A Rational Guide to Fibromyalgia
The science (and not the pseudoscience) of the mysterious disease of pain, exhaustion, and mental fog

“Fibromyalgia” is common disease of widespread chronic pain and malaise without a known cause, the ultimate non-diagnosis. Some people will eventually discover a specific cause — there are several surprising causes of pain that can be overlooked for years at a time — but many never find out what’s going on. Some people do get better, but most do not.
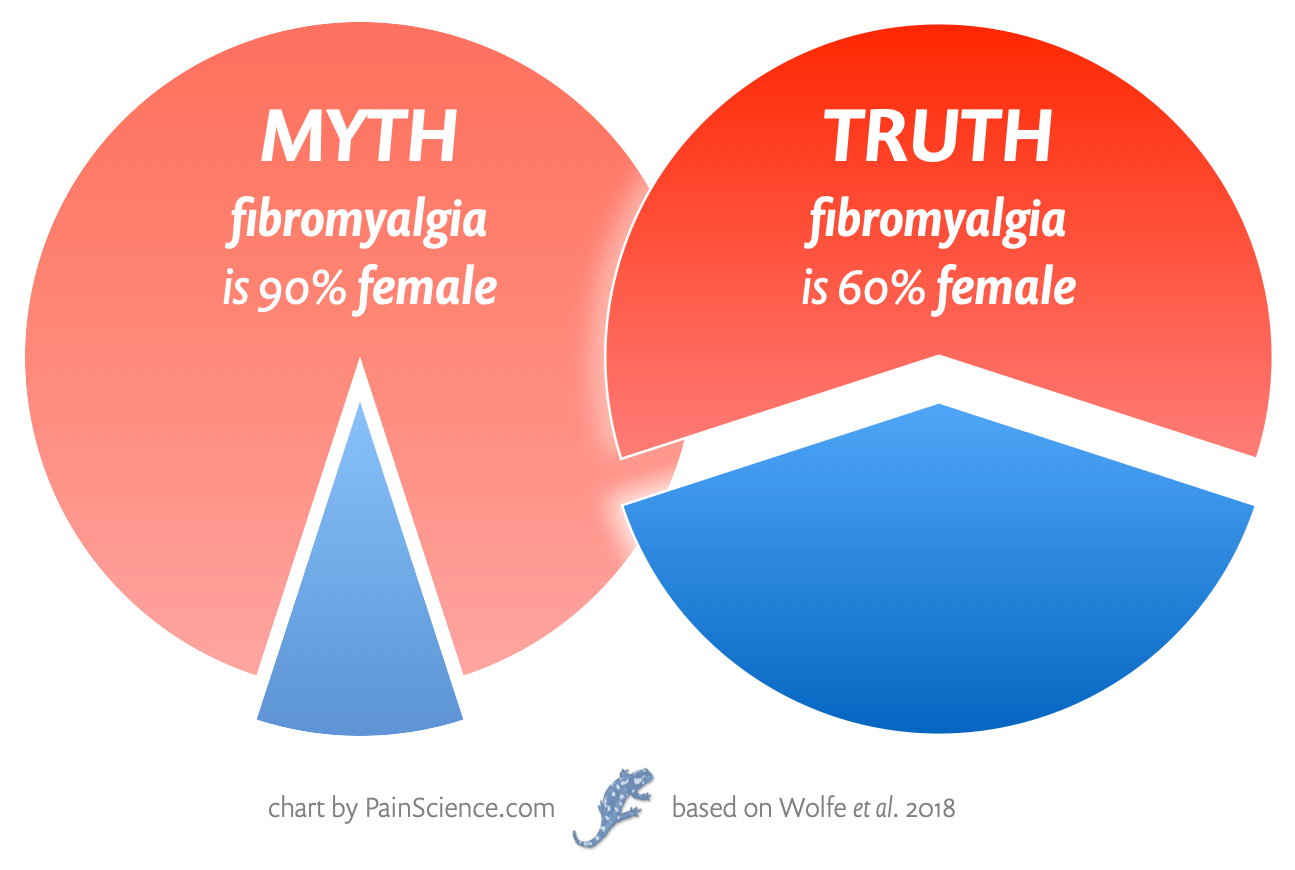
More precisely now: fibromyalgia is a label for a pattern of unexplained stubborn chronic pain,1 stiffness, mental fog, and fatigue … although “fatigue” is an understatement so severe that it’s misleading. It shares that with chronic fatigue syndrome (ME/CFS). It often goes with conditions like irritable bowel syndrome, migraines, and mood disorders. About 1–2% of the population suffer this way — a huge number!2 It is not rare, and affects more women than men — but not nearly as many as widely believed.3
The pain of fibromyalgia is often not particularly severe in any given moment, but intensity alone cannot tell the story: it’s the relentlessness of it that's particularly disconcerting. The multiplication of intensity by duration can make a “mild” pain into a nightmare, like water torture. When you don’t know why it’s happening, it’s hard to optimistic about when it will end. It’s the persistent, diverse, and mysterious character of the pain that make it terrible. Despite all that, the low intensity often discourages fibromyalgia patients from seeking help — or from being taken seriously when they do.
There are some known biological signs of “real” illness in most fibromyalgia patients, but otherwise the pathology remains a near perfect mystery. There are intriguing theories only. For instance, some experts now believe that fibromyalgia is a disease of pathological neurological sensitization — an overactive alarm system — but this remains unproven, and is awkwardly at odds with other things we do know about the condition.
It’s possible that fibromyalgia is the fragile, exhausted feeling that can be caused by any illness, a generic sign that something is wrong, and that something could be almost anything that has no other clear symptoms.
It was fun getting an AI to generate this word art. 🙂 Choosing imagery for “fibromyalgia” is very tricky, but it never occurred to me to just use the word itself… and then a reader suggested it. *chef’s kiss* I’m kicking myself for not thinking of it!
Controversy, stigma, and quackery swirl around fibromyalgia like a bad smell
People with fibromyalgia quickly learn to be cautious who they share the diagnosis with, because so many people think it’s nearly synonymous with hypochondria, anxiety, weakness, and a bad attitude.4 This even includes many healthcare professionals, most of whom are profoundly ignorant about fibromyalgia, and it is one of the best single examples of how hard it is to find good help for chronic pain.5 It is often not diagnosed when it should be, and even more often these days it is diagnosed when it shouldn’t be.6 No medical specialty specializes in it. Rheumatologists and neurologists often get “stuck” with fibromyalgia patients, but have no idea what to do with them unless they’ve taken a special interest in the topic, and few do.
There is no medical consensus on how fibromyalgia should be treated,7 and no one should feel bad about not knowing how to manage it: it’s literally one of the hardest problems in medicine. And although fibromyalgia research is booming, most of it is worthless, junk science whipped up to pad resumés and reputations.
And so alternative medicine has rushed into the medical gap with a dizzying array of crackpot cures, of course — and this article has no patience with those. There will be debunking.
But science and medicine have clearly also let fibromyalgia patients down. Far too many doctors still obnoxiously believe it’s “all in your head” (much like migraines were until surprisingly recently) — an idea that combines disastrously with sexism and other prejudices.
Here’s a solid 1-minute video primer on fibromyalgia from One-Minute Medical School:
Classic fibromyalgia symptoms
- chronic widespread pain and stiffness8
- excessive episodes of pain in specific areas, especially neck and back pain, headaches, and abdominal pain (irritable bowel syndrome)
- fatigue, exercise intolerance
- cannot sleep, or just never feel rested
- mood disorders (depression, anxiety disorder), and mental fog (the infamous “fibrofog”)
Many fibromyalgia symptoms are maddeningly non-specific: that is, they could be the symptoms of practically anything… or nothing. Headaches are the single most common pain complaint, but most have no specific cause. Most diseases cause fatigue! And pain is the most basic response to biological adversity that there is. And every other person you pass on the street is depressed, anxious, insomniac, or all of the above.
It’s almost like fibromyalgia’s symptoms are just a list of the most common sufferings of humanity. It’s only when they cluster and persist — a strong, stubborn pattern dominated by pain — that a diagnosis of fibromyalgia can be taken seriously.
“Fibromyalgia” is a medical UFO: the diagnosis is descriptive, not explanatory
Fibromyalgia is not an explanatory diagnosis. It sheds no light on the nature of the beast; it’s just a label for a distinctive pattern of symptoms. It doesn’t “explain” the condition any more than “UFO” explains a strange object in the sky. Unidentified flying objects aren't identified — it’s right in the name! — and so seeing one doesn’t mean you’ve seen a UFO. And a “diagnosis” of fibromyalgia doesn’t imply any specific cause either: it’s just the word we use to describe feeling a certain way, badly enough, for long enough.
YOU: I have unexplained chronic pain.
DOCTOR: You may have fibromyalgia.
YOU: That is literally what I just said.
Thanks to this confusion, patients often think the diagnosis is more meaningful than it is, like in this case: “Finally, in 1998, McCullough was diagnosed with fibromyalgia, a condition that had only been given a name a decade before. After seven long years, she finally knew what was wrong.”9 But she knew no such thing! She had been classified, that’s all. Don’t get me wrong, getting a diagnosis does have value — but not explanatory value in this case.
The term “UFO” does not explain a strange object in the sky — it only labels the mystery, just like “fibromyalgia.”
Medically unexplained symptoms (MUS) are the UFOs of medicine, and fibromyalgia involves a small flock of them. You could define fibromyalgia for a doctor by saying “it’s a case of MUS dominated by pain.” Calling it fibromyalgia might make it seem like something more specific, but it’s not: it’s still just a pattern of unexplained symptoms, technically a “syndrome” with an idiosyncratic name. Calling it “chronic pain syndrome” would be more honest and clear, but that’s not how things worked out.
A UFO technically refers to an unexplained phenomenon, but that reality is overshadowed by the popular suspicion that it’s aliens! In There is also a popular suspicion about what’s really going on with all MUS: hypochondria! Great numbers of doctors still tend to assume that a fibromyalgia patient is suffering from psychosomatic symptoms. And this is routinely exaggerated by sexism. Fortunately, some doctors understand that there’s probably a better explanation:
Clearly there are many patients who have chronic diffuse pain, fatigue, poor sleep, and other comorbidities. These symptoms often take a great toll on quality of life. Nothing in the scientific discussion about fibromyalgia as a diagnosis calls into question these symptoms. The question is entirely about how we understand the possible cause or causes of these symptoms in order to guide our treatment and research.
Neurologist Dr. Steven Novella, “Is Fibromyalgia Real?”
An avalanche of useless fibromyalgia research
Dr. Fred Wolfe is as expert as a fibromyalgia expert can get: he’s largely responsible for the official diagnostic criteria for fibromyalgia (the original in 199010 and then the important revisions in 2010, 2011, and 2016111213 which, in a nutshell, ditched “tender points,” factored in symptom severity, and eliminated exclusion criteria).
Since 2013, Dr. Wolfe has been blogging erratically but superbly, and in this short post he explains (with snark!) how fibromyalgia is being buried by an avalanche of crappy, useless research.
PubMed reports 659 publications in the last 12 months relating to fibromyalgia. For those who are interested, there are 9,366 articles listed in all the years that data are available. For 1990, the year the American College of Rheumatology 1990 fibromyalgia criteria were published, PubMed cites 95 articles. If you think that after all these years of research you and your patients are much better off, think again. A kind, conscientious physician treating a fibromyalgia patient in 1980 or 1990 will have done as well as the 2016 health workers with access to all of these new publications and expensive if not very efficacious medications.
This is important to bear in mind for the rest of the article. There is very little solid scientific ground in this topic, and that will be most obvious with big meta-analyses of fibromyalgia treatments like Mascarenhas et al., a spectacular case of “garbage in, garbage out” analysis: 220 studies of almost 30,000 people… mostly too junky to prove anything.14
Part 2
Nature of the beast
Types of pain and where fibromyalgia fits in (or doesn’t)
There are two main “conventional” kinds of pain: nociceptive and neuropathic. And yet fibromyalgia doesn’t seem to fit into either.
- The most familiar kind of pain is nociceptive, a type of sensation caused by potential damage to tissues, which is reported to the brain for assessment and modulation before pain is perceived.
- When the reporting system itself is harmed — a crushed nerve, say — you get neuropathic pain.
Two kinds of damage, two kinds of pain.
Fibromyalgia is often classified as something else, a third category, a dysfunction. It involves no confirmed damage to the nervous system, just its apparent misbehaviour, and so it’s not technically welcome at the neuropathy club. It was welcome there, before 2011! But the definition of neuropathy changed to officially exclude anything that didn’t involve a known lesion.15
Maybe there are unknown lesions? Fibromyalgia could simply be a obscure source of nociceptive or neuropathic pain. For instance, maybe someday we’ll learn that most fibromyalgia is caused by some kind of subtle damage to the nervous system, making it a neuropathy.16 There are at least two theories about subtle lesions of this type.17 That would make it just another neuropathy after all, ho hum.
But for now it’s still more plausible that it’s a dysfunction that doesn’t fit into those conventional categories, arising from widespread problems in a complex system, probably at least partially heritable,18 and so no definite and specific point of failure will ever be discovered.1920
But who knows. Science is not finished with fibromyalgia. Hell, it’s hardly begun.
Meanwhile, what do we call this kind of pain? And other miserable pain problems (complex regional pain syndrome, irritable bowel syndrome) that arise from neurological dysfunction? No one has decided. File under “other” for now. But I personally favour “algopathic” pain: pathological perception/sensation.21 It’s the Greek way to say “pain disease.” For more naming possibilities, see The 3 Basic Types of Pain.
What about “central sensitization”?
Fibromyalgia involves more pain with less provocation, a state that is generally known as sensitization. This sensitivity is due to changes throughout the nervous system, many of them mediated by the immune system. Neurology and immunology are elaborately entangled.
Some patients may even feel pain when touched softly, a terrible thing. Fibromyalgia can be hell. (See “allodynia.)
It has become trendy lately to “explain” fibromyalgia with central sensitization especially: that is, pathological sensitization driven by abnormal changes in the central nervous system, making it a disease of dysfunctional perception of pain, misinterpretation of normal nerve signals at the highest level: “hallucinating pain.” This often crosses over into the idea that the sensitization is driven by psychological factors, making it essentially a very fancy way of saying “all in the your head.”
CS clearly occurs in fibromyalgia, but it doesn’t explain it, any more than arterial plaques “explain” heart disease. It’s just a more precise description of the problem (maybe). Even if fibromyalgia is 90% CS, you still need to explain that, which is just as hard a puzzle as why someone would get fibromyalgia. Why would someone get terrible central sensitization? It’s practically the same question.
There’s also plenty going on in fibromyalgia that is not necessarily explained by central sensitization — like fatigue and mental fog, particularly.
It’s important to understand that sensitization is usually a perfectly normal response to trauma and disease. It is basically just the nervous system making us take a physiological situation more seriously. The question with fibromyalgia is whether sensitization is a response to some other disease process that has no other prominent symptoms … or whether the sensitization is the disease process, a kind of complex neuropathy, and the main driver of the problem.
Either way, we don’t know the why of it. Don’t let anyone tell you they have the answers to these questions!
Inflammation as the driver of sensitization
Maybe it’s the constant irritation of systemic inflammation. I think that might get me feeling mighty sensitive.
Fibromyalgia patients do seem to be on fire a little bit: in 2017, Bäckryd et al. studied inflammatory markers in fibromyalgia patients in much greater detail than ever before, and identified an “extensive inflammatory profile.”22 It’s conceivable that this is caused by sensitization, but it’s more likely the other way around: being constantly inflamed all over for a long time turns people into wrecks of sensitization.
If fibromyalgia patients are more inflamed than sensitized, that doesn’t really help us all that much, because we still don’t know why people get so inflamed in the first place — it’s just another puzzle, like the sensitization. There’s always another layer. But it does feel a little less bizarre than a malfunction consisting of “pure” sensitization without inflammation. Bäckryd et al. write:
Fibromyalgia seems to be characterized by objective biochemical alterations, and the lingering characterization of its mechanisms as essentially idiopathic or even psychogenic should be seen as definitively outdated.
But they don’t attempt an explanation of the inflammation they found. 😜
I’ll return to the topic of inflammation below when I discuss my own “inflammaging” hypothesis.
Whenever something painful happens to me, amid all the distress I am surprised at being reminded of how painful pain is. That thought is always followed by another, “What if I hurt like this all the time?” Chronic pain syndromes are extraordinarily debilitating.
Why Zebras Don’t Get Ulcers, by Robert M Sapolsky, p. 396
Is fibromyalgia a “diagnosis of exclusion” or “wastebasket diagnosis”?
Fibromyalgia is still routinely and incorrectly called a diagnosis of exclusion. I did so myself in earlier versions of this article, until I was corrected in early 2021. Although technically wrong, the term is also a seed of truth in a practice-vs-theory way. It’s useful to break this down. And “wastebasket” diagnosis is also worth understanding — for entirely non-technical reasons.
A “diagnosis of exclusion” is achieved by a process of elimination, and that seems simple enough, but it’s not a well-defined concept. By its very nature it tends to only be applied at the edges of medical knowledge, where all fibromyalgia patients live — and things are kind of a mess on the frontier.
What is clear is that fibromyalgia is officially a criteria-based diagnosis these days. We know enough about the condition that specific features are required for diagnosis (Wolfe 2016 again). It is formally defined by what is wrong, not by what isn’t. That makes it a diagnosis of inclusion, not exclusion!
In practice, however, fibromyalgia is often still treated like a diagnosis of exclusion — something doctors tend to bring up only when most other possibilities have been eliminated.
What’s so bad about arriving at “fibromyalgia” by a process of elimination?
You might never get there! Or you might eliminate something you shouldn’t along the way.
Fibromyalgia often co-exists with similar conditions (e.g. rheumatoid arthritis). And so it would be a serious mistake to consider fibromyalgia only in their absence — you might miss the fibromyalgia that is also going on!
Or you might erroneously rule out something like rheumatoid arthritis in your eagerness to explain the symptoms with fibromyalgia.
Don’t rule out ruling-out yet
Exclusion still has a role to play. Right up until 2016, some of the diagnostic criteria were still officially “exclusion criteria” — that is, the diagnosis required exclusion of other conditions. Exclusion had to be included! Is your head spinning yet? It’s not just yours! This was a tad confusing for everyone, including pros, and so the 2016 revision eliminated “the previously confusing recommendation regarding diagnostic exclusions.”23
And yet you cannot entirely eliminate exclusion criteria without throwing some baby out with your diagnostic bathwater. As Wolfe et al. also wrote (my emphasis), “Criteria are to be used after diagnostic possibilities have been narrowed through medical evaluation….”
In short, don’t exclude everything before you start thinking about fibromyalgia, but definitely exclude some things. Here’s a good take from Galvez-Sánchez et al.:24
The need to exclude other related diseases and perform a differential diagnosis has been a somewhat contentious issue with respect to the 2010 ACR criteria. … The strength of the 2016 criteria is the elimination of the previous, confusing recommendations related to diagnostic exclusion. In the 2016 criteria, a diagnosis of FMS does not exclude the presence of other clinically important illnesses.
… in spite of the previous recommendation, the diagnosis of FMS continues to be fundamentally based on the exclusion of other similar diseases in the clinical context.
Clear as mud, right? Again, the basic problem here is that “diagnosis of exclusion” is not actually a well defined term.25 There is lots of messy overlap between “criteria-based diagnosis” and “diagnosis of exclusion” in the real world. Accidentally eliminating things that should not be, or failing to eliminate what should be, is an occupational hazard that just can’t be entirely … eliminated.
And then there’s “wastebasket” diagnosis
A “wastebasket diagnosis” is a junky diagnosis of exclusion: a careless and ignorant process of elimination, instead of an earnest and educated one.
Wastebasket diagnosis is defined by obnoxiously non-medical motives. What motives? At best, it’s a diagnosis given as a pacifier, a kind of diagnostic placebo — well-intentioned but misguided. At worst, it’s a way to just create the appearance of a diagnosis, to justify passing the buck to another physician, to get rid of a patient.
It’s the diagnostic equivalent of pretending to throw a ball for a dog: “Go get it, girl!”
Sadly, “fibromyalgia” is still frequently diagnosed this way in the real world.
Conditions that may be confused with fibromyalgia
Practically everything that can go wrong with human biology seems to be able to cause any of the classic non-specific symptoms that define fibromyalgia. Many people troubleshooting weird health problems have bitterly made the observation that “everything causes everything.” Nearly any symptom can and will occur in at least some people as an atypical variation of nearly any disease.
So this is tricky! But here are some of the conditions that are the most likely to masquerade as fibromyalgia for long periods.
- Myofascial pain syndrome, a closely related diagnosis that mostly exists to try to explain widespread pain — but not so much the fatigue and malaise that fibromyalgia also clearly involves. More on this one below.
- Hypermobile patients get hurt easily and have a lot of chronic body pain. Hypermobility is often the only clear sign of a complex underlying connective tissue disorder, and these patients routinely suffer for years without diagnosis, if not forever. Read more.
- Autoimmune diseases like multiple sclerosis, lupus, and ankylosing spondylitis are often extremely difficult to diagnose in their early stages (“prodrome”) and may strongly resemble fibromyalgia. There is a strong causal link between MS and Epstein-Barr virus, confirmed in 202226 — so we know that the pathological wheels are in motion long before MS patients know they have MS. And we know that weird aches and pains and other woes are extremely common in multiple sclerosis patients up to five years before diagnosis.27
- Myelopathy is the result of spinal cord insult, which can be surprisingly subtle. It is hardest to diagnose when the irritation is intermittent and minor, as with positional cervical cord compression, the pinching of the spinal cord in specific positions only. The erratic and often slight irritation of the spinal cord can cause an incredible variety of symptoms, especially pain and stiffness, which can easily get chalked up to “fibromyalgia.” Multiple-level radiculopathy — many pinched nerve roots — may also resemble myelopathy.
- Mood disorders (depression, anxiety disorder), all of which can cause surprisingly intense physical symptoms, including and especially pain and fatigue
- Vitamin D deficiency is surprisingly common, hard to rule out, and its symptoms are so similar to fibromyalgia that they are practically twins. For much more information, see Vitamin D for Pain. And there’s a third twin …
- Vitamin B12 deficiency is a clinical clone of D deficiency — major symptom overlap, surprisingly common, unreliable testing — but is often more ominous and difficult to treat. See Misconceptions about a B12 deficiency.
- Celiac disease is an “allergic” reaction to gluten, the protein in wheat, barley, rye that makes bread scrumptiously chewy. It is yet another surprisingly common and under-diagnosed condition, notorious for causing a bewildering array of symptoms, and (importantly) not necessarily digestion trouble (although that is common). Countless people have probably been labelled with fibromyalgia before finally getting a celiac diagnosis. And then there’s also the hairy topic of non-celiac gluten “intolerance”.
- Hypothyroidism — which is, fortunately, relatively easy to rule out decisively.
- Some cancers in their early and middle stages can cause mostly just pain and malaise. What finally usually makes a cancer obvious is lumps, weight loss, and the development of other acute symptoms as tumors get big enough to cause trouble.
- Lyme disease (Lyme borreliosis) is an infection that notoriously causes pain, fatigue, stiffness, but also usually involves enough other distinctive symptoms that it can be distinguished from fibromyalgia. Chronic lyme disease is the long-term painful aftermath of some lyme infections, very much like Long COVID in that it clearly exists, and yet we don’t understand it — except, in the case of Lyme disease, maybe we finally do!28
- Small fibre peripheral neuropathy is caused by damage to the most delicate nerves in the body, the unmyelinated “bare wires” of the nervous system. This causes erratic pain, weird sensations, and numbness.29 It has many possible causes, including some of the conditions above, and a large percentage of cases are never explained. SFN could be a cause and/or consequence of fibromyalgia. For now, I will not examine this topic in detail, because of a very high “maybe, maybe not” factor.
- Myalgic encephalomyelitis (also known, less precisely, as chronic fatigue syndrome) is a distinctive disease state that seems to be present in most if not all people with severe chronic fatigue syndrome… and probably also in many fibromyalgia patients. It is likely that ME and FM overlap, but it’s not clear how much or in what way. Their relationship remains a scientific mystery.
Fibromyalgia can be confused with almost any condition that corrodes your vitality or causes weird aches and pains (which is quite a huge list), but without other obvious signs/symptoms that would expose them for what they really are (which is mercifully shorter).
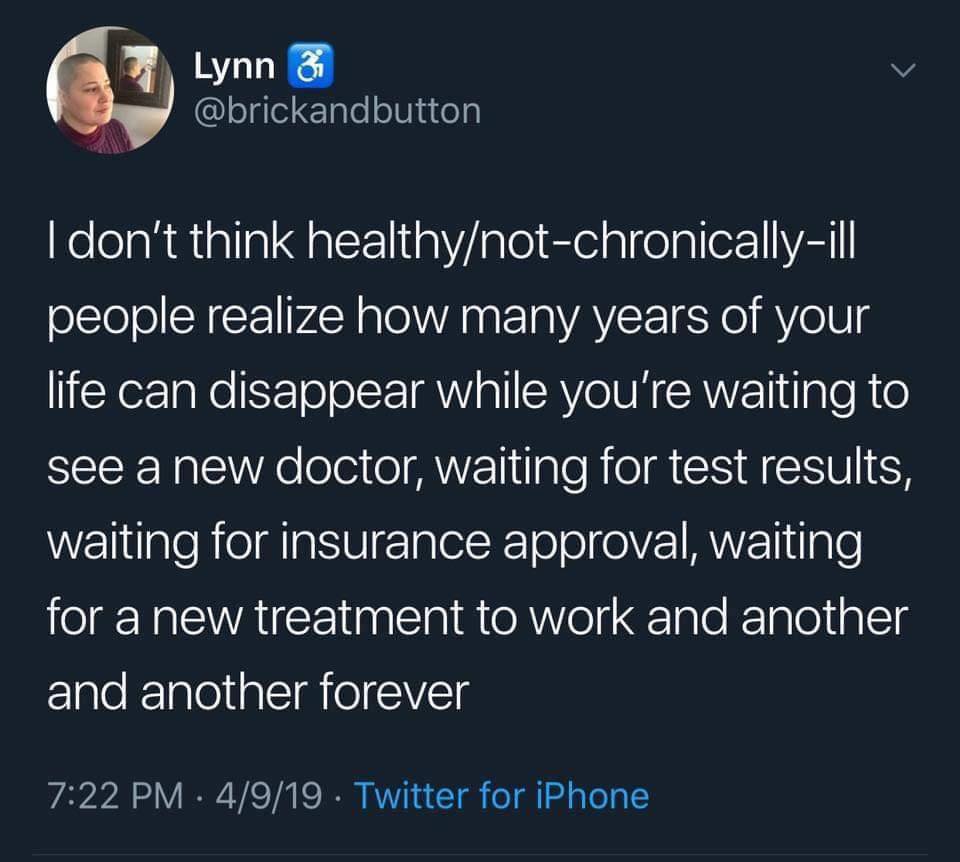
This was written by Lynn (@brickandbutton) on Apr 9, 2019 [original gone]. She added in a comment: “I’ve come to a point after 7 years where I’m still fighting (and waiting) but I expect to be this severely sick forever. Anything else will be a fun surprise.”
The particularly tricky relationship between fibromyalgia and myofascial pain syndrome
They may be related but distinct. Or it may be a word game: different words for different aspects of the same thing. But they are almost certainly not exactly the same thing.
Like fibromyalgia, “trigger points” is another label for a poorly understood phenomenon: sore spots in muscles, which sometimes feel like hard lumps. They are probably little micro cramps, small lesions in muscle tissue,30 as common and unpleasant as pimples (and sometimes a lot worse). When people seem to have many and severe trigger points, another arbitrary diagnostic label is often applied: “myofascial pain syndrome,” which is yet another way of saying “chronic pain syndrome” — but this particular name strongly implies a soft tissue origin.
Severe MPS and mild fibromyalgia are nearly impossible to tell apart. Trigger points and MPS may just be the tip of the fibromyalgia iceberg, or they may be different things with similar symptoms. No one knows.
Most people with fibromyalgia seem to have more than their fair share of trigger points, but it’s hard to tell because people with fibromyalgia tend to be sore everywhere. And yet many people with trigger points would never be diagnosed with fibromyalgia. Robust, healthy people can have temporary trouble with a trigger point.
Tender points vs. trigger points
- Trigger points describe localized pain that can occur in almost any location, but typically occurs in muscles, and which can come and go like the weather, and are often not associated with any other symptoms.
- The tender points of fibromyalgia are a carefully chosen set of spots that tend to be sensitive on anyone, but are excessively sore with FM. It’s not that FM makes those spots sore — it’s that FM makes everything sore, which is most obvious at those spots.
Positional cervical cord compression and fibromyalgia
One of the most interesting ideas to emerge from the fibromyalgia research mess is the possibility that the pain is caused by a subtle pinching of the spinal cord, a form of myelopathy — symptoms caused by poor spinal cord function. The cervical spinal cord is a neurological bottleneck through which every nerve impulse from or to the body must pass. Symptoms caused by trouble at this level of the spinal cord are notoriously variable and can cause trouble essentially anywhere, such as — and this is not widely appreciated — shooting pains in the backs of the legs (sciatica).32
As all over the map as they are, there’s a suspicious overlap between the symptoms of myelopathy and fibromyalgia. Many fibromyalgia patients are quite myelopathy-ish, but without enough classic myelopathy symptoms to attract that diagnosis. Could they be related? Could fibromyalgia be a sub-category of myelopathy?
This possibility was first exposed in a 2004 paper by Heffez et al.,33 and then substantiated in a follow-up study in which they successfully treated 40 fibromyalgia patients by surgically relieving the pressure on their spinal cords.34 This research has virtually been ignored by everyone except Dr. Andrew Holman. His 2008 replication study showed that minor spinal cord pinching was present in a shockingly high percentage of patients with fibromyalgia and chronic widespread pain: about seventy percent of them.35 Specifically, he reported positional cervical cord compression (PC3), which is pinching of the spinal cord that occurs only or mainly in specific positions (mostly with the head tilted back).
And treating PC3 seems to show some promise for treating fibromyalgia. (There’s a whole section about treating PC3 below.)
Unfortunately, conventional MRI images, taken with the neck in a neutral position, will miss a lot of PC3 — at least half.36 Neurologists who would otherwise be interested in fibromyalgia patients may dismiss them because their myelopathy-like symptoms can’t be explained by a neutral MRI that does not reveal the PC3.
The fascinating implication of all of the above: erratic low-grade irritation of the cervical spinal cord could actually be a direct, specific, and mechanical cause of fibromyalgia. That’s a dramatic and sensational hypothesis, but it’s not outrageous. We already know that myelopathy is spooky and unpredictable and often involves widespread pain. We also know that intermittent compression of nerves causes different kinds of symptoms in the peripheral nervous system than constant pressure (see last few citations above), so it’s not much of a reach to guess that the central nervous system also responds differently: an atypical, subtle myelopathy, caused by pinching that’s invisible to all but the most thorough MRI examination … a diagnostic technology that is notoriously unreliable!37
It would hardly be a shock if such a thing had been missed until now.
And then there’s the “autonomic arousal” thing!
There’s one final mind-blowing piece of the PC3 puzzle: irritation of the cervical spinal cord may have unusual properties, different from other parts of the spinal cord. Specifically, PC3 may cause strong arousal of the autonomic nervous system … the same effect as severe chronic stress.
If that is the case, the implications would be astonishing: it would simultaneously provide an organic explanation for many cases of fibromyalgia and support the idea that the disease can also be caused by external stresses. That is an awfully potent explanation for a whole lot.
This suggests that stress could be the underlying mechanism of fibromyalgia — but it can be either life stresses, or “artificial” stress caused by a messed up spine. •mind blown•
All unproven. All needs more research. But there’s a lot of veeery interesting smoke here. There’s even evidence of a similar link with chronic fatigue syndrome!38 And speaking of CFS.…
Two more advanced topics in this article are reserved for members only at this time:
- The fatigue connection: is fibromyalgia just CFS/ME with extra pain? Many people have speculated — people who don’t know better — that fibromyalgia is just CFS/ME with pain as a more prominent symptom. The confusion is understandable, but it needs to be crushed.
- A genetic defect that exaggerates all sensation is closely linked to fibromyalgia.
I choose dorkier, more detailed content to put behind the paywall. More practical information, especially for patients, is kept free — and 95% of the article remains free. But this article will slowly grow into a book, and someday it will all be behind a paywall, so read it while you can. 😉
Most PainScience.com content is free and always will be.? Membership unlocks extra content like this for USD $5/month, and includes much more:
Almost everything on PainScience.com is free, including most blog posts, hundreds of articles, and large parts of articles that have member-areas. Member areas typically contain content that is interesting but less essential — dorky digressions, and extra detail that any keen reader would enjoy, but which the average visitor can take or leave.
PainScience.com is 100% reader-supported by memberships, book sales, and donations. That’s what keep the lights on and allow me to publish everything else (without ads).
- → access to many members-only sections of articles +
And more coming. This is a new program as of late 2021. I have created twelve large members-only areas so far — about 40,000 words, a small book’s worth. Articles with large chunks of exclusive content are:
- Quite a Stretch
- Does Epsom Salt Work?
- Heat for Pain and Rehab
- Your Back Is Not Out of Alignment
- Trigger Point Doubts
- Does Fascia Matter?
- Anxiety & Chronic Pain
- Does Massage Therapy Work?
- Does Posture Matter?
- A Deep Dive into Delayed-Onset Muscle Soreness
- Does Ultrasound or Shockwave Therapy Work?
- A Painful Biological Glitch that Causes Pointless Inflammation
- Guide to Repetitive Strain Injuries
- Chronic, Subtle, Systemic Inflammation
- Vitamins, Minerals & Supplements for Pain & Healing
- Reviews of Pain Professions
- Articles with smaller members sections (more still being added):
- → audio versions of many articles +
There are audio versions of five classic, big PainSci articles, which are available to both members and e-boxed set customers, or on request for visually impaired visitors, email me. See the Audio page. ❐
I also started recording audio versions of some blog posts for members in early 2022. These are shorter, and will soon greatly outnumber the audio versions of the featured articles.
- → premium subscription to the PainSci Updates newsletter +Sign-up to get the salamander in your inbox, 0–3 posts per week, mostly short, sometimes huge. You can sign-up for free and get most of them; members get more and their own RSS feed. The blog has existed for well over a decade now, and there are over a thousand posts in the library. ❐

Change or cancel plans any time. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism. For more information, see the membership page. ❐
The fatigue connection: is fibromyalgia just CFS/ME with extra pain?
Chronic fatigue syndrome (CFS), myalgic encephalomyelitis (ME), and fibromyalgia all often get conceptually tangled up. In the last year, it has become clear that ME is probably entirely or mostly synonymous with Long COVID, which is just the most famous example of a much older problem: post-viral syndrome, or lasting immune system jiggery-pokery in the aftermath of an infection (often severe, but not always). I think it’s getting pretty clear that ME is basically just another name for post-viral syndrome — for the neuroimmune meltdowns that sometimes follow infections.
Although the ME and CFS acronyms are routinely paired (ME/CFS), that frustrates some experts and patients,39 many of whom see ME as the real disease, and CFS as a vague and trivializing pseudo-diagnosis — like saying diabetes/unfit or Parkinson's/clumsiness. Everyone with ME has a bunch of fatigue, but not everyone who always feels fatigued has ME, even if it’s serious. People can be pathologically fatigued but without the distinctive features of ME. Fatigue is just a symptom with many possible causes, and "chronic fatigue syndrome" is merely a pattern of undiagnosed fatigue. But ME is a distinctive and nasty beast.
And myalgic encephalomyelitis isn’t fibromyalgia either, despite some similarities. Many people have speculated that fibromyalgia is just ME with extra pain, essentially the same condition but with symptoms that lean a little more towards pain. The truth is elusive. None of these conditions is defined well enough to exactly how much they overlap.
ME is mostly defined by its severity and resemblance to an illness. It can be savage, and even lethal.40 It’s a systemic neurological “meltdown,” probably usually provoked by a viral infection (but not necessarily); it occurs in epidemics and acts a lot like an infection — think Long COVID! ME causes measurable damage to brains, spinal cords, and organs, often disabling both mind and body. Fibromyalgia is mostly not like this, and in cases
The similarities between the two illnesses are minimal & superficial at best but their differences are truly profound.
Jodi Bassett, “M.E. vs Fibromyalgia”
Fatigue is the shared symptom of both conditions that leads people to suspect that they might have ME instead of FM, or their FM might actually be ME. But while ME is notorious for causing fatigue, it doesn’t always do that. And there’s a crucial difference between the “tiredness” and “brain fog” of fibromyalgia and the cardinal, required symptom of ME, which is not really fatigue but exercise intolerance that causes severe weakness and malaise. Most people with ME feel truly disabled by almost any activity, their brains suffer objective “neural consequences,”41 and exercise therapy notoriously backfires42 — a problem finally “officially” acknowledged in late 2020, after hard campaigning by patient activists.43
But many or most fibromyalgia patients actually benefit from exercise (more coming on this below, of course). ME patients would love to be merely fatigued and bleary.
Some patients diagnosed with fibromyalgia and/or CFS are probably undiagnosed ME patients. However, most are probably suffering from chronic fatigue/pain with other causes (like myelopathy, as mentioned at the end of the last section).
To sum up:
- Myalgic encephalomyelitis: a distinct physiological state, usually following infections, that causes severe exercise intolerance and, often, fatigue, pain, mental fog, and sleep disturbance as well (hence the confusion with fibromyalgia).
- Chronic fatigue syndrome: a loose, lousy term with a lot of baggage, a wastebasket diagnosis, just a label for unexplained chronic fatigue with many other possible causes, but including some that overlap with possible causes of FM.
- Fibromyalgia, more accurately called “chronic pain syndrome,” is another loose label for unexplained chronic pain with all the same kind of baggage as CFS, but with some stronger pathological themes (links to inflammation, spinal cord compression, etc). Nevertheless, it is probably a mixture of several problems — including, perhaps, some cases of ME!
Clear as mud!
A genetic defect that exaggerates all sensation is closely linked to fibromyalgia
There’s a respectable chance that chronic widespread pain patients can be identified by their genes alone. It has been clear for years that chronic pain patients are probably genetically distinctive. We recently got much stronger evidence of that from the largest study of the genetics of chronic pain patients to date, which found 76 genes that are independent risk factors for multisite chronic pain.44
But “it might be your genes” is vague and inevitable science news. Things get more interesting with the discovery that a DNA blooper can mess you up in a specific painful way. And so I think this might be the most interesting pain science of the year so far: chronic pain may be caused by a common genetic defect leading to low levels of the neurotransmitter serotonin.45
A common genetic defect, mind you. Not rare. At ten percent of the population, it’s about five times more common than red hair.
The study was trolling for genetic common denominators in people with a certain kind of chronic pain. They started with data on people suffering from chronic jaw pain. In that big group, they flagged some for further study: several dozen people who also suffered from excessive body sensations (“somatic awareness”). And they found that those people were all running on serotonin fumes.46
Patients with unexplained chronic widespread pain are notorious for having many, many other odd complaints — uncomfortably strong sensations of all kinds. Indeed, the pain often just seems to be the tip of an iceberg of abnormal sensations.
Unsurprisingly, this rather unflattering interpretation is probably wrong, and people with heighted somatic awareness are not just neurotic drama queens. Or another way of putting it: maybe they are, but they obviously have a good reason for it. Everyone alive has, at times, gotten unpleasantly fixated on an uncomfortable sensation, but try to imagine that happening much more often and more intensely than it “should.” See how calm you are.
So how do you know if you have this gene?
If you’ve always suspected that you feel things strongly, you already have a good clue. The researchers identified members of this club with a quiz only slightly more sophisticated that a Cosmopolitan questionnaire: “This 54-question self-test measures people’s tendency to notice and report a broad array of physical symptoms and sensations.” That page is focusing on using that test to identify symptoms of excessive stress and anxiety, but the whole point here is that there may be a genetic explanation for the same thing. Take the test. If you score in the top 25%, there’s a fairly strong chance that you too have the “somatic awareness” gene. And an explanation for your fibromyalgia!
↑ MEMBERS-ONLY AREA ↑
Some sketchy theories about fibromyalgia
In this section, I’ll quickly dismiss several all-too popular ideas about what causes fibromyalgia:
- repressed emotion
- energy disturbance
- adrenal fatigue
- defective metabolism
- infection and/or vaccination
- leaky gut syndrome
If you want to see who disagrees and why, the rest of the Internet is overflowing with people promoting these theories (and the exploitative cures based on them). But in my opinion this is a rogues' gallery of terrible ideas that barely deserve a mention, let alone a serious discussion.
Can we blame infections and/or vaccinations? It’s particularly popular to point a finger at diseases like hepatitis C, Epstein-Barr virus, parvovirus, and — of course — Lyme disease. These are all probably red herrings, however: “There is no clear-cut evidence of fibromyalgia or chronic widespread pain due to infections or vaccinations, no correlations with persistent infection, and no proven relationship between infection, antimicrobial therapies and pain improvement.”47 I don’t think it’s possible to completely rule out infections — microorganisms keeping turning up where we didn’t expect them — but if fibromyalgia is related to an infection, it’s a completely mysterious one.
How about defective metabolism? Excess phosphate? For many years, a common ingredient in cough syrups — guaifenesin, a chemical derived from a tree — has been prescribed as a natural treatment for fibromyalgia based on the idea that it purges an excess of phosphate, which allegedly accumulates due to [insert unclear metabolic defect]. That is what a skeptic would call an “extraordinary claim”: an overconfident explanation of a notoriously unexplained disease. The “guaifenesin protocol” is popular, but has very little expert support, even from alt-med friendly physicians, and was proven ineffective by its own proponents long ago,48 and fibromyalgia patients do not appear to have excess phosphate in the first place.49
Incidentally, guaifenesin is probably not even an effective cough syrup ingredient. •sad trombone•50 However, it is actually a muscle relaxant as well, and maybe that explains why some fibromyalgia patients are pleased with its effects.
Adrenal fatigue probably does not exist,51 so it is unlikely to be the explanation for fibromyalgia, or a major component of it. AF is supposedly caused by chronic stress and “burnout” of the adrenal glands, causing subtle systemic symptoms even in the absence of measurable deficiencies of the hormones they produce. “Adrenal insufficiency” is the legitimate medical problem of measurable and clinically significant deficiencies of those hormones, which can have many causes — but not “stress.” AF gets blamed for fibromyalgia because fatigue is the primary alleged symptom of AF, and also one of the primary symptoms of fibromyalgia. There could be a link relationship between stress and fibromyalgia, but it’s probably more subtle than burned out glands. There may be good reasons for fibromyalgia patients to reduce stress, but not because their adrenal glands are sputtering like a car low on gas. At best, it’s a simplistic guess about the effects of chronic stress that is currently at odds with the poor quality evidence but has a small chance of being vindicated someday. At worst, it’s dead wrong, but is a great way to sell books to fibromyalgia patients.
The answer to whether ‘adrenal fatigue’ or depletion exists or not may not be simple, but different answers can be offered according to the presence of an underlying disease. However, so far, there is no substantiation to show its existence.
Cadegiani et al., 2016, BMC Endocrine Disorders

Please don’t waste your money on aura massage.
An “energy disturbance” is the culprit according to many alternative medicine practitioners. The same practitioners will blame almost anything on disturbed energy, but mysterious problems like fibromyalgia are singled out for special attention. As long as there’s no better explanation available, “energy” remains a contender that many will take seriously, one of the gods of the pathological gaps. It’s the basis for treatment with acupuncture above all, followed in popularity by aura massage: ritualistic movement of the hands through the space around you, a technique ironically called therapeutic “touch” (or the Japanese version, Reiki). It’s all nonsense, debunked ad nauseam for decades now. Acupuncture is ineffective for all pain, never mind complex cases of unexplained chronic pain.52 Therapeutic touch practitioners can’t even detect auras in blinded tests.53 All the benefits derived from energy therapies are easily attributed to the good (social) vibes and optimism we get from being cared for and being impressed by healing rituals, a psychological phenomenon.
Repressed emotions is a common variant of the idea that fibromyalgia is caused by stress. It’s not ridiculous to say that stress might be involved in fibromyalgia, but it is probably ridiculous to put all the blame on emotional repression specifically. For instance, “hypno-psychotherapist” Louise Levy attributes fibromyalgia to “suppressed and repressed emotions such as rage, anger, fear, worry, sadness, hurt etc” and boasts that she has “successfully treated many people … to full recovery [sic].”54 Psychiatrist debunker Dr. James Coyne calls it “a pseudoscientific claim lacking in evidence or credibility” and “a throwback to discredited 1950s version of psychosomatic conditions.”55 Emotions go unrecognized and unexpressed for all kinds of reasons, of course, but it is not at all clear that this is a kind of toxicity that drives serious chronic pain.
Avoidance of psychic conflict is a variant of the repressed emotions theory. That’s a distillation of the tortured logic of Dr. John Sarno’s explanation of fibromyalgia as a “musculoskeletal mind-body syndrome” in his 1998 book, The Mindbody Prescription. It’s pretentious psychoanalytic nonsense, full of huge self-serving leaps of logic — but also exceedingly popular, because it suggests that all that stands between you and a cure is a bit of soul-searching and a convenient attitude adjustment. His book sold well and influenced millions. By all means, search your soul, adjust your attitude — just don’t expect it to fix fibromyalgia.
Leaky gut syndrome is a popular but seriously flawed and hypothesis that irritating “unnatural” modern foods perforate our bowels, so that their contents can seep out into the abdominal cavity and provoke an autoimmune reaction and cause… well, basically any health problem that doesn’t have another definite explanation. The main cure proposed is to eliminate everything from your diet that has ever been considered “irritating” or “unnatural.” The theory is much more full of holes than anyone’s gut, and is one of the most bogus of all common explanations for fibromyalgia. For more about LGS and links to detailed debunking, see my inflammation article.
Stress fibromyalgia
It would be utterly negligent to exaggerate the implications of [how many health problems stress causes]. … Everything bad in human health now is not caused by stress, nor is it in our power to cure ourselves of all our worst medical nightmares merely by reducing stress and thinking healthy thoughts full of courage and spirit and love. Would that it were so. And shame on those who would profit from selling this view.
Why Zebras Don’t Get Ulcers, by Robert M Sapolsky, p181
Many people have suggested that severe/chronic stress is an underlying cause of fibromyalgia, or even the underlying cause. In this section, I’m focusing on stress as something that happens to a person, experiences nasty enough to be considered “traumatizing” — as opposed to the idea of anxiety and depression as self-inflicted wounds from neuroticism (a personality trait), and anxiety and depression as the major specific examples.
It’s important to note that no one has actually come anywhere close to proving that stress and trauma causes fibromyalgia, but we do know that they are strongly linked and that severe stresses do often precede the disease (which fulfils one of many requirements for causality, and important one, but only one). We know that post-traumatic stress disorder and childhood adversity are strong risk factors for developing chronic widespread pain.56
It’s also worth noting that this phenomenon may be more pronounced in women, which might help to explain why women are somewhat more likely to have fibromyalgia in the first place58 — though not nearly as likely as widely believed.59
If stress does cause fibromyalgia, no one knows exactly how it works, but there’s no shortage of possibilities. Some of the ideas already discussed above may simply be a smaller part of this bigger picture. For instance, inflammation may simply be a mechanism by which stress causes trouble.
Theories about how fibromyalgia might be caused by stress range from simplistic crankery like kacked out adrenal glands and repressed emotions on the one hand (both discussed above), to much more cautious-but-expert speculation on the other. The best example of the latter that I know of comes from a 2011 paper by Pamela Lyon, Milton Cohen, and John Quintner,60 summarized in a fairly readable post on FMPerplex.com, “Evolution, Stress and Fibromyalgia.” (Heavy reading, but short and worthwhile.) They suggest that fibromyalgia strongly resembles “sickness behaviour” displayed widely in the animal kingdom, whenever a critter is struggling to adapt biologically to threats and stresses:
When a stress response is prolonged in any organism, for whatever reason, profound changes occur in functioning and behaviour. Chronic SR activation in humans is associated with some of the most medically important diseases in the developed world, including cardio-vascular disease, type 2 diabetes, and metabolic syndrome. … FMS can be seen as a clinical outcome of prolonged activation, or dysregulation of a complex, evolutionarily conserved system designed to defend the organism against threat.
The big question with stress: does it have distinct, measurable biological consequences that can lead to fibromyalgia? It’s not as straightforward as it seems. It seems like a bit of a no-brainer, an easy extrapolation from things like ulcers and heart attacks that are notoriously stress-triggered. But a 2015 study of 2000 Dutch citizens over six years “could not confirm” any biological consequences.61 Their data did affirm the link between having a rough time in life and chronic pain — people who struggle emotionally are definitely at risk of starting to hurt more — but this seems to occur independently of measurable biological changes.
If stress isn’t not biologically toxic, then why the link? The alternative is that stress puts the “psycho” in psychosomatic illness.
Hypochondria, psychosomatic illness, and the all-in-your-head problem
The two most common psychosomatic symptoms are fatigue and pain. They are difficult symptoms to assess because they cannot be objectively measured, they can only be described.
It's All in Your Head, by Suzanne O’Sullivan, 8
Hypochondria is medical anxiety, a phobia of pathology. While fear and hypervigilance may erode quality of life, the pure hypochondriac is not suffering from a medical problem — not at first. It’s definitely a mental illness.
But you’re not paranoid if they’re really after you. And we can all learn fear of disease from disease itself. Or, if you were hypochondriac before you got sick, the disease is like gasoline on that fire.
Importantly, many people with fibromyalgia have no obvious fear of pathology. They are not hypochondriacs by definition. They may be appropriately anxious about their health problems, of course, but that’s not hypochondria. Repeat after me:
- being worried about medically unexplained symptoms is not hypochondria!
- being worried about medically unexplained symptoms is not hypochondria!
- being worried about medically unexplained symptoms is not hypochondria!
But it is also possible for the mind to create or exacerbate symptoms without any obvious medical anxiety in the picture. Psychosomatic illness is a real phenomenon, in which subjective suffering — actual symptoms — become acute or prolonged in the absence of pathology or anxiety. It’s quite likely that, to some extent, pain can be a learned response, a reflexive behaviour (classical conditioning).62
We know these kinds of things can happen from extreme examples. It is possible for the mind to produce impressively severe symptoms and disabilities that definitely do not have a biological mechanism. Functional neurological disorders (FND, formerly known as “conversion” disorders) are real: people can go blind when there is nothing wrong with their eyes, have seizures without abnormal brain activity, or suffer paralysis with intact nerves.63 Neurologist Dr. Suzanne O’Sullivan describes some excellent examples in this fascinating short lecture:
If such horrors are possible, then surely it is not only possible but downright common for people to make themselves sore all over and weary to the point of disaster. But none of this confirms that fibromyalgia in general, or any specific case, is a psychogenic illness. It only means it’s possible. Only an incurious, ignorant jerk would think it’s the only possibility.
And so apparently lots of healthcare professionals are incurious, ignorant jerks. The words “all in your head” have become notorious because so many physicians are much too quick to assume that fibromyalgia is hypochondriac/psychosomatic in the absence of any other convenient explanation. The words have become a symbol for a lack of medical empathy, humility, and imagination. It’s not so much the psychosomatic diagnosis itself that bothers people with fibromyalgia, it’s the dismissal, the practical effect, the suffocation of further investigation that crushes the hope of identifying a pathology that can be treated.
Of course, few doctors actually say “all in your head” these days. Most of them know better, and often even go out of their way to say the opposite, but it’s like they are crossing their fingers behind their back when they say it. Most are still thinking, “Definitely psychosomatic.” They’re just dancing around it diplomatically.
Many fibromyalgia patients realize that it’s possible that their symptoms are psychosomatic, and many of them actively work on treating it as if it is, as best they can, in the hopes that they will get better that way. But they don’t want the conversation to end there. They hope for another diagnosis, a less murky one. They want to make sure there’s nothing more serious brewing, and that’s completely reasonable.
No one knows if all or some fibromyalgia is caused by the mind and/or disease or even more than one disease. It’s all plausible. Dismissively chalking someone’s pain up to a mind game is totally un-cool, because that person absolutely could have an undiagnosed or even unknown pathology.
But patients also must embrace the possibility of psychosomatic illness. And they must recognize that even a doctor who embraces the possibility of pathology may still be helpless to find one.
What about malingering?
Malingering is consciously faking the symptoms of a disease, usually for legal/financial advantage (e.g. proving that you deserve an insurance payout). Malingering can overlap with being a hypochondriac — some malingerers successfully convince themselves that they are sick — but it’s not the same thing. Earnest suspicion of malingering is rare, because malingering itself is extremely rare.64 Most doctors who do suspect psychsomatic symptoms sincerely do not go as far as suspecting deliberate deception.
But some do go that far, out of inexperience, ignorance, and/or prejudice — and so fibromyalgia patients not only deal with their pain, but sometimes the actual belief of doctors that it’s “fake.” Such a belief completely sabotages the clinical relationship, of course.
The inflammaging hypothesis: fibromyalgia as premature aging
In this section, I present one of my own hypotheses, a “pet theory.” It’s based on years of musings, three dozen partially relevant scientific papers, a couple hunches, something brilliant I once overheard, and a prayer to Asclepius. I will not be surprised if it turns out to be either complete trash … or exactly right. Either way, I want to be clear that I know that I am guessing here. But I hope you’ll agree that it’s interesting, worthwhile guessing.
Many people with unexplained chronic widespread pain have observed that it basically feels like premature aging. In fact, friends and family can be very annoyingly dismissive of the symptoms of fibromyalgia as merely symptoms of aging: “Oh, you’re just getting old!” The only fibromyalgia patients who don’t hear this irritating nonsense are in their 20s. It’s nearly impossible to convince people that you’re not merely “sore,” you’re too sore for your age. Especially when there’s no way for any of us to know how many aches and pains we “should” have at any given age.
What if you were actually aging prematurely? What if that’s a fair description of what’s actually going on, not just an analogy? What if some cases of fibromyalgia aren’t just “like” premature aging, but literally are premature aging? What if aging is just harsher for some people, and when it gets bad enough we call it “fibromyalgia”?
It’s clear that fibromyalgia isn’t one thing, and some cases are almost certainly not just a bad case of early aging. But it’s definitely possible that this is in fact the nature of some cases of fibromyalgia.
“Inflammaging” is a real word for a real thing, a well-described phenomenon, the inexorable development of more inflammation as we age. It’s bound to be worse in some people: too much inflammaging, too soon. The worse it is, the more it starts to look like pathology. My inflammaging hypothesis of fibromyalgia is simple:
Inflammaging may be a well-described phenomenon, but it is not well explained. We know it is closely linked to many of the health problems we associate with aging, from arthritis to heart disease and diabetes. We also know it’s linked to chronic stress. Despite Sapolsky’s concern about overstating the importance of stress as a cause of disease, “aging can be defined as the progressive loss of the ability to deal with stress” and “there is some decent evidence that an excess of stress can increase the risk of some of the diseases of aging.”65 That’s where the certainty ends, but the other possibilities are fascinating.66
However it works, it’s clear that inflammaging is a phenomenon, and a variable one — some people are bound to get it worse, and it’s very likely that those people are fibromyalgia patients who feel a lot like they are getting too sore and tired, too easily. Just like premature aging.
Fibromyalgia, alcohol, and hyperalgesia

Fibromyalgia pain motivates more drinking than others. And the drinking might also be making the pain worse.
People have an extremely complicated relationship with alcohol, and chronic pain makes it even more complicated. Fibromyalgia? Even more than other kinds of chronic pain, it turns out. There seem to be three kinds of relationships that fibromyalgia patients have with alcohol:
- Avoidance, because it makes symptoms worse or even triggers whole flare-ups. It’s even possible that
- Attraction, because it helps them cope (pain motivated drinking).
- Both! Yours truly is a classic example of this category.67
“Alcohol use can either enhance or suppress hyperalgesia,” writes Robins et al.68 It’s a messy situation that can tilt one way, the other, balance precariously, or swing erratically back and forth.
Some examples from readers, submitted by message or comment:
“It definitely helps fibro pain. Tylenol and Advil do not touch my fibro pain if it flares up. Anticonvulsants and alcohol do.” [Anticonvulsants are sedative.]
“My fibro flares feel like hangovers … so I can’t see adding booze to make them worse. It’s hell.”
“It’s not like it works for long, but it helps more than anything else I can do. Takes the edge off every time.”
“I have had fibromyalgia noticeable to me since I was about 12. I don’t drink alcohol when I tried when I was younger I didn’t tolerate it very well I made me sick and gave me anxiety really awful and a dreadful hangover. None of my three out of four offspring with fibromyalgia can tolerate it either.”
“Drinking makes the pain & discomfort much worse. It brings on that feeling of my body being squeezed as if in a suction tube. I had to quit completely.”
Does fibromyalgia drives people to drink … or does drink drive people to fibromyalgia?
That’s going to be very tough to sort out, but we do know one new thing for sure now, thanks to a new study: people with alcohol use disorder drink more to self-medicate fibromyalgia than other kinds of pain. Regardless of intensity. Or anxiety or depression.69
The new study, by Hall et al., shows that pain-motivated drinking is motivated quite a bit more strongly by weird pain — that is, chronic and unexplained pain, or “nociplastic” pain — than by other kinds of pain. Not all pain of this kind fits under the umbrella of fibromyalgia, but a lot of it does, and that’s what they focused on. Specifically, people with the combination of alcohol use disorder and fibromyalgia scored about 40% higher on a pain-motivated drinking scale than with other kinds of pain (3.4 out of 5 versus 2.4).
Note that drinking is quite a common method of self-medication, although hardly universal. Many people with fibromyalgia feel so sensitive to alcohol that they don’t drink at all, or very conservatively.
The top-scoring reasons people give for drinking for pain? With fibromyalgia: “to move better or get things done.” For everyone else: “To forget” the pain. But all reasons given were ranked a good bit higher by fibromyalgia patients, and that’s the story here.
People certainly drink to cope with all kinds of chronic pain: there’s been plenty of research about that over the years, and it seemed rather obvious before it was ever put under a microscope. But this is probably the first study to show that drinking-for-pain seems to vary with the underlying problem … and not just because some kinds of pain are more intense. Indeed, pain intensity specifically does not seem to explain it: as reported by Hall et al., it really is the type of pain that’s motivating more drinking, more than higher intensity pain of any type. For instance, you’re more likely to drink for mild fibromyalgia than savage sciatica.
There’s just something about fibromyalgia! Perhaps.
This drinking-link also sticks around even after ruling out anxiety and depression. They are common ingredients in the chronic pain stew, of course, but Hall et al. report no clear pattern of more drinking with more anxiety/depression.
“The only time I ever saw my father smile after his nerve injury was after he’d been drinking. It was totally integral to his lifestyle and functioning before the injury, and taken away after because of medical condition and drug interactions, so it was a rare return to a time without the pain and a marker of sociability.”
a reader
So what direction is the arrow of causality pointing?
This is the big question that data we have cannot actually answer (as usual). There are several possibilities:
- Fibromyalgia ➡️ Alcohol. Maybe this kind of pain makes people more desperate to anaesthetize themselves because it’s uniquely unpleasant in quality, even when it’s milder. Also — and this is a bit of a long shot, but it’s not a ridiculous hypothesis — maybe alcohol is just a uniquely good medicine for the pain of fibromyalgia (independently of its harms; all medications have harms).
- Alchohol ➡️ Fibromyalgia. Or maybe alcohol came first, and the drinking actually screws with some people’s neurology and makes the problem out of nothing, and/or directly aggravates it when used as a coping mechanism.
- Alchohol ↔️ Fibromyalgia. Regardless of which comes first, the causal relationship could be bidirectional from the get-go, or it could get that way after at least one of them is in place. For instance, even if drinking can't create fibromyalgia in an otherwise healthy person, it could still aggravate it after fibromyalgia starts for some other reason … and then escalate as it becomes a coping mechanism, a vicious cycle. Certainly that’s a familiar kind of pattern with drugs of all kinds!
- Something else ➡️ Alchohol & Fibromyalgia. Maybe both weird pain and alcohol use disorder are symptoms of deeper physiological problems — things that make us more vulnerable to both alcoholism and pain. There are quite a few possibilities, and it doesn't seem unlikely. For instance, as one example, it possible that strong neuroticism (anxiety, depression) could explain both alcohol use disorder and fibromyalgia.70 Physiology is more than complex enough for such tangled and subtle relationships.
So, should you drink?
Alcohol isn’t good for anyone, and it may well be even worse for fibromyalgia, so avoid it if you can.
If you cannot avoid it — because it feels like too important a “medication” — have compassion for yourself and try to minimize your usage, especially sharp increases in dosing. Just keep in mind that might be causing or sustaining the very problem you’re try to solve. That is, it might be especially bad for people with fibromyalgia.
And even if it isn’t, it’s really still not good for you. The science on this topic is now clear: alcohol is a poison, and there is no such thing as a healthy regular amount. It differs only from smoking in degree. Although the risk scales with the dosage, the one “healthy glass of wine” is a fantasy. Small doses aren’t very harmful, but they are still harmful. Alcohol made headlines in the early 2020s for being confirmed as a carcinogen even in modest quantities.71
Fibromyalgia seems to involve at least some “alcohol intolerance,” but it’s unclear if it’s actually something about alcohol that specifically triggers fibromyalgia flare-ups (“alcohol hyperalgesia”)… or just that alcohol consumption is physiologically stressful and people with fibromyalgia are just more vulnerable to any physiological stress. Ultimately it doesn’t matter: it’s probably best to minimize as much as you can, without losing your mind if it’s a valued coping mechanism.
Part 3
Fibromyalgia Treatment
Trying to solve one of the hardest problems in medicine
Fibromyalgia treatment is the hardest problems in all of medicine. We’ll probably figure out how to handle Alzheimer’s and rheumatoid arthritis before fibromyalgia. So, please, do go easy on yourself if you’re unsure how to manage unexplained chronic widespread pain. It’s okay! No one actually knows! Truly.
Clinicians should be aware that current evidence for most of the available therapies for the management of fibromyalgia is limited to small trials of low methodological quality.
Naturally, there are people who claim to know, but truly they do not. There are some good ideas, and some of those ideas pan out for some patients, some of the time. But this is a beast with many and diverse heads, and we should definitely not trust anyone who claims to have mastered it.
•
In 2020, Mascarenhas et al. reviewed over 220 studies with almost 30,000 subjects, identifying some “high-quality evidence” that cognitive behavioural therapy… just barely works (good evidence of a minor effect). To an even more modest extent, two classes of drugs — antidepressants and central nervous system depressants — were confirmed to have minor benefits.72
None of those seemingly good-news results actually rose to the level of clinical significance! How far is confirmation of a benefit that is barely noticeable (at best) from just confirming that it doesn’t really work?
And that was the good data.
The rest was the “garbage in” part of the “garbage in, garbage out” equation: data too poor to extract meaningful results from. When most of the data in many dozens of trials is largely worthless, that’s more of a repudiation of fibromyalgia science itself than fibromyalgia treatments. Lots and lots of data that mostly just tells us that most of the studies themselves are worthless. The researchers concluded:
Clinicians should be aware that current evidence for most of the available therapies for the management of fibromyalgia is limited to small trials of low methodological quality.
•
Let’s try another perspective: looking for agreement between formal treatment guidelines. In 2017, Thieme et al. studied four sets of guidelines and found that they were … all over the map.73 While “there were a number of similarities” in their recommendations, there were also maaaaany inconsistencies. The only treatments with strong agreement were:
- exercise
- cognitive behavioural therapy
- the old-school anti-depressant drug amitriptyline
And just because they agreed on these does not necessarily mean that they actually work, or work for everyone. It just means that all four organizations concluded that they might be, perhaps, slightly better than nothing, for at least some people.
Only one treatment was given a 👎 by all four guidelines: opioids. No surprise there.74
And they were collectively equivocal or blatantly contradictory on dozens of other treatment options. For instance, one group strongly recommends against massage therapy, another recommends it (moderately), a third is weakly against it, and the fourth had no comment. So I guess that one’s still a little uncertain! (See my massage guide for a detailed discussion of massage therapy for fibromyalgia for members only.)
Happily, there was only a single example of a treatment that had strong recommendations both for and against (the drug milnacipran). Although there were many contradictions, they were mostly not “strong” ones, so at least there’s that!
Just one guideline seemed to go out of its way to make recommendations against a long list of particularly silly treatment options, a hall of treatment shame, things like relaxation, dance therapy, magnets, lasers and TENS, cryotherapy, local anaesthetic, and several more.
•
For the rest of the article, I will discuss some highlights from treatment options in as practical a way as possible. This article does not yet provide a comprehensive tour of the options — I chip away at updates over months and years — but it does cover most of the more practical and interesting possibilities.
Fibromyalgia and your rheumatologist or neurologist
Fibromyalgia often resembles the early stages of rheumatological diseases like lupus or ankylosing spondylitis. Indeed, fibromyalgia may co-exist with them. And so fibromyalgia patients often end up being referred to rheumatologists … and then many patients and rheumatologists end up frustrated and baffled by each other.
Rheumatology is the medical specialty devoted to arthritis, particularly the inflammatory arthritides (autoimmune diseases). Rheumatologists are appropriately preoccupied with those very serious and complicated problems. Many of them sub-specialize in just one! In the big picture, it isn’t fair or reasonable to expect rheumatologists to “get” fibromyalgia. The only rheumatologists who do are the ones who have taken an interest and gone out of their way to study it. But they are the exception. In Canada, rheumatologists have been told by their professional organization that fibromyalgia is out of their scope of practice — they aren’t technically allowed to help fibromyalgia patients!
Of course, there’s no excuse for a rheumatologist being an insensitive jerk about it, either — and a lot of fibromyalgia patients have witnessed that.
Neurology is the other medical specialty that attracts fibromyalgia cases, which is probably a less bad fit — although neurologists are also appropriately preoccupied with many serious conditions that are much better understood. Many of them sub-specialize in a disease (multiple sclerosis), or a class of neurological problems like movement disorders, and really don’t know the first thing about fibromyalgia, any more than pro football coach would know what to do with a volleyball team. But a few neurologists generalize a bit and take a professional interest in problems like fibromyalgia.
Other relevant medical specialties
In all cases, there’s the potential for good help if the individual professional is keen on the topic of fibromyalgia. But there simply is no speciality that clearly lends itself to that. There just are no “fibromyalgia doctors.” Here are the closest remaining possibilities, after rheumatology and neurology:
Orthopaedists are the “carpenters” of medicine, generally focusing on surgical repairs of (allegedly) biomechanical problems, and sports medicine. They are a rarely a good choice for fibromyalgia patients.
Physical medicine & rehabilitation (AKA physiatry) is one of the newest medical specialties, and PM&R docs are basically like advanced physical therapists. The right one can be quite helpful for fibromyalgia patients.
Pain specialists are usually board certified anesthesiologists, neurologists, physiatrists, psychiatrists, or oncologists with additional training in pain management. They often work in multidisciplinary pain clinics/programs. This can be a good route for fibromyalgia patients, but — yet again — fibromyalgia may be a second class citizen, overshadowed by more dramatic and better understood cases.
Psychiatrists and psychologists are potentially useful not because fibromyalgia is “all in your head,” but to help rule out (or treat) symptoms caused by anxiety and depression. The trick is to find one who agrees to those terms. Popular psychotherapeutic modalities used to treat pain, especially cognitive behavioural therapy, have never demonstrated significant efficacy for chronic pain in controlled tests (see Cognitive Behavioural Therapy for Chronic Pain for a full discussion about that). Despite that, CBT is “technically” the leading evidence-based fibromyalgia treatment, because there is more good quality evidence that it works than there is for any other treatment. But there’s a catch! If you read the fine print, we’re talking about evidence of a benefit so minor that it “might not be clinically important to patients.”75
Massage therapists have little hope of altering the progression of fibromyalgia, but they can offer something almost no other professional can: at least some temporary but meaningful symptom relief, and soothing of the nervous system. "Soothing" may be more valuable than it sounds, more than just relaxation, insofar as a very pleasant sensory experience may actually reduce sensitization to some degree — maybe.
Unfortunately, for several reasons, massage therapists are particularly prone to overconfidence in their ability to actually “cure” fibromyalgia — which is all-to-easy for everyone to believe, thanks to the legitimate benefits mentioned above. They are also often too aggressive, underestimating the fragility and sensitivity that defines the experience of fibromyalgia. While many fibromyalgia patients have been helped by massage, far too many others have been abused by careless or overconfident massage, and I think sometimes even seriously harmed.
This is just a summary. See my massage guide for a detailed discussion of massage therapy for fibromyalgia for members only — there's about ten times the wordage there.
•
For more detailed reviews of the various health care professions that deal with pain patients, see Reviews of Pain Professions. (More detailed, but also less focused on fibromyalgia.)
Exercise for fibromyalgia
All physiotherapists have experienced the anxious expression, the dejected look, the frustrated frown of the individual living with persistent musculoskeletal pain who is asked to partake in exercise.
Reasoning exercise dosage for people with persistent pain, by Paul Lagerman, 30–35
Regular moderate exercise you enjoy is good medicine for fibromyalgia.76777879
Maybe.80
Although exercise is famously “the closest thing there is to a miracle cure” for many medical problems,8182 it’s much less of a slam dunk for chronic pain in general,83 and clearly it can backfire and actually cause pain,84 especially in fibromyalgia patients. Indeed, feeling like you can’t exercise — because it’s painful, because it wipes you out — is one of the signature features of fibromyalgia!
Any advice given for myalgic encephalomyelitis — also known (incorrectly) as chronic fatigue syndrome — is often given for fibromyalgia as well.85 And so these waters have been muddied by the infamous “PACE” trial, a big British experiment which concluded that graded exercise therapy — taking baby steps back to normal exercise levels — was helpful for myalgic encephalomyelitis patients. Their results also implied that ME patients aren’t actually sick and just need to think positively and get moving. But the PACE trial has been tainted by scandal and harshly criticized as “uninterpretable.”868788 Unfortunately, there are good reasons to believe that PACE got it disastrously wrong, and exercise actually hurts ME patients89. Fortunately, most official guidelines now finally get it right.
None of this would have anything to do with fibromyalgia if it weren’t for the constant clumsy conflation of the two conditions. Here’s the one useful nugget we can take from PACE-gate: if you supposedly have fibromyalgia, but you have a particularly hard time recovering from exercise, it might be worth trying to rule out ME.
Or it’s possible that exercise just really does aggravate some (CSF-y?) cases of fibromyalgia!
And yet fibromyalgia is among the most likely of chronic pain conditions to benefit from exercise if you do it right. But what’s right? No one knows for sure, of course, but here are some evidence-inspired tips:90
- Moderation, of course. Either stick to the Goldlilocks zone, or only leave it for relatively short bursts. Dosage is everything. The conventional wisdom is regular moderate exercise, never too much or too little, but I think that’s a bit too simplistic. You may want to exercise intensely because it’s fun, for instance, but that must be balanced with more frequent and generous recovery opportunities than you needed back in the pre-fibromyalgia days.
- Measure ooginess, not pain. Don’t judge how much is too much based only on pain. Rate your readiness much more generally instead: use “subjective units of distress,” or the “ooginess” scale (rather than a pain scale). Basically the idea here is that the real problem is much more complicated than pain, and so pain alone is an unreliable signal. On many days, pain and ooginess will go together. But not always, and by reckoning it this way you might choose to push a bit even when you are in pain but otherwise feel pretty decent … or you might ease up and skip a day even if the pain is low but the ooginess factor is fairly high.91 Avoiding fixation on the pain, pain, pain has other benefits too.
- Timing is everything. As every fibromyalgia patient knows, there are good days and bad days. It’s important to minimize exercise on the bad days, and equally important to seize the opportunity to get back to it on the good days.9293 Again, judge the goodness and badness of days in a general way, not just the pain.
- Aerobic or lifting weights? It doesn’t really matter — they both seem to work.9495 Do what pleases you …
- Make it fun, make it happy. That may sound trite, but exercise may work for fibromyalgia not because of its familiar biological effects, but as a desensitization tool, a brain-changer,96 a way to demonstrate to nervous systems that the world is a “safe and good place.”97 This effect would also go a long way to explaining why one form of exercise seems to work well for one patient, and not at all for another: because its success depends at least partly on how we feel about a workout. For instance, there’s evidence that taiji is helpful98… but I bet it depends on how you feel about taiji!99
Treating spinal cord pinching
If positional cervical cord compression (PC3) is actually a cause of fibromyalgia, it begs the question:100 what on Earth do you do about something like that? Not much. You try to “work around it” — avoid the positions that cause trouble. Which isn’t great.
Note that no one really has any idea how to treat myelopathy without surgery. “You know nothing, Science.” A 2013 review of dozens of papers found exactly no reliable evidence of anything, a big fat nothing burger.101
Or you operate. Which is always a last resort, but especially this delicate surgery.
Keep a stiff neck
Dr. Holman (the researcher most associated with this topic) provides a DVD that is basically a tutorial for physical therapists to help patients stand up straight — just classic “good posture”! He believes that a majority of patients would recover with this “PT protocol.” That seems a bit trite to me, weirdly simplistic and a bit disappointing. (And why do you need a video tutorial for it? Seems like overkill!) On the other hand, we are talking about “positional” spinal cord compression here, so maybe avoiding the position that compresses your spinal cord is just sensible, probably better than nothing, maybe a lot better than nothing … and that does basically boil down to trying to maintain a more erect posture. Permanently being shy of neck flexion and/or extension sounds terrible, but it’s certainly the lesser of evils, if those positions actually are irritating your spinal cord and that is, in turn, ruining your life. And you wouldn’t be alone: there are other conditions that definitely require diligent avoidance of certain neck positions.102
At the same time, I can’t really take this advice seriously as a “treatment protocol” either: it’s just avoiding aggravation. Or maybe I should say it’s “just” avoiding aggravation — basic but not trivial?
Trying to make room for your spinal cord surgically
Trying to fix spinal cord compression, constant or intermittent, is a risky long shot. But the stakes are high, and people try, and sometimes it works out. Depending on the specific mechanical cause of compression, it might be a better gamble. So, how do you decide when it’s time to talk to a surgeon about it? How do you know if you should ever take that gamble? I think three conditions would have to be met:
- The clinical picture is desperate: years of disabling symptoms! Nothing less dire is worth the risk of this kind of surgery.
- A high level of diagnostic confidence, based mainly on the elimination of other diagnoses and a clear self-knowledge that neck position is relevant to your symptoms. Other signs of spinal cord compression (myelopathy) would obviously also clinch the diagnosis.103 And there’s one other diagnostic factor that stands out …
- Imaging evidence of obvious stenosis/PC3. Not mild! Lots of people have mild stenosis as they age — that alone would definitely not be enough.
Having high diagnostic confidence is the tricky one, and not many people are going to be able to tick all three of those boxes. But we can easily imagine a patient who is desperate, has done a thorough job eliminating other diagnoses and confirming this one (e.g. successful provocation tests, a history of feeling better when flexion is avoided, etc), and has imaging evidence of substantial stenosis. It does make sense for that patient to at least consult a surgeon about this.
A grab bag of “reasonable” treatment ideas for fibromyalgia
None of these deserves a whole section, but they are all worth mentioning. Once again I’ll emphasize that there isn’t exactly any known way of treating fibromyalgia, so the lack of detail reflects that ignorance: there’s only so much that should be said about treating fibromyalgia, because there’s only so much that can be justified. This minimalism is a feature, not a bug.
Treat sleep like it’s precious. Learn everything you can about insomnia and sleep problems, learn and practice the best possible sleep hygiene, and protect your sleeping conditions like it’s life or death. It won’t be easy, and it won’t always work. But the only thing worse than the sleep problems associated with fibromyalgia is those same sleep problems aggravated by potentially fixable problems like light and noise pollution, uncomfortable beds, and behavioural factors like logging on to Facebook one last time before bedtime. Be aware that creatine is often recommended for fibromyalgia/CFS because it legitimately reduces muscle fatigue and possibly even mental fog,104 but creatine can also actually make sleep worse in some people. See The Insomnia Guide for Chronic Pain Patients for more on all these points.
Treat the treatable. Fibromyalgia patients have other medical problems, like tendinitis,105 but suffer from them more and longer. Focus on taming whatever issues you have as best you can. It’s an uphill battle, but it’s all the more important. The fewer sources of pain, the better. PainScience.com has many self-help guides for common pain problems and injuries, and a guide to unusual sources of pain.
Change everything. Change your life. If fibromyalgia is a complex disease caused by many factors, if it’s a “meltdown” of our ability to adapt to stress, then assertively seek out a better life. See Pain Relief from Personal Growth. Less drastically, but in the spirit, launch a campaign to eliminate every possible stress from your life — not easy, of course, but worthwhile regardless. Meditation, yoga, and related practices may be appealing and appropriate for some people.
Experiment with “anti”-inflammatory dieting. Although there is clear evidence that fibromyalgia is inflammatory,106 there is none that any kind of diet is likely to help. And yet the only true anti-inflammatory diet is probably just one that is not inflammatory — that is, a “heart healthy” diet. Low stakes, worth a shot, with a worst-case scenario that you’re eating healthier in general. For much more detailed analysis, see Chronic, Subtle, Systemic Inflammation.
Fast, deep breathing exercises (hyperventilation). This is one of the few promising easy and relatively safe methods of reducing systemic inflammation. Cold exposure may enhance the effect (not everyone’s cup of tea). While far from proven, some of the evidence is genuinely persuasive and fascinating.107 This effect may be particularly relevant to some fibromyalgia patients,108 and it may be accessible with a relatively easy and safe protocol.109 For more information, see the blog post “Anti-inflammatory hyperventilation: I’ll huff and I’ll puff and I’ll blow my pain away.”
“Ignore” it. I’m not being cute here, I swear. The suggestion is absolutely earnest. Pain is like noise pollution: the more you pay attention to it, the worse it gets. It thrives on attention and “drama.” Try to act normal and get on with your life as best you can. Embrace stoicism. For much more about this and other “mind over pain” strategies, see Mind Over Pain. We’re talking about mitigation and coping here, not cure, but that can be important.
Try marijuana. The efficacy of marijuana for various chronic pain in general is still unsettled science and over-hyped. The reality so far is a mixture of mediocre and bad science news, and the evidence for fibromyalgia specifically is even worse.110111 As with any drug, some people will undoubtedly be non-responders, and some will have adverse reactions. But it is certainly worth experimenting with, conservatively… if your local laws don’t make it too much of a hassle. I have a full guide to this topic: Marijuana for Pain: The hype versus the science! What does the evidence actually show about cannabis and chronic pain?
Take vitamin D. Vitamin D deficiency is extremely common (especially in northern latitudes), strongly correlated with chronic pain in general and fibromyalgia in particular, and quite safe to supplement. See Vitamin D for Pain.
Stretching for fibromyalgia is quite a reach
There is no specific reason to think stretching is helpful for fibromyalgia patients, but — like most of of self-serve wellness practices, the easy things widely believed to be good for us — it’s one of those things fibromyalgia patients routinely have on their “try everything” list.
For most healthy people, stretching does feel good — so good that it’s hard to believe it doesn’t have some kind of medical benefit. But the scientific evidence is strong that stretching and flexibility are not important pillars of fitness and health — or at least, no more so than any other light activity and stimulation.112 It mostly functions as really light exercise.
And for many people with chronic widespread pain, however, it does not even feel good. The legendary deliciousness of stretch is just not there. When I originally blogged about this, most of the feedback came from folks with fibromyalgia and hypermobility/EDS:
“It just hurts too much. Usually too sore!”
“I hit the end range of my joint miles long before I feel any stretch.”
And so a lot of stretching experiments for fibromyalgia patients end quickly.
For fibromyalgia patients that do like the feeling of stretch, of course there’s never anything wrong with adding some good feelings to your life. But … is it a “treatment”?
Tested: stretching for fibromyalgia
There’s barely any science specifically about stretch for fibromyalgia, and what we have is not inspiring stuff: like Støve et al., published in mid-2026, about a little experiment claiming that a mere six minutes of daily home stretching for six weeks reduced fibromyalgia symptoms by a bit over 18%.113 Not exactly “huge” if true, but good enough, and cheap, and no major flaws leap out of the abstract, so … should I put that in my skeptical pipe and smoke it?
Based on the abstract alone, Støve et al. sure looks like solid good news, but abstracts are like movie trailers: they only show you the good bits.

Støve et al.’s abstract is a perfect example of making the experiment sound much better than the full paper does. (Image source unknown to me.)
The honest conclusion — like an “honest trailer” for a bad movie [YouTube again] — is that a six-minute daily routine with weekly researcher contact improved self-reported fibromyalgia symptoms over six weeks compared to — wait for it — being on a waitlist. 🤦🏻♂️ The abstract only describes “usual care” for the control group, but what is that for a notoriously untreatable disease? Well, nothing of course!
And that is in fact what they got, as revealed in the full text.
And it’s a critical flaw, a cliché of amateur science: a failure to adequately “control” major confounders, also known as the whole point of doing a clinical trial. The paper title claims it is “controlled,” but it’s just not: the “usual care” waitlist design is a what-were-they-thinking choice.114 See that footnote for a full explanation of why this is a deal-breaker.
This paper’s conclusions are implausibly inflated in favour of stretching. If anything, the absence of a better result is damning.115
Clearly stretching is not much of a treatment for fibromyalgia. But by all means do it if it feels nice to you, or just use it like a light form of better-than-nothing exercise. And ideally do it with a dog or cat, so you can at least get some validation and compassion…

Dogs are a superb source of the validation and compassion that were probably the active ingredients in the Støve et al. experiment. A good dog will provide these while you stretch (sometimes while napping).
Hang out in a pressure chamber? Hyperbaric oxygen therapy for fibromyalgia
Hyperbaric oxygen therapy (HBOT) involves sitting in a pressurized chamber with an oxygen-rich atmosphere. The idea is that it squeeeezes extra O₂ into your body! It’s an experimental, expensive treatment with some promising preliminary evidence for some conditions, like autism and migraine. The risks are unknown, but probably minimal.
Predictably, there’s not much evidence on this topic, and what we have is of questionable value (see above, “An avalanche of useless fibromyalgia research”). As of 2017, there are a couple dozen slightly encouraging animal and human trials of HBOT for “chronic pain” in general,116 and just one more intriguing scientific study of HBOT for fibromyalgia in particular,117 with a conclusion that sounds fabulous:
CONCLUSIONS: The study provides evidence that HBOT can improve the symptoms and life quality of FMS patients. Moreover, it shows that HBOT can induce neuroplasticity and significantly rectify abnormal brain activity in pain related areas of FMS patients.
Unfortunately, we have no strong reason think that HBOT is going to be an effective treatment for fibromyalgia specifically, and “a promising treatment is the larval stage of a disappointing one.”118 It’s not a crazy idea, but it’s still a substantial speculative leap from “HBOT facilitates neuroplasticity maybe possibly” all the way to “and therefore fibromyalgia cure!” The whole thing smacks of wishful thinking and perhaps even self-promotion (which is a bit of a plague on HBOT research). Although bias is normal, and nothing actually gets studied if people aren’t keen on it, this is a complex study with a high-risk of bias. These researchers are obviously heavily invested in the idea of HBOT, and the more complicated the study, the more ways there are to unconsciously distort the experiment and its results.
The inclusion of SPECT assessment is fascinating, but it also adds some exotic complexity to what is already a complex trial. Although well-written with good, thorough disclosure of some of the obvious limitations (like the problematic absence of a true placebo control), there’s still too much wiggle room here, and the results are essentially meaningless without good replication… and a solution to the placebo problem. Although the authors think the results were “not likely to be a placebo” and cite a couple reasons why — like the fact that patients actually worsened initially — by no means is that doubt fully resolved.
But there is a bright side: the final results did seem to be quite robust, and they shouldn’t be carelessly dismissed. I just can’t take it too seriously without replication. But watch this space. I wouldn’t have bothered including an HBOT section if I didn’t think there was some potential.
Ozone therapy — a classic example of fibromyalgia snake oil
Ozone is a pale blue toxic gas, widely used as a disinfectant, among many other industrial applications.
And so of course it has been used as a fibromyalgia treatment — because everything with the slightest medicinal reputation has been. And it sounds just science-y enough that it seems believable to many desperate fibromyalgia patients.
The legitimate antibiotic powers of ozone are the seed of truth that has powered its medical reputation for well over a century. Ozone therapy has been a perennially popular snake oil, hurting and killing many people rather than curing anyone of anything, making it one of the best examples of popular but dangerous quackery. It has a colourful history… literally.

For decades consumers could buy ozone generators for self-treatment, like this bizarre vintage medical device of unknown provenance. It still “works”: it produces a strong ozone odour, and the paddle causes the sensation of little sparks when applied to the skin. Photos by neon collector Jenny Beatty, used with permission. See several more high-res photos.
There is no compelling clinical evidence for ozone therapy, and it remains out in medical left field … where it largely belongs, and where it will probably remain indefinitely. It is banned by the FDA for safety reasons at least, and is strongly associated with rank quackery. Even if it could be used legitimately, and even if a few good providers exist, patients can’t find them.
The “science” of ozone therapy for fibromyalgia, such as it is
There aren’t any actual clinical trials for this usage of ozone therapy, not even one. There is a common citation, widely used by naturopathic clinic websites: Tirelli et al. describe their clinical impressions of treating sixty-five cases of fibromyalgia with ozone therapy, claiming “a significative [sic] improvement (>50% of symptoms) in 45 patients.”119 They declare it to be an “effective” therapy in their title, as if they have proven something. But this was not any kind of clinical trial — a controlled test of a medical intervention. This paper is just a low quality collection of anecdotal reports, put together by a group of clinicians who are obviously diehard fans of ozone therapy.
The only other example I’m aware of was an “open label pilot study”120 — more of the same, utterly worthless. This stuff barely even qualifies as junk science — it’s on a lower level than that.
Part 4
Useless but fascinating: the greatest hits of fibromyalgia research
Early on in this guide I mentioned that there’s a lot of crappy fibromyalgia research, but of course it’s not all bad. It’s quite common for researcher’s to learn fascinating new things about fibromyalgia. Unfortunately, even when it’s good and interesting, it’s often almost completely useless to patients or clinicians on the front line.
In this part of the guide, I will highlight research that’s genuinely interesting… but isn’t going actually inform management. I’m launching with a particularly great example: the “transplantation” of fibromyalgia symptoms from humans to mice. Amazing! Almost completely pointless in the short term for anyone but researchers. But amazing.
And now, almost unbelievably, I’ve added another section about another method of transplanting fibromyalgia from humans to mice … with poop. The poop of pain! Fibromyalgia follows fecal matter. And this could be more clinically significant — treating fibromyalgia with healthy fecal transplants — but also isn't 'ready for prime time" yet — see details below.
Miserable mice! Fibromyalgia transplanted to mice…in blood?

Fibromyalgia symptoms have now been diabolically “transplanted” from humans to mice, in a new study by Goebel et al.121
The effect was temporary, thankfully, but for a couple weeks after mice are injected with serum from people with fibromyalgia, they seem to be struck down by fibromyalgia themselves. They get sluggish and weak. They flinch away more dramatically from cold and pressure. Nerves in their skin actually shrivel up (I am not kidding). These signs are all familiar to us from human fibromyalgia.
How is fibromyalgia making the leap to the mice? Goebel et al. had something in mind, because there are many clues that fibromyalgia involves the immune system in some way. The bearer of the bad news appears to be one of our most common antibodies, the immunoglobulin G (IgG), an immune system workhorse. The mice were safe when IgG was filtered out of the serum or when the serum came from healthy humans. Only serum with “bad IgG” from fibromyalgia patients was a threat to the mice.
The mice bounced back as levels of human IgG levels in their little systems slowly declined over a few weeks. Phew! I accept that mice are essential in medical research. Doesn’t mean I have to like it.
What is immunoglobulin G?
Immunoglobulins (Ig) are antibodies, molecules that identify and neutralize invaders, and G is one major class of them, a family of proteins with many properties that distinguish it from other major types. For instance, it’s the only type of antibody that crosses the placental barrier, so it has a crucial role in infant immunity. It’s also strongly associated with allergic responses, including anaphylactic shock.
One key thing to note is that we can’t just get rid of IgG. It’s too important.
And what’s wrong with it in fibromyalgia?
As with all things immune, IgG is just stupidly complex, and it’s more of a family of proteins than “a molecule.” There are many ways that IgG — as a class of antibodies — can be different in fibromyalgia patients.
Just knowing that fibromyalgia patients have “bad IgG” isn’t super helpful, because we don’t know why or how it’s bad — and you can’t just get rid of it. Goebel et al. suggests that therapies that reduce our total IgG supply somewhat “may be effective,” but we have no idea. Blocking their effects is another promising approach, but complicated. All of this will take a lot of work. Still, at least it’s a promising place to look.
(And there are probably several sub-types of fibromyalgia, and they probably don’t all involve tainted rogue IgG.)
Flaws and limitations?
I am not qualified to find specific fault in this quite technical study, but I didn’t pick up on any red flags. Of course it’s “just an animal study,” and we know that “mice lie and monkeys exaggerate,” the biologist’s lament about the unreliability of animal models. Different species can be weirdly impervious to things that are nasty for others.
But this is a bit different from the usual “we learned something about how animals work, but we have no idea if humans are the same.” When a well-described disease in humans can be inflicted on mice with an extremely specific procedure, there’s a good chance it’s an important finding — even if we’re not sure what to do with it yet.
Poop of pain: fibromyalgia follows fecal matter
The last section was about inducing fibromyalgia with blood transplants… and this one is about doing the same with fecal transplants, as shown in a 2025 study.122
Fibromyalgia can be moved from humans to mice in at least two ways! Apparently fibromyalgia is “in” both the blood and poop. Blood matters, and fecal matters too. 🩸💩 Yeah, the poop puns practically write themselves. This section will be thick with them — don’t pooh-pooh it!
(When I first started reading the 2025 study, I got deep into déjà vu before I started to suspect I was just remembering an uncannily similar study from 2021, rather than an “illusion of memory.” Which makes me wonder how often déjà vu seems weirder than it is.)
Recapping the last section for context (not everyone reads my big articles from top to bottom): in 2021, Goebel et al. reported that one of our most common antibodies, the immunoglobulin G (IgG), an immune system workhorse, was the “active ingredient,” but it’s not just one molecule: IgG is a whole family of proteins. But whatever witch’s brew of variables goes wrong with IgG in human fibromyalgia patients, when healthy mice that get a dose of it … they start hurting.
And now this poop thing too? Just how transplantable is fibromyalgia?!
The bacteria that live in the gut excrete all kinds of molecules, like a drug dispensary, which is why they matter. This is a successful long-term relationship, an ancient symbiosis between animals and our tiniest passengers. But it’s not perfect: microbiome dysfunction is already implicated in many pathologies, and we know specifically that fibromyalgia patients have funky gut bacteria.
Cai et al. have the new poop scoop, reporting that a fecal transplant can have much the same effect as the blood transplant did: healthy mice get all sensitive when they get a dose of the gut fauna of a human with the symptoms of fibromyalgia. The transplants also induced immune activation, metabolomic changes, and (this is odd) reduced skin innervation. Holy crap!
They also went an extra step and did a small pilot study to see how 14 women felt when they got fresh, healthy fecal donations. Yes, they felt better — but take that with a kilogram brick of salt, because it was an uncontrolled study, which is basically how you use science to get the results you want to see. It’s a bit of a shitshow. A pilot study like this is genuinely useful for inspiring better research, but it absolutely does not have clinical importance at this time … not that I would blame a desperate fibromyalgia patient for taking the idea of a poop transplant seriously based on this information, but it absolutely cannot be “officially endorsed” at this time. We’re just not there yet.
But the mouse experiment was firm enough. They transplanted both healthy and unhealthy poop into germ-free female mice, raised in sterile conditions. The “poop of pain” caused a whole smorgasbord of pain symptoms: heightened sensitivity to pressure, heat, and cold, along with signs of muscle and spontaneous pain. Importantly, none of that awfulness happened with by transplants from healthy donors.
There are a lot of ways that an altered microbiome could cause systemic health trouble. Cai et al. went looking for some, and noted an uptick in inflammatory markers and overactive microglia (brain immune cells, so “neuroinflammation”), plus altered levels of some neurotransmitters and bile acids (major ingredients in digestive juices).
This is all very intriguing, but of course that human pilot study is worthless for anything except inspiring a better one, and popping poop pills for pain is not a fully baked idea. The mouse experiment was easier to trust, but needs the same caveat I gave for the blood-transplant study: “mice lie,” but … “when a well-described disease in humans can be inflicted on mice with an extremely specific procedure, there’s a good chance it’s an important finding.”
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Part 5
Appendices
Related Reading
I think this is the most credible and useful of the many fibromyalgia books available is Fibromyalgia: The Final Chapter. This article is just a primer: go read Dr. Goldenberg’s book next.
Unfortunately, I personally suffer from unexplained fatigue and chronic widespread pain myself — the direct inspiration for this article more than any other on PainScience.com. Although I was devoted to writing about chronic pain long before it became a serious problem for me, my ironic fate has definitely been a major influence on this website. You can read my chronic pain story: see It’s like Long COVID: Living with a Long-COVID-ish illness since way before COVID.
Another personal story: “DOCTOR MASSEUSE: Or My Personal Pain Puzzle,” by Jared Updike, is a practical and hopeful article by a PainScience.com reader about wrestling with fibromyalgia over the last few years, more or less successfully. But it wasn’t easy:
What do you do when all your effort backfires and makes things worse, where you feel like your body is allergic to effort? (And you tried "resting" or doing nothing for months but that clearly did not work either?) Especially if you are the type of person that thrives on effort (professional life and hobbies and ways to blow off steam?)
For several years, the pain, fatigue, isolation, anxiety and low mood cycles were hell. The harder I tried, the worse it made everything: I was used to trying harder making things better, but this was its own beast. During this time, I had trouble walking without my muscles (eventually my whole system) complaining for days. I had trouble driving. I felt trapped in my apartment.
Jared perfectly demonstrates a thoughtful, systematic approach to learning about fibromyalgia and experimenting with treatments. He’s open-minded, but — crucially — not too open-minded. His writing about that process is a great bonus, clear and interesting. The main article is short, but some of his “Additional Notes” are actually longer and the best part: be sure to click/tap to show those.
While I do not think that chronic widespread pain is generally a psychosomatic illness, I do think patients should be very familiar with the reality of psyschosomatic illness and how it might relate to their case. Some recommended reading on that theme:
- It's All in Your Head: True Stories of Imaginary Illness (book), by Suzanne O’Sullivan. Amazon.com ❐
This book consists mainly of well-told stories of severe psychosomatic illness and functional neurological disorders (neurological symptoms without diagnosable disease). The key take-away is that psychologically powered illness is common and can be amazingly severe. Although Dr. O’Sullivan is clearly concerned about the risk of incorrect diagnosis, and she is cautious and compassionate enough that I think she mostly gets it right (with the notable exception of the chronic fatigue chapter). It’s well-written and fascinating and has plenty to offer. I do wish there were citations.
- Why Zebras Don’t Get Ulcers (book), by Robert M Sapolsky. A fascinating, charming tour of stress science. Although it is detailed to a fault at times, Sapolsky’s attempt to make the topic palatable is downright heroic and relentless insightful and quotable. He is biology’s Richard Feynman. The book’s main lesson is that stress is definitely a serious health issue. Humans have a unique capacity to react to imagined threats — psychological stress — but we differ dramatically in our vulnerability to them. To some extent that vulnerability can probably be managed, but “it’s complicated.” To the extent that we can reduce stress, “80 percent of the stress reduction is accomplished with the first 20 percent of effort.” If the book has a significant flaw, it’s that Sapolsky only acknowledges that stress has been demonized for profit: “it would be utterly negligent to exaggerate the implications of this idea.” Unfortunately, he does not explore or condemn the tsunami of quackery, marketed with hyperbolic fear-mongering about stress (which, to be fair, was still relatively tame when he was writing). For contrast, Purser's much more recent book, McMindfulness, devotes a whole chapter to this topic. Curiously, this book is cited or quoted more than any other single source on PainScience.com: Sapolsky is referenced almost 200 times in about three dozen articles!
- When the Body Says No: The Cost of Hidden Stress (book), by Gabor Maté. Amazon.com ❐ With clarity and passion, Vancouver physician Gabor Maté tells the stories of people whose pain and illnesses emerged from lives filled with stress, anxiety and depression, illuminating the next frontier in medicine: the elusive mind-body connection.
What’s new in this article?
47 updates have been logged for this article since publication (2017). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
Jun 26, 2026 — New section: No notes. Just a new chapter. [Updated section: Stretching for fibromyalgia is quite a reach.]
May — Key point added: Added information about the “character” of fibromyalgia pain, what makes it so discombobulating and bothersome. [Updated section: Introduction.]
2025 — Editing: Just a few minor improvements. [Updated section: “Fibromyalgia” is a medical UFO: the diagnosis is descriptive, not explanatory.]
2025 — New section: No notes. Just a new chapter. [Updated section: Poop of pain: fibromyalgia follows fecal matter.]
2025 — Science update: Added an important point about the bogus idea that fibromyalgia is almost exclusively a female disease, which is probably the single best example of the myth of feminine fragility. Fibromyalgia prevalence is only slightly skewed towards women, probably less than 60% (see Wolfe). [Updated section: Introduction.]
2025 — Editing: Small but important modernization and clarification edits. [Updated section: What about “central sensitization”?]
2024 — Minor improvements: Added some reader comments, a footnote about neuroticism and alcohol, and did a little editing. [Updated section: Fibromyalgia, alcohol, and hyperalgesia.]
2024 — New section: No notes. Just a new chapter. [Updated section: Fibromyalgia, alcohol, and hyperalgesia.]
2023 — Added content: Added fast breathing exercises (hyperventilation) to the list of treatment options worth considering. [Updated section: A grab bag of “reasonable” treatment ideas for fibromyalgia.]
2022 — Science update: Added an interesting citation about the infectious roots of multiple sclerosis (Bjornevik). [Updated section: Conditions that may be confused with fibromyalgia.]
2021 — New section: No notes. Just a new chapter. [Updated section: Ozone therapy — a classic example of fibromyalgia snake oil.]
2021 — New sidebar: Added a bit of comic relief: “Demon tries to inhabit my body … and regrets it.”
2021 — Revised: Significant improvements to the clarity of some tricky concepts. [Updated section: Is fibromyalgia a “diagnosis of exclusion” or “wastebasket diagnosis”?]
2021 — New section: No notes. Just a new chapter. [Updated section: Miserable mice! Fibromyalgia transplanted to mice…in blood?]
2021 — Science update: Added two token citations about cannabis for fibromyalgia. “Token” because the evidence barely exists. [Updated section: A grab bag of “reasonable” treatment ideas for fibromyalgia.]
2021 — Upgrade: Added table of contents.
Archived updates — All updates, including 32 older updates, are listed on another page. ❐
2017 — Publication.
Notes
- More exactly: chronic pain that is not associated with any known pathology that can explain it, especially cancer (“malignant pain,” a huge category of chronic pain, and generally considered and managed very differently from other kinds of chronic pain).
- Jones GT, Atzeni F, Beasley M, et al. The prevalence of fibromyalgia in the general population: a comparison of the American College of Rheumatology 1990, 2010, and modified 2010 classification criteria. Arthritis Rheumatol. 2015 Feb;67(2):568–75. PubMed 25323744 ❐
- Wolfe F, Walitt B, Perrot S, Rasker JJ, Häuser W. Fibromyalgia diagnosis and biased assessment: Sex, prevalence and bias. PLoS One. 2018;13(9):e0203755. PubMed 30212526 ❐ PainSci Bibliography 49948 ❐
Almost everyone thinks that almost everyone with fibromyalgia is a woman, with a traditionally accepted proportion of greater than ninety percent. Imagine my surprise when I learned that this immense gender gap was never supported by good data!
Wolfe et al. used validated criteria and unbiased selection of patients to get a female proportion of less than 60%.
That’s quite the difference! That’s only a minor gender gap, not an immense one.
![A pair of pie charts compares a myth versus the truth about the gender ratio in fibromyalgia. The left chart, labeled “MYTH,” claims that fibromyalgia is 90% female and shows a small blue wedge (male) and a large red portion (female). The right chart, labeled “TRUTH,” states that fibromyalgia is actually only 60% female.]()
In an ironic twist, this distortion was probably created by sexism, and it surely perpetuates it. Srinivasan et al. reported that physician diagnosis is wildly out of sync with diagnostic criteria: “clearly most physicians do not know or pay attention to criteria,” and their judgement is also “biased with respect to sex.” In other words, women are much more likely to be diagnosed with fibromyalgia if they have any symptoms that seem fibromyalgia-ish … even if they don’t actually have fibromyalgia.
And if you’re a man with fibromyalgia? You are unlikely to get diagnosed with it!
Fibromyalgia is the most important and glaring example of the medical myth of feminine fragility: see Chronic Pain and Inequality: The role of racism, sexism, queerphobia, ageism, and poverty in health and chronic pain.
- This stigma is the obvious dark side of the pervasive idea that a positive attitude is actually medicinal, an optimistic delusion so out of control that it has been called “toxic positivity,” harmfully delusional optimism. It is harmful because it implies that anyone who is chronically ill has failed to think positively enough. You cannot believe in the power of mind over body without directly implying that illness is a failure to know and use that power — a belief that mostly inspires only condescending sympathy, rather than respect and empathy. This belief is so common and strong that most people actually believe that cancer outcomes are better with positive thinking (they aren’t) … and if you believe that, then overcoming chronic pain could should be a piece of cake!
Healthcare lets people down in many ways, of course, but it’s especially bad for patients with puzzling and/or persistent pain and injury. Fibromyalgia is one of the best examples, but many kinds of pain patients bounce around the medical system — and its alternative shadow — like they are in an evil pinball machine of disappointment and frustration. They are …
- Serially misdiagnosed, patronized and dismissed, blamed and gaslit, and demonized as drug-seekers.
- Referred to specialists who never seem to be the right specialists.
- Irradiated (scanned) to find copious red herrings that routinely have nothing to do with their pain.
- Indoctrinated in endless examples of fashionable ideology to “explain” their pain, from “your glutes aren’t activating” to “you’re just sensitized.”
- Inundated with dubious treatment options: expensive, distracting, counterproductive, and (surprisingly often) even dangerous.
The whole business of helping people with pain and injury is a shambolic parody of good healthcare. Read much more: Why is it so hard to get good help for pain? Part 1 (Member Post).
- www.fmperplex.com [Internet]. Wolfe F. 75% of Persons in the General Population Diagnosed with Fibromyalgia Don’t Have It, But It Is Worse Than That … – The Fibromyalgia Perplex; 2017 January 11 [cited 17 Jan 19]. PainSci Bibliography 53744 ❐
This is a scholarly commentary on the substantial over and under diagnosis of fibromyalgia, with an estimated 75% of people with diagnosis actually not fitting diagnostic criteria, about 1.5% of the US population:
By our calculations almost 3 million people who do not meet fibromyalgia criteria have been given a fibromyalgia diagnosis. At the other end of the spectrum, there are almost 3 million persons who satisfy fibromyalgia criteria, but have not been diagnosed with the disorder by a physician.
The authors argue that misdiagnosis is driven more by “socially-constructed factors” like pharmaceutical companies aggressively teaching doctors to diagnose fibromyalgia and prescribe (unproven) drugs for it; patient advocacy groups trying to legitimize the diagnosis; and doctors seeking prestige by publishing about fibromyalgia.
They also make some important points about the state of our understanding of fibromyalgia along the way, most notably that central sensitization remains both unproven and problematic as a major cause or mechanism of fibromyalgia.
- Thieme K, Mathys M, Turk DC. Evidenced-Based Guidelines on the Treatment of Fibromyalgia Patients: Are They Consistent and If Not, Why Not? Have Effective Psychological Treatments Been Overlooked? J Pain. 2017 Jul;18(7):747–756. PubMed 28034828 ❐ This paper is an extremely technical analysis of four sets of treatment guidelines for fibromyalgia produced by four different organizations. Although super dense reading, it all boiled down to a really simple conclusion: they don’t agree with each other! The guidelines are inconsistent. I will return to this reference again later.
- Stiffness is a form of mild pain or discomfort with movement with many possible causes that may or may not involve any actually restricted movement — usually not, in the case of fibromyalgia, although it’s possible that some dystonia (abnormal muscle tone) is involved. For more information, see Why Do Muscles Feel Stiff and Tight?
- Anspach, Beth. “From living the ‘perfect storm’ to helping people: After recovering from years of chronic pain, woman helps others.” Dayton Daily News. Undated. Terrible article, basically just an advertisement for McCullough’s book about how to cure fibromyalgia. She believes she recovered from fibromyalgia thanks to “meditating and praying daily … a holistic therapist … visualizing herself as healthy … detoxification.” And this is the person who thinks that she “finally knew what was wrong” because her illness was given a label (as far as we can tell from the reporting).
- Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990 Feb;33(2):160–72. PubMed 2306288 ❐
- Wolfe F, Clauw DJ, Fitzcharles MA, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res (Hoboken). 2010 May;62(5):600–10. PubMed 20461783 ❐
- Wolfe F, Clauw DJ, Fitzcharles MA, et al. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J Rheumatol. 2011 Jun;38(6):1113–22. PubMed 21285161 ❐
The original ACR diagnostic criteria for fibromyalgia were published in 1990 (Wolfe) and the first major revision was published in 2010 (Wolfe), and this paper added the FMS symptom scale, “which measures what the authors call the overall ‘fibromyalgianess’ of a patient.”
This paper is not directly useful to patients, but Neha Garg does a good job of explaining it: New and Modified Fibromyalgia Diagnostic Criteria. See also Wolfe’s 2015 paper, “Editorial: the status of fibromyalgia criteria”.
- Wolfe F, Clauw DJ, Fitzcharles MA, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016 12;46(3):319–329. PubMed 27916278 ❐
- Mascarenhas RO, Souza MB, Oliveira MX, et al. Association of Therapies With Reduced Pain and Improved Quality of Life in Patients With Fibromyalgia: A Systematic Review and Meta-analysis. JAMA Intern Med. 2020 Oct. PubMed 33104162 ❐
- Jensen TS, Baron R, Haanpää M, et al. A new definition of neuropathic pain. Pain. 2011 Oct;152(10):2204–5. PubMed 21764514 ❐
IASP has recently [2008] published a new definition of neuropathic pain according to which neuropathic pain is defined as ‘pain caused by a lesion or disease of the somatosensory system.’ This definition replaces the 17-year old definition that appeared in the Classification of Chronic Pain published by IASP in 1994, which defined neuropathic pain as ‘pain initiated or caused by a primary lesion, dysfunction, or transitory perturbation of the peripheral or central nervous system’. Even though the definition has not been changed dramatically, there are two important changes in the new version: (1) the word ‘dysfunction’ has been removed and (2) a lesion or disease affecting the nervous system has been specified to be a lesion or disease of the somatosensory system.
The whole paper is excellent, but skipping to the cogent conclusion:
A definition of neuropathic pain is only useful if it distinguishes conditions in a clinically meaningful way. If the definition does not provide additional benefit in terms of understanding and treating the condition(s), then there is no reason to keep it. Hopefully, the new definition of neuropathic pain will act as a stimulant to discuss the definition in more detail and provide input for studies that can be used to test the value of the definition.
- Multiple sclerosis attacks nerves in quite a dramatic way, which we could see in autopsies, but the lesions were invisible in living patients until the invention of MRI. It’s plausible that there are still plenty of biological “lesions” that we haven’t yet learned to detect, because they are just too small and transient. Despite all of our modern technological wizardy, most of the action in biology happens at the nanoscale, cells moving molecules and atoms around at dazzling speeds through the chaos of the molecular storm (brownian motion). There are probably nanoscale lesions.
- Both small fibre peripheral neuropathy and positional cervical cord compression are candidate neuropathic causes: both hard to detect, both capable of explaining at least some of the symptoms of fibromyalgia, both associated with people who have been diagnosed with fibromyalgia.
- Light KC, White AT, Tadler S, Iacob E, Light AR. Genetics and Gene Expression Involving Stress and Distress Pathways in Fibromyalgia with and without Comorbid Chronic Fatigue Syndrome. Pain Res Treat. 2012;2012:427869. PubMed 22110941 ❐ PainSci Bibliography 52980 ❐
This is an extremely dense, technical review finding “some support” for both inherited susceptibility to FM/CFS and/or physiological dysregulation of multiple relevant systems.
- Lyon P, Cohen M, Quintner J. An evolutionary stress-response hypothesis for chronic widespread pain (fibromyalgia syndrome). Pain Med. 2011 Aug;12(8):1167–78. PubMed 21692974 ❐ “Drawing on diverse findings in neurobiology, immunology, physiology, and comparative biology, we suggest that the form of central sensitization that leads to the profound phenomenological features of chronic widespread pain is part of a whole-organism stress response, which is evolutionarily conserved, following a general pattern found in the simplest living systems.”
- BetterMovement.org [Internet]. Hargrove T. A Systems Perspective on Chronic Pain; 2014 Oct 23 [cited 16 Sep 12]. PainSci Bibliography 53866 ❐
This deep but beautifully readable article explains, with many pictures and apt examples, how “chronic pain is often driven by dysregulation of a ‘supersystem’ that coordinates defensive responses to injury. The supersystem results from dynamic interaction between different subsystems, most notably the nervous system, immune system, and endocrine system.” The article also manages to make this information seem quite practical, believe it or not.
- Kosek E, Cohen M, Baron R, et al. Do we need a third mechanistic descriptor for chronic pain states? Pain. 2016 Jul;157(7):1382–6. PubMed 26835783 ❐ PainSci Bibliography 53276 ❐
- Bäckryd E, Tanum L, Lind AL, Larsson A, Gordh T. Evidence of both systemic inflammation and neuroinflammation in fibromyalgia patients, as assessed by a multiplex protein panel applied to the cerebrospinal fluid and to plasma. J Pain Res. 2017;10:515–525. PubMed 28424559 ❐ PainSci Bibliography 53589 ❐
Although inflammation has been suspected in fibromyalgia, it has been poorly studied to date. This experiment went much further, employing “a new multiplex protein panel enabling simultaneous analysis of 92 inflammation-related proteins.” They looked for these markers in the cerebrospinal fluid and blood of 40 fibromyalgia patients and compared with healthy controls, finding an “extensive inflammatory profile.”
- Wolfe 2016, op. cit.
- Galvez-Sánchez CM, Reyes Del Paso GA. Diagnostic Criteria for Fibromyalgia: Critical Review and Future Perspectives. J Clin Med. 2020 Apr;9(4). PubMed 32340369 ❐ PainSci Bibliography 51905 ❐
- And even if it was prescriptively mapped out, it would still be at odds with common usage, and all this makes it hard to, er, exclude. “Exclusion criteria” is a precise term, making specific exclusions a requirement, but “diagnosis of exclusion” is looser and more pragmatic, does not require exclusion criteria, and describes a typical messy diagnostic process in which a certain amount of “narrowing” (Wolfe) is both necessary and inevitable.
- Bjornevik K, Cortese M, Healy BC, et al. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science. 2022 01;375(6578):296–301. PubMed 35025605 ❐ PainSci Bibliography 52020 ❐
This study strongly linked the endemic Epstein-Barr to multiple sclerosis by studying millions of subjects over twenty years. Unlike countless other “links” in medical science, there is so much correlation smoke here that there is almost certainly a causality fire. The risk of developing multiple sclerosis thirty-two times greater after EBV infection. And so EBV probably causes multiple sclerosis (in combination with other factors) — an extremely important discovery.
- Wijnands JM, Zhu F, Kingwell E, et al. Five years before multiple sclerosis onset: Phenotyping the prodrome. Mult Scler. 2019 07;25(8):1092–1101. PubMed 29979093 ❐
- Jutras BL, Lochhead RB, Kloos ZA, et al. Borrelia burgdorferi peptidoglycan is a persistent antigen in patients with Lyme arthritis. Proc Natl Acad Sci U S A. 2019 Jul;116(27):13498–13507. PubMed 31209025 ❐ PainSci Bibliography 52327 ❐
Basically, the Borrelia burgdorferi organism appears to poison people with a protein that remains long after the bacteria are dead.
- Although fibromyalgia may include the burning pain or nerve tingling characteristic of SFPN, most patients with SFPN don’t have the hallmark FMS symptom of widespread deep tissue pain or other classic fibromyalgia symptoms like severe fatigue.
- Ingraham. The Trigger Point Identity Crisis: The biological evidence that a trigger point is a lesion in muscle tissue. PainScience.com. 3775 words.
- PracticalPainManagement.com [Internet]. Holman A. Using Dynamic MRI to Diagnose Neck Pain: The Importance of Positional Cervical Cord Compression (PC3); 2017 January 12 [cited 17 Sep 1]. PainSci Bibliography 53754 ❐
A remarkable article for a medical audience, technical and scholarly but cogent, exploring fascinating potential connections between PC3 and/or Chiari malformation and fibromyalgia and chronic widespread pain.
- Chan CK, Lee HY, Choi WC, Cho JY, Lee SH. Cervical cord compression presenting with sciatica-like leg pain. Eur Spine J. 2011 Jul;20 Suppl 2:S217–21. PubMed 20938789 ❐ PainSci Bibliography 53701 ❐
A report on two cases of cervical spinal cord impingement causing leg pain — both examples of pain at a location unusually remote from a subtle lesion (referred pain) — both successfully treated surgically. Notably, both cases involved previous lumbar spine problems.
Interestingly, such distant referred pain is tangentially relevant to the hypothetical phenomenon of cervical spinal cord irritation causing fibromyalgia (see Using Dynamic MRI to Diagnose Neck Pain).
- Heffez DS, Ross RE, Shade-Zeldow Y, et al. Clinical evidence for cervical myelopathy due to Chiari malformation and spinal stenosis in a non-randomized group of patients with the diagnosis of fibromyalgia. Eur Spine J. 2004 Oct;13(6):516–23. PubMed 15083352 ❐ PainSci Bibliography 52751 ❐
Patients with fibromyalgia often also have symptoms of myelopathy (spinal cord impingement), but are often never assessed by a neurologist. In this study, 270 points with a fibromyalgia diagnosis only were given a thorough neurological assessment. Many of them had several clear signs and symptoms of myelopathy, most notably narrowing of the spinal canal, especially positioned in neck extension. The authors concluded: “Our findings indicate that some patients who carry the diagnosis of fibromyalgia have both signs and symptoms consistent with cervical myelopathy, most likely resulting from spinal cord compression.”
Other than a follow-up study by the authors and the work of Andrew Holman (see Using Dynamic MRI to Diagnose Neck Pain), there is no other research on this important topic.
- Heffez DS, Ross RE, Shade-Zeldow Y, et al. Treatment of cervical myelopathy in patients with the fibromyalgia syndrome: outcomes and implications. Eur Spine J. 2007 Sep;16(9):1423–33. PubMed 17426987 ❐ PainSci Bibliography 52887 ❐
This fascinating study follows from an early one (Heffez) that showed a clear link between fibromyalgia and myelopathy (the symptoms of cervical spinal cord compression). They tested the link more directly in this study by treating spinal cord compression surgically in 40 patients with the symptoms of both fibromyalgia, comparing the results to another 31 patients treated non-surgically. “There was a striking and statistically significant improvement” in the surgically treated patients, compared to the non-surgically treated patients.
The surgical treatment of cervical myelopathy due to spinal cord or caudal brainstem compression in patients carrying the diagnosis of fibromyalgia can result in a significant improvement in a wide array of symptoms usually attributed to fibromyalgia with attendant measurable improvements in the quality of life.
- Holman AJ. Positional cervical spinal cord compression and fibromyalgia: a novel comorbidity with important diagnostic and treatment implications. J Pain. 2008 Jul;9(7):613–22. PubMed 18499527 ❐
- Zhang L, Zeitoun D, Rangel A, et al. Preoperative evaluation of the cervical spondylotic myelopathy with flexion-extension magnetic resonance imaging: about a prospective study of fifty patients. Spine (Phila Pa 1976). 2011 Aug;36(17):E1134–9. PubMed 21785299 ❐
This study demonstrates that much more information can be obtained by imaging the neck in a range of positions (dynamic MRI), as opposed to just a neutral position. 50 patients on their way to neck surgery to help with spinal cord trouble were much more thoroughly scanned than they normally would have been. Cord impingement was spotted in just 17 patients in the neutral position, but thirty-seven in extension (and several in flexion as well). Cord inflammation was visible in just 13 patients in neutral position but twenty in a flexed position. The authors concluded that “Dynamic MRI is useful to determine more accurately the number of levels where the spinal cord is compromised.”
- Herzog R, Elgort DR, Flanders AE, Moley PJ. Variability in diagnostic error rates of 10 MRI centers performing lumbar spine MRI examinations on the same patient within a 3-week period. Spine J. 2016 Nov. PubMed 27867079 ❐
In this study, one patient with sciatica was sent for ten MRIs, which produced 49 distinct “findings,” 16 of them unique, none of which occurred in all ten reports. On average, each radiologist made about a dozen errors, seeing one or two things that weren’t there and missing about ten things that were. Yikes. Read a more detailed and informal description of this study.
- Rowe PC, Marden CL, Heinlein S, Edwards 2. Improvement of severe myalgic encephalomyelitis/chronic fatigue syndrome symptoms following surgical treatment of cervical spinal stenosis. J Transl Med. 2018 Feb;16(1):21. PubMed 29391028 ❐ PainSci Bibliography 53054 ❐ “We describe three consecutive patients with severe ME/CFS whose symptoms improved after recognition and surgical management of their cervical spinal stenosis.”
- Brooke. “ME vs. CFS — They’re Not The Same!” DocumentingME.net. Accessed 2017-08-16.
- HFME.org [Internet]. Bassett J. M.E. vs Fibromyalgia; 2017 August 16 [cited 23 Apr 11]. PainSci Bibliography 52984 ❐ This document is the source for most of my specific points on the differences between ME and FM.
- Cook DB, Light AR, Light KC, et al. Neural consequences of post-exertion malaise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Brain Behav Immun. 2017 May;62:87–99. PubMed 28216087 ❐ Brain study of the “neural consequences” of acute exercise in people who suffering from excessive post-exertion malaise (PEM). They claim to have found “objective evidence of the detrimental neurophysiological effects of PEM.”
- I will bring up the scandal-scarred PACE trial later in the tutorial in the exercise section.
Leary, Sian. “New Graded Exercise Warning on Current ME/CFS Guideline.” Dec 11, 2020. MEAction.net.
After years of campaigning to highlight the harm people with ME have experienced when undergoing graded exercise therapy, MEAction UK have just received a momentous email from the National Institute for Health and Care Excellence (NICE), advising us that:
“NICE have updated the warning on the 2007 CFS/ME guideline, directing health professionals to the new draft recommendations on graded exercise therapy which explicitly state:
“Do not offer people with ME/CFS any programme based on fixed incremental increases in physical activity or exercise, for example graded exercise therapy”
- Johnston KJA, Adams MJ, Nicholl BI, et al. Genome-wide association study of multisite chronic pain in UK Biobank. PLoS Genet. 2019 Jun;15(6):e1008164. PubMed 31194737 ❐ PainSci Bibliography 52248 ❐ Interestingly, almost half of the genes identified by Johnston et al. are also risk factors for severe depression, and there’s also substantial genetic overlap between chronic pain and chronic pain and schizophrenia, body-mass index, rheumatoid arthritis, and post-traumatic stress disorder, amongst others.
- Khoury S, Piltonen MH, Ton AT, et al. A functional substitution in the L-aromatic amino acid decarboxylase enzyme worsens somatic symptoms via a serotonergic pathway. Ann Neurol. 2019 Jun. PubMed 31177555 ❐
- Why so little serotonin? Because they all had a glitchy gene that codes for an impaired, sluggish version of an enzyme, critical for serotonin production, specifically “the minor allele of rs11575542, located in the DDC gene,” which is on chromosome 7. If you must know. This gene has an important job: it swaps “an arginine to a glutamine at position 462 close to the C-terminus in the AADC protein.” But the glitchy version does it… way… too… slowly. Oops. There are also genetic variants that result in complete failure to make the AADC protein, and that’s a biological disaster. This gene just makes slow AADC.
- Cassisi G, Sarzi-Puttini P, Cazzola M. Chronic widespread pain and fibromyalgia: could there be some relationships with infections and vaccinations? Clin Exp Rheumatol. 2011;29(6 Suppl 69):S118–26. PubMed 22243559 ❐
- Bennett RM, De Garmo P, Clark SR. A Randomized, Prospective, 12 Month Study To Compare The Efficacy Of Guaifenesin Versus Placebo In The Management Of Fibromyalgia. Arthritis Rheum. 1996;39 (Supplement 9)(S212).
Despite a high risk of bias in favour of this treatment, the authors concluded that “this study provides persuasive evidence that the improvement was not due to a disease specific effect of guaifenesin on the underlying pathophysiology of fibromyalgia.”
- Simms RW, Roy SH, Hrovat M, et al. Lack of association between fibromyalgia syndrome and abnormalities in muscle energy metabolism. Arthritis Rheum. 1994 Jun;37(6):794–800. PubMed 8003050 ❐ “This study demonstrates that under the conditions studied, muscle energy metabolism in FMS is no different than that in sedentary controls. These findings do not support the hypothesis that detectable defects in muscle energy metabolism occur in FMS.”
- Smith SM, Schroeder K, Fahey T. Over-the-counter (OTC) medications for acute cough in children and adults in community settings. Cochrane Database Syst Rev. 2014 Nov;(11):CD001831. PubMed 25420096 ❐ “Three trials compared the expectorant guaifenesin with placebo; one indicated significant benefit, whereas the other two did not.”
- Cadegiani FA, Kater CE. Adrenal fatigue does not exist: a systematic review. BMC Endocr Disord. 2016 Aug;16(1):48. PubMed 27557747 ❐ PainSci Bibliography 52878 ❐
Conclusion:
To our knowledge, this is the first systematic review made by endocrinologists to examine a possible correlation between the HPA axis and a purported “adrenal fatigue” and other conditions associated with fatigue, exhaustion or burnout. So far, there is no proof or demonstration of the existence of “AF”. While a significant number of the reported studies showed differences between the healthy and fatigued groups, important methodological issues and confounding factors were apparent. [Translation: biased, sloppy science! ~ Paul] Two concluding remarks emerge from this systematic review: (1) the results of previous studies were contradictory using all the methods for assessing fatigue and the HPA axis, and (2) the most appropriate methods to assess the HPA axis were not used to evaluate fatigue. Therefore, “AF” requires further investigation by those who claim for its existence.
- Acupuncture has a good reputation that it does not deserve. Although heavily researched, its support comes only from biased junk science, while it fails all the good quality scientific tests. It does not work for pain or anything else and we shouldn’t be surprised: it’s based on mysticism and myths. It’s surprisingly modern rather than ancient and wise, for instance, and cannot actually be used for anesthesia. More study is not needed. For more information, see Does Acupuncture Work for Pain? A review of modern acupuncture evidence and myths, focused on treatment of back pain & other common chronic pains.
- Rosa L, Rosa E, Sarner L, Barrett S. A close look at therapeutic touch. JAMA. 1998 Apr 1;279(13):1005–10. PubMed 9533499 ❐ PainSci Bibliography 56856 ❐
This paper is an entertaining chapter in the history of the science of alternative medicine: a child’s science fair project published in the Journal of the American Medical Association. Emily Rosa’s experiment showed that “twenty-one experienced therapeutic touch practitioners were unable to detect the investigator's ‘energy field.’ Their failure to substantiate TT's most fundamental claim is unrefuted evidence that the claims of TT are groundless and that further professional use is unjustified.”
Therapeutic touch practitioners could not demonstrate any ability to detect a person by feeling their aura, let alone manipulating it therapeutically. The test made them look ridiculous.
Ms. Rosa was just nine years old when she did this experiment, and remains the youngest person to have a research paper published in a peer reviewed medical journal. (It is, of course, likely that she had some parental assistance — but I don’t know the whole story.)
- Levy, Louise. Facebook post, July 11, 2017.
- CoyneOfTheRealm.com [Internet]. Coyne J. When promoting cognitive behavior therapy for fibromyalgia is quackery – Coyne of the Realm; 2017 August 17 [cited 17 Sep 1]. PainSci Bibliography 52989 ❐
- Burke NN, Finn DP, McGuire BE, Roche M. Psychological stress in early life as a predisposing factor for the development of chronic pain: Clinical and preclinical evidence and neurobiological mechanisms. J Neurosci Res. 2016 Jul. PubMed 27402412 ❐
- Boring BL, Mathur VA. Gender Discrimination is Associated with Greater Chronic Pain Interference Among Women. J Pain. 2025 Mar:105376. PubMed 40107587 ❐
How much does chronic pain interfere with your life? Probably more if you’re a woman routinely exposed to sexism! Probably due to the stress. Pain is more of a burden when you’re already angry/scared…as women tend to be.
“Men are afraid women will laugh at them. Women are afraid men will kill them.” ~ Margaret Atwood (attribution endorsed by Quote Investigator)
That’s the implication of this new study by Boring et al., reporting a link between the frequency of daily experiences of gender discrimination and “greater pain interference” (the degree to which pain interferes with life). No such link was found for men.
This result harmonizes nicely with Jin et al., who reported a similar link with social injustice more generally.
This is the kind of “woke” research that is currently being strangled in the US by the Trump administration. 🙄 And that is making women even angrier!
- Coppens E, Van Wambeke P, Morlion B, et al. Prevalence and impact of childhood adversities and post-traumatic stress disorder in women with fibromyalgia and chronic widespread pain. Eur J Pain. 2017 May. PubMed 28543929 ❐
- Wolfe 2018, op. cit. See previous note for details.
- Lyon 2011, op. cit.
- Generaal E, Vogelzangs N, Macfarlane GJ, et al. Biological stress systems, adverse life events and the onset of chronic multisite musculoskeletal pain: a 6-year cohort study. Ann Rheum Dis. 2015 Apr. PubMed 25902791 ❐
- Can chronic pain be a “learned response” (classical conditioning) to things that shouldn’t hurt, like Pavlov’s dogs salivating to the ring of a bell? It’s an interesting idea, with obviously optimistic implications, because what is learned might also be un-learned. If so, it’s a bit of a brain hack, a clever and surprising solution around one of the hardest problems there is. It’s a bit unlikely, but so interesting that it’s worth discussing and exploring. See Chronic Pain as a Conditioned Response: If pain can be learned, perhaps it can be unlearned.
- Espay AJ, Aybek S, Carson A, et al. Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders. JAMA Neurol. 2018 09;75(9):1132–1141. PubMed 29868890 ❐
- O’Sullivan S. It's All in Your Head: True Stories of Imaginary Illness. Chatto & Windus; 2015. p. 160.
For a patient to consciously fake illness is rare. There are always rumours, the woman who put blood in her own urine to convince people that she had a serious kidney disease, the man who rubbed dirt into his wound to cause a deliberate infection. But most doctors will see such behaviour only once or twice in their careers, if at all. And yet somehow the shadow of those who deceive hangs over every person who is deemed to have a physical illness that does not have an organic cause.
Dr. O’Sullivan tells the story of the only case of malingering she believes she encountered. She had a patient in a wheelchair, claiming to be paralyzed. All kinds of alarm bells were going off, and she suspected malingering but couldn’t really do much with it. Not long after, on her way to lunch, she passed the patient on the street, where he was standing up and loading his wheelchair into the back of the car. He turned, saw her, and said, “Oh shit.” Busted!
- Sapolsky RM. Why Zebras Don’t Get Ulcers. 3rd ed. New York: Times Books; 2004. chapter 12, “Aging and death.” Sapolsky explains how there are some confirmed examples of species with biologically programmed deaths — like salmon — that pull their own plug with a flood of stress hormones. They literally poison themselves to death with glucocorticoids, which massively accelerates degeneration. Anything is toxic in excess, so this doesn’t necessarily mean that more moderate doses of glucocorticoids cause premature aging, but it is certainly possible.
- For instance, inflammation is synoymous with immune system activity, which may increase erratically — and permanently — over the years we encounter more microorganisms. The antibodies we develop to fight those infections sometimes match our own tissues, which is basically the modern theory of autoimmune disease. So inflammaging may basically be mild autoimmune disease… or not-so-mild, but not readily classifiable as one of the main autoimmune diseases. For more detail about this secondary, explanatory idea, see the inflammation article.
- I know that “delicate balance” all too well. My drinking is strongly “pain-motivated.” It feels like I drink to survive and cope. My nightly buzz is often the only hour of the day that I get any relief from the constant onslaught of discomfort. The impulse to drink is so strong that I have accepted for the last few years that I sure now have alcohol use disorder (the formal way to say “I’m an alcoholic”). However, I also have to very strictly limit my dosage to roughly one serving … because any more and I risk sabotaging myself, dramatically exacerbating my symptoms for up to a day.
- Robins MT, Heinricher MM, Ryabinin AE. From Pleasure to Pain, and Back Again: The Intricate Relationship Between Alcohol and Nociception. Alcohol Alcohol. 2019 Dec;54(6):625–638. PubMed 31509854 ❐ PainSci Bibliography 51671 ❐
- Hall OT, Rausch J, Entrup P, et al. Nociplastic Pain and Pain-Motivated Drinking in Alcohol Use Disorder. J Pain. 2024 Jan. PubMed 38219852 ❐ PainSci Bibliography 51677 ❐
- Neuroticism is a one of the major personality traits, and is all about having more negative emotions. Neurotic people are likelier to suffer from any negative emotion, but neuroticism is close to synonymous with the more familiar problems of anxiety and depression. Obviously this way of linking alcohol use disorder to fibromyalgia requires buying into the idea of the “fibromyalgia personality,” but remember that anxiety and depression could also be symptoms of an underlying pathology. Confusing!
- CCSA.ca [Internet]. Canadian Centre on Substance Use and Addiction. Canada’s Guidance on Alcohol and Health: Final Report; 2023 [cited 23 Jul 11]. PainSci Bibliography 51290 ❐
- Mascarenhas 2020, op. cit.
- Thieme 2017, op. cit. The four different organizations that produced the guidelines each looked a great deal of research with impressively little overlap: not a single study was referenced by all four, for instance, and 35% was the highest citation overlap reached between any two of them!
- Because opioids are generally ineffective for chronic non-cancer pain and because they are too dangerous: not just the risk of dependence, but also a scary and alarmingly non-rare backfire effect in which opioids actually increase chronic widespread pain (“opioid hyperalgesia,” see Lee, Grace). For more information, see Opioids for Chronic Aches & Pains.
- Mascarenhas 2020, op. cit. Referring to CBT, antidepressants, and CNS depressants, Mascarenhas et al. concluded: “Some therapies may reduce pain and improve QOL in the short to medium term, although the effect size of the associations might not be clinically important to patients.” In fact, the associations between these treatments and good outcomes were “were small and did not exceed the minimum clinically important change (2 points on an 11-point scale for pain and 14 points on a 101-point scale for quality of life).”
- Rain C, Seguel W, Vergara L. Does exercise improve symptoms in fibromyalgia? Medwave. 2015 Dec;15 Suppl 3:e6335. PubMed 26730713 ❐ “We conclude that regular physical exercise probably reduces pain in patients with fibromyalgia.”
- Fernandes G, Jennings F, Nery Cabral MV, Pirozzi Buosi AL, Natour J. Swimming Improves Pain and Functional Capacity of Patients With Fibromyalgia: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2016 Aug;97(8):1269–75. PubMed 26903145 ❐ “Swimming, like walking, is an effective method for reducing pain and improving both functional capacity and quality of life in patients with fibromyalgia.”
- Bidonde J, Busch AJ, Webber SC, et al. Aquatic exercise training for fibromyalgia. Cochrane Database Syst Rev. 2014 Oct;(10):CD011336. PubMed 25350761 ❐ “Low to moderate quality evidence relative to control suggests that aquatic training is beneficial for improving wellness, symptoms, and fitness in adults with fibromyalgia.”
- Busch AJ, Webber SC, Richards RS, et al. Resistance exercise training for fibromyalgia. Cochrane Database Syst Rev. 2013 Dec;(12):CD010884. PubMed 24362925 ❐ “The evidence (rated as low quality) suggested that moderate- and moderate- to high-intensity resistance training improves multidimensional function, pain, tenderness, and muscle strength in women with fibromyalgia.”
- None of that evidence is actually strong. All of those papers have positive results based on low quality evidence, because most trials have major problems. Overall the evidence looks encouraging, but it’s far from proven.
- Academy of Medical Royal Colleges. Exercise: The miracle cure and the role of the doctor in promoting it. AOMRC.org.uk. 2015 Feb. PainSci Bibliography 53672 ❐
This citation is the primary authoritative source of the quote “exercise is the closest thing there is to a miracle cure” (although there are no doubt many variations on it from other sources over the years).
- Gopinath B, Kifley A, Flood VM, Mitchell P. Physical Activity as a Determinant of Successful Aging over Ten Years. Sci Rep. 2018 Jul;8(1):10522. PubMed 30002462 ❐ PainSci Bibliography 53004 ❐
If you want to age well, move around a lot!
We already know that physical activity reduces the risk of several of the major chronic diseases and increases lifespan. “Successful aging” is a broader concept, harder to measure, which encompasses not only a reduced risk of disease but also the absence of “depressive symptoms, disability, cognitive impairment, respiratory symptoms and systemic conditions.” (No doubt disability from pain is part of that equation.)
In this study of 1584 older Australians, 249 “aged successfully” over ten years. The most active Aussies, “well above the current recommended level,” were twice as likely to be in that group. Imagine how much better they’ll do over 20 years …
- Geneen LJ, Moore RA, Clarke C, et al. Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2017 Jan;1:CD011279. PubMed 28087891 ❐
Chronic pain, exercise, and physical activity are all heavily studied, but the result of this massive review of reviews — pooling data from more than 37,000 participants — somehow amounts only to “it’s promising, but more study needed.” It was based on hundreds of studies, but nearly all them underpowered and flawed. Garbage in, garbage out … on a huge scale! But where there’s smoke there’s probably at least a small fire: “The available evidence suggests physical activity and exercise is an intervention with few adverse events that may improve pain severity and physical function, and consequent quality of life.” But it’s far from the conclusion we’d like to see, even from underpowered studies. Obviously some kinds of pain probably respond better to exercise than others.
(See more detailed commentary on this paper.)
Such as fibromyalgia? Hopefully!
- Lima LV, Abner TSS, Sluka KA. Does exercise increase or decrease pain? Central mechanisms underlying these two phenomena. J Physiol. 2017 Mar. PubMed 28369946 ❐ “Regular physical activity is recommended for treatment of chronic pain and its effectiveness has been established in clinical trials for people with a variety of pain conditions. However, exercise can also increase pain making participation in rehabilitation challenging for the person with pain.”
- For instance, in this bad example article with a high Google rank, no attempt is made to distinguish between fibromyalgia, chronic fatigue syndrome, or myalgic encephalomyelitis. “Pacing” is recommended to all, as if there were no difference between the conditions. Caveat lector!
- CoyneOfTheRealm.com [Internet]. Coyne J. Uninterpretable: Fatal flaws in PACE Chronic Fatigue Syndrome; 2017 August 17 [cited 21 Nov 18]. PainSci Bibliography 52990 ❐ Psychiatrist James Coyne has written extensively about PACE-gate. This is his overview of the topic, but there’s much more.
- www.virology.ws [Internet]. Tuller D. Trial by Error: The Troubling Case of the PACE Chronic Fatigue Syndrome Study; 2017 August 17 [cited 21 Nov 18]. PainSci Bibliography 52991 ❐
Tuller starts his exhaustive explanation of the PACE debacle with a juicy selection of damning expert opinions:
Dr. Bruce Levin, Columbia University: “To let participants know that interventions have been selected by a government committee ‘based on the best available evidence’ strikes me as the height of clinical trial amateurism.”
Dr. Ronald Davis, Stanford University: “I’m shocked that the Lancet published it … . The PACE study has so many flaws and there are so many questions you’d want to ask about it that I don’t understand how it got through any kind of peer review.”
Dr. Arthur Reingold, University of California, Berkeley: “Under the circumstances, an independent review of the trial conducted by experts not involved in the design or conduct of the study would seem to be very much in order.”
Dr. Jonathan Edwards, University College London: “It’s a mass of un-interpretability to me … All the issues with the trial are extremely worrying, making interpretation of the clinical significance of the findings more or less impossible.”
Dr. Leonard Jason, DePaul University: “The PACE authors should have reduced the kind of blatant methodological lapses that can impugn the credibility of the research, such as having overlapping recovery and entry/disability criteria.”
- www.nytimes.com [Internet]. Rehmeyer J, Tuller D. Getting It Wrong on Chronic Fatigue Syndrome; 2021 November 18 [cited 23 Aug 30]. PainSci Bibliography 52219 ❐
- Shepherd CB. PACE trial claims for recovery in myalgic encephalomyelitis/chronic fatigue syndrome - true or false? It's time for an independent review of the methodology and results. J Health Psychol. 2017 Aug;22(9):1187–1191. PubMed 28805522 ❐
ABSTRACT
The PACE trial set out to discover whether cognitive behaviour therapy and graded exercise therapy are safe and effective forms of treatment for myalgic encephalomyelitis/chronic fatigue syndrome. It concluded that these interventions could even result in recovery. However, patient evidence has repeatedly found that cognitive behaviour therapy is ineffective and graded exercise therapy can make the condition worse. The PACE trial methodology has been heavily criticised by clinicians, academics and patients. A re-analysis of the data has cast serious doubts on the recovery rates being claimed. The trust of patients has been lost. The medical profession must start listening to people with myalgic encephalomyelitis/chronic fatigue syndrome if trust is going to be restored.
- Booth J, Moseley GL, Schiltenwolf M, et al. Exercise for chronic musculoskeletal pain: A biopsychosocial approach. Musculoskeletal Care. 2017 12;15(4):413–421. PubMed 28371175 ❐
- Lagerman P. Reasoning exercise dosage for people with persistent pain. In Touch. 2018 Autumn;(164):30–35. PainSci Bibliography 52992 ❐ “Incorporating a measure such as the SUDS exchange the word “pain” for the word “distress,” thus considering the wider psychosocial factors that so commonly accompany the postural, structural, and biomechanical aspects of persistent pain.”
- Staud R, Robinson ME, Weyl EE, Price DD. Pain variability in fibromyalgia is related to activity and rest: role of peripheral tissue impulse input. J Pain. 2010 Dec;11(12):1376–83. PubMed 20451465 ❐
Does activity help fibromyalgia or make it worse? Is rest necessary? Maybe a combination of both is the best answer? This is a study of the effects of alternating exercise with rest on 34 FM patients and 36 age-related healthy controls. Strenuous activity was reported as painful for most FM patients, but overall “clinical pain consistently decreased during the rest periods.” Their conclusions:
Alternating strenuous exercise with brief rest periods not only decreased overall clinical pain of FM subjects but also their mechanical hyperalgesia. No prolonged worsening of overall FM pain and hyperalgesia occurred despite vigorous muscle activity. Our findings contribute further evidence that FM pain and hyperalgesia are at least partially maintained by muscle impulse input, and that some types of exercises may be beneficial for FM.
- Nijs J, Kosek E, Van Oosterwijck J, Meeus M. Dysfunctional endogenous analgesia during exercise in patients with chronic pain: to exercise or not to exercise? Pain Physician. 2012 Jul;15(3 Suppl):ES205–13. PubMed 22786458 ❐
Exercise is great medicine for many chronic pain conditions, but there is an important “but”: it’s unclear if it’s a Band-Aid or if it actually “has positive effects on the processes involved in chronic pain (e.g. central pain modulation).” This narrative review concludes that it’s complicated and it depends, and some patients definitely have a “dysfunctional response” to exercise, and thus “exercise therapy should be individually tailored with emphasis on prevention of symptom flares.”
- Hooten WM, Qu W, Townsend CO, Judd JW. Effects of strength vs aerobic exercise on pain severity in adults with fibromyalgia: A randomized equivalence trial. Pain. 2012 Apr;153(4):915–23. PubMed 22341565 ❐
People with fibromyalgia, and many other forms of chronic pain, often benefit from exercise. But what works better: strength training or aerobics? In these fibromyalgia patients, both types of exercise were effective: “This study found that strength and aerobic exercise had equivalent effects on reducing pain severity among patients with fibromyalgia.”
- Andrade A, de Azevedo Klumb Steffens R, Sieczkowska SM, Peyré Tartaruga LA, Torres Vilarino G. A systematic review of the effects of strength training in patients with fibromyalgia: clinical outcomes and design considerations. Adv Rheumatol. 2018 Oct;58(1):36. PubMed 30657077 ❐
This is a systemic review of 22 studies of strength training for fibromyalgia which found that there is evidence of benefit that several weeks of moderate strength training will reduce pain, fatigue, depression, and anxiety. This is a rare example of a review that doesn’t have a “garbage in, garbage out” problem: the evidence may actually be adequate! Imagine.
That said, we have to overlook the fact that the reviewers respected “tender points” as a diagnostic criteria… almost a decade after they’ve been eliminated from the official criteria (see Wolfe).
- Ellingson LD, Stegner AJ, Schwabacher IJ, Koltyn KF, Cook DB. Exercise Strengthens Central Nervous System Modulation of Pain in Fibromyalgia. Brain Sci. 2016 Feb;6(1). PubMed 26927193 ❐ PainSci Bibliography 53576 ❐ “…exercise appeared to stimulate brain regions involved in descending pain inhibition in FM patients, decreasing their sensitivity to pain. Thus, exercise may benefit patients with FM via improving the functional capacity of the pain modulatory system.”
- Hyland ME, Hinton C, Hill C, et al. Explaining unexplained pain to fibromyalgia patients: finding a narrative that is acceptable to patients and provides a rationale for evidence based interventions. Br J Pain. 2016 Aug;10(3):156–61. PubMed 27583142 ❐ PainSci Bibliography 53579 ❐
In the case of FM, the aim of the ‘body reprogramming’ psychoeducational group programme is to empower patients to teach their bodies messages that can be learned only through experience. The two principal messages are as follows:
- The world they live in is a safe place – where actions never lead to stop signals and in particular the stop signal of danger (e.g. movement does not equate to danger). Interventions include relaxation (e.g. mindfulness) and slow graded exercise, but with an emphasis on combining physical movement with a positive mental state.
- The world they live in is a good place – where actions are rewarding as well as being health promoting. Interventions include strategies for reducing negative cognitions and promoting positive cognitions, with an emphasis on behaviour change so as to produce a more rewarding and health promoting lifestyle.
The body ‘learns’ these therapeutic messages through a combination of physical exercise and psychological techniques that are individualised and consistent with evidence based techniques
- Wang C, Schmid CH, Rones R, et al. A randomized trial of tai chi for fibromyalgia. N Engl J Med. 2010 Aug;363(8):743–54. PubMed 20818876 ❐
The study, funded by The National Center for Complementary and Integrative Health, shows that taiji has some beneficial effects for fibromyalgia patients. However, there’s nothing the least bit mystical about that, and it has no business being presented like a victory for “alternative” medicine. This is interesting in itself, but it is also the second embarrassing example of this in the New England Journal of Medicine (see Berman). See Dr. David Gorski’s detailed analysis: Tai chi and fibromyalgia in the New England Journal of Medicine.
- For many people, the mysticism and ritual of exercise like taiji, yoga, and meditation is big a turn off, not a selling point. Read more about the tyranny of yoga and meditation.
- A little proactive defence against pedantry: “Begs the question” originally referred to a logical fallacy in which an assertion tries to support itself, often just by re-phrasing it (“God exists because God is everywhere,” which “begs the question” that has not actually been answered). Pedants are often outraged by the looser modern usage, which means more what it sounds like: a question seems obvious or needful. Neglect of the old meaning for decades has tipped the scales so far towards the new meaning that resistance is futile: I side with Merriam Webster in relegating the original meaning to a formal, secondary sense of the term. The new meaning is clearer.
- Rhee JM, Shamji MF, Erwin WM, et al. Nonoperative management of cervical myelopathy: a systematic review. Spine (Phila Pa 1976). 2013 Oct;38(22 Suppl 1):S55–67. PubMed 23963006 ❐
- Upper cervical instability involves loss of integrity in a critical ligament in the upper spine. If you flex too much, the consequences are severe: a spear of vertebral bone digs into the spinal cord, causing violent disorientation and nausea, or even death in extreme cases. People with this condition have little choice but to avoid neck flexion! It can be surgically repaired, but it’s a serious operation, and many patients choose to avoid that. So they’re either avoiding neck flexion or surgery, making it a more or less perfect analogy to the PC3 question … just with a much clearer risk.
- There are some classic signs of myelopathy that a neurologist can assess, and some that anyone might notice (e.g. really sensitive tendon reflexes, missing gag reflex). But their absence isn’t a deal-breaker: the PC3-fibromyalgia link is based on the idea that there is not any frank myelopathy, just subtle symptoms (like the unusual phenomenon of dysautonomia). If there was relatively obvious myelopathy, it wouldn’t be much of a clinical puzzle! It would just be diagnosed as myelopathy, one would hope. So the absence of clinical signs of myelopathy would be any kind of a deal-breaker for this particular diagnosis. But if they were present, that really boosts the diagnostic confidence that there is serious organic trouble with a spinal cord.
- Gordji-Nejad A, Matusch A, Kleedörfer S, et al. Single dose creatine improves cognitive performance and induces changes in cerebral high energy phosphates during sleep deprivation. Sci Rep. 2024 Feb;14(1):4937. PubMed 38418482 ❐ PainSci Bibliography 49735 ❐
“Tendinitis” versus “tendonitis”: Both spellings are acceptable these days, but the first is the more legitimate, while the second is just an old misspelling that has become acceptable only through popular use, which is a thing that happens in English. The word is based on the Latin “tendo” which has a genitive singular form of tendinis, and a combining form that is therefore tendin. (Source: Stedmans Electronic Medical Dictionary.)
“Tendinitis” vs “tendinopathy”: Both are acceptable labels for ticked off tendons. Tendinopathy (and tendinosis) are often used to avoid the implication of inflammation that is baked into the term tendinitis, because the condition involves no signs of gross, acute inflammation. However, recent research has shown that inflammation is actually there, it’s just not obvious. So tendinitis remains a fair label, and much more familiar to patients to boot.
- Bäckryd 2017, op. cit.
- Zwaag J, Naaktgeboren R, van Herwaarden AE, Pickkers P, Kox M. The Effects of Cold Exposure Training and a Breathing Exercise on the Inflammatory Response in Humans: A Pilot Study. Psychosom Med. 2022 May;84(4):457–467. PubMed 35213875 ❐ PainSci Bibliography 52067 ❐
This fascinating experiment put dozens of healthy young male subjects through days of intense hyperventilation exercises and cold exposure, and then “poisoned” them with injections that caused substantial systemic inflammation. The effect of the poisoning was clearly attenuated by hyperventilation alone, and somewhat more so when combined with cold exposure. This was essentially a test showing that the Wim Hof Method is indeed anti-inflammatory … but also that the whole cocktail probably isn’t necessary, and in particular the cryotherapy isn’t necessary — just the relatively simple and easy hyperventilation exercises are probably the only “active ingredient” you need.
- The “endotoxemia” that Zwaag et al. induced in their brave subjects is a decent stand-in for the kind of inflammation we see in many sick patients with chronic pain, most notably those with autoimmune diseases like rheumatoid arthritis, and it might even be a particularly good proxy for whatever goes wrong in people with fibromyalgia and ME/CFS. For instance, it may specifically induce neuroinflammation, which is a the kind of inflammation that causes “illness behaviour” — feeling fragile and exhausted.
- Hyperventilation and cold exposure are both potentially dangerous if done recklessly, so please exercise some caution and experiment cautiously. If you'd like to experiment, I suggest you start with a couple daily sessions, and each session includes three sets of forty fast, deep breaths while seated or lying down — just enough to get you somewhat light-headed. Take a minute or two to recover between sets, just like doing sets of exercises at the gym. If you get too light-headed, just slow down and stop. For bonus points, take a cool to cold shower between sets or to finish the session. If cold seems too hard, try starting with the coolest you can easily tolerate and then bump it down a couple degrees.
- Walitt B, Klose P, Fitzcharles MA, Phillips T, Häuser W. Cannabinoids for fibromyalgia. Cochrane Database Syst Rev. 2016 Jul;7:CD011694. PubMed 27428009 ❐ PainSci Bibliography 52139 ❐
This is a 2016 review of… hang on a sec, am I reading this right?•rubs eyes, blinks• Just two trials? Oh dear. Two small trials of 32 and 40 subjects. I have never seen a review of just two trials before, but I suppose it’s technically the minimum to be considered a review!
Both studies used nabilone, which is a synthetic cannabinoid. The results were rotten: it didn’t work, and it had a lot of side effects: “We found no convincing, unbiased, high quality evidence suggesting that nabilone is of value in treating people with fibromyalgia. The tolerability of nabilone was low in people with fibromyalgia.”
Alrighty then! For whatever it’s worth.
The actual story here is that cannabis for fibromyalgia hasn’t really been studied. (Nabilone barely counts, even if it was 20 studies.)
- Kurlyandchik I, Tiralongo E, Schloss J. Safety and Efficacy of Medicinal Cannabis in the Treatment of Fibromyalgia: A Systematic Review. J Altern Complement Med. 2020 Dec. PubMed 33337931 ❐
- Stretching is not a pillar of fitness: it isn’t a good warm-up, and it doesn’t enhance peformance, and it won’t prevent or treat soreness or injury. But it can cause injuries, and it can impair performance (slightly). It will boost flexibility, for whatever that is worth — which is surprisingly little (even for most athletes). Many major muscles are just mechanically impossible to stretch in the first place. Stretch might help some kinds of pain, like muscle pain, but stretching is clearly not of much help to most chronic pain patients. There is no “advanced” stretching method that overcomes any of these limitations, but you can spend a lot of money on books and courses and certifications — stretching is surprisingly big, snake oil. But, yes, it does feel good. See Quite a Stretch: Stretching science has shown that this extremely popular form of exercise has almost no measurable benefits.
- Støve MP, Magnusson SP, Thomsen JL, Riis A. Efficacy of a novel home-based stretching program on fibromyalgia symptoms: a randomised controlled trial. Arch Phys Med Rehabil. 2026 Jun:S0003–9993(26)00747–1. PubMed 42242521 ❐ PainSci Bibliography 49278 ❐
This trial cannot separate the effect of stretching from the effects of expectancy, novelty, and weekly contact with a caring researcher, yada yada yada — an especially glaring problem with fibromyalgia, where patients are starved for validation. Participants weren’t blinded either, so the waitlisted group results were probably deflated by disappointment (“frustrebo” effect, performance bias), widening the artifactual gap further. All of this has happened before, like with massage for fibromyalgia.
The authors acknowledge this problem, but they seriously understate how decisively it sabotages the experiment:
“the waitlist design may have induced expectancy asymmetry and limited causal inference compared with an active comparator”
This is like saying that eating potato salad left in the sun for an afternoon may induce facilitated fecal transit. The waitlist design definitely broke the experiment.
- If stretching actually did anything, it would have been added to the predictable effect of therapist attention, resulting in results that were downright impressive instead of modest. In other words, even though this study was doomed to give stretching an unfair advantage, it still couldn’t produce anything better than a modest benefit — and that’s actually a backwards form of negative evidence.
- Sutherland AM, Clarke HA, Katz J, Katznelson R. Hyperbaric Oxygen Therapy: A New Treatment for Chronic Pain? Pain Pract. 2016 06;16(5):620–8. PubMed 25988526 ❐
- Efrati S, Golan H, Bechor Y, et al. Hyperbaric oxygen therapy can diminish fibromyalgia syndrome--prospective clinical trial. PLoS One. 2015;10(5):e0127012. PubMed 26010952 ❐ PainSci Bibliography 53581 ❐
- Bastian H. "They would say that, wouldn't they?" A reader's guide to author and sponsor biases in clinical research. J R Soc Med. 2006 Dec;99(12):611–4. PubMed 17139062 ❐ PainSci Bibliography 51373 ❐
The full quote:
“A promising treatment is often in fact merely the larval stage of a disappointing one. At least a third of influential trials suggesting benefit may either ultimately be contradicted or turn out to have exaggerated effectiveness.”
- Tirelli U, Cirrito C, Pavanello M, et al. Ozone therapy in 65 patients with fibromyalgia: an effective therapy. Eur Rev Med Pharmacol Sci. 2019 Feb;23(4):1786–1788. PubMed 30840304 ❐
- Hidalgo-Tallón 2013, op. cit.
- Goebel A, Krock E, Gentry C, et al. Passive transfer of fibromyalgia symptoms from patients to mice. J Clin Invest. 2021 Jul;131(13). PubMed 34196305 ❐ PainSci Bibliography 52110 ❐
This study tested whether antibodies in the blood of fibromyalgia (FMS) patients could be causing symptoms of the disease. Researchers purified a type of antibody (IgG) from the blood of people with fibromyalgia and injected it into healthy mice. The mice that received fibromyalgia IgG developed signs and symptoms similar to fibromyalgia symptoms in humans, including increased sensitivity to pressure and cold, reduced activity, decreased grip strength, and loss of small nerve fibers in the skin.
In contrast, mice injected with IgG from healthy people—or with serum from fibromyalgia patients that had the IgG removed—did not show these effects.
The study found that these antibodies appear to affect sensory nerve cells outside the spinal cord, specifically in the dorsal root ganglia (DRG). The antibodies did not seem to cause general inflammation or affect neurons in the brain or spinal cord.
This result implies that fibromyalgia could be autommune in nature, but falls well short of proving it. Fibromyalgia is mostly thought of as a disorder of central nervous system sensitization, not an autoimmune disease. This study challenges that view, and, if replicated, could support a shift in thinking toward immune involvement. But that shift is still tentative, and as of 2025 there is still no replication — although there is a weirdly similar study showing that fibromyalgia also follows transplanted bowel bacteria! See Cai.
Other limitations: it was an animal study, and of course, results in mice do not always translate to humans. The sample sizes were modest. The researchers did not find a common antibody target (autoantigen) across patients, making it unclear exactly what the antibodies are binding to.
One author (David A. Andersson) received research support from Eli Lilly, a pharmaceutical company that sells drugs for fibromyalgia.
- Cai W, Haddad M, Haddad R, et al. The gut microbiota promotes pain in fibromyalgia. Neuron. 2025 Jul;113(13):2161–2175.e13. PubMed 40280127 ❐
Gut fauna may contribute to the pain experienced in fibromyalgia. Cai et al. transplanted fecal matter — bowel bacteria, basically — from women with fibromyalgia into mice, which basically gave them fibromyalgia (heightened sensitivity to pressure, heat, and cold, along with signs of muscle and spontaneous pain. Control mice were given microbiota from healthy women, and they were fine.
The mice also changed physiologically: more inflammatory markers, altered bile acid metabolism, and hyperactive microglia (immune cells in the nervous system).
The team also conducted a small open-label clinical trial in 14 women with severe fibromyalgia, giving them gut microbiota from healthy donors. Most felt better. But without a placebo comparison, the results are good “only” for inspiring more rigorous experiments.
Although the authors reported no conflicts of interest, studying the microbiome is complex and full of opportunities to "find" what researchers want to find.
This was weirdly similar to a 2021 study by Goebel showing the same thing with transplanted blood rather than poop.
For a more colourful and detailed exploration of this study, see the blog post, “Poop of pain: fibromyalgia follows fecal matter.”