Guide to Repetitive Strain Injuries
Five surprising and important ideas about repetitive strain injuries for patients and professionals

Anyone can get a repetitive strain injury, but running is like an RSI-generating machine.
Most of the time it’s hard not to heal. You couldn’t stop it if you tried. The body is going to recover from most kinds of injuries almost no matter what — it’s just a matter of time. As long as you were reasonably healthy before you were injured, and you don’t smoke or constantly ruin your sleep or otherwise make yourself biologically vulnerable, healing will almost always progress inexorably.
Chronic pain is different by definition: it doesn’t stop when it’s supposed to. Either healing fails, or the pain continues even when the tissues are actually fine, or an unholy mixture of the two. Overuse injuries or repetitive strain injuries (RSIs) like carpal tunnel syndrome and plantar fasciitis are slow-motion traumas that often seem immune to recovery — this is what makes them both terrible and fascinating. They are not as simple as they seem. There are (at least) five surprising facts about them that few patients or professionals understand:
- RSIs are not inflamed. Not the way we usually think of it, anyway. The idea of acute inflammation continues to be the basis for several dubious treatments. Jump to topic.
- RSIs are not biomechanical failures. They are not in general caused by crookedness or anatomical abnormality, and yet entire industries are devoted to “correcting” your posture, ergonomics, gait, and more. Jump to topic.
- RSIs often just need more rest. Stressed beyond their capacity to recover, the damaged tissues are almost always in dire need of substantial resting and careful management of loading for a long time — avoiding too much or too little, for quite a long time — but this tedious treatment option is often either ignored or recommended only half-heartedly, with the result that few patients ever do anything more than “take it easy.” Jump to topic.
- RSIs can be muscular. That is, they are routinely complicated by muscle pain, which is more treatable, and sometimes muscle pain is actually the entire problem — which is rarely diagnosed correctly, because most doctors and therapists remain more or less oblivious to how bad the “bark” of muscle pain can be. Jump to topic.
- RSIs play head games. Modern neuroscience is crystal clear on this point: the chronicity of pain is intensely psychological and neurological. RSIs are not “all in your head,” but — as with all chronic pain — they are certainly affected by what’s in your head. The state of tissues is amazingly modulated by the central nervous system. Jump to topic.
It’s shocking: although at least half of RSIs heal well,1 they include several of the world’s most infamously frustrating painful conditions. But treatment is overwhelmingly dominated by the myths about inflammation and biomechanics — myths that just won’t die, even decades after the scientific evidence started to debunk them. The nature of these conditions is largely unknown and the implications often ignored — tissues exhausted far beyond their limits that are never rested adequately, muscle pain complications that are rarely even diagnosed (let alone treated), and sensitivity to psychology that is mostly considered completely irrelevant.
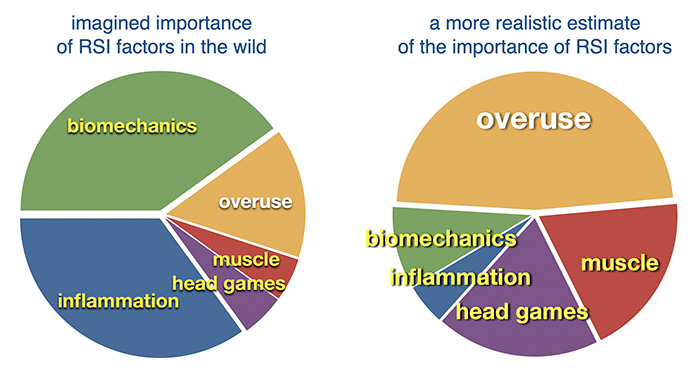
The real and imagined importance of factors in RSIs
Highlights: inflammation is given huge importance in the wild, but actually has almost no importance. It’s almost the same with biomechanics. The disparity is reversed for the importance of rest: it is hugely important, but virtually ignored in practice. Also barely noticed are muscle and “head games,” and they should definitely be solid blips on the clinical radar.
Where’s the fire? RSIs are not inflamed in the usual sense
Andres and Murrell in 2008:2
Recent basic science research suggests little or no inflammation is present in these conditions.
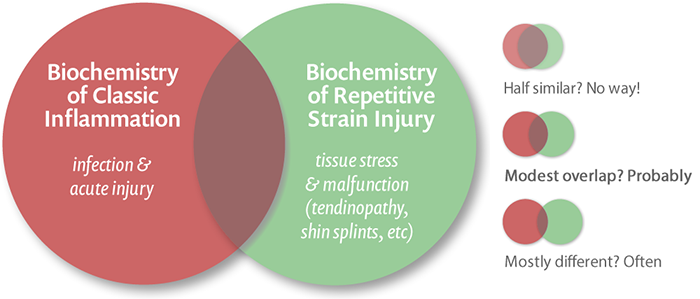
Repetitive strain injuries are still widely assumed to be inflammatory in nature, and that assumption is built right into the name in many cases: the Latin suffix “-itis” means inflammation, and it’s attached to the names of several of these conditions, such as plantar fasciitis, Achilles tendinitis, and supraspinatus tendinitis.3 The mental imagery of inflamed tendons or other anatomy is vivid, something like a car engine part overheating due to excessive friction. Maybe it is like that at first, but it doesn’t stay that way.4
What’s really going on probably has little in common with classic, acute inflammation — the only kind that people are really familiar with, from infections and acute lesions. In those situations, the immune system is out in full force to repel microbes. Under the microscope, the presence of white blood cells is the microscopic signature of acute inflammation. Clinically, things are red, warm, and puffy.
In RSI,
Numerous investigators worldwide have shown that the pathology underlying these conditions is tendonosis or collagen degeneration.
Healthy tendons look white and shiny, almost iridescent. That slick look is a direct consequence of the highly organized molecular structure of the tendon — the same reason that crystals are pretty. Tendons are made of extremely orderly protein molecules. But tendons suffering from overuse injury look increasingly dull, dilapidated, “grey and amorphous to the naked eye and microscopy reveals discontinuous and disorganized collagen fibres that lack reflectivity under polarized light.” (Sorry, no picture, alas.6) The unhealthy tendon looks grey because it has lost that organized feeling, right down to the molecular level. Its proteins have become a bit jumbled and irregular, and the result is a tendon that no longer looks slick.
The microscopic signs of acute inflammation are mostly but not entirely absent — they do crop up a bit, now and then. For instance if there is any actual tearing of the tendon or any frank structural damage, then you’ll see some of the typical signs of inflammation around the site of the tear, as with any other injury.7 But that’s torn tendon, a different critter. And certain types of tendinitis seem to be more prone to inflammation than others — not all tendons and stresses on them are the same, after all.8 But most cases of tendinitis seem to be dominated by the slow breakdown of the proteinaceous substance of the tendon itself.
That tendon “rot” is usually referred to these days as tendinopathy or tendinosis — osis meaning condition — not tendinitis. Although well described by microscopists and pathologists, tendinosis is not well understood — we know what happens, but we don’t know why or how.
Tendinosis is tendon degeneration without clinical or histological signs of an inflammatory response. It appears that tendinosis is the major, and perhaps the only clinically relevant chronic tendon lesion.9
It’s not just tendons that get “osis” — any overloaded tissue is a candidate
The imagery of anatomy “over-heating” with use, like a poorly oiled machine, is so compelling and mentally comfortable that it is virtually impossible, at first, for most people to imagine tendinitis without inflammation. But not all repetitive strain injuries are tendinitises, and this “osis” business doesn’t just apply to tendons. Other tissues involved in RSIs are also generally lacking in inflammation, but are degenerating and struggling to adapt to stress in similar ways.
Two common repetitive strain injuries involve fatigue of an even more different tissue: bone.
Fatigue of bone is probably a common factor in two of the major RSIs: shin splints (tibial degeneration) and patellofemoral syndrome (patellar degeneration). It’s easier to escape the cliché of classic inflammation when we’re talking about bones. We aren’t used to thinking of bone as tissue that would get inflamed (though of course it can — just break one). But what actually happens to over-used bone is suspiciously similar to what happens in abused tendons: it degrades and degenerates. In the case of the shin splints, eventually the tibia will break — a stress fracture — just as a degenerated Achilles tendon will rupture. But a break is preceded by a lengthy period of microscopic erosion. A 2006 paper found tibial “degeneration” in 100% of runners with shin pain.1112 One hundred per cent! For the math-impaired reader, that’s all of them.
Again, this tissue state is basically mysterious. But we can put together a clear general principle without going too far out on a scientific limb. Heavily used tissues are continuously rebuilding and maintaining themselves. If we push them so hard and frequently that the strain begins to exceed the capacity of the tissue to repair and maintain itself, then they will probably start to fall apart.13 (And just to keep this from being too simple, it’s also rather likely that neglected tissue also degenerates. Use it or lose it, anyone?)
It also makes plenty of biological sense that this degeneration would not involve a typical, obvious inflammatory process. Inflammation is primarily an anti-infection system and a function of the immune system, which is why it flares up at every break in the skin, and it even occurs internally without a real risk of infection (because of a fascinating mistake14). But if tissue is degenerating, there may be relatively few broken cells and not much reason for an immune response. The fundamental problem is more likely to be failed healing: that the cells can’t keep up with repairing minor damage to the connective tissue structures they are tasked with maintaining. The cells aren’t broken — they’re just like Lucy trying to keep up with the conveyor belt of chocolates.
And if tendinitis isn’t really an immune system “fire,” what does that suggest about common treatments and therapies for repetitive strain injuries?
“I think that they must have gotten injuries from patting themselves on the back so much… repetitive self-congratulatory strain injury.”
Sarah Weinman, regarding famous FBI profilers Robert Ressler and John Douglas, in a wide-ranging skeptical discussion about criminal profiling, You’re Wrong About: “Mindhunting with Sarah Weinman”
The other side of the story: don’t count inflammation out quite yet
Of course it’s more complicated. There is always another layer. The idea that tendons don’t get inflamed is based mainly on the absence of relatively obvious signs, the classic clinical and pathological signs of a vigorous immune response. But there’s almost certainly more to inflammation than redness and white blood cells swarming the tissue like police trying to control a riot. Inflammation is not one thing: it’s a dizzingly complex spectrum of cells, molecules, and processes, many of which are absent or different or just subtler in RSIs than they are in infection or acute injury. In fact, “classic” inflammation is probably a relatively minor tip of a much larger physiological iceberg.15 Consider that some inflammation is an actual malfunction, a straight-up case of mistaken identity — I’m referring to autoimmune disease, but also a more common “normal” mistake that affects everyone.16
But that is starting to change; experts have started to talk more about this. In a 2009 paper, tendinitis experts Cook and Purdam acknowledge that their basically non-inflammatory model of tendinitis nevertheless “can even encompass … some form of inflammation underpinning the cell and matrix response.”18 (That paper is required reading for pros, by the way.) More recently, in 2017, researcher Stephanie Dakin wrote: “the absence of clinically evident inflammation does not preclude an integral role for inflammatory mediators during the pathogenesis and healing of tendon injuries at a cellular level.”
Translation: just because you can’t see it doesn’t mean it’s not there. Or wasn’t there earlier. Maybe you just have to look better.
Dakin et al. looked better. They simply looked for more subtle signs of inflammation … and found them, seemingly without much ambiguity. Their paper in British Journal of Sports Medicine reported that painful and ruptured Achilles tendons “show evidence of chronic (non-resolving) inflammation.”19
That paper now stands as the best available evidence so far that rumours of inflammation’s demise in tendinopathy are greatly exaggerated/oversimplified. But there are no other important sources I’m aware of — Dakin et al. cite only their own evidence on this.
The inflammatory truth is in the middle
Looking at Dakin et al.’s results, it’s tempting to just concede that inflammation has made a comeback — it was never absent after all, it was just more subtle than the experts thought. Those goofy experts! Always changing their story! It wouldn’t be the first time that kind of oversight has happened in medical science, not by a long shot.
But — and this is important — the busting of the myth of inflamed RSIs remains valid in spirit, because plantar fasciitis is clearly not inflamed as most people understand it. Most anti-inflammatory treatments are aimed straight at classic, acute inflammation. Who cares if a tendon is “technically” inflamed if taking a drug designed to blunt a classic immune response is largely pointless?
With a Schrödinger’s-cat-like duality, RSIs may be both be and not be inflamed at the same time, depending on how you look at it, or when you look. It’s almost a bit of a word game whether or not to call the tissue disturbance of RSI “subtle, chronic inflammation” or just “something else altogether.”
This members-only area is about 7000 words (25 minutes of extra reading). Plenty of free reading continues below that — huge sections about “mechanical” factors, rest and load management, and the contribution of “muscle pain” — a total of about 19,000 words.
Most PainScience.com content is free and always will be.? Membership unlocks extra content like this for USD $5/month, and includes much more:
Almost everything on PainScience.com is free, including most blog posts, hundreds of articles, and large parts of articles that have member-areas. Member areas typically contain content that is interesting but less essential — dorky digressions, and extra detail that any keen reader would enjoy, but which the average visitor can take or leave.
PainScience.com is 100% reader-supported by memberships, book sales, and donations. That’s what keep the lights on and allow me to publish everything else (without ads).
- → access to many members-only sections of articles +
And more coming. This is a new program as of late 2021. I have created twelve large members-only areas so far — about 40,000 words, a small book’s worth. Articles with large chunks of exclusive content are:
- Quite a Stretch
- Does Epsom Salt Work?
- Heat for Pain and Rehab
- Your Back Is Not Out of Alignment
- Trigger Point Doubts
- Does Fascia Matter?
- Anxiety & Chronic Pain
- Does Massage Therapy Work?
- Does Posture Matter?
- A Deep Dive into Delayed-Onset Muscle Soreness
- Does Ultrasound or Shockwave Therapy Work?
- A Painful Biological Glitch that Causes Pointless Inflammation
- Guide to Repetitive Strain Injuries
- Chronic, Subtle, Systemic Inflammation
- Vitamins, Minerals & Supplements for Pain & Healing
- Reviews of Pain Professions
- Articles with smaller members sections (more still being added):
- → audio versions of many articles +
There are audio versions of five classic, big PainSci articles, which are available to both members and e-boxed set customers, or on request for visually impaired visitors, email me. See the Audio page. ❐
I also started recording audio versions of some blog posts for members in early 2022. These are shorter, and will soon greatly outnumber the audio versions of the featured articles.
- → premium subscription to the PainSci Updates newsletter +Sign-up to get the salamander in your inbox, 0–3 posts per week, mostly short, sometimes huge. You can sign-up for free and get most of them; members get more and their own RSS feed. The blog has existed for well over a decade now, and there are over a thousand posts in the library. ❐

Change or cancel plans any time. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism. For more information, see the membership page. ❐
PREVIEW: Headings in the members-only area…
- If there’s no fire, stop hosing it down: treatment implications of the lack of (classic, acute) inflammation
- Ibuprofen and friends: non-steroidal anti-inflammatory drugs (NSAIDS), especially Voltaren® Gel
- The commonest of common anti-inflammatories: vitamin “I” for ibuprofen
- “Mechanical” glitches are not important drivers of RSI
- The harm of hunting biomechanical bogeymen
- Like a rock in your shoe
- “Taking it easy” won’t cut it: RSIs mostly just need rest at first … and plenty of it
- Attitude adjustment usually required: the psychological barriers to resting
- Is there any science about how well resting works, or the best way to do it?
- Disrespectin’ restin’: the chronic underestimation of the value of rest
- Exercise is anti-inflammatory medicine for injuries
If there’s no fire, stop hosing it down: treatment implications of the lack of (classic, acute) inflammation
Effective treatment of athletes with tendinopathies must target the most common underlying histopathology, tendinosis, a non-inflammatory condition.20
Given the common assumption of acute inflammation, medications traditionally used to calm inflammation are the most popular first treatment choice. If it “burns,” take ibuprofen … and “cool” it down with ice. If it burns severely, inject something more potent: corticosteroids, the ultimate anti-inflammatory medication.
That’s the conventional wisdom. Many professionals never question it.
But there are serious problems here, and not just the fact that these treatments are supposed to get rid of a type of inflammation that mostly isn’t there in the first place. The biochemistry (even for icing) is just as complex as the inflammation they probably aren’t helping. They are known as “anti-inflammatories” because of their average effects on classic inflammation — on vigorous immune system activity and associated processes. How they affect the subtler, smouldering, chronic inflammatory biochemistry of an RSI is a more or less a perfect mystery.
We also need to consider the difference between treating pain and treating the pathology. Nothing is known about using medication to actually stop or reverse the degeneration of tissue that is failing under load. Medication for RSIs is entirely about symptom relief. And yet even for that relatively easy goal our ignorance is embarrassing: we don’t even know what makes RSIs hurt to begin with, let alone what will stop it. RSI pain is an infamously uninformative sign of the condition of the tissue. Alarmingly degenerated tendons can be amazingly painless. Ruptures often occur in people who didn’t even know they had a problem. So
So it’s hardly surprising that the collective track record of anti-inflammatory meds in this context is generally shabby and unpredictable, neither completely useless nor remotely reliable. If they worked well and consistently, obviously no one would ever need to read this. To whatever extent they do work for some people, some of the time, is due to unknown and variable chemistry.
What can we do in the face of so much uncertainty? It’s not an unusual dilemma in health care, and the solution goes like this: weigh guestimated costs and possible risks against the speculative hope of benefit, and then favour the options that are the least-bad attractive overall — the least expensive, risky, fussy, and implausible. So let’s apply that principle to some the “anti-inflammatory” options for repetitive strain injury …
Most drugs work on only about a third of the population, they do no damage to another third, and the final third can have negative consequences.
Craig Venter, extremely famous and spooky smart geneticist (public lecture, Vancouver, May 3, 2011)
Ibuprofen and friends: non-steroidal anti-inflammatory drugs (NSAIDS), especially Voltaren® Gel
Once upon a time, some scientists tested an “anti-inflammatory” treatment for tendinitis, something exotic: pifithrin-alpha.21 They had good smartypants reasons to try. PFT-α is a chemical that inhibits a protein, p53, that translates DNA into RNA, regulates the expression of hundreds of genes, making it (among many other things) “an important regulator of inflammation and extracellular matrix homeostasis.”
In short, PFT-α inhibits p53 … and that might ease inflammation in damaged tendons.
It backfired. It altered the inflammatory process, alright, which even looked good at first. But it didn’t make anything better, and then it got corrosive! It “reduced the collagen content” in both injured and healthy tendons, making them significantly weaker over just a few days. Oops. Tendons need p53 to be on the job, apparently.
The moral of the story: we really don’t know how to suppress inflammation … and it’s easy to break things trying. Although it sounded like a clever thing to try, this was the physiological equivalent of deleting part of a huge computer program that you think might be related to something you’re trying to solve. It’s effectively a crapshoot.
So what chance do we have against tendinitis with the commonly available options?
The commonest of common anti-inflammatories: vitamin “I” for ibuprofen

Vitamin “I” — ibuprofen, the main ingredient in drugs like Advil and Motrin — is an almost universal treatment choice for RSIs. (The main over-the-counter alternative, acetaminophen/paracetamol, is largely ignored for this purpose, which may or may not make any sense.22)
The drugs do ease “classic” acute inflammation and fever — something we learned long ago through trial and error — and tendinitis seems to be inflamed, so it’s a perfect match! Or people just take them because it’s a pain-killer and they have pain to kill. For one reason or another, nearly every patient and professional assumes that NSAIDs are at least somewhat helpful, though few are foolish enough to think it’s any kind of a cure.
In fact, the NSAIDs may be one of the weakest treatment options — because of course repetitive strain injuries are not actually very “inflamed,” per se.
Scientific evidence on this topic has always been scarce and discouraging, and even the anecdotal evidence for ibuprofen is weak. Nobody’s even “swearing by” this stuff for tendinitis.23
One rare and interesting example of useful research on this was a 2003 study that actually looked at the effect of diclofenac on inflammation itself. Interestingly, it did indeed show something — it reduce a couple inflammatory biomarkers, and “reduced both edema and the accumulation of inflammatory cells in the paratenon [similar to a tendon sheath].” Alas, this “did not translate into a reduction of tissue damage or a promotion of tissue healing,”24 and had no impact on the “mechanical properties” of injured Achilles tendons. Darn. Not that we were really expecting any of that.
Remember the story of PFT-α. In the same spirit as that more exotic failure, NSAID chemistry is also probably mostly irrelevant to the chemistry of RSI inflammation,26 biological ships passing in the night at best … or, just like PFT-α, they may even interfere with recovery from the connective tissue degeneration that actually is the problem.
And in fact there is evidence of that: NSAIDs may actually retard soft-tissue healing27 (and hard-tissue healing too, for the record28).
Oy! Just what every RSI victim needs! (Fortunately, they don’t actually damage connective tissue, like steroid injections. Probably.) There’s no direct evidence that NSAID use will impede recovery from an RSI, but it’s roughly as plausible as helping. Could go either way!
And it gets even worse with NSAIDs — there are numerous side effects, some of them serious. NSAIDs are also well-known as “gut burners” for their disagreeable and common effects on the gastrointestinal tract, which is a deal-breaker for many patients. And they can, paradoxically, actually cause headaches.29 Oh, and one more thing: they increase the risk of strokes and heart attacks, even in healthy people, at any dose. (Diclofenac [Wikipedia], a popular oral NSAID almost everywhere on Earth but North America, has even worse cardiovascular side effects than the others.30 Oral diclofenac specifically should probably be banned.) Lovely! NSAIDs definitely aren’t the best option for RSI, or even the best over-the-counter medication for the job.
A drug is a poison with potentially beneficial side effects.
Dale Favier, Massage Therapist, poet
I know some readers are thinking right now, “Yeah, well, okay … but I’m still going to take my Vitamin I.” With dosing caution — small doses, short-term use — I have no objection. If there’s any reason to take them, it’s that they might relieve some pain.
Or — and this seems almost crazy, I know — you could just actually heed the science, ignore the conventional “wisdom,” and never bother popping another NSAID unless you’ve got some uncomfortable acute inflammation to take an edge off. Contrast these outcomes …
- The (not-unlikely) worst-case scenario: slowed healing, aggravated pain, GI tract upset, increased chance of a stroke or heart attack, waste of valuable seconds popping pills.
- Best-case scenario: temporary modest pain relief, no side effects.
Speaking of dosing caution …
Voltaren is basically another NSAID (diclofenac, like ibuprofen) in a tube, and a relative newcomer to the range of options. Because you smear it on and it’s absorbed through the skin, you don’t have to carpet bomb your entire digestive tract and circulatory system with the stuff to get it to the problem — and this probably reduces your overall exposure to the risk of side effects31 (very real and serious with oral diclofenac), while still getting a respectable dose into the tissue with the issue.
Voltaren would never have been approved for sale if it didn’t have some promising evidence attached to it (see my main Voltaren article for details). The stuff actually seems to do something for arthritis pain — which may be physiologically somewhat similar to RSI, because arthritis is a bit like a slow-motion overuse injury to the joints. So Voltaren offers a shred of a reason for optimism here and greatly reduced side effects. Yahtzee!
That’s why Bussin et al. tested this in 2021. Their well-designed trial comparing it to a placebo showed … no difference at all. “The regular application of topical diclofenac for Achilles tendinopathy over a 4 week period was not associated with superior clinical outcomes to that achieved with placebo.” Dammit! One study is never the last word, but it’s certainly a discouraging one.32- Worst-case: It could be just as much of a chemical clean miss as any other medication, in which case you’re basically just smearing expensive Vaseline on yourself … and that's what one good scientific test showed.
- Best-case: It could conceivably actually provide some real pain relief, with very low risk of side effects.

Traumeel is a popular homeopathic cream for aches and pains. Even if it has actually has anti-inflammatory properties as advertised, most RSIs aren’t inflamed.
Traumeel — A very different sort of popular ointment, and it makes Voltaren look downright promising. Traumeel is a homeopathic product, which means that it’s a bogus, highly diluted Arnica cream. It is supposed to be “good for” basically any kind of ache or pain, but particularly anything that is supposedly inflamed. Indeed, the entire concept of Traumeel is that the herb Arnica montana has effects “like” the inflammation it supposedly treats … except that Arnica is supposedly anti-inflammatory.33 So this remedy does not even follow homeopathy’s own ridiculous rules! But piling irony upon ineffectiveness, Traumeel is mainly being used as an anti-inflammatory for conditions, like tendinitis, that aren’t even inflamed in the conventional sense.
So this is a product with questionable effectiveness in general, being recommended to treat inflammation that isn’t there, on the basis of a principle of homeopathy that wouldn’t apply even if it made sense. But the details truly don’t matter, because homeopathy is the snakiest of snake oils, and always was. See Does Arnica Gel Work for Pain? and Homeopathy Schmomeopathy for much more information. It’s impossible to overstate how much weirder homeopathy is than most people think. Most people think it’s just herbal medicine — but it’s much stranger than that!
Therapeutic ultrasound. From the edge of alternative medicine to the heart of the mainstream: another popular inflammation-assuming treatment for tendinitis is therapeutic ultrasound … and it’s just about as over-rated as Traumeel, despite its mainstream-ness. Although modern in the big picture, this is a technological therapy that was around for decades before the rise of evidence-based medicine, still found in most physical therapy clinics on Earth — and now increasingly replaced by fancier, more intense “shockwave” ultrasound. Take one look at these machines, and you’ll be convinced it must be good for something, because that’s a whole bunch of technology and industry that’s just going to waste otherwise. Unfortunately, they could win a prize for seeming more legitimate than they are. It has been clearly proven effective for … nothing whatsoever that I am aware of. And not for lack of trying. This is not to say that it never works for any RSI or any person, but it also falls very far short of being clearly evidence-based medicine. I do a full tour of the evidence in another article: Does Ultrasound or Shockwave Therapy Work? They seem like mainstream physical therapies, but warming and vibrating tissues with sound/pressure waves has never been supported by good evidence.
Icing. The apparent value of icing for seemingly “hot” pain is mostly the poetic, non-medical mental imagery of cooling. The problem is not heat, of course, and it can’t be fixed by cooling. If ice can help a repetitive strain injury in any way beyond brief numbing, no one has ever actually proven it,34 or even shown how it might work.
You may have heard that icing actually “interferes” with “natural” inflammation and should be avoided. That’s speculative and quite possibly wrong. You may have also heard that “even the guy who invented the RICE protocol is against icing now,” and that is simply mistaken: that is not what he said, but it has been widely oversimplified in that way. I explain in the introduction of my icing article.
Just as we can speculate that icing might impair healing, we can also reasonably speculate the opposite: it might stimulate miscellaneous minor tissue healing processes. Virtually any stimulatory input to the body, up to a point, can provoke a healthy response, because of the use-it-or-lose-it principle. Stress a tissue, and it will probably get tougher in some way. In broad strokes, that is probably the only plausible therapeutic mechanism of icing. Ice may simply be one of the easiest delivery systems for a bit of non-toxic stimulation — a way to stimulating tissue without overloading it, while simultaneously getting some temporary pain relief from numbing. However, it certainly isn’t “anti-inflammatory” in any meaningful sense as far as anyone has ever shown.
I’ve saved the “best” for last. If “best” means “most complicated and interesting”…
Corticosteroid injections and iontophoresis35 deliver an allegedly potent medication right to the source of the problem (hopefully) — think of them as ibuprofen on, er, steroids. Steroids certainly do have anti-inflammatory properties, in spades: they strongly and broadly suppress immune function. Steroids can work marvels, especially with systemic diseases where the immune system is rampaging out of control. The classic example is the drug prednisone, which has nearly miraculous and often life-saving benefits.36 The price of that potency? Side effects! Many and serious. You cannot generally suppress immune function without consequences.
And so oral steroids are rarely if ever used for RSIs: no point in soaking your entire system in the stuff when you can deliver just where it’s needed.
But even then, there are serious concerns. Steroids also eat away at connective tissue — the same tissue that is already in trouble in most RSIs.
There is half-decent evidence that injecting steroids right into the heart of an RSI can help, especially in the short term. The evidence for short-term benefit is particularly clear in the case of tennis elbow (lateral epicondylitis),37 although there is also evidence that the long term results are much less rosy (or even nasty). It’s reasonable to assume that the effects on other RSIs are a similar mix of good news and bad news, and the evidence confirms that.
For instance, the results of a 2009 study were weird: quite good for hip pain in the short term, but quite poor in the long term, suggesting that not only did the benefit not last, but there was actually delayed harm. Many months later, these patients who did well at first were actually still suffering quite a bit compared to people who did other therapies.39
The notorious rotator cuff of the shoulder is a hotbed of tendinopathy, and one of the most common targets of steroid injections. A 2017 review of 11 studies of 700 patients was particularly scathing. Mohamadi et al.:40
Corticosteroid injections provide — at best — minimal transient pain relief in a small number of patients with rotator cuff tendinosis and cannot modify the natural course of the disease. … Their wide use may be attributable to habit, underappreciation of the placebo effect, incentive to satisfy rather than discuss a patient’s drive toward physical intervention, or for remuneration, rather than their utility.
Ouch. But note that even those authors affirm the temporary benefits. So did the flawed but huge and useful GRASP trial in 2021, which showed that there was no clear difference between the efficacy of steroid injections and exercise after a year.41 But steroids did help many of those people in the short term.
If RSIs aren’t acutely inflamed, then why is a powerful “anti-inflammatory” medication ever effective? Some possibilities:
- Maybe steroids don’t work as well as we are all in the habit of thinking (which seems increasingly likely as the years tick by and we see more reviews like Mohamadi et al.). There might not be all that much a treatment effect to explain. Real but minor.
- Maybe RSIs cause more immune dys/function than it looks like. This is my pick. It’s not hard to imagine that even just a few well-armed neutrophils could wreak disproportionate havoc. As discussed above, RSIs are not un-inflamed, just inflamed differently.
- Maybe cortisteroids are helping for some other reason altogether, a happy biochemical accident — because steroids have many roles in physiology. For instance, they could have an effect on nerve pain, but not inflammation.42
Steroids in a needle are much less risky than steroids in a pill. Just like with the difference between popping NSAID pills and rubbing them on in a cream, injection limits your exposure to one spot. The main risk — and it’s not nothing — is that steroids eat connective tissue. Slowly. It’s not like strong acid. Except when it is!43 This probably explains the data about long term harm …
It is clear that corticosteroid injection into tendon tissue leads to cell death and tendon atrophy. As tendinosis is not an inflammatory condition, the rationale for using corticosteroids needs reassessment, as corticosteroids inhibit collagen synthesis and decrease load to failure.44
Since the nature of repetitive strain injury is that tissue slowly “rots” and frays under stress, steroid corrosion of connective tissue is an ironic hazard — steroids may dangerously exacerbate the basic problem even as they relieve pain. The risk is obviously worst in the case of classic tendinitis, where structurally critical tissue may be weakened. Few people are keen to increase the risk of a rupture just for some short-term pain relief! That’s why physicians wisely limit steroid injections to about three (although that may be overly cautious).
The saving grace is probably that the negative effect on connective tissue integrity is probably minor with limited dosing. Nevertheless, it is an unfortunate collision of potential benefit with potential risk, and some experts have concluded that the evidence is too negative in the long term to keep recommending the treatment.45 There are too many variables and uncertainties here to make a blanket recommendation for all patients: you have to weigh the pros and cons decide for yourself whether you want to “go there.”
- Worst-case: No benefit, direct worsening of the problem (accelerated degeneration of connective tissue), and a poorer long term result.
- Best-case: Significant short term pain relief without any significant adverse effects, and a useful aid in rehab.
“Mechanical” glitches are not important drivers of RSI
You’re probably not suffering from an RSI because of crookedness, asymmetry, poor posture, or "dysfunctional" movement. I will not argue that these things don’t matter at all, but I strongly argue — based on a lot of evidence and experience — that their contribution to the problem is relatively minor, mostly drowned out by overuse itself. Most garden variety kinesiological glitches probably contribute less than 10% to the problem. That might ramp up to 20-30% for the worst glitches in people without some obvious biomechanical oddity.
Just as we find it almost impossible to think of tendinitis without also thinking of the fires of inflammation, we also find it too easy to assume that this failure is the result of some kind of malfunction of a beautiful system of pulleys and levers that has somehow gotten “outta whack.” This extremely strong mental bias is known as “structuralism” or the postural-structural-biomechanical model for pain. To quote myself, from a much more thorough article on this topic:
Structuralism is the excessive preoccupation in the physical therapies with biomechanical factors in pain problems — the biomechanical bogeymen.
Structuralism is a plague on pain and injury medicine, still burning out of control well into the 2020s. But nowhere are the biomechanical bogeymen more numerous than in speculation about the origins of the common RSIs!
One of the best examples of a structuralist theory of an RSI is impingement of the supraspinatus tendon of the shoulder. The idea is that the tendon has limited room between the humerous and the shelf of bone on top of the shoulder (the acromium). It’s a narrow space, and it gets narrower when things are irritated. And so it makes all kinds of “common sense” to make some more room in there — with a scalpel. Zillions of surgical decompressions have been done for people’s pinched supraspinatus tendons … all of them in vain, because as much sense as it seems to make, it’s just wrong.46 The surgery doesn’t work, because the problem is not fundamentally a “mechanical” one. It’s just not a disease of tendon-pinching.47
That is just one of many common-sensical treatments that have been proven ineffective in the 21st Century.48
The problem is that the only biomechanical problems that are much of a problem are the really obvious ones — so obvious they mostly don’t need diagnosing, and are often impossible to fix anyway. Conversely, any problem so subtle that it can’t be diagnosed easily is also not likely to be much of a problem. Most RSI sufferers have no obvious deformity or bizarre walk or blatant muscle wasting. If there’s anything wrong with their biomechanics at all, it isn't adding very much stress to the equation … and yet these theories inspire most of the expensive therapy for RSIs.
Therapy for RSIs is usually barking up the wrong tree. It’s not that these problems don’t exist, it’s that they don’t deserve anywhere near as much time and money as they get.
The harm of hunting biomechanical bogeymen
Treatments for RSI inspired by inflammation are largely inexpensive and harmless (as long as you don’t overuse medications). If you really want to spend money and risk harm, then what you want rehab inspired by the fear of biomechanical glitches: they’re expensive, time-consuming, and risky in a variety of ways, from direct harm to actually making the problem worse.
Surgeries are the easiest to pick on, and unnecessary operations for RSIs are certainly a huge problem.
But others are just as bad. Alternative therapies like chiropractic and massage therapy can burn through many hours and thousands of dollars in pursuit of a more aligned version of yourself — all largely wasted.
What about mainstream rehab, coached by a physical therapist? Maybe someone who has helped elite athletes? These therapists can be just as misguided, entrenched as they often are in the paradigm of “corrective exercise”49 — lots of tedious exercises that are allegedly technical and advanced, but just as futile as trying to “correct” patients with spinal manipulation or fascial stretching.
A truly amazing amount of effort goes into trying to diagnose and treat patients with repetitive strain injuries as if they are malfunctioning in some way. It’s all rather costly in poorly spent time, money, and focus — none of it matters if the tissue continues to be stressed beyond what it can cope with, which is easy to do without a single biomechanical glitch.
It’s all such a major distraction specifically from what really matters: actually resting the tissue. Indeed, structuralist prescriptions are routinely not just aimed at the wrong target, but also involve premature and excessive exercise — just too much, too soon, which is precisely the opposite of what most RSIs need in the early stages of rehab. Loading the tissue can be very helpful, but there is a powerful no-pain-no-gain bias in rehab culture that skews decisions dramatically towards trying to "fix" things with intensity.
Like a rock in your shoe
Once the degeneration of stressed tissues has set in, it’s a bit of a freight train: even if you can successfully identify and correct a subtle biomechanical dysfunction that contributes to it (which is a long shot), it won’t change the forces on that anatomy very much. The “strain” in repetitive strain injury is mostly caused by the ordinary excessive load on anatomy, not by minor imperfections in biomechanics. A biomechanical problem might make some anatomy slightly more prone to failure, but it’s still the overuse that is the main issue.
This is what I call the rock-in-shoe problem: when you have a rock in your shoe, and it starts to cause extreme pain, it’s really not going to help you very much to slightly change your gait, which can only reduce the forces on your foot a little bit. Even with a crazy limp, you still have to put your foot down! What you really need is to get rid of the rock. And if you don’t have the option of taking off your shoe — if the “rock” is built right into your tissues — then your only option is to stop using that anatomy.
Consider supraspinatus tendinopathy again: the rock-in-shoe analogy does a great job of explaining why surgery doesn’t work. The tendon is the “rock” — a painful bit of anatomy stuck in a tight space. The surgery is like loosening your shoelaces a bit. You get a little relief, maybe, and then you’re right back where you started: the “rock” is still there! Fortunately, this rock will slowly get less painful on its own over time.
Much more information about structuralism and the downfall of the postural/structural/biomechanical model of pain is available here:
“Taking it easy” won’t cut it: RSIs mostly just need rest at first … and plenty of it
“Rest” means savvy “load management” that errs on the side of less in the short term. Exercise is a vital part of recovery, but the dosage is critical and it has to be patient baby steps for months. Almost everyone tries to do too much, too soon. Doing it right — doing it slowly and carefully enough — definitely feels like “rest.”
The truth is boring and simple: rest is powerful medicine for RSIs, but also tedious and often spectacularly inconvenient, even a threat to jobs and careers. This boring “miracle cure” is almost never adequately emphasized to RSI patients.
I put the scare quotes around miracle cure because it’s only half wrong. Rest really can be a something of a miracle cure: entrenched RSI cases can still be tamed with an effective resting strategy, long after the patient has given up, years after starting to say “I’ve tried everything.” Although there’s nothing actually miraculous about such a late victory over an RSI, it can certainly seem that way to the patient.
On the other hand, rest does not get full miracle-cure status, because there are quite a few cases that cannot be successfully treated with rest. Rest usually fails because there is something going on that cannot be rested from, an aggravating factor that cannot be eliminated or avoided.50
Regardless, it’s certainly worth trying, and trying well.
One of the things that makes rest particularly relevant to repetitive strain injury is that there is good evidence that it takes a long time for degenerated connective tissue structures to recover. Tendon is metabolically sluggish. It “breathes” only about 10–20% as much oxygen as muscle — a measure of metabolic activity — and even muscle isn’t exactly lightning fast with recovery.51 We know tendons can heal — from some fascinating studies of traces of nuclear bomb tests embedded in tendon52
— but it’s not a quick process.According to Khan et al., it may take as much as two to three weeks of rest before a tendon even begins to start rebuilding, and then the rebuilding itself is achingly slow: about a hundred days for the tendon cells to produce the collagen molecules that make up the bulk of a tendon. That’s three months.
Anyone who has had a sprain (torn ligament) knows that connective tissue is slow to heal. A ripped ligament is usually never quite the same ever again, and spends many months feeling unpleasant after the injury. It’s no different with tendinitis, or any other severely fatigued tissue. “Taking it easy” for a little while simply isn’t going to cut it. This is bad news for a lot of patients, of course … but the biology is what it is.
Attitude adjustment usually required: the psychological barriers to resting
People have an odd tendency — even after a lot of suffering — to act like repetitive strain injuries are relatively minor injuries that “should” get better if they “take it easy.”
Unfortunately, no one sent the RSIs the memo about this, and they refuse to actually be easy to fix.
People can easily go on suffering for years with awful consequences to their lives. There’s nothing minor about a chronic RSI, and the effort and inconvenience involved in trying to beat one has to be scaled to match its severity. If you have a really nasty RSI that is keeping you from working and/or playing, you need to get serious about truly giving it some adequate rest.
This is a psychological hurdle, not a physiological one.
Another major problem with resting as a treatment strategy for RSIs is almost political in nature: therapists and doctors are so preoccupied with treatments based on the assumption of inflammation and biomechanical factors that they fail to emphasize the importance of rest. In many cases, it’s not that they don’t think the rest is important — they do, and they might even say it. But their words have little weight when their actions are devoted to every other possibility. The importance of rest simply doesn’t get the conversational air time that it needs for the message to sink in, often not even from therapists who actually believe it matters.
Is there any science about how well resting works, or the best way to do it?
Not really, no. We really essentially nothing about appropriate exercise dosage for any kind of chronic pain, and the exercise dosage is just a mirror image of resting dosage: less exercise is the same as more resting.53 One of the main conclusions of a major review of “How much is too much?” is that there’s not enough research, and what we do know is mostly from limited data about a few specific sports.54
There are scraps of relevant research here and there, but mostly we have to read between the lines of research on the risks of excessive loading in sport. If too much loading, too fast, is the major risk factor for injury, that strongly suggests that less and slower loading — “resting” — is probably effective injury prevention… and what prevents RSI often also treats it.
Extra early emphasis on resting is not a proven strategy, but I am not exactly going too far out on a science limb by recommending it.
Disrespectin’ restin’: the chronic underestimation of the value of rest
Unfortunately, there are also many examples of rest being dismissed and deliberately de-prioritized as a component of rehab.
For instance, at odds with the evidence, a chiropractor might tell a patient that “no amount of resting will help” because the real cause of the injury is a tilted pelvis, which will require a dozen “adjustments” in the short term and then long term occasional maintenance. In these all-too-common cases, structural therapy has eclipsed resting as an option, and is logically at odds with it. (And this is greatly complicated by the awkward truth that, once in a while, there really is a biomechanical factor that is going to make rest less effective. But that’s rare.)
What patients need are professionals who aren’t locked into structuralism, who have biomechanical theories of RSIs in perspective, and do not recommend “repairs” to alleged structural factors at the expense of resting. But if you have a therapist who only ever (or almost always) thinks in terms of hunting down biomechanical causes for RSIs, then that therapist will place the emphasis of treatment on the wrong thing almost every time.
Even when structuralism isn’t the causes of the distraction, rest still gets short shrift. Even when the rehab plan is just bog standard conventional load management, mostly just baby steps back to normal function — but not the first steps. Everyone is in such a damn hurry!
Exercise is anti-inflammatory medicine for injuries
Exercise has anti-inflammatory effects that combat systemic disease quite brilliantly over the long-term. But what about pain and injury? Especially common repetitive strain injuries like Achilles tendinitis? Is exercise anti-inflammatory for those? Is it like popping an ibuprofen, or … better?
Can you help an overwhelmed tendon by using it more? In the short to medium term? Maybe. Many people will overuse an overuse injury, while others fear wear and tear too much, and those extremes might obscure a valuable sweet spot in the middle — and that is what the science hints at so far. This section explores this possibility in detail, with particularly thorough referencing, especially for the critical premise that “running doesn’t cause arthritis.”
This fact has now spent many years on my top 10 list of things that huge numbers of people still don’t know, but should. If you’re going to believe that exercise is medicinal for joints and tendons, you have to start by accepting that it’s not harmful.
Many people ironically overuse an overuse injury while trying to recover from it, pushing back towards normal too hard, too soon. Overdoing it is the most common of all training and rehab errors, I suspect. Thanks to a strong cultural predilection to believe that there is no gain without pain, the need for rest in the early stages of rehab is often underestimated.
Another irony: the same culture that celebrates intensity in rehab also fears wear and tear out of proportion to the danger. Some people are afraid to push even a little! And that’s also a problem. Overuse can go very badly, which understandably makes some people shy of using their body at all. No one wants another stress fracture!
But tissues clearly thrive on stimulation, and it’s hard to damage them. For instance, we know — from many studies — that even quite a lot of running does not destroy knees with premature arthritis. And here are a whole bunch of citations for that statement, a collection I’ve been curating for about a decade.56575859606162636465
Exercise doesn’t wreck joints because it probably does the opposite: at the right dosage, exercise is probably anti-inflammatory. It probably protects joints and promotes healing.
But getting the dosage right? That’s the hard part! People often go to the extremes during rehab: too much too soon, or too little too late.
Every overuse injury must eventually once again be used. No cartilage, bone, tendon, or muscle can get healthy — or stay healthy — without some action. But when and how much? And if we get it right, can exercise actually be therapeutic for RSIs? Can it rush recovery?
As established above, RSIs are indeed inflamed even when chronic — it’s just subtle. And exercise probably is actually anti-inflammatory — more than most things that are supposedly anti-inflammatory, like ibuprofen. Indeed, it may be the only effective way to manage inflammation long-term. We’ve known this in a broad sense for decades, known that it’s the major mechanism for how exercise prevents cardiovascular disease.66 But we continue to refine our understanding, and exercise probably works its anti-inflammatory magic in musculoskeletal medicine as well.
For instance, in a 2019 experiment, scientists mechanically stressed samples of excised cartilage and cartilage cells, and the loading actually reduced inflammatory signals produced by these cells.67 Cool.
We know that nasty inflammatory back pain — autoimmune disease — actually backs off with regular exercise.68
And so on. There are mountains of indirect evidence like this, many good clues that “load management” matters for preventing and treating injury.69 For instance, when a couple dozen Norwegian students spent the summer doing “progressive and individualized” training, they got hurt quite a bit less in the fall than students who didn’t prepare.70
We clearly do get in trouble with both too much and too little loading, but mechanical loading in the Goldilocks zone probably does the opposite by easing inflammation: a specific and substantive reason why “exercise is medicine” for distressed tendons as well as heart disease.
Is there direct evidence to confirm this? Yes-ish …

I keep talking about “exercise,” but I specifically and mainly mean resistance training, weightlifting — because it’s probably the best way to load specific tissues precisely.
Sports medicine suffers from its usual bizarre shortage of exactly the evidence it most needs, but there are some examples that come close …
- A good quality trial that clearly showed “good, lasting clinical results” for two kinds of exercise for Achilles tendinitis.71
- Another respectable trial of heel lifts also reported good results for plantar fasciitis.72
- The encouraging body of evidence that “exercise therapy benefits patients with patellofemoral pain.”73
- And much the same consensus about strengthening for tennis elbow: “Strengthening … is effective in reducing pain and improving function for lateral epicondylosis but optimal dosing is not defined.”74
But “optimal dosing is not defined” is a problem with all of the evidence, and might be why there are also a bunch of discouraging studies. Dosing alone can probably make or break exercise-as-medicine for an overuse injury, and yet it’s just impossible to know exactly what the just-right dose is. It’s a moving target and a function of many variables, many of them unknowable in practice. For instance, we can easily think they we slept better than we actually did. Or a minor infection draining our physiological resources, undetectable except for feeling a little extra tired or slightly oogy.
We have good reasons to try to get the dose right, though — by backing off a bit on those “off” days, even though we really have no idea what's going on or exactly how much to adjust our load. Those guesses are going to be wrong sometimes, but, if you grok the principle, you can probably improve your accuracy.
And if you get it wrong, if you fail to do good, or if you even make a tendon a bit worse for a couple days? Fortunately, exercise (as always) has its great consolation prize: truly major general health benefits. If you’re going to fail … fail fitter!
Resistance training is a terrific rehab tool not because strength is inherently therapeutic (though it might be), but specifically because it’s a great way to regulate exercise dosage. It can be tidy and precise, and you really want that when you’re doing your best to get the dosage right — you can’t control a lot of other variables, but you can at least control that.
Common anti-inflammatory medications are probably not biologically relevant to the rather subtle, chronic inflammation that characterizes repetitive strain injuries. But exercise is, presumably, highly relevant: it gives the body the only medicine that was possible for millions of years of evolution. Our job is just to tinker with the dosage — which probably means being more patient in the early stages than most of us want to be. And some need to be a bit braver.
All my evidence-inspired speculation about exercise being “anti-inflammatory” for tendinitis and other overuse injuries could be wrong, and it would still be a great idea to try — because it’s an extremely healthy activity otherwise.
↑ MEMBERS-ONLY AREA ↑
The sneaky factor: RSIs can be muscular
Every patient with an RSI, and every healthcare professional treating patients with RSIs, should understand how surprisingly often muscle is a major factor, or even the entire problem. Large numbers of patients are diagnosed with a repetitive strain injury, when what they primarily have is a problem with trigger points, more commonly referred to as muscle knots. Or another way to look at this: muscle can also be repetitively strained, and it often is along with tendons and other anatomy.
What makes trigger points so clinically interesting is their triple threat: their ability to cause problems, complicate problems, and mimic problems. No matter what else might or might not be going on, muscle is often involved one way or another, either getting uncomfortable in reaction to another painful problem, or having its own problem that seems suspiciously similar to another kind of problem, or malfunctioning in a way that significantly aggravates another problem. Let’s take those three things, and look at how they specifically affect RSIs …
Muscle dysfunction/strain as a direct cause of RSI
I went to great pains above to explain how biomechanical issues are not generally a very significant factor in the development of RSIs. However, I also took pains to emphasize that there are some exceptions: and probably the most common kind of exception is that RSIs may be significantly affected or almost entirely caused by muscle fatigue. And this factor, although it has much in common with structuralism, is usually not diagnosed and treated by structuralists, despite the fact that it’s probably quite a bit easier to do so — and more useful — than with most of the more traditional structuralist issues.75
Consider this (oversimplified) example: if you run a lot, and your Achilles tendon cannot quite keep up with the forces you are subjecting it to, it could simply be all the running that is causing the strain, but it could also be the strain on the muscles pulling on the Achilles tendon and/or excess tension applied to the tendon. How much more quickly will you develop a case of Achilles tendinitis if you have also have a major muscle knot in the middle of your gastrocnemius? How much less running will it take before you’re into the “overuse” zone? No one knows the specific answer to those questions, but muscle tone/tightness is probably relevant, and in some cases tension may be so high that the threshold for injury is lowered to the point where it can hardly even be considered to have been brought on by overuse. If injury happens so easily and so fast that overuse doesn’t actually seem to really be the issue, I would consider trigger points and muscle tension to be the real, main cause of the injury, not “overuse.”
One of the strengths of this theory is that, unlike the biomechanical theories, it’s not very subtle, or complicated. Many of the biomechanical theories suffer from excessive subtlety, from very complex and fragile changes of reasoning. But there’s nothing subtle about the idea of having an inflexible, tight muscle yarding on your tendon much harder than it should. Nor is there anything too exotic about treatment. Although exactly what muscle tone is, how trigger points work, and how best to treat them, is all full of scientific mystery, there is no doubt that it is often possible for muscle to “loosen up.” Because treating trigger points can be relatively cheap and almost totally safe, and given that trigger points probably have more to do with many cases of RSIs than any other kind of biomechanical problem, it’s well worth your time to investigate trigger point therapy as a treatment option.
But that’s just the tip of the iceberg!
Muscle pain as a complication of RSI
I do not think cases of RSIs with a significant component of muscle tension are common. Most of the time I suspect it’s merely a case of muscle tension mildly predisposing the patient to the injury — not nearly enough to be considered the cause. But muscle also tends to react negatively to any other kind of pain problem. And that is much more likely to be involved in nearly every RSI case. As common as muscle pain is, most people radically underestimate just how unpleasant it can be.
Take the case of classic carpal tunnel syndrome, where median nerve impingement is significant and confirmed by a nerve conduction test: the nerve cannot work properly, and a whole bunch of symptoms are coming directly from that. There is very low diagnostic ambiguity in such a case. And yet, there are also some other symptoms: diffuse aching throughout the entire forearm, heavy deadness of the limb, a weakness that seems to go beyond just the grip strength affected by the median nerve, and pain in the hand that definitely goes beyond the irritation in the wrist. All of these symptoms are common with cases of carpal tunnel syndrome, and they are all mostly caused by trigger points in the musculature of the forearm — trigger points that were probably present to some degree before everything went to hell, but then got really aggravated in response to the meltdown in the wrist. Treating those trigger points will not cure the carpal tunnel syndrome … but successfully treating them does have the potential to relieve a very large portion of the symptoms. I’ve seen cases of carpal tunnel syndrome that, when trigger points were treated, reduced in severity so much that it was pretty much just as good as a cure. A little numbness and tingling and weakness left in the hands, and the occasional aching in the wrist at night, is certainly still a problem … but it can seem quite trivial compared to the full-blown power of carpal tunnel syndrome plus trigger points.
This phenomenon is quite familiar to most alert massage therapists. It’s relatively obvious that muscle feels awful in the region of other problems. It’s often a bit of a shock to the patient how much of their discomfort can be accounted for in this way, and treated or managed relatively easily.
But that’s still not all …
Muscle pain as a mimic of RSI
Another way that trigger points can “cause” repetitive strain injuries is by outright mimicry: by producing symptoms so similar to RSIs that they easily fool the patient and most healthcare professionals.
A classic example of this is the confusion between trigger points in the hip and “bursitis”. As I mention every chance I get, this condition is almost hilariously over-diagnosed by front-line physicians, and I have enjoyed teasing doctors about it for years: it really does seem sometimes like every single musculoskeletal problem that lands in front of them is “bursitis,” unless there is some other really obvious diagnosis, and sometimes even still then.
I kid the docs. I exaggerate. But not very much.
The musculature of the hip is one of the major gathering places in the body for trigger points. And they cause pain that often feels just like bursitis. Well, not quite “just like”76 — but very similar. For the average healthcare professional and patient, intense and irritating pain on the side of the hip is really very easy to mistake for bursitis.
There are several other clinical scenarios like this: when the pain of muscle just flat out feels like something else, and gets diagnosed as something else. And it’s not all that unusual a clinical situation to have two versions of the pain problem: the real thing, and the trigger point that feels exactly the same or very similar, overlapping. Lovely!
All together now …
Imagine the clinical power of these three muscle issues when they are all combined: knots in your muscles that predispose you to genuine RSIs, knots that make genuine RSIs feel much worse, and knots that just flat-out imitate them.
There is a great deal to learn about trigger points, which is why there is so much about them on this website: they’re clinically relevant to just about everything, and they’re mysterious and complex. But once again, treating them in many cases is relatively cheap and safe, and that’s what we like to hear whenever we’re talking about treatment options. Even if I’m wrong, even if I’ve overestimated their importance, you really can’t go too far wrong investigating the possibility.
This seems like a good time to plug my muscle pain tutorial again:
This educational website provides more than 240 free articles about pain problems to hundreds of thousands of visitors each month, funded by the sale of 10 e-books about some of the most common and stubborn painful problems. Like this one …
The spooky factor: RSIs play head games

RSIs involve a perfect storm of anxiety-producing characteristics that can actually — yikes! — damage your nervous system.
We’re not used to thinking of RSIs as a neurological problems. RSIs are about worn out tissues, not neurology. And yet your brain is the boss of you, the boss of everything. For instance, we know that the reaction of tendons to overuse is mediated by the central nervous system.
For instance, in 2011, Andersson et al. studied how rabbit tendons responded to exercise over a period of weeks (a relatively harmless experiment for the rabbits, as these things go).77 Unsurprisingly, the rabbits’ tendons started to show signs of adaptation and then overuse. The surprising part was that only one side was artificially exercised, but both sides reacted! Changes in the tendons were obviously neurologically regulated: like a slow-motion reflex reaction on sides, reacting to the stimulus on one side.
All stubborn pain problems play “head games” with patients — there’s almost no avoiding it. Chronic pain, almost by neurological definition, involves at least a little haywire neurology, because pain itself changes how pain is processed … and not in a good way.
Every pain problem is disturbing one way or another, but RSIs have a particularly disturbing quality: they specifically strike at our work and our play. Rare is the RSI that happens because of something we didn’t have to do, or want to do. It’s always the typing that we must do, to pay the rent, or the golfing that we want to do, so that life is worth living. And it’s usually the activity we need or want the most, because that’s the one we’re doing the most.
It’s tragic and it’s anxiety-producing, and that makes things hurt more. Pain science research is extremely clear: the emotional context of a pain strongly affects its severity and chronicity. The soldier wounded in combat is often amazingly pain-free — because he knows that his wound is a ticket home. The same traumatic injury in a construction worker with three small kids, a sick wife, and credit card debt will produce massive anxiety, and his pain will probably be much worse. RSIs also routinely interfere with our ability to make a living, but their anxiety-producing super power goes even further.
The traumatically injured construction worker may be in a dire situation, but at least he knows exactly what he’s dealing with. He knows what happened to him and — barring complications — about how long it will take to heal. But the pain of RSIs rarely “computes” for the patient, and because it often worsens with time and use, there is no end in sight.
This is a perfect storm of anxiety-producing characteristics, and RSI patients often show signs of severe emotional fatigue. They usually can’t sleep right, either from the pain or the anxiety or both, and the lack of sleep is yet another major aggravating factor.
The coup de grace is that all the anxiety and suffering can actually change neurology, making patients more sensitive to pain. This is the phenomenon of central sensitization.78 It is the mother of all common denominators in musculoskeletal medicine.
And it gets even worse. Everything I’ve written here so far suggests that sensitization can be a complication of an injury. But what if you were sensitized to begin with? What if people actually got RSIs because they were already sensitized? That’s not just speculation: it is strongly suggested by the results of a 2015 study of two thousand patients with arthritic knees.79 They showed that the patients who hurt were not the ones with the worst knees, but with the worst sensitivity: a trait, not a state. A “trait” of the individual, not the “state” of their knees. It’s not that the worst they had bad arthritis, it’s that they had problems tolerating arthritis.
Never bet against neurology. It’s probably a much larger factor in RSI than has yet been fully appreciated by anyone. It is easy for health care professionals to pay lip service to sensitization without really taking it seriously. It is obvious to almost anyone that fear and frustration make a bad situation worse, but it’s quite another thing to fully respect the therapeutic implications of your nerves, spinal column, and brain actually changing. It has many important implications for treatment, and yet most therapists waste time trying to find and change biomechanical issues that are responsible for 0-5% of the stress on the anatomy. More information about pain neurology and “head games” is available:
Sort of an afterword: RSI and trauma, sittin’ in a tree
In some ways, trauma and RSI are extremely similar: opposite sides of the same coin. Fast injury and slow injury. Each can have aspects of the other. They can very neatly co-exist, not entirely one, not just the other.
When tissue is injured traumatically, it is rendered vulnerable and a lot easier to accidentally “overuse.” Indeed, most injuries that are having trouble healing are in some sense morphing into a sort of RSI. This is a bit of a word game, in a way, but it’s food for thought. It may be helpful to think of an RSI as a slow-motion trauma that just keeps happening … and think of a trauma that won’t heal as an RSI that started rather suddenly.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
The RSIs defined, roughly in order of infamy (and where to find more information about them on PainScience.com)
About half of these are some kind of tendinitis or tendinitis-like condition. This is written to be partly a quick reference guide, directing you to other articles if I have them, but also a readable tour of the common RSIs.
- Carpal tunnel syndrome (CTS) — CTS is an impingement of the median nerve in the wrist, caused by swelling around it in a narrow channel, the “carpal tunnel.” I haven’t written a CTS guide yet (much to the frustration of many readers), but the topic does get some important attention in perfect spots 4 and 5.
- Plantar fasciitis — Nasty pain in the arch of the foot and the leading edge of the heel bottom. See The Complete Guide to Plantar Fasciitis There’s also a perfect spot article for plantar fasciitis.
- Runner’s knee — Not just for runners! There are two kinds, iliotibial band syndrome (ITBS) and patellofemoral syndrome (PFPS). The former is an irritation of the big IT band tendon on the side of the knee. PFPS is more complex, with several possible causes and a wider range of symptoms, but is usually experienced as kneecap or frontal knee pain. If you’re not sure which you have, start with this article that explains the difference in detail, with checklists: Diagnosing Runner’s Knee.
- Rotator cuff tendinitis — The rotator cuff refers to a group of shoulder muscles that surround the shoulder joint like a “cuff” and rotate the humerus in its socket. Shoulder pain is often diagnosed as a tendinitis of one of the members of this group, but it’s routinely a wrong diagnosis. When it is actually a tendinitis, it’s usually supraspinatus tendinitis. Anyone with this diagnosis should focus on reading this article, with particular attention to the information about the role of muscle in RSIs.
- Achilles tendinitis — The most “pure” of the tendinitises — just an unhappy tendon, and that’s it — in the body’s most obvious big tendon.
- Tennis elbow — AKA lateral epicondylitis, and extensor carpi radialis tendinitis (and very closely related to Golfer’s elbow, which is pretty much the same thing but on the other side of the elbow and a lot less common). Tennis elbow often isn’t a tendinitis, but muscle pain, or significantly complicated by it. I have a basic tennis elbow guide. There’s also a perfect spot article for tennis elbow — start there.
- Shin splints — There are (at least) three versions of shin splints (which just means “shin pain”): medial tibial stress syndrome (fatigue of the tissues along the edge of the tibia bone), compartment syndrome (dangerous/painful swelling of the compartment), and stress fracture (if you need that defined, I can’t help you). All are discussed in detail in an advanced shin splints guide. Muscle is also a key factor in shin splints: so see also the perfect spot article for shin splints, about a big tibialis anterior muscle trigger point that often causes shin splinty trouble.
- Bursitis, usually trochanteric (hip) — Bursae are little slippery sacs that reduce friction between heavily used parts of the anatomy. Bursitis is a much less common condition than people think, and this one at the hip is the only one that is common enough to be on this list. I have no article about it, but I explain how often it is misdiagnosed in the introduction to the trigger points tutorial.
- Jumper’s knee — The Latin: patellar tendinitis. That’s the connection between the kneecap and the shin. Sorry, this tendinitis is not discussed on PainScience.com.
- Compartment syndrome — This is another type of shin splints. See above.
- DeQuervain’s tenovaginitis — The “vagina” part of the term refers to the sheath of this big thumb tendon.
- Athletic pubalgia — Another tendinitis, common in athletes, causing lower abdominal and groin pain. It often spreads from the tendon of the abdominal muscles (where they attach to the pubic bone) to the tough membranes that hold our guts in.80
And honourable mentions for:
- Low back pain — Often thought of as an RSI, sort of … but that can be quite misguided, based on the incorrect notion that the spine is a fragile structure that wears and breaks down easily. It’s really not. The cure for this kind of thinking can be found in the low back pain tutorial, which includes an extensive discussion of the dubious RSI-LBP relationship.
- Temporomandibular joint dysfunction (TMJD) — (Not just “TMJ.” That acronym refers only to the joint itself.) TMJS is a bit too complex and different from simple overuse to easily join the RSI club. And yet it is also clearly related to jaw clenching and bruxism — which are pretty overuse-y. Start with Massage Therapy for Low Back Pain. See also the sections on jaw relaxation in Massage Therapy for Bruxism, Jaw Clenching, and TMJ Syndrome.
![Funny animated gif of two strange animated characters rapidly opening and close their jaws.]()
Jaw muscles get used heavily. Sometimes they get worn the heck out.

Related Reading
This article was logistically challenging because a great deal of its subject matter is already covered in detail elsewhere on the website. I did my best to summarize those topics as they relate to RSIs, and also direct readers on to more detailed reading. Here’s a handy chart:
| topic | this article | other resources |
|---|---|---|
| RSIs are not inflamed. | This article is my main source of information and references on this topic. Jump to topic. | None. However, it is discussed in several tutorials concerning allegedly “inflamed” RSIs, i.e. plantar fasciitis. |
| RSIs are not a biomechanical failure. | Summarized, with particular attention to how other factors in RSI specifically outweigh structural factors. Jump to topic. | See Your Back Is Not Out of Alignment, and professionals should read Lederman. |
| RSIs often just need more rest. | Summarized, with emphasis on how rest seems to get badly neglected in the case of RSIs. Jump to topic. | See The Art of Rest. |
| RSIs can be muscular. | Summarized, with some specific examples of how muscle pain relates to RSIs. Jump to topic. | Muscle pain is the single biggest topic on PainScience.com. Start with the introduction to my advanced trigger point tutorial. |
| RSIs play head games. | RSIs are particularly anxiety-producing, and that’s the focus of the section; the neurological effects of that anxiety are only mentioned here, not explained. Jump to topic. | See Pain is Weird: Pain science reveals a volatile, misleading sensation that comes entirely from an overprotective brain, not our tissues. |
What’s new in this article?
Eighteen updates have been logged for this article since publication (2011). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
For a long time, pieces of this article existed in many forms all over the website, my notes, and my head. I pulled it all together for a new article over a few days, in time for a podcast appearance on the topic in 2011.
Nov 14, 2025 — Added Hartwell 2024 to my collection of “running doesn’t wreck knees” citations.
2024 — Substantial editing, revision, and upgrades for the (very large) members only section of this article.
2024 — Updated citations for the claim that "a lot of regular exercise does not inevitably destroy joints." I added a couple news ones (Voinier, Weng), a couple old ones (Luke, Williams), and improved the annotations.
2020 — Extensive editing and modernization. Many minor improvements adding up to a large overall improvement.
2019 — Added new section: “Exercise is also an anti-inflammatory medication.”
2019 — Added fascinating reference about the lack of turnover in tendon tissue (Heinemeier).
2019 — Just one citation added, but a neat one: Marsolais et al. found that anti-inflammatory meds suppressed some gross signs of inflammation in tendinopathy, but had no other benefit. Good to know.
2018 — Major revision to the inflammation discussion, based on new evidence that RSIs may be inflamed after all — just not a classic, acute immune response. This isn’t really a shock, but it sure is interesting, and many changes had to be made to accommodate just a single key new citation (Dakin). This is why my work will never be done!
2017 — Cited new evidence on the limited benefits of steroid injections for rotator cuff tendinopathy (Mohamadi) — an interesting contrast with the effects of steroids on frozen shoulder. Also cited new evidence that shoulder decompression does not work for supraspinatus tendinopathy (Ketola et al.)—a really great example of the problem with looking at RSIs mechanistically.
2016 — Small but important clarification about load management: new first paragraph of resting section.
2016 — Added a mobile-only article summary.
2016 — Significant science update. Revised the “Head Games” section to emphasize the implications of a pair of really interesting references (Andersson 2011 and Neogi 2015).
2015 — Updated discussion of risks and benefits of medications.
2013 — Revised the introduction a bit: just a little richer and creamier.
2012 — Added a small concluding section — didn’t really know where else to put it! “Sort of an afterword: RSI and trauma, sittin’ in a tree.”
2012 — Major updates to the inflammation section. Virtually re-written to emphasize that inflammation is certainly not present in the sense of classic inflammation, but may nevertheless have a little biochemistry in common with it. If allegedly “anti-inflammatory” treatments work, it is probably mainly by different mechanisms, and this is now thoroughly explained, with detailed notes on every major common treatment.
2011 — Improvements to the RSI reading guide.
2011 — Numerous minor corrections and improvements in readability, and a couple more images.
2011 — Publication.
Notes
- Yang J, Tibbetts AS, Covassin T, et al. Epidemiology of overuse and acute injuries among competitive collegiate athletes. J Athl Train. 2012;47(2):198–204. PubMed 22488286 ❐ PainSci Bibliography 52883 ❐ In this 2012 study of common overuse injuries in team sports, half of them did not even knock people out of the game.
- Andres BM, Murrell GAC. Treatment of tendinopathy: what works, what does not, and what is on the horizon. Clin Orthop Relat Res. 2008;466(7):1539–1554.
- But not iliotibial band syndrome, which is an interesting exception — why not IT banditis? Perhaps because it sounds too silly.
- And, in the early days of a new RSI, it might be more like that. The inflammation question is complicated by the possibility that RSIs might start out as more classically inflammatory problems in their earliest stages. However, as you will see, if it happens at all it really doesn’t last long. The science on this has been clear for ages: by the time patients present these problems to health care professionals (or researchers), classic inflammation is no longer a dominant factor, or even a detectable one in most cases.
- Khan KM, Cook JL, Taunton JE, Bonar F. Overuse tendinosis, not tendinitis, part 1: a new paradigm for a difficult clinical problem (part 1). Phys Sportsmed. 2000;28(5):38–48. PubMed 20086639 ❐
- It is not easy to obtain pictures of live human dissections. What few I was able to find were not large enough or anywhere near similar enough to healthy examples for a meaningful comparison. And even if I had found something, it’s unlikely I could have obtained permission to publish it.
- Khan: “Inflammatory lesions and granulation tissue were infrequent, and when found, were in association with partial ruptures. … In partial ruptures, frayed tissue was bordered by fibrin deposits but histopathology remained identical to those cases without rupture. ‘Inflammatory cells, intracellular lipid aggregates and acellular necrotic areas were exceptional’ and not regarded as normal elements of the degenerative process.”
- For instance, some tendinitis involves the thin layer of tissue that surrounds the tendon, as opposed to the tendon itself. When this less tendon-like tissue gets into trouble, it also gets a little more inflamed than the tendon proper. But these cases are the exception.
- Khan 1999, op. cit.
- According to Khan, when researchers “examined bursal tissue in patients with so-called subacromial ‘bursitis' they found an 'absence of plasma cells and a paucity or even absence of neutrophils and lymphocytes'. These features are incompatible with true inflammatory bursitis … .”
- Gaeta M, Minutoli F, Vinci S, et al. High-resolution CT grading of tibial stress reactions in distance runners. American Journal of Roentgenology. 2006 Sep;187(3):789–793. PainSci Bibliography 56137 ❐
- Gaeta also found shin bone degeneration in 16% of runners that didn’t have any symptoms … yet. Silent degeneration has been found in tendons as well. Khan: “A high proportion of asymptomatic volunteers (89-100%) have regions of high signal in the rotator cuff tendon. This suggests, but does not prove, that subclinical tendon degeneration may be a relatively common phenomenon amongst asymptomatic individuals.” It’s not really surprising that the process begins before we notice it, perhaps quite a long time before.
- The system has limits, but evolution tunes biology to cope with failure as gracefully as possible. Like an organization on a tight budget, biology cuts the least essential — i.e. least noticeable — services first, so that the organism can continue to function as well as possible in the short term. Biology is never optimized for long term safety.
- For more detail, see another article on PainScience.com, A Painful Biological Glitch that Causes Pointless Inflammation: How an evolutionary wrong turn led to a biological glitch that condemned the animal kingdom — you included — to much louder, longer pain.
- Medzhitov R. Origin and physiological roles of inflammation. Nature. 2008 Jul;454(7203):428–35. PubMed 18650913 ❐ Medzhitov explains that “although infection-induced inflammation is vital, it might be a special case.” Indeed, classic inflammation seems to be an oddball, and has relatively little in common with lots of other “inflammation” — the immune response to infection is dramatic and conspicuous, but perhaps exceptional and distinctive within the broader context of the biology of healing and adaptation … which is so diverse that it really doesn’t fit comfortably under one umbrella term like “inflammation.”
- Ruslan Medzhitov (emphasis mine): “ … whereas the physiological rationale [clear biological purpose] of infection-induced inflammation is clear, many other types of inflammatory response are only known in pathological settings, and there is no clear understanding of their physiological counterparts. It is not even clear whether there is any physiological counterpart for some inflammatory conditions … The standard view of inflammation as a reaction to infection or injury might need to be expanded to account for the inflammatory processes induced by other types of adverse conditions.” In other words, sometimes inflammation seems to happen for no reason whatsoever.
- Medzhitov again: “The mechanisms of infection-induced inflammation are understood far better than are those of other inflammatory processes. It is unclear how applicable knowledge of infection-induced inflammation is to other types of inflammation.” Also: “Unlike the signals that report infection and injury, the signals that report tissue stress and malfunction, and the molecular sensors that detect these signals, are largely unknown.”
- Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med. 2009 Jun;43(6):409–16. PubMed 18812414 ❐
- Dakin SG, Newton J, Martinez FO, et al. Chronic inflammation is a feature of Achilles tendinopathy and rupture. Br J Sports Med. 2017 Nov. PubMed 29118051 ❐
- Khan 2000, op. cit.
- Marsolais D, Côté CH, Frenette J. Pifithrin-alpha, an inhibitor of p53 transactivation, alters the inflammatory process and delays tendon healing following acute injury. Am J Physiol Regul Integr Comp Physiol. 2007 Jan;292(1):R321–7. PubMed 16902184 ❐
- The NSAIDs are strongly preferred by most people because of the perception that RSIs are inflammatory. NSAIDs are “anti-inflammatories.” But it’s not at all clear that there’s a meaningful difference. In 2018, Hung et al. showed that these medications were all roughly equal for acute injury pain — which aren’t RSIs, for sure, but definitely involve inflammation.
- I’m sure there are some testimonials for ibuprofen — there are for anything. But consider: even though ibuprofen is probably the first or second line of defense for virtually every case, the world is clearly still full of serious, chronic RSIs … that ibuprofen hasn’t stopped.
- Marsolais D, Côté CH, Frenette J. Nonsteroidal anti-inflammatory drug reduces neutrophil and macrophage accumulation but does not improve tendon regeneration. Lab Invest. 2003 Jul;83(7):991–9. PubMed 12861039 ❐
“Whether nonsteroidal anti-inflammatory drugs have a beneficial effect on tendon regeneration is still a matter of debate.” These researchers “tested the hypothesis that a 3-day treatment with diclofenac would protect tendons from inflammatory cell injury and would promote healing,” and found that it did not: “The inhibition of leukocyte accumulation by diclofenac did not translate into a reduction of tissue damage or a promotion of tissue healing, because the mechanical properties of injured Achilles tendons were identical in placebo and diclofenac-treated groups.”
- Many athletes practically mainline the stuff before competition. I’ve even done that myself, taking far more than I should because I’m highly gut-tolerant of the stuff — it just doesn’t seem to make me grumbly in my tumbly. However, in a rare case of good science about a fairly minor issue, good experiments have shown that this practice is nothing more than superstition. In 2006, Nieman et al. tested the effect of ibuprofen on hard-core marathoners. There were 29 ultra-marathoners on high doses of ibuprofen and 25 controls that completed the race without meds. There was no measurable difference in muscle damage or soreness between the two groups. Lead researcher David Niemen: “There is absolutely no reason for runners to be using ibuprofen.” For more detailed reporting on this research see: Convincing the Public to Accept New Medical Guidelines, by Aschwanden.
And there are other, similar studies. For instance, Semark et al. tortured sprinters’ muscles with a savage workout, and the painful results were identical with or without an anti-inflammatory medication. “In conclusion,” they wrote, “the aetiology of the DOMS induced in the trained subjects in this study seems to be independent of inflammatory processes … .” Hmm. Minimal inflammation in delayed-onset muscle soreness too? Not really surprising!
- Heinemeier KM, Øhlenschlæger TF, Mikkelsen UR, et al. Effects of anti-inflammatory (NSAID) treatment on human tendinopathic tissue. J Appl Physiol (1985). 2017 Nov;123(5):1397–1405. PubMed 28860166 ❐ This study reported that “tendinopathic cells are not responsive to ibuprofen.”
- Bittermann A, Gao S, Rezvani S, et al. Oral Ibuprofen Interferes with Cellular Healing Responses in a Murine Model of Achilles Tendinopathy. J Musculoskelet Disord Treat. 2018;4(2). PubMed 30687812 ❐ PainSci Bibliography 52446 ❐ “We conclude that the use of Ibuprofen for pain relief during inflammatory phases of tendinopathy, might interfere with the normal processes of extracellular matrix remodeling and cellular control of expression of inflammatory and wound healing genes.”
- Wheatley BM, Nappo KE, Christensen DL, et al. Effect of NSAIDs on Bone Healing Rates: A Meta-analysis. J Am Acad Orthop Surg. 2019 Apr;27(7):e330–e336. PubMed 30260913 ❐
This is a meta-analysis of 16 trials, showing that common over-the-counter pain-killers interfere with bone healing. Chronic overuse roughly doubles the risk that a fracture will heal slowly or not at all (“non-union,” a very serious complication).
The effect was not evident in children or in lower doses or temporary usage — this bad news applies only to adults taking too much of the stuff for too long. Unfortunately, a lot of people do that! The pain-killers in question are the non-steroidal anti-inflammatory drugs or NSAIDs like aspirin, ibuprofen, and naproxen — already notorious for several other significant side effects, and yet still widely overused.
- Medication-overuse headaches (MOH), formerly known as “rebound” headaches, are probably mostly caused by dependence-and-withdrawal physiology, like getting a headache when you quit drinking coffee, but it might be more complicated. Pain-killers taken for headaches may be a surprisingly common and ironic cause of headaches (though maybe less of a plague than some headlines have led us to fear; see Scher). This topic is obviously of special interest to patients with unexplained headaches, and so I discuss it a lot in my headache guide, but it’s also just a major side effect for anyone treating anything with pain-killers long-term.
- McGettigan P, Henry D. Use of non-steroidal anti-inflammatory drugs that elevate cardiovascular risk: an examination of sales and essential medicines lists in low-, middle-, and high-income countries. PLoS Med. 2013 Feb;10(2):e1001388. PubMed 23424288 ❐ PainSci Bibliography 54748 ❐
Diclofenac is an extremely popular painkiller associated with serious cardiovascular risks, as with other NSAIDs: “There is increasing regulatory concern about diclofenac. … Diclofenac has no advantage in terms of gastrointestinal safety and it has a clear cardiovascular disadvantage.”
- Science Based Pharmacy [Internet]. Gavura S. How risky are NSAIDS?; 2015 Jul 25 [cited 16 Aug 18]. PainSci Bibliography 54751 ❐
A good general discussion of painkiller risks and side effects, but the relative safety of topical treatments is of particular interest:
The main advantage of topical NSAIDs is the reduced exposure of the rest of the body to the product, which reduces the side effect profile. Given the toxicity of NSAIDs is related in part to the dose, it follows that topical treatments should have a better toxicity profile. Consequently, the cardiovascular risks of topical diclofenac, even in those with a high baseline risk of disease, should be negligible with the topical forms.
- Bussin E, Cairns B, Gerschman T, et al. Topical diclofenac vs placebo for the treatment of chronic Achilles tendinopathy: A randomized controlled clinical trial. PLoS One. 2021;16(3):e0247663. PubMed 33661967 ❐ PainSci Bibliography 49693 ❐
- In homeopathy, like cures like, known as the “law of similars” (not actually a law), so you treat inflammation with an extreme dilution of something that causes inflammation. Except that arnica — in its undiluted, non-homeopathic, “just a herbal medicine” form — is actually allegedly an anti-inflammatory herb. So the main ingredient in homeopathy’s most popular product is actually completely at odds with homeopathy’s most important rule. Confused? Welcome to the muddled “logic” of homeopathy.
- Collins NC. Is ice right? Does cryotherapy improve outcome for acute soft tissue injury? Emerg Med J. 2008 Feb;25(2):65–8. PubMed 18212134 ❐
This is a 2008 review of just 6 studies of therapeutic icing, only two of them any good: one with slightly positive results, the other showing no effect. So that’s two studies that showed little or no benefit, which is leaning towards bad news, but it’s just not enough data to clinch it. (Four animal studies showed reduced swelling, but we can’t take animal studies to the bank.) The bottom line is just that “there is insufficient evidence.”
- Iontophoresis is needle-less injection, using a small electric charge to drive a drug through the skin.
- For instance, it was instrumental in treating a nasty but transient form of rheumatoid arthritis, polymyalgia rheumatica, that my father suffered a few years ago. This incredibly painful condition was almost 100% controlled by prednisone for several months. The side effects were substantial, but — and I can’t emphasize this strongly enough — so much less bad than the pain.
- Tonks JH, Pai SK, Murali SR. Steroid injection therapy is the best conservative treatment for lateral epicondylitis: a prospective randomised controlled trial. Int J Clin Pract. 2007 Feb;61(2):240–6. PubMed 17166184 ❐
“On the basis of the results of this study, the authors advocate steroid injection alone as the first line of treatment for patients presenting with tennis elbow demanding a quick return to daily activities.”
- Song A, Higgins LD, Newman J, Jain NB. Glenohumeral corticosteroid injections in adhesive capsulitis: a systematic search and review. PM R. 2014 Dec;6(12):1143–56. PubMed 24998406 ❐ PainSci Bibliography 53477 ❐
- Rompe JD, Segal NA, Cacchio A, et al. Home training, local corticosteroid injection, or radial shock wave therapy for greater trochanter pain syndrome. Am J Sports Med. 2009 Oct;37(10):1981–90. PubMed 19439758 ❐
This was a large, long-term test of three therapies for three hundred patients with greater trochanter pain syndrome. Corticosteroid injections, home exercises, and repetitive low-energy shock wave therapy were pitted against each other, and the results measured at 1, 4, and 15 months. The study glaringly omitted a placebo group, which is a shame.
Those who received steroid injections were the clear winners in the short term, but only in the short term. At four months, they no longer had the lead. And by 15 months, not only were they back to their original pain levels, but those who did home training and shockwave therapy were doing quite well. Those groups probably represent normal healing, since neither of those therapies is known for producing excellent lasting results.
These results imply a surprisingly stark contrast between short and long term results. One implication is that steroids not only help in the short term but actually harm in the long term. “The role of corticosteroid injection for greater trochanter pain syndrome needs to be reconsidered,” the authors suggest.
- Mohamadi A, Chan JJ, Claessen FMA, Ring D, Chen NC. Corticosteroid Injections Give Small and Transient Pain Relief in Rotator Cuff Tendinosis: A Meta-analysis. Clin Orthop Relat Res. 2017 Jan;475(1):232–243. PubMed 27469590 ❐ PainSci Bibliography 52902 ❐ This review sought the answers in eleven mostly small studies of 700 patients (including three studies that included multiple injections). The answers were disappointing, other than confirmation of minor temporary pain relief. There was no effect for most patients at three months, multiple injections made no difference, and five patients needed to be treated to get good results for one.
- Hopewell S, Keene DJ, Marian IR, et al. Progressive exercise compared with best practice advice, with or without corticosteroid injection, for the treatment of patients with rotator cuff disorders (GRASP): a multicentre, pragmatic, 2×2 factorial, randomised controlled trial. Lancet. 2021 07;398(10298):416–428. PubMed 34265255 ❐ PainSci Bibliography 52103 ❐
The GRASP trial is a study of steroids versus exercise for (mainly) shoulder tendinitis, and it basically showed that there are no major differences. They are both equally effective and modest, or equally ineffective. Unsurprisingly, steroids are more helpful in the short term.
This is a large, complex trial with some glaring flaws but also a lot of useful data. I have a large blog post that really digs into it for almost 3000 words. Big study, big analysis! See STUDY: Exercise, Steroids, and Shoulder Pain That Might Be Tendinitis (Member Post). But here are the key takeaways:
- Our poor understanding of what’s actually wrong with these shoulders is a serious limitation. It makes the whole GRASP trial more like a REACH.
- As just mentioned, the lack of a more neutral comparison really makes it hard to know whether steroids and exercise are equally effective… or equally ineffective.
- Maybe “rotator cuff disorders” are generally invincible! It is a tough problem, no doubt about it.
- Nevertheless, it would be reasonable to use this citation to support advising people not to bother with any kind of care for shoulder pain.
- Exercise and steroid injections are two of the very most popular treatment options for shoulder. If they don’t work, it’s not like there’s a bunch of other strong candidates waiting in the wings.
- Some people in every group did better than others, of course. The results were an average. But, as always, good luck identifying those “responders” in advance!
- And so, for instance, steroid injections might be favoured in cases of plantar fasciitis where neuralgia is a suspected factor, and not just an “inflamed” plantar fascia. Nicholl et al.: “Steroids have been shown to be effective in reducing neuralgia. Therefore they have their place in the treatment of plantar fascia but only when directed towards nerve entrapment.”
- Okike K, King RK, Merchant JC, et al. Rapidly Destructive Hip Disease Following Intra-Articular Corticosteroid Injection of the Hip. J Bone Joint Surg Am. 2021 11;103(22):2070–2079. PubMed 34550909 ❐
This study identified a low risk of “rapid hip destruction disease” with one low-dose steroid injection, and “higher” risk with larger and multiple injections. This is hardly the only evidence of harm from steroid injections, but I think it is the most dramatic I have ever seen. RHDD is what it sounds like: premature and accelerated arthritis. Best avoided! This risk is remote, but also as serious as an amputation.
- Khan KM, Cook JL, Bonar F, Harcourt P, Astrom M. Histopathology of common tendinopathies. Update and implications for clinical management. Sports Med. 1999 Jun;27(6):393–408. PubMed 10418074 ❐
- Orchard J, Kountouris A. The management of tennis elbow. BMJ. 2011;342:d2687. PubMed 21558359 ❐ Orchard and Kountouris concluded in a 2011 review of tennis telbow treatments that “Cortisone injections are harmful in the longer term and are no longer recommended in most cases.” Not everyone agrees, but it’s an important opinion to take note of.
- Ketola S, Lehtinen JT, Arnala I. Arthroscopic decompression not recommended in the treatment of rotator cuff tendinopathy: a final review of a randomised controlled trial at a minimum follow-up of ten years. Bone Joint J. 2017 Jun;99-B(6):799–805. PubMed 28566400 ❐
“No significant differences” were found in this straightforward comparison of surgery and exercise therapy for rotator cuff tendinopathy in several dozen patients.
- So, if it’s not the seemingly obvious pinching, what the heck is it? Ketola et al.: “The natural history of rotator cuff tendinopathy probably plays a significant role in the results in the long-term.” In other words, it just does what it does, whether it’s being pinched or not: it’s biology and neurology, not mechanics. Pinching is an probably a factor, not a deciding factor.
- Louw A, Diener I, Fernández-de-Las-Peñas C, Puentedura EJ. Sham Surgery in Orthopedics: A Systematic Review of the Literature. Pain Med. 2016 Jul. PubMed 27402957 ❐ PainSci Bibliography 53458 ❐
A review of a half dozen high quality tests of four popular orthopedic (“carpentry”) surgeries, all showing a lack of efficacy compared to placebos. This review is an excellent academic citation to support the claim that sham surgery has shown to be just as effective as actual surgery in reducing pain and disability. It’s also an eyebrow-raiser that Louw et al. could find only six good (controlled) trials of orthopedic surgeries, and all of them were bad news.
- Tumminello N, Silvernail J, Cormack B. The Corrective Exercise Trap. Personal Training Quarterly. 2017 Mar;4(1). PainSci Bibliography 52905 ❐
The authors decisively but gently tip over the most sacred cow of personal training and therapy: corrective exercise, which is grounded in the assumption that there is something in-correct about patients — fragile, weak, or uneven — which must be fixed by sufficiently expert and precise exercise prescription. Exaggerating the importance of defect-correction is actually dangerous for the patient (nocebic): “When clients are told such things about themselves from an authority figure (as they might be during some corrective exercise evaluations), that this potentially makes one’s clients less resilient and more prone to injury and pain.” Translation sans diplomacy: stop #%&^ telling patients they are fragile and weak!
The corrective exercise trap is also about overconfidence in the value of allegedly advanced rehab exercise, when the evidence is overwhelming that corrective exercise is no better than general exercise. “The danger here” — the trap! — “is that many fitness professionals might end up making their training process more about a formalized evaluation procedure and less about good personal training.”
- A good example of an aggravating factor you can’t get away from would be a cyst in the wrong place: just a random lump of unwelcome tissue in a bad spot, which is irritating whether you are resting or not. Even worse, you might feel better while you are resting — giving you the false impression that rest is working — but then that inescapable aggravating factor immediately becomes a problem once again when you resume normal activities. That sounds bad — and it is — but you can see how even a failed resting attempt can produce useful and valuable information. It’s really important to be able to present results like that to a surgeon.
- Many people need more time to recover from workouts than they realize — many days after the soreness has faded. One of the implications of this is that strength training can be productive with surprisingly infrequent trips to the gym. Less is not less! I have a whole article about that. But think about what it implies about recovery time for tendon. If it takes 10-20 days for muscle to fully heal and adapt after a strong workout … how long will injured tendon, ligament, and cartilage take? Hint: longer.
- Heinemeier KM, Schjerling P, Øhlenschlæger TF, et al. Carbon-14 bomb pulse dating shows that tendinopathy is preceded by years of abnormally high collagen turnover. FASEB J. 2018 09;32(9):4763–4775. PubMed 29570396 ❐
- Polaski AM, Phelps AL, Kostek MC, Szucs KA, Kolber BJ. Exercise-induced hypoalgesia: A meta-analysis of exercise dosing for the treatment of chronic pain. PLoS One. 2019;14(1):e0210418. PubMed 30625201 ❐ PainSci Bibliography 52661 ❐
This is a good quality review of studies of exercise for chronic pain that tried to extract some wisdom about exercise dosage for chronic pain patients. Unfortunately, it failed: the review establishes only that we know essentially nothing about exercise dosage for chronic pain patients. Our ignorance is near total. There’s just not enough of the right kind of evidence to conclude anything, and almost countless confounding factors and variables that have never been studied.
“The lack of dosing studies for exercise means that patients may not be receiving the optimal therapy and/or be receiving a therapy that actually increases pain.”
From a detailed analysis of the review:
Appropriate exercise dosage may not be generalizable beyond the individual patient given their goals and prior activity levels. … Perhaps it isn’t necessary (or even realistic) to find an optimal, generalizable dosage of exercise for pain states, but rather to find appropriate exercise dosage for the individual based on their desired goals.
- Soligard T, Schwellnus M, Alonso JM, et al. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br J Sports Med. 2016 Sep;50(17):1030–41. PubMed 27535989 ❐
- Gabbett TJ. Debunking the myths about training load, injury and performance: empirical evidence, hot topics and recommendations for practitioners. Br J Sports Med. 2018 Oct. PubMed 30366966 ❐ “Rapid increases in training and competition workloads and low chronic workloads are associated with greater injury risk. These findings suggest that appropriately staged training programmes may reduce injury risk in athletes. There is an urgent need for randomised controlled trials to test this working hypothesis.”
- Hartwell MJ, Tanenbaum JE, Chiampas G, Terry MA, Tjong VK. Does Running Increase the Risk of Hip and Knee Arthritis? A Survey of 3804 Marathon Runners. Sports Health. 2024;16(4):622–629. PubMed 37555313 ❐ PainSci Bibliography 49969 ❐
Pounding the pavement is not a major driver of arthritis, as supported by this 2024 survey. It’s far from perfect data, but it harmonizes with a lot of other data, and it shows, at the very least, that some people can “survive” running without OA.
This survey was done by ~3,800 Chicago Marathon participants: only 7.3% reported a doctor’s diagnosis of knee or hip arthritis . That’s lower than rates seen in the general population of middle-aged adults, and the study found no link between arthritis and the number of years running, marathons completed, weekly mileage, or pace.
Instead, the big risk factors were the usual suspects: older age, family history, prior injuries, surgery, and a higher body mass index. As the authors put it, “there was no identified association between cumulative running history and the risk for arthritis.”.
Nearly a quarter of participants said a physician had told them to cut back or quit running — but more than 90% planned to keep racing anyway.
Read more about this paper.
- Luke AC, Stehling C, Stahl R, et al. High-Field Magnetic Resonance Imaging Assessment of Articular Cartilage Before and After Marathon Running: Does Long-Distance Running Lead to Cartilage Damage? Am J Sports Med. 2010 Jul. PubMed 20631252 ❐
Studies have shown that runners probably do not get more knee osteoarthritis than anyone else (e.g. Weng, but many others), which is a bit surprising: surely regular pounding wears out joints? Researchers took a bunch of fancy pictures of the insides of knees before and after a marathon, using a new MRI technique that can detect early cartilage degeneration:
Runners showed elevated T1rho and T2 values after a marathon, suggesting biochemical changes in articular cartilage … the patellofemoral joint and medial compartment of the knee show the highest signal changes, suggesting they are at higher risk for degeneration.
Sounds bad, doesn’t it? Also, perhaps some biomarkers of trouble “remain elevated after 3 months of reduced activity” — but it’s arguable that those results were not actually statistically significant.
So, bad biomarkers in the knee after running, oh noes! But I actually see good news for knees here. It’s not surprising that a lot of running has an effect on joints in the first place, of course, and this data confirms that. (Remember, this was after running a marathon.) But this data also shows that the effect is surprisingly minor, and that most knees recover, either mostly or completely, within three months‚ even from a very large dose of running. That is important information.
Stressfully loading a joint in itself is probably not a problem per se, and could even be healthy, stimulating, toughening — as long as you allow time to recover. It’s excessive loading without adequate recovery, AKA “overdoing it,” that is likely to be the real hazard for runners. I see this as (more) evidence that the average sane runner is nowhere close to wearing out his or her knees — and also that runners who do get into trouble really, really need to rest and let their biomarkers simmer down.
- Williams PT. Effects of running and walking on osteoarthritis and hip replacement risk. Med Sci Sports Exerc. 2013 Jul;45(7):1292–7. PubMed 23377837 ❐
This analysis of about a zillion runners versus walkers found that “running significantly reduced arthritis and hip replacement risk”… but due in large part to the fact that runners were typically skinnier. So weight was a trump factor here.
This data flies in the face of the common assumption that running is much harder on the joints. Instead, what it clearly shows is that running is either neutral or helpful, and weight is a much more important factor regardless of whether you walk or run.
- Lefèvre-Colau MM, Nguyen C, Haddad R, et al. Is physical activity, practiced as recommended for health benefit, a risk factor for osteoarthritis? Ann Phys Rehabil Med. 2016 Jun;59(3):196–206. PubMed 27103057 ❐
This review of the scientific literature on arthritis risk focused specifically on the role of injury in driving arthritis in people who are active and athletic. They reported that moderate activities/sports are “not a consistent risk factor for clinical or radiographic knee/hip OA.” Signs of arthritis visible on x-ray increased with volume of activity and injury risk, but modestly even up to the elite level, and former athletes actually had fewer symptoms despite those signs. Finally, the “risk of injury in different sports may be the key factor to understanding the risk of oseoarthritis related to sport.”
About the review not being “systematic”: it was just experts choosing papers, as opposed to using a reproducible method that anyone, in theory, could use to produce the same list of papers to read.
- Alentorn-Geli E, Samuelsson K, Musahl V, et al. The Association of Recreational and Competitive Running With Hip and Knee Osteoarthritis: A Systematic Review and Meta-analysis. J Orthop Sports Phys Ther. 2017 Jun;47(6):373–390. PubMed 28504066 ❐
This study reports that long-term prevalence of hip and knee osteoarthritis was lowest in recreational runners, and much higher in both sedentary people and competitive runners. They did not control well for confounders, and there are lots of possible ones, but the results were consistent with the predictable wisdom of “moderation in all things,” and that typical walking and running is, if anything, actually inversely correlated with OA progression in both hip and knee. And that conclusion is support by plenty of other evidence (e.g. Voinier, Weng).
- Lo GH, Musa SM, Driban JB, et al. Running does not increase symptoms or structural progression in people with knee osteoarthritis: data from the osteoarthritis initiative. Clin Rheumatol. 2018 May. PubMed 29728929 ❐
This study looked at the relationship between running and arthritis in 1200 aging runners with at least some arthritis, selected from the Osteoarthritis Initiative (a 10-year study of about 5000 arthritis patients). No data is ever perfect or complete, and Lo et al. had to fill in the blanks (imputation) for 8% of the runners. The runners-with-arthritis were divided into groups who got worse or better signs or symptoms over two years, adjusting for factors like age, weight, and sex.
They did not get worse. In fact, the runners — normal people, mostly just a bunch of aging amateur athletes who consider themselves runners — actually had less pain than the non-runners, and the state of their joints (on x-ray) were stable. Conclusion:
self-selected running is associated with improved knee pain and not with worsening knee pain or radiographically defined structural progression.
- Ponzio DY, Syed UAM, Purcell K, et al. Low Prevalence of Hip and Knee Arthritis in Active Marathon Runners. J Bone Joint Surg Am. 2018 Jan;100(2):131–137. PubMed 29342063 ❐
In this survey of 675 marathoners, there was no link between current arthritis symptoms and their running history, and they had a lower rate of arthritis than the general population. That is, no matter how much they ran, they had the same low rate of arthritis: about 9%, compared to 18% in non-runners.
This is good-news evidence that challenges the assumption that relentless “pounding” on the road is hard on joints, as many other studies have. But we’re still far from “proof.” For something closer, see Chakravarty — the best single study on this topic that I’m aware of to date.
- Voinier D, White DK. Walking, running, and recreational sports for knee osteoarthritis: An overview of the evidence. Eur J Rheumatol. 2022 Aug. PubMed 35943452 ❐
Voiner and White reviewed a lot of reviews of the relationship between exercise and arthritis — an “overview of narrative reviews, systematic reviews, and meta-analyses,” twenty of them. They also threw a dozen original trials into the mix. Their clear conclusion, based on “consistent evidence,” is that arthritis just has nothing to do with common kinds of physical activity and exercise, like walking and running and playing softball. Specifically, the “structural progression” is unrelated to physical activity in the general population.
- Weng Q, Goh SL, Wu J, et al. Comparative efficacy of exercise therapy and oral non-steroidal anti-inflammatory drugs and paracetamol for knee or hip osteoarthritis: a network meta-analysis of randomised controlled trials. Br J Sports Med. 2023 Jan;57(15):990–996. PubMed 36593092 ❐ PainSci Bibliography 51421 ❐
This enormous meta-analysis concludes that exercise is a modestly effective treatment for hip/knee arthritis in the short term:
Exercise has similar effects on pain and function to that of oral NSAIDs and paracetamol. Given its excellent safety profile, exercise should be given more prominence in clinical care, especially in older people with comorbidity or at higher risk of adverse events related to NSAIDs and paracetamol.
The data also shows diminishing returns over time, dwindling to a trivial benefit.
But this data shows that exercise is quite safe and somewhat helpful — and therefore also obviously not harmful.
This is not surprising science, of course. That conclusion is based on one-hundred and fifty-two trials. 😮 That is a whole bunch of trials! The effect of exercise on arthritis is one of the better studied questions in the science of pain. We have seen this result before, many times. But it’s nice to see the data synthesized in a mighty meta-analysis for the BJSM.
Nor is it especially exciting science: pain relief in the same league as the common pain meds isn’t exactly dazzling stuff. Last I checked, no one was claiming that their ibuprofen is a miracle cure for their arthritis. Also, your mileage may vary in a big way; not everyone is going to get a pain-relief benefit from a workout, and some will actually get the opposite (“exercise intolerance” is common in people with chronic pain). But ibuprofen can fail and backfire too… and, hoo boy, that stuff is a lot more dangerous than exercise (see Bally), and many people cannot take NSAIDs at all.
The important conclusion here is that exercise might actually help arthritis, and definitely doesn’t generally make it worse.
- Chakravarty EF, Hubert HB, Lingala VB, Zatarain E, Fries JF. Long distance running and knee osteoarthritis. A prospective study. Am J Prev Med. 2008 Aug;35(2):133–8. PubMed 18550323 ❐ PainSci Bibliography 49918 ❐
Chakravarty et al. tracked a few dozen older runners and non-runners for many years — most for more than a decade, some as long as twenty years — and 32% of the non-runners ended up with severe arthritis versus only 20% of the runners. And the runners started with 7%! And therefore…
“Severe OA may not be more common among runners.”
Indeed, it was clearly less common in this study.
This was a good quality prospective trial, which is exactly what this research question needed, but it was also tiny (among other acknowledged limitations). You might well see different results in another few dozen runners just by fluke.
“Much larger studies involving hundreds to thousands of healthy older adults followed for several decades are needed to determine if long-distance running may be associated with a modest decrease in incidence or severity of radiographic OA.”
- Pedersen BK. The anti-inflammatory effect of exercise: its role in diabetes and cardiovascular disease control. Essays Biochem. 2006;42:105–17. PubMed 17144883 ❐
- Fu S, Thompson CL, Ali A, et al. Mechanical loading inhibits cartilage inflammatory signalling via an HDAC6 and IFT-dependent mechanism regulating primary cilia elongation. Osteoarthritis Cartilage. 2019 Jul;27(7):1064–1074. PubMed 30922983 ❐ PainSci Bibliography 52660 ❐
This is a highly technical petri-dish study of the effect of “exercise” (mechanical loading) on the inflammation signalling of cartilage cells. Basically, they mechanically stressed samples of excised cartilage and cartilage cells. The surprising, good-news result was that the researchers reported that moderate loading actually reduced inflammation. That is, fewer inflammatory signals were produced by the cells.
- Zhang M, Liang Z, Tian L, et al. Effects of exercise therapy in axial spondyloarthritis: A systematic review, meta-analysis and meta-regression of randomized trials. Arch Phys Med Rehabil. 2024 Jun:S0003–9993(24)01065–7. PubMed 38942347 ❐
This is an encouraging scientific review of exercise for axial spondyloarthritis — inflammatory pathology of the spine. This is a whole category of related rheumatic diseases, but it’s mostly about inflammatory back pain and ankylosing spondylitis.
Zhang et al. reviewed twenty randomized controlled trials of exercise therapy for spondyloarthritis, including 1700 patients, looking at many different outcomes: four different scoring systems, oxygen consumption and chest expansion (because spondyloarthritis often affects the ribcage), two major biomarkers (C-reactive protein and erythrocyte sedimentation rate), and, last but not least, the two most consistent symptoms of inflammation: pain and fatigue.
That’s ten outcomes, and seven of them improved, most of them quite a bit. That’s a fantastic result! Leading to this unstintingly positive conclusion:
“Exercise therapy is an effective strategy for improving disease control and symptom relief in axial spondyloarthritis.”
So what didn’t improve? The two biomarkers for inflammation, and “chest expansion.” CRP and ESR are rather blunt instruments, and it’s possible that they could not detect clinically significant changes in inflammation in the short term.
I explore the broader implications of this paper, and of the missing biomarker improvement, in a blog post: STUDY: Exercise eases inflammatory back pain—but why?.
- Soligard T, Schwellnus M, Alonso JM, et al. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br J Sports Med. 2016 Sep;50(17):1030–41. PubMed 27535989 ❐
This is the first of a pair of papers (with Schwellnus) about the risks of athletic training and competition intensity (load). Is load a risk for injury and illness? How much is too much? Is too little a problem? These papers were prepared by a panel of experts for the International Olympic Committee, and both them use many words to say the same things formally — but they are good points. Here they are in plain English:
- There’s not enough research, surprise surprise, and what we do know is mostly from limited data about a few specific sports. But there’s enough to be confident that “load management” overall is definitely important.
- Both illness and injury seem to have a similar relationship to load — lots of overlap.
- Too much and not enough load probably increase the risk of both injury and illness. You want to be in the goldilocks zone! But the devil is in the details …
- Not everyone is vulnerable to high load, and elite athletes are the most notable exception: they are relatively immune to the risks of overload, probably because of genetic gifts. Everyone else gets weeded out!
- Big load changes — dialing intensity up or down too fast — are much bigger risks than absolute load. If you methodically work your way up to a high load, it may even be protective.
- “Load” can also refer to non-sport stressors and “internal” loads, which are legion. Psychology, for instance, probably does matter: anything from daily hassles to major emotional challenges, as well as stresses related to sport itself.
- Nyhus Hagum C, Tønnessen E, Hisdal J, Shalfawi SAI. The effect of progressive and individualised sport-specific training on the prevalence of injury in football and handball student athletes: a randomised controlled trial. Front Sports Act Living. 2023;5:1106404. PubMed 37346384 ❐ PainSci Bibliography 49671 ❐
Forty-two Norwegian students were divided into two groups before entry into a sports academy. Half didn’t prepare, and the other half did “weekly progressive, individualized sport-specific training programs.” Each student had their own plan for “increasing the training load gradually when the athlete had adapted to a specific training load or stimuli.” Baby steps, tested.
In their first three months of play, the students who prepared suffered far fewer injuries, a rate of just 11% compared to 19% for any injury, and 7% versus 10% for more serious ones. That’s a 1.8× greater risk of injury for the unprepared, which is quite dramatic.
This is a clear and plausible result, but the small sample of convenience reduces its power quite a bit, and they didn't account for previous injuries. The strength of the result could be a fluke.
- Beyer R, Kongsgaard M, Hougs Kjær B, et al. Heavy Slow Resistance Versus Eccentric Training as Treatment for Achilles Tendinopathy: A Randomized Controlled Trial. Am J Sports Med. 2015 Jul;43(7):1704–11. PubMed 26018970 ❐
Trials have shown promise for eccentric training (contracting while elongating) for Achilles tendinitis (and other tendinitises), but … does it really have to be “eccentric”? Maybe any resistance training will do the job. This trial was designed to test that by comparing eccentric training to a more conventional weightlifting style of heavy slow resistance training.
They tested both approaches for three months in a few dozen people with chronic midportion Achilles tendinitis. The tendons changed! “Significant reduction in tendon thickness and neovascularization”! But …
None of these robust clinical and structural improvements differed between the ECC and HSR groups.
Eccentric wasn’t better. It was actually a little worse in one way: amusingly, people were more satisfied doing the regular exercises — probably because they’re less tedious!
- Rathleff MS, Mølgaard CM, Fredberg U, et al. High-load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12-month follow-up. Scand J Med Sci Sports. 2015 Jun;25(3):e292–300. PubMed 25145882 ❐
Raise a little heel 🎶 raise a little heel 🎶 raise a little heel! If you don’t like what you got, why don’t you change it? If you know there’s something wrong why don’t you right it?
Trooper, from the classic song, “Raise a Little Heel”
In 48 plantar fasciitis patients, Rathleff et al. compared the effect of stretching to heel raises (AKA repeatedly standing up on your tip-toes). A towel was inserted under the toes for a little extra angle. When patients were able to comfortable manage a dozen slow lifts every other day, they added weight: a backpack full of books. Elegant simplicity! They kept this regimen up for several months … but it didn’t take long to help. Although everybody got better eventually, the heel raisers got better a lot quicker than the stretchers. They were already much better off after three months.
This isn’t proof that heel raises are going to work … but it’s more than good enough to justify trying it. Obviously we’ll hope to see replication by other researchers.
- Van Der Heijden RA, Lankhorst NE, Van Linschoten R, Bierma-Zeinstra SM, Van Middelkoop M. Exercise for treating patellofemoral pain syndrome: an abridged version of Cochrane systematic review. Eur J Phys Rehabil Med. 2016 Feb;52(1):110–33. PubMed 26158920 ❐
This paper is the abridged version of a 2015 Cochrane review of exercise for patellofemoral pain, mainly strengthening. It reports on 31 trials including 1690 participants; it’s not the most recent review (as of 2024), but probably still the most credible. It’s not like the evidence situation has improved all that much! It likely remains “very low quality but consistent,” with nearly all of them being “at high risk of performance bias and detection bias due to lack of blinding.”
Despite that, the consistency does suggest that “exercise therapy benefits patients with PFP” — and it also seems clear that we still don’t know the best kind of exercise, and “it is unknown whether this result would apply to all people with PFPS.”
- Raman J, MacDermid JC, Grewal R. Effectiveness of different methods of resistance exercises in lateral epicondylosis—a systematic review. J Hand Ther. 2012;25(1):5–25; quiz 26. PubMed 22075055 ❐
This systematic review of studies for tennis elbow considered just twelve experiments, selected from several hundred candidates. The quality of the trials was generally poor, with only two that would have gotten better than about a C+ grade in school, so it’s got a bit of the “garbage in, garbage out” like most reviews in this field. Good news, though: all of them came to the same plausible conclusion that “resistance exercise resulted in substantial improvement in pain and grip strength.”
The authors note that “optimal dosing is not defined” — that would take a lot more research, and even the research summarize here isn’t adequate. But it is consistent, at least. It also harmonizes with data on strengthening for other repetitive strain injuries.
- Many therapists would protest this point, and in many cases their argument would be: “But muscle balance is a the factor in postural dysfunction! How can you possibly say we don’t diagnose and treat for muscle imbalance?” Oh, don’t get me started! This is really quite easy to answer. A structuralist will invariably emphasize the effect of the muscle tension on symmetry, while I would totally ignore the effect on posture and focus on the actual state of the muscle tissue itself as the problem. A structuralist would also choose a lot of treatments like stretching and strengthening to try to resolve the “imbalance” and “straighten” the poor crooked human. If they choose trigger point therapy at all — if they even know what it is — chances are it’s a back burner skill for them and they aren’t really knowledgeable or qualified. So despite superifical appearances of similarity, a structuralist’s approach to muscle tension is really different than what I’m talking about here.
- Bursitis actually has a very distinctive pain quality, very specific, hot, and sensitive even to light touch, like an infected hangnail. But I’m splitting hairs. These differences are quite subtle for the non-expert.
- Andersson G, Forsgren S, Scott A, et al. Tenocyte hypercellularity and vascular proliferation in a rabbit model of tendinopathy: contralateral effects suggest the involvement of central neuronal mechanisms. Br J Sports Med. 2011 Apr;45(5):399–406. PubMed 20605910 ❐ The “exercise” was electrically stimulated contraction of the triceps surae muscle, as well as a bunch of passive movement (basically just moving a rabbit’s foot over and over again, like that robot chair-stresser at Ikea). Three groups of rabbits were subjected to variations on this regimen, while a fourth group was left unmolested, for comparison purposes. The exercised rabbits showed more tendon cells and blood vessels after three weeks, and signs of damage after six: an overuse injury. The results show the difference between exercise (a good thing) and over-exercise (too much of a good thing).
- Pain itself can change how pain works, so that patients with pain actually become more sensitive and get more pain with less provocation. For more information, see Sensitization in Chronic Pain: Pain itself can change how pain works, resulting in more pain with less provocation.
- Neogi T, Frey-Law L, Scholz J, et al. Sensitivity and sensitisation in relation to pain severity in knee osteoarthritis: trait or state? Ann Rheum Dis. 2015 Apr;74(4):682–8. PubMed 24351516 ❐ PainSci Bibliography 53256 ❐
In more than 2000 people with knee osteoarthritis, or at high risk for it, pain sensitization was associated with knee pain, but not the severity of arthritis as seen on x-ray. Neither pain nor sensitivity clearly correlated with the condition of their knee.
This contradicted the researchers’ expectation that sensitization is driven by the duration and severity of arthritis. Instead, the results suggest that:
sensitization is in fact a ‘trait’ rather than a ‘state’, that is, that hypersensitivity was present before knee osteoarthritis, related to an individual’s predisposition to sensitization rather than being induced by peripheral nociceptive input [pain] from osteoarthritis.
Even more simply stated: people with knee pain have a problem with pain itself, not knees, to at least some extent.
- Elattar O, Choi HR, Dills VD, Busconi B. Groin Injuries (Athletic Pubalgia) and Return to Play. Sports Health. 2016 Jul;8(4):313–23. PubMed 27302153 ❐ PainSci Bibliography 53620 ❐