people who use their muscles intensely. Bodybuilders take creatine so they can lift longer. Muscle cells take longer to tire out when they have extra creatine in their little cellular pantries. It’s an “energy intermediate,” a molecule that is part of the metabolic recipe for replenishing the fuel molecule, adenosine triphosphate (ATP is one of the greatest hits of organic chemistry).
The stuff clearly works on almost everyone,35 and it is perhaps the only popular supplement that does. Examine.com’s mighty creatine page is extremely thorough and balanced. If you want all the creatine science, please go there:
Creatine is among the most well-researched and effective supplements. It can help with exercise performance by rapidly producing energy during intense activity.
For balance, I will point out that some researchers have some reservations — but, notably, they still acknowledge the benefits for muscle recovery. They just aren’t sure if it translates to measurable benefits for anyone but bodybuilders.36
Currently, the scientific literature supports creatine supplementation for increased performance in short-duration, maximal-intensity resistance training. Whether these effects of creatine supplementation lead to improved performance on the field of play remains unknown.
Going beyond sports to other medical benefits is even more of a reach, but there is some evidence that creatine is useful for some other conditions.37 It might improve mental alertness when sleep deprived, even just a single good dose the morning after a bad night.38 It’s unlikely to help osteoarthritis, that most universal of painful conditions (and a good proxy for many others)39 but muscular dystrophy is a very interesting positive example. There’s a common form of muscular dystrophy that routinely goes undiagnosed, and yet causes excessive muscle fatigue and soreness.40 It’s a subtle and specific cause of pain that might actually respond well to creatine, even if you have no idea why.41 But it’s also a perfect example of why a supplement like creatine might help one person’s pain but not most others.
Another intriguing example of the same type: creatine supplementation might relieve a painful side effect of a common class of drug, the cholesterol-lowering “statins” for heart disease prevention (like Lipitor).42 There’s little direct evidence of this so far, but it’s plausible.43 If this effect exists, it’s great for a specific group of patients.
But there isn’t a shred of evidence that creatine’s fatigue fighting benefits have the slightest relevance to pain in general, or any common kind of chronic pain. Nevertheless, it is often recommended for fibromyalgia and chronic fatigue syndrome, which isn’t crazy to try but certainly isn’t based on strong evidence. Also, it may have counter-productive side effects for those patients…
Creatine is super safe, too!
Creatine also appears to be one of the safest of all supplements: “The only consistently reported side effect from creatine supplementation that has been described in the literature has been weight gain.”44
Creatine may give some people trouble with their sleep, and that happened to me (see my insomnia article for the story). But I suspect this isn’t a major issue for many people: it doesn’t get a mention in the scientific literature. It’s just a side effect some people report that I seemed to experience myself. This is an important possibility to be aware of if you're using it for fibromyalgia or CFS, conditions that often involve disturbed sleep to begin with.
Whey protein (AKA protein powder, protein shakes)
Whey powder is what’s in those large buckets you see in supplement stores that seem to cater mainly to bodybuilders, although also very popular with the aspirational market: people who buy it optimistically thinking they will do enough weightlifting to need it, making it one the best-selling of all the non-vitamin supplements (collagen is the other big one). The idea is that it’s a convenient source of fairly pure protein, like egg whites but cheaper and nicer when blended with blueberries.

A whey wall.
The merchandising of whey powders has a very well-established style: lots of big buckets, lots of red, black, blue, and many words that suggest power and size and awesomeness. Mass! Nitro! Titan! Can this stuff possibly be good for chronic pain patients as well as bodybuilders?
It’s a mixture of globular proteins isolated from whey, the liquid material created as a by-product of cheese production. It is prized by athletes as a protein source to aid in building muscle. There is no controversy regarding bodybuilding benefits, but it’s also not doing anything special: it is literally just a more convenient way to eat the large amounts of protein needed by anyone doing a lot of weightlifting.
There is also a lot of wild speculation that it also has anti-inflammatory properties, and/or some other good-for-pain effect. I have had any number of people write to me over the years to tell me that eating a lot of protein (in whey or other forms) had cured their chronic pain. There is exactly zero real data about this — just anecdata.
Despite the fact that it’s basically just protein, there are actually several side effects and safety concerns about whey powder. Glucoasmine is probably safe at recommended doses, but pancreatic damage is possible with more45 These products also routinely contain added sugar — a nutritional hazard. And there’s also the contamination issue with all supplements, which definitely applies to this huge category. In 2018 the Clean Label Project screened 134 products for 130 types of toxins and found that many protein powders contained heavy metals, bisphenol-A (BPA), pesticides, or other contaminants. One protein powder contained 25 times the allowed limit of BPA. Horrifying.
Maybe stick to egg whites and skinless chicken breasts?
Bromelain, the lesser known pineapple-derived anti-inflammatory nutraceutical that has been in research limbo for ages
Bromelain is worthy of a look. It is one of two pineapple enzymes, plus a few other compounds. It’s best known as a meat tenderizer, but may have anti-inflammatory properties as well. Somewhat less of a “nutra” and more of a “ceutical”, bromelain might have the potential to be used as a substitute for anti-inflammatory drugs. It’s a substance with potentially anti-inflammatory properties that just happens to come from pineapple in the same way that aspirin comes from willow bark. But for now — and probably forever — it’s something you get from the supplement store, not the drugstore.
In 2004, Brien et al. reviewed a dozen early studies of bromelain research in Evidence-based Complementary & Alternative Medicine.46 Despite a blatant conflict of interest — Brien works for a bromelain bottler — the review seems balanced,47 and the authors do not fail to point out weaknesses in the evidence (lots) or concerns about adverse effects (definitely possible). Their conclusion is cautiously positive (surprise surprise), and seems to be justified by the evidence reviewed. “The currently available data do indicate the potential of bromelain in treating osteoarthritis.”
However — and this is critical — we already have medications that do “something” to help people with painful osteoarthritis. To qualify as a replacement for existing medications, bromelain would not only have to work just as well, but also have fewer side effects. “Effective but safer alternative treatments would be of benefit to osteoarthritis sufferers,” write Brien et al. And proving fewer side effects is tricky — a high bar to clear, requiring multiple large trials.48
This was not even remotely established in 2004. How about fifteen years later?
2021 bromelain science update: no news is bad news
Almost nothing has happened scientifically with bromelain since 2004. Just a single study strikes me as legit enough to be worth citing, and only barely: it’s just a pilot study… and negative. It showed that bromelain was no better than existing medications for arthritis.49
Other than that,
In short, there really isn’t any bromelain research worth discussing. There is just a remote possibility that pineapples contain a molecule that is not only as useful as existing anti-inflammatory drugs but also has fewer side effects. Literally every single existing anti-inflammatory drug has a unique batch of side effects — so what are the odds that bromelain is both efficacious and safer? Not great.
And yet it’s been in stores the whole time, unproven and unregulated. What could possibly go wrong?
Caffeine improves physical and cognitive performance during exhaustive exercise, but also carries a risk of actually increasing pain
Caffeine is widely believed to be an ergogenic aid — a performance booster — and, for once, the evidence actually supports popular belief (also true of creatine and several other ergogenic aids, because performance is actually relatively easy to trivially boost). It doesn’t even matter how much of it you drink normally: you’ll get a boost from caffeine whether you guzzle the stuff every day, or never touch it.51
I’ve played a lot of ultimate with players who are younger, fitter, and more talented than I am. Truly, I’m just happy that I can play on the same field and not embarrass myself … much. Without a doubt, the most limiting factor is exhaustion: I often make tactical mistakes or throw “swill” (slang for a lousy throw) not because I don’t know how to play the game, but because I’m just too whipped to play it well. The older I get, the more swill happens. 🤷🏻♂️
Caffeine to the rescue!
According to Medicine & Science in Sports & Exercise, caffeine really will “significantly improve” not only endurance performance, but “complex cognitive ability during and after exercise.”52 Sign me up! I’ve already pretty much embraced caffeine as one of those rare pleasures in life that has minimal downside — this is just gravy!
The researchers studied 24 well-trained cyclists, giving them either 100mg of caffeine or a placebo and then testing their endurance and their mental function during and after workouts. The signal was loud and clear: caffeine consumption boosted their performance. I can hardly wait to eat some caffeine before my next game!

Coffee — a good source of performance!
But there are also problems: caffeine makes us hyper, and is probably somewhat exhausting. We pump more adrenalin, exhaust ourselves, lose sleep: risk factors for pain. Chronic, excessive caffeine abuse — vicious cycle of self-medication, caffeine every morning, alcohol every night, very common — could well be an aggravating factor in cases of chronic pain. So here we have a substance that is, on the one hand, almost certainly an effective ergogenic aid, and even a short-term reliever of pain, but probably also a long-term aggravator of pain when chronically abused.53
Bottom line: caffeine is a known mild analgesic and ergogenic aid, but caffeine abuse — which is super common — is a plausible risk factor for chronic pain.
If you’re going to drink it (and you probably are) what’s the best source of caffeine? Scott Gavura reports that “coffee has more caffeine than many energy drinks. A 16 oz ‘grande’ coffee at Starbucks has 320mg of caffeine … in comparison, a Red Bull has 151mg/16 oz.”
So go ahead and enjoy your Red Bull. But when that liquid candy stops appealing to you, I’ve got some shade-grown, bird-friendly, passive-organic, fair-trade, home-roasted coffee for you to try.
(P.S. It also doesn’t dehydrate you. That’s a silly myth.54)
Glutamine and arginine for exercise recovery and soreness? Faith-based supplementation based on the extreme (and controversial) example of critically ill patients
I have always really paid for my workouts. I get DOMS (delayed onset muscle soreness) something awful, and always have — some unsolved mystery about my biochemistry. It starts soon after a run or a game of ultimate, and lasts 3–4 days. The only thing that helps is being as fit as possible at all times: if I take a break, it will be nasty when I get back to it. After griping to my doctor about this one day, he recommended that I try arginine supplementation. Why?
Both glutamine and arginine are abundant non-essential amino acids (protein building blocks). Both are needed for tissue repair, which is the basic reason for thinking they might help with exercise recovery. There is not much reason to emphasize arginine over glutamine, since the rationale for using both is pretty similar — and similarly weak, as their clinical effects are generally complicated and under-studied.
Glutamine is the most abundant of the non-essential amino acids in the body, much of which is stored in muscle. Both glutamine and arginine get depleted in people recovering from major injury and illness, in which case they are regarded as “conditionally essential” — that is, they are essential during emergencies, when there’s lots of tissue rebuilding going on. For this reason, glutamine is used medically to treat the critically ill (controversially, but it’s used; arginine is used less, mostly because of safety concerns).
Extrapolating from that extreme (and sort-of medically endorsed) usage, athletes and bodybuilders take a lot of the stuff because they believe that their exertions may be so harsh that they run low on amino acids in the aftermath — “I worked out so hard it’s like an emergency!” — and they hope that topping them up will help them repair and build muscle. However, it is unlikely and generally implausible that healthy athletes are ever glutamine depleted in the first place,55 and therefore it is also a bit unlikely that they can benefit from supplementation for this reason. And if they can’t get depleted, we probably can’t either.
There are other possible reasons. Both of these amino acids, and a few others, generally have a mess of barely understood properties which might be relevant to exercise performance and recovery,56 such as stimulation of growth hormone production,57 or dilating blood vessels.58
The state of the clinical research for arginine and glutamine supplementation is predictably poor. Their use can only be faith-based, not evidence-based. I spent about a half hour poking around for glutamine/arginine science on the web and PubMed, and determined only that they are nearly unstudied in the context of athletic performance. 99% of search results are places to buy the stuff, with another .9% being blog posts enthusiastically recommending it because “research has shown” that it works (almost always not citing any research). I couldn’t find any thorough critical analysis of either (although MayoClinic.com has dry summaries for both). I found one good-news study, but it’s weak sauce.59
There’s some encouraging scraps of basic science about both amino acids, but even their medical usage — glutamine for critically ill patients — remains controversial because the evidence is incomplete and conflicting. So there’s really no hope that we will know any time soon what, if anything, either of these substances do for something as trivial as a little bit of muscle soreness after exercise.
Meanwhile, there are safety concerns for chronic supplementation of either. For glutamine “neurological effects were the most frequently observed,”60 and arginine is “associated with death in certain groups of heart patients.”
Death. Now there’s a side effect. Remember: gambling with biochemistry.
Branched-chain amino acids: leucine, isoleucine, valine
And sneezy and happy and dopey…
The branched-chain amino acids (BCAAs, or just “protein supplements”) are three of the six essential amino acids in human physiology and they are widely believed to be more important to recovery than the other amino acids for more or less the same reasons (like the non-essential glutamine and arginine, see above): that is, people hope they are better at promoting protein synthesis, and therefore may help muscle growth/repair after exercise, and that in turn might — in theory — also reduce soreness, aid recovery, and generally make muscles better.
For several years there was a lot of excitement (and protein supplement sales) on the strength of promising preliminary evidence about BCAAs… which then failed to be replicated. Yet another case of “promising” research that went nowhere. Recent trials and reviews of this topic are mostly negative.616263 Fedewa et al. is the only recent review to claim victory: “A large decrease in DOMS occurs following BCAA supplementation after exercise compared to a placebo supplement.”64
There’s always the possibility that certain people, with just-so biology, are benefitting way more than others. But clearly its benefit for the average human is not robust enough to be easily confirmed. The BCAAs are on even thinner scientific ice than glutamie and arginine. So really very thin indeed.
Collagen: ever so slightly good for arthritis, maybe
Collagen — you’re basically made of the stuff. It is an extremely abundant proteinacious building block of connective tissue, currently popular as an arthritis treatment in the form of products like Genacol, and also used extensively for skin and nail health. There are a bunch of different forms from various animals sources — pig, cow, fish, shark! The evidence supporting this bazillion-dollar industry is, as usual, embarrassingly weak. A 2019 review described the science as “controversial” and “minimal” — but also “promising”!65
Will a Jello diet help your joints? It’s a short leap of faith from skin health to the health of other important tissues, like cartilage, where there is more hope and even less evidence.
The skeptical perspective is straightforward and predictable: eating collagen is probably mostly or entirely useless. Assuming extra collagen is helpful in any way, it is probably impossible to get it by eating it in the form of a supplement. Pharmacist Scott Gavura for ScienceBasedMedicine.org:
From a dietary perspective, your body doesn’t care (and can’t tell) if you ate a collagen supplement, cheese, quinoa, beef, or chick peas — they’re all sources of protein, and indistinguishable by the time they hit the bloodstream. The body doesn’t treat amino acids derived from collagen any differently than any other protein source. For this reason, the idea that collagen supplementation can be an effective treatment for joint pain, osteoarthritis, or any other condition, is highly implausible, if not impossible in principle.
But evidence! And complexity! Nothing in biology is ever simple. Exactly what kind of collagen may be important, and there’s just enough smoke in the evidence to wonder if there could possibly be a fire here somewhere. There are a bunch of positive studies, but are they positive enough for any sensible person to care? The damned-with-faint-praise problem is substantial. The only major recent scientific review of collagen for arthritis does indeed seem to bring good tidings, but how good? The authors summarize the improvements detected by trials as “significant,” but that’s a classic bit of spin and a well-known science foul: they mean statistically significant, which is not the same thing as important or major.66
In fact the improvements were right around the threshold of clinical significance.67 As Scott says in a much more recent article: “There are inconsistent signs of benefit and of unclear clinical importance with collagen hydrolysate.” Yup.
Medical science tends to produce “promising” results that are later overturned by more and better data.
And then there’s safety: eating pure collagen isn’t harmless. It’s a weird non-food that can definitely mess with people There’s almost no hard data about it, but lots of anecdata and concerns in principle from healthcare professionals. Allergic reactions, hypercalcemia, insomnia, depression, kidney stones, constipation and diarrhea… all possible. This kind of supplementing could absolutely backfire for pain patients.
Remember: like most of the supplements, collagen is a natural part of part of food. Extracting and isolating it and consuming it in quantities far beyond what you’d ever get from a normal diet is not what nature intended.
Turmeric and curcumin: not just tasty
Curcumin is a spice. It’s the interesting molecule in the bright orange South Indian spice, turmeric, a flamboyant cousin of ginger. There are also other similar molecules (the “curcuminoids”), which are polyphenols, huge category of molecules that is associated with astringency and the healthiness of many foods: some fruits and most berries, especially grapes and therefore also wine, plus chocolate and tea. Polyphenols are so diverse and complex that it doesn’t really make sense to think of them as “healthy” and more than you’d think that all snacks are healthy. For instance, they may or may not be “antioxidants,” which in turn are also extremely complex and may or may not actually be healthy.
Is curcumin an antioxidant? Healthy? Good for pain? Yes, probably, and perhaps.
According to Examine.com, “Supplementation of curcumin reliably reduces markers of inflammation and increases the levels of endogenous antioxidants in the body.” Does that translate to benefits for a good proxy for all kinds of pain, like arthritis? As usual, the answer is a bit “meh” — yet another case of “promising” data that doesn’t pass the “impress me” test. From a 2017 review:Curcuminoids may have some beneficial effects on knee pain and quality of life in patients with knee OA. However, they are less effective at relieving pain compared with ibuprofen. Curcuminoids appear safe on the short-term, and may reduce the need for rescue medication. Published RCTs vary in reporting quality, are characterized by small sample sizes, and have all been conducted in Asia.
Less than ibuprofen, eh? Well, I like curry anyway…
In a 2015 study, “curcumin caused moderate to large reductions in pain” in 17 men with extremely sore leg muscles.68 It also helped some aspects of strength loss. The effect size here actually does impress me, and these results constitute the only really good science news about any kind of treatment for exercise soreness, by the way. Now it just needs to be replicated! And it still hasn’t. Good and promising news, but simply unverified, and there are about a thousand ways that one study can be wrong.
There is a complication with curcumin that drives up the cost and risk of wasting your money: although curcumin is widely available, unfortunately it is poorly absorbed without other agents such as black pepper extract (e.g. piperine). Most bottles advertise one method or another of enhancing absorption, and some of them use it to justify a much higher price point, but it’s hard to know (maybe impossible) how well any of them actually work. Just be aware that straight curcumin may not be effective.
As always, anything that can have a positive effect can also have a negative effect. Curcumin isn’t likely to cause anything worse than indigestion for most people, but it does have some odd interactions with common drugs that many aging people take: it can actually boost the effect of diabetes meds and blood thinners (including aspirin); and it can cancel the benefits of antacids.
Tart cherry juice
There’s just enough good news about black cherry juice to justify talking about it. Just.
Recovery from intense exercise can probably be at least partially enhanced with, of all things, tart cherry juice. It’s the antioxidants, see. (That word makes me a little suspicious.) Cherry juice, it seems, is chock-a-block with them and other “anti-inflammatory agents.” None of these things have proven to be especially helpful for muscle soreness before. But the cherry cocktail is special, because apparently if you give cherry juice to several young men and then make them exercise their biceps viciously, they experience a statistically significant 22% less strength loss69 than their poor peers who got fake cherry juice: black cherry Kool-Aid.70
That’s the good news: black cherry juice made a modest but clear and worthwhile difference for those guys in that test. The bad news? It had no effect whatsoever on the symptom everyone actually cares about: the pain. “Relaxed elbow angle and muscle tenderness were not different between trials.”
I was going to run to the store to buy some cherry juice when I read that. Now I think I’ll just walk.
Can tart cherry juice help you sleep?
Probably not much, if at all. Supposedly the stuff contains melatonin, or melatonin precursors (and I won’t even bother going down that rabbit hole; it’s doomed to be a moot point anyway). For context, you should know that your guide is a hard-core insomniac: I have a bonified life-altering sleep disorder, narcolepsy, and narcoleptics have as much trouble staying asleep as we do staying awake. My wife, struggling with her own sleep issues, brought home some tart cherry juice — hard to find and not cheap — because a friend told her it was good for insomnia. Millions have heard the same, because the mere existence of what looks like a positive study is all the Internet needs to justify a kajillion blog posts declaring that cherries can slay our insomnia demons.
The reality is that there are just a handful of pilot studies (I could find only 3 in the last decade) with technically positive but pathetically underwhelming results.717273 There is effectively no actual science here. The onlys tory here is yet another supplement hype case study.
Vitamin D

Vitamin D deficiency is probably more common than once suspected — at least 1 in 20 people in the lowest estimates,74 and possibly many more.75 It can also cause subtle widespread pain that may be misdiagnosed as fibromyalgia and/or chronic fatigue syndrome, including symptoms like muscle and bone aching,76 fatigue and weakness, lower pain threshold, and more acute soreness after exercise that is slower to resolve.
If there’s only one supplement you’re taking for your health and your diet is decent, it should probably be Vitamin D.
Herman Gill, Examine.com editor (Vitamin D reference page)
However, vitamin D supplementation in healthy people is dubious at best. Major reviews have declared it to be nearly useless.7778 Debate rages on, of course, but there is plenty of evidence to support “reasonable doubt.”
I’ve covered this important topic in much greater detail in a separate article: Vitamin D for Pain.
Magnesium

Magnesium crystal. Some processing required before ingestion.
Magnesium is one of the essential minerals — “life finds a way,” but not without a good supply of em-gee it doesn’t! We use a lot of the stuff: it’s one of the big three mineral nutrients, along with sodium and potassium. If it’s missing, blood pressure rises, glucose tolerance drops, and our nerves get just a wee bit trigger happy. Interestingly, fixing an magnesium deficiency is actually sedating! It literally calms your nerves… and that could certainly be relevant to chronic pain. Most plausibly, it makes some sense in principle that it be helpful for cramping and/or neuropathy (pain originating from insult to the nervous system itself).
And yet pain is not on official lists of symptoms for magnesium deficiency! But it remains, just barely, possible that deficiency is a factor in some kinds of chronic pain. Not that it means much, but there are certainly plenty of anecdotes to that effect.
Despite its biological importance and being readily available in food, deficiencies seem to be surprisingly common. This might be because depletion is a side effect of some common drugs, most notably alcohol, diuretics, asthma drugs, and acid reflux drugs.79 Vexingly, it may also “hide” from routine blood tests.80
These factors make magnesium very similar to vitamin D: it might matter to a lot of people, possibly pain patients more than most, and supplementing is quite safe.81 In the extremely scammy world of supplements and nutraceuticals, vitamin D and magnesium both stand out as being less lame (especially for chronic pain patients).
Not that it has actually been studied properly, of course! It is merely plausible, and there are some encouraging hints. But the science is woefully incomplete, and what little there is to cite mostly just punctuates that.8283 To date, I am aware of just one clearly promising test of magnesium supplementation for back pain with a clear neuropathic component84 — good to know, but it’s just one study (unreplicated), and most kinds of pain are not neuropathic.
Magnesium for painful cramps
You will get told to take some magnesium for your cramps … even though many kinds of cramps aren’t caused by magnesium deficiency, and magnesium deficiency doesn’t clearly cause cramps! A 2020 review was all thumbs down for treating cramps with magnesium, except for a ray of hope about pregnancy cramps85 … but then a higher quality 2021 trial gave that a thumbs down as well.86
Note that magnesium is likely not even relevant to exercise-induced cramps.87 The whole idea has never been and is still “not supported by scientific evidence.”88
I explore this topic more in the PainSci guide to cramps and spasms.Eating your magnesium
Unlike with vitamin D, it’s downright easy to get enough magnesium from a reasonably healthy diet. Despite this, Mg deficiency is common even in wealthy places because grains and meat are poor sources, and the good sources are not nearly as popular: salad, basically. Leafy greens and nuts/seeds, especially spinach and pumpkin seeds. And potatoes are also a decent source, which is hardly a hardship. Anyone with a magnesium deficiency can suck it up and eat a nutty salad a couple times a week — or potato salad! — and Bob’s your uncle. So just eat it.
See dietary sources of magnesium.
🎶 How come you’re always such a fussy young man?
Don’t want no Captain Crunch, don’t want no Raisin Bran
Well, don’t you know that other kids are starving in Japan?
So eat it, just eat itWeird Al Yankovic, “Just Eat it”
Bathing in magnesium
Epsom salts baths are basically magnesium baths — is like going a half hour out of your way to buy stale bread from a corner store when you live next to a good bakery. Nevertheless, Epsom salts are extremely popular and widely regarded as a good method of supplementing magnesium. Which is why I cover this topic in substantial detail in my article about Epsom salts.

It’s easy to eat magnesium. You just have to be willing to eat salad. Or potatoes!
But it worked for me! The role of anecdotes and testimonials
Good! But please curb your enthusiasm: even if something really did “work for you,” that doesn’t mean it’s working for anyone else. To be considered safe and effective, a medicine or treatment has to have a solid cost-benefit profile for most people, most of the time. There are lots of treatments that are good for a handful of people, once in a blue moon. If you are one of those lucky ones, please don’t assume it means that the product is the best thing since sliced bread.
It’s more likely that you healed all by yourself, however.
It’s pretty unlikely that any nutraceuticals should get the credit for healing. It was probably all you: lucky natural healing, and maybe some of your mind powers! Placebo, in other words. Placebo is a powerful, extensively studied, and very real and interesting phenomenon. See The Strange Powers of the Placebo Effect ![]() 2:57 for a terrific 3-minute video tour of the “the many strange effects of placebos.”
2:57 for a terrific 3-minute video tour of the “the many strange effects of placebos.”
These products aren’t proven. Placebo is. Consider the startling way that placebo worked just as well as intravenous magnesium as a back pain treatment *at least two weeks* of a six month trial.89 No one could be blamed for misinterpreting that as a full-blown success.
Sometimes you can get a nice synergy between natural healing and placebo which really makes an impression. That is: if your tissues are already just starting to recover naturally (perhaps too little to have even noticed, or not enough to get excited about), and then you add a good placebo effect, recovery can seem striking and rapid. Since desperate patients are nearly always using some treatment or another at the time that this happens, it usually gets the credit — but obviously it shouldn’t. This kind of confusion about the real cause of recovery is the norm, not the exception.
Nowhere in health care do testimonials and anecdotes seem to play a bigger role than they do here: with things you put in your mouth. Unfortunately, they are pretty much worthless.

Big Suppla: Large supplement corporations are not only just as bad or worse than the pharmaceutical one, many of them are the same corporations
Cranking about Big Pharma while giving the supplements industry a free pass really chaps my arse.
It’s not that the pharmaceutical industry is innocent — certainly not! Scandals galore! Seriously major issues, even! (See Bad Pharma, by one of my favourite authors.) But paranoia about Big Pharma has reached a fever pitch that isn’t even remotely proportionate to the problem, and the most shrill critics seem unable to comprehend that the supplements industry — let’s call them “Big Suppla” — is both insanely profitable and much more unregulated and corrupt.
The double standard is maddening.
It’s also critical to understand that Big Suppla is Big Pharma. There’s huge overlap. Pharmaceutical companies own most of the big supplement companies now, and use them to produce massively profitable products with near-zero regulation. A substantial percentage of the profits generated by supplements are going straight into Big Pharma’s pockets.
A 2010 study in the British Medical Journal (which scientifically slams the dynamic duo of supplements, glucosamine and chondroitin) noted that studies funded by Big Suppla tend to produce results that were — here’s a shocker — biased in favour of supplements!90
And the supplement companies that are not owned by Big Pharma? Many of the biggest are far worse than Big Pharma: the deeply scammy multi-level marketers. More on those below.
“Big Suppla” is now evidence-based debunking
The term “Big Suppla” is intended to be a witty delivery mechanism for this debunking truth bomb. It’s quite clever. If Suppla is just as Big as Pharma… well, the whole point is that the implication is so clear that no further explanation is even required.
But does that reach people? Is it an effective debunking strategy? Someone actually tested this, and the results were positive, huzzah! Minds were changed! This is a great relief for me to hear, because I started deploying “Big Suppla” in about 2006. Mijatović et al. tested the effect of this terminology by giving about 250 people three different kinds of information about the supplements industry:91
- Neutral information was just the origins of the words “supplements” and “alternative.”
- Big Suppla information framed the industry as “powerful, profit-oriented, and unregulated.” Which it actually is.
- Baby Suppla information portrayed the supplements industry as a virtue-motivated underdog. Which it definitely is not.
The test results were better than science communicators could have hoped for. Not only did the “Big Suppla” framing change minds, it even worked on some of the hardest targets: subjects who were prone to conspiratorial thinking. Those people were more likely to be keen on supplements to begin with, but they were still persuaded by “Big Suppla.” Perhaps it’s because this debunking method exploits the “follow the money” trope that practically defines conspiratorial thinking.
Will the real underdog please stand up?
Skeptics and debunkers do a lot of joking about how we’re in the wrong line of work, because it would obviously be so much easier to get rich if only we were willing to just lie, tell people whatever they want to hear, and sell easy solutions to hard problems. Which is exactly what the bad guys do. For instance, Alex Jones' Infowars Store — dominated by supplements and survival gear — Made $165 Million Over 3 Years (HuffPost.com). But Alex Jones constantly told his followers things like, “As much begging as I do, we can barely pay the bills.”
That would be a lie even if he’d only made one million dollars, instead of one hundred sixty-five million.
Defy that lie! Tell the truth: false hope and fear are highly profitable, while truth and realism are the actual underdogs.
The Multi-Level Marketing Connection: Supplements and Fraud
Many nutraceuticals and supplements are sold using “multi-level marketing” (MLM), in which products are mostly sold internally to recruited distributors, and the real money is made by getting kickbacks from all your recruits and their recruits. I have direct personal experience with MLMs, having been sucked in by one of them for almost a year in the early 1990s — a very embarrassing chapter of my life, but full of valuable lessons. I know from that experience all too well that MLMs success depends on becoming an intense proselytizer: you have to not only sell the product, but sell the idea that the product is so great that your customer should become a distributor.
The whole thing is powered by hype and dreams of getting rich quick.
That’s all kind of gag inducing, but MLMs are actually fundamentally fraudulent. Many people are under the false impression that some MLM schemes are “not really a pyramid” or otherwise okay, but even the best of them are still dubious, distasteful, and harder to make money with than it seems at first.
It says something about supplements that they are so routinely sold by such scammy methods. Probably every imaginable product has been sold via MLMs, but supplements and snake oils are that industry’s favourite product category by far.
Alternative medicine practitioners are juicy targets for MLM recruiters. Because of their, er, “accepting nature,” they are easily recruited, and simultaneously become victims to a scam themselves … and then start passing it on to their patients. For instance, it’s extremely common for chiropractors and naturopaths to sell nutraceuticals and supplements in their offices, and they are often distributing for an MLM as well as retailing. In my career in massage therapy I encountered many colleagues who attempted to recruit me into an MLM, usually to sell supplements.
MLMs practically constitute a subculture of alternative medicine. Make of that what you will.
Protandim: The most prominent MLM-powered supplement
Protandim is a patented “blend of phytonutrients” from a multi-level marketing company, with slick marketing emphasizing anti-aging effects: “the only supplement clinically proven to reduce oxidative stress by 40%, slowing down the rate of cell aging to the level of a 20 year old.” Anti-aging claims should always set off every caveat emptor alarm you’ve got. The product allegedly treats pain and inflammation via antioxidant effects and “activating” the Nrf2 protein (regarded as the “master activator” of antioxidant gene expression). The biology of antioxidants is dizzyingly complex, and only large, high-quality human clinical trials can establish the efficacy of any product that tries to “hack” it.
There have been a handful of test-tube and animal studies, no human studies related to pain at all, and only two human studies — both irrelevant, both negative. In 2012, Dr. Hall reported on a new human study of Protandim, but still not a trial and almost comically irrelevant … and negative: “Protandim was significantly (p<0.01) worse than placebo. No wonder [Protandim fans] are not bragging about this study!” (Dr. Hall has written quite a bit about Protandim on ScienceBasedMedicine.org over the years.92)
Protandim proponents believe there’s lots of supporting research, but of course that’s what they all say. And the FDA disagrees.
Potential side effects are unstudied and unknown — another red flag for anything that allegedly has potent benefits.
Two sections of this page are reserved for members only, about 2000 words of content and 10% of the article:
- Coenzyme Q10 (~600 words)
- Probiotics and meddling with your microbiome (~1400 words)
Most PainScience.com content is free and always will be.? Membership unlocks extra content like this for USD $5/month, and includes much more:
Almost everything on PainScience.com is free, including most blog posts, hundreds of articles, and large parts of articles that have member-areas. Member areas typically contain content that is interesting but less essential — dorky digressions, and extra detail that any keen reader would enjoy, but which the average visitor can take or leave.
PainScience.com is 100% reader-supported by memberships, book sales, and donations. That’s what keep the lights on and allow me to publish everything else (without ads).
- → access to many members-only sections of articles +
And more coming. This is a new program as of late 2021. I have created twelve large members-only areas so far — about 40,000 words, a small book’s worth. Articles with large chunks of exclusive content are:
- Quite a Stretch
- Does Epsom Salt Work?
- Heat for Pain and Rehab
- Your Back Is Not Out of Alignment
- Trigger Point Doubts
- Does Fascia Matter?
- Anxiety & Chronic Pain
- Does Massage Therapy Work?
- Does Posture Matter?
- A Deep Dive into Delayed-Onset Muscle Soreness
- Does Ultrasound or Shockwave Therapy Work?
- A Painful Biological Glitch that Causes Pointless Inflammation
- Guide to Repetitive Strain Injuries
- Chronic, Subtle, Systemic Inflammation
- Vitamins, Minerals & Supplements for Pain & Healing
- Reviews of Pain Professions
- Articles with smaller members sections (more still being added):
- → audio versions of many articles +
There are audio versions of five classic, big PainSci articles, which are available to both members and e-boxed set customers, or on request for visually impaired visitors, email me. See the Audio page. ❐
I also started recording audio versions of some blog posts for members in early 2022. These are shorter, and will soon greatly outnumber the audio versions of the featured articles.
- → premium subscription to the PainSci Updates newsletter +Sign-up to get the salamander in your inbox, 0–3 posts per week, mostly short, sometimes huge. You can sign-up for free and get most of them; members get more and their own RSS feed. The blog has existed for well over a decade now, and there are over a thousand posts in the library. ❐

Change or cancel plans any time. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism. For more information, see the membership page. ❐
Coenzyme Q10 (CoQ10)
CoQ10 sounds like a Star Wars droid. Bleep bloop? But it’s a vitamin-like nutrient… of sorts. It’s also known as “ubiquinone,” so if nothing else this stuff sounds cool (and it’s a useful ingredient in cosmetics, so there’s that).
It’s an obscure nutrient and antioxidant with all the usual alleged benefits of antioxidants, and all the caveats that go with that (seed of truth but too much hype, etc). It’s everywhere (hence “ubiqinone”), it’s found every cell that breathes, and mainly in the mitochondria. The logic for supplementing it is generally the simplistic logic of all supplements: if this stuff is important to biology, then more must be better. 🙄
I’ve only included CoQ10 here because it’s also popular for relieving the muscle aching side effect of the statin drugs — statin-associated myalgia (SAM) — which might impair CoQ biosynthesis. Every part of that statement is controversial:
- We don’t know that SAM is a real side effect to begin with.
- Even if SAM is real, we don’t know that it’s caused by impairment of CoQ biosynthesis.93
- And the bottom line (still assuming SAM is real), taking CoQ10 orally does not actually seem to help anyone much: decent trials and meta-analyses are discouraging.9495
Let’s get into SAM a bit more, because it’s the entire premise for a lot of CoQ supplementing.
The drugs that lower our blood cholesterol, like Lipitor and Crestor, might also cause pain. Statins are important and widely used drugs, and their deleterious effect on muscle is widely considered a diagnosable condition.96 A few patients, about 1 in 10,000, get a more obvious, serious case of muscle poisoning, rhabdomyolysis,97 and an even rarer and more serious condition afflicts 1 in 100,000: statin-associated autoimmune myopathy.9899
And yet there is also serious confusion and controversy about the prevalence of statin myalgia.100 There’s even clear evidence that it could be some kind of illusion or misunderstanding.101 in one head-scratcher of a study, taking statins only increased pain when patients knew they were taking statins.102 So that’s weird! The truth is probably “all of the above” and “it’s complicated” — it seems likely that some patients are genuinely intolerant of statins, while others are suffering from fear of statins and/or some other cause of musculoskeletal pain (of which there are many). There might also be some tricky X-factors, like vitamin D deficiency, which seems to be linked to statin myalgia.103
So that’s the shaky premise that CoQ supplementation is resting on — and even if all that uncertainty went away, there would still be the evidence showing that CoQ10 doesn’t actually seem to be relieving much pain.
Probiotics and meddling with your microbiome
Probiotics are pills full of living microorganisms that, in theory, can improve the health of the larger and more diverse community of wee beasties in our bellies.
We each have a fully fledged ecosystem in our GI tracts, the gut flora, a dense jungle of diverse micro-critters (bacteria). “Gut health” refers to the health of that ecosystem of thousands of species.105
If the gut microbiome gets out of whack — if the circle of life down there gets a bit scribbly (formally known as “dysbiosis”) — that has consequences. Digestive consequences at the least: gas, diarrhea, constipation, pain, and so on.
But grumbly guts might be the least of your worries. At worst, poor gut health is a driver of disease, even psychological illness (“gut-brain axis”). More literally than “you are what you eat,” you actually are what lives your intestines. It may be impossible to be healthy in general with a muddled gut flora — and that may even be somewhat common, modern diets being a bit of a junk food hellscape.
Legitimate science and a bonanza of junk science and snake oil
Junk food is not the only junk we consume regularly: we also live in an era of unprecedented bullshit and hype about every conceivable aspect of health, and the microbiome revolution has been a magnet for cranks and quacks.
It’s been a particular boon for naturopaths, a profession that was thriving on nutrition claims and supplement sales long before there were headlines about gut health. There’s an eyebrow-raising story right here in Vancouver this week about a naturopath who was selling fecal transplants — very closely related to probiotics — basically by harvesting poop from family members.106 To cure autism, no less. 🙄
Almost all of the legitimate research on this topic so far has been correlative (looking for smoke rather than fire) and preclinical (precious little study of how to actually help people by tinkering with their microbiomes).107 And yet many papers about gut health have already strongly influenced medicine (and quackery).
There does seem to be a robust expert consensus that the microbiome is an important part of our health.108 But can we fix it? Is this stuff ready for the clinic? Let alone self-treatment with supplements?

A scanning electron microscope view of Lactobacillus acidophilus, a common denizen of the gut, and a bacterial species with even more of a relationship (a much older one) with Homo sapiens than cows or chickens. Image by Mogana Das Murtey and Patchamuthu Ramasamy, CC BY-SA 3.0, via Wikimedia Commons / colorized, caption removed.
“Just add bacteria”: poop bugs in pills to the gut rescue?
Enter probiotics. These are actual intestinal bacteria in a pill. Gut microbes. Poop bugs in gel-caps.
They aren’t quite exactly “poop” themselves, but they are a major poop ingredient. The theory is that they are like helpful, hard-working immigrants, new citizens that diversify the intestinal workforce, stabilize its economy. They are often described as “good bacteria,” as though they just can’t help but clean the place up.
But probiotics are mostly just extra bacteria of the species typically found in large numbers in a healthy gut. The idea is quite simplistic. It’s like trying to improve the health of a jungle by introducing more monkeys… because healthy jungles have lots of monkeys. But is “just add monkeys” actually helpful to a sick jungle? Probably not — ecology is more complicated than that. And, similarly, “just add bacteria” hardly a guaranteed recipe for gut health salvation either.
Less cynically, the bacteria in probiotics are indeed typical citizens of healthy microbiomes, and it’s definitely not crazy to think that adding more of them might be a normalizing force.
But we have only barely begun to understand how the microbiome even works, let alone how to manipulate it therapeutically. Just flooding your tubes with an assortment of common gut tenants is definitely a wee bit of a hail mary pass. Even if it does work for some people, it is also going to fail for many others, because by nature the composition of the microbiome is highly individual, as unique as a fingerprint — it’s one of the things that makes us who we are, and everyone is different… so “you’re mileage may vary.”
Probiotics science (especially for pain)
According to the studies, sometimes probiotics do seem to help some kinds of health problems. The evidence is generally “promising” — a word that strikes pessimism into heart of any good science junky, because “a promising treatment is the larval stage of a disappointing one.”109 Very few “promising” treatments for anything ever actually get validated.
But there’s less promising and there’s more promising, and the science of probiotics really does seem to be on the happier end of that spectrum, especially for abdominal and digestive distress (like irritable bowel syndrome). So that’s nice.
Not so much for other kinds of pain though — and that’s the focus of this article. It’s not entirely if or how gut health affects chronic body pain disorders.110 Many people with chronic pain try probiotics, especially if they have unexplained pain (the worse and weirder your pain, the more open-minded people get). The general idea is that gut stuff seems to drive all sorts of inflammatory stuff (as a well-informed friend of mine put it). So:
poor gut health
⬇️
systemic inflammation?
⬇️
higher vulnerability to many kinds of pain?
“Inflammation” is basically synonymous with “immune system activity,” and poor gut health is analogous to a chronic infection. So a complex immunological reaction is certainly plausible, which is probably how the microbiome affects general health in the first place. And we already know that anything that’s good for gut health is probably good for the rest of our health, and a “rising tide lifts all boats.”
That’s about as specific as the rationale can get, but it’s enough to work with. Using probiotics as a general health tonic is not an unreasonable strategy for desperate patients trying to solve an extremely nasty problem,111 … but it is a crapshoot, make no mistake.
I won’t be able to cite much evidence on this topic, because very few probiotics trials are relevant to pain.
There is some research on probiotics for rheumatoid arthritis, which might be relevant to other common painful problems. If probiotics can calm down the 800-lb gorilla of an inflammatory arthritis, it might also plausibly have an effect on back pain or fibromyalgia. But a review 2017 review in Clin Rheumatol was a classic more-study-needed paper: a bit of a signal in the noise (a common inflammatory biomarker was reduced), but clinically? Meh! Probiotics didn’t actually affect the disease.112 In 2022, a review in Nutrients wasn’t even really in the “promising” category:113
Probiotic supplementation might decrease RA activity with a moderate decrease effect on CRP, but lack of evidence and studies' heterogeneity [apples-to-oranges data] do not allow us to propose them to patients with inflammatory arthritis to control their disease.
Meanwhile, a prominent and authoritiative website says, “If you have an inflammatory type of arthritis, probiotics may be especially important”! That “may be” is doing an awful lot of heavy lifting there. 🙄
Probiotics side effects and harms
The probiotics arm of the supplements industry seems as premature as anything I’ve ever seen in this business: a commercial empire rapidly grown from one seed of truth. It’s an obvious “gold rush” to sell probiotics to consumers for every imaginable condition. And we all know that gold rushes can get a bit ruthless and fuel all kinds of shenanigans.
It’s problematic even if we assume that the products all contain what they say they contain, which hardly seems like a safe bet in that barely-regulated industry.114
Remember, these are bacteria, and they can grow out of control and become an infection like any other organism. It’s not likely, but it’s certainly possible.
And bacteria also poop chemicals! Chemicals that may be toxic or just kind of biochemically random. Your microbiome is basically a drug factory. Bacteria produce all kinds of compounds, and that is a major reason why it is relevant to our general health, but that sword has another edge.
Moderate infusions of various common gut bacteria are unlikely to be a serious problem — there’s no known public health disaster unfolding — but on the other hand the supplements industry is also hard at work “innovating” and producing new products with new claims. Quality control could slip.
Reckless overdosing is also a risk. “More is better” thinking is pervasive in healthcare, and plenty of people have made this mistake. I’ve gotten one reader anecdote about excessive probiotics just causing substantial diarrhea, rather than helping IBS.
Probiotics bottom lines
Significant harm from probiotics may be unlikely, but so is significant benefit for most pain patients. I see no specific scientific reason to think that probiotics are going to be useful for patients with any kind of chronic pain (other than irritable bowel syndrome).
Meanwhile, there are clearly safer (and probably cheaper) alternatives, such as live foods (e.g. yogurt, kefir) or even just a substantial diversification of diet.
But I can also see good scientific reasons for some patients to try them — ideally favouring simpler products from well-known brands (which have more to lose from a product disaster). The links between gut health and inflammatory diseases are compelling, and the fairly strong promising-ness of the general research is enough to justify cautious experimentation when the stakes are high.
↑ MEMBERS-ONLY AREA ↑
Information is Beautiful
Here’s a great way to conclude this tour of nutraceuticals: InformationIsBeautiful.net publishes a brilliant, beautiful and interactive visualization of the popularity and effectiveness of popular dietary supplements, which they have kept up-to-date since 2009. It’s a really good graph, but notice that it neglects a crucial factor: risk. No biological benefit of anything you put into your body can ever be meaningful without contrasting it with the possible dangers of doing so, and unfortunately that consideration is routinely overshadowed by discussion — and lovely diagramming — of the possible benefits. Nevertheless, it’s an extremely interesting (and pretty) visualization:
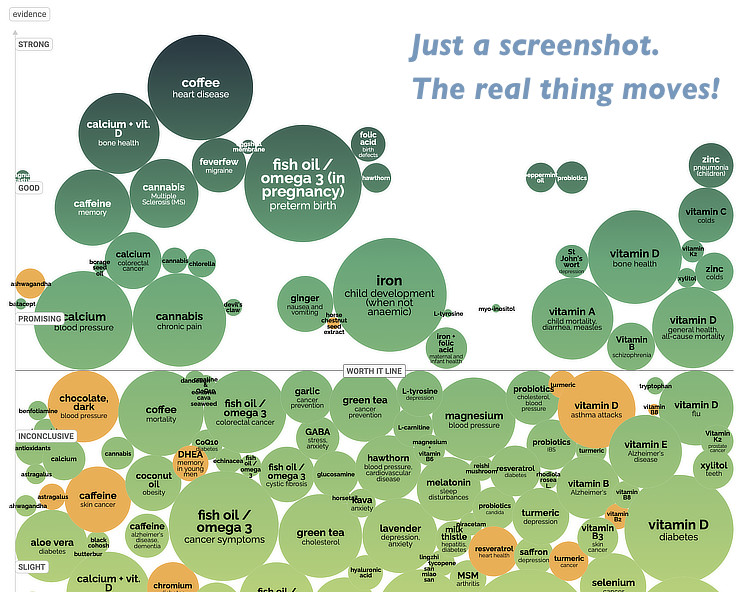
Rather a lot of products are below the “worth it” line! There are also many above the “worth it” line, but please notice that few of those have anything to do with body pain. Just cannabis (and feverfew for migraine)… and cannabis only barely, and even that’s debatable and highly complex (see Marijuana for Pain). Although I mostly agree with what I see here, I think — as always — that evidence is given too much credit for being “promising” when it’s actually really weak sauce.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Related Reading
- Chronic, Subtle, Systemic Inflammation — One possible sneaky cause of puzzling chronic pain
- Anxiety & Chronic Pain — A self-help guide for people who worry and hurt This article covers prebiotics and turmeric/curcumin, which both show some minor potential as treatments for anxiety.
- Other pain medications:
- The Science of Pain-Killers — A user’s guide to over-the-counter analgesics like acetaminophen, ibuprofen, and more
- Voltaren Gel: Does It Work? — The science of the topical pain-killers, which can be effective without dosing your entire system
- Opioids for Chronic Aches & Pains — The nuclear option: Oxycontin, codeine and other opioids for musculoskeletal problems like neck and back pain
- Does Epsom Salt Work? — The science and mythology of Epsom salt bathing for recovery from muscle pain, soreness, or injury
- Marijuana for Pain — The hype versus the science! What does the evidence actually show about cannabis and chronic pain?
- Vitamin D for Pain — Is it safe and reasonable for chronic pain patients to take higher doses of Vitamin D? And just how high is safe?
- Does Arnica Gel Work for Pain? — A detailed review of popular homeopathic (diluted) herbal creams and gels like Traumeel, used for muscle pain, joint pain, sports injuries, bruising, and post-surgical inflammation
- Homeopathy Schmomeopathy — Homeopathy is not a natural or herbal remedy: it’s a magical idea with no possible basis in reality
- Muscle relaxants — This topic is covered in several of my books in detail — low back pain, neck pain, trigger points, frozen shoulder, headaches. There is also condensed (but free) information about them in Cramps, Spasms, Tremors & Twitches.
What’s new in this article?
35 updates have been logged for this article since publication (2010). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
2025 — Refinements to the discussion of indirect harms. That section is now called: “6 ways being a sucker for supplements can go wrong.”
2024 — Minor science updates and additions about creatine.
2024 — Added a sidebar summarizing the potential harms of supplements.
2022 — Added a section about probiotics and the microbiome. Can gel caps full of “good bacteria” treat pain outside the gut?
2022 — Added a section about Coenzyme Q10 and statin-associated myalgia (SAM).
2022 — Added a section, “‘Big Suppla’ is now evidence-based debunking.”
2022 — Added important disclaimer about adulteration and contamination, regarding concerns about the accuracy of a key paper on that topic.
2021 — Substantive science update on the efficacy of treating pain with magnesium.
2021 — Added warning about the slaughter of sharks required for collagen production.
2021 — Added minor new citation and commentary: “Survey says most people don’t care what the science says.”
2021 — Several miscellaneous edits after promoting the rebooted version of this article. Most notably, I added some safety information about curcumin, and a full-blown science update about tart cherry juice for insomnia, but there have been many other minor changes.
2021 — Tied up some loose ends and corrected a bunch of minor errors that crept in during the wave of recent updates. Page is in great shape now, I think. The main thing missing? Some popular supplements! Mostly in the vitamins/minerals category. I will chip away at them over time, of course.
2021 — Many minor improvements to the topics of Glutamine and arginine, branched-chain amino acids, and collagen.
2021 — Science and citation update on the topic of supplement contamination and adulteration.
2021 — A thorough science update on bromelain — such as it is. More like an update on the lack of science. But the section is much more informative now, even if disappointingly so.
2021 — Complete overhaul of everything about ergogenic aids in general, their possible relevance to pain, and creatine as the primary example — still actually effective for muscle fatigue (hooray, something that works!), but probably not for pain.
2021 — Revision and science updates for the glucosamine and chondroitin section. I was particularly exasperated by and sassy about these embarrassingly unimpressive supplements.
2021 — Added an adapted version of Peter Brannen’s highly relevant joke about the simplicity of supplementation versus the complexity of metabolic pathways.
2021 — Rewrote the fish oil section, with significant science updates.
2021 — Major reorganization of the article to make it more useful and comprehensive. Added topics, removed others. A variety of other science updates to come.
A simple version of this article was initially published in January 2010. It was updated semi-regularly for a year, and finally reached a critical mass of worthiness first thing in January 2011. Regular updates have continued ever since.
2021 — Proofreading and editorial polish: corrected about 20 minor errors.
2020 — Minor science update, a couple new citations, and a new section about anti-inflammatory nutrition.
2017 — Added a small but important public service announcement about supplement contamination, based on Rao et al.
2017 — Added a citation about the effect of caffeine on performance.
2017 — Added a footnote about the (lack) of evidence concerning the long term effects ogf caffeine on pain.
2016 — Added new section about vitamin D.
2016 — Added a mobile-only article summary.
2016 — Minor science update about glucosamine.
2012 — Turned around on creatine. That stuff seems to work as advertised.
2012 — Added a reference to a new Protandim study, only the second ever in humans … and it’s irrelevant and negative.
2011 — Added collagen, and some comments about bioavailability.
2011 — A couple more references for arginine and glutamine. Also: improvements to layout of main supplements table.
2011 — Extensive upgrades and expansion of information about glutamine and arginine.
2011 — Added reference information about Protandim, and “bottle of hope” image.
2011 — Added more evidence of underwhelming benefit to chondroitin sulfate.
2011 — Added more information about the connection between nutraceuticals multi-level marketing.
2011 — Added “safety” column and data to main chart.
2011 — Added Protandim. Plus new section, “But it worked for me!” Includes a link to a terrific video: The Strange Powers of the Placebo Effect ![]() 2:57
2:57
January 2010 — Extensive upgrades before promoting this article for the first time.
2010 — Publication.
Notes
- Rodriguez NR, DiMarco NM, Langley S, et al. Position of the American Dietetic Association, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and athletic performance. J Am Diet Assoc. 2009 Mar;109(3):509–27. PubMed 19278045 ❐
This is a dense paper on how nutrition can enhance athletic performance. It describes in great detail the position of the American Dietetic Association, Dietitians of Canada, and the American College of Sports Medicine, so it’s very “official” (for whatever it’s worth). Some highlights:
- they endorse sports drinks (which badly undermines the credibility of these recommendations, because sports drinks are ridiculous, please see Wagner)
- energy and macronutrient needs, especially carbohydrate and protein, must be met when exercising hard
- vitamin and mineral supplements are not needed if adequate energy to maintain body weight is consumed from a variety of foods
- ergogenic aids are poorly regulated and should be used with caution
And of course they recommend the services of a “qualified sports dietitian and in particular in the United States, a Board Certified Specialist in Sports Dietetics.”
- See Do calcium supplements cause heart attacks?
- Warensjö E, Byberg L, Melhus H, et al. Dietary calcium intake and risk of fracture and osteoporosis: prospective longitudinal cohort study. BMJ. 2011;342:d1473. PubMed 21610048 ❐ PainSci Bibliography 55295 ❐
Does long-term supplementation with calcium reduce the risk of fractures? The answer, based on this study, appears to be no: "Gradual increases in dietary calcium intake above the first quintile in our female population were not associated with further reductions in fracture risk or osteoporosis." My interest in this evidence is mainly because it’s a good example of how supplements continue to turn out to be less useful than we all hoped in the 20th Century.
- Chen F, Du M, Blumberg JB, et al. Association Among Dietary Supplement Use, Nutrient Intake, and Mortality Among U.S. Adults: A Cohort Study. Ann Intern Med. 2019 May;170(9):604–613. PubMed 30959527 ❐ PainSci Bibliography 52693 ❐
- This is the “healthy user effect.” See Who takes dietary supplements, and why?
- White CM. Dietary Supplements Pose Real Dangers to Patients. Ann Pharmacother. 2020 08;54(8):815–819. PubMed 31973570 ❐ “Microbial and heavy metal contamination, adulteration with synthetic drugs (including drugs banned from the United States), substituting herbs, and fraudulently specifying ingredients on the label have all occurred.”
- Rao N, Spiller HA, Hodges NL, et al. An Increase in Dietary Supplement Exposures Reported to US Poison Control Centers. J Med Toxicol. 2017 Jul. PubMed 28741126 ❐
- Martínez-Sanz JM, Sospedra I, Ortiz CM, et al. Intended or Unintended Doping? A Review of the Presence of Doping Substances in Dietary Supplements Used in Sports. Nutrients. 2017 Oct;9(10). PubMed 28976928 ❐ PainSci Bibliography 51803 ❐
Substances prohibited by WADA were found in most of the supplements analyzed in this review. Some of them were prohormones and/or stimulants. With rates of contamination between 12 and 58%, non-intentional doping is a point to take into account before establishing a supplementation program.
- Walpurgis K, Thomas A, Geyer H, Mareck U, Thevis M. Dietary Supplement and Food Contaminations and Their Implications for Doping Controls. Foods. 2020 Jul;9(8). PubMed 32727139 ❐ PainSci Bibliography 51802 ❐
Even though controversial positions concerning the effectiveness of dietary supplements in healthy subjects exist, they are frequently used by athletes, anticipating positive effects on health, recovery, and performance. However, most supplement users are unaware of the fact that the administration of such products can be associated with unforeseeable health risks and AAFs in sports. In particular anabolic androgenic steroids (AAS) and stimulants have been frequently found as undeclared ingredients of dietary supplements, either as a result of cross-contaminations due to substandard manufacturing practices and missing quality controls or an intentional admixture to increase the effectiveness of the preparations.
- Mathews NM. Prohibited Contaminants in Dietary Supplements. Sports Health. 2018;10(1):19–30. PubMed 28850291 ❐ PainSci Bibliography 51800 ❐
Poor manufacturing processes and intentional contamination with many banned substances continue to occur in dietary supplements sold in the United States. Certain sectors, such as weight loss and muscle-building supplements, pose a greater threat because they are more likely to be contaminated. Athletes will continue to be at risk for adverse events and failed doping tests due to contaminated dietary supplements until legislation changes how they are regulated.
- This is why many drugs have to be injected: because digestion destroys them, you have to put them right into the blood stream so that they can be used by the body. Some substances can be eaten and absorbed, but many can’t. “Bioavailability” is a significant problem with the logic of several popular nutraceuticals.
- For instance, glucosamine isn’t curing anyone’s back pain. I’ve been working in this field a long time, and I have yet to meet the patient who has told me “hey, glucosamine really did the trick! My pain is gone!” Not one. You get “glucosamine took the edge off a little … maybe” and “I think it’s helping” and “I’m pretty sure,” but there were 5 other possibilities at the same time and the patient is back in trouble a month later. Another example: lots of people claim that they “can’t live without” their glucosamine for their bum knee, but I have yet to meet one who actually no longer had any significant knee pain.
This is a common, odd thing about human nature: people paradoxically tend to brag about a treatment for a problem that isn’t actually solved; if it were solved, they probably wouldn’t even be thinking or talking about it. People without knee pain don’t run around saying, “I used to have knee pain, but now I take glucosamine and I never have the slightest problem.” This is exactly like victims of faith healers who are actually still sick but nevertheless believe they were healed — they rationalize the cognitive dissonance away by claiming that God is simply testing them. This is beautifully explained and illustrated in Radiolab’s signature storytelling style in this episode about placebo, and James Randi and Banachek give another amazing example talking about their adventures debunking faith healer Peter Popoff (interview in this Skeptics Guide to the Universe episode.)
- Blendon RJ, Benson JM, Botta MD, Weldon KJ. Users' views of dietary supplements. JAMA Intern Med. 2013 Jan;173(1):74–6. PubMed 23403846 ❐
Blendon et al. did a survey of 1579 adults looking for users of dietary supplements (but not vitamins or mineral): 38% of those took some supplement in the past two years, and 13% took a supplement regularly, with fish oil topping the chart. Their reasons for taking supplements included: “to feel better” (41%), “improve energy levels” (41%), “boost your immune system” (36%), “digestive issues” (28%), and “lower cholesterol” (21%). Incredibly, only a quarter of them thought they would pass on supplement if a trial concluded it was ineffective.
- www.theatlantic.com [Internet]. Yong E. The Pandemic's Biggest Mystery Is Our Own Immune System - The Atlantic; 2021 May 18 [cited 21 May 18]. PainSci Bibliography 51780 ❐
An extremely well-written piece bout the bewildering complexity of the immune system in the context of the COVID pandemic. As rich an article as it is, I primarily cite it for the useful sentiment baked right into the title: that immunology is so complex that even the most educated guesses about how it works are routinely wrong or incomplete.
- Tsuchiya Y, Yanagimoto K, Nakazato K, Hayamizu K, Ochi E. Eicosapentaenoic and docosahexaenoic acids-rich fish oil supplementation attenuates strength loss and limited joint range of motion after eccentric contractions: a randomized, double-blind, placebo-controlled, parallel-group trial. Eur J Appl Physiol. 2016 Jun;116(6):1179–88. PubMed 27085996 ❐ A small 2016 test of the effect of eight weeks of fish oil supplementation on recovery from weight lifting in 24 men. The researchers measured outcomes in many ways. Although they observed some benefits, the results were modest, and only for range of motion and strength, not for pain (or several other measures, such as various blood test results). There were an assortment of isolated minor wins for fish oil — e.g. less pain on day 3 after the exercise — but that’s to be expected in any set of data (especially when it comes from a group of subjects this small).
- Thielecke F, Blannin A. Omega-3 Fatty Acids for Sport Performance-Are They Equally Beneficial for Athletes and Amateurs? A Narrative Review. Nutrients. 2020 Nov;12(12). PubMed 33266318 ❐ PainSci Bibliography 51787 ❐
- Chowdhury R, Stevens S, Gorman D, et al. Association between fish consumption, long chain omega 3 fatty acids, and risk of cerebrovascular disease: systematic review and meta-analysis. BMJ. 2012 Oct;345:e6698. PubMed 23112118 ❐ PainSci Bibliography 51781 ❐ This review compared many trials of eating fish to many trials of eating fish oil, finding that fish on a plate is measurably better. Based on the data they crunched, eating actual fish twice week reduces stroke risk by about 6% compared to fish oil supplements (which showed a benefit, technically, but a statistically insignificant one). Maybe omega-3 fatty acids just don’t have the same effect in isolation. Or maybe eating more fish just displaces less healthy foods? There are a couple of very beefy paragraphs in the paper discussing all the possible explanations for the difference. Or maybe the data is just misleading! See next reference to Chen et al.!
- Chen C, Huang H, Dai QQ, et al. Fish consumption, long-chain omega-3 fatty acids intake and risk of stroke: An updated systematic review and meta-analysis. Asia Pac J Clin Nutr. 2021;30(1):140–152. PubMed 33787050 ❐ Chen et al. is a very similar study to Chowdhury et al.… but they did not find a difference between fish and fish oil. D’oh!
- Dr. Harriet Hall on ScienceBasedMedicine.org: “The amount of glucosamine in the typical supplement dose is on the order of 1/1000th or 1/10,000th of the available glucosamine in the body, most of which is produced by the body itself. [Dr. Wallace Sampson] says, ‘Glucosamine is not an essential nutrient like a vitamin or an essential amino acid, for which small amounts make a large difference. How much difference could that small additional amount make? If glucosamine or chondroitin worked, this would be a medical first and worthy of a Nobel. It probably cannot work.’”
- In his 2007 book Snake Oil Science, R. Barker Bausell examined all the research evidence. He analyzed the strengths and weaknesses of a Cochrane Review of glucosamine with 2570, a NEJM study with 1583 patients, and an Annals of Internal Medicine study of 222 patients. Based on these large tests, Bausell concluded that glucosamine is ineffective.
- Towheed TE, Maxwell L, Anastassiades TP, et al. Glucosamine therapy for treating osteoarthritis. Coch. 2005;(2):CD002946. PubMed 15846645 ❐
This prominent Cochrane review — #4 in mid-2012 — concludes that glucosamine “failed to show benefit in pain and WOMAC function” with one kind of glucosamine product (non-Rotta), but succeeded with another (Rotta), coming dangerously close to cherry-picking favourable results. Maybe glucosamine of one sort works while others do not, and maybe the authors simply wanted good news and found it in some of the data. For a good taste of how conflicting and confused the evidence still is, read the introduction to his 2009 update — it starts out very positive, but then proceeds with a litany of caveats that makes one doubt the enthusiastic opening statements.
- Wilkens P, Scheel IB, Grundnes O, Hellum C, Storheim K. Effect of Glucosamine on Pain-Related Disability in Patients With Chronic Low Back Pain and Degenerative Lumbar Osteoarthritis: A Randomized Controlled Trial. JAMA. 2010 Jul 7;304(1):45–52. PubMed 20606148 ❐ PainSci Bibliography 55639 ❐
This straightforward and good quality test of glucosamine for low back pain — the first of its kind — found no therapeutic benefit by any measure: “Our findings suggest that glucosamine is not associated with a significant difference in pain-related disability, low back and leg pain, health-related quality of life, global perceived effect of treatment.” Although statistically insignificant, disability was actually greater in those who took glucosamine, and “approximately 30% of the patients reported mild adverse events.” They tested 250 adults who’d had low back pain for more than 6 months, and degenerative lumbar osteoarthritis.
Almost 30% of patients had mild side effects, and 10 patients withdrew because of them, but there were no serious problems.
See also Dr. Harriet Hall’s analysis. She writes:
[This study is] well-designed, randomized and double blind, with 250 subjects, a low drop-out rate, a 6 month duration with a one year follow-up, appropriate clinical criteria for improvement (disability, pain, quality of life, use of rescue medications), intention-to-treat analysis, and even an ‘exit poll’ to insure that blinding had been effective, that patients couldn’t guess which group they were in. It used the doses of glucosamine sulfate that had been called for by critics of previous studies. It was done in Norway, where glucosamine is a prescription drug (in the US it is marketed as a diet supplement under DSHEA regulations so there is a greater possibility of dosage variations and impurities); it was independently funded, with no involvement of industry.
- Sawitzke AD, Shi H, Finco MF, et al. Clinical efficacy and safety of glucosamine, chondroitin sulphate, their combination, celecoxib or placebo taken to treat osteoarthritis of the knee: 2-year results from GAIT. Ann Rheum Dis. 2010 Aug;69(8):1459–64. PubMed 20525840 ❐ PainSci Bibliography 54963 ❐
Even though knee osteoarthritis makes many lives miserable, long-term studies of treatment options are surprisingly few. This badly needed and good quality experiment compared the efficacy and safety of the two most popular supplements for pain — glucosamine, chrondroitin sulphate — as well as the painkiller celecoxib. They were pitted against each other, a supplement combination, and a placebo, in several hundred patients for two years (valuable long-term data that didn’t really exist before).
Alas, none of the treatments worked — less than 2% of patients enjoyed even a 20% improvement. The study authors conclude: “no treatment achieved a clinically important difference in … pain or function as compared with placebo.” As well, adverse reactions were similar in all groups; serious adverse reactions were rare for all treatments. This adds considerable weight to the already substantial evidence that most popular supplements are totally bogus.
But safe! “All of the tested therapies appeared to be generally safe and well tolerated over a two-year period.”
- Wandel S, Jüni P, Tendal B, et al. Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: network meta-analysis. BMJ. 2010 Sep 16;341:c4675. PubMed 20847017 ❐ PainSci Bibliography 55001 ❐
This is a large scale analysis of ten of the largest, best trials of glucosamine and chondroitin, compared with placebo in over 3800 patients. No effect at all was found. Neither one, on its own or in combination, could outperform placebo. Pain was not reduced. Cartilage was not restored.
Predictably, experiments funded by the supplements industry — “Big Suppla”! — produced results biased somewhat in favour of supplements, but even those were still statistically insignificant.
The authors concluded: “Compared with placebo, glucosamine, chondroitin … do not reduce joint pain or have an impact on narrowing of joint space. Health authorities and health insurers should not cover the costs of these preparations, and new prescriptions … should be discouraged.”
- American Academy of Orthopaedic Surgeons. Treatment of Osteoarthritis of the Knee – 2nd Edition. AAOS.org. 2013. PainSci Bibliography 54555 ❐ They also slammed acupuncture, “lube jobs” (injection of joint lubricant), and surgical lavage and debridement.
- Simental-Mendía M, Sánchez-García A, Vilchez-Cavazos F, et al. Effect of glucosamine and chondroitin sulfate in symptomatic knee osteoarthritis: a systematic review and meta-analysis of randomized placebo-controlled trials. Rheumatol Int. 2018 Aug;38(8):1413–1428. PubMed 29947998 ❐
- Gregori D, Giacovelli G, Minto C, et al. Association of Pharmacological Treatments With Long-term Pain Control in Patients With Knee Osteoarthritis: A Systematic Review and Meta-analysis. JAMA. 2018 12;320(24):2564–2579. PubMed 30575881 ❐ PainSci Bibliography 51785 ❐
- Gabay C, Medinger-Sadowski C, Gascon D, Kolo F, Finckh A. Symptomatic effects of chondroitin 4 and chondroitin 6 sulfate on hand osteoarthritis: a randomized, double-blind, placebo-controlled clinical trial at a single center. Arthritis Rheum. 2011 Sep 6;63(9). PubMed 21898340 ❐
- Clegg DO, Reda DJ, Harris CL, et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N Engl J Med. 2006 Feb;354(8):795–808. PubMed 16495392 ❐
This is one of the largest and best designed studies of glucosamine and chrondroitin sulfate to date. More than 1500 patients were treated for six months. The results were trivial. “Overall, glucosamine and chrondroitin sulfate were not significantly better than placebo in reducing knee pain,” and the painkiller celecoxib produced better results.
- Maybe a body that feels stiff, painful, and weak needs “performance enhancement” as much as an athlete… or more. Adaptation to exercise and healing from injury may just be two ends of the same spectrum — different extremes of the same fundamental process. Recovery from exercise may have a lot in common biologically with healing from an injury. Maybe.
- Rodriguez NR, DiMarco NM, Langley S, et al. Position of the American Dietetic Association, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and athletic performance. J Am Diet Assoc. 2009 Mar;109(3):509–27. PubMed 19278045 ❐
This is a dense paper on how nutrition can enhance athletic performance. It describes in great detail the position of the American Dietetic Association, Dietitians of Canada, and the American College of Sports Medicine, so it’s very “official” (for whatever it’s worth). Some highlights:
- they endorse sports drinks (which badly undermines the credibility of these recommendations, because sports drinks are ridiculous, please see Wagner)
- energy and macronutrient needs, especially carbohydrate and protein, must be met when exercising hard
- vitamin and mineral supplements are not needed if adequate energy to maintain body weight is consumed from a variety of foods
- ergogenic aids are poorly regulated and should be used with caution
And of course they recommend the services of a “qualified sports dietitian and in particular in the United States, a Board Certified Specialist in Sports Dietetics.”
- There are many fascinating examples of super-human performance and freakish immunity to pain during emergencies, tragedies, and other exceptional circumstances. These effects by and large cannot be harnessed, but they do at least demonstrate that both performance and pain can dance to the same tune. Pain is weird, volatile and quirky, and so is performance.
- And maybe the only difference between some performance boosters and “medicine” is where you started. If you were healthy to begin with, it’s a performance booster. If you were injured, it’s a medicine. Maybe a body that feels stiff, painful, and weak needs “performance enhancement” as much as an athlete… or more. Adaptation to exercise and healing from injury may just be two ends of the same spectrum — different extremes of the same fundamental process. Recovery from exercise may have a lot in common biologically with healing from an injury. Maybe.
- For instance, exercise soreness and fatigue are almost synonymous — sore muscles are also tired and weak. The everything-hurts fragility of the seriously sick and injured blends seamlessly with being tired, and the same blend of sensitization and exhaustion probably has less obvious causes too. Fibromyalgia is defined by unexplained pain and fatigue, and many people with severe chronic fatigue also have a lot of pain.
- It’s important to acknowledge that some people do not respond to creatine. There are non-responders to every drug, even the most effective drugs ever developed.
- Butts J, Jacobs B, Silvis M. Creatine Use in Sports. Sports Health. 2018;10(1):31–34. PubMed 29059531 ❐ PainSci Bibliography 51778 ❐
- Balestrino M, Adriano E. Beyond sports: Efficacy and safety of creatine supplementation in pathological or paraphysiological conditions of brain and muscle. Med Res Rev. 2019 11;39(6):2427–2459. PubMed 31012130 ❐
- Gordji-Nejad A, Matusch A, Kleedörfer S, et al. Single dose creatine improves cognitive performance and induces changes in cerebral high energy phosphates during sleep deprivation. Sci Rep. 2024 Feb;14(1):4937. PubMed 38418482 ❐ PainSci Bibliography 49735 ❐
- Cornish SM, Peeler JD. No effect of creatine monohydrate supplementation on inflammatory and cartilage degradation biomarkers in individuals with knee osteoarthritis. Nutr Res. 2018 03;51:57–66. PubMed 29673544 ❐
Creatine for osteoarthritis hasn’t been studied much, because it’s not what it’s supposedly good for, not what it “says on the tin.” But these researchers were looking for a link between and ergogenic aid and pain, exactly what this article is all about. They “hypothesized that supplementing with creatine monohydrate for 12 weeks would lower biomarkers of inflammation and cartilage degradation in patients with knee osteoarthritis when compared to placebo.” But they found nothing: not a single difference in anything they measured. Not inflammation, not cartilage condition, not functionality, not strength, and not how the subjects felt about their knees. Absolutely bupkis.
A disappointing result, but kudos to them (and the journal) for just reporting a negative result, without any annoying attempt to spin it as positive (shockingly rare restraint). But someone else did…
A little extra colour: this is a decisively negative study, but that didn’t stop some other researchers for citing it as if it was positive! A particularly extreme example of a bogus citation, in a paper that reads like creatine propaganda, in a journal that might be terrible — probably unethical, maybe outright fraudulent.
- Facioscapulohumeral Muscular Dystrophy (FSHD) is a common, mild form of muscular dystrophy that primarily affects the muscles of the shoulder and face. I have a good friend with this condition, and it’s endlessly useful as a fascinating example of a subtle pathology that can be a surprising cause of unexplained pain. For more information, see 38 Surprising Causes of Pain.
- Pearlman JP, Fielding RA. Creatine monohydrate as a therapeutic aid in muscular dystrophy. Nutr Rev. 2006 Feb;64(2 Pt 1):80–8. PubMed 16536185 ❐
- Statins are important and widely used drugs, and their deleterious effect on muscle is controversially but widely considered a diagnosable condition: statin myalgia, or statin-associated muscle symptoms (SAMS). See Stasi.
- Balestrino M, Adriano E. Creatine as a Candidate to Prevent Statin Myopathy. Biomolecules. 2019 09;9(9). PubMed 31533334 ❐ PainSci Bibliography 51779 ❐
- Kreider RB, Kalman DS, Antonio J, et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr. 2017;14:18. PubMed 28615996 ❐ PainSci Bibliography 51782 ❐
- Wikipedia: “Clinical studies have consistently reported that glucosamine appears safe. However, a recent Université Laval study shows that people taking glucosamine tend to go beyond recommended guidelines, as they do not feel any positive effects from the drug. Beyond recommended dosages, researchers found in preliminary studies that glucosamine may damage pancreatic cells, possibly increasing the risk of developing diabetes.”
- Brien S, Lewith G, Walker A, Hicks SM, Middleton D. Bromelain as a Treatment for Osteoarthritis: a Review of Clinical Studies. Evidence-based Complementary & Alternative Medicine. 2004 Dec;1(3):251–257. PubMed 15841258 ❐ PainSci Bibliography 55428 ❐
So there’s a conflict of interest (COI) — so what? Historically, the worst science has often been funded by people with a strong stake in the results. But it’s not always a deal-breaker. The same bias that can compromise science often comes from the same enthusiasm needed to pay for it in the first place! It’s not reasonable to expect science to only ever be done by people without any skin in the game. Dispassionate objectivity in science is largely a myth. (Journalism too, by the way.) The severity and relevance of a COI has to be evaluated on a case-by-case basis.
Unfortunately, in practice, just accusing researchers of a conflict of interest is probably just as destructive as allegations of outright fraud (see Barnes et al.)!
- Remember that side effects can be rare and widely variable, so even if many people have no problems, lots of others might — you can’t say that bromelain has no side effects just because you got away with taking it!
- Kasemsuk T, Saengpetch N, Sibmooh N, Unchern S. Improved WOMAC score following 16-week treatment with bromelain for knee osteoarthritis. Clin Rheumatol. 2016 Oct;35(10):2531–40. PubMed 27470088 ❐ It’s noteworthy than bromelain appeared to match the benefits of diclofenac, which is an efficacious drug with notoriously severe side effects. But this study was just too small to clearly establish its efficacy or it’s relative safety. At best, this trial is a reason to do a better trial.
- Well-designed clinical trials are expensive and time-consuming. Cart-before-horse basic science papers are something you bang off in a weekend and pad your resumé with, so they exist in huge numbers: jargon-riddled speculation about why [insert molecule] might be useful, because that’s way easier than testing it to see if it actually is.
- Gonçalves LdS, Painelli VdS, Yamaguchi G, et al. Dispelling the myth that habitual caffeine consumption influences the performance response to acute caffeine supplementation. J Appl Physiol (1985). 2017 May:jap.00260.2017. PubMed 28495846 ❐
This trial demonstrated that caffeine supplementation boosts athletic performance even if you are used to its effects. Forty endurance cyclists were divided into groups of low, moderate, and highly daily caffeine intake. They all did three cycling tests after drinking caffeine, a placebo, or nothing at all. Performance on caffeine was clearly best across the board for all participants, regardless of typical caffeine intake.
- Hogervorst E, Bandelow S, Schmitt J, et al. Caffeine Improves Physical and Cognitive Performance during Exhaustive Exercise. Medicine & Science in Sports & Exercise. 2008 Oct;40(10):1841–1851. PainSci Bibliography 56104 ❐
- To be clear, my statements about the role of caffeine in chronic pain here are unsupported speculation, whereas the short-term pain-relieving effects of caffeine are quite clear and evidence-based. And there’s no conflict between what we know about the short effects and what I suspect about the long term effects. It can be “all of the above”! Caffeine can be good for pain in the short term and bad for it in the long term. (Just like booze. We can draw a strong analogy to alcohol, which definitely relieves pain in a meaningful way ... for as long as you’re drunk! It’s the original anaesthetic. But at the same time, we know with extremely high confidence that the stuff is a nasty poison and downright terrible for you when habitually consumed for a long time.)
- Killer SC, Blannin AK, Jeukendrup AE. No evidence of dehydration with moderate daily coffee intake: a counterbalanced cross-over study in a free-living population. PLoS One. 2014;9(1):e84154. PubMed 24416202 ❐ PainSci Bibliography 53892 ❐
Many people believe that coffee is dehydrating. To test this popular idea, 50 men drank four cups (200ml) of either coffee or water each day for three days while their diet and activity were controlled. There were no differences in their body mass, urine volume, and signs of hydration in the blood and urine (pee clarity, basically). If you can drink almost a litre of coffee a day and have no measurable effect on hydration, then it is not “dehydrating” to any meaningful degree. The authors reasonably concluded that coffee “provides similar hydrating qualities to water.”
- Rogero MM, Tirapegui J, Pedrosa RG, Castro IAd, Pires ISd. Effect of alanyl-glutamine supplementation on plasma and tissue glutamine concentrations in rats submitted to exhaustive exercise. Nutrition. 2006 May;22(5):564–71. PubMed 16472983 ❐
- Cruzat VF, Rogero MM, Tirapegui J. Effects of supplementation with free glutamine and the dipeptide alanyl-glutamine on parameters of muscle damage and inflammation in rats submitted to prolonged exercise. Cell Biochem Funct. 2010 Jan;28(1):24–30. PubMed 19885855 ❐
This is a study of rats showing some signs that glutamine supplementation might have some biological effects that would reduce muscle soreness, namely it “may attenuate inflammation biomarkers after periods of training.” It is an example of basic science with possible clinical relevance. However, it is a long way from this evidence to anything like proof that amino acid supplementation actually reduces post-exercise muscle soreness in humans.
- Merimee TJ, Rabinowtitz D, Fineberg SE. Arginine-initiated release of human growth hormone. Factors modifying the response in normal man. N Engl J Med. 1969 Jun;280(26):1434–8. PubMed 5786514 ❐ PainSci Bibliography 55053 ❐
Some ancient, basic physiology science demonstrating that arginine supplementation may stimulated production of growth hormone — which is still used by as a rationale for arginine supplementation for bodybuilders to this day.
- Willoughby DS, Boucher T, Reid J, Skelton G, Clark M. Effects of 7 days of arginine-alpha-ketoglutarate supplementation on blood flow, plasma L-arginine, nitric oxide metabolites, and asymmetric dimethyl arginine after resistance exercise. Int J Sport Nutr Exerc Metab. 2011 Aug;21(4):291–9. PubMed 21813912 ❐
A small study showing that arginine supplementation increased the amount of arginine in the blood, but changes in circulatory function were simply due to exercise — that is, they also occurred in people who took only a placebo.
- Tajari SN, Rezaeee M, Gheidi N. Assessment of the effect of L-glutamine supplementation on DOMS. Br J Sports Med. 2010;44. PubMed 23997909 ❐ PainSci Bibliography 54728 ❐
“These results suggest that L-glutamine supplementation attenuates DOMS effects, muscle damage and downfall of performance in flexor of hip.” However, it’s a weak study, and I don’t think the results do much more than “suggest”: it was a small experiment, and they measured range of motion only (not pain or strength, both of which would have been better choices — DOMS does not particularly limit range of motion, just makes it uncomfortable). Nevertheless, this is a shred of evidence that glutamine might, possibly, help with DOMS a little.
- Garlick PJ. Assessment of the safety of glutamine and other amino acids. J Nutr. 2001 Sep;131(9 Suppl):2556S–61S. PubMed 11533313 ❐
Four studies of the safety of glutamine supplementation in a medical context found that it was “safe in adults and in preterm infants,” but that data was not relevant to concerns about “chronic consumption by healthy subjects.” The authors reviewed more literature on high dietary intake of proteins and amino acids in general, and found more problems, particularly neurological damage in preterm infants. Infants are particularly sensitive to neurological effects, so if they have problems, it certainly means trouble for adults too — just less dramatically. “Because glutamine is metabolized to glutamate and ammonia, both of which have neurological effects, psychological and behavioral testing may be especially important.” In other words, a high dietary intake of glutamine may mess with your head.
- Pasiakos SM, Lieberman HR, McLellan TM. Effects of protein supplements on muscle damage, soreness and recovery of muscle function and physical performance: a systematic review. Sports Med. 2014 May;44(5):655–70. PubMed 24435468 ❐
- VanDusseldorp TA, Escobar KA, Johnson KE, et al. Effect of Branched-Chain Amino Acid Supplementation on Recovery Following Acute Eccentric Exercise. Nutrients. 2018 Oct;10(10). PubMed 30275356 ❐ PainSci Bibliography 52500 ❐
- Estoche JM, Jacinto JL, Roveratti MC, et al. Branched-chain amino acids do not improve muscle recovery from resistance exercise in untrained young adults. Amino Acids. 2019 Sep;51(9):1387–1395. PubMed 31468208 ❐ )
- Fedewa MV, Spencer SO, Williams TD, Becker ZE, Fuqua CA. Effect of branched-Chain Amino Acid Supplementation on Muscle Soreness following Exercise: A Meta-Analysis. Int J Vitam Nutr Res. 2019 Nov;89(5-6):348–356. PubMed 30938579 ❐
- 30681787 “The use of collagen supplementation in dermatology remains controversial due to the lack of regulation on quality and quantity of ingredients in over-the-counter collagen supplements, as well as minimal peer-reviewed literature on the subject.” But “Preliminary results are promising”! 🙄
- The word “significant” in scientific abstracts is routinely misleading. It does not mean that the results are large or meaningful, and in fact is used to hide precisely the opposite. When only “significance” is mentioned, it almost invariably refers to the notoriously problematic “p-value,” a technically-true distraction from the more meaningful truth of a tiny “effect size”: results that are not actually impressive. This practice has been considered bad form by experts for decades, but is still extremely common. See Statistical Significance Abuse: A lot of research makes scientific evidence seem much more “significant” than it is.
- García-Coronado JM, Martínez-Olvera L, Elizondo-Omaña RE, et al. Effect of collagen supplementation on osteoarthritis symptoms: a meta-analysis of randomized placebo-controlled trials. Int Orthop. 2019 03;43(3):531–538. PubMed 30368550 ❐
- Nicol LM, Rowlands DS, Fazakerly R, Kellett J. Curcumin supplementation likely attenuates delayed onset muscle soreness (DOMS). Eur J Appl Physiol. 2015 Mar. PubMed 25795285 ❐
- Connolly DAJ, McHugh MP, Padilla-Zakour OI, Carlson L, Sayers SP. Efficacy of a tart cherry juice blend in preventing the symptoms of muscle damage. Br J Sports Med. 2006 Aug;40(8):679–83; discussion 683. PubMed 16790484 ❐ PainSci Bibliography 53887 ❐
- I don’t think black cherry Kool-Aid would fool me. I’m not sure it would fool anyone!
- Howatson G, Bell PG, Tallent J, et al. Effect of tart cherry juice (Prunus cerasus) on melatonin levels and enhanced sleep quality. Eur J Nutr. 2012 Dec;51(8):909–16. PubMed 22038497 ❐
A small pilot trial of tart cherries for insomnia in 20 subjects, comparing to a placebo and measuring sleep quality and melatonin levels. The conclusion is positive, but the data is mediocre at best: small effects that are barely statistically significant. It's not a negative study, but it's not exactly a convincing positive either.
- Losso JN, Finley JW, Karki N, et al. Pilot Study of the Tart Cherry Juice for the Treatment of Insomnia and Investigation of Mechanisms. Am J Ther. 2018;25(2):e194–e201. PubMed 28901958 ❐ PainSci Bibliography 52136 ❐
A pilot study with 8 subjects. Microscopic! Powerless to actually prove anything. But, for what very little it's worth… technically positive, showing a decent boost to sleep duration (and nothing else they measured).
- Pigeon WR, Carr M, Gorman C, Perlis ML. Effects of a tart cherry juice beverage on the sleep of older adults with insomnia: a pilot study. J Med Food. 2010 Jun;13(3):579–83. PubMed 20438325 ❐ PainSci Bibliography 52142 ❐
A teensy pilot study of 15 people, comparing a tart cherry juice blend to placebo, showing barely-there improvements in insomnia. “Effect sizes were moderate and in some cases negligible. … considerably less than those for evidence-based treatments of insomnia: hypnotic agents and cognitive-behavioral therapies for insomnia.”
- Manson JE, Patsy M B, Rosen CJ, Taylor CL. Vitamin D Deficiency — Is There Really a Pandemic? N Engl J Med. 2016 Nov 10;375(19):1817–1820. PubMed 27959647 ❐
ABSTRACT
The claim that large proportions of North American and other populations are deficient in vitamin D is based on misinterpretation and misapplication of the Institute of Medicine reference values for nutrients — misunderstandings that can adversely affect patient care.
- Holick MF, Chen TC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr. 2008 Apr;87(4):1080S–6S. PubMed 18400738 ❐ PainSci Bibliography 55028 ❐
- Bone aching is caused by osteomalacia, which is bone weakening specifically caused by malfunctioning bone building biology. The Mayo Clinic describes osteomalacia symptoms like so: “The dull, aching pain associated with osteomalacia most commonly affects the lower back, pelvis, hips, legs and ribs. The pain may be worse at night, or when you’re putting weight on affected bones.”
- Bolland MJ, Grey A, Avenell A. Effects of vitamin D supplementation on musculoskeletal health: a systematic review, meta-analysis, and trial sequential analysis. Lancet Diabetes Endocrinol. 2018 11;6(11):847–858. PubMed 30293909 ❐
- Bislev LS, Grove-Laugesen D, Rejnmark L. Vitamin D and Muscle Health: A Systematic Review and Meta-analysis of Randomized Placebo-Controlled Trials. J Bone Miner Res. 2021 09;36(9):1651–1660. PubMed 34405916 ❐
- Tai YT, Tong CV. The Perilous PPI: Proton Pump Inhibitor as a Cause of Clinically Significant Hypomagnesaemia. J ASEAN Fed Endocr Soc. 2020;35(1):109–113. PubMed 33442177 ❐ PainSci Bibliography 52188 ❐ It may be a side effect of the extremely common proton pump inhibitor drugs for heartburn and acid reflux, but the prevalence of the side effect is unknown. There have been more than a couple dozen case reports of serious hypomagnesaemia over the last twenty years, and those are generally the tip of an iceberg.
- This is uncertain. Some experts claim it. For instance, Mauskop et al. point out that most magnesium isn’t stored in the blood, but rather in the bones and other tissue reservoirs. That premise is probably true, but does it follow that blood levels are therefore “inaccurate” for detecting deficiency? Not necessarily, and I have been unable to find direct empirical support for it. This might true and important, or it might not.
- We absorb Mg on an as-needed basis, so excesses are mostly just pooped out — maybe with a little cramping and diarrhea.
- Tarleton EK, Kennedy AG, Rose GL, Littenberg B. Relationship between Magnesium Intake and Chronic Pain in U.S. Adults. Nutrients. 2020 Jul;12(7). PubMed 32708577 ❐ PainSci Bibliography 52160 ❐
This study seemed to go out of its way to try study magnesium for pain without actually talking to a patient with pain — pure data analysis. Tarleton et al. mined some old survey data on the health of more than 13,000 American adults (high-volume data, but also poor quality for this purpose, “low resolution”). They reported a “protective effect” of “increased magnesium intake,” concluding that this “warrants further study.” Which everyone more or less already agreed on, but more data is good… right?
Hm, not if it just muddies the waters. Data like this is can be like yelling in a crowded theatre, “There might be a fire! I think I saw some smoke!”
This is a far cry from conclusive evidence that taking magnesium treats any kind of chronic pain. The allegedly protective “increased magnesium intake” they detected is, I believe, inferred from notoriously unreliable self-reporting of diet. The possibilities for confounding factors are endless.
Bonus eye roll: Amusingly, when Tarleton et al. explained why they did this research — that “there is some evidence that magnesium supplementation results in improved pain management” — they cite only a single supporting paper. And what is that single paper? A twenty-year-old study showing an inflammatory response to severe deficiency… in rats. 🙄
- Banerjee S, Jones S. Magnesium as an Alternative or Adjunct to Opioids for Migraine and Chronic Pain: A Review of the Clinical Effectiveness and Guidelines. CADTH Rapid Response Reports. 2017 Apr. PubMed 29334449 ❐
This paper concluded in 2016 that “magnesium appears to have an analgesic effect.” Great! But don’t read the fine print if you want to hang on to that good feeling. Their own summary of findings doesn’t seem to back up the optimism. They clearly state that conclusions were “not possible” for migraine … that the evidence is conflicting for a rather exotic kind of chronic pain (complex regional pain syndrome) … and they mention only a single trial showing a benefit for back pain (with intravenous supplementation, no less, and for back pain complicated by neuropathy; see Yousef).
And that’s just all they wrote about the data. If there is enough evidence to justify “magnesium appears to have an analgesic effect,” it is not reported in this paper.
- Yousef AA, Al-deeb AE. A double-blinded randomised controlled study of the value of sequential intravenous and oral magnesium therapy in patients with chronic low back pain with a neuropathic component. Anaesthesia. 2013 Mar;68(3):260–6. PubMed 23384256 ❐ PainSci Bibliography 52166 ❐
This is one of the only good quality trials of magnesium supplementation for body pain. However, crucially, they studied only back pain with a neuropathic component. 40 patients were given a placebo, and their progress over 6 months was compared to 40 more who got intravenous magnesium for two weeks, then oral for another month.
The patients who got magnesium clearly did better in the long run.
Both groups did great at first, more than halving their pain. If stopped there, the study would have shown that magnesium was no better than a placebo. But then the placebo group's numbers rebounded, while the magnesium folks stayed low… for six months. The improvement wasn’t huge, but it wasn’t small either. I wouldn’t turn it down.
![]()
This is a clearly positive result on its face — which is such a rarity in this field that it’s cause for too-good-to-be-true concern. It is “just one study,” with unknown flaws, and unreplicated.
This experiment just cannot tell us anything about the effect of magnesium on the most common kinds of pain, which are mostly not neuropathic. Back pain without neuropathy is a good proxy for many other kinds of pain; back pain with neuropathy is more about neuropathy than “back pain.”
But, for whatever it’s worth, it is indeed a properly positive result — and that’s more than we can say for a great many other trials of any intervention for any kind of back pain.
- Garrison SR, Korownyk CS, Kolber MR, et al. Magnesium for skeletal muscle cramps. Cochrane Database Syst Rev. 2020 09;9:CD009402. PubMed 32956536 ❐ PainSci Bibliography 52162 ❐
This review of only a handful of existing studies concluded that “it is unlikely that magnesium supplementation provides clinically meaningful cramp prophylaxis to older adults experiencing skeletal muscle cramps.” Amazingly, the evidence for the effect of Mg on cramps caused by exertion, disease, and pregnancy is just hopelessly inadequate. You’d think someone would at least have studied exercise-induced cramping, given its importance in elite athletics. The last version of this review was in 2012, and almost nothing changed.
- Liu J, Song G, Zhao G, Meng T. Effect of oral magnesium supplementation for relieving leg cramps during pregnancy: A meta-analysis of randomized controlled trials. Taiwan J Obstet Gynecol. 2021 Jul;60(4):609–614. PubMed 34247796 ❐
- Schwellnus MP, Drew N, Collins M. Increased running speed and previous cramps rather than dehydration or serum sodium changes predict exercise-associated muscle cramping: a prospective cohort study in 210 Ironman triathletes. Br J Sports Med. 2011 Jun;45(8):650–6. PubMed 21148567 ❐
Blood samples from 210 Ironman triathletes were checked for electrolytes and other signs of hydration status. 43 had suffered cramps. There were no significant differences between the crampers and the non-crampers in any of the pre-testing or post-testing. Dehydration and electrolyte shortage don’t cause cramps — intense effort does. “The results from this study add to the evidence that dehydration and altered serum electrolyte balance are not causes for exercise-associated muscle cramps.” This is a nice myth-mangler of a paper.
- Minetto MA, Holobar A, Botter A, Farina D. Origin and Development of Muscle Cramps. Exerc Sport Sci Rev. 2013 Jan;41(1):3–10. PubMed 23038243 ❐ PainSci Bibliography 54733 ❐
This dense review of the physiology of muscle cramps asserts that the role of spinal mechanisms has been “proved unambiguously,” but mysteries remain, most notably why cramping is much more likely in some people and some muscles, and (fascinatingly) why they hurt.
- In Yousef et al., previously referenced, both the placebo and magnesium groups experienced equally dramatic benefits at the 2-week point — a good demonstration of how a placebo can easily resemble a robust therapeutic effect and for a surprisingly long time. In this case, the placebo effect had dried up by six weeks while the benefit of magnesium persisted — but we have no idea if that same benefit will happen in other conditions. And we can certainly count on a placebo effect.
- Wandel S, Jüni P, Tendal B, et al. Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: network meta-analysis. BMJ. 2010 Sep 16;341:c4675. PubMed 20847017 ❐ PainSci Bibliography 55001 ❐
- Mijatović N, Šljivić J, Tošić N, et al. Big Suppla: Challenging the Common View of the Supplements and Herbs Industry Affects the Willingness to Try and Recommend Their Products. Studia Psychologica. 2022 Mar;64(1):91–103. PainSci Bibliography 51970 ❐
- ScienceBasedMedicine.org [Internet]. Hall H. Pursued by Protandim Proselytizers; 2011 Oct 11 [cited 12 Mar 16]. PainSci Bibliography 55088 ❐
Dr. Harriet Hall once again summarizes the (lack) of evidence that Protandim helps people. There’s still only one human trial of this stuff … and still none that have anything to do with pain.
Note that there have been no human clinical studies since the one in 2006. The newer studies are just more animal and laboratory studies, so they do nothing to change my previous conclusion. If I were a mouse being artificially induced to develop skin cancer in a lab study, I might seriously consider taking Protandim. But so far, the only study in humans measured increased antioxidant levels by a blood test but did not even attempt to assess whether those increases corresponded to any measurable clinical benefit, for cancer or for anything else.
Dr. Hall also shares some of her contents of her mail bag about this stuff. It’s illuminating, and good for a chuckle. Note that Dr. Hall also has a concurrent article about antioxidants in the print issue (Volume 16 Number 4) of Skeptic Magazine, “Complexities of Antioxidants.”
- Lalani SR, Vladutiu GD, Plunkett K, et al. Isolated mitochondrial myopathy associated with muscle coenzyme Q10 deficiency. Arch Neurol. 2005 Feb;62(2):317–20. PubMed 15710863 ❐
- Taylor BA, Lorson L, White CM, Thompson PD. A randomized trial of coenzyme Q10 in patients with confirmed statin myopathy. Atherosclerosis. 2015 Feb;238(2):329–35. PubMed 25545331 ❐ PainSci Bibliography 52036 ❐ “CoQ10 supplementation does not reduce muscle pain in patients with statin myalgia.”
- Banach M, Serban C, Sahebkar A, et al. Effects of coenzyme Q10 on statin-induced myopathy: a meta-analysis of randomized controlled trials. Mayo Clin Proc. 2015 Jan;90(1):24–34. PubMed 25440725 ❐ “The results of this meta-analysis of available randomized controlled trials do not suggest any significant benefit of CoQ10 supplementation in improving statin-induced myopathy.”
- Di Stasi SL, Macleod TD, Winters JD, Binder-Macleod SA. Effects of Statins on Skeletal Muscle: A Perspective for Physical Therapists. Phys Ther. 2010 Aug. PubMed 20688875 ❐
- “Rhabdo” is a nasty but also very interesting condition. I discuss it in detail in Poisoned by Massage.
- Mammen AL. Statin-Associated Autoimmune Myopathy. N Engl J Med. 2016 Feb;374(7):664–9. PubMed 26886523 ❐
- Regarding classification, professionals should take a look at a great 2004 interview with Eliot A. Brinton, MD: “There are 4 interrelated terms for muscle problems that can occur with statins. Unfortunately, they are often confused even by healthcare professionals … .” (Technical note: this document is freely available, but direct linking will hit a paywall. Medscape only reveals the whole thing to people arriving from a Google search. Simply search for do a Google search for it to get around the paywall.)
- Ganga HV, Slim HB, Thompson PD. A systematic review of statin-induced muscle problems in clinical trials. Am Heart J. 2014 Jul;168(1):6–15. PubMed 24952854 ❐
In this review of several statin trials, only slightly more patients had pain on statins than without (placebo): just 12.7%, compared to 12.4%. You could conclude from this data that there actually is no such thing as statin mylagia! But it probably is a real phenomenon, which is highly plausible based on the existence of rarer but very severe side effects on muscle (see Mammen or Statin Therapy). We don’t have very good data about it, it’s mostly not severe, and it’s hard to distinguish from the “background noise” of many other common causes of musculoskeletal pain.
- Cholesterol Treatment Trialists' Collaboration. Effect of statin therapy on muscle symptoms: an individual participant data meta-analysis of large-scale, randomised, double-blind trials. Lancet. 2022 Aug. PubMed 36049498 ❐
This is an enormous review of nineteen placebo controlled tests of the side effects of statins, following over 30,000 patients for about 4 years on average. A data set like that makes a typical little musculoskeletal medicine study look like a shack in the shadow of the Burj Khalifa.
There was no major difference in the rates of muscle pain and weakness in statins versus placebo. They saw a modest signal in the first year, and for more intensive statin therapy: slightly more myopathy with statins, and mostly mild. Only about 1 in 15 cases of allegedly statin-induced myopathy reported by patients were actually related to statins, according to this data, and those were pretty tame. The researchers concluded:
“Statin therapy caused a small excess of mostly mild muscle pain. Most (>90%) of all reports of muscle symptoms by participants allocated statin therapy were not due to the statin. The small risks of muscle symptoms are much lower than the known cardiovascular benefits.”
This statin evidence cuts both ways: it undermines the Legend of Statin Associated Myopathy, but it also confirms that there is indeed an unpleasant side effect. Even a 5% risk of very mild-but-chronic muscle pain might seem unacceptable to many people. One in twenty is not “rare,” and no amount of chronic pain is cool. So even as it fights excessive hype about SAM, it’s not particularly reassuring either.
Note that statins were directly caught on "camera" meddling in muscle cell metabolism (see Weninger). While not capable of explaining everything about statin myopathy, this significantly boosts the case for a genuine medical side effect.
For a more detailed report on this paper, see “Sign me up for mild muscle pain? The statins dilemma.”
- Gupta A, Thompson D, Whitehouse A, et al. Adverse events associated with unblinded, but not with blinded, statin therapy in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid-Lowering Arm (ASCOT-LLA): a randomised double-blind placebo-controlled trial and its non-randomised non-blind extension phase. Lancet. 2017 Jun;389(10088):2473–2481. PubMed 28476288 ❐
This study was designed to test the existence of the phenomenon of statin myalgia. Taking statins did not increase pain in patients when they were unaware that they were taking them. This suggests that statin myalgia is something people get because they are afraid of it, not because it’s a real side effect. As the authors concluded:
These analyses illustrate the so-called nocebo effect, with an excess rate of muscle-related AE reports only when patients and their doctors were aware that statin therapy was being used and not when its use was blinded. These results will help assure both physicians and patients that most AEs associated with statins are not causally related to use of the drug and should help counter the adverse effect on public health of exaggerated claims about statin-related side-effects.
- Michalska-Kasiczak M, Sahebkar A, Mikhailidis DP, et al. Analysis of vitamin D levels in patients with and without statin-associated myalgia - a systematic review and meta-analysis of 7 studies with 2420 patients. Int J Cardiol. 2015 Jan;178:111–6. PubMed 25464233 ❐
- Sender R, Fuchs S, Milo R. Revised Estimates for the Number of Human and Bacteria Cells in the Body. PLoS Biol. 2016 08;14(8):e1002533. PubMed 27541692 ❐ PainSci Bibliography 52035 ❐
You may have heard that the human body is infested with ten times as more bacterial hitchhikers than the number of our own cells, and even that they have equal mass. Happily, no, we are not quite that disgusting. There’s “only” about the same number of bacteria as the headcount for our own cells, and — because bacteria are quite a bit smaller than our cells — they weigh just a couple hundred grams on average.
Ruth Ley, commenting on the 10th anniversary of the Human Microbiome Project (HMP, see Human Microbiome Project Consortium), for Nature.com:
“The result the first comprehensive catalogue of a healthy US human microbiome: a full list of the genes in the microbes in the gut. The HMP showed that the gut’s cellular organisms consist of thousands of species, with a genetic footprint 150 times the size of the human genome. Eventually, this abundance led biologists to view the microbiome as an environmentally acquired ‘second genome’, hidden in the human host.”
Lindsay, Bethany. “Naturopaths ‘not bound by science,’ lawyer argues in B.C. hearing on fecal transplants for autism..” CBC.com. Jun 29, 2022.
“Klop’s three nephews were the business’s only donors at the time of the complaint and clarified that the lab was in a ground-level unit of the building where the boys lived.”
- Lynch SV, Pedersen O. The Human Intestinal Microbiome in Health and Disease. N Engl J Med. 2016 Dec;375(24):2369–2379. PubMed 27974040 ❐
- Lynch SV, Ng SC, Shanahan F, Tilg H. Translating the gut microbiome: ready for the clinic? Nat Rev Gastroenterol Hepatol. 2019 11;16(11):656–661. PubMed 31562390 ❐
- Bastian H. "They would say that, wouldn't they?" A reader's guide to author and sponsor biases in clinical research. J R Soc Med. 2006 Dec;99(12):611–4. PubMed 17139062 ❐ PainSci Bibliography 51373 ❐
The full quote:
“A promising treatment is often in fact merely the larval stage of a disappointing one. At least a third of influential trials suggesting benefit may either ultimately be contradicted or turn out to have exaggerated effectiveness.”
- Ma P, Mo R, Liao H, et al. Gut microbiota depletion by antibiotics ameliorates somatic neuropathic pain induced by nerve injury, chemotherapy, and diabetes in mice. J Neuroinflammation. 2022 Jun;19(1):169. PubMed 35764988 ❐
- Anything good for your general health has the potential to help chronic pain. The specific cause of chronic pain may often be less important than general sensitivity and biological vulnerability to any pain. The biggest risk factors for pain chronicity are things like insomnia, obesity, smoking, drinking… and they overshadow common scapegoats like poor posture, spinal degeneration, or even repetitive strain injury. How can nothing in particular make us hurt? Because pain is weird, a generally oversensitive alarm system that can produce false alarms even at the best of times, and probably more of them when your system is under strain. See Vulnerability to Chronic Pain: Chronic pain often has more to do with general biological vulnerabilities than specific tissue problems.
- Mohammed AT, Khattab M, Ahmed AM, et al. The therapeutic effect of probiotics on rheumatoid arthritis: a systematic review and meta-analysis of randomized control trials. Clin Rheumatol. 2017 Dec;36(12):2697–2707. PubMed 28914373 ❐
- Sanchez P, Letarouilly JG, Nguyen Y, et al. Efficacy of Probiotics in Rheumatoid Arthritis and Spondyloarthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2022 Jan;14(2). PubMed 35057535 ❐ PainSci Bibliography 52051 ❐
The NIH says that “some probiotic products have been reported to contain microorganisms other than those listed on the label. In some instances, these contaminants may pose serious health risks.”
Anti-quackery activists get much pushback in the form of “what’s the big deal?” or “what’s the harm?” from people who…do not know the answers to those questions. 😜 And why don’t they know the answers? Because they don’t really care, it’s mostly careless ignorance, they don’t even know what they don’t know. And sometimes it’s ideological bias: they actually don’t want to know.
But it is extremely satisfying, once in a blue moon, when you explain and get the response: “Oh! Well! Shit! So that is the big deal. Right then, carry on…”
- And spending money on most supplements is not just wasting it … it’s giving it to assholes. 😱 Straight into the deep pockets of corporate douchebags. Big Suppla is mostly a subsidiary of Big Pharma these days. And most of the exceptions? MLMs! Multi-level marketing scams run by shady creeps raking in the dough at the tops of their pyramid schemes.
- Good health is at least 95% about “the basics.” Health “optimizations” are not just much less important, they also have a significant opportunity cost: every moment and dollar spent on the not-basics is stolen directly from the much more important basics!
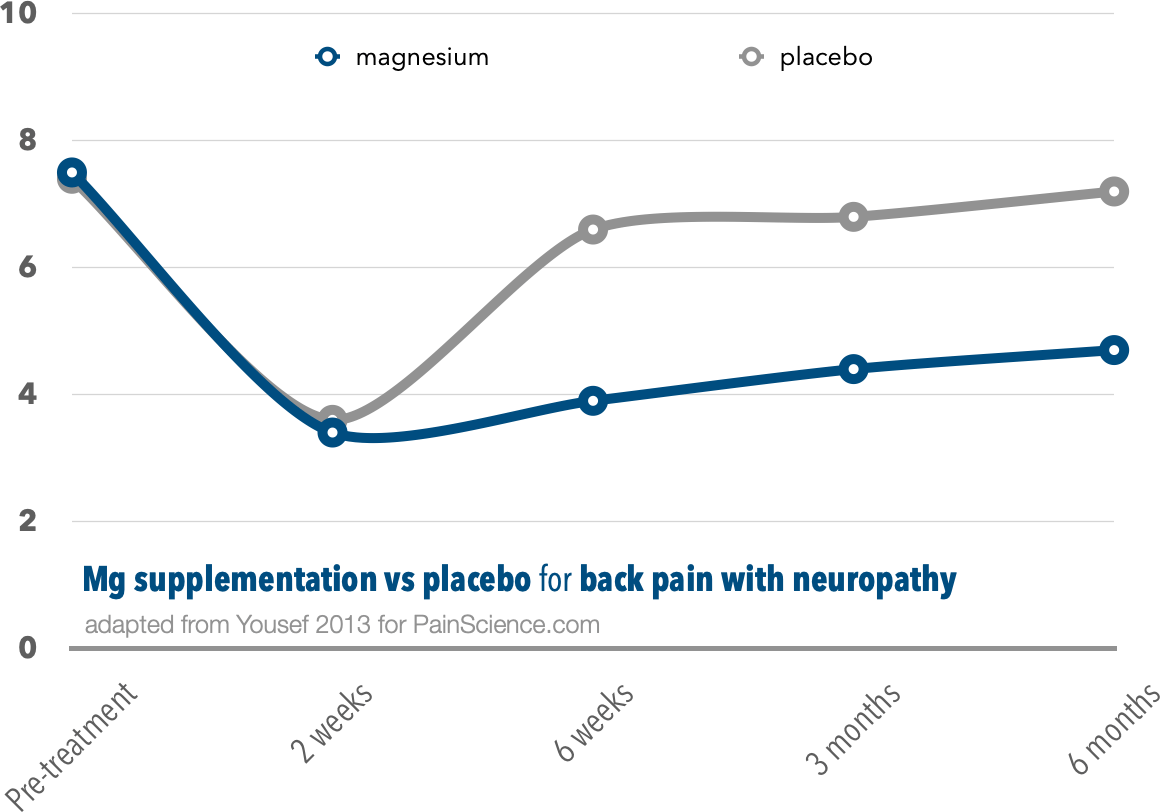
{kind=link}
{kind=link}