Does Fascia Matter?
A detailed critical analysis of the clinical relevance of fascia science and fascia properties
Sheets of fascia can contract a bit like muscle … but how strongly? Enough to make a difference?
Is fascia medically important? Does fascia — sheets and webs of fibrous connective tissue — have any properties that are relevant to healing and therapy? Are there good reasons for therapy to target fascia?
Fascia gets discussed in therapy offices a lot these days, and even at conferences dedicated to the stuff. It is supposedly the key to many a therapeutic puzzle, and is now routinely targeted as a part of all kinds of alternative therapy, especially massage therapy (especially techniques like “scraping massage” with hard-edged tools), chiropractic), and also physical therapy.1 Fascia is fashionable. But does fascia actually matter in therapy?
This article thoroughly explores and questions fascia excitement from a scientific perspective.2
Fascia-nating
Fascia enthusiasts are worrisomely vague about why fascia matters, or how exactly “fascial work” can help people with common pain problems. They speak mainly about how complex and widespread fascia is — so are bones, muscles, nerves, and blood — as if that alone is a good enough reason to focus on fascia. Attempts to get more specific are usually sloppy. Poor clinical reasoning — therapy babble — about fascia seems to be too common, even among the most educated enthusiasts.3 It’s a strong theme in all the bizarre and medically illiterate “shit massage therapists say.”4
Unfortunately, fascial therapy is one of the best examples not only of “manual (hands-on) therapy,” but also one of the best examples of how misguided most manual therapy is in general.5
Fascia babbling examples
I was getting a massage on my 40th birthday (because I really do love massage). The therapist was doing fascial work, of course — you can’t get a massage in Vancouver these days without getting your fascia worked over. She was using some annoying pulling and twisting techniques, trying to “release” my fascia, instead of using the more satisfying, relaxing Swedish styles I craved. She launched into an awkward account of her technique, but words truly failed her:
Well, your problem is fascia. The fascia is the thing you have to do something with. If you fix the fascia, everything gets more … well, the fascia will make everything better.
I didn’t have any problem.6 But fascia fixing was going to help it! Somehow. I wish I could say this extremely murky explanation of fascial therapy was unusual, but I’ve actually heard this sort of thing many times over the years, even from the well-trained massage therapists around here,7 and physiotherapists too …
Fascia apologists are forever trying to convince me that their fetish for this tissue is evidence-based, clinically relevant, and intellectually mature, and yet I just keep hearing stories like this (paraphrased anecdote from a reader, who was horrified):
I nearly broke my hand, and I’ve been recovering from that injury. My physiotherapist was treating it with some massage. She described the technique as ‘fascial release,’ and warned me about a possible side effect: ‘You might feel sad, or even start to cry,’ she said.
Any health care may involve sadness and crying, but “fascial release” is not emotional: being cared for, touched, and manipulated is emotional. Occasionally. But it’s probably not emotional for 99% of patients who just want some rehab help after a wrist sprain. Emphasizing sadness as “side effect” of fascial release in that scenario requires a bizarre meltdown of clinical communication priorities. It wasn’t said because it mattered to the patient — it was pure marketing, a bullet point about the potency and specialness of fascial release.
Weird ideas about fascia are out there in a big way.
Barely known to science!
There is a lot of fascia research going on these days. None of that research is clearly relevant to therapy. Some of it might be, but it’s all quite debatable. There are no slam dunks. In place of firm theories based on hard data, there’s a lot of speculating about why fascia is important, which leads to some claims that it has (clinically relevant) properties and functions that are still barely known to science. For instance, perhaps fascia can actively cinch up like a corset around muscles, or maybe it is the medium of a liquid crystal communication system, or even maybe it melts like butter when you move. Who knows! Anything’s possible!
This pattern is one of the most prominent examples of “mechanism masturbation” in all of healthcare.8
In the history of science and medicine, knowledge gaps get filled with guesses, and the guesses usually turn out to be wrong.9 Exotic biology is rarely useful biology. Interesting, but not useful. No one can get safe, effective, reliable treatment protocols out of barely understood biology. If you could, the biology wouldn’t be poorly understood anymore — and you’d be famous for pushing back the frontiers of human knowledge and reducing human suffering.
Some fascia research is truly intriguing. What many researchers are saying about fascia is reasonable. Many are not reaching awkwardly beyond the data. Unfortunately, many therapists fascinated by fascia are reaching beyond — way beyond — what the science can actually support, or probably ever will. In some cases, in fact, we already know enough to know that an interesting property of fascia is only interesting, and irrelevant to working with patients.
Please beware the implication of therapeutic significance from scraps of basic biology. It is easy to sound cool talking about new biology, because biology is cool. It is hard to make biology useful. Few basic biology facts ever become the basis for any kind of treatment. Certainly a lot of fascia science is “right,” but I question whether or not it matters that it is right.
In fact, on one occasion, a rather pedantic experimental psychologist was telling him about a long, complicated experiment he had done, incorporating all the proper controls and using considerable technical virtuosity. When he saw Crick’s exasperated expression he said, “but Dr. Crick, we have got it right — we know it’s right,” Crick’s response was, “The point is not whether it’s right. The point is: does it even matter whether it’s right or wrong?”
V.S. Ramachandran, telling a story about Francis Crick
En garde! The fascia science challenge
Fascia is biologically interesting! All biology is. But clinical relevance is the central question of this article: if fascia science cannot actually improve treatment, then it makes no sense to be fascinated by it in a therapeutic context. You might as well get excited about the biology of the immune system, or olfaction, or epigenetics, for all they have to do with hands-on healing.
Fascia enthusiasts routinely denounce this article, accusing me of ignorance of the current Science of Fascia. However, you should know that I am pretty up on massage-related research — it’s basically my full-time job — so I feel confident challenging critics to cite even one example of fascia research with clear, direct relevance to what happens in treatment. If such a thing exists, I will be happy to publicly discuss it, and acknowledge my oversight. I could be wrong about fascia. I even hope that I am. Maybe it is important to manipulate fascia specifically.
This article covers:
- For context, some fascia basics from mainstream medicine, which sounds boring, but get ready to cringe (it involves amputation).
- For more context, several of the stranger and sloppier examples fascia “science”: piezoelectricity, fuzz, thixotropy, and the acupuncture connection.
- And the main event: several key examples of allegedly clinically relevant fascia research. We do not have a winner yet.
There is a crack in everything
That’s how the light gets in.Leonard Cohen, Anthem
Definitions: what fascia is (and isn’t)
The term “fascia” is imprecisely defined. Traditionally it refers to “masses of connective tissue large enough to be visible to the unaided eye” (Gray’s Anatomy) mainly consisting of wrappings around anatomical structures like muscles and organs. In other words, the gristle in your steak is fascia. Other fascia-wrappings include the relatively delicate sheaths around nerve and vessel sheaths, and the much tougher and fibrous joint capsules.
In the last twenty-five years, a broader definition has emerged to serve the interests of people who believe that fascia is medically important. It is often imprecisely used to refer to medically important fibrous connective tissue, microscopic and macroscopic. The medical importance of fascia is often attributed to its ubiquity in the human body. Thus, a more inclusive definition supports the alleged therapeutic importance of fascia, and the people who have staked their reputations on it.
Any 1980 physician — and many doctors today — would have found it bizarre to stick the “fascia” label on so many connective tissue structures. Connective tissue is one of the four basic tissue types in the body, along with epithelial (skin), muscle, and nervous tissue. They are understood by experts in terms of their embyronic origins. Connective tissue arises from the mesoderm, one of the three germ layers of tissue in very young embryos. In addition to the most gristle-like tissues, it also includes tendons and ligaments, which are the most obviously connecting of the connective tissues. And then there’s also bone, cartilage, fat, and blood and lymph.
You read that right: fat is connective tissue. But it is not fascia.
The point of this is: all fascia is connective tissue, but not all connective tissue is fascia, not by a long shot. Fascia is rarely considered a meaningful type of connective tissue; it is just one humble sub-type, not even worth a mention in some definitions on connective tissue. Ironically, many people who enthusistically refer to any connective tissue they know about as “fascia” are actually unaware of many less obvious connective tissues (like bone, blood, and fat).
Origins and types of fascial therapy
The idea that fascia is medically important has its most important roots in the 1990s, when physician Stephen Typaldos formulated the Fascial Distortion Model (FDM) in 1991, proposing that most musculoskeletal complaints are caused by deformations of fascia. Typaldos thought deformed fascia could be fixed by skilful force, kind of like banging the dents out of a car.
None of it was truly new, of course — not even in the 1990s. Fascia has been worshipped for decades. For instance, over a century ago there was a chiropractor who got fixated on fascia instead of spinal joints and that became naprapathy, a vintage modality mash-up of spinal manipulation and fascial therapy. Scrape off a layer of quaint, kooky, old-timey bullshit, and you find a central tenet that is indistinguishable from typical modern fascia nonsense and pseudoscience, namely that fascia can “dry up” — which is very recognizably just another kind of “fascial distortion.”10
But most modern ideas about fascia’s medical importance seem to be more inspired by FDM, and vary mainly with competing notions about exactly how best to fix those pesky distortions: how hard, what to pull on, tools or no tools, and so on. Some of these derivatives have been so commercially successfully that they now shine much brighter than the original. Prominent brands claim to “melt” fascia,11 “blast” it,12 and “fix pain fast.”13 Some methods try to change fascia by scraping it with hard-edged tools,14 while others — at the opposite extreme — are “subtle” and meant to lovingly coax fascia to de-distort.15
And the naprapaths are still doing their thing too, because nothing ever really dies in this business — not if you can sell it.
These are all just variations on a theme that has never been validated scientifically.16 No one has ever scientifically demonstrated that any kind of “fascial distortion” exist in the first place, or that anyone is actually helped by any of the many manul therapy techniques intended to correct these alleged distortions, or by any related technique. It was just an idea that went viral. Instead of research that fixes this, all we have is a mess of basic research into the nature and properties of fascia, none of which actually matters.17
Meanwhile, fragile fascia is actually a known pathology
Fascial therapists are chasing speculative connective tissue bogeymen, but there are real diseases of connective tissue that are actually common… and the last thing they need is “release.”
Most importantly, there is a group of related conditions that cause connective tissue fragility.18 The symptom they mostly have in common is some degree of hypermobility, but they are also strongly associated with unexplained chronic widespread pain19 — exactly the kinds of symptoms that fascial therapy is supposedly good for.
These conditions are rarely diagnosed, and most patients with these conditions don’t know what’s wrong.20 But what happens if you try to “release” their fascia? Or, eek, “blast” it? Probably nothing good! I shudder to think how many patients like this have been subjected to intense fascial therapy when they quite literally needed exactly the opposite.
For more information, see Hypermobility and Ehlers-Danlos syndrome: In patients with persistent and widespread muscle pain.
The fascia whisperers: more about gentle fascial release
Subtler fascial therapy has unclear origins and an even murkier rationale than “traditional” FDM-inspired therapy. Although it mostly shares the fundamental goal of fixing “deformed” fascia, it takes a decisive leap away from the Typaldos legacy by proposing that fascial deformations can be repaired by just the right gentle manipulations, by working “smart” rather than hard. Vitalism looms in the background, and many therapists blur the differences between gentle fascial manipulation and “energy work” (see the meridians/acupuncture section below).
There’s nothing to this idea that can’t be chalked up to an all-too-human breakdown of humility.
There is no evidence or any reason to suspect that the state of fascia can be changed even by forceful manual therapy, let alone delicate manipulations. There is no way to think it can be changed gently without faith.
It’s not completely implausible that skilful, gentle manipulations could have an effect on fascia, but there is absolutely no reason to believe it — or believe that it matters therapeutically — just because some massage therapists say it’s so.
Why fascia actually matters medically (get ready to cringe)
All theories and controversies aside, what is the clinical significance of fascia in mainstream medicine? Why would a family doctor or surgeon ever think about fascia? There’s the connective tissue diseases, of course — such as the hypermobility disorders just mentioned above (Ehlers–Danlos syndrome), as well as more obvious ones like Marfan syndrome. But what about the biological role of fascia in healthy people?
In healthy people, fascia is boring but critical: it functions as an important infection barrier. Much like skin prevents pathogens from getting into the body in the first place, layers of fascia limit their spread.21
But there’s a dark side to this vital function — one of the most unpleasant phenomena in all of medicine (which is saying something). If fascia stops the spread of disease, what happens behind the barrier? Well, it can get grim: a blocked infection is also a trapped infection, which can destroy a compartment, with dire consequences.
Things tanked even further once I was on the table. And when I lost blood pressure during the surgery due to the complications of compartment syndrome, the doctor made a real-time call and amputated my arm just above the elbow. He later told me it all boiled down to a choice … between a life and a limb.
“Just a Flesh Wound”, O’Brien (Milesobrien.com)
Now that is clinical relevance. That’s how the properties of fascia medically matter — its toughness as a wrapping, primarily.
Some people leap from here to the idea that people who get compartment syndrome must have something wrong with their fascia — too tough, too tight, needs release to prevent further compartment syndromes. And that might sound like extremely reasonable clinical reasoning to some people, and indeed it’s a reasonable enough hypothesis on its face. But you have to check these things, and someone did, and it’s just not true.23 (And if it’s not true of something like compartment syndrome, it’s probably not true of subtler problems either.)
Perhaps there are subtler fascial properties that also matter. But keep this life-or-death example in mind as we look at why massage therapists and chiropractors think fascia might medically matter, starting with the most dubious ideas …
Part 2
Sloppy fascia reasoning
The next few sections dissect ideas about fascia that are unusually weak, either based on especially irrelevant science or just none — the stuff that doesn’t really stand up to any scrutiny at all. Despite that, many of these ideas are extremely popular, so it’s important to deal with them, even if none of them are good representatives of fascia science. After making short work of these, I’ll get into some more credible fascia science.
One quick pre-emptive rebuttal first: am I attacking “straw men” here? Easy targets that don’t actually represent meaningful beliefs about fascia? No: a straw man would be an idea that no one actually believes or takes seriously — and therefore meaningless to criticize. Certainly not everyone interested in fascia thinks that things like fascial piezeoelectricity or fascial “fuzz” are real or important. However, enough do that it’s no straw man! It may not represent the best thinking in the field, but it is definitely out there in force. This joke would be meaningless if it weren’t (I had a nice meme of this, but removed it due to copyright concern) …
A couple people are standing at someone’s front door, holding a book, and they look like Jehovah’s Witnesses, or some other kind of proselytizers. The man is saying, “Excuse me, but do you believe in the power of fascia?”
Electrified by piezoelectricity
The piezoelectric effect is an electric charge generated by flexing crystals. It’s a popular notion that this fascinating property of crystals is at work in fascia, and that it’s the mechanism for fascial “release.” These ideas have never been more than speculation. The first is possible but unproven. The second goes much too far and is demonstrably false and clearly contradicted by modern researchers, including noted fascia researcher Robert Schleip (more below).
Crystalline properties are a firm pre-requisite for piezoelectricity. To get a piezoelectric “spark,” you have to have crystals. In the famous 1987 book Job’s Body — which I read three times, back in the day — Juhan proposes that connective tissue may behave like a “liquid crystal.”24 A strong emphasis on may: this has never actually been shown to be the case. Juhan was speculating. This doesn’t mean that there is no piezoelectric effect in fascia, and there are plenty of problems with the idea, but it’s not totally out to lunch. We do know that piezoelectricity “sparks” fly when bone is flexed and stressed, and this guides the slow remodelling of bone,25 which is super cool. It’s a terribly clever system!
It’s also a great example of a clinically irrelevant biological property. It has nothing to do with anything a manual therapist could ever do to a bone. It is beautifully evolved to change bone extremely slowly in response to extremely specific stimuli which, presumably, cannot remotely be simulated by manual therapy. Trying to affect that system with your hands is quite futile. That’s going to be the case for the great majority of physiological systems, known and unknown — even if you understand them, it doesn’t mean you can use them, or affect them with your hands.
Maybe fascia does something similar to bone with piezeoelectric effect. It wouldn’t “shock” me. But no one has ever demonstrated that it actually does. Indeed, no one has even tried to find that property of fascia, as far as I can tell.
Some people have run with the idea like it’s a proven fact, though. For instance, James Oschman stated unequivocally and overconfidently that “connective tissue is piezoelectric,” a fact that can be used as a firm foundation for the further speculation that it accounts for the fascial “releases.”26
And it’s simply inconsistent with the reality of fascial plasticity, which we do know quite a lot about. There’s no point in speculating about how fascia responds quickly to manipulation, because it can’t and doesn’t: it’s too tough and slow-changing.27 In contrast to the total absence of research into fascial piezeoelectricity, the properties of fascial plasticity are well studied, and there simply is no short term change in fascia to explain! It can’t respond to the pressures of massage therapy any more than bone can. In addition to the footnote, this will be substantiated in various ways throughout the rest of the article.
Could piezoelectricity be at work in some other way in fascia? Anything’s possible. But now we’re cruising into pure guess work. Do we know anything at all about it, let alone the physiological intricacies of such a phenomenon? Do we know why it evolved? What it does, how it does it? Can we affect it? And, if we don’t know these things, how can we possibly use it to devise a reliable therapy? Obviously we cannot.
Fuzzy logic: Gil Hedley’s “fuzz” speech

Another fine example of imprecise scientific enthusiasm is Gil Hedley’s extremely popular “fuzz” speech. In this video with a bazillion views, Hedley plays fast and loose with a dissection observation: there are cobwebby layers of fine, loose connective tissue between thicker sheets of fascia. The anatomy is interesting — anatomy is always interesting — but Gil Hedley’s interpretations are dubious. His leaps of logic are charismatic, but also large and precarious.
“That stiff feeling you have is the solidifying of the fuzz,” Hedley confidently explains. He thoroughly makes the case that fuzz explains the sensation of stiffness.
At best, that is an unsafe assumption! And one that blithely ignores many well-established explanations for the sensation of stiffness, and other highly relevant factors — like the fact that he’s looking at a dead person. He does not know what happens to that tissue in a living body. In fact, that fuzzy texture only manifests post mortem — according to biotensegrity expert, Dr. Steven Levin.28 This is a very interesting passage, worth reading carefully, but note the emphasized phrase particularly:
In Guimberteau’s video, ‘Strolling Under The Skin’, what you see there is that the ‘fuzzy’ stuff is really dynamic tissue that is under constant change. Tissues don’t ‘slide’, there is no shear, they reconfigure with each movement. The dynamics of a cell ceases with death. Ca++ [calcium ions] flood into the cell and it stiffens — that’s rigor mortis. It starts within minutes of death, as soon as the circulating ATP [energy molecule] runs out. The ‘fuzz’ is connective tissue that is stiffened during rigor mortis, and it doesn’t happen unless you die. It occurs within minutes of death, and you can almost watch it happen. It is like snot hardening. The mucus booger that comes out of your nose quickly hardens and becomes quite stiff; at death, the mucus that connects all our tissues, does the same.
All that ‘melting the fuzz’ is conjecture based on misinterpreted observations on dead tissue. Even so called “fresh” cadavers are but poor players in the game of life.
Almost any amount of normal movement is sufficient to sustain a normal range of motion. “Fuzz solidification” — also often called “adhesions” — either isn’t happening or doesn’t matter, because it’s effortless to move through. Also, there are other explanations for the sensation of stiffness: better, evidence-based, and un-fuzzy explanations. I discuss them in some detail in Why Do Muscles Feel Stiff and Tight?
“Fascial distortions,” especially tightness (contracture) and stuckness (adhesions)
At the heart of most fascial therapy lurks the extremely vague idea that something is wrong with your fascia. This is explicitly the Big Idea in the modality that started it all in 1991, the Fascial Distortion Model, and it is had been recycled extensively ever since. Again, physician Stephen Typaldos proposed that many if not most musculoskeletal complaints are caused by deformations of fascia, and he thought he could repair these with his hands. Most modern modalities are based on this, and in turn it is based on … nothing at all.
This idea is not fascia science but just pure speculation about fascia. There is nothing even close to any biology to back it up,29 so it can’t be a candidate for potentially important fascia science: I cannot emphasize strongly enough that it’s just an idea someone had once. I’ll examine it only briefly, because there is so little to examine. But for those who want to delve, there is a formal paper critiquing fascial distortions, by Christoph Thalhamer.
How might fascia be “distorted” exactly? Supposedly some people’s fascia is like poorly maintained ship’s rigging, too tight or short in some places, too loose in others. Or perhaps maybe it’s stuck (“adhesions”), or lumpy, or frayed, or too thick, or too thin.
Virtually any idea you’ve ever heard about what might be wrong with fascia can and has been included in the idea of “fascial distortion,” but tight and/or stuck are the main ones. Those informal terms correspond loosely to the more technical concepts of contracture and adhesions.
There is no evidence that these things actually happens without frank pathology, or — even if they do — that they would be either clinically significant and/or treatable with anyone’s clever hands.
Contracture is certainly a real phenomenon: it’s the pathological shortening of tissue. For instance, Dupuytren’s Contracture is a mysterious contracture of the fascia of the hand, but even in the early stages it’s obvious that something’s wrong: the hand starts to claw up! This is probably the most obvious problem with idea of fascial distortions: if they happened, they’d be more obvious, just like the other known examples of pathological contracture.
It’s also worth noting that Dupuytren’s contracture isn’t even a very painful condition, even as it actually deforms the hand and significantly restricts range of motion: it’s just restrictive. So the idea that much less obvious contractures are the cause of most/all painful musculoskeletal problems is a mighty reach.
Adhesion is a little murkier than contracture. There’s not much doubt that it occurs — there are clear mechanisms by which layers of connective tissue get “sticky” and tend to cling to each other — but it’s probably either trivial or pathological and beyond the powers of manual therapists to deal with. The idea of adhesions that are both important to our musculoskeletal health, and which can be treated by “releasing” them, has never been validated.
Ida’s idea about thixotropy
A shabby, decades-old idea is still often seriously cited as the explanation for how fascial therapy works: because it softens fascia with “thixotropic effect.” The idea came from Ida Rolf (founder of “Rolfing”). Fascia researcher Robert Schleip:30
Many of the current training schools which focus on myofascial treatment have been profoundly influenced by Rolf (1977). In her own work Rolf applied considerable manual or elbow pressure to fascial sheets in order to change their density and arrangement. Rolf’s own explanation was that connective tissue is a colloidal substance in which the ground substance can be influenced by the application of energy (heat or mechanical pressure) to change its aggregate form from a more dense ‘gel’ state to a more fluid ‘sol’ state.
A quick look at how thixotropy works in human physiology shows that this just doesn’t add up. The thixotropic effect is nifty physiology, but it’s not a therapeutic effect in itself, nor is it the mechanism of one. Ida’s idea was wrong. And, in Ida’s defense, she knew it was! In fact, she later called it nonsense herself!31 That said, however much Ms. Rolf may have wised up over the years, she did a lot of damage with ideas like this in her prime, producing far too many of them, and many refuse to die.32
Thixotropy is an obscure physical property of certain slimy body fluids that get thinner when agitated or stressed. You can easily observe thixotropic effect in beach sand, near the water’s edge: stamp your feet in the sand, and it starts to liquify.
Thixotropic fluids in the human body include synovial fluid in joints, mucus, semen, and the gelatinous and poorly-named goo called “ground substance” — the stuff that gristly connective tissue fibres are embedded in like bits of coconut in Jello. Ground substance is the most plentiful thixotropic substance in the body.
But thixotropy is minor, slow, and temporary, and fascia is too tough to change.
Fascial sheets are incredibly tough, and you can’t “change their density and arrangement” quickly or easily. And thixotropy just isn’t fast enough to explain the relatively speedy, dramatic effects on tissues that therapists claim to achieve. Dr. Schleip: “either much longer amounts of time or significantly more force are required for permanent deformation of dense connective tissues.”33 Thixotropy might slowly make fascia more pliable, but not stretchier. If thixotropy had the power to increase the extensibility of connective tissue, then we would become obviously more flexible just from sitting in a sauna — I’ve tested this repeatedly and never observed any increase in flexibility just from being hot.34
Even if it works in some small way, thixotropic effect is going to be temporary, fading within seconds or minutes after hands are removed.
Last but not least, thixotropic effect is simply a minor effect. It’s occurring a little bit all the time, with or without massage. Massage surely does induce it a little, but just as surely much less than ordinary physical activity — like with circulation. Massage therapists are very fond of claiming that massage “increases circulation,” but the effect is much smaller than what exercise does!35 Perspective matters. And another similar thought experiment: if sustained pressures or shearing could significantly change connective tissue, then working in a chair all day long — or any prolonged postural stress — would also deform your fascia.
The idea of thixotropy is hardly state-of-the-art thinking about fascia, but it is certainly still prevalent among therapists practicing fascially-focused therapy, and trying to explain what they do. Unfortunately, it was never a good idea in the first place, even decades ago.
The acupuncture connection: is fascia actually magic?
Another disconcertingly popular notion about why fascia matters is that the meridians of Chinese medicine correspond directly to fascial anatomy and function. If you polled therapists doing fascial manipulation, I think you would find that a great many believe that they are doing the same thing that an acupuncturist is doing — just in a different way. They believe that fascial therapy works for the same reasons acupuncture works.
Indeed, most fascial therapists probably believe that acupuncture works. And therein lies the problem. Unfortunately for fascial release therapy, acupuncture is not a good ally: it has been failing many fair, good quality scientific tests for years now, and is simply not what it seems to be.
Acupuncture as we know it today is not so ancient after all: its current form is a modern (not ancient) invention of the pediatrician Cheng Dan’an (承淡安, 1899-1957) in the early 1930s.3637 Before that, for most of history, it existed primarily as a method of bloodletting — much like the prescientific medieval European practice. And then there’s the myth of acupuncture’s popularity.38 Even its alleged popularity and widespread use in China is trumped up — it is, for instance, not actually used for anaesthesia,39 despite widespread belief in this phenomenon.
These are embarrassing facts for acupuncture. All of this and more is discussed in more detail (and heavily referenced) in my main acupuncture article:
I was not a skeptic about acupuncture originally. I came to this position only after a long, uncomfortable period of education and gradually eroding faith. But I now accept that acupuncture is obsolete Eastern folk medicine propped up by Western hype and wishful thinking.
Therefore, the proposed association between “fascial meridians” and the “chi meridians” of traditional Chinese medicine is meaningless. Even if meridians and all the other rubric of acupuncture were real, acupuncturists are unable to demonstrate their power clearly: their needles are consistently no more helpful than placebos.40 Even pro-acupuncture researchers have repeatedly admitted that the effect of the needles is small at best. And if the acupuncturists can’t manipulate these meridians effectively enough to achieve clearly measurable effects, why would pulling on fascia be able to do it?
Acupuncture lore has no business in a serious discussion about fascia and its possible importance in therapy.
Not so exotic after all
Piezoelectricity, fuzz, thixotropy, and fascial meridians are four good examples of popular but poor reasons why fascia supposedly matters. There are other better reasons, and discussion of genuine fascia science is coming up. But first I want to make it clear that common fascia talk often fails to even reach the level of being “science-y.” Despite all the talk of exotic properties of fascia, fascia’s clinical importance is usually expressed only in terms of a couple extremely simplistic rationales, which don’t seem exotic at all:
- it’s everywhere and connects everything (well, yeah),
- and it gets tight (not clear, see below).
A strong theme in fascial therapy is the emphasis on the interconnectedness of anatomy via fascia, always making the point that pulling on any one part of fascia affects the whole body, like pulling on the corner of a sweater affects all the threads. (That sweater analogy appears virtually everywhere online that fascia is mentioned. It gets really tiresome, actually. Didn’t think it mattered much ten years ago. Still don’t.)
The main idea of fascial therapy is that the stuff can get tight and restrictive, like clothing a size too small, and needs to be “released,” and that therapists can achieve this by various methods of yanking on it. The yanking may be extremely intense, too — some flavours of fascial therapy are among the most painful of all hands-on techniques.41
And that’s what fascial therapy boils down to most of the time, in the wild. I have personally encountered lots of talking about fascia that is exactly this rudimentary … and even worse, like the example I quoted in the introduction — “The fascia will make everything better!” Many therapists are perfectly capable of discussing the topic more intelligently, of course, but low quality reasoning and communication about fascia is distressingly common (and my exposure is quite extensive, due to the large volume of email I receive).
Consider this gem of simplistic rationalization:
Restricted fascia is full of pockets. When the tissue starts to release, these pockets are opened up. When these pockets open, the sensations that were trapped in them are released.
Such overconfident, poor quality clinical reasoning isn’t universal — just excessively common within the culture of fascia enthusiasts.
Now, let’s get to some real fascia science.
The greatest enemy of knowledge is not ignorance, it is the illusion of knowledge.
Stephen Hawking
Can fascial therapy help COVID patients?

No, fascial therapy absolutely cannot help COVID patients in any important way. However, fascial therapy proponents have jumped on the COVID bandwagon, claiming to be able to help, just like so many other types of alternative medicine.
This is one of the dumbest things I have ever read (in a supposedly scientific journal), and it’s a glaring example of just how distorted and biased clinical reasoning about fascia has become:
“Based on available evidence this paper suggests that the Corona virus travels upon the highway that is the fascial singularity whence it permeates cells on a local and global level. A significant number of post-COVID-19 patients will experience on-going fascia related pain and a wide range of functional issues. Based on current research this short report proposes that appropriate fascia focused manual and movement therapy interventions will assist patients in recovering from the COVID-19.”
This is fascia fetishization at its most out of touch with reality. Specifically what’s bonkers here is the baseless, self-serving, hyperbolic conceit that fascia is pathologically important in COVID and then the spectacular leap to the claim that therefore fascial therapy can help COVID patients.
It is outrageous and disturbing that such embarrassing drivel has an audience — but clearly it does.
Part 3
Real fascia science that supposedly matters
Fascia is much too tough to “release”
“Manual therapists need not feel threatened by the news that we cannot stretch fascia.”
If We Cannot Stretch Fascia, What Are We Doing? Alice Sanvito, Massage Therapist
My original challenge to readers (in the fall of 2011) to suggest fascia science that supports fascial therapy was kicked off with a fine example: one that is just about the exact opposite of what I asked for, undermining the clinical relevance of fascia rather than supporting it. Despite the extraordinary number of comments I received on early versions of this article, few readers answered my challenge directly. Of the handful of scientific papers that were suggested to me, this was the most “interesting”:
The Chaudhry et al. article is indeed “clinically relevant” to fascial therapy … but not in a supportive way. This fascia science actually contradicts the big idea of fascial therapy.
The main point of manipulating fascia42 is to physically change it in some way — to achieve what is usually described as a “release.” Although the concept of release may correspond to some other physiological phenomenon — another discussion — it certainly cannot be explained in general by physically changing the fascia.
What Chaudhry and colleagues showed is that fascia is much too tough to “release" (mechanical deformation43) by stretching it. Although they oddly imply in their summary that it might be possible to do so with the superficial nasal fascia, the main text of the paper makes it clear that even that thin tissue is extremely tough, and would only mechanically deform if subjected to surprisingly intense forces. This is consistent with well-established properties of fascia, namely that it’s extremely tough stuff. Collagen is like that.
If I could write my own conclusion to this paper, it would go more like this:
CONCLUSION: You cannot change the structure of fascia, because it is tougher than Kevlar. If the stuff were thicker, people would be bulletproof.44
CLINICAL IMPLICATIONS: If you want to physically change someone’s fascia by force, you’re going to have to get medieval. This directly contradicts a major popular rationale for fascial manipulation.
This paper is only clinically relevant to fascial therapy insofar as it presents evidence that discourages and undermines existing common practices and beliefs. Therefore, perhaps it was a poor choice to cite it in this context.
It’s also just old news that fascia is too tough to change. For instance, Dr. Robert Schleip debunked the idea in his 2003 paper about fascial plasticity, and if you don’t take his word for it — a well-respected fascia researcher — then whose opinion would be credible enough? He dismisses the traditional explanations of thixotropy and piezoelectric-effect-mediated adaptation, and thoroughly describes fascial toughness. He concludes that plastic fascial change in response to moderate loading is “impossible to conceive.”45
As strongly stated as that may be, I’ll go even further. Dr. Schleip (and virtually everyone else) assumes that “release” is a real thing that needs explaining. I’m not so sure …

“Release” may not even be real
The idea of a “release” refers to the yielding of tissue to an externally applied pressure. It’s the goal of fascial therapy, but it’s more poetry than biology. It does not refer to any known, specific state of soft tissue. It’s vague massage-speak for “better in some way, hopefully for more than ten minutes.” As commonly used, the word strongly suggests an actual change in the flesh … but this assumption derives only from blurry, erratic sensory cues.
Most therapists say — not all of them, importantly, but most — that they can feel tissue changing texture as they work, but that could easily be misinterpreted muscle behaviour and palpatory pareidolia. Patients talk about releasing too: they may experience a kaleidoscopic array of sensations during massage, and call it a release if they perceive an especially significant improvement (from feeling “stuck” to feeling “relieved,” say). But we have almost no idea what any of these sensations imply about tissue state, if anything. People also have profound shifts in sensation from a good back scratch, fervent prayer, and eating cheesecake!
Let’s define release a little more precisely. In the context of fascial therapy, a “release” is:
- a palpable, relatively quick change in tissue texture
- clinically meaningful (makes some kind of real difference to the patient)
- somewhat lasting (if it didn’t last, what would be the point?)
- somewhat predictable (that is, it’s happening because of treatment)
And fascial therapists more or less unanimously assume that it’s fascia, specifically, that is doing the releasing.
No doubt the first thing — a quick change in texture — happens in the course of manual therapy. It is not safe to assume the rest, though. And what’s left of the concept of a release if you take away the clinically meaningful, lasting, and predictable parts? What if it’s just a change in texture, a bit of movement under the skin?
In my many years working as a massage therapist, I felt various and sundry ripplings, twitchings, and shifts under the skin. But in order to qualify as “releases,” those movements should have correlated strongly with my intentions and with the patient’s experience. Sometimes they did, but often they did not. So I always thought they were really quite random, occurring with great variety pretty much no matter what I did, or what patients reported.46 So while I certainly felt something change, I rarely thought of those changes as a meaningful “release.”
Dr. Schleip’s 2003 paper about fascial plasticity47 basically just said that fascia is too tough to change, but muscle may react to touch and pressures, and that this is probably mediated by sensory nerve endings in all soft tissues. In other words, people react when poked and prodded, which doesn’t have anything to do with fascia in particular, which has some nerves in it just like everything else. We have no idea whether or not any of that actually constitutes a meaningful mechanism for a “therapy.” I can also make someone twitch their quadriceps by bonking their patellar tendon: does it matter, other than as a test of the reflex itself?
Most releases are probably just trivial tissue “noise” in the hands-on experience, not a pivotal event in therapy. Or, if they are more meaningful, they are nearly impossible to interpret. It’s not that nothing’s going on, it’s that nothing in particular, knowable, and helpful is going on. But we round it up to something more specific and definite and meaningful, an oversimplification that is more poetic than biologic. I have no objection to using “release” as a description of an experience, but I think it is misleading to pretend that it describes a particular biological event with clinical meaning and value — which is exactly how most therapists imagine it. Why? A thick stew of good intentions, ego, and the human habit of selective perception and imposing simplistic explanations on chaotic systems.
Study of rat gut massage is not really fascia science
Our first serious candidate for relevant fascia science has often been suggested to me as an example of evidence of “fascial release”… of rat guts. But the connection to fascia here is weak.
In this odd rat study, Susan Chappele and Geoffrey Bove tested the effect of “visceral massage” on rat intestines. For context, visceral massage is often perceived as being about fascial manipulation, without much justification, or perhaps any at all. For better or worse, many massage therapists believe that visceral massage is all about releasing adhesions, and that’s the main reason this study is widely regarded as “fascia science.”
Rats were harmed in the making of this science: they were subjected to abominal surgery (an emulation of “running of the bowel,” which is examining the entire bowel for abnormalities). The point of this was to see if the massage would prevent a common post-surgical complication: postoperative ileus, AKA impaired bowel motility, AKA constipation. The poop chute gets balky. This is a real thing that happens to both rats and humans after abdominal surgery, usually temporary, but occasionally more serious and long-lasting.
And apparently massage helped: the treatment “reduced experimental postoperative ileus.” The treated rats had “increased gastrointestinal transit and reduced time to first fecal pellet discharge,” and fewer inflammatory cells in their GI tract. The authors speculate that reducing inflammation may be the mechanism. Chapelle and Bove were so confident in their conclusion that they baked the good news right into the title.
Since then,
The alleged importance of the study is that it demonstrates a meaningful biological effect on fascial tissue. If it’s demonstrable in rats, maybe it’s helpful in humans too? And there might be other effects with more practical clinical implications than trying to reduce post-surgical adhesions.48 That’s fair enough as optimistic speculation, but it is very clearly just optimistic speculation, based on the results of one study of rat gut massage.
And even that speculation has problems. Off the top of my head:
- The paper does not actually report an effect on fascial tissue or adhesions. (It discusses the speculative potential of massage to prevent adhesions: if it reduces post-operative ileus, then it might reduce adhesions.) So it’s not actually clear why anyone would assume that it constitutes evidence of an effect on adhesions/connective tissue, other than just plain wishful thinking and ignoring the details.
- It’s questionable whether massage helped these rats recover by “reducing inflammation.” There’s no good evidence that massage reduces inflammation in any context.49 While they reported, “decreased … numbers of intraperitoneal inflammatory cells,” that is hardly confirmation that massage reduces acute bowel inflammation. This study was not designed to detect changes in pathology (it couldn’t be in principle, because the pathology of ileus is so poorly understood, and you can’t measure meaningul changes in a process no one actually understands).
- Even if massage did help the rats by reducing bowel inflammation, it’s unlikely that this effect is going to be demonstrable anywhere else. Postoperative ileus is a unique phenomenon, specific to bowels that have just been surgically disturbed, and it’s mysterious: we just don’t know why it happens (but it’s certainly not because of adhesions). If massage does indeed help it, we have no idea why, and there’s really no reason to think it has anything to do with how massage affects anything else — and certainly not “fascia” specifically!
- The results are actually quite unsurprising, because we know that there are other easy ways to ease ileus. According to a 2013 study published shortly after Chapelle et al., chewing gum also does the job, just by stimulating bowel contractions.50 This casts strong doubt on the specialness and clinical utility of massage for the same purpose. To be clinically useful, a massage technique should accomplish something that is not otherwise easily accomplished. If chewing gum works, the only reason to add massage is if it’s significantly better somehow — which is conceivable, but simply unknown.
- Abdominal massage for any reason is rarely practiced in general — few patients seek it out, therapists rarely offer it — and massage to prevent post-operative ileus is a special case that most massage therapists have never tried and would probably wisely avoid for safety reasons. There’s no direct clinical relevance of the results because, in the real world, massage therapists almost never do to humans what the researchers did to rats … and they shouldn’t try to, either, because there is not and may never be enough evidence on this topic to justify it.
It’s nice to think massage might help get the bowel moving again after abdominal surgery, but I don’t see how it counts as “fascia science.” It does not show any effect that has anything whatsoever to do with fascia. You could argue that it’s clinically relevant to massage therapy, insofar as it suggests something good that massage might do … but I fail to see how it suggests that anyone should be trying to massage fascia. This is mildly interesting massage science, not fascia science. It definitely does not constitute evidence of an effect of manipulation on connective tissue at all, let alone one that is robust and relevant to common aches and pains and the day-to-day work of most manual therapists.
Does stimulating fascia reduce post-exercise muscle soreness?
Perhaps … but the clinical relevance of this data is tenuous at best — so low that I would never normally be interested in this paper. In fact, I would never have chosen to read it myself, because I don’t think it’s good enough science. I spent some time on it only as an gesture of good faith to a critic, who supplied the paper as an example of basic fascia science that matters. It was probably not a good choice for that purpose.
This is a test tube study showing that naked cells handled stress better (fewer signs of harm) if they were treated with “simulated myofascial release” (MFR). A meaningful, accurate simulation of manual therapy on naked cells is an amusing notion, and it’s clear that what happened to those cells differs dramatically from what would happen in a real living body.
Even if true and reproducible, this data would mainly support the rationale for MFR specifically for post-exercise soreness — something of a dead end for clinical relevance, because exercise-induced soreness has little to do with the main claims of fascial release therapy, which primarily concerns correcting postural asymmetries, eliminating alleged restrictions, and treating chronic pain.
Post-exercise soreness is comparatively trivial, and patients usually don’t seek therapy for it.51 There’s a lot of research showing that exercise-induced soreness is basically invincible anyway.52 For this property of fascia to be clinically relevant, it would have to imply that MFR might be able to treat chronic pain from other causes … not the transient annoyance of soreness after a game of soccer.
This isn’t a rejection of all possible clinical relevance of the data. My point is that there are so many problems that its relevance is watered down to quite a thin sauce — way too thin.
I do concede that the paper shows some evidence that fibroblasts have interesting and perhaps positive responses to mechanical forces. That is inherently interesting biology, and perhaps well worth investigating further — but it’s a long reach to postulate any clinical relevance to what most therapists do, most of the time, with patients’ fascia.
“Reach” is what the authors do, however. I suspect they are deeply interested in validating the notion that “fascia is important,” because they seem to be seeking evidence to support their pre-conceptions — typical of The National Center for Complementary and Integrative Health-funded research, and a hallmark of low quality science. It’s quite likely that if neutral researchers — with no interest in fascial therapy — did this experiment they would not get or report the same results.
The fascia article has always been a particularly dorky article. Most people who are fascinated by fascia aren’t interested in my “negativity,” and not many patients are all that “fascia-nated” to begin with. The audience for the details is the prototypical ideal reader of this website: people who are just really interested in the science of therapy for pain, like I am. If you’ve read this far, you’ve gotten the gist: fascia isn’t exactly all it’s cracked up to be. But there is a lot more scientific detail available for my premium subscribers.
The entire article is a small book at about 32,000 words; I have set aside about 6,000 of them for members: about 25 minutes of extra reading. Everything I explore in detail for members is summarized below.
Most PainScience.com content is free and always will be.? Membership unlocks extra content like this for USD $5/month, and includes much more:
Almost everything on PainScience.com is free, including most blog posts, hundreds of articles, and large parts of articles that have member-areas. Member areas typically contain content that is interesting but less essential — dorky digressions, and extra detail that any keen reader would enjoy, but which the average visitor can take or leave.
PainScience.com is 100% reader-supported by memberships, book sales, and donations. That’s what keep the lights on and allow me to publish everything else (without ads).
- → access to many members-only sections of articles +
And more coming. This is a new program as of late 2021. I have created twelve large members-only areas so far — about 40,000 words, a small book’s worth. Articles with large chunks of exclusive content are:
- Quite a Stretch
- Does Epsom Salt Work?
- Heat for Pain and Rehab
- Your Back Is Not Out of Alignment
- Trigger Point Doubts
- Does Fascia Matter?
- Anxiety & Chronic Pain
- Does Massage Therapy Work?
- Does Posture Matter?
- A Deep Dive into Delayed-Onset Muscle Soreness
- Does Ultrasound or Shockwave Therapy Work?
- A Painful Biological Glitch that Causes Pointless Inflammation
- Guide to Repetitive Strain Injuries
- Chronic, Subtle, Systemic Inflammation
- Vitamins, Minerals & Supplements for Pain & Healing
- Reviews of Pain Professions
- Articles with smaller members sections (more still being added):
- → audio versions of many articles +
There are audio versions of five classic, big PainSci articles, which are available to both members and e-boxed set customers, or on request for visually impaired visitors, email me. See the Audio page. ❐
I also started recording audio versions of some blog posts for members in early 2022. These are shorter, and will soon greatly outnumber the audio versions of the featured articles.
- → premium subscription to the PainSci Updates newsletter +Sign-up to get the salamander in your inbox, 0–3 posts per week, mostly short, sometimes huge. You can sign-up for free and get most of them; members get more and their own RSS feed. The blog has existed for well over a decade now, and there are over a thousand posts in the library. ❐

Change or cancel plans any time. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism. For more information, see the membership page. ❐
PREVIEW: Headings in the members-only area…
- A fascinating etymological digression: are “fascia” and “fascism” related?
- Does it matter that fascia contains muscle cells?
- Fascia strong like bull! Or … mouse?
- Do weak fascial contractions matter?
- No clinical relevance at all? Not even a teensy bit?
- Is fascial contraction even interesting?
- What does Dr. Schleip think?
- Thicker, stiffer thoracolumbar fascia in back pain: what does it mean?
A fascinating etymological digression: are “fascia” and “fascism” related?

A Roman and his fascis. He also has a bunch of fascia & fascicles.
The words fascia and fascism are indeed closely related. They both come from the Latin word fascis, which first referred to leather straps, then to a bundle of sticks held together by those straps, and then a bundle that includes an axe. The fascis represented strength in numbers, and it is extremely old imagery: it emerged from the Etruscan civilization well before the Ancient Romans adopted it as a symbol of political power, law, and jurisdiction. They made it a physical thing, toted around by some actual Romans, the lictors, the bodyguards of magistrates.
The fascis limped into the modern world as an abstract symbol of collective action, which was notoriously revitalized by the National Fascist Party in Italy in 1921: the National Strength-In-Numbers Party, in other words. But it was eclipsed by another symbol of fascism from the ancient world, the swastika, and today hardly anyone recognizes a fascis, even though it persists in all kinds of political and military iconography, despite the negative associations. “How the fasces survived is a mystery: Americans are sensitive, if not hypersensitive, to any potential endorsement of an enemy’s culture, language, or creed in times of war.”
The fascis is the spittin’ image of a bundle of muscle cells wrapped in connective tissue, and so we call that a fascicle, wrapped in fascia — the canonical example of fascia in the human body. A fascis only symbolized strength in numbers, but it is the literal purpose and function of a fascicle.
That’s a whole bunch of linguistic and conceptual convergence.
Etymologically rich trash talk
Skeptics about the clinical significance of fascia sometimes snarkily refer to fascia enthusiasts as “fascia-ists,” which is mostly intended as the cheap pun it sounds like. But its etymological roots go as deep as history, and the insult is much more apt than they realize: it references the empty populism of fascism, suggesting that advocates for fascial therapy have nothing going for their claims except strength in numbers.

Fasces are used everywhere in the imagery of power, but the strongest link to fascism is in the symbol of Italy’s National Fascist Party, founded in 1921.
And what about “fascinate”?
That word similarity actually is just a coincience. Or is it?
Fascination is closely related to enchantment and still strongly connotes a magical effect: to be fascinated is to have one’s attention captured, as if under a spell. In ancient times, it was meant more literally. The Latin fascinum was a phallus-shaped amulet, a penis charm, and to “fascinate” was to use the power of the fascinum to enchant or bewitch. And what’s more enchanting than a penis, amiright? The Romans were really into their penis power, and I can’t imagine anything more Roman than superstitiously wearing a little cock-and-balls around your neck.
So this word similarity seems like a coincidence, but… I can’t help but notice that a fascis is also a rather phallic symbol. To a Roman, the fascis and fascinum might well have seemed like siblings, each broadly symbolizing potency, just in different contexts with different connotations.
Accuracy disclaimer
This is all oversimplified to the brink of error, but history and etymology are messy, and there’s just too much detail and nuance and uncertainty to ever really get this kind of thing truly complete and correct. For instance, it’s not even clear whether it’s a “fascis” or a “fasces,” each one being used by credible sources. If I have readers with relevant expertise, please set me straight.
Does it matter that fascia contains muscle cells?
The next example of fascia science was suggested to me by Gil Hedley. Since he clearly believed me to be ignorant of fascia science and in dire need of educating, I asked him to recommend some reading to me — a favourite paper showing something interesting and clinically relevant about fascia. As expected, he recommended a paper I was already familiar with, because it is something of a classic of fascia science: Robert Schleip’s 2006 dissertation on the contractile properties of fascia. Much more interesting stuff than the previous two examples. I will get into much more detail about this paper than the first two.
Schleip and colleagues convincingly showed that fascia contains muscle cells — sort of53 — and that they can contract, slowly and weakly. That is undeniably interesting biology! But the point of this analysis is to ask: Does it even matter whether it’s right or wrong? Is it clinically relevant? Does it improve how we do therapy? Can we use the knowledge to affect the body with hands? That is the question.
It is also a question that Dr. Schleip and his colleagues have addressed themelves on their website, FasciaResearch.de. What follows is my own analysis, which is generally consistent with theirs. However, interested readers should definitely have a look at their article: it is readable and chock full of useful perspective, answering questions like “Does fascia contract in response to emotional stress?” and “Can fascia contract on its own?”
Important update: Dr. Schleip has read this article and corresponded with me about it amiably, and expressed clear agreement with my main point. Although he also had some thoughtful criticisms, we agree on what matters, and he shares my frustration with clinical overconfidence in fascia. I invited him to make a statement for my readers about this: look for it at the end of this part of the discussion.
Fascia strong like bull! Or … mouse?
Before we get to clinical relevance, I’ll quickly explain what Schleip et al. found: a slightly muscular cell in rat fascia, which they described as “rather unexpected.”54 They also tried out various methods of stimulating them in vitro (test tube) and found that, by golly, those muscle cells did what muscle cells do: they contracted! Slow, weak contractions. But they contracted.

Perspective
By any measure, fascial contractions are dramatically less powerful than muscular contractions. If anything, this diagram gives far too much credit to the power of fascia, which would barely register at all if depicted more accurately.
It’s certainly not difficult research to understand.
Some important context that fascia fans will appreciate: for a long time, fascia was and often still is incorrectly thought of as a fairly lifeless, inert substance, the Saran Wrap of biology. I still hear various educated people referring to it in this way. However, massage therapists and chiropractors (in particular) are prone to swinging to the opposite extreme and talking about fascia as though it is more interesting than a lifetime subscription to National Geographic. The truth is somewhere in the middle.55 Dr. Schleip’s research demonstrates this. Fascia is not inert.
But neither is it all that lively — at least not in terms of contractility. We are not talking about a lot of muscle cells here. If you had blueberries with your cereal in the same proportion, you’d be disappointed — not enough blueberries! It’s just a few muscle cells scattered throughout the fascia. There’s so few that they are visible only when you look very closely and in just the right way.
Nor are we talking about particularly strong contractions. Fascia isn’t going to be ripping apart any chains with its bare hands. The maximum force generated by a small bundle of contractile rat fascia was around 35mN.56 In plain English that’s “not very dang much” or the somewhat more precise “about what it takes to set an AA battery rolling on a nice smooth surface.” (It took me a long time to work that out. I have a weird job.) That’s not bad for a bundle of rat fascia, perhaps, but it doesn’t really hold a candle to middle-of-the-night charlie horses either.
Compared to the power of muscle contraction, fascia power barely even registers.
The “bull versus mouse” comparison is a little unfair though, because it’s not just a matter of strong versus weak. Although fascial contractions may be weak compared to muscles, they could nevertheless be powerful in another way — their effects might, for instance, accumulate over time to produce contractures (permanent “seizing up” of tissues). So it’s still worth considering how these contractions might be clinically relevant.

Do weak fascial contractions matter?
Schleip et al.’s basic finding seems sound enough, and I see no reason at this time to dispute the observation that fascia can contract. If there’s anything wrong with their research methods, I don’t know what it is. But for the property they described to matter to therapists who are choosing to focus their therapeutic attention on fascia — for any biological property to be clinically relevant — it must be significant enough to have an effect on health. (It then must also be something that we can do something about, but let’s start with it mattering in the first place.)
Schleip et al. characterized the raw power of fascial contraction quite differently than I just did. I deliberately made it sound trivial, within the bounds of their numbers.57 In their words, however, in the large sheets of fascia in the low back, the contraction could be “strong enough to influence low back stability and other aspects of human biomechanics.”
Stability? Even if you exaggerate their numbers, they would still only account for a small fraction of the postural muscle power involved in dynamic spinal stabilization, never mind the generally astounding structural toughness and resilience of the human spine. The idea that low back stability could be affected in any way by such a small, slow-motion force is a bit much for me to swallow.5859
And that’s based on an estimate of the theoretical maximum force generated by the biggest, thickest blankets of fascia in human anatomy. In most places in the body, fascia is much less substantial — tough for its weight, but mostly quite thin and wispy, and a lot of it even microscopic.60 The forces generated must be dwarfed by that of muscle itself — in rough proportion to the number and size of contractile cells involved.
That fascial contractions might influence “other aspects of human biomechanics” is a bit vague. A general example of such “aspects” might be that contracting fascia could be involved in biomechanical asymmetries — tighter on one side than the other. The validity of such a concern depends on just how sensitive you think human biomechanics are to forces so subtle that no one really had any idea that fascia contraction was even happening before this study. As regular readers here will know, I think biomechanics are over-rated as a factor in all kinds of pain problems, and there’s extensive evidence that human beings are wonderfully adaptable and cope surprisingly well even with gross deformities, never mind subtle asymmetries and “imbalances.” I make that case in great detail in another article.61
The wording of the conclusions of Schleip et al.’s paper is synonymous with saying that fascial contraction is relevant only if structuralism is a useful mode for doing and thinking about therapy. Also, their phrasing shows a strong bias in favour of the “importance” of fascia. And the study was funded by the International Society of Biomechanics, the Rolf Institute of Structural Integration, and the European Rolfing Association.62
Weak, slow fascial contractions strike me as being scientifically valid and interesting, but clinically minor. Once again, far from making me interested in fascia as a target for therapy, fascia science is convincing me of just the opposite.
No clinical relevance at all? Not even a teensy bit?
If it makes anyone feel better about all this, I’m happy to concede that fascial contractility might be a little bit clinically relevant. Other evidence might even reveal something important — although that would surprise me. It doesn’t hurt my main point to make these concessions. To make my point, all I have to establish is that the clinical relevance is debatable and probably minor at best, rather than the slam dunk it would have to be to support even half of the “excitement” about fascia you see in the therapy industry today.63
In his original dissertation, Schleip limited his speculation about clinical implications to the broad generalization that it can “influence musculoskeletal mechanics,” such as spinal stability. In a follow-up paper for Medical Hypotheses,64 he and several colleagues generally suggest that fascial contractility is a factor in muscle stiffness. The high water mark for potential clinical relevance is spelled out in this passage:
This offers the possibility of a new understanding for many pathologies that involve a chronically increased myofascial tonus. Examples include conditions such as torticollis, low back pain associated with paraspinal compartment syndrome, tension headaches, and others. Similarly a decreased fascial tone could be a contributing factor in conditions that are often associated with decreased myofascial tension, such as in back pain due to segmental spinal instability, peripartum pelvic pain, or fibromyalgia. While usually other factors play a major role as well in these pathologies, it is possible that their progress could be influenced additionally by the regulation of fascial tissue tone …
The emphasized phrase is key — it’s an understatement. For instance, other factors don’t “usually” play a major role in those conditions, they always do. And the role of those factors isn’t just “major,” but probably nearly total — relative to the presumably minor (and still unconfirmed) contribution of a little fascial tension. Some of the items listed are particularly implausible to me. I’ve already mentioned how hyperbolic it is to suggest that fascia could have any serious impact on spinal stability.
Another peculiar item here is fibromyalgia, a fascinating condition that might conceivably be affected in some small way by fascial contraction, but which is overwhelmingly a nasty disease of the nervous system. Suggesting it as a main example65 of how fascial contraction might matter makes about as much sense to me as saying that people with cancer might have some contracted fascia — would it matter if they did?
The most interesting item listed is “compartment syndrome,” which is decidedly not a common complication or cause of back pain, but certainly is a problem (especially in the shins).66 Compartment syndrome is excessive pressure in a fascial compartment, like a sausage swollen in its wrapping. If fascia were to start squeezing a compartment for some reason, it might be a problem. It is the one item listed where there is a clear, direct and logical connection between “fascia can contract” and a way that it could contribute significantly to a health problem. That is clinical relevance. And yet there is still a clear problem with the scale of the forces here. Compartment syndrome is by definition only a problem when the pressure is significant, probably dramatically exceeding the maximum force with which fascia could squeeze the compartment. Visualize a hot water heater that isn’t venting pressure — the valve is busted, and it’s in danger of blowing. The pressure inside is immense, and it would make no practical difference if the hot water heater itself was a little larger or smaller. Again, fascial contraction is probably not nearly strong enough to matter. Still, at least it’s easy to see how it could matter in principle, and the numbers might favour fascial contraction as factor.
And then there’s the fact that we know from Dahl et al. that “structural and mechanical properties are unlikely to explain chronic compartment syndrome. To prevent chronic exertional compartment syndrome, it is necessary to address aspects other than the muscle fascia.”
So you see how this goes: for one candidate example after another, the clinical relevance of fascial contraction is dubious or minor.
Is fascial contraction even interesting?
One of the lower moments in biology history was the labelling of non-coding DNA as “junk DNA” in 1972. The first time anyone with a scrap of imagination heard that, they thought, “Yeah, right.” As biologists slowly figured out what all that “junk” is for,67 there was a lot of “Well, yeah, okay, that’s more like it. Of course.” It’s interesting science, but in some ways those discoveries are still overshadowed by the way we’re all not so very surprised.
Similarly, the presence of muscle cells in fascia is no shocker. I never believed fascia was entirely inert any more than I believed in the junkiness of any DNA. If you spend much time studying biology, it quickly becomes apparent that there are no sharp lines or divisions, and that we consist of an incomprehensibly diverse and interconnected community of cells.
I didn’t know that before it was confirmed, but I certainly don’t find it particularly surprising. I suspect that the slightly contractile properties of fascia are simply at one end of a continuum of motor function. Our muscular system is overwhelmingly our primary means of reacting to stimuli — the major output of our nervous systems — and in general terms the slight contractility of fascia is probably just the fringes of that functionality, a little bit more of the same. There are probably some subtle differences, but they are subtle and arcane and ultimately just a slight variation on the biological theme of muscularity. I’m not saying it’s completely uninteresting, but it’s overshadowed by the much more interesting muscular system as a whole, about which fascia is simply a mildly intriguing subtopic. And, in terms of clinical relevance, the muscular system itself is in turn overshadowed by neurology.
What does Dr. Schleip think?
Recently Dr. Schleip read my article and wrote to express his basic agreement with my key point about his research: “Your comments on the small size of fascial contractions are right on, at least when viewing these within the periods of seconds to minutes, as is usually applicable for bodywork techniques.” He also wanted me to know that he shares my annoyance with the “over-zealous claims and projections” of therapists doing fascial work. He is not thrilled with the way his research is being used to justify premature overconfidence in fascial therapy.
He also offered some thoughtful criticism on some specific points (and I made some changes, and will probably make more). Nevertheless, he had no major objections, and was generally pleased with what he read here: “You have my respect for your detailed and critical analysis of the present work on fascia. Most of the people who criticize you have not done a portion of your reading work and could certainly learn a lot from the debate you started.”
I invited him to make a statement for my readers about this. Here is it in full, with some emphasized highlights:
I share your emotional frustration with the current trend among bodyworkers of attributing anything wonderful or astonishing to the properties of fascia. In fact, our Fascia Research Group at Ulm University has been receiving an almost exponentially increasing number of inquiries from enthusiastic healers (and martial art teachers) worldwide who wish that we would sanctify their claims that fascial contraction provides the explanation for their observed miracle powers. While I do tend to believe that the fascial net plays much larger roles in human functioning than previously assumed in orthopedic medicine, I am afraid that such over-zealous claims and projections are undermining the seriousness of the investigation and academic rigor that characterizes the work of the current leaders in fascia research, such as P. Huijing, H. Langevin, T. Findley, P. Standley and A. Vleeming.
As a bodywork clinician myself, I have learned that
there is hardly a more dangerous attitude among therapists than the hero healer/manipulator who is damn sure about his diagnosis and supposed treatment effects . This of course applies as much to fascia-oriented therapists as it does to those who base their work on supposed neuromuscular or other physiological effects, most of which are still unproven. While scientists can learn a whole lot from the intuitive and experiential wisdom of complementary therapists, particularly about the non-fragmented and connecting properties of the fascial net, we bodyworkers can learn at least as much from the careful, questioning approach of good scientists, who are willing to doubt their own assumptions and to refrain from premature confidence and over interpretation of their findings. It is this mutual learning and interdisciplinary enrichment which in my opinion characterizes the best qualities of the current fascia research field, as expressed in the international Fascia Congress series and associated activities.
Again, Dr. Schleip and I do not agree about everything — but that is unimportant compared to our shared values and commitment to cautiously reserving judgement. We have each placed our bets on this topic, but not closed our minds. I fully support and endorse his enthusiasm to explore the biology … and he supports and endorses the value of my critical analysis.
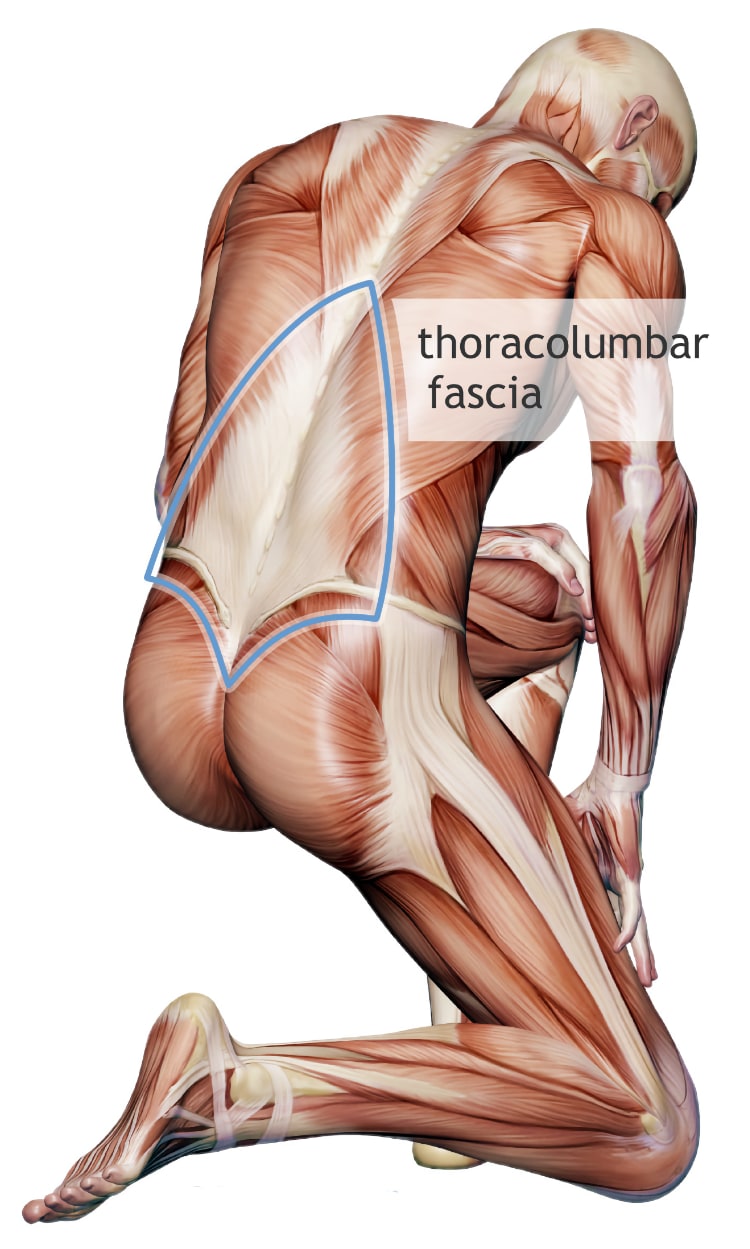
Thicker, stiffer thoracolumbar fascia in back pain: what does it mean?
Over the last couple years, by far the most common answer to my fascia science challenge has been: Langevin, Langevin, Langevin. Specifically Langevin et al.’s 2009 and 2011 papers presenting evidence that the thoracolumbar fascia is thicker and stiffer in people with chronic low back pain.6869 A pair of follow-up studies established that the same fascial stiffness occurs in pigs if you torture them,70 and that it is fairly stubborn once it sets in.71 This is all interesting evidence that comes as close to being a good answer to my fascia science challenge as anything I’ve seen yet, but I still don’t think it actually achieves clinical significance.
The thoracolumbar fascia is the shield-shaped sheet of thick fascia that more or less completely covers the low back.
I’m not going to question the findings at all for now — though of course that is also fair game.72 I’m going to take their results at face value and write only about what they mean to us as thoughtful therapists and patients, keen on biology but wishing to avoid false hope.
Exactly what Langevin et al. have found so far
In people with chronic low back pain:
- The thoracolumbar fascia was about 25% thicker in people with back pain, which is quite a bit, and a surprising finding with potentially major — but unknown — clinical significance. The authors suggest that it could be related to “genetic factors, abnormal movement patterns and chronic inflammation.”73
- The thoracolumbar fascia had about 20% reduced “shear strain,” a measurement of the deformation of a structure. In other words, it was 20% stiffer than in people without back pain. Again, that’s quite a bit.74
And in tortured pigs …
- Injured and/or hobbled pigs exhibit the same kind of increased fascial stiffness as humans with low back pain — and quite a bit more when combined.75 To some extent this constitutes replication of the key finding of Langevin et al.
- Once you’ve given pigs stiffer back fascia, it doesn’t readily loosen up. If you set them free, they return to normal movement, but their fascia stays stiff. If you stretch them for 10 minutes per day — yes, that’s actually what they did — that doesn’t help either.76
What’s it all mean?
Chronic back pain is a notoriously inexplicable and invisible condition. Things that turn up on MRI that seem like they might explain the pain are often irrelevant. A clear, consistent, measurable biological sign of chronic low back pain like thickened fascia would be inherently interesting — downright cool, even!
But that thickened, stiffened fascia is probably not the cause of back pain. At best, it’s probably a clue about the nature of back pain — inflammatory, perhaps?77 But it’s probably even less meaningful: it could be a consequence of pain and limited mobility, something that happens because you’re in trouble.78 And that’s also exactly what the pig-torture experiments showed!
So the most likely explanation is very boring: a simple case of “use it or lose it” — we stiffen up a bit when we’re in pain for a long time. •mind blown•
And if that’s all there is to it, it’s really a big whoop-de-doo.But no one knows. The research didn’t explain a phenomenon, it just identified one … maybe.
Clinical relevance
The purpose of this article is to challenge hype about fascia. The point of the fascia science challenge is that most science does not at this time inform diagnosis or treatment, and therefore there is no scientific justification at this time for “fascial therapy” to be a popular phenomenon.
Langevin et al.’s research clearing comes closer to influencing diagnosis or treatment than anything else I’ve seen, but I think it’s a case of so-close-yet-so-far.
Does knowing that the thoracolumbar fascia is thicker and stiffer inform diagnosis? Not really. Because no clinician can (a) know whether or not it’s actually the case, or (b) has any idea whether it’s a cause of back pain or just a trivial consequence of it.
Not that stretching for 10 minutes per day is likely to be adequate or relevant to human back pain, but it’s worth noting that stretching failed.
Does knowing it inform treatment? No, because (a) no one has the slightest idea if it’s possible to make the thoracolumbar fascia thinner or more pliable with their bare hands (and it’s rather unlikely), and (b) there’s not much point in even trying unless you actually know it’s a cause or complication of back pain. Yes, you could gamble and try to manipulate it and see what happens — but hands-on therapy ain’t cheap, and this is about as experimental as it gets. And bear in mind that stretching did not help the poor pigs.79
It’s conceivable that follow-up research could fill in some of these blanks, but, until then, this research isn’t good for much beyond raising eyebrows. It’s only clinically relevant insofar as it could lead somewhere clinically relevant. If the findings can reproduced. If they can be explained. If the explanation does in fact turn out to be clinically relevant.
That’s a lot of ifs.
A real fascia contracture disease: frozen shoulder
Frozen shoulder is one of the few common, familiar musculoskeletal problems that definitely can be blamed on misbehaving fascia. Its medical name, adhesive capsulitis, pegs it is a disease of “stickyness” of the joint capsule, but in fact the best available evidence to date suggest that it is more a disease of shrinkage — connective tissue contracture.80 Maybe this contracture has something in common with what Langevin et al. observed in the low back?
Anything’s possible.
In the case of the shoulder, joint capsule contracture is quite clearly an etiologic factor: it’s freezing shoulders and causing much woe. In fact, it’s one form of a disease process that also sometimes afflicts the palms (Dupuytren’s contracture), knuckles (Garrod’s pads), foot (Ledderhose disease), and — rather alarmingly — the penis (Peyronie’s disease). Could something like it happen to the back too?
In the case of the back, it’s technically conceivable but extremely unlikely that fascial contracture is the cause of low back pain. But, just for the sake of argument, let’s say it is: imagine that people do get back pain because their thoracolumbar fascia seizes up for mysterious biological reasons, very much like frozen shoulder. It’s not a completely absurd notion, but I don’t actually believe it for a moment: it would be the biggest discovery in the history of musculoskeletal medicine. This is just a thought experiment!
No one — no one honest and humble, anyway — has the foggiest notion how to “melt” a frozen shoulder. That joint capsule is exceedingly tough. When it contractures, that’s it: it yields only to intense, traumatic forces. Frozen shoulder defies manual therapists all the time, despite cocky claims to the contrary. And so, even if back pain is like frozen shoulder and caused by fascial contracture, I don’t think there’s a snowball’s chance in hell that it could be treated with any kind of hands-on manipulation. Both shoulder capsules and the thoracolumbar fascia are super tough human gristle, and are unlikely to change much or for long — if at all — in response to any non-traumatic external stimulus. And the thoracolumbar fascia is not only much tougher — the biggest and thickest sheet of fascia in the body — but it is much harder to apply force to than the shoulder joint (which has a giant lever).
So even in the most spectacular hypothetical scenario, where the thoracolumbar fascia is truly a major cause of back pain … even then it’s still not going to translate into a good treatment option. And so Langevin et al. cannot and should not be used as justification for a clinical obsession with fascia.
↑ MEMBERS-ONLY AREA ↑
Nerve entrapment
Nerves can get a little tangled up in connective tissue and cause peripheral neuropathy. This may be a good example of “fascia” science that actually matters, at least a little.
And yet I came across it myself. No one defending fascial therapy hype has ever brought this idea to my attention — I am including it on my own intiative, not as a response to a claim made by fascial therapists. Apparently it isn’t even on fascia enthusiasts’ radar even though some nerve entrapment may really and truly actually be caused by fascial “distortion” or “adhesions,” by the accumulation of webs of fascia in such a way that nerves that were once free and clear start to snag and pinch. To the extent that this causes peripheral neuropathy, it is obviously clinically relevant.
However, there are also things that probably limit its clinical relevance quite a bit:
- Physical entrapment itself is probably only be part of the story. The true cause of pain may actually be biological vulnerability to the nerve’s predicament.
- Even if the physical entrapment is the main issue, it’s not clear that “fascia” is actually to blame.
- And, regardless, it’s doubtful that a nerve can be sprung from such a trap with manual therapy.
A good example to study: cluneal nerve entrapment
The cluneal nerves pass from the low back and sacrum into the buttocks, just under the skin, and they can get snared in connective tissue on their way.
Cluneal nerve entrapment is a good example because it may be a common undiagnosed cause of back pain that is not obviously neuropathic in character. That is, some cases probably don’t feel like classic back pain, but back pain with a fairly obvious nervy character (superficial, electrical, with some tingling and other distorted sensation).

#1 marks the site of the superior cluneal nerves and where the first surgery freed nerves from “adhesions.” #2 marks the middle cluneal nerve, where the second surgery freed it from entrapment in the ligament. Click to embiggen
In 2016, Aota reported on “a case of severe low back pain, which was completely treated by surgical release of the middle cluneal nerve.”81 The patient suffered from “back and buttock pain radiating to both legs” which was “continuous and severe,” and had come on gradually over a decade. She’d been operated on already, a clean miss, a pointless diskectomy.
She was lucky enough to have a doctor who figured it out and talked her into a surgery I doubt that I would have agreed to: exploratory surgery to identify nerves “entrapped in adhesions.” Freeing it up definitely helped part of the problem, but it didn’t solve it. It took a second attempt to find the main problem, a surgery I would definitely have been reluctant to try myself. But it’s a good thing she did!
They found a tiny spot where the nerve passed through a ligament, cut it free, and that was the ticket: she was decisively cured. Which is pretty cool.
On its face, this seems like an open-and-shut case of a nasty pain problem caused by connective tissue in an abnormal state, and therefore a good example of how fascia can actually matter. (Which no fascial therapist has ever actually mentioned to me as a reason why they are doing fascial therapy.)
But now let’s dampen our enthusiasm.
Entrapment may not be the problem (or not the whole problem anyway)
Maybe her problem was not the nerve “snag” per se but a biological vulnerability to feeling it. The physical predicament of the nerve may have been like kindling for a fire — a fire that was then lit by something else (and then burned for years).82
Admittedly, even if that was the case — and it would certainly be fascinating — diagnosing the vulnerability and solving it might be next to impossible. It might be much more pragmatic to just free the poor nerve, rather than trying to fiddle with the biological dials so that the nerve stops being bothered. No kindling, no fire.
Or it could be as simple as getting off a certain medication, or taking some vitamin D. Who knows.
Was “fascia” really even involved?
The authors of the paper about this case describe the entrapment of the superior cluneal nerve as “entrapped in adhesions,” which was part of the problem, but the case was ultimately solved by freeing the middle cluneal nerve from where it was stuck as it passed through: “entrapped under the deeper layer of the long posterior sacroiliac ligament where it penetrates the ligament.” Nerves often pierce ligaments and layers of fascia — just normal anatomy, or common variations — and it’s usually not a problem.
There are many unanswered questions here. Was there something abnormal about the pathway of this patient’s middle cluneal nerve? Was there any abnormal tissue there, or was the passageway through the ligament just too narrow? Had it always been narrow, and only eventually became a problem for some other reason? Or had it become a problem? Did the pathway get narrower, or stickier? Was the nerve actually impinged, or more like stuck — couldn’t slide freely?
Without the answers to those questions, we can’t really say whether fascia, per se, was the problem. But clearly it was not necessarily so.
Manual release of nerves entrapped in fascia
… is implausible in most cases. Imagine a hair stuck to a hardwood floor by some spilled honey, and covered with a Persian rug. Now try to “release” the hair through the rug. Good luck with that.
This patient probably actually needed surgery. It’s seems unlikely to me that any amount of trying to manipulate that tissue from the outside — through a thick layer of skin, no matter how clever or forceful — was ever going to “free” that nerve.
Part 4
Case study: Frank the adhesion machine
Frank was an “adhesion machine” — for no apparent reason, he was rapidly forming abnormal adhesions in his abdominal cavity, thick cobwebs of connective tissue strung admist his guts. His surgeon described his abdomen as a haunted house.
Frank had survived a chronic pancreatitis nightmare, a disease that runs in his family. His pancreas, spleen, duodenum and part of his stomach were removed in 2016, after several years of ominous medical misery. He was probably dying, and the radical surgery saved his life.
But the adhesions continued to form, probably driven by the same pathology that had almost destroyed him. Medicine is full of mysteries still.
Eighteen months after his surgery, Frank was suffering severe chronic pain and bowel obstructions. Surgery to rescue once again! The surgeon found extensive new adhesions strangling his intestines. They were cut free, and once again Frank was all right for a while. Now that is a fascial “release.”
Six months later, a third surgery was necessary. The surgeon reported that he found, “more adhesions than he would have expected.” Frank was okay again, but for how long?
He decided to try Barnes-style myofascial release the next time… and the next time came soon enough.
Often alleged to be a gentle style of therapy, this was an excellent example of the more typical reality: weeks of brutal sessions in which
You have to admire Frank’s courage!
As he explained, it was a calculated risk his physicians were well aware of. But I can’t help but think “What could possibly go wrong?” I never would have signed off on it — knowing what I know about fascial release would make it impossible to endorse. I don’t think the therapist had any business attempting this. Frank’s history should have completely disqualified him for intense abdominal manipulations. I think she could have killed him.
Of course, he was truly desperate: the enemy was a serious and persistent pathology. And the only other option — surgery — is also potentially disastrous and to be avoided if at all possible. But that’s a devil we know, and the manual fascial release was very much a devil he did not — could not — know. And there wasn’t any trace of the common conceit that the therapy was “melting” his adhesions. This was just brute force, period. The goal was to rip them apart.
And… it seemed to work. Frank got better again, without surgery, despite the rough ride. That’s about when he found this article and first wrote to me: calm, sensible, open-minded, curious. He was curious if I had any comments on his experience. But he was mainly reporting that fascial release seemed to be efficacious for him.
A year later
At the best of times, it can take me weeks to answer non-critical email, often months, and a delay served another purpose in this case — would the results be lasting? So often when I get “therapy X worked for me” messages, that confidence evaporates over the next few months (or people cling to it as “the one thing that helped” even though they continue to have a problem).
Only a few weeks later, Frank was back in hospital, having another surgery that found and cut a major new adhesion, this time choking his liver. It was too serious a medical situation to trust it to manual fascial release. This situation developed so soon after the manual therapy that I have to wonder if it actually partly precipitated it, by causing a lot of extra inflammation while ripping up adhesions.
Why, Frank wanted to know, had he felt better for a while just from fascial release? I can think of a couple reasons:
First, top-down modulation of pain is a potent and common phenomenon.83
Second and more obvious: probably the therapist did manage to destroy a few adhesions! With that brutal approach, and such a clearly abnormal target, that’s hardly a surprising outcome. Doesn’t mean it was a good idea. Doesn’t mean it wasn’t dumb luck she didn’t seriously injure him trying. It might have even made the problem worse with a bunch of post-traumatic inflammation, leading directly to the crisis with his liver.
Even if the therapy really did break some adhesions, it’s clear that it was pissing into the hurricane of whatever pathology is making Frank “an adhesion machine.” Even if it worked, it was clearly doomed to be temporary.
That does not look like a success story to me. It looks like a desperate, risky attempt that didn’t really work. And the fact that any therapist was willing to do it is horrifying to me professionally — but completely unsurprising, more or less exactly the kind of fascia-inspired overconfidence I have come to expect from massage therapists.
Part 5
Conclusions
Results of the Fascia Science Challenge so far …
- Piezeoelectricity may occur in fascia, but its clinical relevance is nil — not enough is known about it to even speculate about how it could be exploited in manual therapy.
- Gil Hedley’s theory that congealing fascial “fuzz” causes stiffness is simplistic and wrong. It is not a plausible explanation for the sensation of stiffness, or a mechanism of action for fascial therapy or stretching.
- Fascial “meridians” relate fascial therapy to the “meridians” of acupuncture, which don’t exist or — even if they do — can’t actually be exploited for any therapeutic effect even by acupuncturists.
- Chaudhry et al. showed that fascia is too tough to “release.” Indeed, even thin fascia is so tough that it is basically inconceivable that it could be physically changed (stretched, loosened) without vice grips. This directly contradicts a major popular rationale for fascial manipulation, and is only clinically relevant to fascial therapy insofar as it presents evidence that discourages and undermines existing common practices and beliefs.
- Meltzer et al. concluded that stimulated fibroblasts might be happier fibroblasts — specifically, they might be more resistant to post-exercise soreness. The results of this test tube study are questionable, but even if you take the data and interpretation at face value, it is a long reach from a test tube study to clinical reality. Treating post-exercise muscle soreness is not even a common goal for manual therapy.
- Schleip et al. established that fascia is contractile, but this isn’t biologically surprising, and it’s clinically trivial. It is definitely not a factor in any of the common problems most manual therapists work with — maybe none at all — and, even if it was, it is somewhat unlikely that hands-on therapy could make a difference.
- Chapelle et al. hurt some rats to prove that abdominal massage prevents post-surgical constipation, but so does chewing gum. Although this has been widely regarded as an important “fascia” study and justification for visceral manipulation, the paper does not actually report an effect on fascial tissue or adhesions, and it would have very limited clinical utility even if it did. It’s mildly interesting massage science, not fascia science.
- Langevin et al. and subsequent studies have shown that the thoracolumbar fascia is thicker and stiffer in people with back pain, and they injured some pigs to induce the same condition and establish that stretching does not relieve it. Of all the fascia science evaluated here, this comes the closest to clinical relevance. Unfortunately, it’s a case of so-close-yet-so-far: even if they’ve identified a real phenomenon, it still isn’t established whether the change in the fascia is a cause or a symptom of back pain, and it can’t actually inform diagnosis or treatment.
There is more fascia science, and I will extend this article with more analysis in the future. I honestly hope that there is clinically relevant fascia science — that would be terrific. So far, however, I see no good reason for therapists to be fascinated by fascia and to make it a target tissue.
A few more alleged fascial properties and clinical relevance issues I intend to address eventually (definitelyb not a complete list):
- The claim that fascia contains “memories” or that it “stores trauma” in some sense. I will likely dispute both the property and its relevance.
- The claim that fascia is structurally important and tensegrity is interesting (agree), and that this is clinically relevant (disagree). Much of my rebuttal on this score already exists in my article about structuralism. For another sneak preview, see also this amusingly vague bit of junk science about “tensegrity-based” massage.
- The claim that the phenomenon of “force-transmission” means that much “muscle” tightness is actually attributable to fascial restriction. Although there is little doubt that fascia transmits and distributes force in interesting and probably counter-inuititive ways, I will probably dispute that the phenomenon is clinically relevant, because I doubt that it is either abnormal or treatable.
- The claim that “fasciotomes” exist and can explain pain experiences and patterns that are not otherwise already explained by existing neurology. This is a minor sub-topic, but thematically perfect for this article, so I’ll cover it properly at some point. Meanwhile, see the footnote for the simple analysis.84
The stakes: extreme “fascial release” therapy injures a patient, maybe permanently
Hype about fascia is not harmless, and that’s why this article matters.
This is one of the most striking stories of incompetent and harmful manual therapy that I have ever received from a reader. (And I get a lot.) It is notable not only for the seriousness of the outcome, but also for the glaring excess of the treatment: so unnecessary! If condemnation and negativity isn’t justified here, I don’t know where it would be: the degree of fascia-o-centric incompetence and poor clinical judgement is just appalling. What happened to this patient needs to be discussed openly. Although this is an unusually nasty example, negative outcomes like this are shockingly common, and almost never reported to the therapist who perpetrated them — or, if it is, the therapist rationalizes it away as a “healing crisis” or any one of a list of other intellectually dishonest evasions.
The story
I have re-written the story a little to anonymize and condense it, but it is otherwise presented as it was received:
I visited a massage therapist a month ago for treatment for soreness/achiness in the balls of both feet and in the toes. Claiming that tight calf muscles and hamstrings were causing my heel to lift too far (thus placing pressure on the balls of my feet), she proceeded with a half hour fascial release therapy on my calves, using her full weight and her elbows.
It was extremely painful, but I gritted my teeth, thinking it necessary "to break up the knotty muscles." She moved from point to point up and down my calves, twice. A week later I had another such treatment, and she also persuaded me to buy a rubber roll so that I could do the "therapy" at home. She told me I should try to reproduce the same pain level, on calves and hamstrings. I did this every day for one hour for five days. I did the same with a wooden roller under my feet, using my own weight.
During that time, I started getting stabbing and burning pains in my feet, the backs of my legs, and then later my hands and armpits. The stabbing pains varied from a pinprick feeling to electric-shock/lance-like, and they varied in their frequency rate. The burning was either tingly or felt like bad sunburn. The pain seemed to be aggravated by walking, and was always worse by afternoon/evening. I had trouble sleeping, because I could not have heavy bedclothes on my feet, and nor could I put one leg on top of the other, without pain.
I returned to my GP, had blood tests, x-rays, a CT scan. Because my symptoms seemed neuropathic in nature, I was referred to a neurologist. After eliminating a number of other diagnoses, the neurologist thinks the problem is biomechanical or related to muscles, and that the MFR may have caused an oversensitivity to pain.
I then searched the Internet for information about myofascial release being damaging or making pain worse. It was very difficult to find, because of all the "positive" hype around MFR. Fortunately, I found your website …
The implications
What happened here? Aggressive and intense manual therapy with no regard for the state of the patient’s nervous system or the potential to sensory injury (by provoking central sensitization — pathological pain amplification). This patient’s prognosis is impossible to call: it could last another week, or this patient could suffer excessively for the rest of her life.
For the duration of my decade as a massage therapist, I had a reputation as a gentle therapist, and many of my patients were “refugees” from excessively intense treatment, many of whom vented angrily to me about the abuse they had received from other therapists. Vancouver is a “fascial release” mecca, with many therapists who believe that there is no gain without pain, and many or all painful problems are caused by fascial “restrictions” that must be painfully “released.” As a therapist who defined himself in opposition to this obvious trend, I was treated to many, many outraged patient anecdotes about the brutality of other therapists.
Having also personally experienced that intense style of fascial release many times, I knew all too well what these patients were talking about. Almost none had found the courage to discuss their concerns with the confident (overbearing?) therapists who had mistreated them. Almost all had even earnestly tried to like it, at first. Sometimes, rather sadly, they were even still trying to rationalize it as positive, i.e. “I’m sure it was probably what I needed, but I just couldn’t take it anymore!”
Of course some people enjoy intense therapy — and hey, if your nervous system is okay with it, that’s fine. Most of those therapists have many devoted patients who, for various reasons biological and psychological, are more willing and able to tolerate extreme therapy. However, they are also leaving behind them a trail of angry, injured patients … patients who never raised a word of objection.
That’s why stories like this are important. There are bound to be therapists reading this who have actually done this to patients, who do it every day. Many will react defensively. Many will delude themselves into believing that they are the more judicious exception to the rule. But some, perhaps a few who are already questioning their own methods, will probably be moved further in that direction. I hope.
Better still if patients feel emboldened to reject such treatment more quickly.
The conceptual cancers at the heart of this incident are structuralism and the for-profit trademarking and packaging of treatment methods, what I call modality empires — and “fascia” is a defining, central feature of several of the most famous modality empires. Fascia sells. Its prevalence in the marketplace has much more to do with marketing than sound clinical reasoning.
Now, back to the science.
The “Father of Fascia” is so over it
What better way to end this article than with the momentous news that Tom Myers is “pulling back from that old ‘fascia’ buzzword” … but cells are still neat, therefore therapy!
I’m genuinely pleased to see Myers write this (and he must have known when he wrote it that it would be enthusiastically quoted by his critics):
I am so over the word ‘fascia’. I have touted it for 40 years — I was even called the ‘Father of Fascia’ the other day in New York (it was meant kindly, but … ) — now that ‘fascia’ has become a buzzword and is being used for everything and anything, I am pulling back from it in top-speed reverse. Fascia is important, of course, and folks need to understand its implications for biomechanics, but it is not a panacea, the answer to all questions, and it doesn’t do half the things even some of my friends say it does.
I don’t think it has important implications for biomechanics, and I don’t think it does a tenth as much. But this is still progress!
Cells are neat, therefore therapy

Not actual cells.
After pulling back from that old “fascia” buzzword in top-speed reverse, Myers goes on to tell us about some science about how cells sense the texture of their surroundings:
Organismic movement and stretching — yoga, pilates, training, manual therapy — can help cells to their proper tension environment by relieving pressure or strain, and this results in better functioning all over. Why should yoga help digestive problems, or some of my bodywork clients report increased regularity of their periods? This points the way.
No, there is no way-pointing here: it’s nifty cellular biology, but it’s about as relevant to our macroscopic activities as knowing how oxygen binds to hemoglobin. We’re talking about molecular scale structures that are the functional equivalent of nerve endings, “feelers” that tell cells “whether they are on a rigid or a soft surface,” cell proprioception. I’m glad for the cells, and I’m glad someone maybe identified how they do this. That’s great, truly it is, go Team Science!
But it’s also about as surprising in principle as a tree in a forest. Such a mechanism more or less had to be there. Cells are marvellous little critters, so of course they must know all about what’s going on around them, and doubtless they do it in many clever ways.
Connecting that to yoga and manual therapy is an odd but inevitable spin. Read that again: he goes from cells have cool molecules that detect tension to bodywork makes periods more regular. That’s quite a leap — over a thousand other variables and mechanisms of vitality!
And this is a perfect example of what has always been the problem with the fascia hype: torturing basic biology until it confesses to being relevant to $1+/minute manual therapy. That is really what this article is about.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Part 6
Appendices
Related Reading
- Your Back Is Not Out of Alignment — Debunking the obsession with alignment, posture, and other biomechanical bogeymen as major causes of pain.
- Pain is Weird — Pain science reveals a volatile, misleading sensation that comes entirely from an overprotective brain, not our tissues. The role of the nervous system in chronic pain is the major alternative to focusing on fascia. It has much clearer clinical relevance.
- The Complete Guide to Trigger Points & Myofascial Pain — An extremely detailed guide to the unfinished science of muscle pain, with reviews of every theory and treatment option. Includes a section on the relationship between fascia and trigger points (e-book customers only).
- Greg Lehman, a chiropractor and physiotherapist has a thoughtful new fascia article, “Fascia Science: Stretching the power of manual therapy.”
- Todd Hargrove, a Rolfer and writer (BetterMovement.org), has a good post on fascia and foam rolling and fascia under the microscope.
- “If We Cannot Stretch Fascia, What Are We Doing?,” Alice Sanvito, Massage-StLouis.com. Massage therapist Alice Sanvito’s clear summary of Dr. Robert Schleip’s theory that fascial “release” may be attributable to changes in muscle tone stimulated by mechanoreceptors in fascia and other soft tissues, and not by plastic deformation of fascia.
The major myths about massage therapy are:
- Massage increases circulation. Probably not… and definitely not as much as a little exercise.
- “Tightness” matters. The three most common words in massage therapy — “you’re really tight” — are pointless.
- Massage detoxifies. It’s actually the opposite, if anything.
- Massage patients need to drink extra water to “flush” the toxins liberated by massage.
- Massage treats soreness after exercise. Studies have shown only slight effects.
- Massage reduces inflammation. An extremely popular belief based mainly on a single seriously flawed study.
- Fascia matters.
- Scars and adhesions can be scraped away. Often uncomfortable, sometimes dangerous, always expensive and ineffective.
- The psoas muscle is a big deal.
- Massage stimulates endorphins (natural opioid) and reduces cortisol (stress hormone). They do not.
- “Trigger points” are evidence-based. Actually, the science is seriously half-baked.
- Massage therapists have spooky palpation skills. No, it’s just ordinary expertise… and misleading.
The complete list of dubious ideas in massage therapy is much larger. See my general massage science article. Or you can listen to me talk about it for an hour (interview).
And massage is still awesome! It’s important to understand the myths, but there’s more to massage. Are you an ethical, progressive, science-loving massage therapist? Is all this debunking causing a crisis of faith in your profession? This one’s for you: Reassurance for Massage Therapists: How ethical, progressive, science-respecting massage therapists can thrive in a profession badly polluted with nonsense.
What’s new in this article?
33 updates have been logged for this article since publication (2012). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
Sep 6, 2025 — Minor addition: Added more detail about James Oschman in a footnote. [Updated section: Electrified by piezoelectricity.]
2024 — Added information: Discussed naprapathy as a great example of the older, deeper roots of modern fascia pseudoscience. [Updated section: Origins and types of fascial therapy.]
2021 — New section: No notes. Just a new chapter. [Updated section: Can fascial therapy help COVID patients?]
2020 — New section: This is not an important addition to the article, but it does add a lot of colour, and was a delight to write about an extremely rare convergence of three major but extremely different interests: language, musculoskeletal medicine, and ancient Rome. [Updated section: A fascinating etymological digression: are “fascia” and “fascism” related?]
2019 — New section: No notes. Just a new chapter. [Updated section: Case study: Frank the adhesion machine.]
2019 — General edit: Corrected a large batch typos and other minor errors generously compiled by reader M.M.
2018 — New section: No notes. Just a new chapter. [Updated section: Nerve entrapment.]
2018 — New sub-topic: Discussed the relevance of real pathology of connective tissue. [Updated section: Origins and types of fascial therapy.]
2018 — Minor clarification: Added some information about adhesions. [Updated section: “Fascial distortions,” especially tightness (contracture) and stuckness (adhesions).]
2018 — New sub-topic: Added information about gentle and subtle forms of fascial therapy. [Updated section: Origins and types of fascial therapy.]
2017 — Upgraded: Added information on the nature of and main claims made by several branded methods of fascial release. [Updated section: Origins and types of fascial therapy.]
Archived updates — All updates, including 23 older updates, are listed on another page. ❐
Notes
- Physical therapists are less likely to be excited about fascia than their colleagues in alternative medicine, but they are certainly not immune to it, or other dubious treatment ideas. One of the largest fascia-centric modality empires was founded by a physical therapist.
- This article is quite “negative” — in the sense that critical analysis is always negative. But I have fun taking therapy seriously. Criticism and deconstruction of ideas is normal and healthy and necessary for therapy professions to grow and change. See Why So “Negative”?
- I got an interesting note from someone with a solid science background who attended the big fascia conference in 2018, the Fascia Research Congress. She described it as cringe-inducingly amateurish, the most unimpressive scientific conference in her experience: basic science whipped up into excessive and unsupportable marketing and clinical claims. You can easily see that vibe in this promotional video. The Fascia Congress is as much a pep rally as it is a scientific conference.
- Ingraham. 💩 Massage Therapists Say: A compilation of more than 50 examples of the bizarre nonsense spoken by massage therapists with delusions of medical knowledge. PainScience.com. 11683 words.
- “Manual therapy” refers mainly to massage, spinal manipulation, acupuncture, and many other methods and techniques for assessing and treating common musculoskeletal problems and injuries with hands and/or tools. Most of this is done to/for patients, so it is also sometimes called passive therapy as opposed to active (mainly exercise therapy). It exemplifies the best that alternative medicine offers — the time, compassion, and touch that medicine lacks — but it is also a pseudoscientific dumpster fire fueled mostly by faith that tissue can be “fixed.” What little good research exists shows modest medical benefits at best. The time required for it is costly, and the intensity of some methods means that there are some risks. Although mostly the domain of massage therapists and chiropractors, physical therapists are also surprisingly invested in it, and notorious for their dubious methods (e.g. ultrasound). And yet! There probably is a signal somewhere in all that noise. Rational practitioners can ethically offer more plausible techniques; and the power of touch, compassion, and novel sensations to inspire and comfort should not be underestimated. See Manual Therapy: What is it, and does it work? The science of "fixing" tissue with hands-on treatments like massage and spinal manipulation.
- I hadn’t presented her with any musculoskeletal problem. She was pathologizing at random. It was supposed to be a relaxation massage, in a spa. And yet she was a Registered Massage Therapist — unusually well-trained in this neck of the woods. And that’s probably exactly why she felt compelled to strut her stuff and “troubleshoot” my case and talk about fascia. Fascia enthusiasm constantly inspires this kind of well-intentioned over-reaching.
- Massage therapy training in British Columbia, Canada, is unusually rigorous compared to most places in the world. When I trained in the late 90s, the requirements included a 3000-hour training program, an internship, and some challenging certification exams.
“Mechanism masturbation” is wishful and fanciful thinking about why/how treatments might work. Science journalist Jonathan Jarry (once upon a time on a place called “Twitter,” now removed, but you can listen to an interview about it):
“There is a fascinating phenomenon in the complementary and alternative medicine literature we could call ‘mechanism masturbation’ where the authors, faced with the tiniest of positive signals in a small study, write paragraph after paragraph hypothesizing how, mechanistically, watermelon seeds might cure schizophrenia.”
Musculoskeletal and pain research, alternative as well as more mainstream research, is rotten with “mechanism masturbation” — often because it’s just all there is. There’s no good clinical trial data, so we get wishful thinking and wild speculation instead, even in scientific publications. The field is surprisingly afflicted with cart-before-horse speculation about how they how they could work, might work, should work, maybe work… when the clinical trials (if they exist at all) tend to show that they don’t actually work, or not very well.
Jonathan’s satirical example really nails the flavour of “research” like this:
“It might interfere with the hypothalamic-pituitary-adrenal axis… One of its compounds does bind to alpha receptors in this cell type… Could play a role in this cascade... Anyway, preliminary results from n = 6. More studies needed!”
Yes, that definitely reads like about a thousand papers I’ve wasted my time reading over the last decade. I’m always looking for the rare scraps of basic science I can actually consider interesting/promising instead of more post-hoc rationalization for someone’s meal ticket. 🙄
- The poor track record people have guessing about how things really work is a well-known principle. It is enshrined in a scientific concept: the “null hypothesis,” the assumption that ideas are probably wrong until proven right.
Jonathan Jarry of McGill’s (very nifty) Office for Science & Society explains that fascial “drying” is a central tenet of naprapathy: “it creates knots, and these knots pull bones out of alignment, leading to pain and an assortment of related problems.” Quoting Jarry quoting me:
“‘Fascia is to massage therapy … what subluxation is to chiropractic.’ A convenient villain.”
Fascial “distortions” are imaginary scapegoats in massage therapy just like spinal “subluxations” are in chiropractic. You have to blame people’s pain on something … and ideally something that can plausibly be repaired with bare hands, or maybe some simple tools.
To create naprapathy, chiropractors just shifted the blame from subluxations to fascia. A bit of a modality mash-up. This kind of conceptual mixing and matching has been going on for decades in manual therapy, and none of it really matters. Most of whatever value people are getting from any kind of hands-on healing method is coming from the only seriously active ingredients: touch, time, and relationship. When you get some decent pain relief from a session with a massage therapist or a chiropractor — or even a naprapath — that is almost always what should get the credit.
- “The MELT Method® (MELT®) is a simple self-treatment that reduces chronic pain and helps you stay healthy, youthful, and active for a lifetime.” Dramatic health claims are made on the about page: sleep better, more energy, improve posture, lose weight!
- The FasciaBlaster™ is a massage tool that allegedly “lessens the look of cellulite, improves blood flow, helps reduce pain, accelerates muscle recovery.”
- Airrosti’s slogan is “We Fix Pain Fast” and they claim that “Most patients report complete injury resolution in an average of only 3.2 visits.” Although Airrosti is not obviously related FDM, and fascia isn’t barely mentioned on their website, it is clearly a member of the myofascial release family, and may even have been directly “inspired” by FDM, an alleged copycat method — which I am neither affirming nor refuting. See Can Airrosti Really Resolve Most Chronic Pain in Just Three Visits?
This is instrument-assisted soft tissue mobilization (IASTM), best-known from the Graston Technique and Astym brands. They claim to break up “scar” tissue (a “fascial distortion” by another name) and stimulating healing by provoking an inflammatory response. I discuss this “breaking some eggs to make an omelette” philosophy in Tissue Provocation Therapies in Musculoskeletal Medicine.
![Photo of a Graston technique, a massage modality, being applied man’s upper back and shoulders, using a chrome tool about a foot long, slightly curved.]()
The steel massage tools of
Graston Technique®.- The main example of this style is John Barnes’ Myofascial Release.
- Thalhamer C. A fundamental critique of the fascial distortion model and its application in clinical practice. Journal of Bodywork and Movement Therapies. 2017 2017/10/30. PainSci Bibliography 52740 ❐ “A literature review found no clinical trials or basic research studies to support the empirical foundations of the FDM contentions.”
Thalhamer again:
In the context of fascial therapies, results from theory and basic research are frequently transferred to the clinical setting. Such transfer is not permissible since this strategy has often been shown to lead to false conclusions (Ioannidis 2005; Guyatt 2008). An appropriate first step to rectify this situation would be to conduct randomized controlled clinical trials with appropriate long-term follow-up to verify whether FDM actually has a specific treatment effect. Only when such a specific effect has been discovered does it make sense to speculate about the plausible mechanisms of action underlying FDM treatment.
- Most notably hypermobile-type Ehlers–Danlos syndrome (EDS), and several more sub-types of EDS, and then several more poorly understood conditions under the umbrella of hypermobility spectrum disorders (HSD). “The essential difference between HSD and hEDS lies in the stricter criteria for hEDS compared to the HSD.” But it’s very tricky, and those criteria are all very new: see the 2017 EDS International Classification.
- Scheper MC, de Vries JE, Verbunt J, Engelbert RH. Chronic pain in hypermobility syndrome and Ehlers-Danlos syndrome (hypermobility type): it is a challenge. J Pain Res. 2015;8:591–601. PubMed 26316810 ❐ PainSci Bibliography 52758 ❐ Hypermobility is “highly prevalent among patients diagnosed with chronic pain.”
- Rodgers KR, Gui J, Dinulos MBP, Chou RC. Ehlers-Danlos syndrome hypermobility type is associated with rheumatic diseases. Sci Rep. 2017 Jan;7:39636. PubMed 28051109 ❐ PainSci Bibliography 52757 ❐
hEDS patients may see multiple subspecialists without realizing a connection between their joint symptoms and multi-systemic involvement of the disease; they are often dismissed as hypochrondriacs, and report feelings of isolation from the lack of diagnosis.
Perhaps due to a lack of gravitas surrounding the hEDS diagnosis, management of the disease varies among practitioners, and clinical workup does not often extend beyond the joint and skin examination.
Gray’s Anatomy for Students:
Clinically fascias are extremely important because they often limit the spread of infection and malignant disease. When infection or malignant diseases cross a fascial plain, a primary surgical clearance may require a far more extensive dissection to render the area free of tumor or infection.
A typical example of a fascial layer would be that overlying the psoas muscle. Infection within an intervertebral body secondary to tuberculosis can pass laterally into the psoas muscle. Pus fills the psoas muscle but is limited from further spread by the psoas fascia, which surrounds the muscle and extends inferiorly into the groin pointing below the inguinal ligament.
- Milesobrien.com [Internet]. O’Brien M. “Just a Flesh Wound”; 2014 Jun 22 [cited 14 Nov 27].
- Dahl M, Hansen P, Stål P, Edmundsson D, Magnusson SP. Stiffness and thickness of fascia do not explain chronic exertional compartment syndrome. Clin Orthop Relat Res. 2011 Dec;469(12):3495–500. PubMed 21948310 ❐ PainSci Bibliography 53566 ❐
Biopsies of the fascial compartment of the anterior tibialis muscle were taken from several patients with compartment syndrome, with compartment syndrome and diabetes, and some healthy individuals for comparison. Although there was a lot of variability between individuals, on average there were no important differences, and in fact stiffness was 70% greater in the healthy patients — exactly the opposite of what one would expect to see if compartment syndrome was caused by stiff, thick fascia. The authors concluded that “structural and mechanical properties are unlikely to explain chronic compartment syndrome. To prevent chronic exertional compartment syndrome, it is necessary to address aspects other than the muscle fascia.”
- Juhan D. Job’s body: a handbook for bodywork. expanded ed. Barrytown; 1998.
If you can manage the density of the language, Job’s Body is thick with creative insights into physiology and healing. Perhaps too many of them, and perhaps too creative — but very stimulating.
Juhan tries to explain why bodyworkers often seem so uncannily effective, which is a job that certainly needed doing.
In trying to explain bodywork, Job’s Body is a philosophical introduction to the science of the human body — a physiology textbook with a heart. Many chapters are devoted to pure science — just barely accessible to the layperson, and mainly offering perspective for the health care professional.
Still more chapters are devoted to pure philosophy. Juhan frequently dares to ask and answer the hardest questions in the health sciences: why and so what? It’s a mixture of the genuinely thoughtful and deepities that would drive me nuts today. (A deepity is a vague idea that sounds “deep” but is actually either profound-but-false or true-but-trivial.)
I took a workshop with Juhan many years after I first read his book. I’m sorry to say that he seemed cocky and jaded. My main impression was that he had drunk too much of his own Kool-Aid, and was bored with the subject matter.
- The full details of how bone responds to stress are spelled out in Dr. Harold Frost’s Mechanostat model. For more information, see Tissue Provocation Therapies in Musculoskeletal Medicine.
- This kind of (wild) speculation is hardly unusual for Oschman: his writings are laced with much stranger ideas. His entirely pseudoscientific body of work is routinely cited by those who want to believe in “energy medicine.” I was actually a fan of his in the years before I learned some critical thinking skills. Unfortunately, as soon as I developed a basic understanding of how science works, I quickly figured out that he’s one of the best modern examples of a pseudo-scientist and not even remotely credible. Not everything he says is wrong, of course–like many pseudo-scientists, he usually leads his pronouncements with a series of easily defended premises to get you nodding (yeah, CT is ubquitous, wow, cutting edge stuff there) … but then he starts making unjustified leaps of logic and extrapolations. He’s supremely overconfident about what is known and knowable, and his publications unfailingly provide support for alternative therapies, especially “energy medicine.” And fascia fans just eat it up: anything that makes fascia seem more magical!
- Dr. Robert Schleip, from his 2003 article, “Fascial plasticity: a new neurobiological explanation”:
The half-life span of non-traumatized collagen has been shown to be 300–500 days, and the half-life of ground substance 1.7–7 days (Cantu & Grodin 1992). While it is definitely conceivable that the production of both materials could be influenced by piezoelectricity, both life cycles appear too slow to account for immediate tissue changes that are significant enough to be palpated by the working practitioner.
- The quoted passage is from my personal correspondence with Dr. Levin, and is used with his permission and endorsement. For information about Dr. Levin’s work, see Biotensegrity: A new way of modeling biologic forms.
- You could argue that Bishop et al. 2016 is an example of the biology of fascial distortion: evidence of thickened fascia in people with back pain. There’s an entire section about that below, but it doesn’t amount to much, and even if it did it’s important to note that it came twenty-five years after the founding of FDM: that’s a long time to be guessing!
- Schleip R. Fascial plasticity: a new neurobiological explanation. Journal of Bodywork & Movement Therapies. 2003 Jan;7(1):11–19. PainSci Bibliography 54759 ❐
Reader Jeff Linn, “something of an apostate Rolfer and instructor at one of the major structural integration schools,” offers a nifty clarification for me on this point. He has done extensive research in the Rolf Institute and Guild for Structural Integration archives and has listened to quite a bit of Rolf’s lectures. He has an audio clip of Rolf saying that the sol/gel idea is a “nonsense teaching.” Transcript:
… under your hands you feel the change. Now this is going to call for some smart researching sometime. And who’s going to do this I don’t know. I hope somebody is going to come out of the blue who is going to be peculiarly well-fitted for this kind of a job. And I haven’t the foggiest idea what it means. Possibly it means a general change in pH of the tissue locally. Possibly it means, this is the simplest way to express it, the greater energy that goes in there and makes the sol, the gel a sol. Possibly this is what it means. This is what I’ve taught that it means. But this is a nonsense teaching really! What does it make into ‘sol’? Does it make the wall of the blood vessel sol? This is absurd!
Mr. Linn: “My impression from listening to somewhere around 100 hours of Rolf’s lectures is that many of her ideas regarding her theory were preliminary and/or provisional and that she expected research to be done (which never really was). Her provisional ideas were simply assumed to be gospel and elevated to dogma and transmitted accordingly.” The transcript is from Tape A5 1970, Side 1, available to members only on www.rolfguild.org.
A reader asked me: “Why would a bodyworker yank painfully on my nostrils?”
Why indeed! My answer: pure therapy theatre. Specifically, this a melodramatic clinical gesture intended to impress patients with the therapist’s creative, eccentric wisdom, and exotic skill… but which is, in fact, utter bollocks. 🙄
This particular bit of bollocks was popularized by Ida Rolf. It is pretentiously called “nasal work,” a part of “cranial work.” Arguably it is the apotheosis of bullshit in massage, and the rationale for it was delusional, self-aggrandizing nonsense. This is from an interview of Jim Asher in The “Journal” of the Rolf Institute (December 2012), talking about Ida Rolf’s mentorship on the subject of nasal/cranial work:
DG: You mentioned that in her nose work, she didn’t go all the way in. Did she talk about going into the three conchae?
JA: Yes. She’d say there are three conchae in there, and that the goal is to get them open. She’d say, “You do what you can do.” Sometimes she would just get into the bottom one, which is the largest. She’d have you look at your anatomy book, and she wanted you to visualize those three conchae opening. Ida was a big believer in visualization. You visualized what’s underneath the skin and the connections [while you were working on it]. When you’re doing the sacrum, you’re visualizing the dural tube and all the way up, feeling up through the body.
DG: Did she ever mention any esoteric reasons for doing the nose work, like doing a Rolfing session on the brain or opening the third eye, or anything like that?
JA: Yes. She would have you visualize the pituitary gland, say “You’re affecting the pituitary gland.” She was especially interested in the pituitary. Sometimes she would talk about the third ventricle as well.
And that’s the tip of the nonsense iceberg. I wish I could say it was just colourful 1970s silliness, but it lives on. This is still an embarrassingly common kind of pseudoscience in massage therapy to this day … and very closely associated with fascial therapy.
Here’s Dr. Schleip’s full reasoning from his article, “Fascial plasticity: a new neurobiological explanation”:
In most systems of myofascial manipulation, the duration of an individual ‘stroke’ or technique on a particular spot of tissue is between a few seconds and 1½ minute. Rarely is a practitioner seen — or is it taught — to apply uninterrupted manual pressure for more than 2 minutes. Yet often the practitioners report feeling a palpable tissue release within a particular ‘stroke’. Such rapid — i.e. below 2 minutes — tissue transformation appears to be more difficult to explain with the thixotropy model. As will be shown later, studies on the subject of ‘time and force dependency’ of connective tissue plasticity (in terms of creep and stress relaxation) have shown that either much longer amounts of time or significantly more force are required for permanent deformation of dense connective tissues (Currier & Nelson 1992).
- Some people will undoubtedly protest this, claiming that they certainly get more flexible in a sauna. Heat alone, without stretching, will definitely make us feel less stiff (a change in sensation), but does not actually increase flexibility. I’ve tested this very carefully myself: see A Stretching Experiment.
- Ingraham. Does Massage Increase Circulation? Almost certainly not in a clinically important way, and definitely not as much as even a small amount of exercise. PainScience.com. 11473 words.
- ScienceBasedMedicine.org [Internet]. Kavoussi B. The Acupuncture and Fasciae Fallacy; 2011 Jan 13 [cited 14 Sep 24]. PainSci Bibliography 54882 ❐
- ScienceBasedMedicine.org [Internet]. Ramey D. Acupuncture and history: The “ancient” therapy that’s been around for several decades; 2010 Oct 18 [cited 20 Sep 10]. PainSci Bibliography 54827 ❐
- ScienceBasedMedicine.org [Internet]. McKenzie B. How popular is acupuncture?; 2011 Mar 28 [cited 12 Feb 19]. PainSci Bibliography 55276 ❐)
- ScienceBasedMedicine.org [Internet]. Atwood KC. Acupuncture Anesthesia: A proclamation from Chairman Mao; 2009 May 15 [cited 12 Feb 19]. PainSci Bibliography 55489 ❐
- Berman BM, Langevin HH, Witt CM, Dubner R. Acupuncture for Chronic Low Back Pain. N Engl J Med. 2010 Jul 29;(363):454–461. PubMed 20818865 ❐ PainSci Bibliography 54942 ❐
A bizarre and already infamous paper: bizarre because the authors clearly acknowledge that acupuncture is no better than a placebo, and bizarre because they conclude that it should be recommended, and most bizarre of all because it is published in The New England Journal of Medicine. Truly, one of the lowest moments in the history of that famous journal!
The best criticisms of the NEJM’s editorial choices here can both be found on Science-Based Medicine, by Drs. Crislip (NEJM and Acupuncture: Even the best can publish nonsense) and Novella (Acupuncture Pseudoscience in the New England Journal of Medicine). Dr. Crislip’s post is really quite funny.
- Some fascial therapy is gentle, but I have personally encountered intense fascial therapy in the wild on numerous occasions. I prefer gentler therapy and usually request it. Despite being a confident and assertive communicator about my preferences, I have still had many unpleasantly intense fascial therapy experiences.
According to a great many therapists. Not all, but probably most. It’s spelled out clearly by a prominent fascial therapy pioneer, Luigi “Inventor of Fascial Manipulation” Stecco (see Stecco). This is someone who has the respect of large numbers of fascial therapists; his thinking about how fascial therapy works can be considered strongly representative not only of common thinking about fascial therapy, but also of its bleeding edge. In his review of the rationale for fascial manipulation, he repeats the basic idea of tissue stuckness in need of releasing in an impressive array of fancier terms. This is just a small sample:
Once a limited or painful movement is identified, then a specific point on the fascia is implicated and, through the appropriate manipulation … movement can be restored.
- “Mechanical deformation” is lasting change in the shape of the tissue, like working clay. This is in contrast to elastic deformation, where the tissue snaps back to its pre-manipulation state. To “deform” in this context is not a bad thing (as in deformity), but a change in form — the goal that therapists generally have, in fact.
- People are not bulletproof thanks to their fascia, alas — wouldn’t that be handy! And yet the hyperbole is definitely true in a sense. Fascia is mostly much too thin to actually be bulletproof. If fascia was just as thick as a Kevlar vest, it might well be just as bulletproof (or a little more, or a little less). This is just like how spider silk is “stronger than steel cable” — pound for pound, it is. The catch in the comparison is that fascia most likely doesn’t have the same “puncture resistance” property that Kevlar does. There are many kinds of toughness (i.e. bones resist compression exceedingly well, but are quite vulnerable to torsion). The point was simply that the research showed quite clearly that the forces required for plastic deformation of fascia significantly exceed what can be applied to it with hands. Whatever therapists are feeling when they claim to detect a “release,” it’s not that.
- Schleip R. Fascial plasticity: a new neurobiological explanation. Journal of Bodywork & Movement Therapies. 2003 Jan;7(1):11–19. PainSci Bibliography 54759 ❐
While high-velocity thrust techniques might create forces within that range, it seems clear that the slower soft tissue manipulation techniques are hardly strong enough to create the described tissue response [plastic deformation of fascia]. This research leads to a simple thought experiment. In everyday life the body is often exposed to pressure similar to the application of manual pressure in a myofascial treatment session. While the body naturally adapts structurally to long-term furniture use, it is impossible to conceive that adaptations could occur so rapidly that any uneven load distribution in sitting (e.g. while reading this article) would permanently alter the shape of your pelvis within a minute.
- Sometimes I felt things that seemed “big” that the patient seemed not to notice at all. Sometimes the patient had a profound sensory experience when I had noticed no change in the tissue whatsoever. I could not consistently elicit anything clearly. I am not a dumb guy, but I found it all quite uninterpretable and mostly unpredictable. I got tired of trying to find meaning in my sensations, and by my last three years in practice I abandoned all conceit that I could induce specific changes in tissue, and started focussing on my patients’ sensations rather than my own.
- Schleip 2003, op. cit.
- I am almost quoting a prominent fascia researcher here: this is exactly how he described the significance of the findings in a discussion on Facebook. It’s not an unusual interpretation of the study in my experience, but I want to emphasize that it was spelled out by someone with great credibility to fascia enthusiasts.
- Ingraham. Massage Does Not Reduce Inflammation: The making of a new massage myth from a high-tech study of muscle samples after intense exercise. PainScience.com. 5631 words.
- Yin Z, Sun J, Liu T, et al. Gum chewing: another simple potential method for more rapid improvement of postoperative gastrointestinal function. Digestion. 2013;87(2):67–74. PubMed 23306595 ❐
- If it’s bad enough to think that you need help, you’re also too sore to want anyone to touch you (let alone push on you). In any case, post-exercise muscle sorness is usually all wrapped up before patients can get to an appointment.
- Ingraham. A Deep Dive into Delayed-Onset Muscle Soreness: The biology & treatment of “muscle fever,” the deep muscle soreness that surges 24-48 hours after an unfamiliar workout intensity. PainScience.com. 17437 words.
Not actually “muscle cells,” but myofibroblasts. That is, they are like a cross between a muscle cell and a fibroblast, the fibre-generating cells that build connective tissue. Myofibroblasts are cousins of muscle cells, and I’ve oversimplified for a mixed audience here and just called them muscle cells, which expresses their most relevant feature: they are contractile. You could also oversimplify in the other direction and describe them as a type of fibroblast. Regardless, they are definitely a distinct subspecies and interesting in their own right. Because they are “muscular,” reader Annemarie Frank, a Brazilian physical therapist who teaches workshops on this topic, calls them “hulk fibroblasts.” A couple of other interesting points about them:
Myofibroblasts are not always present in fascia; they only form in specific biological situations, like the combination of inflammation with mechanical tension. And they are also quite potent collagen producers, just like regular fibroblasts.
For more about these fascinating cells, see “Mysterious Myofibroblast: A Cell with Diverse Origin and Multiple Functions” and Boris Hinz’s review, “Myofibroblasts”.
- Is it really surprising? I’ll return to that question below. That phrasing doesn’t actually come from the paper, so you won’t find it there, but from a poster they made to summarize the paper.
- Or perhaps somewhat to one side of the middle …
- A millinewton is 1000th of Newton, which is a measurement of force. A full Newton is not a lot: enough to accelerate a mass of one kilogram at a rate of one meter per second squared, without friction. Imagine what it would take to get a small weight moving a little bit … in space. Now divide by a thousand.
- I’d like to think I made it sound “accurate,” and the result just happens to be trivial.
- A little personal perspective: my lovely wife has titanium in her back, installed to stabilize a massive fracture of her T12 vertebra in 2010. Such is the toughness of spines that the titanium fixations installed to protect her actually broke on both sides — came loose from the brackets screwed into her bones. Similarly, severe scoliosis can twist titanium fixations like pretzels as it advances. Those are the kinds of forces involved in the back. Fascial contractions are a miniscule part of such impressive equations.
- It is also noteworthy that the contractions they described were slow motion contractions, taking many seconds to develop at their fastest.
- Analogy: in the circulatory system, there are only a few gigantic blood vessels, but countless fine and microscopic ones. The fascial system is similar: a few large, obvious sheets of fascia, a bunch of more modest and delicate structures, and then a nearly infinite network of extremely thin and microscopic structures. This is why I say that we are wrapped in fascia “fractally.”
- Ingraham. Your Back Is Not Out of Alignment: Debunking the obsession with alignment, posture, and other biomechanical bogeymen as major causes of pain. PainScience.com. 21878 words.
- Despite what it seems like, I am not actually accusing Schleip et al. of having any overt or serious conflicts of interest. COIs are more common and less of a big deal in science than people think: where there is science there is funding, such is life, and funding sources affect science in muddy, complicated degrees ranging from not really at all to truly, madly, deeply. This seems like a borderline case to me, somewhere on the edge of being a problem. It’s safe to say that these organizations probably would not fund — or continue to fund — research that came to the opposite conclusion, i.e. not “strong enough to influence low back stability and other aspects of human biomechanics.”
- This is another form of what I call failing “the impress me test.” Usually I bring that up to make the point that there needs to be strong evidence that treatments works before they can be considered “proven” — small and temporary treatment effects should not impress anyone. In this case, though, it’s the clinical relevance of fascial contractility that is failing to impress.
- Schleip R, Naylor IL, Ursu D, et al. Passive muscle stiffness may be influenced by active contractility of intramuscular connective tissue. Med Hypotheses. 2006;66(1):66–71. PubMed 16209907 ❐
- If you’re not going to list really good, relevant examples here, where are you going to do it?
- I have written quite a lot about compartment syndrome with regards to their role in shin splints (see Shin Splints Treatment, The Complete Guide). The lower leg is by far the most common place in the body for compartment syndromes, both in the shins and the calf. They are more or less unheard of elsewhere in the body — rare and generally minor and self-limiting. If fascial compartments were prone to problematic contraction, we’d constantly be getting “compartment syndromes” all over the body.
- Basically, only a fraction of the genome is for coding proteins, but that important minority is regulated and tweaked by the rest of the non-coding DNA. So a (very rough) analogy is that the coding DNA is like software that makes you who you are, but the “junk” DNA is the operating system that it needs to run on. Not so junky.
- Langevin HM, Stevens-Tuttle D, Fox JR, et al. Ultrasound evidence of altered lumbar connective tissue structure in human subjects with chronic low back pain. BMC Musculoskelet Disord. 2009 Dec;10:151. PubMed 19958536 ❐ PainSci Bibliography 53554 ❐
- Langevin HM, Fox JR, Koptiuch C, et al. Reduced thoracolumbar fascia shear strain in human chronic low back pain. BMC Musculoskelet Disord. 2011 Sep;12:203. PubMed 21929806 ❐ PainSci Bibliography 53517 ❐
- Bishop JH, Fox JR, Maple R, et al. Ultrasound evaluation of the combined effects of thoracolumbar fascia injury and movement restriction in a porcine model. PLoS One. 2016;11(1):e0147393. PubMed 26820883 ❐ PainSci Bibliography 52796 ❐
- Langevin HM, Bishop J, Maple R, Badger GJ, Fox JR. Effect of stretching on thoracolumbar fascia injury and movement restriction in a porcine model. Am J Phys Med Rehabil. 2017 Sep. PubMed 28901961 ❐
- Back pain is an extremely complex phenomenon, and these findings may not be consistently measurable: no other researchers have even tried yet (2017). It’s par for the course for findings like this to be elusive. As ever in science and life, what you “see” depends on how you “look.”
- Langevin 2009, op. cit. They measured the thickness of lumbar connective tissues with ultrasound in 60 chronic low back pain patients and 47 health people.
- Langevin 2011, op. cit. This is an ultrasound study of the motion of layers of connective tissue in the low back in 70 people with chronic low back pain compared to 50 healthy people. Subjects lay on a motorized table that flexed their lower backs, while a probe inserted under their skin took an ultrasound “movie” of their thoracolumbar fascia.
- Bishop 2016, op. cit. “The combination of injury plus movement restriction had additive effects on reducing fascia mobility with a 52% reduction in shear strain compared with controls and a 28% reduction compared to movement restriction alone.”
- Langevin 2017, op. cit.
This experiment injured pigs as in Bishop 2016, but then attempted to reverse the fascial stiffness they’d induced by restoring normal movement and/or stretching the pigs for a few minutes a day.
In a nutshell, they failed.
Thirty pigs which were divided into three groups: ten that were unmolested, ten that were injured, and ten that were injured and hobbled for eight weeks. After that, a few of the hobbled pigs remained hobbled, while the rest were either set free and stretched for 10 minutes per day, or just set free. Removing the hobble improved the pigs’ gait speed — imagine that — but adding stretching was no better. The fascial stiffness induced by the torture did not change. Their conclusion:
Reduced fascia mobility in response to injury and movement restriction worsens over time and persists even when movement is restored. Reversing fascia abnormalities may require either longer than 1 mo or a different treatment "dose" or modality.
- Langevin et al. speculate about the cause: “genetic factors, abnormal movement patterns and chronic inflammation.”
- Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. The thoracolumbar fascia: anatomy, function and clinical considerations. J Anat. 2012 Dec;221(6):507–36. PubMed 22630613 ❐ PainSci Bibliography 52795 ❐
The reduction in shear-strain could be due to tissue adhesions induced by previous injury or inflammation, and could then be consistent with the proposed etiology suggested by Dittrich (1963) and Bednar et al. (1995). However, as the authors of this recent study [Langevin 2011] emphasize themselves, it is also possible that the observed tissue changes are merely the result of a reduction (immobility) in everyday lumbar movements related to low back pain. In this case, the fascial changes would be the effect of low back pain rather than a cause.
- Not that 10 minutes per day was likely to do the job or is in any way comparable to fascial therapy for humans — but it is a clue that you can’t just pull on the stuff to loosen it up.
- Nagy MT, Macfarlane RJ, Khan Y, Waseem M. The frozen shoulder: myths and realities. Open Orthop J. 2013;7:352–5. PubMed 24082974 ❐ PainSci Bibliography 53682 ❐
The nature of frozen shoulder is addressed in detail in my full frozen shoulder tutorial.
- Aota Y. Entrapment of middle cluneal nerves as an unknown cause of low back pain. World J Orthop. 2016 Mar;7(3):167–70. PubMed 27004164 ❐ PainSci Bibliography 53097 ❐
- Probably because of biological x-factors, non-structural problems. Biochemistry. Nutrition. Cellular business. Maybe patient X is vulnerable to that cluneal nerve impingement because of a vitamin D or magnesium deficiency. Or a medication side effect. The biological consequences of sleep deprivation, or sleep apnea (blood gases get weird with that condition). Or the chronic stress of social isolation. Or “inflammaging.” Or any one of about ten thousand other possibilities. The list of could-be’s is almost literally endless.
- Modern pain science shows that pain is as hard to predict or control as the weather, a function of countless chaotic variables, surprisingly disconnected from seemingly “obvious” causes of pain. Pain is jostled by many systemic variables, but especially by the brain’s filters, which thoroughly “tune” pain and often even overprotectively exaggerate it — so much so that sensitization can get more serious and chronic than the original problem. This has complicated all-in-your-head implications: if the brain controls all pain, does that mean that we can think pain away? Probably not, but we do have some neurological leverage — maybe we can influence pain, if we understand it. See Pain is Weird: Pain science reveals a volatile, misleading sensation that comes entirely from an overprotective brain, not our tissues.
- Stecco C, Pirri C, Fede C, et al. Dermatome and fasciatome. Clin Anat. 2019 Oct;32(7):896–902. PubMed 31087420 ❐
This paper tries hard to use fascia as a way to explain the imprecision of dermatomal patterns (areas of skin sensation arising from nerve roots), a well-known phenomenon that has a variety of simpler explanations, and wasn’t particularly in need of another one. It even substantially duplicates an existing idea (sclerotomes).
While potentially interesting and not necessarily all wrong, the paper is generally poor quality, overconfidently reaching well beyond both evidence and plausibility in a variety of ways, but it’s basically just a partisan opinion about why fascia matters — which is catnip for fascia therapists, who are starved for scientific legitimacy and have frequently cited this paper as if it actually matters. It really doesn’t.

{kind=link}