Chronic, Subtle, Systemic Inflammation
One possible sneaky cause of puzzling chronic pain

Do you seem to have more than your fair share of aches and pains? It’s probably not your imagination. There are many possible explanations for chronic pain and fragility, but this article is about one of the most insidious and interesting. It’s most relevant to you if you’re struggling with your weight and/or severe chronic stress, or if you feeling like you’re not just aging but maybe prematurely. So really quite a lot of people.
Everyone over 40 knows that it gets more uncomfortable to get out of beds and chairs as we age, and we’re plagued by ever more pains that come and go without much rhyme or reason. Most people chalk this all up to “arthritis,” but that’s rarely a significant factor until much later in life.1 Conditions like fibromyalgia and myofascial pain syndrome, as common as they are, certainly can’t account for all of it. Some medications cause general sensitivity as a side effect,2 but that still doesn’t explain a widespread problem either. So what could be going on?
A little bit of inflammation spread all over the place is one possible culprit. And I have to strongly emphasize that this is an unproven idea, and there is plenty of guessing in this article: well-informed and evidence-based guessing, but definitely speculation. Nevertheless, this may be one of the major fundamental mechanisms of vulnerability to chronic pain and injury over time.
Chronic low grade inflammation is increasingly seen as a part of other orthopaedic conditions such as osteoarthritis — once considered a ‘cold’ wear and tear problem (as opposed to the far more overt and ‘hot’ inflammation of rheumatoid arthritis).
Summer is coming — Frozen Shoulder, Cocks (Noijam.com)
Why would anyone be a little bit inflamed all over? Causes of inflammation
Inflammation is a part of life, the inevitable cost of having an immune system. Just like a society must balance police and military powers against civil liberties, evolution has had to juggle the pros and cons of a potent defense system. It has to be strong enough to get the job done, but not so strong that you become collateral damage. It is obviously not all bad, and it may have been excessively demonized in recent decades.3 There’s almost always some inflammation going on somewhere in the body, and it even fluctuates in natural daily rhythms.
For instance, inflammation is suppressed at night, which has many clinical implications, such as why morning pain may be such a familiar annoyance for humans.4
For all kinds of reasons, from the boring to the sinister, it can get a bit out of hand. Especially as we age.
Most chronic low-grade inflammation is probably just an aging thing. This has a name: it is quaintly known as “inflammaging.”5 To be old is to be more inflamed! And to be inflamed excessively may be synomous with premature aging … which is probably affected by both your genes and lifestyle. Things that are unhealthy — smoking, sedentariness, stress, sleep deprivation — don’t so much make you feel old as literally age you.
Do some of us get too inflamed, too soon, too chronically? Almost certainly. Exactly how it happens — and how to reverse it, or at least slow it down — is where the mystery lives. But it’s not all a mystery. Most of the solution, for most people, is just fitness.
It’s not the years, honey. It’s the mileage.
Indiana Jones
Metabolic syndrome
A lot of inflammaging — probably most — is the cost of “metabolic syndrome,” a set of biological dysfunctions that is more or less synonymous with being “out of shape.” It’s the collective consequence of poor fitness, obesity, aging, genetics, and hard living. It is the roots of heart disease and diabetes. Metabolic syndrome, systemic inflammation, and aging are all so strongly associated that they are almost synonymous.
We know that metabolic syndrome is clearly linked to common body pain problems like neck pain6 and back pain.7 We also know that obesity is linked to tendinopathy specifically, even in joints that aren't weight-bearing.8 We know that even relatively healthy people with back pain have junkier diets and high cholesterol:9 clear signs that they are headed for metabolic syndrome, but — and this is interesting! — already in pain years before they get there. Maybe being unfit actually drives pain in the relatively short term?
On the other hand, how easy do you think you’d find it to stay in shape if you were already inflamed for other reasons? We still don’t yet know that metabolic syndrome — early or late in the process — actually causes pain, or if it just tends to be found in the same kinds of people who get chronic pain for other reasons. It could even be the reverse: chronic inflammation could drive metabolic syndrome! Definitely maybe!10
Metabolic syndrome is also linked to severe chronic psychological stress … or even stress that happened long ago, during childhood.11 It’s also quite possible that stress is inflammatory independently of metabolic syndrome (if they can be separated). The role of stress and trauma is too complex, indirect, and long-term for clarity, but it’s a near certainty that it does play a role. Chronic low-grade inflammation is probably not just about the metabolic syndrome stereotype of “old, fat, unfit.”
From here, the waters only get muddier, the speculation thicker. But there are definitely quite a few other possible drivers of inflammaging.
The role of weight and fat, especially belly fat
Obesity is the most visible outward metabolic syndrome, and it is definitely strongly linked to a wide range of health problems, including roughly double the risk of chronic pain. But fat is not inherently unhealthy. It can be fine, or it can be a problem: the “obesity paradox.”
- Not all obviously overweight people are unhealthy.
- Not all skinnier people are safe from the health risks of obesity.
The explanation for that contradiction is that the real culprit is excess visceral fat — which is more likely in people who are heavier overall, but can still occur without a high body fat percentage. You can have a minor middle-aged bulge and still be at risk. In fact, it’s the “tight”, non-flabby middle age bulge that is most likely to be a problem!12
Like any other tissue, fat is lively and complex, and it can be healthy or unhealthy depending on genes, life, and midnight snacks. Extra belly fat — visceral fat — is more likely to be stressed and oozing inflammatory signals … which drags the liver into the equation (it’s right there) …which in turn throws the whole system off kilter.13
More specifically still — and now obviously more relevant other “structural” tissue failures — visceral fat secretes signals that contribute to epigenetic changes that accelerate tissue degeneration, in addition to other mechanisms for chronic pain, like sensitization.14 This is probably why there's also strong link between diabetes, dyslipidemia, and obesity and tendinitis, even in joints that don’t carry our weight around — with some extremely high odds ratios, like 6× the risk of Achilles tendinitis and 10× the risk of tennis elbow.15
Excess weight probably is somewhat bad for you biomechanically, but that’s much less of a factor than people assume. The real concern is that some fat is bad for you metabolically. In addition to the obvious threat of extra loading, excess visceral fat especially — which can occur even without a high BMI — is systemically pro-inflammatory, corrosive to connective tissue, and sensitizing, affecting all tissues.
Menopause is probably inflammatory
Aging women often feel like they are on fire, and many will also tell you — if you ask nicely — that is menopause comes with a significant degradation in physical resilience, a feeling of aging more rapidly than ever before. This is an example that applies to only one phase of the lives of half the population, but I can hardly imagine a better example of what makes inflammaging work.16 McCarthy and Raval:
“Emerging evidence is showing that peri-menopause is pro-inflammatory and disrupts estrogen-regulated neurological systems. … Estrogen receptor-beta has been shown to regulate a key component of the innate immune response known as the inflammasome, and it also is involved in regulation of neuronal mitochondrial function. This review will present an overview of the menopausal transition as an inflammatory event, with associated systemic and central nervous system inflammation…”
For instance, men also go through roughly analogous hormonal changes, so-called “manopause.” Good chance that’s at least a little bit inflammatory too.
And you’re probably underestimating how many subtle pathologies are out there, or just random odd health headwinds thanks to genetics and microorganisms.
Chronic subtle infections
Inflammaging probably worsen with time as we accumulate infections and their consequences. There are many pathogens and other invaders we know about that set up shop in the human body forever — “tenants” we cannot evict. The obvious ones are famous (e.g. herpes, measles, HIV, etc). For every obvious one, there might be several subtler ones that only mildly arouse our defenses, infections that will never be diagnosed, let alone treated. As we move through life, we encounter more and more of these pathogens, some tougher than others. Accumulate enough of them, et voila, “inflammaging.”
Another scenario: there’s good evidence that a weak immune system can also allow some common minor infections to “reactivate” after lying dormant in our cells for years or even decades.17
But we may carry on suffering from infections even when we successfully fight them off. Many infections “leave a mark” — permanent damage.
Autoimmunity and collateral damage: antibodies are forever
Autoimmune disease was originally thought of as a baffling biological blooper: the body mysteriously attacking itself, the “why are you hitting yourself?” school of pathology.18 Some autoimmune disease may indeed be perverse, dysfunctional “self-abuse,” but there is a more modern perspective, a hypothesis that autoimmune disease is mostly the price of doing business: collateral damage from unavoidable, ongoing battles with pathogens. Just a cost of doing immune business.
Or, worse, it could be collateral damage from battles that ended long ago, like stepping on a land mine from an old war.20
We make new antibodies for every pathogen (and other antigens, like allergens). Sometimes, those antibodies are not a perfect match for their target alone: they might also be match for a few of our own proteins, causing our immune systems to spend the rest of our lives over-reacting to healthy tissues that “look” a little bit similar to that old nemesis. The more wee beasties we fight off, the more potential there is for random, on-going, low-grade inflammation here there and everywhere.
Allergies as a source of chronic inflammation
Autoimmune disease is basically an allergy to yourself, while actual allergies are an immune system reaction to a non-toxic foreign substance in the body, something harmless to most person but irritating or even deadly to a few.
The immune system can be a terrible thing when riled up.
Inflammaging may be partly attributable to an escalating number of allergies — another kind of collateral damage. As we build up our defenses against infection (antibodies), our immune system trained by all the antigens we’ve “met” (both pathogens and allergens), those defenses start reacting to a wider range of foreign substances in addition to some of our own proteins. Which is why allergies often appear in middle age: we acquire them. For example… allergies might seem a bit boring as a topic, but consider this one …
Meet mammalian meat allergy (MMA), a bonkers allergy to beef and pork that we can get after exposure to certain kinds of tick bites, and which can probably cause long-term chronic inflammation that’s nearly impossible to diagnose — a sensational example of many such possible sources. Here’s how this works…
First you get bitten by a very particular tick, like the delightfully named “paralysis” tick in Australia (predictable), plus a few others around the world.
Then you probably think you’re fine! You might not even know you got ticked. But your immune system is starting to over-react to a molecule delivered in the tick spit — one that we do normally eat, but do not get injected.
And then you carry on with your life getting sick to varying degrees 2-10 hours after eating a steak or lamb kebab. (And it can be quite nasty.)
Et voila, now you have MMA! Crazy.
And don’t underestimate the diagnostic challenge of connecting delayed symptoms to such an unsuspected trigger!
MMA is not just about meat
MMA is AKA alpha-gal syndrome (AGS). “Alpha-gal” is the pronounceable short version of galactose-alpha-1,3-galactose, the carbohydrate molecule injected by the tick. It is found mainly in mammalian meat. It is notably absent from poultry, eggs, and seafood.
But molecules are teensy and they get everywhere, like glitter. AGS can be found in small amounts in all kinds of odd places — like gelatin capsules for common| drugs — and some people may be so sensitive to alpha-gal that they are often reacting to those subtle sources.22
That’s an obscure wellspring of chronic, erratic flares of inflammation that could easily go undiagnosed, because this nonsense was only discovered in the 2000s, and today it is still “an underrated serious disease.”23
Immune over-reactions are a bewilderingly bottomless pit of pathological possibilities, and many allergies are underdiagnosed and underestimated, flying well under the medical radar. The immune system may be a terrible thing when riled up, but it’s actually the tamer cases that interest me. Because of the inflammaging. And vulnerability to pain and injury escalates in sync with inflammaging.
I am not suggesting that MMA (or any other weird allergy), is a common cause of “inflammaging” in itself — it’s too rare for that. But it is clearly a source for some people, and — this is the point — it is just one of many odd kinds of immune hijinks that are collectively common.
Inflammation is just following (neurological) orders
People don’t really think “neurology” when they see obviously inflamed tissue, but in fact inflammation is partly regulated by neurological signals, and some chronic systemic inflammation is probably could well be attributed to neurological factors. That is, it’s a “neuroimmunological” thing, a product of the complex relationship between neurology and immunology. Here’s a vivid example of neurologically-regulated superficial inflammation that demonstrates the existence of that relationship…
In this image from Azimi et al., we see how an inflammatory skin disease greatly improves where nerves aren’t working.24 No nerve supply, no inflammation! 🤯 Or a lot less, anyway. The top photo shows psoriasis in remission after the radial and median nerves were injured by a shoulder dislocation, and the bottom shows how the psoriasis is coming back as the nerves recover.

This is a great demonstration of how much inflammation can be regulated by the nervous system. This is just one of 19 cases Azimi et al. describe showing “near or complete resolution of pre‐existing skin lesions occurred in areas directly or indirectly supplied by a subsequently injured nervous system.” Another example: scleroderma backing off in the aftermath of a stroke.
The effect isn’t universal: in 4 cases, skin inflammation worsened despite the loss of nerve supply, due to unknown variables. “It’s complicated.”
Nevertheless, this is one of those phenomena that gives us a bit of a peak behind the curtain at what’s really going on with a pathology. How many other chronically inflamed tissues work like this to some degree? How much systemic inflammation is going on because the central nervous system said “make it so”? Likely a fair bit! We’ll dig into that idea in the next several sections.
The next part of the article is for PainSci subscribers only; it delves into the scientific details of the nature of the beast for about 4000 words (15 minutes of extra reading). Plenty of free reading continues below that — including practical self-help advice, ideas about what can you do about inflammation and inflammaging — for a total of about 24,000 words — this is still a large and useful article even without the members-only area.
Most PainScience.com content is free and always will be.? Membership unlocks extra content like this for USD $5/month, and includes much more:
Almost everything on PainScience.com is free, including most blog posts, hundreds of articles, and large parts of articles that have member-areas. Member areas typically contain content that is interesting but less essential — dorky digressions, and extra detail that any keen reader would enjoy, but which the average visitor can take or leave.
PainScience.com is 100% reader-supported by memberships, book sales, and donations. That’s what keep the lights on and allow me to publish everything else (without ads).
- → access to many members-only sections of articles +
And more coming. This is a new program as of late 2021. I have created twelve large members-only areas so far — about 40,000 words, a small book’s worth. Articles with large chunks of exclusive content are:
- Quite a Stretch
- Does Epsom Salt Work?
- Heat for Pain and Rehab
- Your Back Is Not Out of Alignment
- Trigger Point Doubts
- Does Fascia Matter?
- Anxiety & Chronic Pain
- Does Massage Therapy Work?
- Does Posture Matter?
- A Deep Dive into Delayed-Onset Muscle Soreness
- Does Ultrasound or Shockwave Therapy Work?
- A Painful Biological Glitch that Causes Pointless Inflammation
- Guide to Repetitive Strain Injuries
- Chronic, Subtle, Systemic Inflammation
- Vitamins, Minerals & Supplements for Pain & Healing
- Reviews of Pain Professions
- Articles with smaller members sections (more still being added):
- → audio versions of many articles +
There are audio versions of five classic, big PainSci articles, which are available to both members and e-boxed set customers, or on request for visually impaired visitors, email me. See the Audio page. ❐
I also started recording audio versions of some blog posts for members in early 2022. These are shorter, and will soon greatly outnumber the audio versions of the featured articles.
- → premium subscription to the PainSci Updates newsletter +Sign-up to get the salamander in your inbox, 0–3 posts per week, mostly short, sometimes huge. You can sign-up for free and get most of them; members get more and their own RSS feed. The blog has existed for well over a decade now, and there are over a thousand posts in the library. ❐

Change or cancel plans any time. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism. For more information, see the membership page. ❐
PREVIEW: Headings in the members-only area…
- The major environmental pollutants
- Microplastics … and nanoplastics now, too
- Surgical implants, especially the meshes
- Mould as a pollutant
- Food additives (and other things we aren’t good at digesting)
- Inflammation and fibromyalgia
- Inflammation and stress
- Neuroinflammation — A fire in the nervous system
- Neuroinflammation — Sickness behaviour
- Neuroinflammation — Subtler examples?
- Neuroinflammation — When neuroinflammation goes wrong (mostly by going long)
- Neuroinflammation — A response to perceived threats?
The major environmental pollutants
In early 2021, I shared a disturbing example of environmental pollution: otherwise safe pipes becoming toxic when heated by wildfires. “I cannot help but wonder,” I wrote, “how many of these poisons in our environment undermine our health in ways that contribute to chronic pain?”
It took me years more to try to answer the question. I am extremely wary of demonizing “toxins” or “chemicals,” because our fears about them are already so aggressively fanned by quacks selling bogus detox solutions. I’m so wary that I put this topic off for years.
But I could put it off no longer (than mid-2024). I’m more skeptical of the detox cures than the “toxins” themselves. At least some are truly dangerous (e.g. lead poisoning). The question is whether any of them matter for chronic pain patients. Wouldn’t it be nice if you could get a realistic, science-informed threat assessment? From someone who isn’t trying to sell you the cure? It’s your lucky day! I’m only selling education and (fingers crossed) reasonable, science-informed speculation …
I am painfully aware that “it’s the chemicals” is the message many readers will take from some of this content… no matter how much I protest that we really truly do not and cannot know the actual risks at this time. But we really don’t, and we really can’t.
I would be interested in detoxing … if I thought it were possible.
At least three times in the last few years I have endured several days of thick smoke in Vancouver. Days of “unhealthy” or “very unhealthy” and sometimes even “hazardous” smoke, with Air Quality Index scores from 150 to 350 that spell unavoidable physiological stress even at the low end. Some prevention is possible (air filters), but treatment? De-toxing what I’ve inhaled? If only!
Unfortunately, we mostly just cannot “detox” much of anything beyond what our organs already do for us (which is quite a bit, but humans can still easily be poisoned). There are only a handful of specific medical treatments for some kinds of poisons, such as anti-venoms or chelation therapy. The massive detox industry is almost pure bullshit, along with basically all popular beliefs about detoxing. For instance, we cannot sweat out toxins,25 or suck them out of our bodies with Epsom salts baths.26
But, like every good scam, detox quackery is based on a seed of truth, and this particular seed is unusually robust and sad: our world is badly polluted, an uncontrolled experiment on a brain-breaking scale. And our food system isn’t exactly pristine either! Trans fats alone are probably worse than several other candidates put together.
Okay, that's enough disclaimers about detox quackery. Let's get on with it…
The four main kinds of environmental toxins
Pollutants in the air, water, and food supply are probably most of what people hope to purge when they do a “detox.” People who talk about detoxing are almost never specific about what toxins, exactly, they are talking about. If they knew enough, what should they be talking about? There are four main candidates from the last few decades …
- The persistent organic pollutants (POPs): pesticides, flame retardants, and polychlorinated biphenyls (the notorious PCBs, now banned, but formerly ubiquitous in many a plastic piece of crap). They include well-known dangerous chemicals like DDT and dioxins, along with dozens of more obscure examples. There is a broad scientific consensus that these are hazardous substances, but the practical public health risk varies greatly with the details.27 But there sure are a lot of them, with collectively substantial risk.
- “Forever chemicals,” the per- and poly- fluoroalkyl substances (PFAS), all combine fluorine with carbon-hydrogen (alkyls); they started with Teflon and have since ballooned into an immense family of (I’m not joking) several million distinct chemicals. There are a lot of ways to combine fluorine with alkyls! This is a disturbing POP subcategory that is still defined by scientific uncertainty: only about 10% of PFAs have been studied for health effects as of 2024, and most of those not enough.28 In most cases we know little or nothing about the hazard, and even less about the risk. But we certainly know that they are all around us, not going anywhere, and some widespread harm is plausible.
- Heavy metals, mainly lead! Lead is a useful element that happens to absolutely mess with animal physiology, known for being harmful at literally any dose, no matter how small.29 It might seem like a quaint, old-timey thing that we don’t have to worry about much anymore, but … nope, unfortunately it is still an alarmingly common pollutant, doing plenty of harm. It accounts for (very roughly) half of the known damage from all tracked chemical hazards.30 This hazard and risk are as real and serious as a heart attack … and in fact, weirdly, heart disease is one of the main effects of lead.31 The mechanism? Basically inflammatory. Acute lead poisoning is relatively rare, but it’s fair to guess that long-term exposure to small, accumulating doses is a significant health headwind that makes a small but relentless contribution to inflammaging in a great many of us, and more in an unlucky minority.
- Traffic-related air pollution, and especially diesel exhaust with its sub 100 nanometre “ultrafine” particles, is a well-documented health hazard, that we nevertheless probably continue to underestimate. A good example from some researchers local to me: just breathing diesel exhaust immediately alters brain function! Not much, but it’s disturbing because it “shouldn’t” be possible at all.32 This challenges an old assumption that the brain is likely safe from direct pollution damage, thanks to the blood-brain barrier. The authors reckon that the ultrafine particles are either getting in “via the olfactory bulb and/or secondary transmission of inflammation,” circumventing the barrier.33

Air pollution is a well-known health hazard. But does it have anything to do with chronic pain?
This is a recent photo of a huge, dramatic fire in my own neighbourhood. That’s my wife in the foreground (barely ever seen on PainScience.com). I took the photo moments after we spotted the smoke, and right after it brought a crane down on a major street. We could easily smell it a kilometre away.
All of these well-known pollutants can definitely be found in our environment and our bodies, where they mostly get trapped in fat or otherwise sequestered — but they can also potentially be a source of physiological stress, and therefore chronic inflammation.
And there’s really not anything we can do about them. But we’re not entirely helpless…
Cleaning the air
A little ray of light on this dark topic: we can reduce the risks of air pollution significantly. We have the technology! Cleaning indoor air is one of the best bang-for-buck options we have for protecting ourselves from air pollutants.
For instance, I have lovely, smart Corsi-Rosenthal boxes powered by computer fans, a very efficient DIY air filter design which can move a lot of air surprisingly quietly. And with air quality, “clean air delivery rate is all that matters!”

This is my handmade (from a kit) Corsi-Rosenthal box, which uses PC fans for quiet-but-high-volume air movement through the filters. There’s another filter on the other side of the box.
Unfortunately, the air-cleaning industry is choked with bullshit and misleading claims, and many products are just junk (including some expensive ones). You need a trusted guide. I strongly recommend the “It’s Airborne” blog, by Joey Fox, which does a superb job of filtering out the nonsense. Start with his list of favourite air cleaners. (← Not an affiliate link! I don’t do that. And that’s partly why you pay me for this content — so that I can afford to make recommendations like this without the corruptive force of kickbacks.)
Microplastics … and nanoplastics now, too
Tiny plastic garbage has been much in the news lately: dust-sized particles, microscopic ones, and now we know that there are even nano-scale particles (like diesel's ultrafine grit). The health effects of this kind of pollution have not yet been studied well enough to know how great the danger is, but there’s plentiful plant and animal evidence so far, and plenty of cause for concern.34 But the surprisingly recent confirmation of ultrafine particles probably increases the exposure and hazard, and therefore the risk.
An important and interesting clue that microplastics might be dangerous is the extreme example of surgical meshes implanted in your body. That is not settled science — but it is definitely possible that some surgical meshes are breaking down and causing making people sick (more on this below). Relatively low-grade exposures to the skin, lungs, and gut surely aren’t as dangerous as a higher dosage right in our flesh, but I doubt that they are entirely safe either.
Nanoplastics are already found in most of our fruits and vegetables.35 This kind of pollution is happening to everyone, everywhere, forever, and still accelerating, and probably cumulative. Even if it’s not a problem in the early 2020s, the 2030s may be a different story.
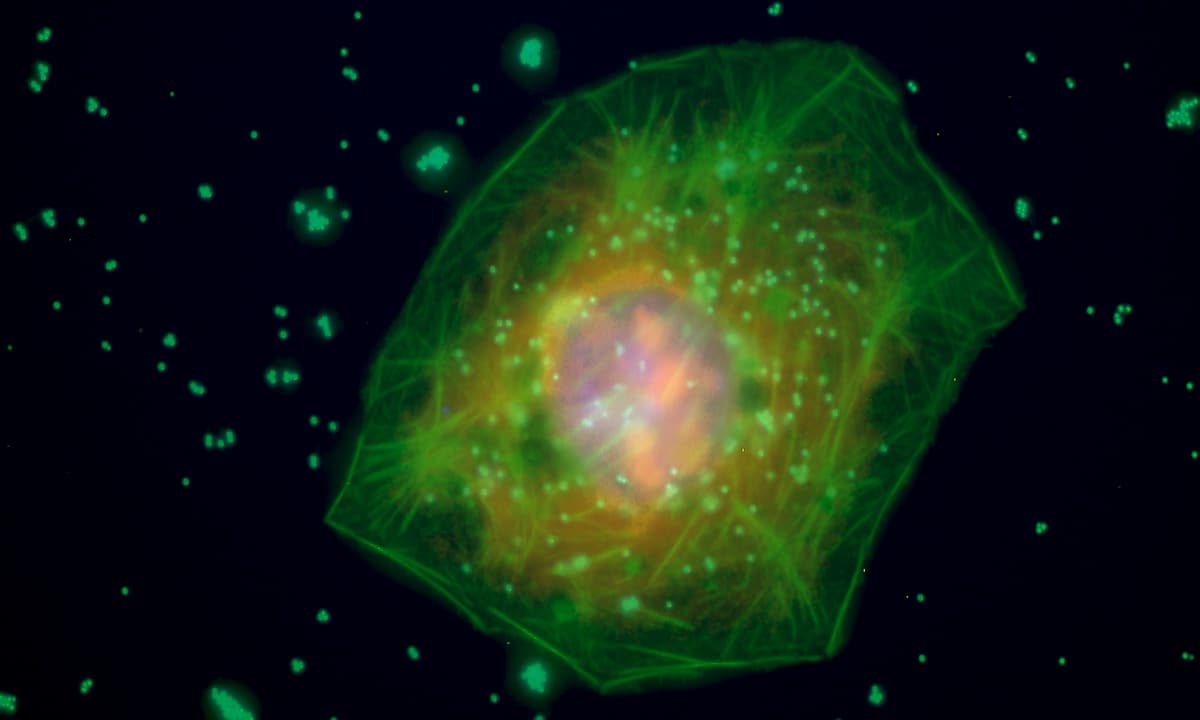
The small green spheres in this image are microplastics particles around and inside a liver cell. They are each about 0.5 μm across — two thousandths of a millimetre. And we know they can get much smaller still. Technically, we don’t yet know if or how harmful this is, but it does seem very what-could-possibly-go-wrong?
Surgical implants, especially the meshes
Surgical implants are a tragic example of a “pollutant” — a pollutant that is deliberately put right into our bodies, where it then clashes with our physiology in some way and causes complications to varying degrees.
While there is plenty of controversy about this, it’s not speculative or paranoid in broad strokes: some kinds of surgical implants have definitely harmed people. They absolutely can undermine general health. But how much, and how badly?
Awareness of the danger probably began with a surprisingly recent and well-documented disaster with metal-on-metal joint implants that poisoned people in the 2000s.36 but since then other kinds of implants have been implicated in chronic illness and pain, with varying degrees of credibility. But poorly designed and regulated surgical implants are generally a major concern.
The surgical mesh mess
Surgical meshes are the hottest sub-topic here. Various kinds of meshes are used mainly for repairing hernias, pelvic organ prolapses into the vagina, and stress urinary incontinence. Unfortunately, there is still very little hard data on long-term and systemic complications, and the issue continues (for years now) to be powered mainly by patient activism — which I do not dismiss, but I also cannot cite. The anecdotal evidence is certainly a very strong justification for better research … which we still don’t have.
Unfortunately, it is highly plausible that surgical meshes have made many people very sick. If true, you can bet that milder cases are far more common than the dramatic ones — people who just feel a bit cruddy and fragile. If you’ve had a mesh implant, and you feel like you’ve never really been quite right ever since, you should probably start reading. Do not uncritically accept that this probably explains your problems! There are a thousand ways to be wrong about this stuff. But there’s also too much smoke here to ignore the possibility.
I recommend continuing your reading with this balanced topic review from PatientSafetyLearning.org. I don’t think it reaches beyond the limited evidence, but also takes patient reports seriously. It’s actually a really great demonstration of how to think about this kind of controversy.
Mould as a pollutant
This is a little further out in left field than other, but not entirely out of the ballpark.
The “mouldies” are people that attribute their serious chronic illness to toxic mould in the environment. Almost anyone who has been hurting and suffering for no apparent reason for a long time will eventually stumble on this and wonder: “Could it be mould?” I think it’s one of the most unanswerable of all such questions, just impossible to call.
Mould can be toxic, and it surely does explain some illness. But I suspect you’d probably have to be quite unlucky to have case bad enough to matter, but mild enough to easily evade diagnosis. Unless…
Most mouldies have a hypothesis that reaches beyond the obvious toxicity: they think people can get so sensitive to it that even trace sources are dangerous, and effectively unavoidable. I do not dismiss the idea, and there are some reasons to consider it. But I have strong doubts, and the mouldies don’t exactly making it easy for a rational person to support them. Their claimed affliction seems identical in spirit to "electromagnetic sensitivity," which is a glaring example of a serious psychosomatic illness that has crystallized around a much less plausible explanation — a thoroughly debunked sensitivity to electromagnetic fields and radiation, like Wi-Fi. The only real difference seems to be that the mould hypersensitivity hypothesis is harder to falsify.
But if it’s even partially correct, it would be important. I neither accept nor reject the idea that mould traces are harmful to some people.
If you’d like to learn more, there is only one book to recommend: Through the Shadowlands, by Julie Rehmeyer, a science journalist who embarked on an epic journey to understand her own chronic illness, and ended up mostly falling down the rabbit hole of the mould threat.
I felt as though I was taking one more step away from the naïve assumption that, given time, science would save me. At this rate, the universe would come to an end first.
Still, it hardly made me abandon science. I held on to the knowledge that my illness could and should be understood scientifically. I continued to use my scientific skills and mindset to try to understand and treat it. And most of all, I continued to claim my citizenship in the land of science.
Through the Shadowlands, by Julie Rehmeyer
Food additives (and other things we aren’t good at digesting)
Talking about food additives risks fanning the flames of detox quackery and chemical paranoia even more than talking about pollutants — but there is another robust seed of truth here too. We have not come unscathed through over a century of industrialization and intense commercialization of the food system. There are some prominent historical examples, and there will probably be more in the future, and for every relatively obvious example there are probably several subtle ones that will never be confirmed.
Most things that we put in our mouths that cause systemic inflammation will probably do so through the intermediary of irritable bowel syndrome: our guts are important, so bowel stress and dysfunction leads to more widespread problems. Most of those are probably non-specific responses to mild irritants. They don’t have to be individually “dangerous” to be of concern collectively, and this is partly why we have so much scientific uncertainty about these things — because all the attention and research goes to more sensational dangers.
- Trans fats are the best example of what puts the “junk” in junk food: partially hydrogenated oils powerfully boost cardiovascular disease risk because they exacerbate metabolic syndrome with systemic inflammation. There are many paths to metabolic syndrome, but eating piles of trans fats is taking a highway to heart disease. Although banned in a steadily growing list of countries, they are still widely used around the world… and even where banned they remain in small quantities that can still add up, especially in extremely tempting snack foods. (And junk food is still junky for other reasons, of course.)
- Manufactured citric acid is an old food additive, rather boring and old-school — it has been around for over a century in many different foods,37 so long ago that it was already old when the US FDA got going … and they just gave it a pass and its safety has never really been studied properly. And yet there are specific biological reasons to suspect that it could be mildly toxic to some people.38
- Nonceliac gluten sensitivity is a tricky topic (understatement), but one way or another it is probably an example of struggling to tolerate something we eat — if only we knew exactly what, and how. The major candidates are gluten, FODMAPs, and the amylase-trypsin inhibitors (ATIs). FODMAPs have gotten a reputation for being the real troublemaker in wheat, rather than gluten, but that’s still not clear, and we do know that FODMAPs do not cause an inflammatory reaction — an “intolerance,” not a “sensitivity.”39 But gluten and the ATIs do trigger the immune system (inflammation) in some people. All three factors likely interact in complex ways for different reasons in different people. A practical takeaway from this mess: it is reasonable to be concerned that some people do in fact have allergy-like systemic inflammation triggered by something in wheat. The problem is probably being grossly overstated by many people, but I do think it’s real. I used to roll my eyes at wheat-fear, but I stopped when I learned more.
- Milk is a classic example of one of those things that some of us just aren’t very good at digesting: good old lactose intolerance, notoriously under-diagnosed, is one of so many things that can chip away at us sneakily. Lactose intolerance is not an immune system reaction (although there are also dairy allergies that are), but “it is now [2005] clear that lactose can cause a range of debilitating systemic symptoms, in addition to the well known gut symptoms.”40 At least 50% of people with lactose intolerance report muscle and joint pain.
- Olestra/Olean is an artificial fat (sucrose polyester) that infamously causes one of the most cringe-inducing symptoms of them all: anal leakage! But that’s just the tip of the iceberg of intestinal outrage.41 It’s likely that it has systemic health effects through the intermediary of IBS. And it’s still around in related forms! The sucrose esters are mostly dead as the basis for branded fat-replacement products, but they are still widely used as a food additive in smaller and less obvious ways.
- Artificial sweeteners are perpetually controversial, their safety endlessly ambiguous. Despite all of the research and media attention, most of that has focused on carcinogenicity, and the remainder has been about hormonal/metabolic effects (e.g. do artificial sugars make us insulin-resistant). A lot of those concerns are probably over-heated, classic examples of fear-mongering about chemicals. But what about the effect of artificial sweeteners on gut health? Which might actually drive inflammaging? Scientific crickets! A 2016 review declared that we know essentially nothing, and yet there are perfectly good where-there’s-smoke-there’s-fire reasons for the research.42 This is the more plausible way that artificial sweeteners could be a problem, and yet it’s the hazard that has not been studied.
A Canadian brand of “cyclamate,” the least potent of the common artificial sweeteners, and the one I like the best. I use a half packet in my coffee every day. I have wondered about its effect on my digestion, but also failed to confirm anything, despite a major effort.
Inflammation and fibromyalgia
The pain of fibromyalgia is an unexplained sensory dysfunction resulting in widespread oversensitivity to stimuli, exhaustion, and mental fog, among other things. It is stigmatized and both under and overdiagnosed,43 and all too often it is used as a way to dismiss the complaints of people who have unexplained pain, with the insinuation that they are “sensitive” or “dramatic” and don’t really have anything “real” wrong with their tissues.
That mistake does a great disservice both to patients who don’t really have fibromyalgia and those who actually do.
But you’re not paranoid if they’re really after you, and you’re not “sensitive” if you’re actually inflamed. And fibromyalgia patients are probably actually inflamed!44 Inflammation may be why they are so (literally) sensitive. Or perhaps even the other way around.
Fibromyalgia does routinely seem to involve sensitivity — the nervous system is over-reacting to stimuli — but inflammation can constitute an actual insult to tissues. Molecules produced by immune system activity, normally associated with infection and injury, are stimulating nerve endings (nociception). The information is sent to the spinal cord and brain for consideration, where the experience of pain may or may not be generated (but it probably will be).
Subjectively, it is nearly impossible — maybe impossible in principle — to tell the difference between the pain of an oversensitive nervous system and the pain of a nervous system that is actually detecting inflammation all over.45 And yet the conceptual difference is enormous. For instance, Lasselin et al. discovered in 2016 that chronic pain patients who are actually inflamed — confirmed with lab tests — are less responsive to behavioural therapy.46
Fibromyalgia may involve sensitivity and/or inflammation. Each of them might cause or aggravate the other, though it’s more likely that inflammation drives sensitization.
Inflammation and stress
The brain has a vast potential for sticking its nose into the immune system’s business.
Robert M Sapolsky, Why Zebras Don’t Get Ulcers, 2004, p. 144
There are strong but murky links between chronic pain and psychological stress.47 We still don’t know if stress directly causes chronic pain and other health problems — though there are signs that it can48 — or if it “just” feeds back into it, ramping up pain’s intensity and the suffering it causes.49
But they are certainly linked. We feel literally aged by adversity. We speak darkly of terrible events actually shaving time off our lifespans. And aging is nothing if not painful. And it is certainly possible that low-grade chronic inflammation is one of the main ways that stress can become painful. If stress is painful, inflammation is the most likely mechanism.
Inflammation is mostly immunity’s fingerprint,50 and we know (or strongly suspect) that “immunity is tuned by one’s emotions, personality, and social status as well as by other life style variables like sleep, nutrition, obesity, or exercise.”51
This is all a bit counterintuitive, because any smartypants “knows” that stress suppresses immunity, and that stress hormones — corticosteroids — are impressively anti-inflammatory.52 There are even viruses that monitor those hormones, waiting until we are weak to attack,53 or even meddling to trigger and exploit immunosuppression.54 Fascinating and horrible! This is specifically why certain kinds of viral flare-ups predictably occur when we are stressed.
So why would we worry about stress causing inflammation, which is nearly synonymous with immune function? The response changes over time. It’s insanely complicated, but prolonged and severe stress probably gets the immune system revved up, even to the point of causing autoimmune disease.
In the very short term (minutes), stress is an immune stimulator (inflammatory). But then, almost right away, that effect gets reeled in to prevent collateral damage: you don’t want sustained immune stimulation! This suppressive effect is robust, and it’s why stress/steroids suppress inflammation. But in chronic stress, the stimulatory phase keeps happening over and over again, and the suppressive phase never quite catches up, and so overall immune system activation gradually ratchets up and up and up. Ergo, long term stress is inflammatory.55 For instance, we know that nervous-wreck monkeys are inflamed, their immune systems a mess56 — and the same thing probably happens in humans. We suspect that rough childhoods may be a risk factor for several disorders that may share inflammation as a mechanism.57
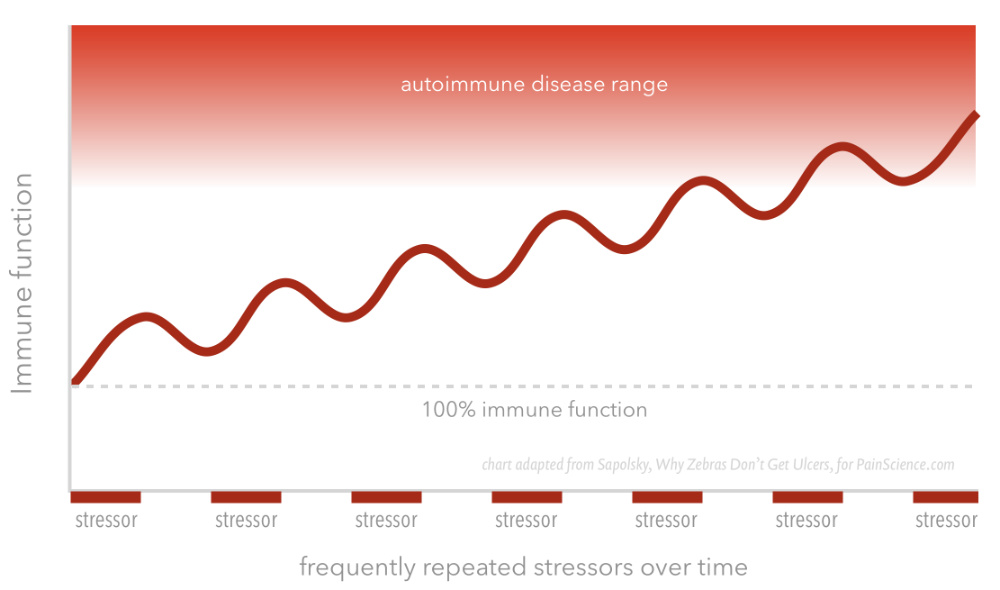
“A schematic representation of how repeated stress increases the risk of autoimmune disease,” adapted from Sapolsky’s Why Zebras Don’t Get Ulcers.
More stress inflammation links! 🔗
- The relationship between metabolic syndrome and inflammation is clear, and there may also be a link between metabolic syndrome and stress,58 and is almost certainly a link with sleep disturbance (which overlaps with stress, obviously).59 If true, it means that metabolic syndrome could affect millions of people who would not otherwise be likely victims.
- We know that sleep deprivation (one of the most common forms of chronic stress) actually ages us in an objectively measurable way,60 and we know that age is strongly linked to inflammation (inflammaging).
- There’s evidence that suggests that various soothing forms of treatment — yoga, meditation — may reduce chronic low-grade inflammation.61 Disclaimer: this is a very complicated, conflicted area of the scientific literature, possibly polluted with a lot of wishful thinking.
- Neuroinflammatory sickness behaviour (which includes sensitization) is a well understood basic physiological response to major injuries and illness: serious threats to the system. Neuroinflammation may also be triggered solely by perceived threats: a very psychological driver of painful inflammation. See below for more on this sub-topic.
It’s really quite a lot of “circumstantial” evidence, isn’t it? This is hardly a complete tour of inflammation-stress science, but three times as much wouldn’t change the punchline: there’s probably a very complicated link.
Neuroinflammation — A fire in the nervous system
Any tissue or system in the body can get inflamed, with many possible consequences, but inflammation of the nervous system is of special interest for patients with excessive aches and pains, more serious unexplained chronic body pain (fibromyalgia), and other medically unexplained symptoms (MUS).
An “inflamed nervous system” sounds like sensationalistic nonsense preceding a sales pitch for something that puts out the fire, but bear with me (and there’s nothing for sale). The nervous system gets inflamed in many ways for many reasons — neuroinflammation isn’t monolithic, any more than inflammation in general is. But there are some strong, and neuroinflammationis probably a major shared mechanism of misery in several kinds of puzzling chronic pain and illness.
Infection aching is a good introduction to neuroinflammation — an easy way to start understanding it.
Cold, flu, and covid often start with weakness, malaise, and nasty widespread muscle and joint aching — the “infection aches.” Not everyone gets infection aches,62 but most of us have had the displeasure at some point. It’s a distinctive sensation, and strikingly similar to post-exercise muscle soreness, and to the widespread aching routinely suffered by many people with fibromyalgia, and other puzzling chronic pain. When I finally got my first case of Covid in the summer of 2021, my infection aches were extreme — but also eerily similar to my normal chronic pain problems.63
Why does the aching that often precedes infections feel exactly like some other common kinds of chronic pain? What do they have in common?
It’s probably not a coincidence. They are likely both powered by neuroinflammatory sensitization — one of the major symptoms of “sickness behaviour.”

Neuroinflammation — Sickness behaviour
Being sick or injured is a double whammy: we get the symptoms of that illness/injury plus the general malaise that “encourages” us to retreat from life and take fewer risks with our bodies. That gross feeling of exhausted fragility is known as “sickness behaviour.”
Sickness behaviour is a constellation of disabling symptoms that happen in all animals as a normal response to threats to our health.64 The symptoms are neuroinflammation. Just like a fever, sickness behaviour is a defensive reaction imposed on us by our immune system for our own good. It’s not just a random shitty side effect of immune system activation! Its symptoms have a critical functional purpose: it forces rest and isolation. “No foraging this week!” Much like the acute pain modifies behaviour to protect us from immediate tissue threats, so does sickness behaviour, just more slowly and generally.
Sickness behaviour is so effective at keeping us from making bad illness/injury situations worse that it’s a highly “conserved” trait — which is a biologist’s way of saying that it’s too important for any organism to evolve away from. Critters have probably been getting neuroinflamed for as long as there have been critters (about 600 million years). Very cool biology.
But it is unpleasant! This system is extremely burdensome even when it’s working exactly as nature intended, in situations where the need for it is relatively obvious (e.g. fighting off a major infection). But it may have unsuspected and poorly understood triggers, including some that don’t make much sense. It might even get downright dysfunctional.
Neuroinflammation — Subtler examples?
In modern medicine, sickness behaviour has traditionally been defined as a response to major infections, but it’s clearly not limited to that.
It also fires up after major injuries, for instance. After my wife’s terrible accident in 2010 — a major brain injury and spinal fracture, plus several other less serious fractures and lacerations — a doctor warned her not to underestimate how profound and prolonged her fatigue would be, and indeed she was utterly exhausted for a good year. Healing is metabolically expensive, and so we need rest after major injuries … and neuroinflammation enforces it.
Research is revealing that neuroinflammation is kind of a big deal, a complex generalized response to almost any kind of major stress. And the most dramatic examples of sickness behaviour are probably not the only examples. They are almost certainly the tip of an iceberg of subtler examples. Neuroinflammation probably has many forms and triggers, and may go wrong in sneakier ways than is generally appreciated.
It’s not too surprising that a fierce viral infection might knock the immune system off kilter. But sickness behaviour may also have some dysfunctional triggers.
Neuroinflammation — When neuroinflammation goes wrong (mostly by going long)
Neuroinflammation can definitely be painful. It can cause sensitization (that’s how the infection aches work). Lowering pain thresholds has an obvious functional role to play in sickness behaviour: what better way to force an animal to take it easy than to make everything hurt a bit too much? This link has not been firmly established yet, but science is closing in. We do already know for sure that chronic widespread pain is closely linked to sensitization. So sensitization might bridge the gap between the clinical problem of chronic widespread pain and the biological mechanism of neuroinflammation, and so “neuroinflammation drives widespread chronic pain via central sensitization.”65
Why chronic, though?
The most obvious way that neuroinflammation can go wrong is to drag on. Once it starts, it might be somewhat self-sustaining, a perpetual malaise machine, obnoxiously persisting even without an ongoing threat. This is actually one of the top Long Covid theories: the neuroinflammatory process spins out of control (“immune dysregulation”), and just won’t wind down when the infection is over.66 It’s a strong hypothesis.
If that’s what’s going on with Long Covid, then it’s probably also what’s happening with a lot of ME/CFS and fibromyalgia. In 2019, Albrecht et al. published the first in vivo evidence of neuroinflammation in fibromyalgia patients,67 and there has been plenty more related evidence since then.
Neuroinflammation — A response to perceived threats?
The signs and symptoms of neuroinflammation accompany all chronic and serious diseases and traumas. But do we actually have to get sick or hurt to trigger sickness behaviour? Could it also get fired up without any actual physical danger? What if sickness behaviour could be caused by the fear of danger alone? Humans are extremely good at imagining threats, much better than cats or capybaras (or zebras, which is “Why Zebras Don’t Get Ulcers”68). Are we good enough at it to fool the body into a reaction normally reserved for actual physiological trauma?
If we are, it would go a long way to explain some cases of medically unexplained symptoms and chronic pain. Many of those illnesses involve the classic symptoms of “sickness behaviour” without any obvious actual injury or illness.
We know that childhood traumas are not just inflammatory (as cited above) but specifically neuro-inflammatory69 — the developing brain is quite vulnerable to intense psychological stresses. We also know that those people suffer more chronic pain in adulthood.70 And serious psychological distress is linked to neuroinflammation in adults too: for instance, people with PTSD have more neuroinflammation.71 PTSD is defined by the inability to stop perceiving, remembering, and re-living serious threats — so who better to imagine threats vividly enough to trigger sickness behaviour? If it happens at all, it must happen there.
So there’s not really any doubt that psychological stress is neuroinflammatory. That leaves just one key question: is it enough of the right kind of neuroinflammation to drive sickness behaviour? That question has not been scientifically answered yet.
Nor is it just a matter of waiting for confirmation of the obvious. We really just don’t know, and there are good reasons to doubt it. I have been writing about neuroinflammation like it’s one thing, but of course it’s not: it’s a broad class of immune interactions with the nervous system. Stress could certainly be neuroinflammatory by some reckonings, and yet still fall well short of causing sickness behaviour. Woodburn et al. argues persuasively that the kind of neuroinflammation caused by major physical trauma or disease is just in another league, and it isn’t plausible that any psychological stress could ever trigger anything like that, let alone merely being anxious and burned out — which is the kind of “stress” the vast majority of people suffer from.72
↑ MEMBERS-ONLY AREA ↑
Leaky gut syndrome
This is a fake disease, based on the “hypothesis” — it barely deserves that word — that our modern diets are so full of irritating substances that our bowel is literally full of holes. Those substances, and gut bacteria as well, seep out into the abdominal cavity and provoke an autoimmune reaction. Leaky gut syndrome has been nominated as the root cause of nearly every unexplained syndrome there is, anything that can be plausibly linked to “inflammation.”
The alleged cure? Usually it’s just to eat like a prehistoric human. The autoimmune protocol (AIP) diet, which is a strict version of the trendiest of all trendy diets, the “paleo” diet: basically anything humans have eaten since the stone age is considered risky. This is obviously just an elimination diet that casts a wide net over everything you can put in your mouth that has ever been demonized, from food additives to gluten to dairy to nightshades. It’s a classic example of the naturalistic fallacy at work.
The theory is much more full of holes than anyone’s gut. The whole thing is nasty faddish pseudoscience being profitably marketed by all the usual suspects. For serious debunking, see the Canadian GI Society. For a more whimsical and snarky one, which is probably all it really deserves, see Dr. Mark Crislip’s analysis.
Part 2
What can you do about inflammation and inflammaging?
No one really knows, of course, and quite possibly nothing. But here are some ideas …
Exercise and fitness: Of course. You knew this was coming. Regular moderate exercise really is the closest thing we have to a miracle drug or a fountain of youth.73 The older you get, the more you should avoid the extremes: too much and too little are likely both a problem, especially for tissues that are already hard-pressed. But exercise in the Goldilocks zone is absolutely broadly anti-inflammatory over the long-term,74 — we know this for sure. And it starting to seem increasingly clear that it’s also anti-inflammatory for more specific tissues and their issues over weeks or months instead of years. Weight loss is not just a biomechanical relief — literally lightening the load — but also a metabolic upgrade.
Substantial weight loss can eliminate the danger and even reverse damage. This is famously easier said than done, of course! But diet, exercise, surgery, and now (finally) medications are all effective to varying degrees. Strength training is a surprisingly important tool — see next item.
Even at its fastest, the anti-inflammatory effects of exercise and weight loss are never going to deliver dramatic or immediate results, but it still may be the single best option we’ve got. Fitness is a rising tide that (probably) lifts all “boats,” reducing the intensity of many kinds of painful problems. One important exception: the exercise intolerance that accompanies many illnesses doesn’t completely block this option, but it certainly makes it much harder.
Exercise for strength especially: Do you even lift? You should! It’s not for everyone, but it is for many people who haven’t realized it yet. It’s a more well-rounded and efficient workout than most people realize.75 It is probably the most effective kind of anti-inflammatory exercise, because muscle pumps out anti-inflammatory signalling molecules when you “pump iron.”76 And weight lifting specifically fights metabolic syndrome77 and neuroinflammation.78 That’s because building muscle is a particularly good way to reduce excess visceral fat. To some extent it actually even “targets” belly fat, that holy grail of exercise for vanity!79 For more about strength training, see Strength Training for Pain & Injury Rehab.
Anti-inflammatory nutrition: It’s also possible to eat an anti-inflammatory diet to some extent — but it isn’t nearly as promising as that sounds. Things like Dr. Weil’s “Anti-Inflammatory Food Pyramid” are full of wishful thinking and make the science of anti-inflammatory diets seem way more complete and tidy than it actually is. Or there’s the autoimmune protocol (AIP) diet for “leaky gut syndrome,” which is all nonsense (see the leaky gut syndrome section). The smart money is on a diet that is just generally healthy, mostly by being low in obvious junk food (especially the ones that are a challenge to blood sugar regulation). Supplements and anti-inflammatory “superfoods” are mostly a pipe dream and the stuff of marketing. But there are a handful of quitegoodfoods with a bit more evidence of health benefits than normalfoods: Examine.com (well-known for good critical analysis of nutrition claims) votes for garlic, dark berries, spirulina, and leafy greens. I might add a couple foods rich in omega-3 fatty acids (mostly some fish and nuts/seeds).
Lose weight: and not by fasting, and not with a massive exercise effort (though it could be involved). I’m talking about good old-fashioned calorie restriction … and/or the substantial and near-miraculous assistance of semaglutide injections (Ozempic etc). The oversimplified version of this advice is that "belly fat is inflammatory," and reducing it is effectively anti-inflammatory, probably regardless of any other factor. This point harmonizes with several other ideas here, but also effectively stands on its own as an evidence-based claim, thanks to a very important 2024 study that showed that knee arthritis improves significantly with weight loss assisted by semaglutide.80
Ketogenic diets and fasting: Just as scientifically sketchy as any other kind of anti-inflammatory dieting! But possibly worth experimenting with nevertheless. More below.
Reduce stress: Even though it’s really not confirmed that there is a link between stress and inflammation, stress management has so many benefits that it is worth pursuing regardless. You don’t have to meditate or do yoga (unless you want to). Often the best place to begin is troubleshooting major sources of chronic stress, like insomnia or anxiety.
Quitting bad habits: Consider finally ditching habits that are obviously putting a strain on your biology, especially smoking (of course, smoking is a well known independent risk factor for pain) or drinking too much too often (anything more than a couple drinks per day). Any kind of “hard living” is suspect. Coffee in reasonable doses, mercifully, is not an obvious suspect (it doesn’t dehydrate you, for instance81) — but if you’re drinking so much that it’s aggravating emotional stress with caffeine-powered agitation and anxiety, that’s another matter.
Predictably, these treatment options all look suspiciously similar to common treatment recommendations for fibromyalgia.
Can low-grade inflammation be diagnosed with blood tests?
A lot of inflammation is not easy to detect. It may hide effectively in specific tissues and systems, only detectable with complicated, expensive, invasive testing. This is one of the main reasons that some diseases have been so mysterious for so long.
There are more accessible blood tests that are quite sensitive to various signs of inflammation, but — because biology is messy — they are not super reliable, and even people with serious inflammatory diseases do not always get a clear result.
Many tests are not available as clinical tests for ordinary folks at all; they’ve just been used by scientists to show that:82
concentrations of inflammatory factors in these conditions are overall slightly higher than in healthy populations, but still remain in the healthy ranges. It is therefore hard to determine whether a specific patient exhibits ‘low-grade inflammation.’
Nevertheless, it’s worth asking your doctor. In particular, check your “CRP” (C-reactive protein). This is a common and easy test, and who knows: you might discover that you have not-so-low-grade inflammation. But the absence of a clear CRP signal does not mean that you aren’t inflamed.
Tickling your vagus nerve: vagus nerve stimulation, or just relaxation?
The vagus nerve is the “relaxation” nerve, deep in the neck, passing through a hole in the bottom of your skull. Relaxation involves several physiological changes stimulated by vagus nerve activity. If you could stimulate your vagus nerve by any means, it would relax you, and a lot of people get excited by the idea of a shortcut to profound relaxation, a calming “switch.” It’s not really in doubt that this is possible in principle, but it is very much in doubt whether it’s practical, or meaningfully better than just, you know, relaxing.
So how do you stimulate a vagus nerve? Well, mostly you don’t, not without an implant (more on that below). In a self-help context, some people have argued that relaxing is how you “stimulate the vagus nerve,” and that meditation is basically just focused, “formal” relaxation. The simplistic rationale is just that, if the vagus nerve induces relaxation, then relaxation must “stimulate” the vagus nerve. That’s doubtful. And, if you’re already relaxed, why stimulate the vagus nerve anyway?
Well, vagus nerve stimulation might go beyond just “relaxing” us. It might also reduce inflammation — or fail to do so.
The vagus nerve regulates immune system activity by detecting and responding to signs of inflammation — the “inflammatory reflex.” Immune regulation is insanely complex, but the inflammatory reflex is a major component of that system, and it’s a simple enough idea in itself. Too much inflammation? Vagus nerve does its thing. The inflammatory reflex may be impaired in people with excessive inflammation.83
Still genuinely interesting topic, though.
You can’t pay for vagus nerve stimulation yet, even if it is a great idea. So how else could vagus nerve stimulation be achieved? Pavlov and Tracey devote dizzyingly complex passages to “novel therapeutic approaches” that might achieve “cholinergic suppression of inflammation” either by inspiring the vagus nerve to do it, or by doing it directly by other means. Mostly it’s about exotic drugs, and there’s a passage about implanted vagus nerve stimulators (none of which is practical or accessible). There’s some discussion of the effects of nutrition (much more accessible).
What they do not discuss is how normalization of the inflammatory reflex might be achieved by extra relaxation — that is certainly implied, and seems well worth exploring. It is possible that some kind of artificial stimulation or simulation might constitute some kind of a kick-start for a glitchy inflammatory reflex, but it’s also possible that a big boost in relaxation — a new meditation habit, for instance — is actually easier and better. No one really knows.
How about massage? You certainly aren’t going to stimulate the vagus nerve with massage in any meaningful way — the “vagal manoeuvre” (carotid sinus massage) can stimulate one reflex that isn’t actually mediated by the vagus nerve, and would only involve a small portion of it if it was. For much more information about this, see Can neck massage stimulate the vagus nerve? For better or worse? [members only]. The answer is a decisive “no,” but the explanation and details are quite fascinating (for physiology dorks).
Reducing inflammation with a ketogenic (very low carb) diet
Diets that force you to mainly burn fat for energy, instead of carbohydrates — like the infamous Atkins diet — may be anti-inflammatory and/or otherwise metabolically salubrious. This also includes fasting and intermittent fasting, discussed more below, but I’ll start with low-carb diets, which have been popular for much longer.86
Ketogenic diets are low enough in carbohydrates (sugars) that they force the body to burn an alternate fuel source, ketone bodies. This state is known to treat epilepsy surprisingly effectively in some children,87 and we can infer from that success story that the biology of this treatment might also have an effect on some kinds of inflammation and pain (especially neuropathic pain, the pain of damaged nerves88). Although speculative, there are some reasons to think this might work, and some indirect (animal) evidence that it does.89 Like seizures, some kinds of pain may involve “overexcited” neurons, and can be partially treated with anticonvulsant drugs (although with highly variable results and significant side effects and hazards, especially in older patients90). Ketone metabolism “produces fewer reactive oxygen species,” a contributor to inflammation; and it produces adenosine signalling, which is a suspected pain-killer in other contexts (exercise, possibly acupuncture).
This is an experimental treatment. However, just like an anti-inflammatory diet (AKA “healthy”), it has a non-crazy rationale, and it’s safe and inexpensive to dabble in. As long as you don’t get extreme, the worst-case scenario is putting up with a fussy and unpleasant change in eating habits. Nevertheless, I am obliged to suggest that you run this by your physician and/or a nutritionist.
You should probably spend at least two to four weeks in a ketogenic state to be sure that you’ve given it an adequate chance to work its magic. If you see a clear reduction in symptoms, that’s a strong sign that it’s working. In a spirit of moderation, I do not recommend trying to stay in a ketogenic state for any more than several weeks at a time, and you should probably take breaks — give your system a rest from ketogenesis once every week or two.
Is intermittent fasting anti-inflammatory?
Atkins is so 2005. These days, the cool kids are inducing ketogenesis with some intermittent fasting — also known as “skipping some meals.” This practice has achieved Hype Factor 10, and almost everyone seems to believe that it has substantial general health benefits, a special metabolic sauce that improves us. Not-eating as actual medicine. “Would you like to not eat this? It’s good for you! 🎶”
I’m focusing on the more specific claim that fasting is anti-inflammatory.91
In late 2019, intermittent fasting was given a huge publicity boost by a widely cited New England Journal of Medicine paper, basically a fancy opinion piece,92 and their opinion is: “fasting is probably great!” The paper contains an on-the-nose assertion for our purposes here: “intermittent fasting reduces markers of systemic inflammation.” That statement is supported by four references. That seems like plenty. But are the references persuasive? Not so much. Did a stoned undergrad pick those out? Do peer reviewers even look at the footnotes?93
As far as I know, there is literally only one solid study showing clear evidence of an anti-inflammatory effect in humans.94 (It is even more recent than the NEJM paper, so it wasn’t cited there.)
So the “growing body of evidence” has been exaggerated by everyone, surprise surprise, and fasting has not yet been shown to be “anti-inflammatory” per se. Yet. That’s the bad news. The good news…
I believe (opinion alert) that there’s actually a decent chance that an anti-inflammatory effect of fasting will be confirmed in time. It’s actually quite plausible, based on lots of indirect evidence — animal, cell, more general research, and so on — which truly is accumulating.
It’s also just a reasonable diet. The worst-case scenario for any non-extreme attempt is just getting pretty hangry (angry from hunger). And it’s probably perfectly good as a weight-loss diet if nothing else. You’ll even save time and money, making it a great rarity in rehab — even the most harmless treatment experiments usually take some money/time.
And here’s a simple idea to end on: it may not be that fasting is anti-inflammatory, but rather that long-term overeating is inflammatory, and fasting is just a rather dramatic way of swinging the pendulum away from that metabolic trap. So we’re back to the idea that the only “anti-inflammatory” diet is just one that isn’t inflammatory.
Some further reading on intermittent fasting: Martin Berkhan’s LeanGains.com (start with his myths of fasting), and Dr. Bojan Kostevski’s thesis paper, “The Effects of Intermittent Fasting on Human and Animal Health.”
Pass the bag of pain! Junk food as an inflammation driver

Bag of yum? Definitely (well, maybe if it was a better brand). Bag of pain? Disturbingly plausible. Although not as fast-acting as a poison that causes inflammation, a lousy diet might actually be able to cause pain in the relatively short term. But if that’s true, it’s also probably reversible.
For many years I have been encouraging pain patients to be as fit and healthy as possible as a way of preventing metabolic syndrome while improving the long-term odds of getting pain-free.95 It’s possible that I have underestimated just how good that advice was — how strong and fast-acting, more like actual medicine.
Removing excessive junk food might be directly anti-inflammatory for some people in the same way that we might expect relatively short term health improvements from quitting smoking or drinking.
That claim and this section were inspired by evidence from a new study by Elma et al.96 They didn’t produce the most robust data I can imagine, but it is intriguing, and it makes me want to instantly stop eating potato chips, just in case.
Which is a tall order. I really like potato chips. But I would give them up for pain relief! (And obviously there are junkier foods than potato chips. They're just one very familiar example.)
Elma et al. showed that people with back pain eat quite a bit more junk food, and have a lot more fat in their blood. This doesn’t necessarily mean that the poor diet actually caused their pain — but it might. It’s disturbingly plausible. The implication is that there wasn't just a correlation between back pain and eating poorly, but the consequences of it.
The long game versus short-term effects
I always thought a good diet was a smart long game for pain patients, but I never thought eliminating chips and beer was going to be a pain-reliever in the short term. It was more of a “rising tide lifts all boats” thing, a general and slow-acting tonic. I didn’t think junk food was inflammatory per se, “just” that it corrodes health in a way that makes pain likelier and nastier over time.
This new study encourages me to consider revising that in the best possible way: maybe we can reduce pain in the relatively short term by improving diet after all. Maybe it can happen about as fast as we can bring our cholesterol levels down — so roughly three months for most people.
Unless you have a genetic issue that keeps it high, like familial hypercholesterolemia, which affects about one person in 200 — yours truly being one of them.
More about the study
The researchers compared the diets of healthy people versus folks with unexplained chronic low back pain, about fifty of each. Everyone did a three-day food diary, filled out questionnaires, and had the pleasure of a going through a test for pain sensitivity (thank you for your sacrifice, study participants).
The diets of the back pain group were worse in every way. And they had more fat in their blood. And more inflammation. They also ate less of a few foods “known for their anti-inflammatory and antioxidative properties.”97
Three days of a food diary and a few dozen subjects with pain isn’t enough to prove anything (especially “causality”), and there are certainly some reasons why these results might not be quite what they seem. There are always sneaky confounders in diet and pain research, and it’s clear that there must be other variables in this equation — because obviously not everyone with high cholesterol has chronic pain, and not everyone with chronic pain has high cholesterol.
How this data fits into the bigger picture
The evidence may not be strong and it does not show causality, but it also isn’t exactly a big break with what we already knew. There is plentiful evidence that dysfunctional eating causes metabolic syndrome over long periods, which is nearly synonymous with systemic inflammation … and so an obvious risk factor for pain. But that has always seemed like an indirect and delayed hazard, like the danger of eventually getting cancer from smoking.
This new evidence from Elma et al. suggests that a terrible diet could be more of a clear and present danger: you could be hurting right now because you’ve been eating garbage recently. And if the cholesterol comes down, so might the pain. Not necessarily. But quite possibly. See also Bakshi, who reported in 2021 that dietary cholesterol is linked to pain sensitivity — again, not necessarily causally linked, but it’s certainly not a crazy idea.98
We must never forget that “correlation is not causation,” but we must also not forget that “it sure is a hint.”99 Causality is definitely possible here.
The implications are … healthy
The implication of the data is that pain patients should consider minimizing junk food. While I wouldn’t want to deprive suffering people unncessarily of cheap, easy, comforting foods, it’s not like you’re going to do yourself any real harm by eating better (especially as a temporary experiment). Compare and contrast this with the costs, risks, and shockingly low plausibility of so many other ways of treating pain! This one is extremely tame by comparison.
Three months to less fatty blood and less pain — if it actually works for anyone — is still not a quick fix by our impatient modern standards, but it’s sure a lot faster than “years.” Many people will read this and, just like me, immediately start looking at a bag of chips with deep suspicion. Like it might just be a bag of pain! Like it might make you more fragile in a season, rather than a decade.
Massaging the inflammation away
Basically there isn’t a shred of evidence that any kind of massage can reduce any kind of inflammation in a clinically meaningful way. However, you see this claim touted surprisingly often, because of course it sells massage tools and services, and it’s suitably non-specific and technical sounding — even better than “increasing circulation.”
Although it’s not crazy to check for an anti-inflammatory massage effect, all such scientific efforts thus far have failed. There are two particularly notorious examples of over-hyped research on this score:
- In 2012, Crane et al. very elaborately studied changes in the proteins that cells constantly make (“gene expression”).103 They compared muscle tissue samples with and without massage and concluded that “massage therapy appears to be clinically beneficial by reducing inflammation and promoting mitochondrial biogenesis.” Unfortunately, this was quite misleading, and the results of this study were really quite negative: the data showed that massage has no significant effect on gene expression in muscle cells. There were several major problems with the study. For very detailed analysis, see Massage Does Not Reduce Inflammation.
A much more recent hype-storm formed around the work of Seo et al., who made this extraordinary claim in 2021: “robotic” massage of mice supposedly helped their little muscles heal.104
This was another overly elaborate and technical study, this time massaging injured mouse muscles with high doses of vibration, again purporting to find evidence that massage is “antinflammatory” and “regenerative.” While some of the findings are intriguing, it’s extremely unlikely that they are replicable or clinically relevant in people. The study is a classic example of a “fishing” expedition: a search for meaningful signals in a lot of complex data. You can read my detailed analysis here: “Robotic Mouse Massage: Is It ‘Regenerative’ and ‘Anti-Inflammatory’?”
More ordinary clinical tests of massage for exercise-induced soreness have showed either nothing or only trivial benefits. I report on that research at length in A Deep Dive into Delayed-Onset Muscle Soreness.
Hyperventilation + cold exposure = anti-inflammatory (maybe)
Meditation, breathing, and cold exposure have all been touted as anti-inflammatory, often by gurus with dubious credibility. There’s a long history of half-arsed science about all of these things, and it’s disheartening to try to get anything useful out of that literature. But we do have good reasons to believe that something in that mess seems to have some “anti-inflammatory” effects (to oversimplify). So I was quite happy to see an interesting 2022 experiment that focused specifically on trying to identify the “active ingredients.”
Zwaag et al. observed a clear anti-inflammatory effect from hyperventilatory breathing exercises both alone and when combined with cold exposure. Cold exposure alone had no effect, but it did seem to enhance the effect of the breathing exercises.105
This experiment was impressively gruelling for the participants: the researchers put a few dozen healthy young men through several days of intense breathing and/or cold exposure training, for hours at a time, and then artificially cranked up their systemic inflammation with injections of bacterial lipopolysaccharides. Serious business! Lots of care and ethical oversight required to do a study like this safely.
The breathing exercises mainly consisted of extensive hyperventilation. Most people would find the full protocol prohibitively challenging and exhausting. Happily, the researchers also tested easier methods… and were convinced by their data that a much tamer and simpler protocol had the same effect. Yahtzee.
The cold exposure protocol was even more intense, and impractical for most people to even attempt.
All of the hyperventilating certainly seemed to reduce objective signs of endotoxemia (assuming no statistical jiggery-pokery, which is always possible of course).
The simplest practical implication is that hyperventilation exercises alone might reduce some systemic inflammation in ways that could be helpful for some kinds of chronic pain … and that breathing probably works better with a bunch of added cold exposure. There’s plenty of uncertainty here, and in particular the required dosage might just be too much for a lot of people, but the data clearly shows that there is potential in principle. The word “promising” gets overused in this business, but I think it might actually be applicable in this case.
For additional perspective on this paper, see the blog post “Anti-inflammatory hyperventilation: I’ll huff and I’ll puff and I’ll blow my pain away.”
Hungry, hungry humans balance the energy budget by … cutting inflammation?! The detailed case for exercise as anti-inflammatory medicine

The bad news? You have to burn quite a few calories. The good news? We know better than ever exactly why it’s so good for you.
There is lots of decent indirect evidence that fitness is fairly potent anti-aging and anti-inflammatory medicine (summarized earlier with several citations), but new science emerged in 2021 and 2022 that daily physical activity is linked to meaningful reductions in generalized inflammation. Yes, we are still learning!
It turns out that maybe exercise can convince our body to spend a bit less energy on defence: reduced immune system activity, AKA inflammation, that holy grail of general health. Optimistic, science-based life hacks are not my usual style, but I think this one’s cromulent (wouldn’t publish it if I didn’t). It takes some proper splainin’, but the journey is interesting, and the destination useful: an excellent new scientific justification for exercise as medicine for chronic pain.
First you need to know that humans are unusually fuel-hungry critters. We burn through calories much faster than any other primate. The old idea was that homo sapiens uses energy like other animals, but that reasonable assumption was knocked over surprisingly recently, by evolutionary anthropologist Herman Pontzer.106
In fact, humans need quite a lot of fuel, probably because of all the brains. Brains are expensive.
Pontzer et al. used the most new-fangled methods to measure energy usage in people of all ages — 8 days to 95 years. Highlights:
- Toddlers are the metabolic champs, hitting 50% more energy burning than their parents.
- The power hunger declines to adult levels by about the age of 20.
- After 20, metabolic demand remains relatively stable for a long time, declining quite slowly over forty years, even during pregnancy.
- In the seventh decade, larger declines in calorie-burning start to kick in.
That’s all “fun facts,” but another result might be a little more consequential.
All brains are metabolically “expensive,” but this one burns extra calories from all the wiggling.
Homo sapiens is also amazingly good at balancing the energy budget
We keep our total cost of activity surprisingly consistent over time. If we exercise more, our clever biology starts to actually cut back on other metabolic expenses — so we don’t burn as much extra fuel as we expect.
This does not mean that the exercise is futile! Despite some hype to contrary (doubling down on the idea that “you cannot outrun your diet”), exercise is still a valuable part of any weight loss plan, for instance.
But every calorie counter knows all too well how much harder it is to get rid of calories than it is to shovel them into our pie holes in the first place … and this new data means the deck is even more stacked against us than we thought.
So: the body tends to actually reduce overall metabolic spending, the better to afford extra exercise. That budgeting adjustment is cool, and not especially controversial as far as I know. (Although saying that is like casting a magic spell that summons an expert to put me in my place: “experto correctium!”) Now for the cool part…
Where exactly do these metabolic spending cuts happen?
What gets sacrificed? This is where this all plugs into the world of pain science. Pontzer postulates (as quoted by Gibbons):
“I think we’re going to find these adjustments lower inflammation, lower our stress reaction. We do it to make the energy books balance.”
That is quite a thought. Is Pontzer nuts? No, it’s just legitimate speculation. If true, it would be a tidy new way to explain why exercise is such good medicine.
The need to conserve fuel for exercise may reduce how “seriously” the body takes its stress — how much energy we invest in maintaining better-safe-than-sorry levels of immune system function.
Fresh evidence that exercise does indeed tame inflammation
While this post sat in my drafts folder for a while, Pontzer’s team published the results of a test of this hypothesis.107 Bravo! Nice timing!
They crunched the numbers in a big health database to find a long-term relationship between energy expenditure and inflammation, and found it: sustained daily physical activity was linked to reductions in the several major biomarkers for systemic inflammation, like C-reactive protein (CRP) and white blood cells. Cool.
So this intriguing idea is now at least partially evidence-based, and relevant to chronic pain — which is often more about biology than biomechanical strain and tissue failure.
Exercise is probably good medicine for many kinds of pain
There’s really no longer any question that exercise is broadly anti-inflammatory over the long term, specifically and especially exercise that emphasizes muscle (resistance training). This is now very well established. The “myokine hypothesis” is that muscles actually secrete anti-inflammatory compounds when they are used, and it has been demonstrated in several ways over the years,108 and continues to be.
For instance, we now know that exercise can even ease the suffering caused by severe autoimmune diseases, like axial spondyloarthritis (inflammatory pathology of the spine).109 Inflammation doesn’t get much more serious than that … and yet it seems to back off enough to matter if you exercise! It’s not a cure, of course, but it’s frankly amazing that it works at all.
And there’s plenty of evidence that the right dosage of exercise — not too much, not too little — may even be anti-inflammatory for “minor” musculoskeletal injuries like Achilles tendinitis or plantar fasciitis or frozen shoulder — not at all minor if they are keeping you from doing your job, or playing your sport! This remains unproven, but there’s a good case for it, which I explore thoroughly in my guide to repetitive strain injury.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Part 3
Appendices
Related Reading
- A Painful Biological Glitch that Causes Pointless Inflammation — How an evolutionary wrong turn led to a biological glitch that condemned the animal kingdom — you included — to much louder, longer pain
- 38 Surprising Causes of Pain — Trying to understand pain when there is no obvious explanation
- The Complete Guide to Trigger Points & Myofascial Pain — An extremely detailed guide to the unfinished science of muscle pain, with reviews of every theory and treatment option
- The 3 Basic Types of Pain — Nociceptive, neuropathic, and “other” (and then some more)
- Vulnerability to Chronic Pain — Chronic pain often has more to do with general biological vulnerabilities than specific tissue problems
What’s new in this article?
41 updates have been logged for this article since publication (2016). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
Oct 16, 2025 — Science update: Some small but important evidence-based improvements to the exercise and weight-loss prescription. [Updated section: What can you do about inflammation and inflammaging?]
Oct 16, 2025 — New section: No notes. Just a new chapter. [Updated section: The role of weight and fat, especially belly fat.]
2025 — New section: No notes. Just a new chapter. [Updated section: Inflammation is just following (neurological) orders.]
2024 — New content: Added a more general summary of the case for exercise being “anti-inflammatory. [Updated section: Hungry, hungry humans balance the energy budget by … cutting inflammation?! The detailed case for exercise as anti-inflammatory medicine.]
2024 — Science update: Updates, clarifications, and additions based on new evidence. [Updated section: What can you do about inflammation and inflammaging?]
2024 — Major upgrade: Added new examples and much more detail, plus a new image. [Updated section: Food additives (and other things we aren’t good at digesting).]
2024 — Upgrade: More detail, added an image. [Updated section: Microplastics … and nanoplastics now, too.]
2024 — Major upgrade: More detailed hazard and risk assessment, much more information about lead, new images, and useful good news about indoor air quality management options. [Updated section: The major environmental pollutants.]
2024 — New section: No notes. Just a new chapter. [Updated section: Mould as a pollutant.]
2024 — Upgraded: Expanded and improved the discussion of surgical meshes, especially acknowledging the degree of controversy and lack of evidence. [Updated section: Surgical implants, especially the meshes.]
2023 — New section: No notes. Just a new chapter. [Updated section: Pass the bag of pain! Junk food as an inflammation driver.]
2023 — Rewritten: Significant revision of all neuroinflammation content. [Updated section: Neuroinflammation — A response to perceived threats?]
2023 — Rewritten: Significant revision of all neuroinslammation content. [Updated section: Neuroinflammation — When neuroinflammation goes wrong (mostly by going long).]
2023 — Rewritten: Significant revision of all neuroinflammation content. [Updated section: Neuroinflammation — Subtler examples?]
Archived updates — All updates, including 27 older updates, are listed on another page. ❐
Notes
- Not many middle-aged people have enough arthritis to account for the sheer number of variety of aches and pains that they often report. Arthritic pain is typically well localized to specific joints, and usually not serious in middle age (unless the joint is vulnerable to early arthritis due to an injury).
- The main ones to watch out for are the bisphosphonates (Alendronate, risedronate, Actonel, Atelvia) and statins (Lipitor, Crestor, Mevacor, Zocor, Lescol). For more information, see 38 Surprising Causes of Pain.
- Gauldie J. Inflammation and the aging process: devil or angel. Nutr Rev. 2007 Dec;65(12 Pt 2):S167–9. PubMed 18240542 ❐
This is a short and technical exploration of reasons not to demonize inflammation. There is some evidence that it might actually be a relatively innocent bystander to the some pathologies it has been blamed for. Otherwise, the article is mainly just a reminder that inflammation is synonymous with immune function and dazzlingly complex, and suppressing it in general is best avoided unless absolutely necessary (which is not wrong, but also so obvious I wonder if it actually needed to be said).
- Hand LE, Hopwood TW, Dickson SH, et al. The circadian clock regulates inflammatory arthritis. FASEB J. 2016 Aug. PubMed 27488122 ❐
- Franceschi C, Campisi J. Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases. J Gerontol A Biol Sci Med Sci. 2014 Jun;69 Suppl 1:S4–9. PubMed 24833586 ❐ PainSci Bibliography 53291 ❐ “Human aging is characterized by a chronic, low-grade inflammation, and this phenomenon has been termed as "inflammaging." Inflammaging is a highly significant risk factor for both morbidity and mortality in elderly people, as most if not all age-related diseases share an inflammatory pathogenesis. Nevertheless, the precise etiology of inflammaging and its potential causal role in contributing to adverse health outcomes remain largely unknown.”
- Mäntyselkä P, Kautiainen H, Vanhala M. Prevalence of neck pain in subjects with metabolic syndrome—a cross-sectional population-based study. BMC Musculoskelet Disord. 2010;11:171. PubMed 20670458 ❐ PainSci Bibliography 53456 ❐ This study found that neck pain is prevalent in people with metabolic syndrome. The relationship is definitely not necessarily causal, but it certainly might be. This evidence certainly suggests a need for more research to find out.
- Hussain SM, Urquhart DM, Wang Y, et al. Fat mass and fat distribution are associated with low back pain intensity and disability: results from a cohort study. Arthritis Res Ther. 2017 Feb;19(1):26. PubMed 28183360 ❐ PainSci Bibliography 52908 ❐
This important paper shows evidence of the metabolic roots of back pain, and perhaps other kinds of chronic pain as well. The majority (82%) of 5000 Australians reported back pain on a questionnaire, and in 27% of them it was bad enough to be disabling. When compared to their fat mass fat distribution — known indicators of metabolic disorders — a clear pattern emerged: back pain intensity and disability go up with measures of fat mass and distribution. This data does not suggest that weight is a “mechanical” problem — greater weight causing greater stress on spinal joints. Instead, it suggests that “systemic metabolic factors associated with adiposity play a major role in the pathogenesis of LBP.” The weight isn’t the problem, but the biochemistry of being out of shape.
This is a particularly excellent example of what I mean when I argue that we need to look beyond trivial physical stresses and biomechanical factors to the messy “wet” factors in chronic pain, the things that make us more vulnerable to pain.
- De Luca P, Grieco G, Bargeri S, et al. The interplay between metabolic disorders and tendinopathies: Systematic review and meta-analysis. J Exp Orthop. 2025 Jul;12(3):e70429. PubMed 40937086 ❐ PainSci Bibliography 49292 ❐
This paper strongly links diabetes, dyslipidemia (high cholesterol), and obesity not just to any kind of “chronic pain” (like Zhu) but specifically to tendinitis — with some extremely high odds ratios, like 6× the risk of Achilles tendinitis and 10× the risk of tennis elbow. The study is a systematic review and meta-analysis pooling 53 observational studies (cohort, case‑control and cross‑sectional), with all the usual caveats (correlation is not causation, but it can be a good hint).
- Two key references for that are Bakshi 2021 and Elma 2023, but I’ll return to this topic in much more detail below.
- Esposito K, Giugliano D. The metabolic syndrome and inflammation: association or causation? Nutr Metab Cardiovasc Dis. 2004 Oct;14(5):228–32. PubMed 15673055 ❐
- Burke NN, Finn DP, McGuire BE, Roche M. Psychological stress in early life as a predisposing factor for the development of chronic pain: Clinical and preclinical evidence and neurobiological mechanisms. J Neurosci Res. 2016 Jul. PubMed 27402412 ❐ “Early-life adversity increases the risk of developing a number of disorders, such as chronic pain, fibromyalgia, and irritable bowel syndrome.”
- Visceral fat — the kind that collects deep around the organs — often gives the abdomen a firm, round, tense appearance. It doesn’t feel soft or floppy because it’s packed internally, pushing the abdominal wall outward like a drum. By contrast, subcutaneous fat (under the skin) is what creates the looser, jiggly flab most people associate with “fatness.” It’s more metabolically benign and distributed in more pliable layers just beneath the skin. The “beer belly” that looks and feels hard is typically visceral fat, and the soft “love handles” and belly roll type fat are mostly subcutaneous. It’s one of those counterintuitive cases where the firmer look is actually the more dangerous one.
- Blüher M. An overview of obesity-related complications: The epidemiological evidence linking body weight and other markers of obesity to adverse health outcomes. Diabetes Obes Metab. 2025 Apr;27 Suppl 2(Suppl 2):3–19. PubMed 40069923 ❐ PainSci Bibliography 49319 ❐
This is one of a couple of key citations on this topic included here. Blüher's paper is a detailed review of the state of obesity science as of 2025, focusing on the biology, and there’s a thorough “translation” of it in the PainSci bibliography. For the full scientific case that “belly fat is painful,” see Vulnerability to Chronic Pain.
- Zhu J, Wang Y, Yu G, et al. Association between metabolic score for visceral fat and chronic pain: a cross-sectional analysis of NHANES 1999-2004. Front Nutr. 2025 May 14;12:1545774. PubMed 40444245 ❐ PainSci Bibliography 49318 ❐
This citation does not fully support that statement — it mainly just confirms that there is a strong association between visceral fat and any kind of chronic pain. However, it’s reasonable in this case to make some strong educated guesses about how that link probably works, and there’s plenty of other relevant evidence pointing the same way.
This is one of a couple of key citations on this topic included here. For the full scientific case that “belly fat is painful,” see Vulnerability to Chronic Pain.
- De Luca P, Grieco G, Bargeri S, et al. The interplay between metabolic disorders and tendinopathies: Systematic review and meta-analysis. J Exp Orthop. 2025 Jul;12(3):e70429. PubMed 40937086 ❐ PainSci Bibliography 49292 ❐
- McCarthy M, Raval AP. The peri-menopause in a woman's life: a systemic inflammatory phase that enables later neurodegenerative disease. J Neuroinflammation. 2020 Oct;17(1):317. PubMed 33097048 ❐ PainSci Bibliography 51940 ❐
- Bennett JM, Glaser R, Malarkey WB, et al. Inflammation and reactivation of latent herpesviruses in older adults. Brain Behav Immun. 2012 Jul;26(5):739–46. PubMed 22155500 ❐ PainSci Bibliography 53327 ❐ “Persistent pathogens such as latent herpesviruses and chronic bacterial infections can act as a source of inflammation. Herpesviruses, including Epstein-Barr virus (EBV) and cytomegalovirus (CMV), establish latent infections following primary infection and reactivate when the cellular immune system is compromised.” In this study of 222 older adults (~64), activity of these two viruses was associated with more inflammatory markers (CRP and IL-6). “Thus, reactivation of multiple herpesviruses may drive inflammation and could contribute to poorer health among older adults.”
- Autoimmune disease is inflammatory by definition, and is extremely unpredictable. Even full-blown autoimmune diseases are notoriously difficult to diagnose, because they tend to erratically affect many systems. It’s likely that some people have minor autoimmune disease, effectively undiagnosable. It’s not even a case of having “early” autoimmune disease: AD is so unpredictable that it might back off before getting severe enough to be diagnosed.
- CBC.ca [Internet]. Quirks & Quarks. Have researchers been wrong about Alzheimer’s? A new theory challenges the old story; 2018 Dec 8 [cited 19 Jun 16]. PainSci Bibliography 52274 ❐ The infamous brain plaques of Alzheimer’s have always been a mystery. Evidence increasingly suggests that they are actually “nets” of a sophisticated infection-fighting strategy, designed to trap a common pathogen — but at a price that gets steeper over the years.
- Microbeminded.com [Internet]. Proal A. Re-evaluating the theory of autoimmunity; 2019 June 6 [cited 19 Jun 19]. PainSci Bibliography 52273 ❐
This is a clear and concise summary of an intriguing and plausible hypothesis: that autoimmune disease is not caused by the body’s immune system “attacking itself,” but by collateral damage when the immune system fights infections with antibodies that also happen to match our own proteins. This may also be the explanation for “inflammaging”: as we accumulate antibodies from infections over the years, we basically start to get mild “autoimmune disease.”
- www.newscientist.com [Internet]. Williams C. How to extinguish the inflammation epidemic; 2017 July 18 [cited 19 Jun 17]. PainSci Bibliography 52866 ❐
This article was really hot for a while. It has superficial credibility, but actually offers just a lot of oversimplified wishful thinking about inflammation as the one true cause of all of our problems, and a few unremarkable treatment suggestions. The author aggressively demonizes stress and “modern living” as the major cause of systematic inflammation (far beyond what the evidence can support), and gives only token attention to the devil in the details.
In particular, she gets carried away with the idea that “inflammation has an off switch,” acknowledging too late that one of her expert sources, Dr. Derek Gilroy, “warns against getting too carried away with the resolvin story.” Dr. Gilroy’s quote (too little, too late) reads like a desperate attempt to undermine the story the author is hell-bent on telling:
“The inflammation that we have in diseases like Alzheimer’s, cancer, autoimmune diseases like osteoarthritis, all of these are very different inflammatory processes,” he says. “It is hard for me to understand, given that there are many ways that a disease occurs, that they can resolve by the same mechanism.”
Despite all of Williams’ optimism, the article coughs up a ridiculous list of five tepid inflammation-fighting recommendations: lose weight, relax, take aspirin in low doses, and — facepalm — stretch (a particularly desperate item, unwisely based on a scrap of evidence from Berrueta et al.). These aren’t completely meritless, but they are blatantly a very weak sauce.
- Dunkman WJ, Rycek W, Manning MW. What Does a Red Meat Allergy Have to Do With Anesthesia? Perioperative Management of Alpha-Gal Syndrome. Anesth Analg. 2019 Nov;129(5):1242–1248. PubMed 29847378 ❐ “There is growing recognition of allergic reactions in these patients to other drugs and medical devices that contain alpha-gal” (Dunkman et al.)
- Zhan M, Yin J, Xu T, Wen L. Alpha-Gal Syndrome: An Underrated Serious Disease and a Potential Future Challenge. Glob Chall. 2024 Jul;8(7):2300331. PubMed 39006061 ❐ PainSci Bibliography 49904 ❐
- Azimi E, Lerner EA, Elmariah SB. Altered manifestations of skin disease at sites affected by neurological deficit. Br J Dermatol. 2015 Apr;172(4):988–93. PubMed 25132518 ❐ PainSci Bibliography 50072 ❐
- Imbeault P, Ravanelli N, Chevrier J. Can POPs be substantially popped out through sweat? Environ Int. 2018 Feb;111:131–132. PubMed 29197670 ❐
- Epsom salt in your bath is cheap and harmless and it makes the water feel “silkier,” but it’s unlikely that it has a therapeutic effect on aches and pains. It definitely doesn’t “detox” anything. Magnesium supplementation might be helpful for some people with deficiency and chronic pain, but it probably can't soak through the skin. The soothing heat of a nice bath is probably the main source of health benefits. The case for the healing powers of Epsom salt is mostly made by people selling the stuff, or recommending it as casually and imprecisely as an old wives’ tale. See Does Epsom Salt Work? The science and mythology of Epsom salt bathing for recovery from muscle pain, soreness, or injury.
- An important basic idea about poisons is the distinction between hazard and risk. "Hazard" is the harm that a substance would cause if you took a shower in it — how inherently nasty is it — while "risk" is the chance that you'll ever actually be exposed to enough of it to get hurt. Another way to put it: it’s the difference between how dangerous something is in theory (hazard) versus practice (risk).
- Shirke AV, Radke EG, Lin C, et al. Expanded Systematic Evidence Map for Hundreds of Per- and Polyfluoroalkyl Substances (PFAS) and Comprehensive PFAS Human Health Dashboard. Environ Health Perspect. 2024 Feb;132(2):26001. PubMed 38319881 ❐ PainSci Bibliography 49865 ❐
This paper is a “systematic evidence map,” a kind of scientific review, of evidence about the health effects of per- and polyfluoroalkyl substances (PFAS), AKA the “forever chemicals.”
They looked for epidemiological and mammalian bioassay evidence that could inform human health hazard identification for 345 PFAS previously flagged by the US EPA for potential toxicity, mainly identified by in vitro toxicity — in other words, PFAs that can murder cells in a petri dish. Despite the large number of candidates studied here, there are still plenty of other PFAs to assess!
They trolled through more than 13,000 studies were identified from scientific databases, whittling the list down to mammalian bioassay and epidemiological studies for just 41 PFAs, only about 10% of the 345 they were looking for data on.
“No epidemiological and/or mammalian bioassay evidence were identified for most of the PFAS included in our search.”
- WHO.int [Internet]. World Health Organization. Lead poisoning; 2023 Aug 11 [cited 24 Aug 14]. PainSci Bibliography 49870 ❐
- WHO.int [Internet]. World Health Organization. The public health impact of chemicals: knowns and unknowns; 2021 [cited 24 Aug 14]. PainSci Bibliography 49871 ❐
- Chowdhury R, Ramond A, O'Keeffe LM, et al. Environmental toxic metal contaminants and risk of cardiovascular disease: systematic review and meta-analysis. BMJ. 2018 Aug;362:k3310. PubMed 30158148 ❐ PainSci Bibliography 49868 ❐
- Gawryluk JR, Palombo DJ, Curran J, Parker A, Carlsten C. Brief diesel exhaust exposure acutely impairs functional brain connectivity in humans: a randomized controlled crossover study. Environ Health. 2023 Jan;22(1):7. PubMed 36641507 ❐ PainSci Bibliography 49863 ❐
Some interesting details and disclaimers:
The precise functional impact of the changes seen in fMRI are unknown but are likely modest given the small magnitude of change, as expected with such limited exposure. That said, real-world exposures are often more persistent, particularly in regions of the world for which levels such as those we use are not uncommon. It is hypothesized that chronic exposure is effectively a series of short-term exposures (only one of which our participants were exposed to) that ultimately leads to accumulated deficits through a stress on allostatic load, but whether or not this applies to pollution in the neurocognitive realm, while hypothesized, requires further study. That being said, our results are consistent with a study of chronic air pollution exposure in Germans.
- Gawryluk et al. elaborate a little, citing Oberdörster et al.’s animal research: “More precise mechanisms have been elusive to date, though a link to neuroinflammation (difficult to measure directly in the intact human), potentially secondary to particle migration via the olfactory bulb as seen in animal models, seems likely.”
- Blackburn K, Green D. The potential effects of microplastics on human health: What is known and what is unknown. Ambio. 2022 Mar;51(3):518–530. PubMed 34185251 ❐ PainSci Bibliography 49860 ❐ Note that this study specifically calls out inflammation (“provoking immune responses”):
“Whilst definitive evidence linking microplastic consumption to human health is currently lacking, results from correlative studies in people exposed to high concentrations of microplastics, model animal and cell culture experiments, suggest that effects of microplastics could include provoking immune and stress responses and inducing reproductive and developmental toxicity.”
- Lazăr NN, Călmuc M, Milea ȘA, Georgescu PL, Iticescu C. Micro and nano plastics in fruits and vegetables: A review. Heliyon. 2024 Mar;10(6):e28291. PubMed 38545146 ❐ PainSci Bibliography 49864 ❐
- Cohen D. How safe are metal-on-metal hip implants? BMJ. 2012;344:e1410. PubMed 22374741 ❐ PainSci Bibliography 53447 ❐
A scholarly analysis of the safety of MoM implants:
Hundreds of thousands of patients around the world may have been exposed to toxic substances after being implanted with poorly regulated and potentially dangerous hip devices, a BMJ/ BBC Newsnight investigation reveals this week. Despite the fact that these risks have been known and well documented for decades, patients have been kept in the dark about their participation in what has effectively been a large uncontrolled experiment.
Cobalt-chromium implants have been used successfully in orthopaedics for years—for example, in knee operations and fracture repair. They are known to release metal ions, but some metal-on-metal prostheses do so on a much greater scale than previously thought. These ions can seep into local tissue causing reactions that destroy muscle and bone and leaving some patients with long term disability.
Harris tells the (chilling) story of metal-on-metal hip implants in Surgery: The ultimate placebo, one of the best-ever (and freshest) examples of surgical overconfidence.
- Sodas, juices, powdered beverages, candies, frozen foods, some dairy products, and most canned produce. Here's a weird one: cheap ice.
- Sweis IE, Cressey BC. Potential role of the common food additive manufactured citric acid in eliciting significant inflammatory reactions contributing to serious disease states: A series of four case reports. Toxicol Rep. 2018;5:808–812. PubMed 30128297 ❐ PainSci Bibliography 52323 ❐
Citric acid is a natural substance in fruits and vegetables, but manufactured citric acid (MCA), a ubiquitous food additive. MCA is made from the fungus Aspergillus niger, which is a known cause of allergies. MCA is “generally recognized as safe” by the FDA despite a complete lack of safety research. This paper present four cases of patients with symptoms of systemic inflammation following ingestion of MCA (most likely related to the fungus used to produce it, and not the citric acid itself). They suspect that the MCA was harming these patients. Their observations do not constitute evidence of a risk, but further study may be warranted.
- Verbeke: >“FODMAPs trigger gastrointestinal symptoms in subjects who are hypersensitive to luminal distention owing to osmotic effects, attracting water to the intestinal lumen, and bacterial fermentation, resulting in (excessive) gas production. As such, the immune system is not involved in symptom generation, and the symptoms should be classified as food intolerance rather than food sensitivity. Although intolerance to fructans and other FODMAPs may contribute to NCGS, they may only explain gastrointestinal symptoms and not the extraintestinal symptoms observed in NCGS patients, such as neurologic dysfunction, psychological disturbances, fibromyalgia, and skin rash. Therefore, it is unlikely that they are the sole cause of NCGS.”
- Matthews SB, Waud JP, Roberts AG, Campbell AK. Systemic lactose intolerance: a new perspective on an old problem. Postgrad Med J. 2005 Mar;81(953):167–73. PubMed 15749792 ❐ PainSci Bibliography 49866 ❐
- Kelly SM, Shorthouse M, Cotterell JC, et al. A 3-month, double-blind, controlled trial of feeding with sucrose polyester in human volunteers. Br J Nutr. 1998 Jul;80(1):41–9. PubMed 9797642 ❐
- Spencer M, Gupta A, Dam LV, et al. Artificial Sweeteners: A Systematic Review and Primer for Gastroenterologists. J Neurogastroenterol Motil. 2016 Apr;22(2):168–80. PubMed 26932837 ❐ PainSci Bibliography 51289 ❐ “The 2 main areas on which there is data to suggest that artificial sweeteners affect the GI tract include motility and the gut microbiome.
- Walitt B, Katz RS, Bergman MJ, Wolfe F. Three-Quarters of Persons in the US Population Reporting a Clinical Diagnosis of Fibromyalgia Do Not Satisfy Fibromyalgia Criteria: The 2012 National Health Interview Survey. PLoS One. 2016;11(6):e0157235. PubMed 27281286 ❐ PainSci Bibliography 53271 ❐ “The majority of clinically diagnosed fibromyalgia cases in the US do not reach levels of severity necessary and sufficient for diagnosis. The clinical diagnosis of fibromyalgia is disproportionally dependent on demographic and social factors rather than the symptoms themselves. Diagnostic criteria for fibromyalgia appear to be used as a vague guide by clinicians and patients, and allow for substantial diagnostic expansion of fibromyalgia.”
- Bäckryd E, Tanum L, Lind AL, Larsson A, Gordh T. Evidence of both systemic inflammation and neuroinflammation in fibromyalgia patients, as assessed by a multiplex protein panel applied to the cerebrospinal fluid and to plasma. J Pain Res. 2017;10:515–525. PubMed 28424559 ❐ PainSci Bibliography 53589 ❐
Although inflammation has been suspected in fibromyalgia, it has been poorly studied to date. This experiment went much further, employing “a new multiplex protein panel enabling simultaneous analysis of 92 inflammation-related proteins.” They looked for these markers in the cerebrospinal fluid and blood of 40 fibromyalgia patients and compared with healthy controls, finding an “extensive inflammatory profile.”
- In theory, the way to tell the difference would be the absence of other classic fibromyalgia symptoms like poor quality sleep, fatigue, memory and mood issues — the infamous “fibrofog.” In practice, those are common, messy, and overlapping sensations (even more so in people who’ve had a lot of aches and pains for years). The sensations in an inflamed person could strongly resemble those in someone with fibromyalgia.
- Lasselin J, Kemani MK, Kanstrup M, et al. Low-grade inflammation may moderate the effect of behavioral treatment for chronic pain in adults. J Behav Med. 2016 Oct;39(5):916–24. PubMed 27469518 ❐ PainSci Bibliography 53548 ❐
Forty-one patients with chronic pain (at least six months, many much longer) were tested for signs of systemic inflammation. They all had stable medications, and no major complications. Then they were provided with two kinds of behavioural treatments for several weeks, measuring their progress in several ways.
Unfortunately, no one did well: “No substantial overall effect of behavioral treatment on pain intensity and pain-related variables was found in the present study.” So that’s a sad result for these behavioural therapies.
However, there is a scrap of backwards good news here: the patients with more inflammation “were more resistant to the improvement in pain intensity and in psychological variables contributing to pain.” Note that the mechanism of that effect is probably not that inflammation directly makes pain harder to treat, but actually modifies mental state and behaviour and that makes the pain harder to treat.
The authors believe that this data tentatively “suggests that the inflammatory state may be one of the mechanisms of the persisting behavioral alterations in patients who do not respond to treatment, corresponding to previous studies on treatment resistant depression.”
- And all of the stress cousins: anxiety, insomnia, depression, weak social connections, low social status, and so on. When I refer to “stress” here, I’m talking about any and all of the psychological stresses, and psychologically adjacent.
- Thompson T, Correll CU, Gallop K, Vancampfort D, Stubbs B. Is Pain Perception Altered in People With Depression? A Systematic Review and Meta-Analysis of Experimental Pain Research. J Pain. 2016 Dec;17(12):1257–1272. PubMed 27589910 ❐
Although “clinical studies suggest depressed patients may be more vulnerable to pain,” it’s far from proven. It’s not clear, and it still isn’t after this meta-analysis of 32 studies. The only real finding here was that there’s so much variety in the results of studies that “it depends” in a big way, on many variables.
This analysis actually found that in some ways depressed patients were less vulnerable to pain — a “small but significant” higher mean sensory threshold and pain threshold — which is interesting but probably not meaningful, given the complexity of the data.
- Elbinoune I, Amine B, Shyen S, et al. Chronic neck pain and anxiety-depression: prevalence and associated risk factors. Pan Afr Med J. 2016;24:89. PubMed 27642428 ❐ PainSci Bibliography 53545 ❐
- Not exclusively. There are inflammatory mechanisms that have nothing directly to do with immunity. A major example of this is neuroinflammation, discussed further along.
- Lasselin J, Alvarez-Salas E, Grigoleit JS. Well-being and immune response: a multi-system perspective. Curr Opin Pharmacol. 2016 Aug;29:34–41. PubMed 27318753 ❐
- Corticosteroids are potent anti-inflammatory agents (and not the same thing as the anabolic steroids taken by bodybuilders), but their potency also means they have a lot of side effects. Oral steroids can be invaluable for management of severe widespread inflammatory conditions — like rheumatoid arthritis, say — but they are also overkill for almost any painful “hot spot,” because they are a bit of a bull in a biological china shop. And so injection is preferred for its precision wherever it makes sense… though even then there are major caveats (e.g. see Okike).
- More Sapolsky (p. 170):
The next clever thing that viruses have done? They don’t reactivate at any old time. They wait until the immune system of the host organism is lousy, and then gun for some quick rounds of replication. And when are immune systems often at their lousiest? You got it. It’s been endlessly documented that latent viruses like herpes flare up during times of physical or psychological stress in all sorts of species. It’s the same thing with some other viruses that go latent, like Epstein-Barr virus and varicella-zoster (which causes chicken pox and shingles).
Herpes doesn’t measure how your immune system is doing. It measures something else that, for its purposes, gives it the information it needs—it measures your glucocorticoid levels. Herpes DNA contains a stretch that is sensitive to elevated glucocorticoid signals, and when levels are up, that DNA sensor activates the genes involved in coming out of latency. Epstein-Barr and varicella-zoster contain this glucocorticoid-sensitive stretch as well.
And still more Sapolsky (continuing from last note):
And now for something even more fiendishly clever. You know what else herpes can do once it infects your nervous system? It causes your hypothalamus to release CRH which releases ACTH which raises glucocorticoid levels. Unbelievable, huh? So you don’t even need a stressor. Herpes infects you, artificially pushes you to step 2 with your elevated glucocorticoid levels, which gets you to step 3, and allows the virus to come out of latency. Moreover, elevated glucocorticoid levels impair your immune defenses against activated herpes. This leads to step 4—a cold sore flare-up. And we think we’re so clever with our big brains and opposable thumbs.
- Sapolsky RM. Why Zebras Don’t Get Ulcers. 3rd ed. New York: Times Books; 2004. Chapter 8: Immunity, Stress, and Disease; p. 144–185. Sapolsky goes deep on this topic, and I am completely relying on him for this point. I hope I’ve boiled it down to the essentials correctly. His bottom line: “The system apparently did not evolve for dealing with numerous repetitions of coordinating the various on-and-off switches, and ultimately something uncoordinated occurs, increasing the risk that the system becomes autoimmune [inflammatory].”
- Dr. Robert Sapolsky, regarding a study of low-status monkeys (Snyder-Mackler et al.), who have hard lives:
At the end of the day, being a chronically subordinate nonhuman primate and being a human mired at the bottom of the socioeconomic scale are similar in the most fundamental ways. You have remarkably little control and predictability in your life, your outlets for frustration are limited, and it’s relatively hard to access social support. That’s the prescription for chronic, stress-related maladies.
- Burke 2016, op. cit.
- Gohil BC, Rosenblum LA, Coplan JD, Kral JG. Hypothalamic-pituitary-adrenal axis function and the metabolic syndrome X of obesity. CNS Spectr. 2001 Jul;6(7):581–6, 589. PubMed 15573024 ❐ Prolonged chronic stress can probably contribute to metabolic syndrome by messing with the hormonal balance of the hypothalamic-pituitary-adrenal axis (HPA-axis).
- Koren D, Dumin M, Gozal D. Role of sleep quality in the metabolic syndrome. Diabetes Metab Syndr Obes. 2016;9:281–310. PubMed 27601926 ❐ PainSci Bibliography 53564 ❐
- Carroll JE, Cole SW, Seeman TE, et al. Partial sleep deprivation activates the DNA damage response (DDR) and the senescence-associated secretory phenotype (SASP) in aged adult humans. Brain Behav Immun. 2016 Jan;51:223–9. PubMed 26336034 ❐ PainSci Bibliography 53312 ❐ “Age-related disease risk has been linked to short sleep duration and sleep disturbances…”
- Bower JE, Irwin MR. Mind-body therapies and control of inflammatory biology: A descriptive review. Brain Behav Immun. 2016 Jan;51:1–11. PubMed 26116436 ❐ PainSci Bibliography 53640 ❐
This is a qualitative review of 26 randomized controlled trials of the biological effects of mind-body therapies like Tai Chi, Qigong, yoga, and meditation. The studies show “mixed effects” on inflammation (CRP, IL-6, stimulated cytokine production, etc), and more consistent results for “genomic markers.” Based on this evidence, it seems likely that these activities are meaningfully good for you, and probably helpful for some kinds of chronic pain.
- Something I was surprised to learn at some point many years ago. Almost all the infections I have ever had have begun with that nasty aching. It’s like a biological tradition for me, as predictable as Old Faithful, or Elon Musk screwing up Twitter in strange new ways. It is roughly proportionate to the overall severity of the infection.
- I didn't have a single infection during the pandemic proper. When I finally got Covid, it had been four years since my last chance to compare infection aches to my every day pain … and I was amazed all over again by the strength of the resemblance. My acute Covid infection aches were *qualitatively identical* to my chronic pain. The Covid version was definitely stronger … but not by all that much. They really felt like the same thing.
- Lyon P, Cohen M, Quintner J. An evolutionary stress-response hypothesis for chronic widespread pain (fibromyalgia syndrome). Pain Med. 2011 Aug;12(8):1167–78. PubMed 21692974 ❐ This paper explores a striking similarity between fibromyalgia and “sickness behaviour” in animals.
- Ji RR, Nackley A, Huh Y, Terrando N, Maixner W. Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology. 2018 08;129(2):343–366. PubMed 29462012 ❐ PainSci Bibliography 52332 ❐
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023 Mar;21(3):133–146. PubMed 36639608 ❐ PainSci Bibliography 51215 ❐ One of the major outstanding mysteries is whether it’s truly “dysregulation” — excessive and unnecessary — or whether there’s actually still a good reason for the neuroinflammation, such as viral persistence, or even just subtle but extensive damage. Maybe people with Long Covid still feel sick because they are still sick.
- Albrecht DS, Forsberg A, Sandström A, et al. Brain glial activation in fibromyalgia - A multi-site positron emission tomography investigation. Brain Behav Immun. 2019 Jan;75:72–83. PubMed 30223011 ❐ PainSci Bibliography 52325 ❐
- Sapolsky RM. Why Zebras Don’t Get Ulcers. 3rd ed. New York: Times Books; 2004.
- Andersen SL. Neuroinflammation, Early-Life Adversity, and Brain Development. Harv Rev Psychiatry. 2022;30(1):24–39. PubMed 34995033 ❐ PainSci Bibliography 51630 ❐
- Coppens E, Van Wambeke P, Morlion B, et al. Prevalence and impact of childhood adversities and post-traumatic stress disorder in women with fibromyalgia and chronic widespread pain. Eur J Pain. 2017 May. PubMed 28543929 ❐
- Lee DH, Lee JY, Hong DY, et al. Neuroinflammation in Post-Traumatic Stress Disorder. Biomedicines. 2022 Apr;10(5). PubMed 35625690 ❐ PainSci Bibliography 51625 ❐
- Woodburn SC, Bollinger JL, Wohleb ES. The semantics of microglia activation: neuroinflammation, homeostasis, and stress. J Neuroinflammation. 2021 Nov;18(1):258. PubMed 34742308 ❐ PainSci Bibliography 52006 ❐
True, full-blown neuroinflammation is defined by some well-known physiological characteristics, and it is unlikely to occur with anything short of extreme psychological stress, if at all. Even if stress can provoke partial neuroinflammation or something similar-but-different, it might be a bit ridiculous to call it “neuroinflammation,” in the same way that rusting metal is technically “combusting” but it is not “on fire.” No stress that most people will ever deal with is likely to cause the same degree (and maybe not the same kind either) of total immune system freakout that we see in people who are nearly killed by injury or illness. Woodburn et al.:
When I first read this paper, I realized I had gone too far promoting the role of stress as a driver of neuroinflammation, and I wrote a really silly blog post about my mistake. It’s silly but also substantive and worthwhile if you want to learn more about this.“Preclinical research demonstrates that neuro-immune responses to stress are distinct from CNS disease, injury, or infection and should not be characterized as neuroinflammation.”
![Photo of a set of indoor stairs. Each stair is labelled with a cumulative calorie-count in half calories increments: 0.5 calories, 1.0 calories, 1.5 calories, up to 6.5 at the top of the photo.]()
The calorie-counting stairs (click to zoom). Stairs are the most ubiquitous, accessible “gym equipment” in the world
It has been said that exercise is the closest thing there is to a miracle cure. “All the evidence suggests small amounts of regular exercise (five times a week for 30 minutes each time for adults) brings dramatic benefits,” we “age well” when we are active (Gopinath): less anxiety (Schuch), prevention of dementia (Smith) and a laundry list of other diseases (Pedersen), and as little as just 10 minutes per week might push back death itself (Zhao). It’s also superb for sleep quality (Giannaki). It may even be good medicine for musculoskeletal injuries (more info).
But why is it so awesome? Exertion mobilizes extensive networks of biological resources that are relatively dormant while we’re watching Netflix. It’s biologically “normalizing,” pushing systems to work the way they are supposed to work. Exercise cannot normalize everything, but it does stimulate an incredibly broad spectrum of biological function — way more than any medicine, supplement, or superfood.
- Klasson CL, Sadhir S, Pontzer H. Daily physical activity is negatively associated with thyroid hormone levels, inflammation, and immune system markers among men and women in the NHANES dataset. PLoS One. 2022;17(7):e0270221. PubMed 35793317 ❐ PainSci Bibliography 51450 ❐ More on this important study later.
- Research shows strength training is a much more efficient form of exercise than most people realize, and almost any amount of it is much better than nothing. You can gain strength and all its health benefits fairly easily. For more information, see Strength Training Frequency: Less is more than enough: go to the gym less frequently but still gain strength fast enough for anyone but a bodybuilder.
- Pedersen BK. The anti-inflammatory effect of exercise: its role in diabetes and cardiovascular disease control. Essays Biochem. 2006;42:105–17. PubMed 17144883 ❐
This paper is one of dozens by exercise physiologist Dr. Bente K. Pedersen, who has studied exercise as medicine for non-communicable disease for thirty years, and especially “the myokine concept.” This explores the early (mid-2000s) evidence for the hypothesis that “skeletal muscle is a endocrine organ with the capacity to produce so called ‘myokines,’ i.e. cytokines and other peptides that are produced, expressed, and released by muscle fibers and exert either autocrine, paracrine or endocrine effects” (as summarized here), and those molecules mediate "beneficial health effects against chronic diseases associated with low-grade inflammation such as diabetes and cardiovascular diseases.”
That hypothesis has generally been confirmed over years. For Dr. Pedersen’s 2023 update (concise and readable), see “From the discovery of myokines to exercise as medicine.”
- Bakker EA, Lee DC, Sui X, et al. Association of Resistance Exercise, Independent of and Combined With Aerobic Exercise, With the Incidence of Metabolic Syndrome. Mayo Clin Proc. 2017 Aug;92(8):1214–1222. PubMed 28622914 ❐ PainSci Bibliography 52977 ❐ “Participating in resistance exercise, even less than 1 hour per week, was associated with a lower risk of development of metabolic syndrome, independent of aerobic exercise. Health professionals should recommend that patients perform resistance exercise along with aerobic exercise to reduce metabolic syndrome.”
- Liu Y, Chu JMT, Yan T, et al. Short-term resistance exercise inhibits neuroinflammation and attenuates neuropathological changes in 3xTg Alzheimer's disease mice. Journal of neuroinflammation. 2020 01;17(1):4––4. PubMed 31900170 ❐ PainSci Bibliography 52495 ❐
Lifting weights: good for Alzheimer’s? Good chance. This study clearly showed a neuroprotective effect from resistance training in mice. Compared to mice who were not given cute little barbells! Specifically, they found:
“improved cognitive performance and reduced neuropathological and neuroinflammatory changes in the frontal cortex and hippocampus of mice… [and] inhibition of pro-inflammatory intracellular pathways.”
Obviously a human study would be more persuasive (always), but it’s still early days for studying neuroinflammation. Lots of what we now know about exercise physiology we learned from mice initially. It’s likely (or at least highly plausible) that the effect will be confirmed in humans as well, despite the fact that “mice lie and monkeys exaggerate” in research.
It has been clear for many years now that exercise in general is neuroprotective — that is, it has an anti-inflammatory effect in the brain and slows down Alzheimer’s disease progression — but that insight mostly comes from studies of aerobic exercise. This study extends that effect to resistance training, which is why the conclusion isn't much of a reach: we already know that another kind of exercise does this, and we already know that resistance training is an excellent way to exercise.
And now, just for fun… how exactly do you strength train mice? A ladder with a treat at the top, and teensy weights attached to their tails! I am not even joking: that really is how they did this. “The mice were motivated to climb up the ladder to a total of 15 times, with progressively heavier weights attached to their tails and a 2-minute rest in between each climb.” Sounds like more fun than my gym visits.
- Wewege MA, Desai I, Honey C, et al. The Effect of Resistance Training in Healthy Adults on Body Fat Percentage, Fat Mass and Visceral Fat: A Systematic Review and Meta-Analysis. Sports Med. 2022 Feb;52(2):287–300. PubMed 34536199 ❐
This review of 58 decent trials — actually not “garbage in, garbage out” for once, because there’s a lot of research on this topic — concluded that muscle growth is indeed an effective “fat-burning workout.” It actually reduces BFP — including and even especially visceral fat.
- Bliddal H, Bays H, Czernichow S, et al. Once-Weekly Semaglutide in Persons with Obesity and Knee Osteoarthritis. N Engl J Med. 2024 Oct;391(17):1573–1583. PubMed 39476339 ❐
This trial of Ozempic (semaglutide) versus placebo for knee arthritis showed a clinically meaningful difference in weight loss and pain reduction in hundreds of subjects over more than a year, with minimal side effects. The results are good enough to raise the concern that they are too good to be true, and the study was funded by Ozempic manufacturer Novo Nordisk. However, the design was rigorous and provides good protection against bias, there are no major flaws, and the results are also consistent with a substantial and rapidly growing body of evidence of mechanistically predictable benefits.
Blinding may have been compromised in the semaglutide group, because people tend to notice when they lose ~14% of their body weight. Ironically, the more the objective weight-reduction, the higher the risk of biasing the pain-reduction results! The obvious weight loss caused by semaglutide, the higher the risk that the reported pain relief reflects patient expectations rather than a purely biological benefit. But this is far from a fatal flaw. There might not have been any inflation, or not much, and the results are impressive enough that some uncertainty is hardly a deal-breaker. A legitimate effect on pain is highly plausible and even predictable given substantial weight loss, however it is achieved, and the weight-loss result is not in doubt here.
Although this study was not designed to confirm that those benefits is metabolic in nature (rather than biomechanical load reduction), it is plausible and likely. For instance, we know from a huge 2025 observational study (Xie et al.) that literally dozens of conditions are helped (while problems are relatively rare and minor).
For much more detailed analysis of this paper, see “Ozempic works for arthritis, and probably other pain (Member Post).”
For broader scientific context on the relationship between pain and obesity, especially visceral fat, see “Belly fat and chronic pain: the waistline plot thickens.”
- Killer SC, Blannin AK, Jeukendrup AE. No evidence of dehydration with moderate daily coffee intake: a counterbalanced cross-over study in a free-living population. PLoS One. 2014;9(1):e84154. PubMed 24416202 ❐ PainSci Bibliography 53892 ❐ “These data suggest that coffee, when consumed in moderation by caffeine habituated males provides similar hydrating qualities to water.”
- Lasselin, J. Low-grade inflammation and the brain. www.bodyinmind.org. Accessed 2016-12-08.
- Pavlov VA, Tracey KJ. The vagus nerve and the inflammatory reflex—linking immunity and metabolism. Nat Rev Endocrinol. 2012 Dec;8(12):743–54. PubMed 23169440 ❐ PainSci Bibliography 52724 ❐ This paper discusses the role of the inflammatory reflex in obesity specifically, but frequently mentions the potential relevance to other conditions associated with chronic inflammation. The paper is all about “the intriguing possibility that dysregulation of vagus nerve-mediated signalling might contribute to the pathogenesis of obesity and its related comorbidities.”
- Koopman FA, Chavan SS, Miljko S, et al. Vagus nerve stimulation inhibits cytokine production and attenuates disease severity in rheumatoid arthritis. Proc Natl Acad Sci U S A. 2016 Jul;113(29):8284–9. PubMed 27382171 ❐ PainSci Bibliography 53670 ❐
- All kinds of data hijinks could be hiding in a study that technical. My main concern is the use of the word “significantly” in the abstract, without any details (effect size in particular). All too often that wording, without clarification, means there was a statistically significant but clinically trivial result. With many treatment trials I can go digging for the effect size to confirm, but not here, the reading is too difficult for me to form any meaningful impression without spending an hour, and even then it might not be clear. And even if the paper does indicate a clinically meaningful result it’s still got “too good to be true” written all over it and may well prove to be difficult to reproduce.
- Atkins started in 1989, if you can believe that — practically ancient history now — though it didn’t achieve fad-diet status until the mid 2000s.
- Kossoff EH, Zupec-Kania BA, Rho JM. Ketogenic diets: an update for child neurologists. J Child Neurol. 2009 Aug;24(8):979–88. PubMed 19535814 ❐
- There are two main kinds of pain: nociceptive and neuropathic, or the more familiar pain of tissue damage and the more exotic pain caused by a damaged nervous system. Some pain isn’t easy to classify (fibromyalgia). For more information, see The 3 Basic Types of Pain: Nociceptive, neuropathic, and “other” (and then some more).
- Masino SA, Ruskin DN. Ketogenic diets and pain. J Child Neurol. 2013 Aug;28(8):993–1001. PubMed 23680946 ❐ PainSci Bibliography 53476 ❐
ABSTRACT
Ketogenic diets are well established as a successful anticonvulsant therapy. Based on overlap between mechanisms postulated to underlie pain and inflammation, and mechanisms postulated to underlie therapeutic effects of ketogenic diets, recent studies have explored the ability for ketogenic diets to reduce pain. Here we review clinical and basic research thus far exploring the impact of a ketogenic diet on thermal pain, inflammation, and neuropathic pain.
- Leung MTY, Turner JP, Marquina C, et al. Gabapentinoids and Risk of Hip Fracture. JAMA Netw Open. 2024;7(11):e2444488. PubMed 39535796 ❐ PainSci Bibliography 50057 ❐
Leung et al. looked at data on about twenty-eight thousand older Australians with hip fractures between 2013 and 2018, whittling that down to 2600 who had consumed at least one prescription for a gabapentinoid (mostly pregabalin), and another thirteen thousand that didn’t as controls. They also studied two other major known risks for hip fracture, kidney disease (30% of the subjects) and general frailty (45%).
The main finding was that gabapentinoids are quite powerfully linked to a risk of hip fracture, via the mechanism of dizziness causing a risk of falling:
- 30% more breaks even in the healthiest subjects (1.3×)
- 75% more in the frail (1.75×)
- 140% with kidney disease! (2.4×)
Those are shocking numbers. That’s a lot of serious harm for a class of drugs that is notoriously over-prescribed for many types of pain that they mostly cannot help. I discuss this in much more detail in a blog post.
This experiment had a lot of self-control. That is, subjects acted as their own controls in multiple ways: a fancy “case-case-time-control” design that compared subjects to themselves at different times (“case-crossover”), but also to other patients across time (“case-time-control”). It’s too nerdy a design even for the salamander to ramble on about! It was fancy and interesting, and that’s enough said here (but try your luck with a good technical description).
That design means that the results probably weren’t a statistical illusion. But there were some limitations (as always): reliance on prescription data rather than actual drug use, and frailty assessments based on hospital data rather than direct clinical evaluation.
- If fasting really does have general health benefits, there are all kinds of metabolic pathways to that happy ending, but it’s extremely likely there’s an anti-inflammatory effect in there somewhere. It’s the most likely specific example of how it would work as a broad metabolic tonic. While it’s conceivable that fasting could be good for us without an inflammatory effect, it’s unlikely.
- de Cabo R, Mattson MP. Effects of Intermittent Fasting on Health, Aging, and Disease. N Engl J Med. 2019 12;381(26):2541–2551. PubMed 31881139 ❐
- Two are underpowered studies that damn with faint praise; two are (sigh) actually a bit negative, true citation backfires. Tch tch: the NEJM authors didn’t read the fine print in what they were citing! So it’s truly a poor selection of citations to support the assertion that “fasting is anti-inflammatory.”
- Jordan S, Tung N, Casanova-Acebes M, et al. Dietary Intake Regulates the Circulating Inflammatory Monocyte Pool. Cell. 2019 Aug;178(5):1102–1114.e17. PubMed 31442403 ❐
- Anything good for your general health has the potential to help chronic pain. The specific cause of chronic pain may often be less important than general sensitivity and biological vulnerability to any pain. The biggest risk factors for pain chronicity are things like insomnia, obesity, smoking, drinking… and they overshadow common scapegoats like poor posture, spinal degeneration, or even repetitive strain injury. How can nothing in particular make us hurt? Because pain is weird, a generally oversensitive alarm system that can produce false alarms even at the best of times, and probably more of them when your system is under strain. See Vulnerability to Chronic Pain: Chronic pain often has more to do with general biological vulnerabilities than specific tissue problems.
- Elma Ö, Tümkaya Yılmaz S, Nijs J, et al. Proinflammatory Dietary Intake Relates to Pain Sensitivity in Chronic Nonspecific Low Back Pain: A Case-Control Study. J Pain. 2023 Aug. PubMed 37659446 ❐
- This result is a bit puzzling to me, since no food has ever actually been demonstrated to be significantly anti-inflammatory, nothing that you can eat that’s like popping an ibuprofen (either in the short term or the long term). I’d already be eating any such food! My guess is that this finding is there just because junk food eaters do not tend to go for those foods — and that’s a great example of a research artifact.
- Rahm Bakshi, Brooke Stansel, Larissa Strath, et al. Dietary Cholesterol is Associated with Increased Pain Sensitivity in Individuals with Chronic Low Back Pain. The Journal of Pain. 2021;22(5):588. PainSci Bibliography 51634 ❐
- The famous rule — “correlation does not imply causation” — is an important idea, but also a misleading oversimplification. At the very least it’s missing a word, and it should be “correlation does not necessarily imply causation.” Or you could just rephrase it entirely. Edward Tufte, an American statistician who made the same point quite a while ago, suggested that a good informal re-wording would be, “Correlation is not causation but it sure is a hint.” Because correlation actually does “imply” causation, and many (if not most) events that occur in sequence that appear to be causally related are in fact causally related. Their correlation is not a coincidence. Clapping makes noise, braking stops cars, hot coals burn fingers.
- Davis B, Liu YH, Stampley J, et al. The Association between Poor Diet Quality, Physical Fatigability and Physical Function in the Oldest-Old from the Geisinger Rural Aging Study. Geriatrics (Basel). 2021 Apr;6(2):41. PubMed 33920900 ❐ PainSci Bibliography 49872 ❐
- Azzolino D, Arosio B, Marzetti E, Calvani R, Cesari M. Nutritional Status as a Mediator of Fatigue and Its Underlying Mechanisms in Older People. Nutrients. 2020 Feb;12(2):444. PubMed 32050677 ❐ PainSci Bibliography 49873 ❐
- Ultraprocessed foods may be extra “proinflammatory” (Asensi), and they are probably linked to depression and anxiety (Hecht), and even cognitive decline (Bhave) — though it’s still not clear that they are causally linked. (The UPFs are also a magnet for profitable fear-mongering, and they may well be guilty only by association with the many other health headwinds in people who live on instant noodles.)
- Crane JD, Ogborn DI, Cupido C, et al. Massage therapy attenuates inflammatory signaling after exercise-induced muscle damage. Sci Transl Med. 2012 Feb;4(119):119ra13. PubMed 22301554 ❐
- Seo BR, Payne CJ, McNamara SL, et al. Skeletal muscle regeneration with robotic actuation-mediated clearance of neutrophils. Sci Transl Med. 2021 Oct;13(614):eabe8868. PubMed 34613813 ❐
- Zwaag J, Naaktgeboren R, van Herwaarden AE, Pickkers P, Kox M. The Effects of Cold Exposure Training and a Breathing Exercise on the Inflammatory Response in Humans: A Pilot Study. Psychosom Med. 2022 May;84(4):457–467. PubMed 35213875 ❐ PainSci Bibliography 52067 ❐
- Pontzer H, Yamada Y, Sagayama H, et al. Daily energy expenditure through the human life course. Science. 2021 08;373(6556):808–812. PubMed 34385400 ❐ PainSci Bibliography 51994 ❐
- Klasson 2022, op. cit.
- Pedersen BK. The anti-inflammatory effect of exercise: its role in diabetes and cardiovascular disease control. Essays Biochem. 2006;42:105–17. PubMed 17144883 ❐
- Zhang M, Liang Z, Tian L, et al. Effects of exercise therapy in axial spondyloarthritis: A systematic review, meta-analysis and meta-regression of randomized trials. Arch Phys Med Rehabil. 2024 Jun:S0003–9993(24)01065–7. PubMed 38942347 ❐
This is an encouraging scientific review of exercise for axial spondyloarthritis — inflammatory pathology of the spine. This is a whole category of related rheumatic diseases, but it’s mostly about inflammatory back pain and ankylosing spondylitis.
Zhang et al. reviewed twenty randomized controlled trials of exercise therapy for spondyloarthritis, including 1700 patients, looking at many different outcomes: four different scoring systems, oxygen consumption and chest expansion (because spondyloarthritis often affects the ribcage), two major biomarkers (C-reactive protein and erythrocyte sedimentation rate), and, last but not least, the two most consistent symptoms of inflammation: pain and fatigue.
That’s ten outcomes, and seven of them improved, most of them quite a bit. That’s a fantastic result! Leading to this unstintingly positive conclusion:
“Exercise therapy is an effective strategy for improving disease control and symptom relief in axial spondyloarthritis.”
So what didn’t improve? The two biomarkers for inflammation, and “chest expansion.” CRP and ESR are rather blunt instruments, and it’s possible that they could not detect clinically significant changes in inflammation in the short term.
I explore the broader implications of this paper, and of the missing biomarker improvement, in a blog post: STUDY: Exercise eases inflammatory back pain—but why?.

{kind=link}