The Complete Guide to Low Back Pain
An extremely detailed guide to the myths, controversies, and treatment options for low back pain

We can put a man on the moon, but back pain is just as miserable as ever, and more costly to society than ever. Most information available online is awful.1 There are no miracle cures or back whisperers. Not one popular treatment has ever been shown to work well.2 When we are “shot by the witch,”3 it’s going to run its course like a head cold or a headache in most cases, drag on much longer in a few … and there’s just not much anyone can do about it.
There is room for improvement, however! We could, at least, not add insult to injury with largely pointless and expensive testing, therapies and exercises, surgeries, and countless “hacks” that are almost entirely meant to find and fix biomechanical problems that are mostly not there — or they are there, but they are not the real problem.
Despite overwhelming scientific evidence to the contrary, it is still sadly routine for back pain to be seen as a “mechanical” problem, as if the spine is a fragile structure which breaks down.4 There is some truth in that old way of looking at it, but there are many other factors in back pain. It’s hard to treat because “it’s complicated.” Like cancer, back pain is not one disease, but a large family of disorders, many of them cryptic.
Has nobody noticed the embarrassing fact that science is about to clone a human being, but it still can’t cure the pain of a bad back?
Pain, by Marni Jackson, p. 5
A tragic low back pain myth
This pervasive myth of spinal fragility has many unfortunate consequences, such as unnecessary fusion surgeries — a common and routinely ineffective procedure — and low back pain that lasts for years instead of months or weeks. The seriousness of chronic low back pain is often emphasized in terms of the hair-raising economic costs of work absenteeism, but it may well be far worse than that — a recent Swedish study shows that it probably even shortens lives.5 The stakes are high. “Tragedy” is not hyperbole.
Even worse is that good information exists: many medical experts do “get it,” but they have fought a long, losing battle trying to spread the word to their own medical colleagues on the front lines of health care.6 Back pain treatment in the real world is notoriously out of step with guidelines and best practices,7 and the average family doctor is just not educated enough.8
And as if that wasn’t bad enough, doctors who are more interested in back pain are even worse,9 probably because “a little knowledge is a dangerous thing.” Similarly, experts have failed to get the word to alternative health professionals — most of whom don’t even read medical journals.10
In this tutorial, you will meet those experts and find out what they know and believe and why. Their ideas about low back pain are neither “conventional” nor “alternative” — they simply come from the best minds in the business.
The evidence that tissue pathology does not explain chronic pain is overwhelming (e.g., in back pain, neck pain, and knee osteoarthritis).
Lorimer Moseley, “Teaching people about pain — why do we keep beating around the bush?” Pain Management. 2012.
How do so many health care professionals go wrong when they treat low back pain?
Why does the myth of mechanical back pain, the premise for so much ineffective treatment, get repeated endlessly on the Internet and in health care offices around the world? (All of these points above will be explained and substantiated in detail further along — these are just the highlights.)
- Repairing spinal joint “misalignment” is an easy idea to sell, but it’s hard to actually do. Chiropractors often can’t even agree on which joints need “adjusting” — even with only five lumbar joints to choose from.
- Poor posture and crookedness is another popular scapegoat — it seems obvious that posture is relevant. Many professionals assume that back pain is some kind of postural problem that you can exercise your way clear of. Unfortunately, the evidence shows that no kind of exercise, not even the most hardcore of core strengthening, has any significant effect on chronic low back pain. Although exercise is still a great idea for back pain patients for other reasons, it’s not medicine for most back pain.
- The almost magical power of MRI to look inside the back gives both doctors and patients something to point at and blame, but most are unaware that MRI has been proven (many times) to be a lousy diagnostic tool for back pain. The things you see on MRI scans are rarely the real problem — and every radiologist seems to see something different!
- Orthopedic surgeons (especially American ones) profit handsomely from the most complex low back surgeries (especially spinal fusion), so they are strongly inclined to think of back pain as a mechanical problem in need of physical repair — in spite of piles of scientific evidence to the contrary. This is the best example of how “entire professions appear to depend on the problem remaining unsolved.”11 If all you have is an incredibly profitable hammer …
- Sports medicine specialists have great expertise about injuries, so they often assume that back pain involves some kind of damage — but the evidence clearly shows that low back pain often has nothing to do with tissue damage.
- Patient education is important, and yet it rarely happens, because the topic is just too tricky — many professionals don’t have enough knowledge to pass on a useful amount of it. And so education is “always first line but never headline,”12 a systemic weakness in back pain care.
- Overconfidence based on a lack of personal experience with back pain.13
- The power of the mind over back pain has been badly over-hyped by some experts (ironically as a well-intentioned backlash against some of the ideas above). Nowhere is this more glaring than in Dr. John Sarno’s famous books,14 which has convinced countless patients and pros that low back pain is entirely a mind game … and that’s just going too far.
Plus, of course, there are an almost unbelievable number of sketchier treatments for sale, easily marketed to desperate souls. Is low back pain treatment really this much of a mess? Sadly, I believe so.15 I clearly remember graduating clueless myself. If I hadn’t spent many years doing post-grad study of low back pain, I wouldn’t know 98% of what’s in this tutorial.

Over-rated?
Yes, stress is one factor in low back pain … but meditation, yoga, relaxation, and other mind-body treatments are over-rated and inappropriate for many people. This guide does not deny the role of the mind, and explores it thoroughly — but the focus is on more practical options.
The journey to relief begins with better back beliefs (but it doesn't end that way)
These are the most important upgrades to beliefs about backs:
- Treatments such as strong medications, injections, and surgery are not effective or necessary in the overwhelming majority of cases.
- Low back pain is rarely a serious medical condition, rarely persists, and rarely deteriorates later in life. Even when it does persist, much of it isn’t related to tissue damage and arthritic degeneration, and scans are rarely helpful in diagnosing the cause of back pain.
- Pain with exercise and movement is mostly not a useful warning that harm is being done to the spine. Even intense exercise doesn’t cause “wear and tear” damage, and flare-ups don’t mean you’ve damaged something and have to rest.
- Low back pain is not caused by weak “core” muscles or prevented by strong ones.
Each of these contradicts a major myth or two about back pain, and is strongly supported by the science.16 By the end of this tutorial, I hope you’re convinced of each one. But initially? Most people will have trouble swallowing them. Even professionals will — especially the ones whose income depends on denying these.
Embracing them, instead of the myth of fragility and all its implications, is half the battle. But it’s really tough when you’re facing intense, chronic back pain. Sure, most acute low back pain fades steadily — up to 90% of it, for uncomplicated cases.17 And so does a lot of so-called “chronic” low back pain!18
But not all. This tutorial is mainly for patients with unusually stubborn low back pain and sciatica, and for the doctors and therapists who want to help. (It’s overkill for new and acute cases.) Even for these really entrenched cases, there is hope…

An excellent “back facts” infographic from O’Sullivan et al. Examples: getting older is not a cause of back pain, poor posture does not cause back pain, and scans rarely show the cause.
Click to embiggen.
The case for hope: some “incurable” chronic low back pain can still be cured
While it’s true that most chronic lower back pain will not yield to any popular back pain treatment, it’s also true that some really stubborn “incurable” cases do eventually turn out to be curable. People who believed for years that their pain was invincible have still found relief. Not always, and often not completely — but sometimes any relief is far better than nothing. How can extremely stubborn pain finally ease up? Simple: because many cases weren’t truly stubborn to begin with, despite all appearances. So many health professionals are poorly prepared to treat low back pain that
And it’s always amazing to me how chronic pain can, with the right approach, finally melt away — it’s not common, but it does happen. Lots of people who thought they’d “tried everything” for lower back pain read this tutorial and then write to me and say, “Well, I guess I hadn’t tried everything!”
Similarly, many athletes with “career-ending” injuries are far from finished. Bret “The Glute Guy” Contreras, from You’ll Never Squat Again:
Numerous powerlifters over the years have come back following ‘career-ending injuries’ to set all-time personal records. Donnie Thompson is the only man to total 3,000 lbs (1,265 lb squat, 950 lb bench, 785 lb deadlift). Many people don’t know this, but several years back Donnie suffered a horrendous back injury and herniated three discs. He could barely walk, but he got out of bed and rehabbed himself every day. Within three months he was back to heavy squatting and setting personal records. Got that? Setting personal records three months following an injury that herniated 3 discs!
How could that be? It’s almost like herniated discs aren’t necessarily as scary as everyone seems to think. Hm!
I have never met a patient — no matter how experienced or self-educated — who could not gain at least some new insights and new hope from this tutorial.19
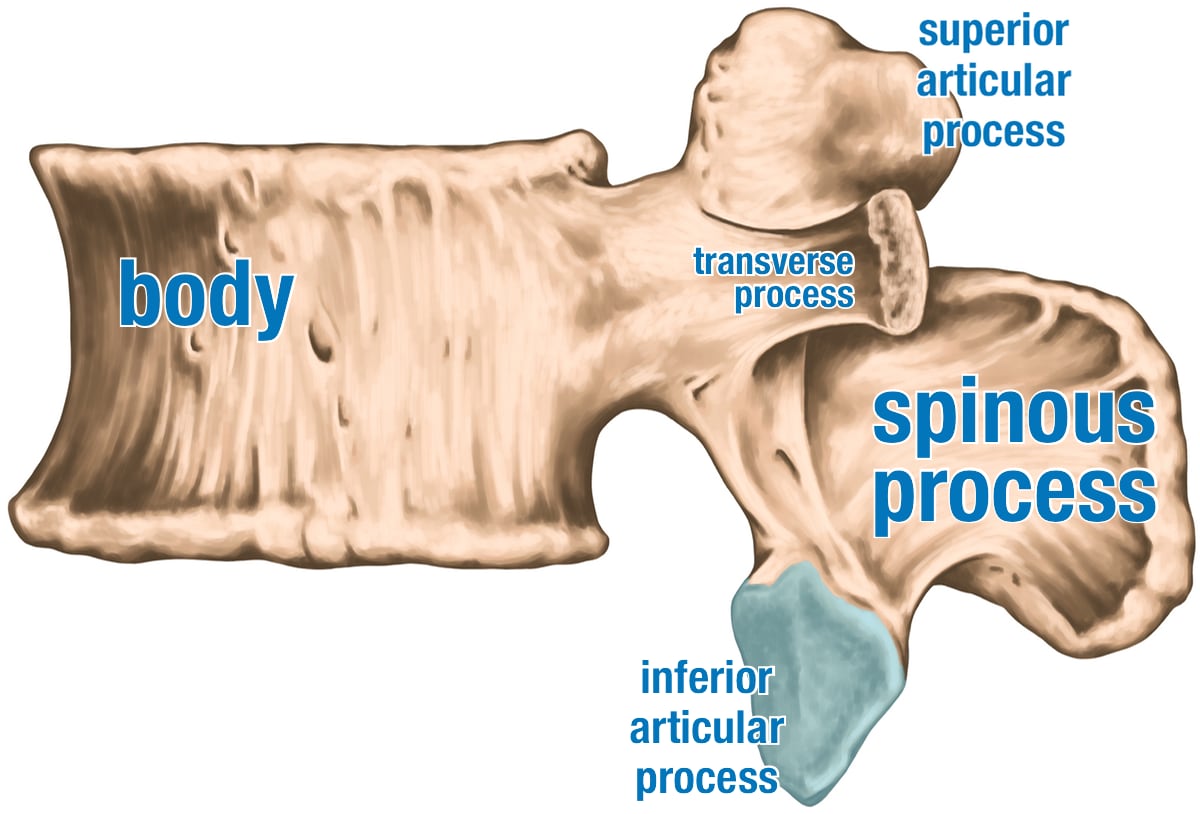
A lumbar vertebra
Vertebrae are the scaffolding of the back. A lot of back pain doesn’t have much to do with spinal structure, especially the bones themselves, but you do need to know a little about the anatomy to properly wrap your head around the subject.
“What if there’s something seriously wrong in there?”
“How do you know I’m not seriously hurt?”
“Could it be cancer? A tumor?”
You’re not paranoid if they really are after you! Only about 1% of back pain has a nasty cause,20 and only a few of those are really scary. But it happens. Andy Whitfield, star of Spartacus, thought he just had back pain from his intense gladiatorial training. In fact, he had a tumour. It killed him in 2011.
The most dangerous thing about trying to reassure low back pain patients is the unnerving possibility that I might reassure someone who should not be. But reassurance is almost always appropriate. Most back injury feels worse than it is — its bark is worse than its bite.
But how do you know if you’re the exception? Can you recognize the early warning sign of cancer, infection, autoimmune disease, or spinal cord injury? These things often cause other distinctive signs and symptoms, and so they are usually diagnosed promptly. If you are aware of these red flags, you can get checked out when the time is right — but please avoid excessive worry before that.
The rule of thumb21 is that you should start a more thorough medical investigation only when three conditions are met:
- it’s been bothering you for more than about six weeks
- the trend is strongly negative — the pain is severe and/or not improving, or even getting worse
- there is at least one other red flag (see below)
And there are also two rare situations where you shouldn’t wait several weeks before deciding the situation is serious …
- Pain and weakness in both legs, especially if it’s also hard to pee.22
- Any accident with forces that may have been sufficient to fracture your spine. Please seek thorough medical assessment promptly, including an X-ray to look for a fracture. You really do need an X-ray to ensure that your spine is not actually broken. They aren’t necessarily as obvious as you’d think!
This free article explains in more detail (including a list of red flags) and is strongly recommended to anyone who feels nervous:
In all other cases, you can safely read this tutorial first. For instance, even if you have severe pain or numbness and tingling down your leg, you can safely read this first. Or, even if you have an obviously severe muscle tear from trying to lift your car or something, you can safely start here — rest and read. Your back is not as fragile as you probably think, and understanding why is a great starting place for healing in nearly all cases of low back pain.
Don’t confuse threat and risk. Working at the edge is a risk. But then again, so is walking out your front door.
Is back pain a symptom of COVID-19? (Or other common infections?)
Back pain is not specifically a prominent feature of COVID-19. However, infections always lower our pain thresholds, and so all common aches and pains are more likely to be triggered or aggravated by any systemic infection — but perhaps COVID-19 more than most, simply because it’s unusually good at causing widespread body aching,23 and backs are included in that. But back pain doesn’t stand out any more than any other common locations for aching or soreness (with the exception of headache, which occurs in 8–14% of cases.2425).
So, if you were already at risk of a flare-up of back pain, it could emerge during any infection, exposed like a rock that is only visible at low tide.
Part 2
Low Back Pain Diagnosis & The Nature of the Beast
Your low back is not fragile! Most of what is supposedly “wrong” with spines and backs is nonsense
Spines haven’t changed in the last century,26 and yet humanity suffers from a great plague of low back pain.27 Contrary to popular belief, this plague almost certainly afflicts “primitive” societies just as much as industrialized ones.28 The real causes of most back pain are obscured by medical mythology and misunderstanding,29 and a thick fog of nonsense constantly spewing forth from an army of quacks trying to compensate for medicine’s failure to help.
Before I discuss what kind of things might be the “real causes” of low back pain, it’s extremely important to talk about what does not cause it. In this section, I will challenge the main myths in just a few paragraphs, supported by dozens of references to the best scientific information available.
Most people — and most health care professionals — believe that back pain is usually caused mainly by structural problems, either injury or degeneration of the spine. This idea is not supported by the scientific evidence. Indeed, just the opposite is more the case: “The evidence that tissue pathology does not explain chronic pain is overwhelming (e.g., in back pain, neck pain, and knee osteoarthritis).”30
Spines do degenerate, and that can and does hurt in some people — clearly — but mostly not for the reasons most people think they do: genetics and physiology are much likelier drivers of degeneration.31 Not your posture, your office chair, or your mattress. Not spinal alignment, or core stability, or subtle long-term stresses … or really anything else that low back pain sufferers have been taught to blame their pain on (by the people selling the alleged solutions).
People with arthritic spinal degeneration are not the ones who develop back pain, and that is not a casual statement: it’s based on high quality data,32 and there is a mountain of other evidence to back it up (much more science ahead). Spinal degeneration is involved, but it does not explain the tragedy of back pain.
Belief in spinal fragility and instability is unjustified but deeply held, based on ignorance of a complex subject and on an obsolete mechanical view of biology that has dominated medical thinking for centuries … and still does to a surprising extent. And when structural problems are exaggerated, you also get a plague of barking-up-the-wrong-tree treatments based on that exaggeration.
END OF FREE INTRODUCTION
Purchase full access to this tutorial for USD$1995. Continue reading this page immediately after purchase. See a complete table of contents below. Most content on PainScience.com is free.?
Almost everything on this website is free: about 80% of the site by wordcount, or 95% of the bigger pages. This page is only one of 10 that have a price tag. There are also hundreds of free articles, including several about low back pain. Book sales — over 75,500 since 2007?This is a tough number for anyone to audit, because my customer database is completely private and highly secure. But if a regulatory agency ever said “show us your math,” I certainly could! This count is automatically updated once every day or two, and rounded down to the nearest 100. Due to some oddities in technology over the years, it’s probably a bit of an underestimate. — keep the lights on and allow me to publish everything else (without ads).
Q. Ack, what’s with that surprise price tag?!
A. I know it can make a poor impression, but I have to make a living and this is the best way I’ve found to keep the lights on here.

Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
| company | PainScience.com |
|---|---|
| owner | Paul Ingraham |
| contact | 778-968-0930 |
| refunds | 100%, no time limit +Customers are welcome to ask for a refund months after purchase — I understand that it can take time to decide if information like this was worth the price for you. |
| more info | policies page ❐ |
| payments |
- What do you get, exactly? An online tutorial, book-length (182 chapters). Free updates forever, read on any device, and lend it out. E-book only! MORE
- Secure payment takes about 2 minutes. No password or login: when payment is confirmed, you are instantly granted full, permanent access to this page.MORE
- Collect them all. Get an “e-boxed” set of all 10 PainScience.com tutorials, ideal for pros … or patients with a lot of problems.MORE
Q. What am I buying? Is there an actual paper book?
A. Payment unlocks access to 175 more chapters of what is basically a huge webpage. There is no paper book — I only sell book-length online tutorials. This format is great for instant delivery, and many other benefits “traditional” e-books can’t offer, especially hassle-free lending and updates. You get free lifetime access to the always-current “live” web version (and offline reading is easy too).

Read on any device. Lend it out. New editions free forever.
Q. I just don’t like reading on the computer! Is there any way around that?
A. The design and technology of the book is ideal for reading on tablets and smart phones. You can also print the book on a home printer.
Q. Can I lend the tutorial out?
A. Yes! Feel free to lend your tutorial: I do not impose silly lending limits like with most other ebooks. No complicated policies or rules, just the honour system! You buy it, you can share it. You can also give it as a gift.
Q. Is it safe to use my credit card on your website?
A. Literally safer than a bank machine. Payments are powered by Stripe, which has an A+ Better Business Bureau rating. Card info never touches my servers. It’s easy to verify my identity and the legitimacy of my business: just Google me [new tab/window].
Q. I can really get a refund at any time?
A. Yes. All PainScience.com ebooks have a lifetime money-back guarantee.
Q. Why do you ask for contact information?
A. To prevent fraud and help with order lookups. You aren’t “subscribing” to anything: I never send email to customers except to confirm purchases.
Q. Can I buy this anywhere else? Amazon?
A. Not yet. Maybe someday.
See the “fine print page” for more about security, privacy, and refunds. No legalese, just plain English.
Save a bundle on a bundle
The e-boxed set is a bundle of all 10 book-length tutorials for sale on PainScience.com: 10 books about 10 different common injuries and pain problems. All ten topics are (all links open free intros in a new tab/window): muscle strain, muscle pain, back and neck pain, two kinds of runner’s knee (IT band syndrome and patellofemoral pain), shin splints, plantar fasciitis, and frozen shoulder. (Headache coming soon, fall of 2019.)
Most patients only need one book, because most patients have only one problem. But the set is ideal for professionals, and some keen patients do want all of them, for the education, and for lending to friends and family. And, of course, you do get a substantial discount for the bulk purchase. But no rush—complete the set later, minus the price of any books already bought. More information and purchase options.
You can also keep reading more without buying. Here are some other free samples from the book, and other closely related articles on PainScience.com:
- EXCERPT Neuropathies Are Overdiagnosed
- EXCERPT Don’t Worry About Lifting Technique
- EXCERPT Chronic Low Back Pain Is Not So Chronic
- EXCERPT The Mind Game in Low Back Pain
- EXCERPT The Tyranny of Yoga and Meditation
- EXCERPT Do Nerve Blocks Work for Neck Pain and Low Back Pain?
- MRI and X-Ray Often Worse than Useless for Back Pain
- How to Treat Sciatic Nerve Pain
- 6 Main Causes of Morning Back Pain
- When to Worry About Low Back Pain
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
The back pain misinformation explosion
I hope that this page is one of the saner sources of back pain information available online, while also being much more thorough and friendly than the big medical sources. Since I first started treating low back pain in 2000, there’s been an explosion of free online information about it, of course — countless poor quality articles (see Starman). Literally hundreds of thousands of them. Back in the day, we actually had to go to a doctor or buy a book to get shoddy back pain information — now it’s just a Google search away.
Over the years, I’ve collected some interesting examples of just how bad it gets. Here’s three, shared for the chuckles and the teachable moments…
Exhibit A: The worst possible website about pain
ThePain.net is one of the worst examples I’ve seen: a large, stale, ugly thing by Pekka Palin, MD. There are hours of terrible reading there! Dozens of blandly composed, shallow, rambling, and frequently irrational mini-articles on every imaginable pain subject, all 100% unreferenced, laid out in huge blocks of text without a subheading for many screens (a typographic travesty).
There’s soooo much badness, but I really got a chuckle out of this perfectly pointless phrase: “The most common term used for general, temporary low back pain is lumbago.” Now “lumbago” means “back pain” (see the definition of lumbago on Wikipedia), so Dr. Obvious has helpfully explained that the cause of back pain is, er, back pain. The Internet, at your service!
Exhibit B: Awful back pain information from Consumer Reports
Dr. Harriet Hall, critiquing a recent issue of Consumer Reports about back pain:
I found the [Consumer Reports] articles on back pain very disappointing. I hope I can still trust Consumer Reports when shopping for a washing machine, but I have no confidence that I can trust them when looking for an effective medical treatment. They seem not to understand the difference between anecdotes and data, between a popularity contest and a controlled scientific study. These articles may do harm by encouraging readers to try treatments that don’t work and by suggesting that it is reasonable to prioritize testimonial evidence over scientific studies. On the other hand, these articles may do some good insofar as they may dissuade some patients from rushing to a doctor and demanding imaging studies or prescription drugs.
Well, at least there’s that! But most of what CR published was horrifyingly naive and misleading. I scanned this issue in a grocery store lineup and was rolling my eyes within seconds. And then fuming: it seems like the flood of misinformation about back pain is infinite! I’ve been actively debunking back pain myths for about 15 years now, and the need for it has barely changed in all that time. So-called information like this, reaching a massive audience, seriously exacerbates the problem.
I think Consumer Reports has made serious mistakes in other domains over the last few years, and they are quickly burning the credibility it took decades to earn. Sadly, they will still have a strong enough reputation for years to come to do plenty of damage with content like this.
Even many better articles still have serious “attitude” problems. Usually the attitude problem is unjustified optimism. For instance …
Exhibit C: A widely praised “high quality” article full of flaws
This extremely popular 2017 article on Vox.com the “new science” of low back pain was praised by many because it superficially seems to be very modern and science-y, and it correctly dismisses a number of myths, but I think it’s an exasperating failure. It creates a strong impression of being scientifically rigorous without actually being so. It brims with promising science news about alternative treatments that do not actually stand up to more cynical and experienced analysis.
Adding to the façade of scientific credibility, many of the right caveats and disclaimers about the “new science” are technically there — warnings about small effect sizes, mixed evidence, and potential flaws — but these cautions are also belated and consistently understated. The tone is overwhelmingly sunny and naïve, as though we are on the verge of a revolution in back pain treatment thanks to … a bunch of stuff that has been around forever and has clearly not been saving the world from chronic low back pain.
The low point of the article is definitely the advice to try to find a “back whisperer.” Back pain is too difficult a problem for anyone to have that role, no matter how expert and experienced. I think the idea of a back whisperer dangerously promotes false hope.
So who can you trust?
You’d think that you might be able to escape this mess by reading medical journals, but that’s hardly guaranteed. Even back pain guidelines published in medical journals are often misleading. They are not all good. The committees that write these things do not necessarily know the science. One of the best reviews of back pain research ever published — Machado 2009, more on this one later — found something really interesting: “treatment recommendations from recent clinical guidelines do not align with the results of this meta-analysis.” In fact, quite a few disproven pain treatments are still cheerfully recommended in otherwise sensible professional guidelines. Eek. So I am realistic about the limits of the science, much of which is pretty junky. +The quality of science is a huge topic, but here’s one simple example of an extremely common problem with back pain science: control groups that don’t control. Rather than comparing a treatment to a good, carefully selected placebo, most studies use a comparison to a treatment that is allegedly neutral, underwhelming, or placebo-ish. That makes the results hard to interpret: if each works about the same, it could mean that the treatments are equally effective … or equally ineffective! So much back pain science has this problem — or any one of a dozen other weak points — that you can effectively ignore at least 80% of all back pain research, because it’s so far from the last word on anything. Good science is essential to solving these problems, but really good studies are also difficult to design and rare.
So why trust this tutorial? Well, you don’t need to take my word for anything — you can just take the word of the many low back pain medical experts that I quote extensively, and the hard evidence that their opinions are based on.+ (At the same time, I am realistic about the limits of the science, much of which is surprisingly junky.)

Don’t take my word for anything. Take this guy’s word for it. Dr. Richard Deyo has been busting myths about low back pain for longer than I’ve been alive.

Or this guy’s word. Dr. Nikolai Bogduk has authored dozens of scientific papers about low back pain. He also questions and challenges many common beliefs about low back pain, and is one of the expert sources this tutorial relies upon.

Or this guy’s. Dr. Siegfried Mense is the world’s foremost expert in muscle pain. He is the author of an authoritative text on that subject, and one of this guide’s more important sources.
And, most importantly of all, I’m not selling a cure: the purpose of this guide is “just” education. It’s best for people who like to understand their problems. Its dorky, quirky thoroughness is unique. I will not just tell you what you want to hear. Understanding low back pain as well as possible is valuable, but it will not necessarily lead to a cure. Sadly, some low back pain cannot be fixed.
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
Further Reading
Other articles on PainScience.com about back pain (lots of them, as if this book wasn’t long enough):
- Back Pain & Trigger Points — A quick introduction to the role of trigger points and massage therapy in back pain
- Massage Therapy Kinda, Sorta Works for Back Pain — It works, but not very well, and “advanced” techniques are no better than relaxation massage
- Do Nerve Blocks Work for Neck Pain and Low Back Pain? — Analysis of the science of the “block & burn” therapies, stopping the pain of facet joint syndrome with nerve blocks, joint injections, and nerve ablation
- (Almost) Never Use Ice on Low Back Pain! — An important exception to conventional wisdom about icing and heating
- 6 Main Causes of Morning Back Pain — Why is back pain worst first thing in the morning, and what can you do about it?
- How to Treat Sciatic Nerve Pain — A user-friendly, evidence-based guide for patients about how to manage buttock and leg pain (which may or may not actually involve the sciatic nerve)
- The “perfect spots” to massage back pain:
- Massage Therapy for Low Back Pain — Perfect Spot No. 2, in the erector spinae and quadratus lumborum muscles in the thoracolumbar corner
- Massage Therapy for Back Pain, Hip Pain, and Sciatica — Perfect Spot No. 6, an area of common trigger points in the gluteus medius and minimus muscles of the hip
- Massage Therapy for Low Back Pain (So Low That It’s Not In the Back) — Perfect Spot No. 12, a common (almost universal) trigger point in the superolateral origin of the gluteus maximus muscle
- Massage Therapy for Low Back Pain (Again) — Perfect Spot No. 13, The Most Classic Low Back Pain Trigger Point
- The Bath Trick for Trigger Point Release — A clever way of combining self-treatment techniques to self-treat your trigger points (muscle knots)
- Spinal Subluxation — Can your spine be out of alignment? Chiropractic’s big idea has been misleading patients for more than a century
- Spinal Fracture Bracing and Fixation — My wife’s terrible accident, and a whirlwind tour of the science and biomechanics of her spine brace
- Does Spinal Manipulation Work? — Spinal manipulation, adjustment, and popping of the spinal joints and the subluxation theory of disease, back pain and neck pain
- Does Posture Matter? — A detailed guide to posture and postural correction strategies (especially why none of it matters very much)
- The Trouble with Chairs — The science of being sedentary and how much it does (or doesn’t) affect your health and back pain
- Psoas, So What? — Massage therapy for the psoas major and iliacus (iliopsoas) muscles is not that big a deal
Other good reading about back pain:
- Mind Over Back Pain: A radically new approach to the diagnosis and treatment of back pain (book), by John Sarno. A classic in the field, flawed and aging still but worthwhile, written before Dr. Sarno started to treat his approach like a panacea. The book emphasizes a lot of right ideas for the wrong reasons.
- “The Pain Perplex,” a chapter in the book Complications, by Atul Gawande. Gawande’s entire book is worth reading, but his chapter on pain physiology is certainly the best summary of the subject I have ever read, and a terrific reminder that good writing for a general audience can be just as illuminating for professionals. Anyone struggling with a pain problem should buy the book for this chapter alone, though you are likely to enjoy the whole thing. Much of the chapter focuses on one of the most interesting stories of low back pain I’ve read, and it is a responsible and rational account — although Gawande, like most doctors, seems to be unaware of the clinical significance, or even existence, of myofascial trigger points.
- Dr. Jerome Groopman has written brilliantly about back pain, from personal experience. In How Doctors Think he puts back pain in the context of how medical thinking is influenced by marketing and money, giving us a somewhat chilling insiders’ view of the surgical treatment of back pain. In The Anatomy of Hope, he tells his own story of super severe back pain. It has a happy ending! Both books are also otherwise worthwhile. “Marketing, Money, and Medical Decisions,” a chapter in the book How doctors think, by Jerome Groopman. Groopman, writing from personal experience with chronic back pain and a spinal fusion surgery, discusses back pain as intelligently as any medical expert I’ve come across, but he does so in a way that will fascinate patients. In this chapter, his discussion of back pain is placed in the context of how medical thinking is influenced by marketing and money, giving us a somewhat chilling insiders’ view of the surgical treatment of back pain.
Reader feedback … good and bad
Testimonials on health care websites reek of quackery, so publishing them has always made me a bit queasy. But my testimonials are mostly about the quality of the information I’m selling, and I hope that makes all the difference. So here are some highlights from the kind words I’ve received over the years … plus some of the common criticisms I receive, at the end. These are all genuine testimonials, mostly received by email. In many cases I withold or change names and identifying details.
As an author and a chronic lower back pain sufferer, after spending the day with your book I am supremely impressed. You present such useful information in such an entertaining fashion. I’ve been laughing and learning and feeling completely uplifted and delighted and confident that I’ll be able to sort out my back pain issues with your book as a guide.
Anna Herald
I was reading your info about lower right back pain and I love how you say not to worry about everything, and add that even if it IS serious, it can most likely be cured. While reading it, I realised later that my acute pain had slightly subsided.You’re doing such a great service for so many people. I’m almost glad I was in such pain (on a weekend, of course) that I had to look up medical information myself. Yours is readable, understandable, funny, humble, and....tight on!
Elsie Ventura
Just wanted to thank you for your clear, well-organized, credible, and thorough information about back pain. I am experiencing back pain that’s barking loudly for the first time in my 72 years. I now have an idea of the possibilities and degrees of seriousness. Thank you again for making the time and effort to write well.
Braydon Aldred
I stumbled upon your writings this morning, when I was wishing I was at the gym, where I would usually be. It was some kind of kismet, for sure, because everything I read made total, absolute sense. Thank you, thank you, thank you. You have given me the courage and resolve to sit out this sprain so I can get back up again intact, and stay that way. Your writings about joint mobilization also make me realize I have some tactics to improve my current state now, even though I am recovering. A huge lightbulb has gone off for me. Thank you, again! Finally, I love your statement about going and putting your 110% into something else while you are healing. Best advice ever.
Stacey Simons
Thanks again for putting together all the back pain research — a good percentage of it anyway — into an easy-to-read publication.
Nojus Proctor
Thank you immensely for the best, most sensible and credible information on back pain. So glad you came up in my google search. Credible, reassuring, and humorous too.
Suzanne Haslett, Suzanne Haslett, Masters in Human Development (Oxford)
I purchased the low back tutorial recently and got the free trigger points one also. Many thanks. They are great! I had already accessed the perfect spot series and have been working on my trigger points. It is very pleasing to have the full discussion of the physiology, and I now have a much better idea about the whole ghastly business.
Leah Brannen, Saskatoon, Canada
I bought two of your eBooks last week, and I’m enjoying going through them. Your presentation is excellent. It’s far too early to say, of course, but I think I’ve already begun to benefit from your approach. One of the things I like most about your approach is your respect for “science,” as opposed to “merchandising.” You've put so much into those two eBooks, it's going to take time to do them the justice they deserve.
David Calderisi, Toronto, Ontario
David diligently followed up a month later with the following comment: “By now I’m convinced your research and recommendations are right on the money. Thanks. I’ve recommended you to a few people who, like myself, have had back problems on and off for years. Thanks for having provided such a useful tool.” ~ Paul
I spent seven hours straight sitting at my computer and my back didn't hurt at all! You’re a genius! Thanks so much.
Isabelle Deguise, Graduate Student
I had suffered from undiagnosed and seemingly untreatable low back pain since late August last year. Three physiotherapists, my GP, two RMTs, and my generally excellent personal trainer failed to help me make any progress. At my last visit to my GP in late December, he maintained his insistence that I just needed to loosen up my hamstrings! The systematic approach you took to reviewing all the supposed cures and providing a clear analysis of each and no doubt saved me thousands of dollars and months of frustration. That gave me the focus to work on trigger points known to cause LBP (with the help of some additional books and a great TP therapy app for my phone). My back pain isn’t totally gone, but I’m 95% there and I’ve got a handle on it.
Erin Banks
One more noteworthy endorsement, with regards to this whole website and all of my books, submitted by a London physician specializing in chronic pain, medical education, and patient-advocacy (that’s a link to his excellent blog):
I’m writing to congratulate and thank you for your impressive ongoing review of musculoskeletal research. I teach a course, Medicine in Society, at St. Leonards Hospital in Hoxton. I originally stumbled across your website whilst looking for information about pain for my medical students, and have recommended your tutorials to them. Your work deserves special mention for its transparency, evidence base, clear presentation, educational content, regular documented updates, and lack of any commercial promotional material.
Dr. Jonathon Tomlinson, MBBS, DRCOG, MRCGP, MA, The Lawson Practice, London
What about criticism and complaints?
Oh, I get those too! I do not host public comments on PainScience.com for many reasons, but emailed constructive criticism, factual corrections, requests, and suggestions are all very welcome. I have made many important changes to this tutorial inspired directly by critical, informed reader feedback.
But you can’t make everyone happy! Some people demand their money back (and get it). I have about a 1% refund rate (far better than average in retail/e-commerce). The complaints of my most dissatisfied customers have strong themes:
- Too negative in general. Some people just can’t stomach all the debunking. Such customers often think that I dismiss “everything” … which I disagree with.
- Too negative specifically. Some are offended by my criticisms of a treatment option that they personally use and like. Or sell!
- Too advanced. Although I work hard to “dumb” the material down, quite a few people still just find it too dense and dorky.
- Too simple. Some people think they already know everything about the topic. Maybe they do, and maybe they don’t. I always wish I could give these readers a pop quiz. 😉 In my experience, all truly knowledegable people get that way by embracing every new persective and source of information.
Acknowledgements
Thanks to every reader, client, and book customer for your curiosity, your faith, and your feedback and suggestions, and your stories most of all — without you, all of this would be impossible and pointless.
Writers go on and on about how grateful they are for the support they had while writing one measly book, but this website is actually a much bigger project than a book. PainScience.com was originally created in my so-called “spare time” with a lot of assistance from family and friends (see the origin story). Thanks to my wife for countless indulgences large and small; to my parents for (possibly blind) faith in me, and much copyediting; and to friends and technical mentors Mike, Dirk, Aaron, and Erin for endless useful chats, repeatedly saving my ass, plus actually building many of the nifty features of this website.
Special thanks to some professionals and experts who have been particularly inspiring and/or directly supportive: Dr. Rob Tarzwell, Dr. Steven Novella, Dr. David Gorski, Sam Homola, DC, Dr. Mark Crislip, Scott Gavura, Dr. Harriet Hall, Dr. Stephen Barrett, Dr. Greg Lehman, Dr. Jason Silvernail, Todd Hargrove, Nick Ng, Alice Sanvito, Dr. Chris Moyer, Lars Avemarie, PT, Dr. Brian James, Bodhi Haraldsson, Diane Jacobs, Adam Meakins, Sol Orwell, Laura Allen, James Fell, Dr. Ravensara Travillian, Dr. Neil O’Connell, Dr. Tony Ingram, Dr. Jim Eubanks, Kira Stoops, Dr. Bronnie Thompson, Dr. James Coyne, Alex Hutchinson, Dr. David Colquhoun, Bas Asselbergs … and almost certainly a dozen more I am embarrassed to have neglected.
I work “alone,” but not really, thanks to all these people.
I have some relationship with everyone named above, but there are also many experts who have influenced me that I am not privileged to know personally. Some of the most notable are: Drs. Lorimer Moseley, David Butler, Gordon Waddell, Robert Sapolsky, Brad Schoenfeld, Edzard Ernst, Jan Dommerholt, Simon Singh, Ben Goldacre, Atul Gawande, and Nikolai Boguduk.
What’s new in this tutorial?
This tutorial has been continuously, actively maintained and updated for 22 years now, staying consistent with professional guidelines and the best available science. The first edition was originally published in September 2004, after countless hours of research and writing while I spent a month taking care of a farm (and a beautiful pair of young puppies) in the Okanagan.
Regular updates are a key feature of PainScience.com tutorials. As new science and information becomes available, I upgrade them, and the most recent version is always automatically available to customers. Unlike regular books, and even e-books (which can be obsolete by the time they are published, and can go years between editions) this document is updated at least once every three months and often much more. I also log updates, making it easy for readers to see what’s changed. This tutorial has gotten 261 major and minor updates since I started logging carefully in late 2009 (plus countless minor tweaks and touch-ups).
Jun 9, 2026 — Additions: Added the least-poor interventional pain medicine options, and did some other miscellaneous tweaking. [Updated section: Now what?: An action-oriented summary of recommendations.]
June — Revision: Added a better overview of the minimally invasive treatments that are more drastic than the conservative options, but less than surgery (interventional pain medicine), along with a variety of other minor improvements. [Updated section: Getting professional help: A consumer’s guide to buying therapy and medical care for low back pain.]
June — New section: The topic of epidural steroid injection is another member of the “interventional pain medicine” family and very closely related to the “block and burn” treatments discussed in other chapters. So for a long time this book just had light coverage of it along with those. But it is a distinct treatment … and extremely widely prescribed, so it is particularly deserving of its own better-late-than-never chapter. And here it is at last — a major addition to the book, about 3000 words. [Updated section: Enough with the gratuitous epidural steroid injections already.]
2025 — Minor update: Did a little quick review to make sure that nothing major has changed on this topic in the last few years, and then did a few minor edits and clarifications. [Updated section: Antibiotics for back pain: a debacle.]
2025 — Major update: This intro to “getting professional help” contains a bunch of thumbnail sketches of treatment options that are review in more detail later on. They were all quite overdue for updates and revision. Half of them said things I stopped believing years ago! I also added chapter links, making the section into high quality annotated table of contents for this whole part of the book. [Updated section: Getting professional help: A consumer’s guide to buying therapy and medical care for low back pain.]
2025 — New section: No notes. Just a new chapter. [Updated section: Injections: AMG0103 rescues spinal discs in preliminary drug trial in 2025.]
2025 — News: Noted that CFT training is now for sale, and added a substantive footnote explaining “what could possibly go wrong.” [Updated section: Cognitive Functional Therapy (and the too-good-to-be-true 2023 study that launched it to stardom).]
2025 — Science update: It took years, but there was finally enough good quality new science to update the introduction to all treatment options for back pain — mostly thanks to Cashin et al. on the manual therapies, and Wang et al. on the medical (injections etc). Now, if only we could get some decent placebo-controlled trials of microdiscectomy… [Updated section: Introduction to treatment and self-treatment: So what’s the plan?]
2025 — Upgraded: Extensive improvements and refinements following up on the February re-write, and after sharing the excerpted chapter with members (which always pushes me to polish content to a particularly high shine). [Updated section: Diagnose, schmiagnose! Physical exam reliability is poor.]
2025 — Major science update: After years of underwhelming and mixed evidence, a new 2025 review has concluded that spinal injections and nerve ablations are collectively very unimpressive … and the doctors have responded with demands for retraction of the evidence. It’s not a good look. [Updated section: Kill it with fire! Treatment by nerve destruction.]
2025 — Revision: More and clearer detail, but no substantive changes — the chapter still says essentially the same thing, but better. I confirmed a lack of any important new evidence. [Updated section: Sitting and sedentariness, chairs and ergonomics.]
2025 — New topic: Added another treatment to the “Hall of Shame” chapter: laser therapy. [Updated section: A few more snack-sized reality checks: brief comments on treatments to avoid.]
2025 — New chapter: A significant new overview of medical testing for specific causes of back pain, one of those “basic” topics that was missing from the original, quirkier version of the book for too many years. This is a good step towards rounding it out and making it a more complete guide to the topic for a wider range of readers. [Updated section: Medical tests for specific causes: an introduction to doctorly diagnosis.]
2025 — Rewritten: Major chapter overhaul and expansion. There is now much more detail (2800 words!) about the art and science of diagnosing specific causes of back pain with a physical examination. [Updated section: Diagnose, schmiagnose! Physical exam reliability is poor.]
2024 — Science update: First update to this section in eight years, because the basic point has been sound the whole time. What changed? Better science, just a particularly good and relevant study that supports the gist of this introduction more strongly than anything that was available before. [Updated section: Low Back Pain Diagnosis & The Nature of the Beast: Your low back is not fragile! Most of what is supposedly “wrong” with spines and backs is nonsense.]
2024 — New sub-topic: [Updated section: Are you crooked? The alignment and posture villains: short legs, pelvic tilts, and spinal curves.]
2024 — New chapter: No notes. Just a new chapter. [Updated section: Walking it off.]
2024 — Minor addition: Added a bit of a rant, some summary perspective and colour: “Chasing posture as a cause of back pain is a dead end.” [Updated section: Are you crooked? The alignment and posture villains: short legs, pelvic tilts, and spinal curves.]
2024 — New chapter: New chapter, inspired by new evidence, about how being out of shape is probably worse for your spine than biomechanical glitches, and how back pain patients eat more junk food. [Updated section: Could it be metabolic?]
2024 — Revised: This is mostly an old chapter, but reframed, revised, with significant clarifications and caveats added. Despite being mostly the same, it’s quite different! [Updated section: Does fear of movement cause back pain? Or just fear? The vicious cycle hypothesis.]
Archived updates — All updates, including 205 older updates, are listed on another page. ❐
2005 — Publication.
Notes
In 2012, the The Journal of Foot & Ankle Surgery ranked 136 websites about common foot and ankle diagnoses. Expert reviewers gave each a quality score on a scale of 100. The average score? Just below fifty. Fifty! See Smith et al.
Or see Starman et al. for a review of other kinds of health care information (with nearly identical grades).
P.S. These references are aging now… but nothing’s really changed!
- Cashin AG, Furlong BM, Kamper SJ, et al. Analgesic effects of non-surgical and non-interventional treatments for low back pain: a systematic review and meta-analysis of placebo-controlled randomised trials. BMJ Evid Based Med. 2025 Mar:bmjebm–2024–112974. PubMed 40101974 ❐
This is the best single reference showing the lack of efficacy from all popular back pain treatments, but there’s lot more to say — much more information about treatment efficacy will be presented later on in this tutorial.
- Hexenschuss is a German word for back spasm or lumbago, but translated literally it means shot by the witch (hexe = witch and Schuss = shot). Those Germans have a word for everything! Hat tip to reader Richard Moison for teaching it to me.
Here’s the first of many expert opinions and quotes about this, from a 2013 paper by Max Zusman, explaining why low back pain is still such an incredibly costly problem for society:
It is extremely difficult to alter the potentially disabling belief among the lay public that low back pain has a structural mechanical cause. An important reason for this is that this belief continues to be regularly reinforced by the conditions of care of a range of ‘hands-on’ providers, for whom idiosyncratic variations of that view are fundamental to their professional existence.”
Well said, but perhaps a bit wordy. Here’s the simple version: patients believe back pain is caused by structural fragility, and careers are built on catering to that belief. I would also say that it is difficult to alter that belief in anyone, patient or professional. This preoccupation with fragility isn’t just reinforced by the practices of many therapists, it’s a major reason for them.
- Jansson C, Mittendorfer-Rutz E, Alexanderson K. Sickness absence because of musculoskeletal diagnoses and risk of all-cause and cause-specific mortality: A nationwide Swedish cohort study. Pain. 2012 May;153(5):998–1005. PubMed 22421427 ❐
- Williams CM, Maher CG, Hancock MJ, et al. Low back pain and best practice care: a survey of general practice physicians. Arch Intern Med. 2010 Feb;170(3):271–7. PubMed 20142573 ❐ PainSci Bibliography 55582 ❐
“Usual care provided by general practitioners for low back pain does not match the care endorsed in international evidence-based guidelines and may not provide the best outcomes for patients. This situation has not improved over time.”
- A series of 2018 back pain articles in The Lancet (see Foster, Hartvigsen, Buchbinder) expressed what has become almost standard outrage at the useless back pain treatments still constantly provided by all kinds of professionals. This has been going on for decades now: the experts bemoaning the pitiful state of the standard of care for back pain. The experts just keep saying it, seemingly with more force every year — more presitigous journals, citing better evidence than ever — while the average clinician remains largely oblivious.
- Most doctors lack the skills and knowledge needed to care for common aches, pains, and injury problems, especially the chronic cases, which they tend to underestimate the complexity of. This has been shown by many studies, like Stockard et al., who found that 82% of medical graduates “failed to demonstrate basic competency in musculoskeletal medicine.” It’s just not their thing, and people with puzzling or stubborn pain should take their family doctor’s advice with a large grain of salt, and even lower their expectations of specialists (who tend to be too specialized). See The Medical Blind Spot for Aches, Pains & Injuries: Most physicians are unqualified to care for many common pain and injury problems, especially the more stubborn and tricky ones.
![Cartoon of a man sitting in a doctor’s office. The doctor is holding a clipboard with a checklist with just two items on it: stress related and age related. The caption reads: “An extremely general practitioner.”]()
- Buchbinder R, Staples M, Jolley D. Doctors with a special interest in back pain have poorer knowledge about how to treat back pain. Spine (Phila Pa 1976). 2009 May;34(11):1218–26; discussion 1227. PubMed 19407674 ❐
- I was an alternative health professional myself for many years — a Registered Massage Therapist, trained in Canada (which has unusually good training standards). Of course, some of my colleagues in alternative medicine were diligent students of medical science. However, in my experience, most were certainly not — indeed, many lacked even the most basic knowledge of how medical science works or how to keep current about recent discoveries with clinical implications.
- Moseley GL. Whole of community pain education for back pain. Why does first-line care get almost no attention and what exactly are we waiting for? Br J Sports Med. 2018 Jul. PubMed 29982226 ❐
- Moseley 2018, op. cit. Dr. Moseley again. He notes that “education is universally recommended as first-line treatment for acute and persistent back pain but it attracts little attention … Is this because health professionals intuitively know what education is and how to do it? Our research suggests not6—most doctors (although there are precious exceptions) do not know what it is, do not know how to do it, do not have the content knowledge and, even if they did, do not have the time.”
- Patients new to pain often assume that healthcare pros must know what it’s like… but most can’t actually relate, not without living with it. And so obnoxious overconfidence is common. Exhibit A: When Internet-famous physical therapist Adam Meakins had an episode of severe back pain, he received endless bizarrely arrogant, judgemental, condescending reactions from his colleages! Adam Meakins:
“Out of all the debates and debacles I’ve had on social media I don’t think I’ve ever been accused of, or called so many negative and nasty things by so many clinicians since I’ve been a person in pain documenting my progress over these last 9 days! #GiveMeStrength 🙄🤦🏻♂️🤫”
I have seen this nonsense myself with regards to my own chronic pain. The subtext (or just the text!) is always the same: “If you were competent like me, you could prevent/solve your own painful problem.” Ironically, the truth is almost certainly the opposite: their arrogance clearly results in ignorance and incompetence. Most of them are doomed to be humbled by their own pain someday.
- My original inspiration for this tutorial was Dr. John Sarno’s 1984 book Mind Over Back Pain: A radically new approach to the diagnosis and treatment of back pain, which is generally excellent, but a little too radical, too excited about one big idea. His more recent work (Healing Back Pain: The mind-body connection) makes too many empty promises and has serious flaws. See my Sarno review.
![[Cover of Mind Over Back Pain, by Dr. John Sarno]]()
Dr. John Sarno’s original best-seller about low back pain.
- Why is musculoskeletal and pain medicine in general such a mess? Many reasons! But mainly: professional pride and tribalism, ideological momentum, and screwed up incentives (certification rackets, freelancing, insurance, huge profits); the love of “advanced” and technological treatment methods; ignorance of the history of science and critical thinking skills; and the obscurity of newer and better ideas, especially the major neurological and biological factors that we’re still learning about, which many frontline clinicians are still oblivious to. I explore the all of this in more detail in A Historical Perspective On Aches ‘n’ Pains: Why is healthcare for chronic pain and injury so bad?
- There are many relevant sources, but these recommended beliefs are all cribbed directly from a short but sweet 2020 paper in the British Journal of Sports Medicine, “Back to basics: 10 facts every person should know about back pain”. It’s a good, readable explanation of back pain myths, and includes a fine “back facts” infographic. ❐ Here are the “unhelpful” low back pain beliefs identified by O’Sullivan et al., all “culturally endorsed and not supported by evidence”:
- Low back pain is usually a serious medical condition.
- Low back pain will become persistent and deteriorate in later life.
- Persistent low back pain is always related to tissue damage.
- Scans are always needed to detect the cause of low back pain.
- Pain related to exercise and movement is always a warning that harm is being done to the spine and a signal to stop or modify activity.
- Low back pain is caused by weak “core” muscles and having a strong core protects against future Low back pain.
- Repeated spinal loading results in “wear and tear” and tissue damage.
- Pain flare-ups are a sign of tissue damage and require rest.
- Treatments such as strong medications, injections and surgery are effective, and necessary, to treat Low back pain.
Good list! But I decided that a list of “helpful” beliefs would be more, well, helpful than a list of unhelpful ones, and editorially inverted them. 😉
- Coste J, Delecoeuillerie G, Cohen de Lara A, Le Parc JM, Paolaggi JB. Clinical course and prognostic factors in acute low back pain: an inception cohort study in primary care practice. BMJ. 1994;308:577–80. PubMed 8148683 ❐ PainSci Bibliography 57081 ❐
This paper presents some unusually optimistic old data about low back pain recovery: in a sample of about 100 patients, “90% of patients recovered within two weeks and only two developed chronic low back pain,” which is “much higher than reported in other studies,” but the authors suggest some good reasons why their number makes sense.
- There is an anxiety-producing myth that low back pain is serious and chronic if you can’t shake it after the first several weeks, when in fact many people recover just fine after that “deadline.” An entire section below is devoted to the strong scientific evidence about this.
- Once in a great while some cranky reader (always a guy) writes to tell me, “I didn’t learn anything from your book.” I’m a little skeptical about that, and it’s always tempting to start quizzing! There’s a great deal of information here, including analyses of recent research. Sure, readers who have already done a lot of reading about back pain might already be familiar with a lot of it — but you will know that going in, of course, and you’ll find the nuggets of new information and perspective that any keen reader is always looking for.
- In older adults, about 6% of cases have a serious cause, but 5% of those are fractures — which are serious, but they aren’t cancer either. The 1% is divided amongst all other serious causes. For people under age 55, the odds are even better.
- This is my translation/interpretation for patients of the somewhat more detailed information for physicians published in “Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society”.
- This is the best red flag we have for cauda equina syndrome (trouble with the lower spinal cord) — better than the more conventional . For more detail, see later in the book or When to Worry About Low Back Pain. But the main citation for this is Angus 2021.
All systemic infections can cause body aches, fatigue, and fever, because these symptoms are functions of the immune system, not the disease — but some diseases, like COVID-19, provoke it more than others.
The symptoms of most infections are not directly caused by damage they do to our tissues, especially at first. We cannot feel cells being killed by a virus; what we actually do feel is our immune system’s reaction to the invasion. One purpose of that reaction is to force us to stay still — also known as rest — mostly by making movement feel incredibly difficult and unpleasant. This “sickness behaviour” is a generalized reaction to a wide variety of biological threats found in all animals (see subtle systemic inflammation).
- Lei S, Jiang F, Su W, et al. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. EClinicalMedicine. 2020 2020/04/06. PainSci Bibliography 52605 ❐
- Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Accessed 2020-04-06.
- Ruhli FJ, Henneberg M. Clinical perspectives on secular trends of intervertebral foramen diameters in an industrialized European society. Eur J Spine. 2004 Apr 1. PubMed 15057552 ❐
This study of changes in spinal characteristics (in Swiss adults) since the late 19th century found … well, basically nothing. Spines are pretty much the same now as they were then. At least in Switzerland.
- Dr. Richard Deyo, one of the great myth busters of low back pain research, believes that “low back pain is second to upper respiratory problems as a symptom-related reason for visits to a physician” — only the common cold causes more complaints. Hart et al. puts low back pain in fifth place (lower because Hart oddly excludes chronic low back pain). Chronic low back pain is usually the kind that this book will examine. Andersson writes: “Although the literature is filled with information about the prevalence and incidence of back pain in general, there is less information about chronic back pain … .” Indeed, it is almost impossible to measure how much chronic low back pain there is: for every time that acute low back pain is the main reason for a visit to a physician, how many times does a patient mention low back pain as a secondary problem? Or sees an alternative health care professional about it instead? (Answer: pretty danged often.) So it’s actually possible that low back pain is the single most common reason that people seek help.
- I will cover this in more detail later, but the main citation for this is a 2017 paper by James Steele, PhD. He makes the case for this in detail and uses it as a premise for the hypothesis that back pain probably has something to do with a basic vulnerability in human biology, something we all share. See “An evolutionary hypothesis to explain the role of deconditioning in low back pain prevalence in humans”.
Nachemson says, “Rarely are diagnoses scientifically valid … .” And Deyo: “There are wide variations in care, a fact that suggests there is professional uncertainty about the optimal approach.” Many other researchers have made this point, but Sarno (p. 111) states it most eloquently:
There is probably no other medical condition which is treated in so many different ways and by such a variety of practitioners as back pain. Though the conclusion may be uncomfortable, the medical community must bear the responsibility for this, for it has been distressingly narrow in its approach to the problem. It has been trapped by a diagnostic bias of ancient vintage and, most uncharacteristically, has uncritically accepted an unproven concept, that structural abnormalities are the cause of back pain.”
- Moseley L. Teaching people about pain — why do we keep beating around the bush? Pain Management. 2012;2(1):2–3. PubMed 24654610 ❐ PainSci Bibliography 54762 ❐
- Battié MC, Videman T, Kaprio J, et al. The Twin Spine Study: contributions to a changing view of disc degeneration. Spine J. 2009;9(1):47–59. PubMed 19111259 ❐ “The once commonly held view that disc degeneration is primarily a result of aging and wear and tear from mechanical insults and injuries was not supported by this series of studies. Instead, disc degeneration appears to be determined in great part by genetic influences. Although environmental factors also play a role, it is not primarily through routine physical loading exposures (eg, heavy vs. light physical demands) as once suspected.”
- Kasch R, Truthmann J, Hancock MJ, et al. Association of Lumbar MRI Findings with Current and Future Back Pain in a Population-based Cohort Study. Spine (Phila Pa 1976). 2022 Feb;47(3):201–211. PubMed 34405825 ❐
This is a large study of the relationship between back pain and common signs of spinal arthritis, finding mostly that … there wasn’t much of one. The correlation was there, it was just rather puny. MRI findings, on average, “do not have clinically important associations with low back pain.”
The study was a bit unusual and quite useful because it was a big “longitudinal” one: observing the same group of people for a long time. We don’t see a lot of those in back pain research, especially of this size/duration: about 3300 people studied for over six years. That design gives us insight into the order of things, producing what I think is the most important single result here: pain didn’t develop in people who started out with signs of spinal degeneration. It’s not just that signs and pain aren’t strongly correlated, it’s that pain doesn’t follow the signs. More formally stated by the authors:
“We found most MRI findings were not associated with future LBP-severity regardless of the presence or absence of baseline pain.”
And the signs don’t follow the pain either!
Another way to sum this study up: most spinal arthritis isn’t painful, which sounds a bit radical. But none of this is actually news. It’s just excellent new data that really drives the old point home that most back pain is not really about spines being all cruddy with arthritis.

![[Cover of Mind Over Back Pain, by Dr. John Sarno]](/assets/images/books/book-sar-s.jpg)
There are 701 more footnotes in the full version of the book. I really like footnotes, and I try to have fun with them.
Jump back to:
The introduction
Paywall & purchase info
Table of contents
Top of the footnotes
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help