Does Ultrasound or Shockwave Therapy Work?
They seem like mainstream physical therapies, but warming and vibrating tissues with sound/pressure waves has never been supported by good evidence

The pressure wave therapies are huge in physical therapy: both ultrasound therapy (US) and extracorporeal shockwave therapy (ESWT) are used to treat pain and injuries like plantar fasciitis, stress fractures, muscle strains, or runner’s knee.
Therapeutic ultrasound has been one of the staples of musculoskeletal medicine and manual therapy since the 1950s.12 It is of several major examples of “passive” therapies that are done to a patient. It is still widely used in mainstream physical therapy clinics today. You can buy your own DIY ultrasound machine at the drugstore.
It’s fancier and more potent cousin, shockwave therapy, has been steadily replacing it in the 21st Century.
Shockwave therapy is ultrasound… reborn!
Although ultrasound and shockwave therapy are different … are they really? All their variants are used in the much same ways for mostly the same conditions. They are all vibration delivery systems, intended to stimulate or even damage tissue — which might, depending on the details, induce regenerative and anti-inflammatory effects in injured bone, cartilage, and tendon. They belong to a family of vibration therapies with massage guns, jacuzzis, and vibrating exercise platforms, all very similar in spirit.
Most people and professionals assume that all of this is good technology, proven medicine — but that just doesn’t seem to be the case. Although there are some interesting exceptions and tantalizing hopes for some conditions, neither ultrasound nor shockwave therapy are good evidence-based medicine. There is a jarring, bizarre lack of quality research for such mainstream treatment modalities, and the results are not encouraging. At best, it’s complicated and unreliable. At worst, there is just no rational basis for hitting tissues with pressure waves at all, and it’s all just modern snake oil. Shockwave therapy is routinely marketed along with much more blatant kinds of quackery — which reveals its true nature.
Ultrasound and shockwave therapy are probably useful for some patients, some of the time — with just-right settings and variables that have never actually been confirmed by research, and little hope that they will be any time soon. Meanwhile, they enjoy far more credibility than they deserve.
I do not like the principle of using magic machines to treat.
“Nari,” physical therapist, in an internet forum discussion
Ultrasound versus shockwave
Shockwave therapy is often considered a new kind of ultrasound, but shockwave therapy isn’t “ultra” sound — it’s infra!
Also not actually “sound.”
Ultrasound uses high-frequency sound waves, above the range of human hearing (> 20,000 Hz) — which vibrates tissue so quickly that it warms up from the friction, like a gentle microwave. The point of ordinary therapeutic ultrasound is that it’s like a heating pad with a more penetrating warmth. It’s mostly a “heat ray.” It’s cheap, ubiquitous, harmless … and mostly useless.
Shockwave therapy is, weirdly, much more like a powerful vibrating massage “gun.” Its pressure waves are slow but high-energy, smacking the tissue hard, at frequencies in the infrasound range, well below the range of human hearing (< 20 Hz). And yet shockwaves aren’t technically “sound” waves: they are high-energy pulses of pressure rather than continuous oscillations, like sharp mountains rather than rolling hills. This produces much more potent “stimulation,” strong enough to shatter calcifications, and cause micro-injuries that might “kickstart” healing. This is much more expensive than ultrasound, and often painful.
So if the vibrations of ultrasound are like an electric toothbrush …
Shockwave therapy is a jackhammer.
That difference matters — you can certainly feel it — and nd yet shockwaves are *also* “mostly useless” clinically, as I will show below. It’s all just playing with the parameters of pressure waves to stimulate tissue in different ways.
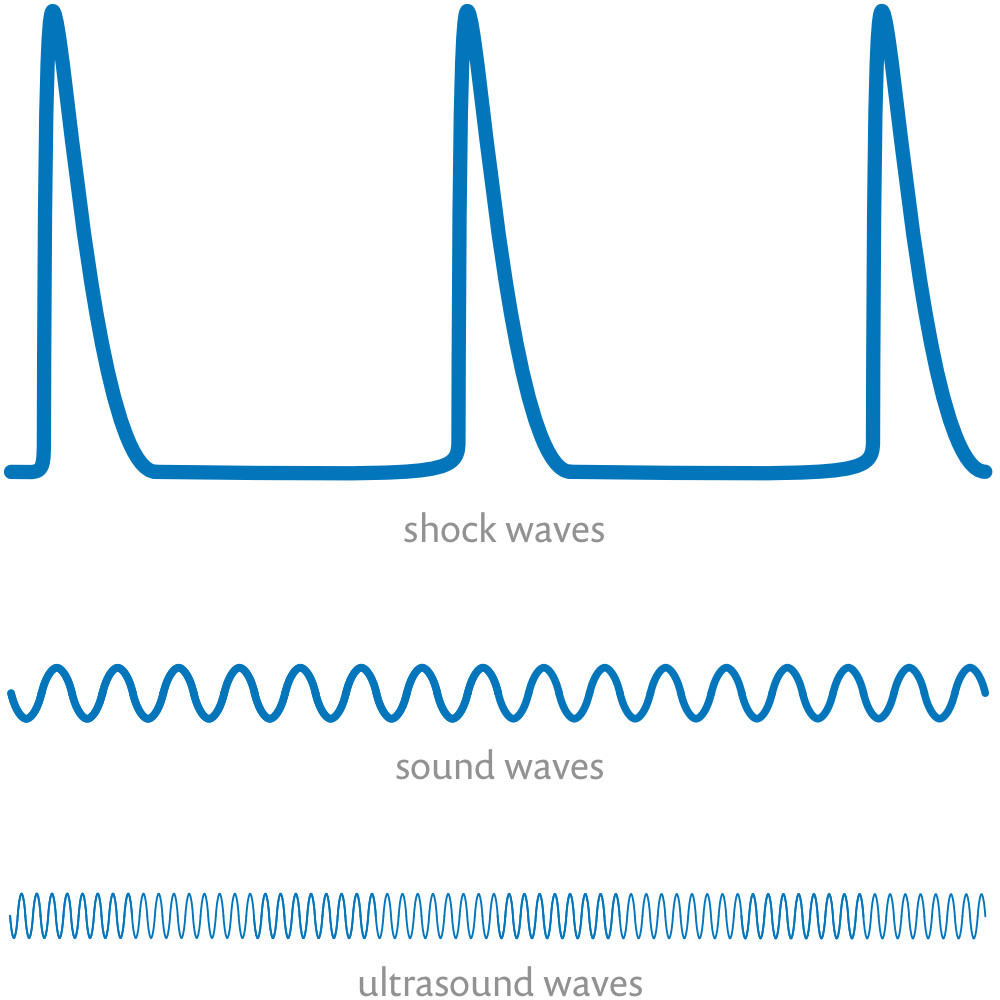
A schematic contrasting the overall shape of shock waves, sound waves, and ultrasound waves … not to scale! Ultrasound waves are dramatically more frequent that shock waves, or even low-frequency sound waves: you might only get a few big shock waves per second, but ultrasound machines will pump out more than 20-30 thousand much smaller sound waves in the same second! Any properly scaled diagram that shows one of them clearly will render the other effectively invisible.
The lack of science about ultrasound and shockwave therapy
When I started studying for this article — back in the mid-2000s! — I was surprised by how little there was to study. I had not yet learned that there’s not enough evidence about anything to do with injury rehab and chronic pain rehab.
Back then, every scientific paper about ultrasound pointed out there was not enough research on this topic, or at least not enough good research.
That hasn’t changed. We’re still starving for decent evidence as of 2024, and I think that will be a safe summary until at least 2030.
For instance, a 2015 paper about ultrasound for rotator cuff tendinopathy found only six trials, all poor quality. A big 2020 review of ultrasound for back pain found just 10 trials, and was scathingly critical of their quality: all bad! “The certainty of the evidence for all outcomes was very low.” And so on, with no real improvement since. (These and many other citations coming up below.)
That’s not a lot to go on, and it’s saldy typical for the field of pain treatment and injury rehab. But the poverty of evidence for this topic is a bit shocking. We’re talking about ultrasound, here: one of the staples of physical therapy. Hardly a fringe treatment. It practically defines the experience of going to a physiotherapist. Everyone has had that cold gel slapped on an injury, and felt that tingling, penetrating … placebo?
Ultrasound and shockwave therapy are pseudo-quackery
There’s a troubling disconnect between the popularity of these therapeutic modalities and the near total lack of good research. A handful of good quality studies is a joke for therapies that are worth billions in the marketplace, something sold to countless pro athletes over the decades. How can that much therapy be sold for so long without a satisfactory body of evidence that it works? Bizarre!
It is bizarre, but it’s also almost … standard.
Ultrasound and shockwave are just among the best of many other examples of “pseudo-quackery” — popular treatments that aren’t obvious quackery, but still fall well short of being evidence-based medicine, are sold with excessive confidence, and are usually considered mainstream rather than alternative.
This does not mean that US never works for anyone. It does mean that it has been prescribed and sold to patients for decades with unjustified confidence, often with the mistaken belief that there is much more evidence than there is. And that is not cool!

Therapeutic ultrasound
Ultrasound uses high-frequency sound waves, and is familiar to almost anyone who’s had any kind of physical therapy in the last fifty years… and certainly anyone who had it before 2010. Although still widely available in clinics, and on drugstore shelves, ultrasound is slowly dying out, increasingly replaced by shockwave therapy. Some ultrasound basics:
- Garden-variety therapeutic US is cheap and available everywhere. There are many consumer ultrasound products, some of them quite cheap and small.
- Treatment is brief and painless, even at high intensities, and is applied to almost all common musculoskeletal problem — almost indiscriminately, really.
- Healthy young adults can hear sounds up to about 20,000 hertz. Ultrasound machines produce sound waves at even higher frequencies. The slowest ultrasound might be just audible as a faint mosquito whine to a young patient with exceptional hearing.
- Those sound waves can be low or high intensity, but all of it is low intensity compared to shockwave therapy.
- Deep heating is the main point of ultrasound. Vibrating the molecules of tissue causes diffuse friction and therefore warmth, and sound waves can vibrate deep tissues — as opposed to the superficial heat provided by a heating pad.
- At high enough frequencies and energies, ultrasound can actually burn you! Fortunately, this is quite rare in a physical therapy context.
- Ultrasound also has "mechanical" effects, which can be thought of as "micro massage" — basically just moving tissue fluids and gasses. But not far!
- Ultrasound can be pulsed to minimize warming. This is almost literally just turning the thing off and on again, which prevents heat from building up.
- Low-intensity pulsed ultrasound (LIPUS) is a significant variant of ultrasound, mostly used (rather speculatively) to promote bone healing.
The dubious rationale for ultrasound
The big idea is — this will blow your mind! — that cells and tissues respond “well” to being shaken (not stirred). In theory, ultrasound works by vibrating tissues back to health, which sounds like something you’d hear on an infomercial, or the Dr. Oz Show. What, exactly, does vibration do to tissues? Does anyone actually understand it?
No!
In 2001, Physical Therapy published a review of the biological effects of ultrasound. More than ten years earlier, the authors — Baker, Robertson, and Duck — explained that it had already been at least two decades since it was first pointed out that “physical therapists tended to overlook the tenuous nature of the scientific basis for the use of therapeutic ultrasound.”3 They also point out — it’s the point of their whole paper — that the situation had not improved in the twenty years before 2001:
The frequently described biophysical effects of ultrasound either do not occur in vivo under therapeutic conditions or have not been proven to have a clinical effect under these conditions. This review reveals that there is currently insufficient biophysical evidence to provide a scientific foundation for the clinical use of therapeutic ultrasound …
So this was already an old problem in 2001.
There is lots of interesting ultrasound biology to consider, and scientists may eventually nail down effects that might be the basis for new evidence-based therapies. For instance, a decade later, Tsai et al. declared that “There is strong supporting evidence from animal studies about the positive effects of ultrasound on tendon healing”4 — but animal studies are notoriously misleading, and they certainly can’t justify the use of ultrasound (especially when US has already been tested on human tendinopathy with underwhelming results).
Another great example: the persistent hope that rattling cells might speed the healing of bone fractures, particularly low intensity pulsed ultrasound (LIPUS). Such an effect, if proven, would certainly be a fascinating bit of weird good news. Unfortunately, it is probably dis-proven. In 2017, the British Medical Journal published an excellent review with a very negative conclusion for fresh fractures.5 However, the authors have to concede that “the applicability to other types of fracture or osteotomy is open to debate … ” because it’s impossible to know for sure that there are no black swans anywhere — one could be right around the corner!
But the negative conclusion was echoed in another review in 2023.6 The report that “few studies” even reported on patient outcomes. “It is probable that LIPUS makes little or no difference to delayed union or non‐union.” It’s also noteworthy that they only found a single test of shockwave therapy, and none at all of high-intensity ultrasound.
Meanwhile, there is still just no basis for thinking that ultrasound has a basis. The entire empire of ultrasound rests on the single, oversimplified idea that “stimulation is good” and the hope that we might someday figure out exactly why.
The state of the evidence for ultrasound
In most cases I consider ultrasound less than useless — that's 8-10 minutes wasted that could be used doing something that might actually help.
Jason Silvernail, DPT, Board-Certified in Orthopedic Physical Therapy, in an internet forum discussion
Ultrasound is an easy treatment to test scientifically.7 Just compare results in patients who received real ultrasound to patients who get a fake instead! And yet there are just a few dozen such experiments (controlled by a sham) in the scientific literature, and even most of them are still rather flawed. Conclusions from evidence reviews like this one from van der Windt et al. are typical:
As yet, there seems to be little evidence to support the use of ultrasound therapy in the treatment of musculoskeletal disorders. The large majority of 13 randomized placebo-controlled trials with adequate methods did not support the existence of clinically important or statistically significant differences in favour of ultrasound therapy.
van der Windt et al., 1999, Pain
Did not support the “existence of”? Ouch! Ultrasound’s therapeutic effect has an existential crisis.
Several reviews give a nod towards some ray of hope. For instance, van der Windt et al., despite their overwhelmingly negative conclusion, also noted that “findings for lateral epicondylitis [tennis elbow] may warrant further investigation.” But, naturally, that optimism about tennis elbow is contradicted by other studies.8 The science is mostly a discouraging, unimpressive mess — a classic case (yet another one) of a damning failure to impress.
| van der Windt 19999 | musculoskeletal disorders | strongly negative review of 13 “adequate” trials did not support “the existence” of therapeutic effects |
| Robertson 200110 | pain and injury | “little evidence” of therapeutic benefit in 10 “acceptable” trials out of 35 candidates; 2 positive trials, 8 negative |
| Baker 200111 | biological effects | “insufficient biophysical evidence” to justify therapeutic use for pain and injury |
| Buchbinder 200612 | tennis elbow | nine studies produced “platinum” level (better than gold!) evidence of “little or no benefit” (for ESWT) |
| Ho 200713 | tennis elbow | conflicting, “unconvincing” evidence of efficacy from a few trials (of ESWT again) |
| Ho 200714 | rotator cuff tendinopathy | limited evidence “supports … ESWT for chronic calcific rotator cuff tendinitis,” but no non non-calcific |
| Rutjes 201015 | osteoarthritis of knee | a positive update to a previously negative review, which is strange because it’s based on just 5 small, poor quality trials with trivial “positive” results |
| Shanks 201016 | lower limb conditions | inconclusive review of 10 of 15 candidates: “no high quality evidence available” |
| van den Bekerom 201117 | ankle sprains | inconclusive but discouraging review of “five small placebo-controlled trials”; the “potential treatment effects of ultrasound appear to be generally small” |
| Page 201318 | carpal tunnel syndrome | inconclusive but slightly encouraging review of “only poor quality evidence from very limited data” from 11 trials |
| Desmeules 201519 | rotator cuff tendinopathy | negative review “does not provide any benefit … based on low to moderate level evidence” from 11 weak trials |
| Ebadi 202020 | chronic low back pain | inconclusive and underwhelming review of 10 little trials, none of them good quality |
The scientific bottom line on therapeutic ultrasound
Standard therapeutic ultrasound probably does little or nothing for most people and conditions. A sliver of hope remains that some specific conditions will respond to ultrasound with just the right settings.
Therapeutic ultrasound … has fallen out of favor as research has shown a lack of efficacy and a lack of scientific basis for proposed biophysical effects.
Baker et al., 2001, Physical Therapy
Except it hasn’t fallen out of favour! It’s still widely used. The only professionals it’s fallen out of favour with, I imagine, are a small minority of scientists and unusually alert clinicians.
Patient cynicism about therapeutic ultrasound
There is nothing a cold slimy prickling ultrasound wand can do that a pair of warm hands can’t do way better.
If only I had a buck for every time a patient or reader has told me that they are skeptical about “that ultrasound thing they always do to you at physiotherapy”!
Patients often express irritation with a common physical therapy business model: working with several patients at once, rotating between rooms or beds, often leaving patients with passive therapies (like a moist hot pack from a hydrocollator — nice enough, but worth a steep fee?) Many patients often go a step further and complain specifically about ultrasound and TENS, skeptical that these treatments really do anything.21
And so few patients are singing the virtues of standard US. It not only fails to generate testimonials, but actually generates many annoyed antimonials.
Patients do not (yet) feel the same cynicism about shockwave therapy. As a more expensive and painful medicine, ESWT is a hope-generating machine. Having spent their hard-earned dollars and endured the discomfort of treatment, patients are more subject to expectation effects (placebo) — and much less willing to entertain the possibility that it was all a waste. At this stage in their quest to feel better, more people will report ambiguous results if they were positive (“Yeah, I think it did some good!”), and even negative reports will often be toned down (“I didn’t seem to get that much out of it, but I guess it works really well for some people.”) This could go on for years.
Shockwave therapy

Super-duper ultrasound
ESWT is high tech. The main differences for the patient? It ain’t cheap, and it’s much more intense.
Extracorporeal Shock Wave Therapy (ESWT) is often shortened to just “shockwave therapy, because “extracorporeal” just means “generated outside the body,” which seems obvious — you don’t swallow it, and it’s not a surgical implant.22 It looks almost exactly like ultrasound: a gadget that you pass over an injury like a magic wand. But it’s the more-is-better cousin of therapeutic ultrasound, so it’s more intense, more technologically impressive, and more expensive.23 Radial “shock” wave therapy is a common variant with lower-energy waves.24
Shockwave therapy generates much lower frequency, faster pressure waves than ultrasound. Those waves slap tissues with much higher energy than ultrasound: the travel much faster than the speed of sound (in flesh), about 1500 meters per second.
They also come at a leisurely tempo that you could almost dance to — mostly under 10 Hz, thousands of times lower than ultrasound. In fact, five shockwaves per second (5 Hz) is quite a bit slower than tap dancing, which can get up to about 18 Hz! But that is way below the range of human hearing, which starts around 20 Hz. So shockwave therapy is closer to infrasound than ultrasound.25
Shockwaves also aren’t technically “sound” waves: they are high-energy pulses of pressure rather than continuous oscillations, like sharp mountains rather than rolling hills.
Adding injury to injury: shockwave therapy’s big idea
It’s not clear why kidney-stone smashing tech was adopted by physical therapy. Why “slap tissues with much higher energy than ultrasound”? What’s the point? This section is all about shockwave therapy’s Big Idea, the reason that you can supposedly gain from that pain: damage is healing. 🤯 Maybe you can microtraumatize yourself back to health, “kickstart” healing, induce some therapeutic biological effects.
There are two main differences in how ultrasound and shockwave therapy “stimulate” tissue:
- Shockwaves are too slow for thermal effects, but ultrasound is literally warming, and can even cause burns — but this is never done deliberately.
- But shockwaves can cause physical trauma, which ultrasound cannot do — and this is done deliberately. (They can also break up calcifications, which is the technology’s original claim to fame: it can smash kidney stones. But this ability is of much less certain value in musculoskeletal medicine.)
Maybe that damage is like exercise: a slightly stressful stimulus that the body can respond to constructively.
This section critically analyzes the principles of shockwave therapy. It’s all a bit nerdy, and so it’s for PainSci members only, about 1800 words. It includes an audio version.
Most PainScience.com content is free and always will be.? Membership unlocks extra content like this for USD $5/month, and includes much more:
Almost everything on PainScience.com is free, including most blog posts, hundreds of articles, and large parts of articles that have member-areas. Member areas typically contain content that is interesting but less essential — dorky digressions, and extra detail that any keen reader would enjoy, but which the average visitor can take or leave.
PainScience.com is 100% reader-supported by memberships, book sales, and donations. That’s what keep the lights on and allow me to publish everything else (without ads).
- → access to many members-only sections of articles +
And more coming. This is a new program as of late 2021. I have created twelve large members-only areas so far — about 40,000 words, a small book’s worth. Articles with large chunks of exclusive content are:
- Quite a Stretch
- Does Epsom Salt Work?
- Heat for Pain and Rehab
- Your Back Is Not Out of Alignment
- Trigger Point Doubts
- Does Fascia Matter?
- Anxiety & Chronic Pain
- Does Massage Therapy Work?
- Does Posture Matter?
- A Deep Dive into Delayed-Onset Muscle Soreness
- Does Ultrasound or Shockwave Therapy Work?
- A Painful Biological Glitch that Causes Pointless Inflammation
- Guide to Repetitive Strain Injuries
- Chronic, Subtle, Systemic Inflammation
- Vitamins, Minerals & Supplements for Pain & Healing
- Reviews of Pain Professions
- Articles with smaller members sections (more still being added):
- → audio versions of many articles +
There are audio versions of five classic, big PainSci articles, which are available to both members and e-boxed set customers, or on request for visually impaired visitors, email me. See the Audio page. ❐
I also started recording audio versions of some blog posts for members in early 2022. These are shorter, and will soon greatly outnumber the audio versions of the featured articles.
- → premium subscription to the PainSci Updates newsletter +Sign-up to get the salamander in your inbox, 0–3 posts per week, mostly short, sometimes huge. You can sign-up for free and get most of them; members get more and their own RSS feed. The blog has existed for well over a decade now, and there are over a thousand posts in the library. ❐

Change or cancel plans any time. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism. For more information, see the membership page. ❐
PREVIEW: Headings in the members-only area…
- So crazy it might just work?
- The hormesis hope
- The role of “biological effects” in medical science
- Biological effects of shockwave therapy
- Potent therapy raises expectations
- Would you like to fry with that? The irrational double-standard for ultrasound versus shockwave
- You can’t kickstart a motorcycle that’s already running
- Mechanism masturbation par excellence
So crazy it might just work?
Adding injury to injury may seem perverse, but there is an intelligible and testable hypothesis here: that shockwaves have clinically useful biological effects, that their intensity can stimulate recovery, either speeding up normal healing, or — shockwave’s main claim to fame — giving a boost to healing that wasn’t already doing a good enough job for some reason.
Failed healing is a real thing: we don’t know why, but sometimes healing glitches like a bad robot. The best example is the awful phenomenon of fracture non-union, where the bones just do not knit. But that is also the only well known example. It’s possible that something similar but subtler can also happen to soft tissue injuries, but not actually known, let alone why.
Doing a little damage is supposedly a “kickstart” for stalled or insufficient healing, a signal to the body: Hey, do your job! Clean up this mess! This is why shockwave therapy is routinely called a “regenerative” therapy.
So now we have both a hypothesis about what’s wrong and a hypothesis about how to fix/improve it.
But most crazy ideas do not work. There are a lot of problems here.
The hormesis hope
“Hormesis” is the term for a familiar pattern in biology: something that is biologically beneficial at a small dose, even though a higher dose would be dangerous. This describes how exercise works, for instance: too much exercise is injurious, but less is very healthful.
The term can make damage-induced-healing sound more cromulent. And it is a seed of truth here … but it is probably inadequate. There is a major conceptual problem with invoking hormesis to explain the benefits of shockwave therapy.
Exercise leverages adaptive responses tuned by evolution, and hormesis simply reflects the common sensical reality that we can only adapt to so much of a stimulus. As long as we can adapt to it, it’s helpful. If it’s too much to adapt to, it’s dangerous.
Biology mostly evolves adaptations and responses to common and consequential natural stimuli, and will only respond to artificial ones insofar as they resemble the natural ones. A highly artificial passive stimulus like shockwave therapy — never encountered by any animal in the history of life, and not really resembling anything else — is unlikely to provoke a useful response. We are full of “mechanoreceptors” for detecting and responding to a great variety of physical stimuli, and it is not inconceivable that shockwaves could trigger a useful reaction … but it is far likely that cells will respond productively to being slapped by high energy pressure waves.
And then it’s yet another big leap to the hope that they will respond productively when they are already in trouble.
The role of “biological effects” in medical science
Biological effects are a dime a dozen. Cells will react to practically anything! If you slapped my face — and shockwave enthusiasts might be in the mood for that — my skin will redden. Slapping indubitably has biological effects. But they’re not therapeutic effects!
Just because cells react to a stimulus doesn’t make it clinically useful. And yet the reactions of cells can be studied in infinite detail, and can always easily be touted as maybe useful. Pair these very science-y findings with overconfident opinions about the “promising” clinical research, and the combination is highly seductive.
Half the output of biomedical science is devoted to churning out over-interpreted evidence of biological effects.
Biological effects of shockwave therapy
There are dozens of papers about the biological effects of shockwave therapy, science that will excite nerdy, explorative minds, because biology is still a fascinating wilderness. But it’s all half-baked.
Cells react to practically any stimulus … but is it a useful reaction?
“The underlying mechanism of action,” write Sokolakis et al. in 2019, “is mostly unclear and currently under investigation.” Nothing important is different in 2024: “there is no exact mechanism of shock wave therapy in the treatment of orthopedic disorders,” wrote Yazdani et al.
Even the researchers most responsible for shockwave hype acknowledged in 2018 that “the mechanism of action of ESWT remains unknown” … but Moya et al. then talk about those MOAs with scholarly excitement. It’s almost like they think they are indeed known, and that saying “unknown” was just performative humility!26
They quote four possible mechanisms, all first proposed in 1997 by Haupt: chondroprotective! angiogenic! anti-inflammatory! anti-apoptotic! Gosh!27 All their jargon can be reduced to the same plain English idea: shockwaves make cells dance … and supposedly in a useful way. According to the clinical research. According to Moya et al.
According to me? See below.
Potent therapy raises expectations
The strong sensations of shockwave therapy are probably rocket fuel for placebo. “Potency bias” is our tendency to assume that stronger medicines are better. We truly believe that there is no gain without pain, and we assume that pain is justified by gain.
A funny example: people love to love Buckley’s cough syrup, a notoriously foul-tasting Canadian “medicine” with no conventional active ingredients, just gross ones like lots of camphor and pine needle oil, advertised with the slogan, “It tastes awful. And it works.” That slogan taps directly into the pro-potency bias! It’s practically an explanation for it. People can’t love Buckley's because it’s actually effective, because it cannot possibly be, so they love it simply because the taste is horrifying … and they think intense medicines must be more potent. Surely no one would sell such diabolical swill if it wasn’t good medicine?! Right?
There are many sketchy no-pain-no-gain therapies that capitalize on the potency bias, a rogues gallery of “provocation therapies”: prolotherapy, dry needling, cupping, fascial therapy, “scraping massage” (e.g. Graston), and so on.
Even if it works, shockwave therapy is not from a great neighbourhood.
Would you like to fry with that? The irrational double-standard for ultrasound versus shockwave
Consider this weird contradiction: ultrasound’s thermal effects are definitely capable of causing internal burns, but no one ever acts like that’s a good idea. Why not?
Doing damage is not just acceptable in shockwave therapy, it’s the point. So why not in ultrasound? Other than the fact that “internal burns” is nightmare fuel, what’s the difference between tuning infrasound to cause slight mechanical damage versus tuning ultrasound to cause slight thermal damage? Damage is damage — you clearly don’t want too much of it, even if you do accept that just the right amount is “regenerative.”
Ultrasound damage is only ever considered a serious error, malpractice … but people pay for shockwave’s minor, diffuse, microtraumatizing powers? What a weird world.
You can’t kickstart a motorcycle that’s already running
And one more conceptual glitch with shockwave therapy: the reason most overuse injuries don’t heal is probably not because healing has “failed,” per se, but rather because it simply cannot keep up with the mechanical strain on the tissue. The healing is happening, but it feels like Lucy trying to keep up with the chocolates on the conveyor belt. Do you want to add more strain to that equation? Do you think that Lucy would do better with more chocolates?
And yet shockwave therapy is probably applied to overuse injuries more than any other kind of condition! And there’s probably nothing wrong with the healing in many such cases, if not most.
It’s almost like no one has really thought any of this through.
Mechanism masturbation par excellence
All of this is classic “mechanism masturbation” — a perfect term coined by science journalist Jonathan Jarry, describing premature speculation about how a treatment works before showing that it actually does work.28 Shockwave therapy is the best example of it that I can think of
It doesn’t matter what shockwaves do to tissues if it doesn’t translate into a practical, clinical benefit. And it mostly seems not to.
Shockwave therapy remains unproven for any condition. The evidence is still inadequate even for its greatest hits, plantar fasciitis and fracture healing. There are putatively positive studies of shockwave therapy for several conditions, but all are flawed and dubious, and there are plenty of negative ones as well.
None of which is surprising, considering the shaky theoretical foundations of shockwave therapy.
I fact-checked this to death this before publishing. I didn’t want to be embarrassed by my overzealous cynicism. But I have read more than enough of the literature recently to hold my ground: shockwave therapy has minor benefits at best. Like a UFO skeptic, I’d truly like to believe in a more amazing world, where aliens are visiting us, and shockwaves are regenerative medicine … but I think the “evidence” for either of those is a joke. Shockwave science isn’t quite as bankrupt as UFO-ology, but it ain’t far off.
To stretch that metaphor a little further, yes, some of the evidence is “hard to explain.” But that doesn’t mean it’s actually inexplicable — just that we don’t actually know exactly what fraud or error was committed. Never forget that scientific fraud isn’t nearly as rare as it should be, and it’s downright common for scientists to work in the gray zone between fraud and error, cheerfully torturing data until it tells them what they want to hear — whatever will advance their reputations and make it easier to get more funding.
I review the evidence below.
↑ MEMBERS-ONLY AREA ↑
Break it up: shattering calcifications with pressure waves
Breaking up calcifications is a more specific goal of shockwave therapy, and there’s no question that it can be done. Whether it is therapeutically valuable or not is another question, since calcifications are probably mostly just another symptom, and not the cause of a problem. They aren't even particularly hard. Quoting from my own book about plantar fasciitis, a condition that is often blamed on bone spurts:
Unfortunately for common sense, bone spurs aren’t very bone-y, and it’s not like having a rock in your shoe. Spurs are a slight calcification of the plantar fascia, brittle and thin. It’s as much like bone as tinfoil is like sheet metal. They make the back part of the plantar fascia a bit crispy.29 Stepping on them is more like stepping on a cracker than a nail. A thin cracker.
So it isn’t too surprising that lots of people have painless spurs. Even when there is pain, it’s not the spur that hurts but the plantar fascia itself or other soft-tissue structures.3031 And surgically removing a bone spur does not necessarily relieve pain, so was it likely to be causing it in the first place?3233 Spurs also tend to just grow back, because they are probably a by-product by the same chronic inflammation that causes the pain.
All this casts shade on the goal of breaking of calcifications. It may just be missing the point: a seemingly obvious target for therapy that actually just doesn't matter. Shockwave therapy could work for other reasons. But does it? Let's get into the evidence.
Hype about the shockwave therapy: profitably misrepresenting the strength of the evidence
Enthusiasm about shockwave therapy has raced ahead of the evidence. Consider this marketing language from a Canadian company, Shockwave Institute, specializing in ESWT:
Provided you are a candidate for this type of treatment, clinical studies suggest there is a 80–85% chance this technology will improve your condition.
from the Shockwave Alberta FAQ, as of Nov 30, 2009 (and still a good representative example today)
Shockwave Alberta certainly doesn’t think ultrasound has fallen out of favour! Here we have an entire company devoted to delivery of therapeutic ultrasound, and selling it with the implication that it is not only proven to be effective, but exactly how effective — to within 5%!
Based on the available evidence, do you think it’s actually possible or meaningful to declare that ESWT is exactly “80–85% effective”? Where are the scientific review papers confirming this marvellous triumph of US over whatever ails you? Where is the data to support such a specific promise of therapeutic success? You sure couldn’t find them in 2009. Many years later, it’s still not much clearer.
Shockwave evidence
Things seem to have changed for the better, though “80-85% effective” would still be a hard claim to defend.
Bizarrely, ESWT is being used to treat conditions as unexpected as erectile dysfunction, stroke, and venous leg ulcers. There’s even some preliminary evidence for such uses… though not all, and mostly not very much. It is really easy to wave a hand in the direction of a few studies that certainly make it seem like ED can be treated with shockwaves, but your optimism will quickly be ruined by reading the fine print. And the not-so-fine. Really, just reading the print is discouraging. (ED evidence detail below.)
But there are now some positive reviews of ESWT for its more common uses, like stubborn cases of plantar fasciitis, a painful irritation of the arch of the foot. A good 2016 example is Lou et al., who concluded that “ESWT seems to be particularly effective in relieving pain associated with recalcitrant plantar fasciitis.”34 Plantar fasciitis is by far the most widely ESWT-treated condition for some reason: other conditions may be a completely different matter, but certainly the evidence for plantar fasciitis is surprisingly good, almost amazingly so (a strong contrast with the vast majority of treatments for musculoskeletal conditions).
A 2009 test of shockwave therapy for hip pain (greater trochanteric pain syndrome) was clearly positive on its face.35 Exciting!
In a similar 2010 test for proximal hamstring tendinopathy, shockwave therapy seemed to handily “win.”36 Good news!
Good grief, even erectile dysfunction can be shocked away, according to what looks like a perfectly good 2023 trial.37 Hard news!
All that is sounds pretty great, right? Especially about plantar fasciitis.
The bad science news
The evidence is actually extremely unclear … even for plantar fasciitis. Which is what happens when there isn’t all that much evidence, most of it what we have isn’t particularly good quality, and/or there’s very little real treatment signal to compete with all the noise in the data. Unfortunately, a few positive studies just doesn’t mean what it once did — modern musculoskeletal science is badly polluted with underpowered studies with untrustworthy “promising” results that are mostly good for the CV’s of the researchers who produce them. Cynicism is powerfully justified.
That plantar fasciitis evidence, for instance? A good example a bad result is Heide et al., in which shockwave therapy for plantar fasciitis couldn’t beat a sham in a good quality 2024 test38 — following the classic pattern of “better studies undermine weaker early ones.” One proper negative trial in a “promising” body of evidence is like finding a toenail clipping in your soup: it can easily spoil the whole thing! Good quality negative evidence is a great deal less likely to be wrong. (I talk about all of this quite a bit more in my plantar fasciitis book.)
And this how it almost always goes.
This was a good test of the most widely used type of shockwave therapy for its most popular target. And if it goes that way with plantar fasciitis, arguably the star of the shockwave show, what are the odds for other conditions?
For instance, there’s never been any replication of those hip results, surprise surprise. Two 2023 studies both compared shockwave therapy to other treatments for greater trochanteric pain syndrome, reporting no advantage over either steroid injections39 or exercise.40 They tried to sound positive, but they weren't. And neither study compared shockwave to a sham, making them very low value in any case.
Pathetically, 2024 saw two new systematic reviews of the very sparse data on this topic, both pitch perfect examples of this new breed: junky scientific reviews of junky science! One of them considered eight trials, seven of which had a high risk of bias,41 the other just five controlled trials.42 The latter has the gall to declare that “low-quality evidence” has “established” that there are “improvements favouring SWT,” which is just a load of nonsense. The evidence hasn’t established anything at all, and favouring is how lesser scientists say that a result could be called positive if you ignore the fact that it’s actually statistically insignificant and meaningless. There have actually been papers written by real scientists about how important it is not to use terms like that in conclusions.
But you can be told by countless physical therapists around the world that your hip shock waves are totally “evidence-based.”
Shockwave therapy for adhesive capsulitis (frozen shoulder) is also being routinely sold to patients without adequate evidence. There is scarcely any evidence, just a tiny handful of weak studies — including that one that seems most promising.43 For full analysis, see my frozen shoulder article.
And not all reviews have happy endings! A notable general review in the British Medical Journal of Sports Medicine in 2018, of ESWT for “common lower limb conditions,”44 found only a “low level of evidence” that it “may” be effective for some conditions, which is getting pretty wishy-washy. They rejected thirteen studies for a high risk of bias and noted that “a relatively small number of research groups account for the majority of research.” And finally:
There are no occasions where multiple high-quality studies exist for a single pathology, hence for any individual pathology there are low and very low levels of evidence.
More recently, in 2023, Ko et al. concluded that “the overall confidence in non-surgical treatments from all included trials was very low. No recommendation of the best treatment option can be made.” And the least-lame option they identified was not shockwave but … eccentric training.45 Which is itself known to be no better than any other kind of strength training.
Shockwave therapy absolutely cannot be considered evidence-based medicine, despite years of hype to that effect. There’s just not enough (good) evidence — as usual — and what we have is just not that encouraging.
But more and more, as better trials are finally conducted — better controlled, comparing shockwave to sham — we are now seeing some entirely negative results.46| Zheng 202047 | tennis elbow | A negative review of shockwave for tennis elbow, reporting a weak positive signal at best, but mostly just inconclusive — not enough good data: GIGO. |
|---|---|---|
| Korakakis 201848 | lower limb conditions | The most recent major review of shockwave for Achilles tendinitis (with others), reporting such thin evidence that it cannot possibly be evidence-based. That was echoed in 2023 by a more general review, and a higher quality trial in 2024 … |
| Alsulaimani 202449 | Achilles tendinitis | Good quality trial comparing radial shockwave to sham … 100% negative, not a flicker of a result, with no major limitations. |
| Searle 202350 | fracture healing | Negative review reports absence-of-evidence for acute fractures and shockwave therapy, and that ultrasound makes “little or no difference to delayed union or non‐union.” |
| Yazdani 202451 | Dupuytren’s contracture | An unambiguously positive but dubious conclusion, based on poor data, that I do not trust.52 |
| Liao 202453 | osteoarthritis | Another clearly “positive” review I don’t trust, and only for mild osteoarthritis, not severe. These authors didn’t even consider risk of bias in the trials they reviewed, let alone their own. If I could grade it? D! |
| Harding 202454 | greater trochanteric pain syndrome | Classic GIGO review that disingenuously wrings a positive conclusion out of barely-there evidence with clearly negative results: “no statistical differences” for pain or function. |
| Zhang 202255 | frozen shoulder | And yet another “positive” review of “limited” data, reporting what “seems to be beneficial” results … in the short term only … and not that much benefit … and even less benefit over time.56 |
| Canguven 202157 | erectile dysfunction | Ambivalent and mediocre results from all reviews.58 There is just a single positive result from a trial with no obvious flaws.59 |
The gate control mechanism: a particularly bogus rationale for both ultrasound and shockwave therapy
Physical therapists often cite "counterstimulation and the gate control mechanism as a justification for US and ESWT (and some other popular treatments, especially TENS). This is nonsense, and a great example of why patients should be cautious, especially with the expense of ESWT. It sounds much smarter than it is.
The “gate control” mechanism is an important idea in pain science, proposed in 1965 by Dr. Ronald Melzack and Dr. Patrick Wall,60 and still accepted today as an explanation for a familiar phenomenon: the way we rub injured body parts for a little pain relief. The idea is that pain signals pass through a “gate” in the spinal column, which can be blocked by other sensations, which are (weirdly) given priority by the nervous system.
So the idea with US is that the stimulation of the sound waves closes the gate to pain. This may well occur, because counterstimulation is a real phenomenon — but it’s also nothing to write home about. It’s just a mechanism for transient, minor pain relief. It can be achieved just as easily by rubbing the area yourself! It certainly doesn’t “fix” anything, which is what ultrasound is supposed to be doing. So bringing it up is just a bit of bafflegab, a scientific-sounding rationalization for an expensive therapy. There is no reason to think that any kind of ultrasound closes the gate better or longer than any other stimulus.
The reasons for doing ultrasound are not at all clear, and adding this one is just a way to pad the list — especially handy when you’re trying to sell expensive ESWT, which might also exploit the term counter-irritation — but is actually almost meaningless. It’s disturbingly marketing-savvy, but not at all medically savvy.
A study of ultrasound therapy shows a clear effect on trigger point sensitivity
File this one under “intriguing”: Canadian researchers treated trigger points (muscle knots) in 50 patients with either ultrasound or a sham, and the amount of pressure on the trigger point required to induce pain was measured before and after. Trigger points treated with ultrasound were more tolerant of pressure than those that were not treated, at 1, 3 and 5 minutes after treatment.61 The improvement was no longer significant just 10 and 15 minutes later, however — so the effect in this case was brief. The authors concluded:
… low-dose ultrasound evokes short-term segmental antinociceptive effects on trigger points which may have applications in the management of musculoskeletal pain.
They are not necessarily proposing that ultrasound is a useful treatment for myofascial pain syndrome, but producing evidence of an interesting effect that may prove to be clinically significant in time — an important distinction.
Although it may be surprising in contrast to the generally unimpressive evidence of the effectiveness about therapeutic ultrasound, it nevertheless reinforces that ultrasound does indeed do some interesting things to tissues: it’s just not clear exactly what. An important caveat is that there is significant scientific debate about what “trigger points” really are.62 Some would say it’s hard to study the effect of ultrasound on a phenomenon that may or may not even exist!
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Related Reading
- Zapped! Do TENS and friends work for pain? — The peculiar popularity of being gently zapped with various kinds of electrical stimulation therapy. TENS is a near sibling to ultrasound: two nearly identical treatment ideas, differing only in the form of stimulation delivered to tissues.
- Tissue Provocation Therapies in Musculoskeletal Medicine — Can healing be forced? The theme of hormesis in pain and injury medicine.
- Cold Laser Therapy Reviewed — A critical analysis of treating pain and injury with frickin’ laser beams.
- Heat for Pain and Rehab — A detailed guide to using heat as therapy for acute and chronic pain and recovery from injury. The discussion of infrared radiation particularly relevant.
- The Chiropractic Controversies — An introduction to chiropractic controversies like aggressive billing, treating kids, and neck manipulation risks.
- Pseudo-Quackery in Physical Therapy — A large and dangerous grey zone between evidence-based care and clear quackery in rehab and pain treatments. Ultrasound is one of the best examples of something in that zone.
- Guide to Repetitive Strain Injuries — Five surprising and important ideas about repetitive strain injuries for patients and professionals.
What’s new in this article?
Seventeen updates have been logged for this article since publication (2009). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
2025 — Science update. Added two new citations to the shockwave evidence review, and more polish and details for the ones that were already there.
2025 — Added a small sidebar about TECAR therapy (diathermy), which is identical to ultrasound in principle.
2024 — Added a new citation to the shockwave evidence highlights, plus some older ones.
2024 — Major expansion of “Adding injury to injury: shockwave therapy’s big idea.” This nerdy new members-only section roughly doubled in size over the last couple days of writing and revision, and now most notably includes a much more complete discussion of the biological effects of shockwave therapy.
2024 — Several improvements to the review of clinical studies of shockwave therapy. More still coming.
2024 — Science update: several citations about shockwave for erectile dysfunction (just one line in the article, but the footnotes are practically a mini-article unto themselves).
2024 — Improvements to the section, “Adding injury to injury: shockwave therapy’s big idea.”
2024 — Continued improvements to shockwave content. Today I added more detail about shockwave’s ability to cause microtrauma and break up calcifications.
2024 — More extensive changes and reorganization, with substantial upgrades to all the information about shockwave therapy.
2024 — Minor but widespread improvements, and some science updates. Shockwave therapy is becoming a more prominent part of the article as it replaces low-intensity ultrasound in the marketplace.
2024 — Science update for ESWT for plantar fasciitis.
2022 — Added a sidebar: “Self-serve shockwave therapy? Buyer beware”
2018 — Some science updates for shockwave therapy.
2018 — A couple minor science updates on shockwave therapy (one good news, one bad).
2017 — Science update, cited Schandelmaier et al., an excellent (and completely negative) British Journal of Medicine review of LIPUS for acute fracture/osteotomy healing.
2017 — Added a brief acknowledgement of the surprisingly positive evidence for shockwave therapy for plantar fasciitis, plus a bunch of miscellaneous editing.
2016 — Big science update — Added a table of summarized recent reviews, including six new citations from the last decade (basically all still about scanty, crappy evidence). Several related editorial changes.
2009 — Publication.
Notes
- Wong RA, Schumann B, Townsend R, Phelps CA. A survey of therapeutic ultrasound use by physical therapists who are orthopaedic certified specialists. Phys Ther. 2007 Aug;87(8):986–94. PubMed 17553923 ❐ PainSci Bibliography 55380 ❐
Ultrasound is widely used. This 2007 survey of the usage of ultrasound, the first such American survey for almost 20 years (see Robinson 1988), “examined the opinions of physical therapists with advanced competency in orthopedics about the use and perceived clinical importance of ultrasound.” They found that “ultrasound continues to be a popular adjunctive modality in orthopedic physical therapy. These findings may help researchers prioritize needs for future research on the clinical effectiveness of US.”
- Armijo-Olivo S, Fuentes J, Muir I, Gross DP. Usage Patterns and Beliefs about Therapeutic Ultrasound by Canadian Physical Therapists: An Exploratory Population-Based Cross-Sectional Survey. Physiother Can. 2013;65(3):289–99. PubMed 24403700 ❐ PainSci Bibliography 53385 ❐
This 2013 Canadian survey of the usage of ultrasound found that “despite the questionable effectiveness of therapeutic US, physical therapists still commonly use this treatment modality, largely because of a belief that US is clinically useful. However, US usage has decreased over the past 15 years.”
- Baker 2001, op. cit.
- Tsai WC, Tang ST, Liang FC. Effect of therapeutic ultrasound on tendons. Am J Phys Med Rehabil. 2011 Dec;90(12):1068–73. PubMed 21552108 ❐
- Schandelmaier S, Kaushal A, Lytvyn L, et al. Low intensity pulsed ultrasound for bone healing: systematic review of randomized controlled trials. BMJ. 2017 Feb;356:j656. PubMed 28348110 ❐ PainSci Bibliography 52780 ❐ From the abstract: “trials at low risk of bias failed to show a benefit with LIPUS, while trials at high risk of bias suggested a benefit” and “LIPUS does not improve outcomes important to patients and probably has no effect on radiographic bone healing.”
- Searle HKC, Lewis SR, Coyle C, Welch M, Griffin XL. Ultrasound and shockwave therapy for acute fractures in adults. Cochrane Database Syst Rev. 2023 Mar;3(3):CD008579. PubMed 36866917 ❐ PainSci Bibliography 49769 ❐
- In particular, even though there are many “flavours,” it’s easy to standardize it for apples-to-apples comparisons, and it’s really easy to fake treatment for a good controlled and blinded test. It’s basically effortless to create a perfect “sham” version of ultrasound, so that the study subjects can’t tell if they are getting the real thing. Many other popular interventions in manual therapy are difficult or even impossible to standardize and/or fake — so it makes more sense that there’s long-term uncertainty about their effectiveness. Ultrasound has much less excuse in this regard.
- Staples MP, Forbes A, Ptasznik R, Gordon J, Buchbinder R. A randomized controlled trial of extracorporeal shock wave therapy for lateral epicondylitis (tennis elbow). J Rheumatol. 2008 Oct;35(10):2038–46. PubMed 18792997 ❐
- van der Windt DA, van der Heijden GJ, van den Berg SG, et al. Ultrasound therapy for musculoskeletal disorders: a systematic review. Pain. 1999 Jun;81(3):257–71. PubMed 10431713 ❐
- Robertson VJ, Baker KG. A review of therapeutic ultrasound: effectiveness studies. Phys Ther. 2001 Jul;81(7):1339–50. PubMed 11444997 ❐ PainSci Bibliography 55377 ❐
- Baker KG, Robertson VJ, Duck FA. A review of therapeutic ultrasound: biophysical effects. Phys Ther. 2001 Jul;81(7):1351–8. PubMed 11444998 ❐ PainSci Bibliography 55382 ❐
- Buchbinder R, Green SE, Youd JM, et al. Systematic review of the efficacy and safety of shock wave therapy for lateral elbow pain. J Rheumatol. 2006 Jul;33(7):1351–63. PubMed 16821270 ❐
- Ho C. Extracorporeal shock wave treatment for chronic lateral epicondylitis (tennis elbow). Issues In Emerging Health Technologies. 2007 Jan;(96 (part 2)):1–4. PubMed 17302021 ❐
- Ho C. Extracorporeal shock wave treatment for chronic rotator cuff tendonitis (shoulder pain). Issues In Emerging Health Technologies. 2007 Jan;(96 (part 3)):1–4. PubMed 17302022 ❐
- Rutjes AW, Nüesch E, Sterchi R, Jüni P. Therapeutic ultrasound for osteoarthritis of the knee or hip. Cochrane Database Syst Rev. 2010 Jan;(1):CD003132. PubMed 20091539 ❐
- Shanks P, Curran M, Fletcher P, Thompson R. The effectiveness of therapeutic ultrasound for musculoskeletal conditions of the lower limb: A literature review. Foot (Edinb). 2010 Dec;20(4):133–9. PubMed 20961748 ❐
- van den Bekerom MP, van der Windt DA, Ter Riet G, van der Heijden GJ, Bouter LM. Therapeutic ultrasound for acute ankle sprains. Cochrane Database Syst Rev. 2011 Jun;(6):CD001250. PubMed 21678332 ❐
- Page MJ, O’Connor D, Pitt V, Massy-Westropp N. Therapeutic ultrasound for carpal tunnel syndrome. Cochrane Database Syst Rev. 2013 Mar;(3):CD009601. PubMed 23543580 ❐
- Desmeules F, Boudreault J, Roy JS, et al. The efficacy of therapeutic ultrasound for rotator cuff tendinopathy: A systematic review and meta-analysis. Phys Ther Sport. 2015 Aug;16(3):276–84. PubMed 25824429 ❐
- Ebadi S, Henschke N, Forogh B, et al. Therapeutic ultrasound for chronic low back pain. Cochrane Database Syst Rev. 2020 Jul;7(7):CD009169. PubMed 32623724 ❐ PainSci Bibliography 49771 ❐
A technically inconclusive but completely underwhelming review of 10 small trials of ultrasound for chronic low back pain … none of them good quality. This is an update to a 2014 version, and since then the authors’ confidence in all the evidence was “downgraded for imprecision and serious limitations in design,” and for “very serious imprecision” in a couple cases. The evidence is so sketchy that “we do not know,” but “the current evidence does not support the use of therapeutic ultrasound in the management of chronic LBP.” As always, it’s a subtle but particularly damning kind of result when even biased trials fail to collectively produce a compelling positive result.
- TENS may be more evidence-based than ultrasound, particularly for some specific medical situations, but its widespread, indiscriminate use is definitely dubious. Like ultrasound, it is clearly sold to patients for more purposes than the evidence can possibly support. For more information, see Zapped! Do TENS and friends work for pain?
- This technology was adapted from a revolutionary method of smashing gall stones and kidney stones with pressure waves, one of the greater victories of modern medicine, back in the 1980s. That technology was known as “extracorporeal” to emphasize the fact that you didn’t have to cut into someone, or insert a probe up the urethra — which, eek, had been routine! In a physical therapy context, we don’t much care about the fact that there’s no cutting, so the term is often dropped.
- This requires much more expensive and sophisticated machinery, and it was extravagantly expensive for a long time. It’s come down a lot, but even now it will run you at least $100 per visit, often much more, with a typical prescription of three to six treatments. I last checked prices in 2024.
- There are actually several different types of extracorporeal shockwave therapy. Radial shockwave therapy is often called “shockwave” therapy, but probably shouldn’t be, because it uses much lower velocity waves. Radial ultrasound is a couple orders of magnitude slower than other shockwave therapies — about 100 meters per second, instead of 1500. It’s might not even be fair to lump them all in together when assessing shockwave therapy … but I’m going to do it anyway for now. Until such time as there’s compelling evidence that one flavour has impressively different and better effects than another, it’s all just trivial variations on a consistent theme.
- Below the range of human hearing is “infrasound,” which doesn’t come up much. Some animals, like elephants, use infrasound for communication. Not therapy, as far as we know, but I wouldn’t put it past them! Elephants are clever. Other infrasound communicators: hippos, alligators, whales. Cat purring drops down almost to infrasound range.
- Moya D, Ramón S, Schaden W, et al. The Role of Extracorporeal Shockwave Treatment in Musculoskeletal Disorders. J Bone Joint Surg Am. 2018 Feb;100(3):251–263. PubMed 29406349 ❐ They are clearly “true believers” in shockwave therapy, a collaboration of several authors from around the world who have generated most of the shockwave therapy research currently indexed by PubMed. There are issues with the quality of their review, but it is (at least) a fine overview of what these shockwave proponents believed as of 2018, and likely still believe now.
- Haupt G. Use of extracorporeal shock waves in the treatment of pseudarthrosis, tendinopathy and other orthopedic diseases. J Urol. 1997 Jul;158(1):4–11. PubMed 9186313 ❐ This paper was probably a major inspiration for the invasion of shockwave therapy into orthopaedic medicine. Twenty years later, Moya et al. cite (at least) 36 papers to support Haupt’s quite speculative claims, and it’s an impressive-looking list. But it’s really more like about a half dozen a citations, because the diversity of authorship is quite low, and there’s a lot of overlap and repetition — mostly papers by people who are all co-authors on that review, especially a couple of prolific Chinese authors.
“Mechanism masturbation” is wishful and fanciful thinking about why/how treatments might work. Science journalist Jonathan Jarry (once upon a time on a place called “Twitter,” now removed, but you can listen to an interview about it):
“There is a fascinating phenomenon in the complementary and alternative medicine literature we could call ‘mechanism masturbation’ where the authors, faced with the tiniest of positive signals in a small study, write paragraph after paragraph hypothesizing how, mechanistically, watermelon seeds might cure schizophrenia.”
Musculoskeletal and pain research, alternative as well as more mainstream research, is rotten with “mechanism masturbation” — often because it’s just all there is. There’s no good clinical trial data, so we get wishful thinking and wild speculation instead, even in scientific publications. The field is surprisingly afflicted with cart-before-horse speculation about how they how they could work, might work, should work, maybe work… when the clinical trials (if they exist at all) tend to show that they don’t actually work, or not very well.
Jonathan’s satirical example really nails the flavour of “research” like this:
“It might interfere with the hypothalamic-pituitary-adrenal axis… One of its compounds does bind to alpha receptors in this cell type… Could play a role in this cascade... Anyway, preliminary results from n = 6. More studies needed!”
Yes, that definitely reads like about a thousand papers I’ve wasted my time reading over the last decade. I’m always looking for the rare scraps of basic science I can actually consider interesting/promising instead of more post-hoc rationalization for someone’s meal ticket. 🙄
- Some bones spurs are undoubtedly thicker and harder than others, just like some people have much larger calluses than other people. (I have a callus on one foot that is always far thicker and sturdier than I seem to need.) But regardless, the spur tends to disintegrate the further it gets from the heel.
- Osborne HR, Breidahl WH, Allison GT. Critical differences in lateral X-rays with and without a diagnosis of plantar fasciitis. J Sci Med Sport. 2006 Jun;9(3):231–7. PubMed 16697701 ❐
From the abstract: “ ... the key radiological features that differentiate the groups were not spurs but rather changes in the soft tissues.”
- Tountas AA, Fornasier VL. Operative treatment of subcalcaneal pain. Clin Orthop Relat Res. 1996 Nov:170–8. PubMed 2663678 ❐
This paper reports on a study of twenty patients in the years after surgical removal of bone spurs. Although most of the patients had “excellent” or “good” results three years later, their spurs had reformed in many cases, and analysis of the soft tissues showed that “changes within the fascia, rather than the spur, are primarily responsible for the pathogenesis of the syndrome.”
- Onwuanyi ON. Calcaneal spurs and plantar heel pad pain. Foot. 2000;10.
From the abstract: “Calcaneal spurs cause plantar heel pad pain, but the roles of other co-morbid factors are significant. The excision of these spurs does not necessarily abolish pain.”
- Fishco WD, Goecker RM, Schwartz RI. The instep plantar fasciotomy for chronic plantar fasciitis. A retrospective review. J Am Podiatr Med Assoc. 2000 Feb;90(2):66–9. PubMed 10697969 ❐ In this study, surgical outcomes were similar — and generally good — with or without heel spur removal.
- Lou J, Wang S, Liu S, Xing G. Effectiveness of Extracorporeal Shock Wave Therapy Without Local Anesthesia in Patients With Recalcitrant Plantar Fasciitis: A Meta-Analysis of Randomized Controlled Trials. Am J Phys Med Rehabil. 2016 Dec. PubMed 27977431 ❐
- Furia JP, Rompe JD, Maffulli N. Low-energy extracorporeal shock wave therapy as a treatment for greater trochanteric pain syndrome. Am J Sports Med. 2009 Sep;37(9):1806–13. PubMed 19439756 ❐
33 patients were given low-energy shockwave therapy for greater trochanteric pain syndrome, while 33 others were treated with other forms of conservative therapy. Those who got shockwave therapy were the lucky ones: the results were clear and positive, both statistically and clinically significant, and sustained as long as a year later. The study is underpowered and cannot be taken too seriously, but it’s certainly positive on its face. Conclusion: “Shock wave therapy can be an effective treatment for greater trochanteric pain syndrome.”
- Cacchio A, Rompe JD, Furia JP, et al. Shockwave Therapy for the Treatment of Chronic Proximal Hamstring Tendinopathy in Professional Athletes. Am J Sports Med. 2010 Sep. PubMed 20855554 ❐
- Kennady EH, Bryk DJ, Ali MM, et al. Low-intensity shockwave therapy improves baseline erectile function: a randomized sham-controlled crossover trial. Sex Med. 2023 Oct;11(5):qfad053. PubMed 37965376 ❐ PainSci Bibliography 49752 ❐
A controlled trial with no obvious flaws and a strongly positive result for shockwave therapy for erectile dysfunction. See also the long-term follow-up, Lange et al., which reports that the results were lasting: “durable improvement in erectile function for the first 2 years with a peak treatment effect at 1 year. Treatment effect appears to decline between 2 and 3 years.”
If that’s all we had to go on I certainly would be wondering if shockwave for ED actually does work somehow. But the rest of the literature on this is highly equivocal, with only mediocre results.
If this were about pain, I’d dig in more. But ED isn’t exactly my professional focus.
A controlled trial with no obvious flaws and a strongly positive result for shockwave therapy for erectile dysfunction. See also the long-term follow-up, Lange et al., which reports that the results were lasting: “durable improvement in erectile function for the first 2 years with a peak treatment effect at 1 year. Treatment effect appears to decline between 2 and 3 years.”
- Heide M, Røe C, Mørk M, et al. Is radial extracorporeal shock wave therapy (rESWT), sham-rESWT or a standardised exercise programme in combination with advice plus customised foot orthoses more effective than advice plus customised foot orthoses alone in the treatment of plantar fasciopathy? A double-blind, randomised, sham-controlled trial. Br J Sports Med. 2024 Jul;58(16):910–918. PubMed 38904119 ❐ PainSci Bibliography 49858 ❐
This trial was designed to test the efficacy of radial extracorporeal shock wave therapy (rESWT) for plantar fasciitis, by comparing it to a sham, an exercise program, and just advice and orthoses). They recruited 200 patients and split them up into four groups, and checked on at the start and then after 3, 6, and 12 months. The shockwave group got three treatments.
There were “no statistically significant between-group differences,” so it was a wash: not only no measurable difference between real and fake shockwave therapy, but exercise, advice, and orthoses also all failed to be helpful. The authors concluded:
“In patients with plantar fasciopathy, there was no additional benefit of rESWT, sham-rESWT or a standardised exercise programme over advice plus customised foot orthoses in alleviating heel pain.”
- Çağlar Yağcı H, Yağcı İ, Bağcıer F. Comparison of shock wave therapy and corticosteroid injection in the treatment of greater trochanteric pain syndrome: A single-blind, randomized study. Turk J Phys Med Rehabil. 2023 Jun;69(2):180–187. PubMed 37671381 ❐ PainSci Bibliography 49731 ❐
- Notarnicola A, Ladisa I, Lanzilotta P, et al. Shock Waves and Therapeutic Exercise in Greater Trochanteric Pain Syndrome: A Prospective Randomized Clinical Trial with Cross-Over. J Pers Med. 2023 Jun;13(6):976. PubMed 37373965 ❐ PainSci Bibliography 49728 ❐
- Rhim HC, Shin J, Beling A, et al. Extracorporeal Shockwave Therapy for Greater Trochanteric Pain Syndrome: A Systematic Review with Meta-Analysis of Randomized Clinical Trials. JBJS Rev. 2024 Aug;12(8). PubMed 39297780 ❐
- Harding D, Cameron L, Monga A, Winter S. Is shockwave therapy effective in the management of greater trochanteric pain syndrome? A systematic review and meta-analysis. Musculoskeletal Care. 2024 Jun;22(2):e1892. PubMed 38777616 ❐
- Hussein AZ, Donatelli RA. The efficacy of radial extracorporeal shockwave therapy in shoulder adhesive capsulitis: a prospective, randomised, double-blind, placebo-controlled, clinical study. European Journal of Physiotherapy. 2016 Mar;18(1):63–76.
This test of shockwave therapy for frozen shoulder hits all the highlights of well-designed experiment. The researchers gave real shockwave therapy to one group of 52 patients weekly for a month, and sham shockwave therapy to the other group, and measured pain and function. The real shockwave group did “significantly” better, with the researchers notably claiming both statistical and clinical significance of the results … but not reporting the actual effect sizes in the abstract, which is always suspicious — in general impressive effects are featured!
Despite the good design, a major concern here is that sham treatment. Shockwave therapy is high energy, and uncomfortable at best, painful at worst. In the sham group, the shockwaves were simply “blocked.” It seems like many or most patients would certainly know that they weren’t getting the real shockwave therapy … which would spoil the data for sure.
So the results are seem promising, but it’s a mystery why shockwave therapy would work (read: highly implausible), and the effect they observed was not very large, and there’s probably one huge flaw that would be a deal-breaker.
- Korakakis V, Whiteley R, Tzavara A, Malliaropoulos N. The effectiveness of extracorporeal shockwave therapy in common lower limb conditions: a systematic review including quantification of patient-rated pain reduction. Br J Sports Med. 2018 Mar;52(6):387–407. PubMed 28954794 ❐
A very tepid “positive” conclusion about based on lousy evidence, and yet the conclusion sounds better than the actual results, which seem downright discouraging to me. So, yet another “garbage in, garbage out“ review that damns with faint praise.
- Ko VMC, Cao M, Qiu J, et al. Comparative short-term effectiveness of non-surgical treatments for insertional Achilles tendinopathy: a systematic review and network meta-analysis. BMC Musculoskelet Disord. 2023 Feb;24(1):102. PubMed 36750789 ❐ PainSci Bibliography 49666 ❐
- Alsulaimani B, Perraton L, Vallance P, Powers T, Malliaras P. Does shockwave therapy lead to better pain and function than sham over 12 weeks in people with insertional Achilles tendinopathy? A randomised controlled trial. Clin Rehabil. 2024 Dec:2692155241295683. PubMed 39704142 ❐
More shockwave data…more negativity! We didn’t much need another thumbs-down trial of this, but we got it anyway: radial shockwave versus sham in 76 people over 3 months, measuring mainly VISA-A scores. Result? “No evidence for between-group differences” at any time, for any outcome. 😕
Some minor caveats for this trial:
- The dosage might be a bit dodgy. More shocking waves could conceivably have worked better.
- Some missing masking. The providers shouldn’t know who got the sham! It’s probably not a serious error in this case — unblinded trials tend to swing towards false positives, not false negatives — but nevertheless a classic science foul.
- And the sham had a touch too much potential to actually treat via the same mechanism as shockwave itself: causing discomfort, conditioned pain modulation, but in my opinion that’s quite unlikely. See Counterstimulation, Counterirritation, and Gate Control.
- Zheng C, Zeng D, Chen J, et al. Effectiveness of extracorporeal shock wave therapy in patients with tennis elbow: A meta-analysis of randomized controlled trials. Medicine (Baltimore). 2020 Jul;99(30):e21189. PubMed 32791694 ❐ PainSci Bibliography 52060 ❐
- Korakakis 2018, op. cit.
- Alsulaimani 2024, op. cit.
- Searle 2023, op. cit.
- Yazdani A, Nasri P, Baradaran Mahdavi S. The Effects of Shock Wave Therapy on the Symptoms and Function of Individuals With Dupuytren Disease: A Systematic Review. Arch Phys Med Rehabil. 2024 Oct;105(10):1985–1992. PubMed 38866227 ❐
Yazdani et al. looked at twenty-six trials of shockwave therapy for Dupuytren’s contracture, tossed out twenty, and reviewed the remaining six teeny tiny studies — just 145 patients covered by all of them. But studies don’t have to be big to be worthwhile, and these researchers judged five to be “good” quality, and one “fair.” I think they might have been a bit too generous.
But — good news, everyone! — those six studies of uncertain quality collectively showed “remarkable improvement” in pain and function, as measured by the pain-scale and various disability questionnaires. One study also reported improved grip.
And another reported actual shrinkage of the distinctive bumps and lumps of Dupuytren’s contracture! So maybe shockwave therapy can “melt” contractures somehow? That would be a way bigger deal than merely improving pain and function — that’s changing the course of the disease. If it really does, that’s some crazy physiology, fascinating and important. But I rather doubt it. And so do Yazdani et al., who rated their confidence in that evidence “low.” (Even though it came from a study they rated as “fair”? Seems like a bit of a contradiction there.)
The review concludes (with some slightly stilted English):
Shockwave therapy can lead to significant pain improvement, functional rehabilitation, and patient satisfaction with no adverse effect in the management of Dupuytren disease. Pain may return over time, but not to that severity [sic] before the intervention.
For whatever a small review of a small body of evidence is worth. Reviews are worse than laws and sausages: the more we know about how they’re made, the less we like them (hat tip to Mark Crislip).
- It may be correct, of course, but this is a small review of dubious quality, looking at a handful of tiny studies that almost certainly had a high risk of bias. Garbage in, garbage out. Similar reviews of shockwave therapy for conditions in this pathological family (e.g. Peyronie’s) are much the same, and some are more negative. For more detailed analysis, see the shockwave section in my Dupuytren’s contracture guide.
- Liao PC, Chou SH, Shih CL. A systematic review of the use of shockwave therapy for knee osteoarthritis. J Orthop. 2024 Oct;56:18–25. PubMed 38765896 ❐ PainSci Bibliography 50166 ❐
This review of shockwave for osteoarthritis comes to a clear positive conclusion: “This review demonstrated that ESWT was effective for knee osteoarthritis.” Well, mild osteoarthritis anyway. Not severe. Which seems important. But I don’t trust this paper’s conclusions even about mild osteoarthritis. Sometimes I read a paper carefully to see if there are any clear, good reasons for my concern. This is what I found:
- It is not a particularly well written paper. That doesn’t mean it’s wrong, but data that is poorly explained is harder to trust.
- These reviewers seem to assume the efficacy of shockwave generally, and provide an “excuse” for its weak showing in meta-analyses to date (“heterogeneity,” different settings of course). The authors reference other notoriously ineffective modalities as though they think they are effective. So I think they have a significant bias, and I strongly suspect they were looking for data to confirm that bias.
- And that is ironic, because they not only failed to factor “risk of bias” into their review … the word “bias” literally does not even appear in paper. Huge red flag.
- “Significant” is used (abused) repeatedly to characterize the effect of shockwave without even attempting to make a distinction between statistical and clinical significance. “Effect size” is another key term completely missing from the paper. Even the statistical significance isn’t impressive: the only p values even mentioned were p < .05, the bare minimum required for statistical significance.
- They conclude that “the efficacy of ESWT for knee OA has been confirmed.” Confirmed, eh? Big word! Ridiculously overconfident for such a hotly contested modality, and also contributes.
- Their limited discussion of limitations is focused on perceived weaknesses in the evidence they reviewed, rather than how they reviewed it.
There are no obvious, objective major flaws in the review, except perhaps the failure to integrate risk of bias. But after a careful read, I definitely still don’t like it or trust it, and strongly suspect that it’s a classic example of not just the “garbage in, garbage out” problem, but “finding the signal you want to find in the garbage” inserted into the middle.
It’s a bit awkward for a skeptic to scoff a paper mostly just citing “probably GIGO and biased.” But it’s not an unreasonable skepticism, given what we know about the body of evidence on this topic (mixed!), the generally low quality of trials, the implausibility of the mechanism, etc. If I looked at the same trials, I strongly doubt that I would come to the same conclusion.
- Harding 2024, op. cit.
- Zhang R, Wang Z, Liu R, et al. Extracorporeal Shockwave Therapy as an Adjunctive Therapy for Frozen Shoulder: A Systematic Review and Meta-analysis. Orthop J Sports Med. 2022 Feb;10(2):23259671211062222. PubMed 35141337 ❐ PainSci Bibliography 50163 ❐
- The greatest reported benefit was on “immediate” pain relief. Less for “short term.” And less still for long term! (The long-term data “were heterogeneous, and the conclusions were not reliable.”) And even for immediate analgesia, we’re talking about a barely-there effect, just over the line. How do I say this nicely? For people with frozen shoulder, very unreliable evidence of minor-at-best improvements in pain or function over a year or so is not a positive result. That’s not helping! 😡 Shockwave is just sucking money out of their wallet while they continue to have essentially the same experience of that extremely frustrating condition … even if the small benefit is real, which is probably isn’t!
- Canguven O, Khalafalla K, Al Ansari A. Low-intensity extracorporeal shockwave therapy for erectile dysfunction. Arab J Urol. 2021;19(3):340–345. PubMed 34552784 ❐ PainSci Bibliography 49753 ❐ See next note for some analysis.
A reader contacted me, skeptically curious about all the positive studies of shockwave for erectile dysfunction, along with a few examples. I cynically predicted that they would plug nicely into a traditional pattern: generally poor quality, with the worst studies producing the most allegedly positive results, and the best being ambivalent or negative.
There isn’t really a coherent hypothesis for why shockwave therapy would improve ED in the first place. ED is a tip-of-iceberg problem, a symptom resulting from diverse and diffuse issues. It’s weird that anyone would even think to use shockwaves for it, but that's the power of the mindset behind "provocative" therapies.
So a benefit from shockwave for ED, while not impossible, is definitely implausible — and that tends to produce bogus statistical significance (Pandolfi). If you want false positives from trials, study low-plausibility hypotheses, et voila! So basically the bar is high when you’re studying sketchy claims, and these studies probably aren’t going to clear that bar, and all the positive reviews are likely just false-positive-garbage-in, false-positive-garbage-out.
So that was my guess in advance. Was my cynicism justified?
- Canguven et al.: Shockwave for ED’s “role in human clinical trials is still controversial”, so that’s not any kind of positive, false or otherwise. Also, they only report statistically significant improvement in any case, and that’s basically meaningless without effect size — which was probably really small or it would have been reported and touted. This is precisely how results are distorted in the direction of a positive.
- Lu et al.: “most” trials are “encouraging” and “suggest” that shockwave “could” improve ED … wow, ambivalent much? I don’t actually see this as a particular positive conclusion either. It’s just not a clear signal in the data, and the language of the conclusion reflects that. This is exactly the sort of “promising” evidence that is extremely unlikely to hold up.
- Dong et al.: Here we have a perfect example of “statistical significance” being used to obscure missing clinical significance. The mean improvement was 2 points on the 30-point scale … and guess what the minimal clinically important difference is for that? Four points. So that’s just noise, period. It’s a negative result. And then they conclude by declaring “improvement” and “better results,” but without acknowledging that we’re talking about a literally imperceptible change in most cases. Disingenous bullshit, absolutely typical of the industry’s problem with junky little bias-powered papers.
And two of those are Chinese papers, which have a poor scientific track record. So my guess in advance held up better than I expected. I would rate all three of those reviews as next to worthless, and the lack of a clearer signal damns shockwave for ED with extremely faint praise.
- Kennady 2023, op. cit.
And if that’s all we had to go on, I certainly would be wondering if shockwave for ED actually does work somehow. But the rest of the literature on this is highly equivocal, with only mediocre results (see previous note). And If this were about pain, I’d dig in more. But ED isn’t exactly my professional focus. 🙂
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965 Nov;150(3699):971–9. PubMed 5320816 ❐
This is Melzack and Wall’s seminal paper arguing that (emphasis mine) “pain perception and response is triggered after the cutaneous sensory input has been modulated by both sensory feedback mechanisms and the influences of the central nervous system. We propose that the abstraction of information at the first synapse may mark only the beginning of a continuing selection and filtering of the input.” Among other things, this is the paper that described the mechanism of gate control and ultimately gave rise to the highly influential concept of the neuromatrix (Melzack).
- Srbely JZ, Dickey JP, Lowerison M, et al. Stimulation of myofascial trigger points with ultrasound induces segmental antinociceptive effects: A randomized controlled study. Pain. 2008 Oct 15;139(2):260–6. PubMed 18508198 ❐
- The dominant theory is that a trigger point is basically an isolated spasm affecting just a small patch of muscle tissue. Unfortunately, it’s still just a theory, and trigger point science is a bit half-baked and somewhat controversial, and it’s not even clear that it’s a “muscle” problem. The pain is certainly real, but it isn’t necessarily coming from the muscle at all. See Trigger Point Doubts.