Does Epsom Salt Work?
The science and mythology of Epsom salt bathing for recovery from muscle pain, soreness, or injury

A cup or two of Epsom salt in a bath supposedly helps sore muscles, mainly by “detoxifying” or delivering magnesium. Is it medicine or myth? Does Epsom salt actually work? If it does work, how does it work? What does it do, what are the biological effects? This is a deep dive into the topic from a scientific perspective.
Epsom salts are specifically thought to be a good treatment mainly for muscle pain from over-exertion (delayed-onset muscle soreness), arthritis, myofascial pain syndrome (“trigger points”), fibromyalgia, but also for speeding healing1 from minor injuries such as muscle strains and tendinitis. The “exact” mechanism given is almost always detoxification, perhaps via osmosis, with no further information provided. A few proponents say that it’s good for pain because it’s a good source of magnesium, or they just think it’s a good way to get some if you are magnesium deficient (hypomagnesemia).
Claims and recommendations of this nature can be found by the thousands online. Bags and cartons of Epsom salts are available at any drugstore. Why, I have a package right here.2 It says:
Dissolve desired amount (1–2 cups) of crystals in a hot bath to produce a mineral water treatment to aid in the relief of muscular aches and pains.
All the claims are critically analyzed here. Spoiler alert: none of them are well-supported. On the other hand, there are few firm conclusions here either. The only thing that’s certain is that the “osmosis” idea is total bollocks, just biologically incoherent.
Says who? How does it work?
When I went through my massage therapy training — an unusually rigorous 3-year full-time program — my instructors suggested Epsom salt baths as a good thing to prescribe to our clients.
Mostly my colleagues and mentors just made vague references to “detoxifying” the muscles, perhaps “by osmosis.” Nothing more exact was ever discussed because, frankly, I am sure that not one person in the building could have even named the compound “magnesium sulfate.”3 Me included.
I have wondered ever since if there was anything to it.
I am strongly skeptical of all health-related claims involving “toxins,” mostly because people who toss that word around never seem to know which toxins they are talking about.4 I have thoroughly studied the subject of post-exercise muscle soreness — probably the leading cause of hot baths — only to discover that it’s basically been proven that there are no known remedies for it.5 And after a long, hot Epsom salt bath of my own one night — which had no apparent effect on my unusually sore muscles, as usual — I decided it was time for a proper reality check. I started studying this topic (and I’ve never really stopped).
Does an Epsom salt bath actually do anything? Does brining yourself like a turkey do any good? Can you pickle your pain away? Is there any plausible way that Epsom salts could have an effect on your sore muscle tissue, or on the healing of injuries?
What is Epsom salt? (And why do people always stick an S on the end?)
Epsom salt is magnesium sulfate heptahydrate, usually shortened just to magnesium sulfate (note also the British spelling “sulphate”). It was originally obtained by boiling down mineral waters at Epsom, England. The magnesium is considered the “active ingredient.”
It is often quaintly referred to in the plural — Epsom salts instead of Epsom salt — but it is just one kind of salt, and other than tradition there’s no more reason to say “salts” than there is to say “please pass the table salts.” It’s just an odd affectation, and both the singular and plural form are fine.

Other than tradition there’s no more reason to say Epsom “salts” — plural — than there is to say “please pass the table salts.”
The chemical structure of Epsom salts … so that you know this is a serious article.
Almost no Epsom salt science
A search for scientific evidence concerning Epsom salt baths is disappointing. There are basically no studies of their effect on body pain. There weren’t when I first tackled this topic in the early 2000s, and there still aren’t any as of 2024. There may never be.
Folk remedies are often neglected by researchers, but not usually so completely. There are usually at least a few experiments testing popular remedies kicking around. Why wouldn’t the use of Epsom salts for muscle soreness be similarly blessed?
There is plenty of research relevant to other medical uses of Epsom salts.6 For instance, on my package of Epsom salts, instructions are also given for internal usage as a laxative — which does work78 and is actually FDA approved9 and probably the most common and generally known medical usage. Other (internal) uses of magnesium sulfate include the treatment of magnesium deficiency,10 which causes irregular heart rhythm and cramps. A couple conditions that cause severe cramping (tetany) or seizures, like eclampsia11 and tetanus,12 can be partially treated with magnesium. There will be more about the causes, symptoms, and treatment of magnesium deficiency below.
There are also some incredibly bogus and crazy (dangerous) uses of Epsom salts. For instance, naturopaths may use it to try to dissolve gallstones — which doesn’t work, and can cause serious poisoning.
But there appears to be simply nothing at all published about alleviating aches and pains by any means.
It’s not just researchers who’ve neglected it. For instance, Epsom salt baths do not even rate a mention in Home Remedies: Hydrotherapy, massage, charcoal, and other simple treatments, a large and credibly referenced compendium of traditional remedies assembled by a pair of doctors. They describe five other medicated baths — alkaline (soda) baths, starch baths, oatmeal baths, peroxide baths, and sulfur baths — for conditions ranging from poison ivy rashes to diabetic gangrene (!), but they never mention Epsom salt baths.
In the near perfect absence of directly relevant science, all we can do is speculate scientifically about the possible mechanisms of action. And that I will now do, at absurd length.
“(With) a grain of salt,” (or “a pinch of salt”) in modern English, is an idiom which means to view something with skepticism, or to not take it literally.
Part 2
Toxins & Osmosis
What “toxins” do Epsom salts supposedly get rid of?
Regardless of whether Epsom salts baths might work, it’s important to understand that the words “detoxification” and “osmosis” — the ideas most commonly invoked to explain the point of Epsom salts baths — are hopelessly misleading and explain nothing.
A poison is literally any harmful substance, and even something safe in typical doses becomes a poison in overdose — so you can be poisoned by either lots of water or a minuscule amount of lead. Toxins are technically poisons produced by living things, like venom or metabolic wastes, but informally the word is synonymous with poison.
There’s a staggering variety of poisons and toxins, but the two major categories that most people imagine purging are pollutants and metabolic “wastes”:
Pollutants are poisons in the environment around us that get into us from the outside. The most obvious specific candidates would be the persistent organic pollutants like pesticides, flame retardants, and polychlorinated biphenyls (PCBs, now banned, but formerly ubiquitous in many plastics). Lead is also still an alarmingly common environmental poison, and still does more harm than any other known chemical hazard. There are major open scientific questions about the threat of the forever chemicals (the PFAS) and microplastics. And, of course, a huge source of poisoning is really ordinary: smog! And food additives are a minor subcategory of “pollutant,” massively over-hyped, but there probably are a few problematic chemicals in our diet. I review all of these and more in detail in Chronic, Subtle, Systemic Inflammation: One possible sneaky cause of puzzling chronic pain.
Metabolic “wastes” is a much murkier category, because most of them aren’t actually wastes at all. Cellular chemistry produces a lot of molecules, with many fates. Technically these are toxins because they are biologically produced and they would be harmful in abnormal concentrations… but they are normal products of biology, and so most of them are either safely excreted, or actually re-used and re-cycled. As in the rest of nature, not much in cellular chemistry is wasted. Lactic acid is the ultimate example: misunderstood for decades, even by many people who should know better, lactic acid is not a persistent waste product and you wouldn’t want to “flush” it or “suck” it out of your muscles even if you could.13 If the mythology and misconceptions about lactic acid are this bad, it’s unlikely that there’s some other metabolic waste that is a better candidate for something that is regularly poisoning us and needs to be purged. I review this topic in more detail in Why Drink Water After Massage?.
Osmosis: not what most people think
Why does osmosis even come up for this topic? It seems to be the average person’s notion of how Epsom salts detoxify. I guess they visualize toxins being sucked out of the body through the skin. But even if those nasty toxins are in there and need out-sucking, that is not how osmosis works.
Many people get osmosis bass-ackwards: they believe it refers to the movement of things floating in water across a membrane, but that is wrong by definition. It’s actually the water itself that moves. Osmosis refers to the movement of water only across thin membranes, towards the side that is “thicker” with dissolved particles.15 Take it from the Osmosis Cats! show cats16
You can demonstrate this clearly by soaking a potato in salty water. The water is clearly “sucked” osmotically out of the potato’s cells: it loses its plumpness and goes limp. Poor little potato. It’s the water that moves around. (Or cats.)
And so, by definition, Epsom salts baths cannot suck the toxins out of anyone or anything (or suck magnesium ions into anyone or anything).
What about sweating? And ionic attraction?
A reader spelled out a couple of other commonly paired ideas about how Epsom salts baths might detoxify:
I always thought epsom salt baths were supposed to detoxify by opening your pores, and then the salts (ionized) help to supplement your body’s own detox processes (sweating toxins out through pores) by drawing the toxins out through the pores. It’s not osmosis, although the scientifically uninitiated might confuse it with such. It’s just toxins coming out through sweat pores, like they’re supposed to do, only with a little boost because of an ionic attraction.
The “scientifically uninitiated” might also think we sweat out toxins. This is one of the most obviously ridiculous of all ideas about detox. Sweating is for cooling, not taking out the trash — it’s not a significant excretory pathway.17
No one has ever cured anything but stress in a steam room. A sweat lodge has never saved anyone from any kind of poisoning. And even if sweat-to-detox was a thing, you’d still have to explain how cooler, non-sweaty salt soaks are supposed to detox.18
Ionic attraction is just some icing on this quackery cake. It’s an awful idea, most widely known from “ionic foot baths,” one of the oiliest of all snake oils.
Ionic bonding is electrostatic stickiness, the atomic scale equivalent of rubbing a balloon and then sticking it to your hair. It doesn’t reach out and grab things like a tractor beam, let alone across a multicellular structure like a sweat gland; it’s more like velcro, bonds forming only when ions actually touch each other. Even if sweat glands did squirt out toxins, ionic attraction can’t help out by reaching across the gland any more than a charged balloon is going to scoot all the way across a room to get to your hair. Sweat glands are a lot bigger than ions. To an ion, a gland might as well be a giant train station.
There’s more,1920 but this is too silly to cover in depth. Detoxing by ionic attraction is pure marketing bafflegab, found only on websites like SacredHeartHolisticHealing.com.
And now back to osmosis …
Part 3
Absorption
Can Epsom salts actually get through your skin in the first place?
Skin is definitely waterproof (and therefore also osmosis-proof)
If Epsom salts do get into the body, or pull anything out of it, it’s definitely not by osmosis. Osmosis doesn’t work through the skin, because skin is almost perfectly waterproof. If it weren’t, you would dehydrate like an earthworm on a sunny sidewalk. (You do dehydrate significantly by sweating in a bath, of course21… but Epsom salts do not boost that (see last section).
The top layer of the skin, the stratum corneum, consists of dead, dry cells stuffed with a kind of embalming substance, keratin, a fibrous protein. Water can’t go through or around the keratin, thanks to a microscopic “uniquely structured fatty layer” between them, which no one knew existed until 2012.22 The presence and arrangement of lipids betwixt the keratin molecules results in “exceedingly low permeability.”23
There are routes past the stratum corneum, “shunt pathways” such as hair follicles and sweat glands, and some water molecules end up there, in contact with relatively naked cells — but these are waterproof in their own right.
Plus we have glands that coat the skin in waterproofing oils! So there’s that too. When those oils wash off, the dead skin cells can soak up a little water and swell a bit, like soaked beans. (Fun fact: that’s not the cause of skin pruning. Skin pruning is actually an active process for improving grip in wet conditions.24)
What is waterproof is osmosis-proof by definition. The skin is an effective barrier to diffusion of water molecules and therefore of osmosis. This is not to say that nothing gets past the skin, just not much, and definitely not water.
Skin: also a booze barrier
“Human skin has unique properties of which functioning as a physicochemical barrier is one of the most apparent. The human integument is able to resist the penetration of many molecules.”25
Alcohol molecules, for instance, maybe. You can’t get drunk through your skin, alas. Contrary to the Danish myth. As amusingly shown by Danish researchers in late 2010.26 It’s funny, but it’s not a joke. Of course, the Danish experiment isn’t perfect, and may be contradicted/complicated by other studies in the future. (It would be interesting to see what happens with ethanol, for instance.)
But the point is that it’s completely non-obvious to people what substances can or cannot get through the skin. Ask your friends: most of them will guess that some alcohol probably does get through the skin — maybe not enough to get drunk (or booze baths would be a more popular practice), but some. In fact, obviously either very little or none at all gets through, contrary to “common sense.”

It isn’t obvious to anyone what kinds of substances in a bath can or cannot “soak” through the skin.
This next part of this article — seven sections — has delivered the most detailed information available on the web about the transdermal absorption of magnesium for well over a decade now. And yet all the average reader needs to know is that soaking in the stuff is kind of a terrible way to get magnesium into your tissues… if it works at all. It’s complicated, of course, but absorption clearly doesn’t work all that well.
But why? And what are the limits of our knowledge? The scientific details are superfluous for most people, but genuinely fascinating! Which makes this subject matter ideal members-only content. The free article continues below the members area — there’s still a great deal of reading left! Even without the extensive absorption digression. The whole article is a beast at 22,000 words; I have set aside about 4,200 of them for members: about 15 minutes of extra reading.
Most PainScience.com content is free and always will be.? Membership unlocks extra content like this for USD $5/month, and includes much more:
Almost everything on PainScience.com is free, including most blog posts, hundreds of articles, and large parts of articles that have member-areas. Member areas typically contain content that is interesting but less essential — dorky digressions, and extra detail that any keen reader would enjoy, but which the average visitor can take or leave.
PainScience.com is 100% reader-supported by memberships, book sales, and donations. That’s what keep the lights on and allow me to publish everything else (without ads).
- → access to many members-only sections of articles +
And more coming. This is a new program as of late 2021. I have created twelve large members-only areas so far — about 40,000 words, a small book’s worth. Articles with large chunks of exclusive content are:
- Quite a Stretch
- Does Epsom Salt Work?
- Heat for Pain and Rehab
- Your Back Is Not Out of Alignment
- Trigger Point Doubts
- Does Fascia Matter?
- Anxiety & Chronic Pain
- Does Massage Therapy Work?
- Does Posture Matter?
- A Deep Dive into Delayed-Onset Muscle Soreness
- Does Ultrasound or Shockwave Therapy Work?
- A Painful Biological Glitch that Causes Pointless Inflammation
- Guide to Repetitive Strain Injuries
- Chronic, Subtle, Systemic Inflammation
- Vitamins, Minerals & Supplements for Pain & Healing
- Reviews of Pain Professions
- Articles with smaller members sections (more still being added):
- → audio versions of many articles +
There are audio versions of five classic, big PainSci articles, which are available to both members and e-boxed set customers, or on request for visually impaired visitors, email me. See the Audio page. ❐
I also started recording audio versions of some blog posts for members in early 2022. These are shorter, and will soon greatly outnumber the audio versions of the featured articles.
- → premium subscription to the PainSci Updates newsletter +Sign-up to get the salamander in your inbox, 0–3 posts per week, mostly short, sometimes huge. You can sign-up for free and get most of them; members get more and their own RSS feed. The blog has existed for well over a decade now, and there are over a thousand posts in the library. ❐

Change or cancel plans any time. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism. For more information, see the membership page. ❐
PREVIEW: Headings in the members-only area…
- So, what does get across the skin? Because obviously some things do
- Testing magnesium absorption on harvested human skin samples
- Some evidence against absorption: Israeli soldiers smear magnesium all over themselves in high concentrations and it doesn’t get inside
- Frequently cited evidence for absorption: Rosemary Waring’s little unpublished 2006 study
- Hot hot hot! Does heat increase skin permeability?
- Maybe up your bum? Or hoo hoo? Nostrils? Absorption via mucus membranes
- Absorption “conclusions”
So, what does get across the skin? Because obviously some things do
The skin is not a perfect barrier to all substances in all ways, which is obvious because of medicinal patches and creams, allergic reactions, and contact poisons. So some things do indeed get past that fibrous, fatty outer layer to interact with the living cells beneath, and some even go straight into the cells without an invitation (no receptor, no active transport). For instance, DMSO (dimethyl sulfoxide), the industrial solvent and pain nostrum, diffuses not only through the skin, but passes through cell membranes like they aren’t even there, and so it quickly spreads through the whole body. For this reasons, it is used in drug patches to aid absorption — though there are trials showing that the “carrying” part doesn’t necessarily help.27
So how do some compounds get through the skin, even though it is generally a very sturdy barrier? There are many factors.
Size might matter. If molecules are small enough, they can slip through the skin like a small fish through a loose net. In 2000, Bos and Meinardi argued that a teensy enough molecule, smaller than an atomic mass of 500 Daltons, can drift through the stratum corneum28 — the “500-Dalton rule.” And the magnesium ions in an Epsom salt bath are way smaller than 500 Daltons, at a barely-there molecular weight of just 24 Daltons.
I’m sure we can just stop there. There’s probably no debate or uncertainty about this, probably no other obscure and technical chemistry considerations. The magnesium is small enough to get through, case closed.
Ha ha, just kidding!
It’s likely that size doesn’t matter at all in some contexts. Bos and Meinardi were not the last word on the 500-Dalton rule: they knew that most contact allergens were sub-500 molecules, but they didn’t realize that most other relevant molecules are too.29 Contact allergens don’t actually have to get through the stratum corneum to cause trouble — they can get through glands and hair follicles.30 Size might still matter for drugs,31 but it does not for allergens.
And still more complexity: magnesium ions have some special properties that might be highly relevant to their absorption. Bizarrely, they may swell dramatically when wet, like tapioca! In fact, this has been the conventional wisdom for some time, and one of the main reasons that many experts have dismissed the possibility of magnesium absorption.32
So … now is the case closed? Wet magnesium gets too fat for absorption? Still no! It turns out this rabbit hole goes way deeper than any rabbit would ever care to burrow. The conventional wisdom about Mg ion swelling has been challenged by some recent research. And I’m going to get into it, because whee, science is fun! But I’ve already gone far enough to make the important meta point here: no one bloody knows how this actually works, and if you think you can guess whether or not magnesium ions get through the skin, please give your head a shake. Biology and chemistry is mind-bogglingly complex and the details are truly, madly, deeply non-guessable.
Testing magnesium absorption on harvested human skin samples
Science: Hey, can I have that skin off your belly? You don’t need it right?
Tummy Tuck Patient: Um, sure …
Science: Thanks! Got to find out if magnesium ions can get through that.
This section is all about one odd experiment33 that involves a number of strange rituals performed on skin samples, like gluing hair follicles shut with super glue. It almost answers the tricky scientific question of whether magnesium ions can be absorbed through the skin, but it still falls short.
It does convincingly show that magnesium ions can diffuse through the stratum corneum, and that hair follicles probably facilitate that movement, but it does not establish that they do so in clinically meaningful numbers, especially in the conditions of a typical Epsom salts bath. Regardless, it’s neato science.
- They tested the skin as-is, but for comparison they also tested skin that was damaged by applying tape and ripping it off, 30 times!
- And they tested skin with hair follicles that they actually plugged with tiny little microscopic dabs of super glue (the details are a bit technical, but basically that’s what they were up to).
- And they used a fluorescent dye that binds to magnesium ions, so they could track its progress through the skin.
Like I said: an odd experiment.
They tested 5, 15, and 60-minute exposures of two concentrations of magnesium solution, medium and strong, corresponding to ocean water and the Dead Sea respectively. (Note that these concentrations are much greater than the concentration of salt in a typical Epsom salt bath. Which matters.) Their key findings:
- “topically applied magnesium permeates through human stratum corneum”
- “magnesium permeability varies based on concentration and time of exposure”
- “hair follicles have significant contribution towards magnesium penetration through skin”
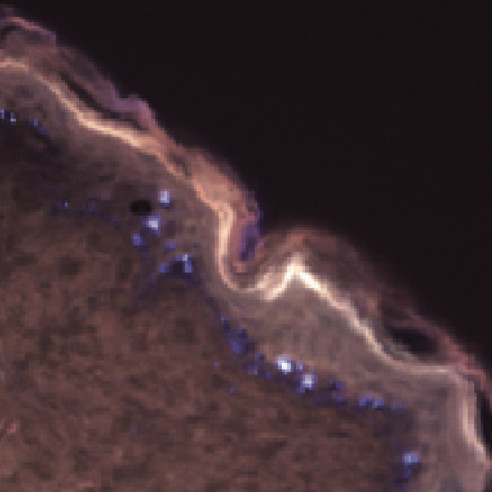
Magnesium ions diffusing through the stratum corneum. The brighter the warm-toned pixels here, the more magnesium.
So, voila, absorption! But there are some major caveats, of course.
- It’s clear from their imagery that a lot of Mg ions remain “stuck” in the most superficial layer of the stratum corneum, like hair in a drain filter.
- Even at concentrations much higher than anyone would normally put in their bath, “a significant increase was only observed at 60 minutes.” Almost nobody is taking super salty hour-long baths (except at “float spas,” more on this below). At 15 minutes, the medium concentration exposure is barely different from none at all.
- Although they claim a “significant” contribution of hair follicles, this is an irritatingly poor word choice. They mean statistically significant, not “important” or “large”… and it’s right on the very margin even of statistical significance (p <0.05).
I got into the details of this science not because it proves that magnesium soaks through skin, but because it’s charmingly weird, and because it proves that the whole problem is so absurdly complicated that we absolutely cannot guess the solution. Not even an extremely educated guess. Walter White couldn’t guess it. There are just too many ways the messy details of biology might surprise us. The only way to actually find out is to set aside the speculation about what’s possible in principle, and just do some proper before-after testing of magnesium absorption, in actual medicinal situations …
Some evidence against absorption: Israeli soldiers smear magnesium all over themselves in high concentrations and it doesn’t get inside
This quote from a book by Dr. Kenneth B. Singleton35 was submitted to me by a reader as an allegedly “authoritative” opinion on absorption:
Regularly bathing in hot water to which Epsom salts have been added can help draw out toxins from the skin.
Actually, that is not an authoritative opinion: it’s a vague and silly one. That anyone would mistake it for authoritative is rather depressing.36 The only thing that can determine whether magnesium heptahydrate is absorbed from a bath is careful, thorough testing — opinion is irrelevant, even from a real expert.
Fortunately, not all my mail is so depressingly gullible. Hat tip to reader Bryan B. who found an interesting Israeli military study and sent it to me. (I love it when readers do that.) It’s a safety study of a lotion developed “to improve protection against chemical warfare agents.”37 Like suntan lotion, but for chemical burns. Yikes.
This lotion had rather a lot of magnesium in it. And soldiers were not poisoned by the magnesium. Indeed, it didn’t appear to cross the skin at all: “there were no significant differences in magnesium levels between the placebo and the study groups in any of the applications.” The delivery system — lotion — could be quite different than soaking in water with dissolved magnesium sulfate. But it is pretty noteworthy evidence that absorption is minimal or nil when putting high concentrations of Mg on the skin.
That information is not necessarily correct, but it is certainly more authoritative and worth bearing in mind, than the opinion of Dr. Singleton.
Frequently cited evidence for absorption: Rosemary Waring’s little unpublished 2006 study
In 2006, Rosemary Waring, a British biochemist at the University of Birmingham, did a nice science experiment with Epsom salts.38 She did more or less exactly what any curious person would do if she wanted to know whether or not Epsom salts can get past skin: she measured magnesium and sulfate in the blood and urine both before and after people bathed in Epsom salts.

Dr. Rosemary
Waring
She found them to be higher after the baths! 16 out of 19 people had more magnesium and sulfate in their blood after the baths than they did before the baths.39
Dr. Waring’s results are straightforward. No therapeutic effects of Epsom salt were studied or claimed — she just studied absorption, and did not try to make any more of it, showing the restraint of a pro. What could be simpler?
I was so interested in these results (although still a bit skeptical) that I contacted Dr. Waring by email. “I agree that it is a bit surprising,” she replied, “but the results are certainly there and in fact there are hints in the past literature that this could happen.”
And how would it work, I asked, this crossing of the skin? Dr. Waring:
I don’t have any evidence as to how magnesium sulphate crosses the skin, though I have always assumed that it simply diffuses across the stratum corneum, helped by the fact that it’s in a hot bath.
Possibly not the best science ever done
Dr. Waring’s study has been cited thrown in my face by countless people over the years who think I am not aware of it. Every member of this widely distributed angry mob read this article only just far enough to get angry enough about my skepticism to send an email. Many of them claimed to have read the whole thing, but apparently they missed Dr. Waring’s name in a heading, her photo, or the full section of analysis. And, shocker, none of them seemed to be aware of the potential problems with Dr. Waring’s research.
And there are some problems.
For starters, unfortunately twenty years later, her tiny experiment has never actually been published,40 and that’s a major reason for caution.41 It is a basic rule of science that evidence can’t really be taken too seriously until it has been exposed to peer review and repeated by other scientists. Just because experimental results haven’t been replicated yet doesn’t mean we ignore them, but it does mean that we have to take them with a grain of salt. (That pun was simply unavoidable.) Also, Dr. Waring also has a relevant bias: she’s interested in magnesium supplementation as an autism treatment.42
I also think it’s notable that Dr. Waring’s speculation about mechanism is extremely basic. People assume because of her unpublished study that she’s a big time salt absorption expert, but obviously she wasn’t considering any of the chemical complexities discussed above … or below. She assumed, like most people, that the heat of a bath probably increases the permeability of the skin. But that’s not a safe assumption, or an expert assumption.
Hot hot hot! Does heat increase skin permeability?
Enough of it sure does. But probably not bath heat. Speaking of studies that get thrown in my face, someone haughtily hurled this one at me as if it was the last word, absolute proof that a hot bath boosts magnesium absorption. Let’s look …
A 2008 experiment showed that brief, intense heating of the skin can dramatically increase its permeability.43 Park et al. tested short bursts of heat: 5 milliseconds to 5 seconds at 100 to 315 degrees Celsius. With more heat, dramatically more molecules could cross (the duration of exposure had less effect). Skin permeability was increased by a few multiples in the low end of the range, all the way up to three orders of magnitude at the most extreme temperatures. Wow.
The mechanism is fascinating:
Is any of this applicable to baths and the absorption of magnesium sulfate?
The highest comfortable bath temperature for most humans is around just 40˚C (104˚F), which is far cooler than the coolest temperature tested in this experiment. The effect studied mostly depends on actually damaging the skin. It is conceivable that permeability starts increasing at lower temperatures with longer exposures … but sixty degrees lower? For the duration of a bath? Probably not for most substances. Skin probably evolved to be a good barrier across the range of temperatures humans are exposed to, which would certainly include 40˚C.
Also, not all substances will respond the same way to heat. If you studied transdermal delivery of many different substances at 100˚, you’d probably see a wide range of effects. The only way to know if the skin is more permeable to magnesium at 100˚ or 40˚than at room temperature (as with a lotion) is to check — and no one has, to the best of my knowledge.
And so this study definitely does not actually show that the heat of a bath enhances magnesium absorption … and neither does any other study I’m aware of.
Maybe up your bum? Or hoo hoo? Nostrils? Absorption via mucus membranes
How else could magnesium sulfate possibly get into the bloodstream? If it does, as Dr. Waring’s experiment seemed to show? Reader Adrian J. had an unusual idea:
Is it possible that the salt diffuses across the epithelium in the anus if the rectum relaxes to some degree in the warm water?
Wow, that’s some awesome lateral thinking! And I think it’s actually plausible, because now we’re talking about a “mucus membrane,” a completely different and much more permeable layer than skin. For what it’s worth, we know that alcohol absorbs quite handily through the rectum — rather too well, in fact, so do not try at home.44 But it has to be pretty much injected. (Live a little: click that footnote!)
But I find myself uncomfortably wondering … just how much do I relax in a hot bath? That much? And how much salt could diffuse across that more permeable but much smaller membrane? It’s a tiny target!
I shudder to think of the methods required to test this.
Vaginal absorption?
The up-yer-bum hypothesis was surprising, but you’d be even more surprised by how many readers have asked if the vagina might be an absorption route. A fair question, but this has the same problem as anal absorption: too small and too tight. After quizzing several bemused femme-friends about it, I am confident that it would be highly irregular for any respectable quantity of bath water to percolate into one’s ya-ya.
And you thought an article about salt baths would be boring! No wonder this is the most popular Epsom salts analysis on the Internet!
There is absolutely no relevant science on this topic that I’m aware of, and there may well never be. Obviously there are studies of vaginal absorption of various medications — it’s not in doubt that mucous membranes — but not of magnesium in bathwater. All we can do is consider the mechanistic plausibility that there’s sufficient exposure of mucous membranes to the salty water to matter. And that plausibility is super low.
How about inhalation? Another possibility for mucus membrane absorption
Maybe salt can be inhaled with steam. There’s actually a therapy (“halotherapy”) based on this, but it’s a weak idea in general and impossible as a salt delivery system: when water evaporates, it leaves most solutes behind, salt in particular.45 Many substances evaporate with water and “contaminate” steam — lots of volatile compounds and assorted tiny particles basically just getting thrown around, which is why we can smell a bubbling pot of soup — but these occur only in trace amounts, mostly nowhere near enough to be plausibly medicinal. Human olfaction, despite being shabby by animal kingdom standards, can still get a nice rich scent from a mind-bogglingly small number of molecules. Water from a soup is still remarkably pure despite the odour, and definitely has no salt in it.
Another related possibility is that we might inhale tiny droplets of water (aerosols of salt water) that float over the surface of a bath. Such droplets would contain dissolved salts at the same concentration as the bath, but these are nearly microscopic tiny water droplets. Remember that most people can swallow an entire magnesium pill with no obvious effect, which contains insanely more magnesium than you could ever absorb from the air over an Epsom salt bath, assuming there’s any at all, most of which would never even come close to a mucus membrane. Again, not really a plausible source of medicinal absorption.
Absorption “conclusions”
The Epsom Salt Council claims, without detail or nuance, that “magnesium sulfate is absorbed through your skin,” citing the opinion of the notorious Dr. Christiane Northrup to support the point, without so much as a link to substantiate that this is in fact her opinion. But it probably is: Dr. Northrup is not stingy with her beliefs. She’s on the record expressing belief in chakras, astrology, angels, mysticism, feng shui, and Tarot cards, and she has earned extensive, harsh criticism for the way she “famously pushes woo in the cause of women’s health.” But the Epsom Salt Council is happy to cite her.
The same page is littered with similar examples of shallow reporting and appeals to dubious “authority.” For instance, further along, they also cite Carolyn Dean on this topic … a former MD who had her Canadian license to practice medicine revoked. And so on.
That’s the kind of quality scholarship The Epsom Salt Council has brought to the conversation.
In this article, I’ve presented several lines of evidence, demonstrating that the absorption question is surprisingly complicated, interesting, and inconclusive. We will have to live with the mystery.
Meanwhile, it is obviously reasonable to be skeptical, as many experts are. There are many reasons to suspect that absorption is trivial. A thorough 2017 scientific review of both the evidence and rationale for transdermal absorption of magnesium makes a critical point: although there may now be adequate evidence to suggest that some transdermal absorption is possible in the right conditions, that evidence is not nearly strong enough to support claims that it is superior to oral supplementation.46 Gröber et al. conclude that they “cannot yet recommend the application of transdermal magnesium.”
It’s not just a matter of whether Epsom salts can be absorbed … it also has to be a better way of getting magnesium into the body than simply swallowing it, which is very easy. That’s a much higher bar to clear.
And then there’s the question of whether or not a little extra salt in your blood actually matters medically. And that finally brings us to the second major part of the article …
↑ MEMBERS-ONLY AREA ↑
Part 4
The therapeutic value of Epsom salt
If magnesium and sulfate ions can get from bath to blood, what exactly do they do when they get there?
If Epsom salts do get across the skin, so what? Is it any good to have some extra ions of magnesium and sulfate kicking around your bloodstream? Why did the ions cross the skin anyway? What’s the point?
Magnesium deficiency (hypomagnaesemia) may be a real problem, and it may also be related to pain, and so supplementation might make sense, and soaking in the stuff could be a way of getting some magnesium…
But probably nowhere near as good as just eating the stuff.
Sulphate deficiency could also be thing, but to a much lesser degree, and much less clearly. It’s a much more obscure topic, nearly science-free.
There is little doubt that extra magnesium sulfate has some effects on physiology in some contexts. Some of those effects are well known, including some common medical applications mentioned earlier. These include unpleasant effects, like diarrhea!
But, judging from the established medical uses/effects of Epsom salt, there is definitely no particular reason so far to believe that adding magnesium or sulfate to your blood is going to be much use to you — unless you have eclampsia, tetanus, or a confirmed magnesium deficiency.
Or possibly migraines or neuropathy. Or cramps. Maybe.
I’m aware of only one science experiment that seems to be directly relevant to the effect of more magnesium in the bloodstream for a symptom that might inspire an Epsom salt bath — muscle aching. It was a study of the acute effects of injected magnesium sulfate, which is presumably much like absorbing it, just faster. The injections “did not reduce muscle pain” and caused “unpleasant side effects.”47 Yuck! Not exactly encouraging!
So there’s not really any particular reason to believe anything about the therapeutic effects of Epsom salts for aches and pain. We can really only speculate. And speculating about basic biology is really difficult. It’s a great way to be wrong.
See also Examine.com’s magnesium page. Examine has a great team of experts and published terrific independent reviews of the science.
Sulfate supplementation (what little there is to say)
Magnesium is a mainstream electrolyte, a famous molecule, and many people are supplementing magnesium, for better or worse. But sulfate is obscure, and sulfate supplementation is quite rare. The magnesium information below is resting on fairly firm foundations, plenty of science; sulfate is an information desert by comparison. You can find a few popular articles about sulfate deficiency… most of which actually have very little to say about sulfate and quickly veer off into magnesium. There’s almost no science at all about sulfate deficiency.
I asked Dr. Waring to speculate about the therapeutic effects of Epsom salt, and she asserted that patients with rheumatoid arthritis are known to have “low sulfate levels,” but this is not really established science.48
And that’s really all I have — all anyone has — on the topic of sulfate supplementation. For the rest of the article, I’ll just be focusing on magnesium, which is on much firmer ground conceptually…
Magnesium deficiency and supplementation
Magnesium is one of the essential chemical elements, an element that is a critical biological ingredient — “life finds a way,” but not without a good supply of em-gee it doesn’t! We use a lot of the stuff: it’s one of the big three mineral nutrients, along with sodium and potassium.
If it’s missing, blood pressure rises, glucose tolerance drops, and our nerves get just a wee bit trigger happy. Interestingly, fixing an magnesium deficiency is actually sedating! It literally calms your nerves… and that could certainly be relevant to chronic pain. Most plausibly, it makes some sense in principle that it be helpful for cramping and/or neuropathy (pain originating from insult to the nervous system itself).
And yet pain is not on official lists of symptoms for magnesium deficiency! But it remains, just barely, possible that deficiency is a factor in some kinds of chronic pain. Not that it means much, but there are certainly plenty of anecdotes to that effect. I’ll explore what little science there is on the topic below.
Despite its biological importance and being readily available in food, deficiencies seem to be surprisingly common. This might be because depletion is a side effect of some common drugs, most notably alcohol, diuretics, asthma drugs, and acid reflux drugs. Vexingly, it may also “hide” from routine blood tests.49
These factors make magnesium very similar to vitamin D deficiency and pain: it might matter to a lot of people, possibly pain patients more than most, and supplementing is quite safe.50 In the extremely scammy world of supplements and nutraceuticals, vitamin D and magnesium both stand out as being less lame (especially for chronic pain patients).
Another extremely popular idea about magnesium is that it prevents cramps. This idea is mostly driven by the myth that cramps are caused by dehydration and a shortage of electrolytes, chiefly magnesium. Infamously for those who have followed performance science in the 21st Century, exertional cramps are almost certainly not caused by electrolyte loss or dehydration, acute or chronic.51 If low Mg doesn’t cause cramps, adding Mg probably won’t prevent them. We don’t actually have any direct evidence one way or the other, however. What little we do know about using magnesium to treat cramping with no obvious cause doesn’t seem to work,52 but it remains plausible that some specific types of cramping can be treated with magnesium. For a more detailed discussion of this sub-topic, see Cramps, Spasms, Tremors & Twitches.
Magnesium deficiency causes
How does one develop hypomagnesemia in the first place? From alcohol abuse and diarrhea.
It’s also a side effect of proton pump inhibitor drugs for heartburn and acid reflux. They are extremely widely used, but the prevalence of the side effect is unknown.53
And from a crappy diet with no salads! There’s plenty of magnesium in a decent diet. Despite this, deficiency occurs even in wealthy places because grains and meat are poor sources, and the good sources are not nearly as popular: salad, primarily. Leafy greens and nuts/seeds, especially spinach and pumpkin seeds. And potatoes are also a decent source, which is hardly a hardship. But anyone with a magnesium deficiency can suck it up and eat a nutty salad a couple times a week — or potato salad! — and Bob’s your uncle. So just eat it.
🎶 How come you’re always such a fussy young man?
Don’t want no Captain Crunch, don’t want no Raisin Bran
Well, don’t you know that other kids are starving in Japan?
So eat it, just eat itWeird Al Yankovic, “Just Eat it”
Magnesium deficiency symptoms
- weakness
- muscle spasms and seizures
- irregular heart beat
- and many more!54
“People who develop magnesium deficiency can suffer both neurologic and cardiac problems if their levels fall low enough,” writes Dr. Christopher Labos.55 “Patients with low magnesium levels can develop muscle spasms, presumably because a deficiency in magnesium lowers the electrical threshold at which nerve cells become depolarized, which makes them hyper-excitable. In peripheral nerves, low magnesium causes spasms in the muscles, but when it happens in the central nervous system, it can cause seizures.”
But does deficiency hurt?
Of course, deficiency has been widely anecdotally reported as a cause of miscellaneous body pain, and that increased magnesium intake is helpful. But hey, what hasn’t been so reported?
Pain is not a standard symptom of acute magnesium deficiency. This doesn’t mean that body pain couldn’t be a symptom of milder deficiency but not of more obvious deficiency, but that would be a surprise. If magnesium is involved in any kind of pain, it’s probably in a roundabout, risk-factor way.
For instance, intriguingly, deficiency and low-grade inflammation appear to be “interactive risk factors” — that is, they tend to go together.56
And fixing a deficiency tends to be sedating! It literally calms your nerves, and that seems like it certainly could be relevant to chronic pain.57
But it’s not like anyone has demonstrated that all (or most, or some) neuropathy patients are Mg deficient! Given its mighty reputation as a factor in neuropathy, you’d think someone would have done that study. But the link between hypomagnesaemia appears to be almost entirely based on biological plausibility.
Interesting as all this may be, the only thing that matters is the clinical question: does supplementation truly help? If it doesn’t, all the speculation about how magnesium might be a pain driver is a bit of a moot point. I devote a section below to this question. Spoiler alert: there’s very little evidence, and what little there is doesn’t clearly support a magnesium-pain link.

It’s easy to eat magnesium. You just have to be willing to eat salad. Or potatoes!
Bioavailability: magnesium is easy to get… sorta
In a hospital context, “Treating magnesium deficiency is both very easy and very hard,” says Dr. Labos. “In fact, the amount of time and effort spent replacing magnesium deficiency on the medical ward is somewhat mindboggling.” Why? There are issues with both intravenous and oral supplementation. Oral is “often not tolerated by hospitalized patients,” but when put directly into the bloodsteam, “blood levels spike temporarily and then about 50% of that magnesium is subsequently excreted in their urine within a few hours.” So you’d only do that if the deficiency is severe and acute — basically to stop seizures.
If you’re not in hospital, making a point of getting extra magnesium from pills or baths probably isn’t necessary: just eat right! That will work for most people, most of the time.
Unlike with vitamin D, which is a bit tricky for a lot of people to get, it’s downright easy to get enough Mg from a reasonably healthy diet. Despite this, Mg deficiency is common even in wealthy places because grains and meat are poor sources, and the good sources are not nearly as popular (salad, basically — leafy greens and nuts are especially good). But
So while some people might need magnesium, and deficiency might be related to pain, it’s easy to fix with food and even easier to fix by taking pills. Bathing in the stuff is like going a half hour out of your way to buy stale bread from a corner store when you live next to a good bakery.
But I’ll get into it anyway, just to be thorough.
“There is little role for supplementation in the absence of a documented deficiency, or in circumstances where a medical condition (e.g., celiac disease) or a medication (e.g., a proton pump inhibitor) may be interfering with dietary magnesium absorption.”
Scott Gavura, BScPhm, MBA, RPh, "Magnesium oil: Not so magical" on ScienceBasedMedicine.org
Does magnesium therapy for pain work?
The things that normal people use to self-treat their pain are rarely tested in good clinical trials. Today’s example: magnesium supplementation for chronic pain. Can it actually help patients? Is it basically a pain-killer? And shouldn’t we know that for sure by now?!
Of course we should! But of course we don’t. In this section, I’ll look at some of the scraps of science we do have, and the salamander will make some recommendations.
Testing magnesium with a keyboard and mouse
A 2020 study seemed to go out of its way to try to answer this question without actually talking to a patient with pain — pure data analysis.58 Tarleton et al. mined some old survey data on the health of more than 13,000 American adults (high-volume data, but also poor quality for this purpose, “low resolution”).
They reported a “protective effect” of “increased magnesium intake,” concluding that this “warrants further study.” Which everyone more or less already agreed on, but more data is good… right? Hm, not if it just muddies the waters. Data like this is can be like yelling in a crowded theatre, “There might be a fire! I think I saw some smoke!”59
But this is a far cry from conclusive evidence that taking magnesium treats any kind of chronic pain. This alleged protective effect of “increased magnesium intake” is inferred from notoriously unreliable self-reporting of diet. The possibilities for confounding factors are endless.
Not a great paper.
A Canadian review of not much magnesium therapy science
Banerjee et al. concluded in 2016 that “magnesium appears to have an analgesic effect.”60 Hooray? But don’t read the fine print if you want to hang on to that good feeling.
Their own summary of findings doesn’t seem to back up the optimism.61 And that’s just all they wrote about the data. If there’s enough evidence to justify “magnesium appears to have an analgesic effect,” it is not reported in this paper.

One of the few good trials of magnesium for neuropathic pain
In 2013, Yousef et al. did a true trial of magnesium supplementation for back pain62 — but, crucially, only back pain with a neuropathic component.63 40 patients got intravenous magnesium for two weeks, then oral for another month, and their progress was compared to 40 patients who got a placebo in the same ways.
The patients who got magnesium clearly did better in the long run.64 The improvement wasn’t huge, but it wasn’t small either. I wouldn’t turn it down.
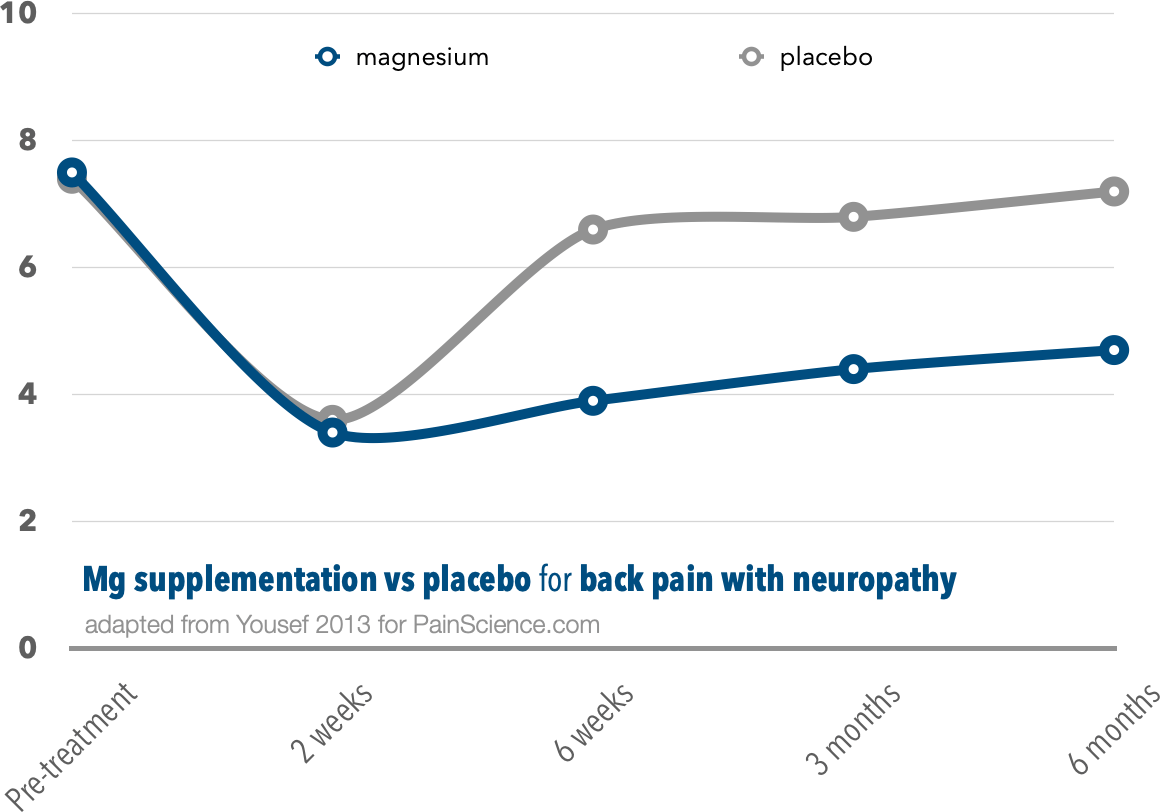
This is a clearly positive result on its face — which is such a rarity in this field that it’s cause for too-good-to-be-true concern. It is “just one study,” with unknown flaws, and still unreplicated as of 2024. Most important, this experiment just cannot tell us anything about the effect of magnesium on ordinary aches and pains… which are probably mostly not neuropathic.
But, for whatever it’s worth, it is indeed a properly positive result — and that’s more than we can say for a great many other trials of any intervention for any kind of back pain. It is noteworthy. If I had neuropathy, I’d probably start eating more salad.
Magnesium as a pain-killer after surgery
Here is some evidence that magnesium may reduce pain because it is a “calcium channel blocker and N-methyl-D-aspartate antagonist,” as in a 2009 experiment.65 (There’s a section devoted to calcium channel blocking below.) Several other studies have been done, with conflicting results, and generally poor quality (of course). Most of these were reviewed in 2007:66 four showed a minor but technically positive effect, seven showed no effect greater than a placebo, and in one experiment the subjects actually experienced more pain (ouch).
And so, although “the biological basis for [magnesium’s] potential antinociceptive effect is promising,” the authors actually concluded that no pain-killing effect could be found.
These conclusions were basically repeated in a 2018 review,67 despite the inclusion of some positive studies (like the 2009 one cited above). So much for the miracle of calcium channel blockage: the data taken as a whole doesn’t just fail the “impress me” test, it is actually convincing in the other direction.
•
Despite the discouraging state of the evidence, the question is just not answered yet, and there actually is a plausible mechanism for magnesium ions reducing pain. While it is clearly neither well understood nor reliable, it does exist, and it might shine in the right circumstances. But I doubt those circumstances are an Epsom salt bath.
Epsom salts baths as a source of magnesium
To embrace Epsom salts baths as a helpful method of supplementing magnesium, at least three things need to be established:
- Magnesium deficiency has to actually be causally linked to common aches and pains — not more serious/chronic pain. While it would be a big deal if we knew that magnesium deficiency was a factor in chronic or serious pain, it wouldn’t have anything to do with the legend of Epsom salts, which are supposedly good for minor acute pain.
- Magnesium supplementation has to actually be an effective treatment (regardless of the source). Even if a lack of the stuff is a problem, simply oversupplying the system will not necessarily help. Not all deficiencies are caused by an inadequate supply! The classic example is malabsorption of iron as a cause of iron deficiency: it doesn’t matter how much you consume if you can’t absorb it.
- An Epsom salts bath specifically has to be actually better than dietary sources or oral supplementation — otherwise, just eat the stuff!
None of these things has actually been established, and the absence of any one of them is a deal-breaker for bathing in magnesium.
Magnesium as a pain treatment — as an analgesic — has just never been tested properly, and I’ll get into that in considerable detail below.
Magnesium absorption versus consumption
Even if it is effective to “just add magnesium” as a treatment for aches and pains, it’s extremely unlikely that bathing is the best way to add magnesium to your body… especially when there are such obviously viable, convenient alternatives. And likely more effective ones. Dietary and oral supplementation is likely to be much more effective. Or consider that one positive study I just mentioned: intravenous supplementation!
The increased levels of magnesium ions shown by Dr. Waring’s experiment — the most absorption-friendly evidence available — were quite small (and there was no increase at all in some subjects). Consistency in dosing would also be impossible by bath, since we simply haven’t got a clue how much gets absorbed, if any, never mind its chemical fate after that.
While it is of course possible that we can supplement magnesium by soaking in it, I can’t really see why anyone would actually prefer that option to just eating some extra nutty salads. And potatoes. See dietary sources of magnesium.
No matter what magnesium can do, it can’t do everything
This is a classic problem with all kinds of supposedly amazing pain cures: pain has too many different causes for one medicine to be really effective. There are many types of body pain that have little or nothing at all in common with each other physiologically. To name just a few examples of pain causes that are biologically distinct from each other:
- drugs side effects
- vitamin D deficiency and pain — good luck treating that by soaking in magnesium
- traumatic injury pain (acute inflammation)
- repetitive strain injury (subtle, low-grade inflammation and tissue degeneration)
- idiopathic neuropathy
- genetic hypermobility
- sensitization
- analgesic rebound
- muscle cramping (just one of many kinds of muscle pain)68
- delayed-onset muscle soreness
All of these work in different ways, and so no one thing can possibly treat them all effectively, or even a few of them. (And it’s not even a complete list! Here’s a complete list.) For instance, an anti-inflammatory medication would fail with almost all of them except the acute inflammation of a recent injury. Even the subtle, low-grade inflammation of repetitive strain injury seems to be too different from acute inflammation for those medications to work.
While it’s certainly possible that increasing levels of magnesium ions in the bloodstream could help with one or two kinds of pain problems, it’s extremely unlikely that it would help enough different sorts of pain to be generally “good for” pain, especially the kind of acute soreness that we all occasionally suffer from.
Similarly, Epsom salts probably cannot simultaneously perform both of the two tricks most often touted: “relieve pain” and “speed healing.” Those are completely different things, and it’s unlikely that one substance can help with both goals.
Those goals might even be mutually exclusive. For instance, the primary source of injury pain is inflammation — a complex and painful physiological process intended to … wait for it … speed healing. Indeed, the only known mechanism by which you can in principle recover faster from an injury would be to increase inflammation. If bathing in Epsom salts did that, it would make you hurt more, not less. Of course, there could be other ways to speed up healing — in an “anything’s possible” kind of way — but it’s still pretty far-fetched that a single molecule could pull off both that miracle and reduce pain at the same time.
The point here is just that the conventional wisdom about epsom salts is pretty murky and non-specific about exactly what and how and it is supposed to help.
Good for “brain troubles”
Salt has been used for well, just about everything. Like these effervescent brain salts. Cory Doctorow: “The best thing about effervescent brain salt is that it’s not immediately clear whether it’s salt to make effervescent brains even more delicious, or salt to give you an effervescent brain, or effervescent salt for brains. Also, it appears to come in a Tabasco bottle, and everything that comes in a Tabasco bottle is always awesome.”
What’s a calcium channel, how do Epsom salts block it, and who cares?
Once in a blue moon, you’ll see Epsom salts (or magnesium in particular) described as a “calcium channel blocker” with the implication that this is obviously good for pain. Unsurprisingly, this is another misleading oversimplification. Although it’s more specific and impressive sounding to talk about calcium channel blocking, it’s not a heck of a lot more meaningful than talking about “detoxification.”
Calcium channels are itsy bitsy holes — molecular scale holes69 — in cell walls that let calcium in and out as a trigger for a bunch of biochemical business. They exist primarily in muscle tissue, blood vessels, and neurons. There are a number of druggy ways to interfere with them, including magnesium. Calcium channel blocking is fairly well understood physiology, and the main clinical application is to decrease blood pressure (which it does by reducing the strength of muscle contraction in the heart and blood vessels). Although other effects undoubtedly exist, there is no particular reason to believe that they have any potent effect on any flavour of pain. In fact, there is an excellent reason to believe that they don’t: because no one is even claiming it.
Calcium blockers aren’t rare drugs; lots of people have these chemicals in their blood. But
Yes, it is possible that magnesium absorbed through the skin does something different, something good, for certain kinds of pain. After all, different calcium blocker drugs have different effects! But there’s not a shred of good, direct evidence of it. So it really boggles the mind that anyone would toss this idea around with any confidence. Seriously, they’re pretty much making it up as they go — wild speculation.
Another possible biological effect: antibacterial? Osmosis and all the wee beasties
Reader Dorrie B. pointed out something interesting: Epsom salts might be an effective treatment for topical skin infections, as salt is certainly inhospitable to many microganisms. It can suck them dry, like the potato in the classic osmosis demonstration. This is probably the explanation for some rare prescribing practices I’ve heard about, such as recommending Epsom salts baths for anal fissures.
Yes, my email inbox has anal fissures in it.
An Epsom salt bath definitely cannot disinfect a puncture wound (as one of my readers was told). A strong salt solution is anti-bacterial, but the problem with rusty nails is the risk of deep injection of Clostridium tetani — far beyond the reach of any soak.70
But this is also a great example of how complex these medical puzzles can be, because salt bathing might also damage populations of other bacteria on the skin, and/or make the skin more habitable for bacteria (moister), resulting in more vulnerability to infection rather than killing one.71
Do people who bathe or swim in salt water regularly suffer any ill effects? Are they more susceptible to new infections? They might well be: even a 10% or 20% difference would not be obvious to the victims, but would nevertheless be clinically significant and biologically interesting. That research hasn’t been done, but my point is just that it’s always surprisingly difficult to say whether or not a given biological effect is good. Usually “it’s complicated” — the official slogan for this article.
Mixing up the effects of salty and non-salty baths
Obviously non-salty baths have some benefits of their own. People like baths “because reasons.”72 What’s funny is that Epsom salts routinely get the credit for these benefits. Here’s how this happens in six easy steps:
- Patient has a chronic ache or pain and tries to treat it with non-salty hot baths or soaking. However, because it’s just a bath and expectations are low, this effort is never particularly diligent. This is key to the setup: the patient has never really given non-salty soaking a good try.
- Patient gets the idea to try Epsom salts! This seems much more promising. Now there’s medicine in the bath.
- Thus inspired, the patient proceeds to soak quite diligently — much more diligently than ever before.
- When some benefit is then observed, the patient attributes this to the salt — of course. Maybe it is, but maybe it’s just the unusual regularity of the nice hot soaking. Relaxation alone is definitely a potentially relevant effect. But the point is that we obviously can’t know … but the patient is now officially biased in favour of salt.
- If the benefits are at all notable, this person will usually start proclaiming to anyone who will listen that they “know” that Epsom salts work.
- When challenged (“It might be just the hot bath, eh?”), they will almost certainly object and claim (correctly!) that they have tried simple hot soaking without results. They have indeed. But it was never actually tried well enough to really know.
Tricksy, the human mind is.
Flotation therapy
Is there any other reason to put Epsom salts in your bath? Well, Epsom salts dissolved in your bath does make the water feel nice. 😉 No research is required to prove that: just try it! Most people agree that the water feels smoother, slicker, silkier.
And then there’s the buoyancy, which is actually the basis of an entire industry.
Salt makes you floatier! Infinitesimally floatier. High concentrations of Epsom salt in your bath will increase the water’s specific gravity (density) to the point where you will start to float — just like in the Dead Sea, or Utah’s Great Salt Lake — because the body is, on average, much less dense than salty water. The concentrations of salt required for flotation therapy are much higher than Epsom salt packaging recommends, by the way.73 However, any salt in your bath — Epsom or otherwise — is going to make you at least a little bit lighter in the water.
Most people don’t bathe in high concentration of Epsom salts for long periods — probably 99.9% of all Epsom salts baths are home baths with very low concentrations.
But that’s at home! You can also pay to bathe in much, much higher concentrations. Flotation baths and tanks are quite popular, and I have tried them and I’ve enjoyed them. Although the floating industry is not new — sensory deprivation tanks have been around for decades — it has definitely been surging. There are several new float spas here in Vancouver in the late 2010s. In some places, the flotation industry is selling frequent and long salt baths, up to two hours of soaking and floating at a time. That much time is a luxury very few people can afford! Shorter floats are much more common.
It’s plausible that bathing in such high concentrations has different effects than home Epsom salt bathing, but no one is studying that.
The main purpose of flotation therapy is to reap the benefits of deep relaxation, which are noteworthy.74 It’s a lovely experience, but it’s also irrelevant to the relief of muscle aches and pains except via the straightforward (and perfectly legit) mechanism of relaxation.
For more detailed discussion of flotation and immersion therapies, see Get in the Pool for Pain: Aquatic therapy, aquajogging, water yoga, floating and other water-based treatment and injury rehab options.
Part 5
Wrapping it up
Consider the source
98% of the time, “osmosis” and “detoxification” are the concepts presented as the justification for bathing in Epsom salts. Don’t trust advice that is so obviously simplistic. It involves huge leaps of logic and avoidance of detail… all made by people who are usually trying to sell the stuff. Consider the source.
Epsom salt bath prescriptions are often embellished with some really strange claims of healing powers. For instance, I found one website that recommended taking Epsom salts internally as well as bathing in them:
Researchers in nutrition, through controlled experimentation, have found that Magnesium sulfate accelerates the body’s healing time by 30%. As an example, if an injury required three weeks to heal under normal or standard conditions, it would only require two weeks to heal if Magnesium sulfate was added to the diet as a nutrition [sic].75
That’s really ludicrous. Accelerated healing time is a comic book concept — something Wolverine does — not an even remotely legitimate medical concept. And imagine the unpleasant surprise of the hapless reader who takes this advice when they discover the laxative effects of ingesting Epsom salts! Naturally, no source for this alleged experiment was given.
Epsom salts bathing is often recommended carelessly and overconfidently, without any genuine knowledge of the physiology or science (or lack thereof). Those who claim to “know” that Epsom salts work cannot seem to demonstrate that they also “know” much about physiology or science. While it certainly remains possible that there is a therapeutic effect, it’s pretty clear that we shouldn’t take their word for it.
Selected questions and answers
Some questions too common to ignore… some questions too funny not to try to answer… and one or two that are just good questions.
Q. Why would the FDA allow studies to be published that show Epsom salts are more effective than their muscle relaxers and pain pills? For $1/lb of epsom salt this would kill their market and profits.
A. Industry protectionism for baths? Preposterous! The FDA has literally nothing to do magnesium sulfate research. Any Big Pharma/FDA conspiracy against Epsom salt is clearly failing, because the stuff is available literally everywhere, and the FDA actually approves it for use as a laxative and a variety of external uses. Approval seems like kind of a funny way of implementing an anti-salt agenda. In short, this question is just knee-jerk anti-mainstream medicine paranoia based on major misunderstandings of what the FDA is and how it works. Nevertheless, it is a concern I’ve often see expressed, so I decided it was time to address it here.
Ironically, if there is any relevant commercial bias, it is one in favour of Epsom salts. For instance, the Epsom Salt Council exists to promote the industry and is “eager to let everyone know the benefits of our product and … spread the word about the wonder that is Epsom salt.” They prominently publish uncritical and unequivocal claims of medical benefit on their website.
Q. So you don’t believe that Epsom salt will do anything in a bath. How about sea salt? You believe it’s the same? Useless for muscle aches and stuff like that?
A. Yes, I believe it is “the same,” at least insofar as it is probably “useless muscle aches and stuff like that.” Of course there is much more chemistry going on in sea water than Epsom salt baths, but not in any way that seems to make any practical difference. In fact, it’s pretty clear that people who swim in the ocean a lot are not enjoying impressive pain-killing benefits the rest of us are missing out on — which is yet another example of how the skin is a pretty effective barrier. Sea water isn’t medicine, and no one who matters thinks it is.

Do not try at home
Oddly, there are a lot of electric baths in medical history. Electricity was a wonderful way to make health ideas based on vitalism seem more real and science-y.
Q. Maybe there’s a “bio-electric” function to Epsom salts in water. There’s more and more being discovered about small electric/magnetic fields and how we are affected by them.
A. Er, no, I think not. It’s not inconceivable, but it is pretty far-fetched. It’s generally true that biology ingeniously exploits most properties of nature to get things done, including electromagnetism, and we likely still have things to learn about that (that’s what the book The Body Electric was about, and despite its age and flaws it’s a darned interesting read). But whatever those systems might be, it’s super unlikely that they have any meaningful interaction with a slightly salty bath, let alone one that’s relevant to aches and pains. It’s even less likely that any such effect wouldn’t be much more obvious in, say, sea water (see last question). Even if salty baths just bestowed a vague feeling of well-being and vitality, like mountain air, that would be biologically remarkable … but also still well short of a useful medical effect. And in fact salty baths do not have an obvious mountain-air like goodness.
Q. Why does the bag of epsom salts (and other random places online) warn that diabetics should not take baths with epsom salts?
A. That’s a bit of a stumper. As far as I can tell, it’s just about the fact that diabetic feet are vulnerable, and soaking increases the risks of infection that they might miss due to impaired sensation. The foot has a very thick and often damaged superficial layer of the skin (stratum corneum), which might make it a little more vulnerable to damage from soaking, but that’s any kind of foot soaking: I see no obvious reason for singling out Epsom salt soaks, except that it’s popular. Maybe diabetics, with their many foot problems, are somewhat more likely to want to soak their feet. Ironically, one of the few good medical benefits of Epsom salts may actually be infection control. It might be bit of a topical antibiotic… but it could also help microorganisms, a caveat we explored earlier.

Q. Is Epsom salt good for a hangover? Something to do with electrolytes …
A. Electrolytes are ions (like magnesium) in an electricity-conducting solution (which includes blood), and they have countless roles in our physiology. Getting drunk can deplete and/or disturb electrolytes (“electrolyte chaos” is a thing with alcoholics). So that’s the kernel of truth here, but there are many problems on the way from the kernal to the idea that Epsom salt actually being “good for a hangover.”
Let’s start with the fact that it’s fairly unlikely that soaking in Epsom salts is actually an effective way to get some magnesium into you in the first place. Meanwhile, food is hands-down the best form of electrolyte supplementation, and water is the best overall treatment for hangover because most of the symptoms are due to dehydration, not electrolyte depletion/chaos. And then there’s the fact that magnesium is only one of several important electrolytes. And then there’s the biggest problem: with your garden variety hangover, there is some electrolyte imbalance due to the dehydration, but not major shortages of electrolytes. The mechanism for significant electrolyte depletion is a lot of vomiting, diarrhea, and sweating, which is only going to be applicable to the very worst of all hangovers. That’s a lot of problems!
But Epsom salt is mainly reckoned to be good for a hangover for the same simplistic reasons it’s touted for everything else: detoxification and relief from aches and pains. A hangover hurts, right? And you’ve basically poisoned yourself! Since the thinking about Epsom salts never even remotely attempts to get specific about what kinds of toxins or aches and pains, really any of them are candidates.
It doesn’t work. Believe me, I’ve tried. This is the kind of “medical” advice you’re going to get only from celebrities and amateurs.
Q. I am currently pregnant and looking into ways to treat fluid retention. Many websites say that epsom salt baths will “draw out” the excess fluids but I can’t find any information about this being studied at all. I will probably try it tonight anyway, but as a scientist I would love to know if there is any basis to it.
A. This idea about Epsom salts bathing is relatively rare, but it is also much more about the idea of osmosis than the more common detoxification claim. Any talk about the “drawing out” of water is definitely about osmosis (whether the speaker knows it or not). There’s a classic science classroom demonstration of osmosis, which involves sucking the fluids out of a potato by soaking it in salt water. That’s a perfect analogy for this claim. If a potato could be “bloated,” it could take an Epsom salts bath to solve the problem, and osmosis would be the mechanism.
Unfortunately, we are not like potatoes, and this simply will not work for bloated humans, because the skin is totally impermeable to water, as discussed thoroughly in the first third of this article. Nor is there any plausible pathway for osmosis across mucus membranes — unless you’re taking a very weird bath, there simply isn’t enough contact between any mucus membrane and bathwater.
Final thoughts
I can do no better in defense of Epsom salt bathing for aches and pains than “anything is possible.”
Although this folk wisdom may someday prove to have a sound rationale, clearly there is none that its advocates have thought of — or even tried to think of, it seems.
There is no good or specific reason to believe that bathing in dissolved Epsom salts will have the slightest effect on common kinds of aches and pains, muscle soreness after exercise, injury recovery, let alone any more serious kind of pain (migraine, neuropathy). Even if magnesium was effective for any of those things — which is far from established — it’s not going to be effective for all of them, and absorption is clearly inferior to dietary sources and oral supplementation in any case.
There’s decent evidence that Epsom salts just can’t get past the skin barrier — Israeli soldiers can smear on magnesium rich cream without the slightest effect on their blood levels of magnesium. That’s pretty damning.
On the other side of the evidence, thanks to Dr. Waring, we know that it’s still possible that we are a living experiment in absorbing magnesium sulfate ions every time we bathe in dissolved Epsom salts! And maybe, just maybe, they do something worthwhile once they get past the skin. And it’s very cheap, and almost certainly safe — just as no one is obviously getting any miracle cures out of Epsom salt bathing, they aren’t suffering any obvious ill effects either.
So, why not? At the very least, they’ll make your bath feel silkier! And at most? Who knows — maybe those magnesium and sulfate ions do have some healing powers. It’s not impossible. Just don’t buy into all the crap about osmosis and detoxification. As the old Scottish proverb says, “Always keep your mind open — but not so open that your brains fall out!”
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Part 6
Appendices
Still need help with myofascial pain? Now that you probably won’t be counting on Epsom salts …
If you think this article is detailed, you should see my tutorial about muscle pain and myofascial pain syndrome! This kind of exhaustively researched writing about Epsom salts is only possible because I sell some of the other articles on this website. No writer can afford to create truly good, detailed content and then just give it all away: we have to make a living somehow. Please reward my efforts by taking a look at my tutorials. Although Epsom salts seem unlikely to be a significant source of relief, there are plenty of other options for self-treatment of muscle pain. PainScience.com publishes an extremely thorough tutorial about myofascial trigger points (muscle knots):
Related Reading
- The Complete Guide to Muscle Strains — Muscle strain (pulled muscle) and muscle pain explained and discussed in great detail, plus reviews of every imaginable treatment option, with lots of referencing
- A Deep Dive into Delayed-Onset Muscle Soreness — The biology & treatment of “muscle fever,” the deep muscle soreness that surges 24-48 hours after an unfamiliar workout intensity
- Hot Baths for Injury & Pain — Tips for getting the most benefit from a hot soak, the oldest form of therapy
- For fun, see this short, excellent example of a typically terrible popular article about Epsom salt: its title asks, “Quick Cures/Quack Cures: Is Epsom Worth Its Salt?” but there is not a critical thought anywhere to be found. The writer assumes that Epsom salts are “effective, affordable therapy,” and then proceeds to try to “explain” it with a not-actually-a-quote from Dr. Waring. If Dr. Waring actually said that, she was speculating beyond the reach of science, but it’s more likely the journalist simply paraphrased to make her speculation sound much more definite than it was. And of course the article parrots the osmosis error: “draws foreign bodies.” No no no! That’s not osmosis! Grade school chemistry fail!
- PainSci guides to other types of pain medications:
- The Science of Pain-Killers — A user’s guide to over-the-counter analgesics like acetaminophen, ibuprofen, and more
- Voltaren Gel: Does It Work? — The science of the topical pain-killers, which can be effective without dosing your entire system
- Vitamins, Minerals & Supplements for Pain & Healing — Critical analysis of most popular “nutraceuticals” — food-like pseudo-medicines taken for medicinal purposes, especially glucosamine and creatine, mostly as they relate to pain, arthritis, and recovery from exercise and injury
- Marijuana for Pain — The hype versus the science! What does the evidence actually show about cannabis and chronic pain?
- Vitamin D for Pain — Is it safe and reasonable for chronic pain patients to take higher doses of Vitamin D? And just how high is safe?
- Does Arnica Gel Work for Pain? — A detailed review of popular homeopathic (diluted) herbal creams and gels like Traumeel, used for muscle pain, joint pain, sports injuries, bruising, and post-surgical inflammation
- Muscle relaxants — This topic is covered in several of my books in detail — low back pain, neck pain, trigger points, frozen shoulder, headaches. There is also condensed (but free) information about them in Cramps, Spasms, Tremors & Twitches.
Other interesting reading:
- Magnesium sulfate on Wikipedia.com.
What’s new in this article?
Twenty-six updates have been logged for this article since publication (2006). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
This is one of the very oldest and most thoroughly updated articles on PainScience.com, still changing and improving over a decade after the original version was first written in late 2006. It has always been popular, and has always attracted lots of feedback, including some great questions that have inspired many corrections, improvements, and entertaining tangents. However, after the 2018 reboot, it will probably now yield to many other writing priorities and remain relatively stable for a long time.
2024 — Added sidebar: Added a sidebar for colour and whimsy: “Weird health claims about magnesium.” [Updated section: Magnesium deficiency and supplementation.]
2021 — Upgrade: Much more and clearer information about hypomagnesemia and it’s possible role in pain. [Updated section: Magnesium deficiency and supplementation.]
2021 — Science update: Added citations and extra information about cramping and magnesium. [Updated section: Does magnesium therapy for pain work?]
2021 — Major upgrade: Added much more detail (and science) about the efficacy of treating chronic pain with magnesium supplementation. Merged with previous information on managing post-surgical pain. [Updated section: Does magnesium therapy for pain work?]
2020 — Medical update: More and better information about the causes, symptoms, and treatments for magnesium deficiency. [Updated section: Magnesium deficiency and supplementation.]
2020 — Audio version reboot: The audio version of this article has been re-recorded from scratch, including dozens of updates over the last couple years. I’ve also changed the way I produce audio versions so that I can easily updated individual chapters in the future. The audio is available on request to visually impaired readers, and as a perk for all eboxed set customers.
2019 — Science update: Cited a more recent review of the science on this topic, Peng. Still negative. Did some related editing. [Updated section: Does magnesium therapy for pain work?]
2019 — Upgraded: Just more and clearer information. [Updated section: No matter what magnesium can do, it can’t do everything.]
2019 — More detail: Added more information about magnesium supplementation as it relates to muscle cramping. [Updated section: Magnesium deficiency and supplementation.]
Archived updates — All updates, including 18 older updates, are listed on another page. ❐
Notes
- “Relieves pain” and “speeds healing” are as different from each other as a flying dream is from actual flying. Actually speeding up healing is kind of a big deal.
- Of course! Can’t very well debunk it without trying it, can I? I’ve had many Epsom salts baths!
- I still can’t remember it reliably, because chemical names stick in my head about as well as my cousins’ birthdays. Ambush me with the question sometime: “What’s the chemical name for Epsom salts? Schnell, schnell!” I’ll be stumped as likely as not.
The idea of “toxins” is usually used as a tactic to scare people into buying some kind of de-toxifying snake oil. Obviously there are dangerous substances; the problem is with the kind of people who toss the idea around, the reasons they do it (fear, profit, ignorance), and because toxin claims are usually so vague that they are literally meaningless, except as a marketing message. Indeed, “detoxification” may be the single most common marketing buzzword in alternative health care.
The body deals with undesirable molecules in many ways. It eliminates some and recycles others; some are trapped in a safe place; and quite a few can’t be safely handled at all (metals). Most alleged “detox” treatments are focused on stimulating an excretion pathway, like sweating in a sauna. But it’s not like sweating is broken and the sauna is fixing it! The only truly “detoxifying” treatments help the body eliminate or disarm molecules the body cannot process on its own. A stomach pump for someone with alcohol poisoning is literally “detoxifying.” So are chelation for heavy metals, and antivenoms.
I cover the specific idea of “flushing” toxins in Why Drink Water After Massage? (Massage is wonderful for all kinds of reasons — it doesn’t need the support of the idea that it detoxifies.) For more general consumer advocacy and education about toxins, see “Detoxification” Schemes and Scams (from QuackWatch.org).
For more detail, see another article on PainScience.com, A Deep Dive into Delayed-Onset Muscle Soreness: The biology & treatment of “muscle fever,” the deep muscle soreness that surges 24-48 hours after an unfamiliar workout intensity. Basically what it boils down to is that the top 5 effective treatments for muscle pain after exercise are:
- diddly
- zilch
- zip
- zero
- maaaaybe massage, but probably not
- Swain R, Kaplan-Machlis B. Magnesium for the next millennium. South Med J. 1999 Nov;92(11):1040–1047. PubMed 10586828 ❐ See also the Wikipedia article Magnesium sulfate (Wikipedia).
- Izzo AA, Gaginella TS, Capasso F. The osmotic and intrinsic mechanisms of the pharmacological laxative action of oral high doses of magnesium sulphate. Importance of the release of digestive polypeptides and nitric oxide. Magnes Res. 1996 Jun;9(2):133–138. PubMed 8878010 ❐
“A common use for high doses of oral magnesium salts is to produce a laxative effect to treat constipation,” explain the authors of this scientific paper. “In the intestinal lumen the poorly absorbable magnesium ions (and other ions such as sulphate) exert an osmotic effect and cause water to be retained in the intestinal lumen.”
- James LP, Nichols MH, King WD. A comparison of cathartics in pediatric ingestions. Pediatrics. 1995 Aug;96(2 Pt 1):235–238. PubMed 7630676 ❐
This paper compared the effectiveness of different laxatives, showing that Epsom salts do indeed move the bowels along … but not as quickly as sorbitol.
The FDA only requires evidence of efficacy for drugs (not proof). For everything else they regulate, they are focused on safety. For instance, FDA approval of food additives and medical devices mainly just means “probably safe.” For medical devices, which includes everything from lasers to acupuncture needles, they officially require “valid scientific evidence that there is a reasonable assurance that the devices are safe and effective for their intended uses” (FD&C Act Chapter V: Drugs and Devices, section §360d, “Performance standards”). What they mean by “effective” is not medically beneficial (“efficacious”), but just that it does what it says on the tin. For example, FDA approval of a laser therapy device means that it does in fact emit lasers •pew pew!• and it won’t hurt people when used appropriately… not that doing so is known to solve any medical problem.
And the FDA screws up, and their approval is hardly a guarantee of anything in any case. Just because they have certified something as safe and effective doesn’t mean it actually is. There’s a long history of embarrassing examples of things the FDA should never have approved!
- As occurs with chronic diarrhea, magnesium malabsorption, alcoholism, diuretic use, proton pump inhibitor drugs (for acid reflux), and a few other disorders.
- A dangerous and fairly common complication of pregnancy, which can cause seizures resulting from low magnesium in the central nervous system.
- Bacterial infection with Clostridium tetani, which produces the neurotoxin tetanospasmin, causes severe muscle spasms.
Lactic acid (lactate) is the poster boy for the “waste” metabolites, but it’s not a dead-end waste product at all: it’s actually a useful molecule with a productive metabolic fate, even re-use as a fuel, and it’s not the cause of muscle pain at any time. Research has shown that acute muscle fatigue — the “burn” — is probably caused by calcium physiology (see Bellinger, Fredsted, Wiltshire).
Many massage therapists still think lactate can be “flushed” by massage (which may actually backfire, see Wiltshire) If people needed massage to help them “clear” lactic acid, sprinters would drop like flies without emergency massage after every race.
Lactate as a “bad” molecule is one of the most persistent silly myths in all of exercise science. See Lactic Acid Is Not Muscles' Foe, It's Fuel
- I’m deliberately over-simplifying the definition of osmosis there, just for readability. Osmosis actually involves the movement of any solvent across a membrane. And water is a solvent, of course. I referred only to water in this context because, unless you bathe in turpentine, the only solvent in your bathing-osmosis equation is going to be good ol’ H2O.
- Full, formal definition of osmosis: “Osmosis is the spontaneous net movement of solvent molecules through a selectively permeable membrane into a region of higher solute concentration, in the direction that tends to equalize the solute concentrations on the two sides. It may also be used to describe a physical process in which any solvent moves across a selectively permeable membrane (permeable to the solvent, but not the solute) separating two solutions of different concentrations”
- A reader asked: “Isn’t that cat diffusion?” Good question, because that would be the easier visual metaphor, and you could easily caption it that way. But this caption makes it clear that the cats here are representing solvent molecules (e.g. water molecules) and not solute (which isn’t represented by anything). So the cat is a water molecule “flowing” across the “membrane.”
- Imbeault P, Ravanelli N, Chevrier J. Can POPs be substantially popped out through sweat? Environ Int. 2018 Feb;111:131–132. PubMed 29197670 ❐ Good quality reporting on this study from National Geographic: “Fact or Fiction: Can You Really Sweat Out Toxins?”
- Early claims about the benefits of bathing in salty water significantly predate hot baths: they were about salty bodies of water like the Dead Sea, where sweating is not a factor. If heat/sweating was actually required for the mechanism of action in an Epsom salts bath, that would leave its antecedents in need of some other mechanism. And that would definitely be at odds with the principle of Occam’s razor.
- Sweat is already very salty. Adding salty bathwater to salt sweat is not biologically interesting.
- Nothing moves through a sweat gland freely: it’s not an open tunnel, but more like a jet engine, full of moving parts doing extremely specific things. The gland is doing metabolically expensive active transport, working hard to pump specific molecules out of body (mostly water). A bit of salt in solution on the outside of the gland is not going to have much impact on that. Sweat glands are gonna do what they do, regardless of what’s in solution on their doorstep.
- If you weigh yourself before and after a bath or sauna, you may find a surprising 1-5 pound weight reduction. This fairly obvious effect is presumably due to fluid loss from sweating. The amount is impressive, considering that you may well have consumed fluid at the same time that you were getting rid of it through your sweat glands. However, it’s certainly consistent with the well-known hazard of fainting in that context, which every public hot tub has very clear warnings about. So I think it’s a reasonably safe assumption that we really do sweat a lot in a hot bath!
- Iwai I, Han H, den Hollander L, et al. The human skin barrier is organized as stacked bilayers of fully extended ceramides with cholesterol molecules associated with the ceramide sphingoid moiety. J Invest Dermatol. 2012 Sep;132(9):2215–25. PubMed 22534876 ❐ This is a really cool paper; NewScientist.com has a nice plain English translation: “Strange fat explains skin’s waterproof properties.”
- Potts RO, Francoeur ML. The influence of stratum corneum morphology on water permeability. J Invest Dermatol. 1991 Apr;96(4):495-9. PubMed #2007788. “The stratum corneum (SC) provides the barrier to water loss for the skin of mammals. A significant body of evidence now exists suggesting that extracellular SC lipids are primarily responsible for this barrier. … These results are interpreted in terms of the unique morphology of the SC, where lipids form an extracellular continuum that is highly tortuous. Thus, the exceedingly low permeability of the SC may be due, in large part, to its unique morphology.”
- The stratum corneum swells, but only a little, and we know it’s not the cause of pruning because it doesn’t happen when the nerve supply to the fingers is damaged, which means it’s a neurologically regulated phenomenon. We’ve known this for a long time, but we didn’t have any good idea why until quite recently. This video and this article in Nature explain in detail. Basically, “wrinkly fingers improve our grip on wet or submerged objects, working to channel away the water like the rain treads in car tyres.” The mechanism is constriction of the blood vessels under the skin: as they constrict, they pull the skin with them. And testing has confirmed that this actually improves grip on wet surfaces, which “could have helped our ancestors to gather food from wet vegetation or streams.” I’ll be darned!
- Bos JD, Meinardi MM. The 500 Dalton rule for the skin penetration of chemical compounds and drugs. Exp Dermatol. 2000 Jun;9(3):165–9. PubMed 10839713 ❐
- Hansen CS, Færch LH, Kristensen PL. Testing the validity of the Danish urban myth that alcohol can be absorbed through feet: open labelled self experimental study. BMJ. 2010;341:c6812. PubMed 21156749 ❐ PainSci Bibliography 54850 ❐
Can you get drunk through your skin? In this whimsical MythBusters-style experiment, three adults were “tested” in the office of a Danish hospital: specifically, their feet were submerged in a bowl filled with vodka — three 700 mL bottles of vodka, to be precise.
The main outcome measure was the concentration of plasma ethanol: “blood alcohol level.” It was measured every half hour for three hours of foot submersion, so there was some real dedication here!
They also asked the subjects how drunk they felt, got them to rate their self-confidence, urge to speak, and — I am not making this up — counted the “number of spontaneous hugs.” Danes get huggy when drunk, I guess.
Alas, the hug rate did not increase! The subjects did not become intoxicated, and their blood alcohol levels did not change, although “the urge to speak increased slightly at the start of the study, probably due to the setup.” The authors concluded:
Our results suggest that feet are impenetrable to the alcohol component of vodka. We therefore conclude that the Danish urban myth of being able to get drunk by submerging feet in alcoholic beverages is just that; a myth. The implications of the study are many though.
Indeed. It’s hard to tell if the researchers were actually serious about any of this, but they obviously had fun doing it.
- Simon LS, Grierson LM, Naseer Z, Bookman AAM, Shainhouse ZJ. Efficacy and safety of topical diclofenac containing dimethyl sulfoxide (DMSO) compared with those of topical placebo, DMSO vehicle and oral diclofenac for knee osteoarthritis. Pain. 2009 Jun;143(3):238–245. PubMed 19380203 ❐ This trial tested to see if DMSO has delivered a drug, diclofenac, through the skin better than not using it … and it failed. Diclofenac is absorbed just fine all by itself — which is how the mainstream arthritis product Voltaren works.
- Bos 2000, op. cit.
They argued it in three ways:
- Virtually all common contact allergens are under 500 Daltons, larger molecules are not known as contact sensitizers. They cannot penetrate and thus cannot act as allergens in man.
- The most commonly used pharmacological agents applied in topical dermatotherapy are all under 500 Daltons.
- All known topical drugs used in transdermal drug-delivery systems are under 500 Daltons.
- Roberts DW, Mekenyan OG, Dimitrov SD, Dimitrova GD. What determines skin sensitization potency-myths, maybes and realities. Part 1. The 500 molecular weight cut-off. Contact Dermatitis. 2013 Jan;68(1):32–41. PubMed 22924443 ❐
- Roberts DW, Aptula AO. Determinants of skin sensitisation potential. J Appl Toxicol. 2008 Apr;28(3):377–87. PubMed 17703504 ❐
Dr. Roberts was kind enough to explain this point for me by email:
For skin sensitization, of course the chemical has to get to the site of action. The way we now see it, this can be taken for granted. Although most of the chemical applied to the skin may remain on the outer surface, a small proportion always gets through via "shunt pathways" such as hair follicles and sweat glands (from the perspective of a single molecule, even with a molecular weight >500, these are cavernous). "Classical" penetration through the lipid "mortar" of the stratum corneum plays little if any role in skin sensitization.
Dr. Roberts again:
Of course skin sensitization is not the only reason for interest in ability of chemicals to get past the stratum corneum. For topical drug delivery, one wants a substantial proportion of the drug to get though, and “classical” penetration is much more important, so high MW is not good. Even here though, I’m not convinced about the 500 Dalton “rule.”
- Jahnen-Dechent W, Ketteler M. Magnesium basics. Clin Kidney J. 2012 Feb;5(Suppl 1):i3–i14. PubMed 26069819 ❐ PainSci Bibliography 52761 ❐ Chandrasekaran et al. regarding this paper: “The radius of the hydrated magnesium ion has been reported to be 400 times higher than its dehydrated form, leading to the assertion that it is almost impossible for magnesium ions to pass through biological membranes.”
- Chandrasekaran NC, Sanchez WY, Mohammed YH, et al. Permeation of topically applied magnesium ions through human skin is facilitated by hair follicles. Magnes Res. 2016 Jun;29(2):35–42. PubMed 27624531 ❐
For context, I’ll repeat this quote from Chandrasekaran et al.: “The radius of the hydrated magnesium ion has been reported to be 400 times higher than its dehydrated form [Jahnen-Dechent et al.], leading to the assertion that it is almost impossible for magnesium ions to pass through biological membranes.”
However!
“When we re-examined this calculation, it was found that the volume of the magnesium ion is 451.76 Å3 [4 (4.76)3] in the hydrated state, but based on the ionic radii of dehydrated and hydrated magnesium ions, i.e., 0.87 Å and 4.76 Å respectively [10-13], we calculated that the hydrated radius of the ion is only 5.47 fold (4.76Å) greater than its dehydrated radius. Based on our recalculation … we postulated that the hydrated magnesium ion could potentially penetrate by bulk diffusion through the 10 Å pores formed by protein subunits in the lipid membrane [5, 14], or by other means, such as hair follicles.
- Singleton, Kenneth B. The Lyme Disease Solution. 2008. p396.
- Medical training credentials are not remotely a guarantee of an intelligent opinion, and this demonstrates it beautifully. All it does is show the kinds of ridiculous things that get said about Epsom salts without a shred of evidence or even an intelligible biological rationale.
- Eisenkraft A, Krivoy A, Vidan A, et al. Phase I study of a topical skin protectant against chemical warfare agents. Mil Med. 2009 Jan;174(1):47–52. PubMed 19216298 ❐
- Waring RH. Report on Absorption of magnesium sulfate (Epsom salts) across the skin. Unpublished. 2006. PainSci Bibliography 56301 ❐
- The others had increased urine levels of magnesium, implying that “the magnesium ions had crossed the skin barrier and had been excreted via the kidney, presumably because the blood levels were already optimal.” In other words, whatever magnesium was absorbed into the bloodstream was promptly removed by the body.
- When I asked Dr. Waring about publication, she explained “we just haven’t got around to it yet. I hope to do a bit more and then publish with my London colleague.”
There are any number of flaws in the experiment that we can’t know about. For example, one reader sent me this interesting point by e-mail:
Dr. Waring could not possibly have measured absolute MgSO4 blood content: the only way to do that would be through dialysis or post-mortem, only relative concentration. Any degree of dehydration would have an absolute effect on relative concentration; i.e., all solutes would show increased concentration due to dehydration, including any magnesium already present in the bloodstream. Since the study is unpublished, it’s not possible to know whether the Dr controlled for this.
- Dr. Waring has done other research claiming to show that autism is correlated with magnesium deficiency, and her primary reason for studying Epsom salt absorption through the skin was to investigate it as a possible autism treatment. This is not a serious bias, but it’s worth noting, because it could certainly mean that she was hopeful when she did the experiment that Epsom salts bathing would constitute a meaningful method of supplementation … and data and its interpretation tends to get warped by wishful thinking, which is exactly why studies need to be replicated, and why it’s more of a shame that this one hasn’t even been published, let alone replicated.
- Park JH, Lee JW, Kim YC, Prausnitz MR. The effect of heat on skin permeability. Int J Pharm. 2008 Jul;359(1-2):94–103. PubMed 18455889 ❐ PainSci Bibliography 52769 ❐
See 2007 Darwin Awards: The Enema Within, in which a man died from an alcohol enema. “In order to qualify for a Darwin Award, a person must remove himself from the gene pool via an ‘astounding misapplication of judgment.’ Three litres of sherry up the butt can only be described as astounding.”
See also, if you dare, this real news item about a frat boy who almost killed himself “butt chugging” — getting drunk from alcohol injected into the butt. Seriously. “The only thing more embarrassing than almost dying from allegedly butt-chugging is hiring a lawyer to deny it.” No doubt.
- Water vapour is mostly pure H2O by definition. There is such a thing as solutes that get “dissolved in steam” and carried along with it without technically “evaporating,” but that’s a fairly exotic phenomenon. Your standard salts neither evaporate nor get carried away with evaporated water.
- Gröber U, Werner T, Vormann J, Kisters K. Myth or reality-transdermal magnesium? Nutrients. 2017 Jul;9(8). PubMed 28788060 ❐ PainSci Bibliography 52771 ❐
- Chestnutt WN, Dundee JW. Failure of magnesium sulphate to prevent suxamethonium induced muscle pains. Anaesthesia. 1985 May;40(5):488–490. PubMed 4014628 ❐
Muscle pain is one of the side effects of suxamethonium chloride, an anaesthetic drug used to cause short-term paralysis. In this study, injecting magnesium sulphate had no benefit compared to doing nothing, and was “followed by unpleasant side effects.“
Granted, the relevance of this kind of muscle pain to the more common kinds is unknown. But it is suggestive. Molecules produced by the inflamed tissues in these patients may interfere with the production of a protein that is used to produce sulfate from another molecule (cysteine), thus lowering sulfate levels. In Dr. Waring’s words:
“The cytokines released in the inflammatory state actually depress the expression of cysteine dioxygenase, the rate-determining step in the conversion of cysteine to inorganic sulfate. About 80% of the in vivo requirement of sulfate goes through this pathway as sulfate is not well-absorbed from the gut.”
However, low sulfate levels are a possible result of having rheumatoid arthritis, not a cause — and thus boosting them back up again will not necessarily solve anything. And even if it did, that’s a therapeutic effect that is very particular to rheumatoid arthritis — a serious, agonizing joint disease — which probably has little or nothing to do with the kinds of pain that most people put Epsom salt in their baths for.
It would be great if Epsom salt baths helped people with rheumatoid arthritis, but good evidence of that would, in a way, pretty much shoot down the other claims of therapeutic effect, which rely on completely different ideas about how and why Epsom salt might work. But, of course, there is as yet no evidence one way or the other.
This idea is frequently repeated, but I have been unable to find a citation that directly supports it. A 2012 paper (Mauskop et al.) argues for giving all migraine patients magnesium and repeats the claim clearly:
“Of the total body magnesium, 67% is found in the bone and 31% is located intracellularly. Only the remaining 2% is in the measurable, extracellular space, and therefore the levels found on routine blood tests do not reflect true body stores.”
However, despite a long reference list, no citation is provided! I don’t really doubt that “only 2%” is in the blood; that premise is probably true. But does it follow that “true body stores” are what actually matters? There are many biological complexities that could foul up that inference. My impression is that this idea is useful for advocates of using magnesium therapeutically, but it doesn’t mean it’s actually true or important. It might be. It might not.
- We absorb Mg on an as-needed basis, so excesses are mostly just pooped out — maybe with a little cramping and diarrhea.
- Schwellnus MP, Drew N, Collins M. Increased running speed and previous cramps rather than dehydration or serum sodium changes predict exercise-associated muscle cramping: a prospective cohort study in 210 Ironman triathletes. Br J Sports Med. 2011 Jun;45(8):650–6. PubMed 21148567 ❐
Blood samples from 210 Ironman triathletes were checked for electrolytes and other signs of hydration status. 43 had suffered cramps. There were no significant differences between the crampers and the non-crampers in any of the pre-testing or post-testing. Dehydration and electrolyte shortage don’t cause cramps — intense effort does. “The results from this study add to the evidence that dehydration and altered serum electrolyte balance are not causes for exercise-associated muscle cramps.” This is a nice myth-mangler of a paper.
- Garrison SR, Korownyk CS, Kolber MR, et al. Magnesium for skeletal muscle cramps. Cochrane Database Syst Rev. 2020 09;9:CD009402. PubMed 32956536 ❐ PainSci Bibliography 52162 ❐
This review of only a handful of existing studies concluded that “it is unlikely that magnesium supplementation provides clinically meaningful cramp prophylaxis to older adults experiencing skeletal muscle cramps.” Amazingly, the evidence for the effect of Mg on cramps caused by exertion, disease, and pregnancy is just hopelessly inadequate. You’d think someone would at least have studied exercise-induced cramping, given its importance in elite athletics. The last version of this review was in 2012, and almost nothing changed.
- Tai YT, Tong CV. The Perilous PPI: Proton Pump Inhibitor as a Cause of Clinically Significant Hypomagnesaemia. J ASEAN Fed Endocr Soc. 2020;35(1):109–113. PubMed 33442177 ❐ PainSci Bibliography 52188 ❐ There have been more than a couple dozen case reports of serious hypomagnesaemia over the last twenty years, and those are generally the tip of an iceberg.
- Swaminathan R. Magnesium metabolism and its disorders. Clin Biochem Rev. 2003 May;24(2):47–66. PubMed 18568054 ❐ PainSci Bibliography 52191 ❐
- McGill.ca [Internet]. Labos C. Magnesium: The Often Forgotten Mineral; 2019 August 22 [cited 19 Oct 17]. PainSci Bibliography 52610 ❐
- Rodríguez-Morán M, Guerrero-Romero F. Serum magnesium and C-reactive protein levels. Arch Dis Child. 2008 Aug;93(8):676–80. PubMed 17641003 ❐
- Chronic pain often involves a phenomenon known as sensitization: more pain with less provocation. It is broadly plausible that any sedative effect could blunt sensitization. Potent sedative drugs (like benzodiazepines) have limited efficacy and often backfire and actually cause more pain. Addressing a magnesium deficiency might be a much safer, healthier method of “sedation.” And that’s pure speculation.
- Tarleton EK, Kennedy AG, Rose GL, Littenberg B. Relationship between Magnesium Intake and Chronic Pain in U.S. Adults. Nutrients. 2020 Jul;12(7). PubMed 32708577 ❐ PainSci Bibliography 52160 ❐
- Bonus eye roll: Amusingly, when Tarleton et al. explained why they did this research — that “there is some evidence that magnesium supplementation results in improved pain management” — they cite only a single supporting paper. And what is that single paper? A twenty-year-old study showing an inflammatory response to severe deficiency… in rats. 🙄
- Banerjee S, Jones S. Magnesium as an Alternative or Adjunct to Opioids for Migraine and Chronic Pain: A Review of the Clinical Effectiveness and Guidelines. CADTH Rapid Response Reports. 2017 Apr. PubMed 29334449 ❐
- They clearly state that conclusions were “not possible” for migraine … that the evidence is conflicting for a rather exotic kind of chronic pain (complex regional pain syndrome) … and they mention only a single trial showing a benefit for back pain (with intravenous supplementation, no less). More on that one below.
- Yousef AA, Al-deeb AE. A double-blinded randomised controlled study of the value of sequential intravenous and oral magnesium therapy in patients with chronic low back pain with a neuropathic component. Anaesthesia. 2013 Mar;68(3):260–6. PubMed 23384256 ❐ PainSci Bibliography 52166 ❐
- Back pain without neuropathy is a good proxy for many other kinds of ordinary body pain… but back pain with neuropathy is more about neuropathy than “back pain.”
- Both groups did great at first, more than halving their pain. If stopped there, the study would have shown that magnesium was no better than a placebo. But then the placebo group’s numbers rebounded, while the magnesium folks stayed low… for six months.
- Kogler J. The analgesic effect of magnesium sulfate in patients undergoing thoracotomy. Acta Clin Croat. 2009 Mar;48(1):19–26. PubMed 19623867 ❐
- Lysakowski C, Dumont L, Czarnetzki C, Tramèr MR. Magnesium as an adjuvant to postoperative analgesia: a systematic review of randomized trials. Anesth Analg. 2007 Jun;104(6):1532–9, table of contents. PubMed 17513654 ❐ The authors of the review concluded: “These trials do not provide convincing evidence that perioperative magnesium may have favorable effects on postoperative pain intensity and analgesic requirements.”
- Peng YN, Sung FC, Huang ML, Lin CL, Kao CH. The use of intravenous magnesium sulfate on postoperative analgesia in orthopedic surgery: A systematic review of randomized controlled trials. Medicine (Baltimore). 2018 Dec;97(50):e13583. PubMed 30558026 ❐ PainSci Bibliography 52717 ❐
Echoing the conclusions of Lysakowski et al. in 2007, magnesium sulfate does not seem to be an effective pain medication for patients after orthopaedic surgeries. Although the authors think it has potential, the data disagrees, and they are forced to concede that “these trials do not provide convincing evidence of beneficial effects.”
- Consider the seminal text, Muscle Pain: Understanding its nature, diagnosis and treatment. It has nine chapters devoted to nine different kinds of muscle pain. It also doesn’t mention Epsom salts. Not once.
- Learn.genetics.utah.edu [Internet]. Cell Size and Scale; 2010 [cited 17 Jan 21]. PainSci Bibliography 55677 ❐
A beautiful animated tool for visualizing the scale of cells.
- There are a lot of microorganisms that might be on a rusty nail, but CT is the scary common one that can kill you very unpleasantly (a chance of death by muscle spasm, arg). The reason you get a tetanus shot in that situation is that it is a very effective just-in-case prevention, good bang for buck. The idea that anyone would recommend an Epsom salt bath as a replacement for that is quite terrifying, a fine example of dangerous ignorance. While a very strong Epsom salt solution might kill every bacteria in a shallow wound, a deep wound can put bacteria into the bloodstream that leaves the site in seconds — completely inaccessible to any topical antibacterial solution. Ironically, as mentioned above, magnesium heptahydrate is actually a treatment for the muscle spasms caused by CT — but it can’t prevent the infection via a puncture wound in the first place.
- It is now well understood that every microscopic nook and cranny of our skin — indeed, our entire body, inside and out — is thickly populated with an ecosystem of microorganisms, more diverse than any jungle (see We Are Full of Critters). It is also likely that one of the primary functions of these teensy jungles is to maintain a balance of power, where it’s difficult for any organism to dominate. If soaking in salt water kills bacteria, it might kill off the bacteria that normally live on the skin as well.
- “Because reasons” is a bit of cute slang.
- Which actually suggests an interesting point: if modest amounts of Epsom salts in your bath allegedly has therapeutic effects, then it is reasonable to guess that the much higher concentrations of salt used in flotation therapy or found in the famous salt lakes would have a really dramatic effect — perhaps even a toxic effect. But bathing in much higher concentrations of salt has no significant effect at all … other than making people float.
- A UK flotation tank manufacturer’s website, floataway.com, admirably restrains itself from extravagant claims of medical benefits, discussing only the benefits of relaxation. As for Epsom salt, the website says it is used “because it raises the density of the water, making it easy to float, and because it has a silky feel which is very good for the skin.” I’m not sure what they mean by “good for,” but I’m guessing it just feels pleasant.
- RacingSmarter.com [Internet]. Epsom Salt & Apple Cider Vinegar Treatments Nature’s Healing & High Energy Bath; 2006 [cited 10 Nov 2, page defunct].