
There are many paths to pain that never make headlines.
38 Surprising Causes of Pain
Trying to understand pain when there is no obvious explanation
In healthcare, we’re always trying to help people with problems we don’t fully understand, using treatments we don’t fully understand. The world is full of unexplained pain particularly, with many dozens of possible causes. By far the most important thing to understand about treating chronic pain is that it is difficult because it almost never has one cause: it is extremely multifactorial. It’s always a game of Whac-A-Mole with chronic pain — but with some really strange moles. And well-camouflaged moles.
I publish a busy website about pain, and so I get email like this more often than I change my socks:
I’ve been to every medical specialist you can imagine. They can’t find anything wrong with me. The psychiatrist says it’s not in my head, and the rheumatologist says it’s not in my body. But something is causing my pain. It’s not an infection or a fracture or a cancer. It’s not a sprain or a pinched nerve or a cattle prod. What else is there? What else is left?
What else indeed? When “obvious” and known causes of pain have been eliminated, what next? What else causes pain? How else can pain start, change, worsen? This article summarizes 38 of the not-so-obvious ways to hurt, the things that might help you understand pain that has defied diagnosis or explanation so far. There are a lot more possibilities, but it’s a start, and this article hopefully focusses on the most important.
A lot of pain is unexplained
A man hid a little wad of marijuana up his nose, and then lost it up there and then forgot it for almost twenty years — oops! — until it started causing severe headaches:
Through the years he suffered recurring sinus infections and had trouble breathing out of the right side of his nose. But he didn’t connect the problems to his lost cannabis. It wasn’t until 18 years later — when he was struggling with headaches and had a CT scan of his brain — that doctors finally discovered the petrified pot.
Doesn’t get much more surprising than that! There are countless other less bizarre possibilities. The “official” causes of all kinds of chronic pain break down into three roughly equally large categories, plus one small “other” category:1
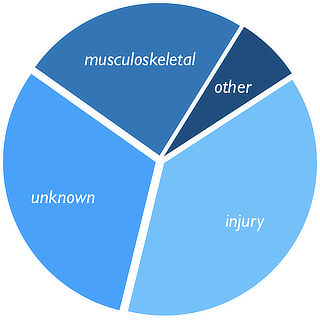
- injury (38%)
- unknown (31%)
- musculoskeletal (24%), a vague category dominated by arthritis, the rheumatic diseases, and headaches
- other (7%), which is mostly cancer and abdominal pain plus “everything else” (mostly pain related to major physiological systems, and one-in-a-zillion cases like petrified pot up your nose)
Arthritis and the rheumatic diseases should probably be in their own major category, and almost everything else filed under “unknown.” Pain after injury is surprisingly murky: sure, it might have started with an injury, but two years later is that still the “cause”? It has usually transmogrified into something else, and exactly how that works is much more about the “unknown” than “injury.” Many cases of chronic pain are hard to put in just one of these categories (or they only seem easy to place). As you browse around this article, you’ll notice that most causes of pain are hard to categorize.
Misdiagnosis is routine, of course, especially self-diagnosis. We desperately want answers — pain “demands” an explanation by nature… and it usually gets one, whether it makes a damned lick of sense or not. We need to be quite cautious about reaching beyond our knowledge.
Hypochondriac nightmare fuel
A lot of the examples in this article are high-grade hypochondriac nightmare fuel, and it’s always risky to share information like that: stories about horrifying, insidious causes of pain can truly freak patients out (with a nocebo, the opposite of a placebo2), but most of them have pain that is not this ominous and will pass soon enough.
But such stories are also useful data points about the extreme diversity of hard-to-diagnose causes of chronic pain — an underestimated diagnostic challenge that needs more light. Both pros and patients need to have greater respect for that challenge because there are so many individually rare possibilities that they are collectively common. The chances of having any one weird cause of pain are extremely low, but the chances of having some pathological curve ball… not so rare!
Table of Contents
Basic mechanisms, processes, and concepts (potentially relevant to many injuries or illnesses, and a lot of these overlap partially or even completely):
- Sensitization (somatic and visceral)
- Chronic pain does not work like acute pain
- Psychological amplification
- All in your head: pure psychosomatic pain
- Pain with literally no specific cause
- Muscle spasm, tension, contracture
- Referred pain
- Spatial summation
- The pain of stuckness
- Pain as a learned response (classical conditioning)
- A genetic defect that exaggerates all sensation
- Stupid, stupid neutrophils
- Chronic systemic inflammation and “inflammaging”
- “Toxins” and poisons
- Neuroinflammation
- Unexplained neuropathy (especially channelopathy)
- Non-obvious nerve entrapment
- Loneliness, social isolation, and “social distance”
- Smoking (probably just a major proxy for “poor health”)
- Stealthy foreign objects
And some specific pathologies (things that can be diagnosed, and in some cases treated)…
- Trigger points
- Complex regional pain syndrome (CRPS)
- Myelopathy (spinal cord impingement, especially and probably intermittent)
- Radiculopathy (e.g. sciatica) is surprisingly weird … and then there’s multiple-level radiculopathy
- Claudication: the pain of impaired blood flow
- Ehlers–Danlos syndrome and the hypermobility spectrum disorders
- Nutritional deficiencies: vitamin D and magnesium
- Mitochondrial disease
- Adenosine monophosphate deaminase 1 (AMPD1) deficiency
- Post-viral syndrome: chronic immune activation after infection
- Syphilis
- Early stages of …
- Drug related:
Appendices: Examples and relevant musings
- Two stories of diagnosing mysterious pain
- Pain demands an explanation … and it usually gets one, whether it makes a damned lick of sense or not
Sensitization
Pain itself often modifies the way the central nervous system processes pain, so that a patient actually becomes more sensitive and gets more pain with less provocation. This is called “central sensitization.” (And there’s peripheral sensitization too.) Sensitized patients are not only more sensitive to things that should hurt, but also to ordinary touch and pressure as well. Their pain also “echoes,” fading more slowly than in other people. This phenomenon is usually superimposed over other problems, but it can also occur acutely and be the primary issue, as in complex regional pain syndrome, or amplified pain syndrome, which can happen to anyone but affects more girls and young women.
Importantly, sensitization can affect our guts more than skin, muscles, and joints. Visceral sensitization can be caused by stress, which may be one reason why stress is so closely linked with abdominal pain.
Sensitization is the Boss of All Risk Factors. Most conventional risk factors for common pain problems are surprisingly bad at predicting who’s going to do poorly. When combined with sensitization, they get much more predictive.3 For example, signs of arthritis on a scan correlate poorly with actual pain; but arthritis + sensitization does! That’s a big deal. Fortunately, it is relatively easy to self-asses your own sensitization status: see Sensitization in Chronic Pain: Pain itself can change how pain works, resulting in more pain with less provocation.
Chronic pain does not work like acute pain
Chronic and acute pain are radically different. Chronic pain is not just acute pain that kept going. Over several weeks, the nature of pain changes. Unfortunately, we actually still don’t have a good understanding of how it changes. It probably involves a complex stew of the ideas in this article. For instance, sensitization (see above) is clearly a major factor. Emotional and physical stresses are strongly linked to chronic pain, but we’re not sure exactly how.
The “neuromatrix” theory of pain suggests that pain is produced by “widely distributed neural network in the brain rather than directly by sensory input evoked by injury, inflammation, or other pathology.”4
Translation (and the important thing for desperate patients to understand): chronic pain rarely continues to be driven by tissue in trouble, and starts to become a kind of “neurological habit” — regardless of whether any tissue is still in trouble. In many cases, it’s not! The pain is a kind of ghost of the original, a tormenting poltergeist. The analogy to “phantom limb pain” is strong: it’s like phantom limb pain, but without losing a body part.
Psychological amplification
Not pain that’s “all in your head” pain, but pain that is seriously “aggravated by your head.” The brain may amplify pain substantially as a consequence of stress, anxiety, fear. Like an ulcer, there can be a physical problem, but one that is also sensitive to your emotional state.5 Sometimes, the brain’s interpretation of a situation becomes a major part of the issue, or even the dominant factor — still not “all” in your head, but “a lot” in your head. Like picking at a scab, the brain can become excessively focused on a pain problem. For more information, see Pain is Weird: Pain science reveals a volatile, misleading sensation that comes entirely from an overprotective brain, not our tissues.
Amplified pain exists near one end of a spectrum: acute pain with a clear cause is at one end, chronic pain driven entirely by the mind at the other. With a clear traumatic trigger, the diagnosis of “amplified” pain seems apt: there was a painful problem originally, it just got exaggerated by the power of the mind. The more disproportionate that amplification gets, the more like pure psychosomatic pain it gets.
Please note that this concept is quite controversial, with passionate and nuanced views from one of the spectrum of possibilities to the other, and no sign of a definitive answer in sight.
All in your head: true psychosomatic pain
Pure all-in-your-head chronic pain is probably quite rare. Unexplained chronic pain is routinely chalked up to psychology. “Patients often find themselves trapped in a zone between the worlds of medicine and psychiatry, with neither community taking full responsibility.” (O’Sullivan) But, in most cases, there’s a diagnosable cause that simply hasn’t been diagnosed yet, and that’s the main reason this article exists. Most pain patients need better diagnosis, not a psychiatrist.
But at least a few probably do need a psychiatrist. Pure psychosomatic pain probably does exist. Some tension headaches are probably good examples of how mental state can directly drive pain with no clear intermediate mechanism. Amplified pain is a much more extreme example, which makes it quite clear that psychological factors can dominate chronic pain. The phenomenon of functional neurological disorder (FND, formerly known as “conversion” disorder) makes it even clearer: seizures, paralysis, blindness, and other neurological symptoms in the absence of neurological disease.67
Even the most psychological of all cases of chronic pain likely still have a seed, something that originally inspired the pain, making them extreme cases of “amplified pain” (see previous section), and not technically “pure” psychosomatic pain. But if the trigger is subtle enough, relative to the psychosomatic consequences, then it’s psychosomatic for all intents and purposes, and the trigger no more defines the problem than a grain of sand defines a pearl.
Pain with literally no specific cause, especially just poor health
Like other complicated things in life, pain may not have any specific cause at all. Although we often speak of pain being multifactorial, we still tend to assume that just one of those factors is the specific cause of pain, and the other stuff — sleep loss, stress, etc — is just piling on, making a bad situation worse. That picture may be wrong: some chronic pain is probably an emergent property of a big mess of synergistic stresses and poor health and fitness, with literally no specific cause. It may crop up only with an unholy combination of many factors. This is a systems perspective on pain and malaise.
How does nothing in particular actually make us hurt? There are two main neurobiological suspects: sensitization and neuroinflammation lower our thresholds for pain and malaise. They can occur independently but are usually entangled. They are certainly set in motion by major trauma and disease, but — and this is the systems perspective — probably mainly just by being really out of shape, our health and fitness ground down by many forces. There are definitely cases of pain with "no specific cause" in seemingly fit people, but not many, and many of them probably are simply unfit in non-obvious ways.
Major factors in poor health — sleep deprivation, smoking, obesity, social isolation — are all well known to correlate with pain, and all of these get more attention below. But the general principle of pain without any particular cause is very important, and poor health and fitness is probably the most important example of how that works. It may be a good news scenario in the sense that it might be treated by simply getting into shape. But it’s bad news in the sense that getting into shape is often a lot easier said than done.
“Spasms”: cramps, dystonia, spasticity, etc (including and especially when they have a pathological origin)
Muscle tissue is everywhere — our most massive biological system — and its subtler hijinks can cause a lot of discomfort without giving itself away. No one has any doubt about the cause of pain when they get a massive calf or foot cramp. And there are morbidly fascinating examples of extremely painful cramping, like the literally lethal spasticity of rabies, a disease that literally kills with cramps, yikes.8
But not all cramps are so obvious! There are many types of insidious, uncomfortable and dysfunctional muscle contractions, and it is a perpetual mystery exactly how much they account for common kinds of pain.
For instance, although dystonia is often obvious, it can also be subtle and get mistaken for ordinary musculoskeletal problems, like the case of a hockey referee who spent months investigating a presumed knee injury — but he was actually in the early stages of Parkinson’s disease, and physical therapists and surgeons all missed it for too long.9 Or another example of an even younger athlete, where diagnosis was a little less delayed, but still looked like “typical musculoskeletal symptoms” for a while at first, and the patient even seemed to respond well to being treated as such.10
This is a broad category of trouble, which contains a number of specific examples, some of which are discussed below, like “trigger points” and the “multiple sclerosis hug” (spasticity of the ribcage), and vaginismus (spasticity of the vaginal and pelvic floor muscles). Using just a wide brush for now, the types of unwanted contractions that cause the most trouble without being easy to diagnose are cramps, dystonia, and spasticity. “Spasm” — as in a “back spasm” — is an informal and non-specific term that could be used to “explain” a lot of musculoskeletal pain, and could refer to any of the more specific types of pathological contractions.
Fun fact: if your muscles are contracted for long enough, they will actually “freeze” like that: essentially scarred into place, a phenomenon called “contracture.”11
See Cramps, Spasms, Tremors & Twitches: The biology and treatment of unwanted muscle contractions.
Referred pain
Referred pain results in an amazing amount of medical barking up the wrong tree.
Anything that hurts inside the body — anything deeper than skin — is harder for the brain to locate. This is partly because we literally just don’t have enough nerve endings for it, and partly because the nervous system isn’t perfect and signals literally get “crossed.” The practical result of this is that internal pain with any cause may be felt somewhere completely different. Despite the fact that this phenomenon is well known, it still results in an amazing amount of medical barking up the wrong tree. Referred pain isn’t exactly a “cause” of pain, but it belongs in this list because it’s an important concept that can help to explain many pain problems that otherwise don’t make sense. For instance, both of the examples at the beginning of this article were cases where referred pain fooled doctors — in both cases, the pain was caused by a trigger point in a nearby muscle, not by vital organs. The doctors simply looked in the wrong place!
Spatial summation and why some body areas suffer more, like the neck and back
If five bees stung you all at once, in one small area on your back, you would probably think you had been stung by one super-bee (or maybe that you’d been poked with a cattle prod). Two sources of pain close together will be felt as one larger painful spot, a neurological effect called “spatial summation.” Pain perception is low resolution, and the brain can merge pains that are up to 20cm apart.12 This might explain why some areas of the body, like the neck and back, are more prone to pain: either the brain can “sum” more widely spaced sources of pain in some places than others, and/or some areas simply have more to sum up, more potential sources of pain. Just recently, research showed that we have roughly the same perceptual “resolution” for pain everywhere in the body,13 so the spine is probably not a common trouble spot because we cast a wider summation net there. This makes it even more likely that there’s just more to sum in the spine: lots and lots of tissues that often have minor problems, which get perceived as a smaller number of worse problems. This could also help to explain the chronicity of spinal pain: if you have “one” back pain problem that is actually coming from two nearby sources, you’re going to think you have the same back pain problem until both sources are relieved, which is probably going to take longer.
The pain of stuckness
Here’s a simple experiment: assume an awkward posture and stay there. How long can you last? Within an hour you will probably be in severe pain. Why? You haven’t actually damaged anything! But we seem to be wired to avoid stagnancy, probably because every cell in our body depends on nearly constant movement to survive. The exact mechanism of pain is probably nerve endings that detect tension on cartilage, ligaments, and tendons, and which in turn is interpreted by the brain as a surprisingly serious threat. But here’s the kicker: this effect is potent enough that it can be triggered without an obviously awkward posture. It can be caused by surprisingly subtle postural stresses (like from poor ergonomics), or anything that deprives tissue of full movement. When a joint feels “stuck,” for instance, and there is no obvious way (and sometimes no anatomical way) of moving to get “unstuck,” the sensation can escalate to a screaming itch-you-can’t-scratch. This may be the main cause of neck cricks, for instance, and scads of other miscellaneous aches and pains.
Pain as a learned response (classical conditioning)
Some chronic pain may be a “learned response” to things that shouldn’t hurt, like Pavlov’s dogs salivating to the ring of a bell — classical conditioning. It’s an interesting idea, with obviously optimistic implications, because what is learned might also be un-learned. Classical conditioning is not widely believed to be a factor in chronic pain, but it’s broadly plausible, with several lines of reasoning and evidence that point straight to it (without taking us all the way there).
For instance, it’s already well-established that people can have truly serious pain experiences as a response to the perception of threats that don’t actually exist, like the one about the guy who was in agony from a nail that had been driven through his boot… but it had actually gone between his toes. Such stories are a novelty when the illusion of danger can be definitively dispelled, but threat perception is usually messier — and likely to crop up again and again in response to subtle sensory cues. If you always respond the same way to the same stimuli, boom, that’s a perfect setup for classic conditioning. That’s how we might “learn” to hurt.
No one knows if or how much this actually occurs, but it’s a fascinating concept, and I consider it a neglected area of research. For much more information, see: Chronic Pain as a Conditioned Response: If pain can be learned, perhaps it can be unlearned.
A genetic defect that exaggerates all sensations (pain included)
This is just one of several possible causes of sensitization (discussed above), but it deserves to be singled out because it’s so interesting: some cases of chronic pain may be partly or entirely caused by a common genetic defect,14 a good specific example of how unexplained pain is linked to genetics.15
This glitch results in low levels of the neurotransmitter serotonin, which appears to exaggerate bodily sensations, which is rich soil for chronic pain to take root in. Patients with unexplained chronic widespread pain are notorious for having many, many other odd symptoms.
And it’s a common genetic defect, mind you. Not rare. At ten percent of the population, it’s about five times more common than red hair. Wow. Read more.
Again, this is only one of many examples of genes that contribute to pain.16 If we are "programmed" to suffer, why even bother trying to treat pain? Because the only thing worse than mysterious chronic pain… is mysterious chronic pain complicated by factors that might have been preventable if only we'd tried.17
And you’re probably underestimating how many subtle pathologies are out there, or just random odd health headwinds thanks to genetics and microorganisms.
Stupid, stupid neutrophils
Neutrophils are defender cells that are supposed to destroy bacteria that invade wounds, a normal part of the inflammatory response to injury. Bizarrely, neutrophils go to work even when the wound is sterile, not open to the outside world. Like an overzealous police force with nothing better to do, they also attack a common cellular organ, mitochondria, whenever it is spilled from cells by injury. Mitochondria are actually honoured symbiotic guests that convert our food to energy for us. Normally we live out our lives in perfect harmony with mitochondria, biological BFFs. But when they get the chance, neutrophils target and hunt them like they are invaders18 because for millions of years they haven’t gotten the evolutionary memo that mitochondria should be left in peace.
Inflammation often seems excessive because it is, because
For more information, see A Painful Biological Glitch that Causes Pointless Inflammation: How an evolutionary wrong turn led to a biological glitch that condemned the animal kingdom — you included — to much louder, longer pain.
Chronic systemic inflammation and “inflammaging”
Chronic systemic inflammation associated may be a factor in stubborn musculoskeletal pain (as well as much else). We get more inflamed as we age, a process quaintly known as “inflammaging” (real word). Inflammation may be how other problems do their painful work, or it might seem to exist for no obvious specific reason — either an obscure cause, or just many things. Inflammaging correlates strongly with poor fitness and obesity, also known as metabolic syndrome, the biological precursor to diabetes and heart disease. And that, in turn is linked to chronic psychological stress, and of course biological stresses like smoking, alcohol abuse, and sleep deprivation. The “harder” we live, the more inflammaging and metabolic syndrome we get.
It’s not the years, honey. It’s the mileage.
Indiana Jones
And there are some other less certain but still plausible reasons why inflammation might escalate as we age, sometimes too much too soon:
- chronic subtle infections and/or collateral damage from past infections
- “Toxins” and poisons
- menopause
- allergies, which often worse in middle age
- “hard living” is a problem, but so is soft-living: sedentariness is probably directly inflammatory
A separate article covers these in more detail, with many specific examples, plus ideas about mitigating them, and some of the more eyebrow-raising examples are highlighted in other sections here (the green links in the list above).
“Toxins” and poisons
I am loathe to demonize “toxins” or “chemicals” because quacks are so busy doing that already. But detox scams benefit greatly from a large seed of truth: there are many poisons in our world. None are likely to be the main, direct cause of pain, but they might cause general vulnerability to pain and injury in a variety of ways (but mainly inflammation). These are only likely to be relevant to pain if they are in a speculative Goldilocks zone: severe enough to matter, but not enough to be easily diagnosed. But there are very likely some like that.
- Pollutants are a huge category, the nastiest of which are in the subcategory of persistent organic pollutants: hundreds of chemicals like DDT, dioxins, flame retardants, and the notorious polychlorinated biphenyls. All of those are known hazards, but the risk in practice varies widely. Lead is also still an alarmingly common environmental poison, and does more harm than any other known chemical hazard. And, of course, a huge source of poisoning is really ordinary: smog! Traffic-related air pollution, especially diesel exhaust, is a very real danger for all non-rural humans.
- There are major open scientific questions about the emerging threats of the forever chemicals (the PFAS) and microplastics. We know they are there, but the hazards are poorly understood, and the risks are still a near total mystery.
- Surgical implants and especially surgical meshes are another interesting example. While many people claim to have been made sick by surgical meshes (and I am inclined to believe them), it remains essentially undocumented. Some other surgical implants are well-documented examples of internal poisoning.
- Drug “side effects” may be caused by contamination, or by allergic reactions and other kinds of idiosyncratic sensitivities and intolerances. While the individual risk is probably low, the pool of possibilities here is vast.
- Mould can certainly be toxic, but it’s unknown whether it can be a subtle threat. There's a hypothesis that some people can become hypersensitive to mould, greatly increasing their danger, but this is untested.
- Food additives have always been especially popular scapegoats for cranks, quacks, and grifters. However, there probably are a few problematic chemicals in our diet. Trans fats aren't a "food additive" per se, but they are ubiquitous and shockingly harmful. Artificial sweeteners probably don’t deserve their reputation as carcinogens and metabolic wrecking balls (both well studied), but they may well be a strain on gut health (not studied). The fat replacers (sucrose polyesters) are known gut irritants, and still in the food supply in small doses. The very old modern additive "manufactured citric acid" may be harmful, but no one has ever really checked.
- Some actual foods are also problematic for some people: setting aside frank allergies (which are common), there are plenty of intolerances and sensitivities that often go undiagnosed, most notably lactose intolerance. Even celiac disease, a serious pathological gluten sensitivity, can fly under the diagnostic radar, but there are likely other kinds of sensitivity and intolerance to the chemistry of wheat (gluten and/or the FODMAPs and/or the amylase-trypsin inhibitors).
All of these are explored in much more detail, with citations, in my inflammation article.
Neuroinflammation
Imagine an inflamed nervous system — it’s probably just as unpleasant as it sounds! In fact, it is nearly synonymous with feeling “sick.”
What we’re only just beginning to understand is that milder versions of neuroinflammation may be more subtle and insidious. It may have non-obvious causes, or happen more than it’s supposed to (like an autoimmune disease). It’s even possible — though highly speculative — that it could be triggered by severe chronic stress (see the “systems perspective”). Like stress itself, neuroinflammation is a generalized response — regardless of the trigger, the system has the same effect.
This may explain how many baffling symptoms work,20 even just hurting too much. What better way to force an animal to take it easy than to make everything hurt too easily? Neuroinflammation probably drives “sensitization” — lowered pain thresholds, basically.21
Unexplained subtle neuropathy (especially channelopathy, especially small fibre neuropathy)
“Neuropathic” pain is the ultimate false alarm: pain caused by trouble with the nervous system itself. It’s the difference between engine trouble and trouble with that light on your dashboard that says there’s engine trouble. There are many blatant neuropathic pain problems, such as spinal cord impingement (discussed below), but humans also suffer from a surprisingly high rate of unexplained and/or subtle neuropathies, where the pain-reporting system is just kinda a bit wonky for very complex and poorly understood reasons. Neurologists are often stumped by their patients!
Up to one-third of people seen in an average general neurology clinic have neurological symptoms that cannot be explained and, in those people, an emotional cause is often suspected.
It's All in Your Head, by Suzanne O’Sullivan, 9
Suspected but probably often wrong (see psychosomatic pain). Specifically, for instance, a lot of this trouble may be driven by channelopathy and small fibre neuropathy, which are poorly understood genetic pathologies related to “dysfunction of ion channels located in the membranes of all cells and many cellular organelles.”22 There are hundreds of possible genes involved. It’s a surprisingly common type of problem that’s basically still beyond the power of medicine to deal with. In other words, it’s about a common glitchiness at the tiniest scale of biology. It doesn’t just affect nerves, but, when it does, they misbehave in all kinds of ways, many of them probably painful.
Small fibre neuropathy is the most obvious type of channelopathy that causes neuropathic pain. It is caused by progressive degeneration of small-diameter nerves, and ultimately caused by a mixture of genetic and other unknown factors; it is linked to erythromelalgia, fibromyalgia, Ehlers–Danlos Syndrome, and long covid. SFN can be a clear diagnosis, but — and this is the point — for every obvious case, there are probably many that aren’t.
Unexplained neuropathy has many pathological explanations, if only we could see them. See also neuroinflammation and mitochondrial disease, other possible root causes of puzzling neurological problems.
Non-obvious nerve entrapment
Usually when you have a pinched nerve, the symptoms are obvious: zinging “electrical” pain, tingling, and numbness are the signatures of a distressed nerve. Unfortunately, peripheral neuropathy does not always announce itself so clearly. Sometimes all you get is pain.23 This predicament usually leads to a wild goose chase for more “mechanical” causes of pain. Consider this remarkable case study of cluneal nerve entrapment…
The cluneal nerves pass from the low back and sacrum into the buttocks, just under the skin, and they can get tangled up with ligaments and connective tissue on their way, potentially causing chronic low back pain. In 2016, Aota reported on “a case of severe low back pain, which was completely treated by release of the middle cluneal nerve.”24 Exploratory surgery identified nerves “entrapped in adhesions.” They cut them free … and that was the ticket. The patient was decisively cured. Which is pretty cool. But that was after years of suffering, and a pointless surgery on her intervertebral discs.
As straightforward as that example is, it is also possible that her problem was not the nerve “snag” per se but a biological vulnerability to feeling it. It’s likely that nerve entrapments only cause trouble when combined with other hard-to-diagnose problems… like some of the other things in this article. No one really knows.
Loneliness, social isolation, and “social distance” (and not the way we mean it in the pandemic)
Social isolation — “loneliness” if you’re unhappy about it — is a major general health suppressor in the same league as other major vulnerabilities like sleep deprivation or smoking.25 It almost certainly involves increased vulnerability to chronic pain as part of the deal.26 We do know that sensitization and pain chronicity are driven by catastrophization and social factors, and injury and disability are going to seem more threatening — more “catastrophic” — to people without good social connections, all other things being equal.
It can be tough to make friends, stressful even, and often it’s hardest for the people who need it the most27 — but it’s a worthwhile investment.
The term and related concept of “social distancing” was hijacked by the COVID-19 pandemic. It used to refer to the chasm between social classes. Inequality and prejudice undermine health in many insidious ways, including “loneliness,” but definitely not limited to it. See Chronic Pain and Inequality (“Physical distancing” is the better term in the context of disease prevention!)
Stealthy foreign objects
There are some amazing stories of foreign objects embedded painlessly in flesh for years or even decades at a time before they finally flare up and get identified and excised. For instance, Art Lampitt had a serious car accident in 1965 — and then, fifty years later, his arm started to ache and swell. An x-ray revealed a strange, thin third arm bone: the turn signal lever from the 1963 Thunderbird he had crashed in. It had been embedded in his forearm, nestled between his ulna and radius, invisible and asymptomatic for decades.28
Another man had a bullet in his hand for seventy-five years before it started to bother him.29 Interestingly, it also migrated several centimetres from the original scar.
What fascinates me about these cases is the “why now?” factor. Why would a foreign object suddenly start causing trouble, after so many years? Although rare, the principle is important and there are probably ten minor cases for every dramatic one. I suspect there are quite a few puzzling pain stories out there that are caused by something much harder to diagnose than a turn signal or a bullet.
Smoking (probably just a major proxy for “poor health”)
Smoking doesn’t hurt per se — not directly — but smokers hurt. Smoking has already come up in the context of things that probably increase systemic inflammation, which is likely a major way that it increases the risk of pain. However, it’s such a powerful independent predictor of pain30 — that is, smokers are quite a lot more likely to suffer from pain, regardless of anything else about their health status — that it probably does its dirty work in multiple ways, and should be called out as a cause of pain in its own right. That seems reasonable for anything that makes several types of pain two to three times more likely.
Most likely this is just yet another strong sign that poor health is the real problem, which works in many ways, and almost any amount of smoking just guarantees poor health. See Smoking and Chronic Pain.
Muscle Knots
Most of us have some unexplained sore spots, which mainly feel like sensitive muscle tissue (but also tendons and ligaments). And some of us have a lot of them.
These are often called muscle knots informally, or “myofascial trigger points” only slightly more formally (and many other names over the decades). They seem to be involved in a lot of the world’s aches and pains.
There’s good news: as common and vexing as these sore spots are, many seem to be relieved by a bit of simple stimulation, just a little rubbing, like scratching an itch. For a basic primer, see Basic Self-Massage Tips for Myofascial Trigger Points. For an insane amount of information, see my book on this topic: The Complete Guide to Trigger Points & Myofascial Pain.
Complex regional pain syndrome (CRPS), the most extreme specific form of sensitization
Most pain “sensitization” — lowering the pain threshold — is a normal, temporary reaction to injury, a common, and temporary state. You cut your finger and the tissue around the cut is much more delicate while it heals.
But sometimes this reaction spins out of control, becoming a disease in its own right. The most extreme example of this phenomenon is complex regional pain syndrome, which causes extreme pain, usually in a limb, and usually following some relatively minor tissue insult like an insect bite, a minor cut, or a small fracture.
When it’s full-blown, the seriousness CRPS is impossible to understate — patients describe it as “an act of evil” that results in “becoming sub-human.”See “A malevolent force”: The profound, bizarre impact of CRPS.
And yet there almost certainly are milder variations of it. Many times in my career I have become quite convinced that a patient had to be suffering from some lesser form of CRPS, awful but not enough to clinch a CRPS diagnosis.
Whenever something painful happens to me, amid all the distress I am surprised at being reminded of how painful pain is. That thought is always followed by another, “What if I hurt like this all the time?” Chronic pain syndromes are extraordinarily debilitating.
Why Zebras Don’t Get Ulcers, by Robert M Sapolsky, p. 396
Myelopathy and dysautonomia
An irritated spinal cord — usually irritated by being slightly pinched by a narrow spinal canal — can cause an astonishing variety of problems, including pain, without ever clearly giving itself away. Symptoms can be in virtually any location in the body, if the location of the trouble is high in the spine. This can go on for years, bad enough to cause pain but never bad enough to be easily diagnosable.
Worse, there’s some intriguing evidence that “minor” irritation of the upper spinal cord may be uniquely problematic, causing “dysautonomia” — excessive sympathetic arousal, causing you to react as if stressed.31 This weird low-grade crazy-making effect is new and still uncertain, but it is nicely consistent with the much firmer, recent discovery that the autonomic nervous system is very disturbed in the aftermath of major spinal cord injuries, causing organ failure32 — a clinical reality historically overshadowed by the seriousness of paralysis. Subtle dysautonomia from chronic mechanical irritation of the spinal cord is definitely a plausible, sinister, and thoroughly obscure explanation for some chronic pain and anxiety.
Radiculopathy (e.g. sciatica) is surprisingly weird … and then there’s multiple-level radiculopathy
Radiculopathy is irritation of the thick nerve roots that emerge from the spine, and subdivide into nerve trunks and branches that carry motor and sensory information to and from the musculoskeletal tissues. Radiculopathy causes "radicular" pain, and sciatica is the canonical example: buttock and/or leg pain, sometimes zapping all the way down to the feet. It also includes weakness and sensory disturbances that can be quite weird. That’s the “surprising” part.
As usual with musculoskeletal medicine, it’s not as forward as it seems like it should be: pinch a big nerve somehow, get a big pain, sort of like hitting your funny bone but deeper and slower. But the fates of nerve roots are complex. It's not mechanical compression alone that irritates them, but the whole metabolic milieu. Anatomical variation accounts for considerable variety in exactly where symptoms are felt. For reasons no one really understands, sometimes the pain is on what seems to be the wrong side. And so on. Symptom chaos! Plenty of radiculopathy is obvious, but quite a bit of it is not.33
For lumbar radiculopathy, lower leg pain is the only fairly consistent symptom, and it’s more likely to be radicular pain if it’s also worse than any back pain, and if it comes with some pins and needles. The situation in the neck is analogous: pain radiating to below the elbow that's worse than the neck, plus some parasthesia. (Thoracic radiculopathy is happily rare.)
But for a startlingly awful kind of nerve root pinching, you need to pinch more than one nerve root. Multiple-level radiculopathy is one of the more spectacular and surprising ways to hurt. This is unlikely (maybe even impossible) without some other kind of serious health problem, especially a spinal disease like ankylosing spondylitis (a dangerous spinal arthritis). And yet the kaleidoscopic radiculopathy symptoms may be the first sign of trouble. Patients struggling with profound, chaotic, and non-specific neurological trouble — and therefore many resemble fibromyalgia patients.
Claudication: the pain of impaired blood flow
Sometimes an artery gets narrowed or pinched off and causes serious pain. Although simple in principle, it tends to get missed in younger people, where it’s a relatively rare problem, and so the suspicion falls on other things. It also gets missed because “musculoskeletal” is a realm of medicine where circulatory function is rarely considered at all. But it should be an easy diagnosis: claudication tends to cause a deep aching pain exclusively with exertion (when tissues are demanding oxygen), which isn’t how most musculoskeletal problems behave. Sometimes it is easy, like a straightforward case of a cyclist with a couple months of leg pain and weakness with exertion.34
And sometimes it’s not easy…
A patient had sciatica-like leg pain for thirty-five years and was misdiagnosed many times until finally getting not only a definitive diagnosis but a cure.35 He had a narrowed artery (arterial stenosis causing “claudication,” the pain of impaired circulation). That’s it! Not even a difficult diagnosis in the end, really. There were some pretty glaring clues there that got ignored by a lot of people who should have known better.
But not only was he misdiagnosed many times over more than three decades, he was misdiagnosed fashionably: that is, each misdiagnosis neatly fit a paradigm in physical therapy (better than it fit his symptoms). This carried on right up to and including the present day fascination with psychosocial factors and sensitization (which served him no better than any of the other paradigms had). Taylor and Kerry:
Interestingly, the patient’s belief that something ‘was actually wrong’ had remained with him throughout the journey. This, of course, had been explained away to him (more recently) by current research and evidence-based thinking on central sensitization and pain.
Just fascinating. The authors thoughtfully explore the implications of this rather shameful episode. The bottom line? Good diagnostic skills are never out of fashion. Or shouldn’t be, anyway!36
Hypermobility spectrum disorders and Ehlers–Danlos syndrome
Hypermobile patients get hurt easily and have a lot of chronic body pain.37 There are many types of hypermobility, with a wide range of severity, from trivial party trick flexibility in one or two joints (“double-jointed”) with no apparent consequences — especially early in life — all the way to full-blown genetic disorders of the connective tissue with many serious medical consequences. There’s a huge grey zone in the middle of under-diagnosed and under-treated people, who are definitely having problems but may never figure out why or what to do about it.
Hypermobility spectrum disorders (HSD) are a group of conditions defined by joint hypermobility — unexplained joint looseness. HSD is a bucket diagnosis for people with symptomatic hypermobility, but without a connective tissue disorder that explains it, like Ehlers–Danlos syndrome or Marfan syndrome. Most connective tissue disorders are relatively obvious, but EDS can easily evade diagnosis, making it a prime suspect in many cases of chronic pain…
Ehlers–Danlos syndrome (EDS) is a group of conditions that includes hypermobility along with fragile tissues that injure easily and heal poorly (especially skin), with many consequences. The most common form of EDS is hypermobile EDS (hEDS). It’s tricky to distinguish hEDS from HSD.38 However, hEDS is probably associated with serious rheumatic diseases (i.e. psoriasis, ankylosing spondylitis, rheumatoid arthritis)… and this is fresh science and likely to be missed, “perhaps due to a lack of gravitas surrounding the HEDS diagnosis.”39
Given the musculoskeletal troubles that we know hEDS can cause, it is reasonable to guess that less severe hypermobility (HSD) may also be both clinically important and yet even less obvious.
So, hEDS/HSD is serious … but it’s not taken seriously. Even doctors who know about hEDS/HSD usually assume that it’s mostly a minor condition, and would definitely not refer patients on to a rheumatologist.
For more information, see the PainSci guide to hypermobility: Hypermobility and Ehlers-Danlos syndrome: In patients with persistent and widespread muscle pain.
This was written by Lynn (@brickandbutton) on Apr 9, 2019 [original gone]. She added in a comment: “I’ve come to a point after 7 years where I’m still fighting (and waiting) but I expect to be this severely sick forever. Anything else will be a fun surprise.”
Vitamin D and magnesium deficiencies
There is not a single supplement or anti-inflammatory superfood that is clearly beneficial for any common kind of pain, but there are a couple nutritional deficiencies that stand out as more legitimate suspects in many chronic pain cases. Pain might be the only symptom of either one.
Vitamin D deficiency is on the firmest ground. It is probably more common than once suspected — at least 1 in 20 people in the lowest estimates,40 and possibly many more.41 It can cause subtle widespread pain that may be misdiagnosed as fibromyalgia and/or chronic fatigue syndrome, including symptoms like muscle and bone aching,42 fatigue and weakness, lower pain threshold, and more acute soreness after exercise that is slower to resolve. For more information, see Vitamin D for Pain.
Magnesium deficiency is also a suspected factor in chronic pain, especially migraines and neuropathy.43 Some people are aware that magnesium supplementation is one reason for Epsom baths, a dubious method of getting the stuff into your body (especially compared to oral supplementation). We just don’t know yet if magnesium is helpful for pain44 or any kind of cramping.45 Ironically, magnesium (in a clinical setting) is known to actually induce cramping and severe muscular pain, so none of the biology is straightforward. What biology is?
Mitochondrial disease
Mitochondria are the microscopic organs that generate energy, invariably described as the power plants of our cells. They produce energy and, it turns out, they may also distribute it, like a network of power lines.46 Mitochondria can malfunction like anything else in biology: disease on an extremely small scale, of literally microscopic “organs.” There’s still a great deal of research to be done to understand the problems mitochondria have, but we do know that it can cause an astonishing variety of symptoms including chronic pain and, of course, fatigue.47 Although rare, it has even been identified in cases of isolated muscle pain.48
Mitochondrial disease might prove to be the key to understanding some of the mysterious syndromes as well as a deeper explanation for more familiar diseases, especially in neurology. Notably for pain patients, there’s probably overlap between this topic and neuroinflammation and channelopathy, other low-level biological problems linked to chronic pain, like sensitization and neuroinflammation.
Adenosine monophosphate deaminase 1 (AMPD1) deficiency
This is yet another example of a disease that can cause chronic pain and yet easily go undiagnosed for years: adenosine monophosphate deaminase 1 deficiency (AMPD1). Rare, but not crazy rare (we’ve all met probably someone with this). Genetic. Often asymptomatic.
But when there are symptoms? Muscle pain, cramping, weakness, fatigue. Vague, non-specific symptoms. All symptoms of other things! Such symptoms often don’t even trigger suspicion. When people have mild to moderate symptoms like this they often just think things like “aging sucks” and “I’m just weird that way I guess.”
Even when the symptoms are more serious, and people take more seriously, they know that it’s very hard to get doctors to take vague symptoms seriously. Or they quickly find out the hard way.
Post-infection syndromes: chronic immune activation after infection
You can “win” the battle with an infection and still lose the war, suffering for long after, because some pathogens pollute our biology in a way that does permanent damage or just keeps causing new damage. For instance, the Borrelia burgdorferi bacteria causes Lyme disease, but many people continue to suffer even when all the B. burgdorferi are dead — a previously unexplained phenomenon called post-Lyme disease syndrome. The cause — entirely unknown until quite recently — is probably a lingering molecule produced by the bacteria during their campaign. In 2019, researchers discovered that B. burgdorferi sheds a peptidoglycan (PGBb) molecule while it grows, which collects in joints especially and continues to provoke an immune system response, causing ongoing inflammation and malaise.49 Although “just one study” of a controversial topic, the study was highly persuasive, especially the part where they induced acute arthritis in mice by injecting them with PGBb.
Although the primary symptom is painful arthritis, a chronic immune response like this would also tend to provoke generalized illness — fatigue, malaise, sensitization — via the mechanism of neuroinflammation.
If correct, then this study has solved one of the bigger puzzles in medicine — a big deal — but it also demonstrates an extremely important general principle: immunity is a double-edged sword with many, many complications that are impossible to guess. If this can happen, and avoid detection for decades, you can be damn sure there’s more like it. There are many examples of the poorly understood long-term consequences of infections, such as the link between Epstein-Barr virus and multiple sclerosis50 — and MS can have a long period of vague symptoms before diagnosis.
And then, of course, there’s long COVID. Long COVID hurts: a whopping 12% of patients still have painful, swollen joints a year after infection.51 COVID is also known to actually murder both nerve and muscle cells (inflammation and necrosis) long after acute infection, probably due to prolonged circulation of inflammatory molecules (cytokines) rather than direct infection of the cells.5253 Neuromuscular complications like this are known from many other viral infections: COVID is just a particularly good, well-studied example.
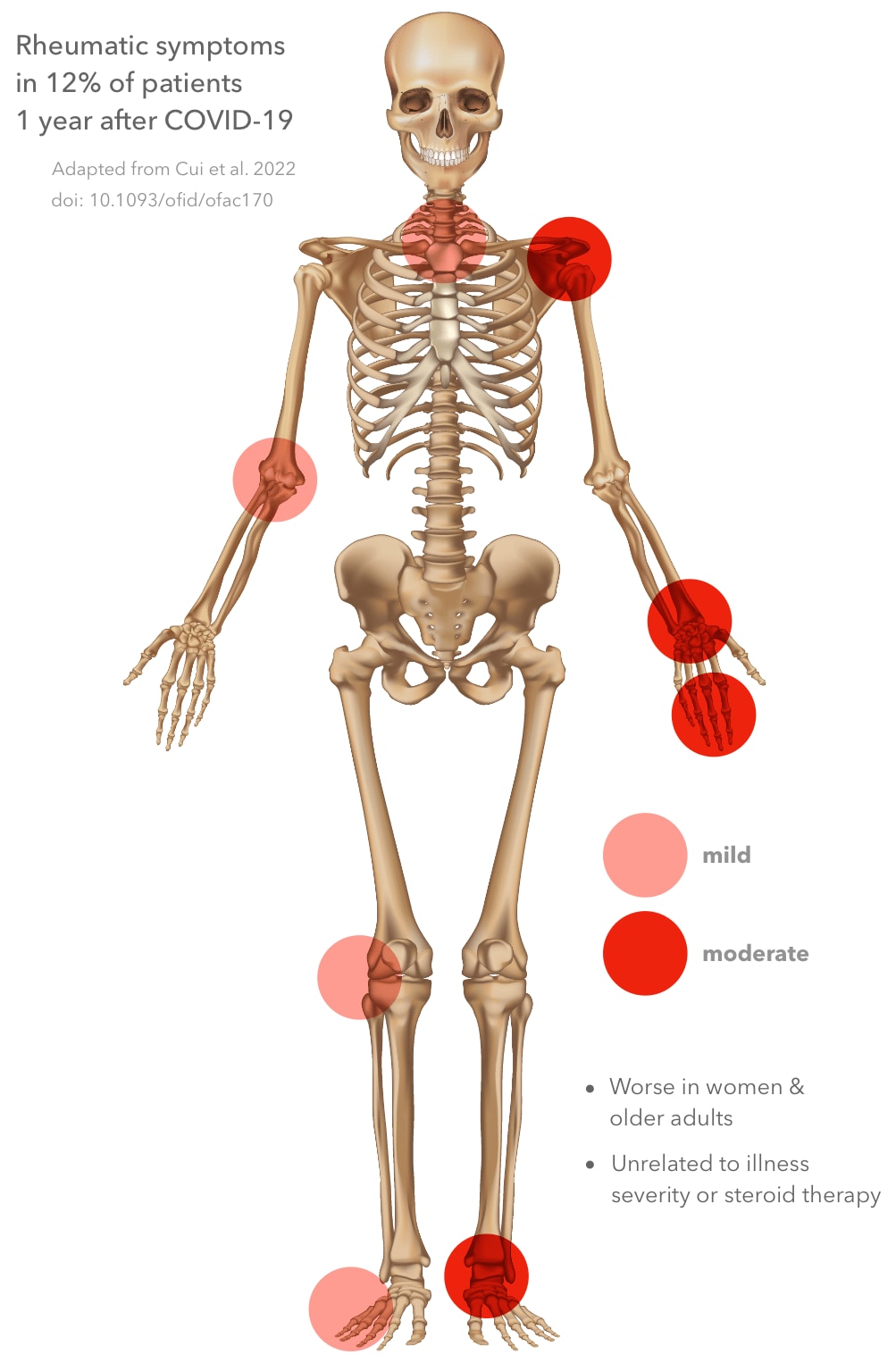
Diagram of the human body showing joints most affected by rheumatic symptoms. Adapted from Cui 2022, PMID # 35611349.
Multiple sclerosis prodrome [early stages]
Another classic hypochondriac’s diagnosis, multiple sclerosis is all too real, and the most common autoimmune disorder of the central nervous system. So it’s another autoimmune disease, but it’s one that is particularly common, serious, and prone to causing pain and other woes well before diagnosis. It definitely does not cause primarily pain in every patient; the classic onset of multiple sclerosis is more blatantly neurological in character (tingling, numbness, weakness, and so on). But some patients definitely start with pain, and spasm is the primary mechanism. One particularly good and sinister example: the “MS hug,” which feels like a painfully tight band around the chest. Although the feeling of constriction is the classic symptom, many patients also just experience widespread and erratic pain in the chest wall, probably from erratic, isolated painful contractions.
A diagnosis of multiple sclerosis usually isn’t anywhere near as slow to come as, say, a lupus diagnosis. It will probably reveal itself sooner rather than later. But there is definitely potential for a period of unexplained pain.
Syphilis
Yes, believe it or not, syphilis can actually be a stealthy cause of pain. The first sign of syphilis is a lesion that is often minor and easily missed: usually painless, often inaccessible, nearly identical to a canker sore when it’s in the mouth. The second stage consists a few weeks of malaise and rashes. If the rashes aren’t clear enough, this stage is often mistaken for the flu or just an inexplicable phase of the blahs. The disease then goes dormant to some degree, for years, or forever, but in some people it will develop into the final stage, which is where the chronic aches and pains may develop (just one of a great variety of possible symptoms). It’s a slow disease that can affect many organ systems, so diagnosis often takes a long time, despite frank pathology that can be easily diagnosed with the right tests. Some patients with unexplained chronic widespread pain (fibromyalgia) probably have syphilis.
Facioscapulohumeral Muscular Dystrophy [early stages]
I have a good friend, someone I’ve known for most of my life, who has this common and usually mild form of muscular dystrophy. It was undiagnosed for decades because the symptoms were subtle and he wasn’t even trying to figure it out. By his late 30s, his upper trapezius wasting away, he was initially misdiagnosed with frozen shoulder among other things, until he finally got the correct diagnosis — and then he started to see how the disease explained an awful lot about his life, many experiences and personal “quirks”… like a lifelong tendency to excessive soreness after exercise!54
Even his father’s life made more sense: the disease is genetic, and he obviously struggled with it, stoically, undiagnosed from cradle to grave. Biology is destiny, and this condition is a really good example of it. How many people out there are in that multi-decade period of wondering why they get so sore so easily, before finally being diagnosed with FSHD?
Autoimmune diseases [early stages]
The autoimmune diseases are a huge class of pathologies that can cause essentially any non-specific symptoms for a long time before diagnosis. These are conditions like lupus, rheumatoid arthritis, celiac disease, inflammatory back pain (spondyloarthritis, a common cause of the phenomenon of morning back pain), and many, many more. Lupus is one of the most common and notoriously unpredictable and slow to develop. Some people with a variety of weird aches and pains and other symptoms are going to end up getting diagnosed with lupus eventually, but it can take literally years for the situation to clarify. It’s a classic hypochondriac’s diagnosis, because of its many possible vague symptoms that overlap with anxiety symptoms.
Also note the interesting possibility but that subtle/atypical autoimmune disease may be synonymous with excessive "inflammaging" (the systemic inflammation that affects us all as we age, but too much and too soon in some people).
Lymphoma (cancer of the lymphatic system, lymph nodes)
Lymphoma is a cancer of the infection-fighting cells of the immune system, cells in the lymph nodes, spleen, thymus, bone marrow, and other parts of the body. These cells grow out of control. Although relatively easy to treat, as cancers go, it’s also notorious for causing unpredictable symptoms for long periods before diagnosis. There is a classic first sign that’s hard to miss — badly swollen lymph nodes — but quite a few cases are more subtle, mainly just various forms of “the blahs” and a couple more distinctive symptoms like night sweats and itching. The swollen nodes are not painful, and pain is not a classic symptom … but it can happen, depending on where tumours are forming and what they are pressing on, and possibly because of ramped up systemic inflammation.
Other cancers
Cancer is not one disease, but a complex family of disease with many faces. Lymphoma is relatively common and notorious for causing pain as an early symptom, so I singled it out above. But other cancers can do this, and collectively they are a non-rare source of puzzling pain … even problems that seem like very conventional body aches and pains. For example, Physical therapist Michelle Morrow on the tingling in her right hand and forearm:
“My symptoms mimicked cubital tunnel syndrome very well and even had an acute onset after overuse.”
But it was not a common neuropathy. It was a brain tumour. 😬 Yet another case of a “simple” musculoskeletal problem that was the tip of a central/systemic iceberg.
So what’s the teachable moment? Why share a story like this, when it really could make some readers worry excessively about their tingles? The point is to combat the plague of oversimplification in sports/pain medicine, where simplistic “mechanical” diagnoses constantly drown out the messier physiological factors that are often the real story. Very few of those causes are ominous, of course, but it is the scary ones that make the most vivid examples. They remind us to think a little bigger than the traditional bogeymen of musculoskeletal medicine: posture, scar tissue, spasms, spinal alignment and such.
Reserve a few minutes to read this: “The wilderness of the medically unexplained.” This is a really well-written and heart-wrenching tale of a cancer that flew under the diagnostic radar for quite a while. It’s going to be poignant for anyone who has felt like a medical mystery … so, you know, just about everyone with chronic pain. I’m not sure that anyone involved could have done much better. Things that are tough to diagnose are tough to diagnose, and that’s just life. And death.
But please, doctors (and anyone responsible for diagnosing): try to remember that when you hear hoofbeats in Texas, sometimes it really is bloody zebras, not horses.
Drug side effects
Some drugs are notorious for causing joint and/or muscle pain as a side effect. Other kinds of pain are possible too, especially headaches, but they are usually more obviously side effects — like the odd example of nitroglycerin, a vasodilator that is sometimes used on injuries, but is also well-known for triggering migraines, even in people who don’t normally get them.55
Joint and muscle pain are easily mistaken for the ordinary aches and pains of aging, removing suspicion from the drugs that are actually causing them. Some of the usual suspects are:- statins (for lowering cholesterol)
- bisphosphonates (for osteoporosis and Paget’s disease)
- fluoroquinolones (a class of antibiotics)
- retinoids (for skin conditions, like Accutane for acne)
- Trintellix (an antidepressant)
Some of these may actually be innocent, others almost certainly do cause trouble: it’s surprisingly unclear, like most of medicine. Here’s some more detail about statins and bisphosphonates …

Actonel (risedronate) is one of the more popular bisphosphonate drugs, any of which may cause severe musculoskeletal pain years after first exposure.
The bisphosphonates — On January 7, 2008, the U.S. Food and Drug Administration alerted health care professionals and consumers to the unusual severe side effects of a popular class of drugs for osteoporosis and Paget’s disease, the Bisphosphonate (Wikipedia). They can cause “severe and sometimes incapacitating bone, joint, and/or muscle pain” which “may occur within days, months, or years” after first taking the medication. This medication has almost certainly explained some otherwise inexplicable pain in some of my patients over the years! Alendronate and risedronate (Actonel) are the two most popular bisphosphonates, and they are usually prescribed for osteoporosis or for a bone-deforming condition called Paget’s disease. If you are 40+ and grappling with a mysterious pain problem, check your medicine cabinet for bisphosphonates in particular, but of course any other medication that could cause pain as a side effect.
The statins — The drugs that lower our blood cholesterol, like Lipitor and Crestor, may also cause pain. Statins are important and widely used drugs, and their deleterious effect on muscle is widely considered a diagnosable condition: statin myalgia, or statin-associated muscle symptoms (SAMS).56 A few patients, about 1 in 10,000, get a more obvious, serious case of muscle poisoning, rhabdomyolysis,57 and an even rarer and more serious condition afflicts 1 in 100,000: statin-associated autoimmune myopathy.5859
And yet there is also confusion and controversy about the prevalence of statin myalgia.6061 There’s even clear evidence that it could be some kind of illusion or misunderstanding: in one head-scratcher of a study, taking statins only increased pain when patients knew they were taking statins.62 So that’s weird! The truth is probably “all of the above” and “it’s complicated” — it seems likely that some patients are genuinely intolerant of statins, while others are suffering from fear of statins and/or some other cause of musculoskeletal pain (of which there are many). There might also be some tricky X-factors, like vitamin D deficiency, which seems to be linked to statin myalgia.63
Fortunately, for the genuinely statin intolerant — and you probably do exist — it’s easy to solve by lowering the dose or switching to another statin.
Note that drugs may also be contaminated, and may contain ingredients that people are allergic or otherwise sensitive to.
Opioid-induced hyperalgesia

Ripening seed head of an opium poppy.
This is basically the mother of all side effects, with a generous dose of tragic irony.
Opioids are, of course, the cause of an enormous amount of misery and controversy right now. Most people assume opioids are “powerful medicine,” and of course they are in some ways, but what few people realize is that they are surprisingly ineffective for many kinds of chronic pain, completely ineffective for a fairly high percentage of the population with a certain gene … and they can backfire in anyone. “Opioid induced hyperalgesia” is a nasty fate in which opioids actually cause pain instead of relieving it.64 It’s so counter-intuitive that many people on opioids take a long time to figure out that their “pain medication” is causing pain.
Medication-overuse headache (formerly known as “rebound” headache)
This almost counts as a drug side-effect, but it’s an important enough phenomenon in its own right that it deserves separate description. When you take a lot of analgesics — pain-killers — it’s possible to pre-empt the production of your body’s own pain-fighting molecules. Endorphin production, for instance, will drop. This can have disastrous consequences when you stop taking the drugs, resulting in worse pain than ever. It mainly seems to cause headaches, but it’s disturbingly possible that it can make other kinds of pain worse as well. This is part of the phenomenon of the well-known serious withdrawal symptoms from some drugs; it is a less well-known problem with over-the-counter pain-killers. Although this phenomenon isn’t particularly mysterious or difficult to identify, it does show us something important about how pain works: we aren’t entirely without our own defenses, and those defenses can actually be undermined by artificial help. And there are scenarios where analgesic rebound may be difficult to detect. Given how extremely common analgesic usage is, it’s likely that people with recurrent headaches may be suffering primarily from bouts of rebound pain, occurring in the occasional gaps between erratic but generally intensive self-prescribing of pain killers.
I have a good story about a terrible withdrawal-induced headache: see my headache tutorial. For more about all kinds of pain-killers, see The Science of Pain-Killers: A user’s guide to over-the-counter analgesics like acetaminophen, ibuprofen, and more.
Benzodiazepine withdrawal syndrome
The benzos, Valium and many others, are potent tranquilizers, which sedate us by simulating a flood of an important neurotransmitter that is one of the body’s built-in sedatives. We can quickly develop powerful physical dependence on benzos, and rushed withdrawal is notoriously brutal. Withdrawal symptoms can even develop while we are still taking the drug, going a little bit into withdrawal before the next dose, which basically causes erratic and minor but frequent withdrawal symptoms.
In benzo withdrawal, you are the opposite of tranquilized: you’re anti-tranquilized. Huge chunks of your biology are way too excitable. The list of potential side effects is endless — benzo withdrawal is notorious for the freakish variety of symptoms it causes — but they all revolve around a strong theme of jittery misery, like being over-caffeinated but more extreme. Sensory distortion in general is the rule, and everything hurts more than it should.
In some people, withdrawal symptoms are long-term. It’s unclear what the mechanism for this persistence is, but it’s likely that the ferocity of withdrawal results in a poorly calibrated pain system (sensitization), and a tough neurological tailspin to pull out of. Another way of putting it is that withdrawal is basically so surreal and traumatic that it can permanently disrupt our nervous system’s ability to interpret stimuli, especially threatening stimuli, leading to long-term erratic false alarms.
Chronic pain as a destiny: many causes for many years!
Nothing’s ever simple and chronic pain least of all: it’s usually caused by a sinister stew of factors that eat away at people for a long time. Chronic pain may be “destiny” with roots going back many years, even decades.65 Trying to solve it by fixing one thing — like vitamin D, say — may be about as feasible as trying to fix a broken engine with just one tool. It can be an impossible puzzle to even understand, let alone treat. Elisa Arnaudo:
Medically unexplained symptoms (MUS) represent a major challenge for healthcare systems in industrialised countries. These symptoms are so prevalent that they are assessed in up to 50% of consultations in primary care.
Probably almost all MUS involve chronic pain, and Arnaudo’s post seems to be mostly about fibromyalgia. She proposes MUS patients are a stumper because of “an inadequate explanatory framework of disease.” In other words, we’re not just missing some pieces from a puzzle; it’s that we probably don’t even know what kind of puzzle we’re looking at.
And … not necessarily such a puzzle.
Ending with a ray of hope
It’s also possible that many of the explanations we need are really hovering just out of our current reach, and really not so tricky after all — just too subtle to be easy. They get missed not because the problem requires godlike medical insight, but because most doctors just don’t know that much about chronic pain and economics keeps appointments relatively short and so even some pretty straightforward things just get missed.
That possibility is the inspiration for this article. Some of the ways to hurt described above may be the main factors, or even the only factors, for some people.
Did you find this article useful? Interesting? Maybe notice how there’s not much content like this on the Internet? That’s because it’s crazy hard to make it pay. Please support (very) independent science journalism with a donation. See the donation page for more information & options.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Appendix: Two stories of diagnosing mysterious pain
Some extraordinarily desperate people came to see me when I was working as a massage therapist. Two memorable examples:
- A woman spends three days in the hospital with severe abdominal pain, but is cleared of every possible ominous medical cause … and then comes to see me?! A massage therapist!
- A man gets a ride in an ambulance with severe chest and left shoulder and arm pain, but doctors cannot find anything wrong with him … and then he comes to see me.
I got lucky with both of these cases, and I was able to treat both of them quickly and easily. There are many ways to hurt, and success was hardly guaranteed. I saw many patients with strange pains I was never able to diagnose. But both of these cases involved surprisingly clear and treatable trigger points: hypersensitive spots in muscle tissue, causing more pain than anyone thought possible.
In the woman’s case, the trigger point was in her iliopsoas muscle, a muscle deep in the abdomen and extending downward through the pelvic that is the subject of much hype and legitimate skepticism. However, it is possible to massage it in some patients. There’s very little to tell: I guessed that it might be the problem, found the trigger point, gently massaged it for a few minutes … and that was the end of her misery. Just like that!
The man’s case was even more straightforward: he had a trigger point in his pectoralis major muscle. It was easy to find, as the muscle twitched violently when I palpated it, the most robust example of a “jump sign” I ever saw. It was nasty, but in twenty minutes of massage we reduced the “heart attack” pain by 80%. The next day it was gone, and it stayed gone for as long as I knew him — years after that. I tell his story in more detail in my trigger points book.
Appendix: Pain demands an explanation
Ever notice how rare it is for people to just say “I have chronic pain” without also including some kind of theory, some hypothetical diagnosis? This always reminds me of the way almost everyone thinks they are above average. 😏 Many people believe that they understand their pain, and some surely do, but they cannot possibly all be right — not even close. The ideas range widely, from the medically mainstream, to more creative but reasonable hypotheses, to odd pet theories, to muddled clichés, to full-blown crackpottery.
The craving to make sense of pain is potent and primal. Pain does indeed “demand” an explanation, and usually gets one … whether it makes a damned lick of sense or not! People are prone to flailing a little — or a lot — when trying to figure out the nature of their pain. I am not saying that people shouldn't indulge the impulse to try to explain, and several reader comments emphasize how irresistible and understandable that “demand” is.66
I begrudge no one’s need to know, no matter where it leads. We do not have a snowball’s chance in hell of actually resisting the temptation to explain our own pain, even when we have no Earthly idea.
But we should be aware of the danger of bad theorizing! We have all kinds of cravings in life that we need to tame and temper, and it’s always easy to be led into serious errors by them. So we should make every effort to understand and mitigate that risk.
How? Education and some restraint. You’re going to have theories, and you’re going to care about them, but try not to over-commit to them. “Strong opinions, loosely held.”
(And then some more education.)
Finally, I reserve the right to be amused by the wackiest ideas that people cook up. But, obviously, I would never make fun of anyone directly for being hilariously wrong.
Related Reading
- A Painful Biological Glitch that Causes Pointless Inflammation — How an evolutionary wrong turn led to a biological glitch that condemned the animal kingdom — you included — to much louder, longer pain
- Pain & Injury Survival Tips — Dozens of ideas (and links) for evidence-based rehabilitation and self-treatment for common pain problems and injuries
- A Rational Guide to Fibromyalgia — The science (and not the pseudoscience) of the mysterious disease of pain, exhaustion, and mental fog
- Chronic, Subtle, Systemic Inflammation — One possible sneaky cause of puzzling chronic pain
- Chronic Pain and Inequality — The role of racism, sexism, queerphobia, ageism, and poverty in health and chronic pain
- Anxiety & Chronic Pain — A self-help guide for people who worry and hurt
- Sensitization in Chronic Pain — Pain itself can change how pain works, resulting in more pain with less provocation
- Pain is Weird — Pain science reveals a volatile, misleading sensation that comes entirely from an overprotective brain, not our tissues
- Chronic Pain as a Conditioned Response — If pain can be learned, perhaps it can be unlearned
- Vulnerability to Chronic Pain — Chronic pain often has more to do with general biological vulnerabilities than specific tissue problems
- The 3 Basic Types of Pain — Nociceptive, neuropathic, and “other” (and then some more)
- Pain Relief from Personal Growth — Treating tough pain problems with the pursuit of emotional intelligence, life balance, and peacefulness
What’s new in this article?
37 updates have been logged for this article since publication (2007). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
Jun 26, 2025 — Clarified information about channelopathies and added information about small fibre neuropathy.
2024 — Complete re-write of the toxins and poisons section.
2024 — Added another good example of early onset Parkinson’s that looked like typical sports injuries.
2023 — Added small new section about foreign objects, inspired by a good new example (a bullet embedded in someone's hand for decades before it started to hurt).
2023 — Two new main sections about pollutants and food additives, radiculopathy (especially multiple-level radiculopathy), plus a new appendix about how “Pain demands an explanation.” Miscellaneous revision and editing.
2023 — Cited a case study about mistaking Parkinsonian dystonia for a knee injury.
2022 — Added a new section about cancer in general as a cause of some kinds of seemingly simple musculoskeletal pain.
2022 — Science update. Added rheumatic symptoms from Long COVID to post-viral syndrome section.
2022 — Added a section about adenosine monophosphate deaminase 1 (AMPD1) deficiency.
2022 — Minor science update: added an interesting citation about the infectious roots of multiple sclerosis (Bjornevik).
2021 — Minor science update: added a couple citations about magnesium.
2021 — Added a section about pain as a learned behaviour (classical conditioning).
2021 — Added a small but good citation to a case study of circulatory impairment in a cyclist causing leg pain (Brindisino).
2021 — Rewrote the section on neuroinflammation. It had been hastily excerpted and abridged from another article. Now it’s a proper standalone summary and much clearer.
2020 — Added short commentary on the ethics of sharing “high-grade hypochondriac nightmare fuel.”
2020 — Added a section about smoking, expanded the discussion of poor health, and added an interesting blurb about the pre-pandemic meaning of “social distancing.”
2019 — Added new section: “All in your head: pure psychosomatic pain.”
2019 — Added minor-but-nice perspective about the “official” major categories of causes of pain. Pie chart included.
2019 — Added new section about chronic immune activation after infection.
2019 — Two new sections about mitochondrial disease and neuroinflammation, plus a bunch of editing to integrate those topics with some of the others. Also changed the introduction to emphasize that chronic pain is seriously multifactorial, some critical context previously neglected.
2019 — Added a section about a newly identified common genetic defect linked to exaggerated awareness all kinds of sensation. Really fascinating.
2019 — Added section about benzodiazepene (tranquilizer) withdrawal.
2019 — Added section about social isolation and loneliness, the first of a series that I will be adding about non-specific vulnerabilities to illness and chronic pain.
2019 — Added a listed other possibilities that I’m considering for future updates. I think the list itself has value, even without elaboration.
2019 — New section: “Spatial summation and why some body areas suffer more, like the neck and back.”
2018 — New section: “Non-obvious nerve entrapment.”
2018 — New section: “Claudication: the pain of impaired blood flow.”
2018 — New section: “Syphilis.”
2018 — New section: “Pain with literally no specific cause.”
2018 — Major reboot and expansion. This is now a much more comprehensive review of possible causes of pain. There’s more to do and suggestions and requests for additions are very welcome. I hope this will become one of the most useful articles on PainScience.com.
2018 — More information about other drugs with painful side effects.
2017 — Science udpate — Cited evidence that statin myalgia could be bogus, not actually a real problem.
2017 — Added a table of contents. A few minor edits.
2016 — New conclusion, with both discouraging and encouraging perspectives, taken from a recent blog post about the challenge of medically unexplained symptoms.
2016 — Added Vitamin D deficiency and chronic low-grade inflammation.
2016 — Minor addition: a sidebar about “the wilderness of the medically unexplained.”
2016 — Added sidebar about the basic types of pain, nociceptive and neurpathic. Added #10, about exaggerated inflammation.
2007 — Publication.
Notes
- Painaustralia. The cost of pain in Australia. Deloitte Access Economics. 2019 Mar. PainSci Bibliography 52620 ❐
“Nocebo” is roughly the opposite of placebo: instead of relief from belief, it’s grief from belief. The word is Latin for “I shall harm” (great supervillain slogan). It refers to the harmful effect of … nothing but the belief in or fear of a harmful effect. Give someone a sugar pill and then convince them you actually just fed them a deadly poison, and you will probably witness a robust nocebo effect. Nocebo is one of the chief hazards of excessive X-raying and MRI scanning: showing people hard evidence of problems that often aren’t actually a problem is a great way to make them suffer.
- Akin-Akinyosoye K, Sarmanova A, Fernandes GS, et al. Baseline self-report 'central mechanisms' trait predicts persistent knee pain in the Knee Pain in the Community (KPIC) cohort. Osteoarthritis Cartilage. 2020 Feb;28(2):173–181. PubMed 31830591 ❐
Easily identified signs of “central mechanisms” of pain in more than 1400 patients were linked to having worse knee pain a year later. Also, other risk factors had more impact in people with strong signs of sensitization.
- Melzack R. Pain and the neuromatrix in the brain. J Dent Educ. 2001 Dec;65(12):1378–82. PubMed 11780656 ❐
ABSTRACT
The neuromatrix theory of pain proposes that pain is a multidimensional experience produced by characteristic "neurosignature" patterns of nerve impulses generated by a widely distributed neural network-the "body-self neuromatrix"-in the brain. These neurosignature patterns may be triggered by sensory inputs, but they may also be generated independently of them. Acute pains evoked by brief noxious inputs have been meticulously investigated by neuroscientists, and their sensory transmission mechanisms are generally well understood. In contrast, chronic pain syndromes, which are often characterized by severe pain associated with little or no discernible injury or pathology, remain a mystery. Furthermore, chronic psychological or physical stress is often associated with chronic pain, but the relationship is poorly understood. The neuromatrix theory of pain provides a new conceptual framework to examine these problems. It proposes that the output patterns of the body-self neuromatrix activate perceptual, homeostatic, and behavioral programs after injury, pathology, or chronic stress. Pain, then, is produced by the output of a widely distributed neural network in the brain rather than directly by sensory input evoked by injury, inflammation, or other pathology. The neuromatrix, which is genetically determined and modified by sensory experience, is the primary mechanism that generates the neural pattern that produces pain. Its output pattern is determined by multiple influences, of which the somatic sensory input is only a part, that converge on the neuromatrix.
Weren’t ulcers proved to be caused by a bacterium? That they were. Helicobacter pylori was famously hunted down in 1983 by Australian scientists Barry Marshall and Robin Warren. Although its link with ulceration was initially met with much skepticism, science came around relatively quickly — convinced by evidence, just like it’s supposed to work. By the mid-90s it was widely accepted that H. pylori infection causes ulcers, and Marshall and Warren got a Nobel prize in 2005 (acceptance speech).
But! Most people infected with the bacterium have no symptoms, and there are many variables that determine the severity of the infection and whether or not it leads to ulcer. Stress is one of those factors (see Guo et al. and Jia et al.). Thus ulcer is very likely both an H. pylori infection and a “stress-sensitive” condition.
- Espay AJ, Aybek S, Carson A, et al. Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders. JAMA Neurol. 2018 09;75(9):1132–1141. PubMed 29868890 ❐
- O’Sullivan S. It's All in Your Head: True Stories of Imaginary Illness. Chatto & Windus; 2015.
This book consists mainly of well-told stories of severe psychosomatic illness and functional neurological disorders (neurological symptoms without diagnosable disease). The key take-away is that psychologically powered illness is common and can be amazingly severe. Although Dr. O’Sullivan is clearly concerned about the risk of incorrect diagnosis, and she is cautious and compassionate enough that I think she mostly gets it right (with the notable exception of the chronic fatigue chapter). It’s well-written and fascinating and has plenty to offer. I do wish there were citations.
- The catastrophic spasticity of a rabies infection might be the most dramatic example of the power of cramping in all of medicine. The infamous “fear of water” is caused by agonizing cramping of throat muscles in response not only to actual swallowing, but even the suggestion of it. Yikes. Read more: The awful power of cramps demonstrated by rabies.
- Ferreira D, Araújo R. A professional sportsperson with subtle motor symptoms and signs: early-onset Parkinson's disease. Lancet. 2023 Feb;401(10377):e18. PubMed 36841616 ❐ PainSci Bibliography 51317 ❐
Dr. James Noake describes a case that looked like “typical” musculoskeletal symptoms — sciatica initially — but was actually early onset Parkinson’s:
This lady had some improvement in pain post deep gluteal space sciatic nerve decompression. But at review, her lower limb control deteriorated, poor coordination, gait pattern continuing to change. … It seems the relatively subtle changes in neuromuscular control due to the central neuro condition led to her ‘typical’ MSK symptoms: lumbopelvic, hip, leg pain, then subacromial pain. Neurologist acknowledged he’d seen this evolution of symptoms before in young sporty patients.
Dr. Noake on “lessons learned”:
Stay open-minded about wider medical diagnoses. Review & safety net if things don’t quite add up. Ask questions, don’t accept at face value.
- Csapo R, Maganaris CN, Seynnes OR, Narici MV. On muscle, tendon and high heels. J Exp Biol. 2010 Aug;213(Pt 15):2582–8. PubMed 20639419 ❐ PainSci Bibliography 55265 ❐
Chronic heel wearers, for instance, do have shortened calf muscles, stiffer Achilles tendons, and a smaller ankle range of motion. It doesn’t actually seem to cause much of a problem, but the tissue does shorten.
- This depends on many other factors. For instance, if you can clearly see that you’ve been struck by two paintballs, 15cm apart, your brain is probably not going to experience one mighty paintball sting — brains are not idiots, and they can use lots of data sources to generate higher fidelity perception.
- Holbert MD, Pedler A, Camfermann D, Harvie DS. Comparison of spatial summation properties at different body sites. Scand J Pain. 2017 Oct;17:126–131. PubMed 28850365 ❐ These researchers compared summation in the neck and back to the extremities, and found that it works about the same way: in any region, painful sites separated by as much as 15-20cm will be “summed” by the brain, making the entire area feel painful.
- Khoury S, Piltonen MH, Ton AT, et al. A functional substitution in the L-aromatic amino acid decarboxylase enzyme worsens somatic symptoms via a serotonergic pathway. Ann Neurol. 2019 Jun. PubMed 31177555 ❐
- Johnston KJA, Adams MJ, Nicholl BI, et al. Genome-wide association study of multisite chronic pain in UK Biobank. PLoS Genet. 2019 Jun;15(6):e1008164. PubMed 31194737 ❐ PainSci Bibliography 52248 ❐
This is the biggest study of the genetics of chronic pain patients to date, which found 76 genes that are independent risk factors for multisite chronic pain in 380,000 British citizens. Many of those genes are used in the brain and associated with neuroplasticity, and many were also linked to cell division (very fundamental biological processes). This is consistent with the idea that pain has such deep roots in our biology that it is hard to separate from life, which is why it’s so hard to suppress while also preserving consciousness.
Almost half of these genes are also risk factors for severe depression, and with some fancy statistical work they showed that pain actually causes the depression but, interestingly, not the other way around — which is probably not evidence that pain is psychologically depressing (although it is), but rather that something about the genetics of chronic pain also leads to depression.
They also found a bunch of genetic overlap with genes linked to several other diseases: schizophrenia, body-mass index, rheumatoid arthritis and post-traumatic stress disorder, among others.
- Zorina-Lichtenwalter K, Meloto CB, Khoury S, Diatchenko L. Genetic predictors of human chronic pain conditions. Neuroscience. 2016 Dec;338:36–62. PubMed 27143481 ❐ PainSci Bibliography 52509 ❐
Zorina et al. reviewed genetic factors implicated in chronic pain conditions, reporting that there are “several strong-effect mutations” — mutations that directly cause painful pathologies, the more obvious genetic factors in pain. But they also reported “minor contributions from a large number” of minor genetic typos (single nucleotide polymorphisms).
For instance, in migraine and musculoskeletal pain patients, “nearly half” of what makes them genetically distinct from healthy people is … fishy. The difference “alters neurotransmission pathways.” That is, those people are biologically different in ways that affect how nerves do their thing — and that’s probably not a coincidence.
Nearly half! That’s a lot of subtle genetic contribution to how bodies feel.
When I first read Zorina et al., I was tempted to write something a bit snarky about the futility of obsessing over trivial modifiable risk factors — things like posture, core weakness, vitamin D deficiency, and many more half-assed ideas about what drives pain (ranging in credibility from “maybe a bit of a thing, but overhyped” to “just silly bullshit”). But then I remembered how my own chronic pain has driven me to fight like hell to control whatever risk factors I possibly can. If there’s any reasonable hope that a chronic pain patient can do something to avoid making a bad situation worse — even if it’s a long shot — it’s not just an understandable choice, it’s a rational one. Many of those efforts are doomed to be inefficient or even wasted. But so what? There are worse things than inefficiency.
And so I controlled my impulse to snark. We certainly should be aware that there are many truly uncontrollable factors in pain, but that doesn’t mean we shouldn’t also be keen on doing whatever we can do to avoid making a bad situation even worse.
- McDonald B, Pittman K, Menezes GB, et al. Intravascular danger signals guide neutrophils to sites of sterile inflammation. Science. 2010 Oct;330mcd(6002):362–6. PubMed 20947763 ❐
- Lyon P, Cohen M, Quintner J. An evolutionary stress-response hypothesis for chronic widespread pain (fibromyalgia syndrome). Pain Med. 2011 Aug;12(8):1167–78. PubMed 21692974 ❐ This paper explores a striking similarity between fibromyalgia and “sickness behaviour” in animals.
- Albrecht DS, Forsberg A, Sandström A, et al. Brain glial activation in fibromyalgia - A multi-site positron emission tomography investigation. Brain Behav Immun. 2019 Jan;75:72–83. PubMed 30223011 ❐ PainSci Bibliography 52325 ❐ This study provides the first in vivo evidence of neuroinflammation in fibromyalgia patients.
- Ji RR, Nackley A, Huh Y, Terrando N, Maixner W. Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology. 2018 08;129(2):343–366. PubMed 29462012 ❐ PainSci Bibliography 52332 ❐
- Kim JB. Channelopathies. Korean J Pediatr. 2014 Jan;57(1):1–18. PubMed 24578711 ❐ PainSci Bibliography 53026 ❐ “Channelopathies that primarily affect neurons include certain types of epilepsy, ataxia, migraine, hyperekplexia, blindness, deafness, and peripheral pain syndromes.”
- It might be accompanied by subtle signs of neuropathy, such as a slight buzzing quality to the pain, but not enough to raise clinical suspicion of a nerve pinch. There’s clearly a range, but at least some significant percentage of cases are not obviously nerve-y.
- Aota Y. Entrapment of middle cluneal nerves as an unknown cause of low back pain. World J Orthop. 2016 Mar;7(3):167–70. PubMed 27004164 ❐ PainSci Bibliography 53097 ❐
- Sapolsky RM. Why Zebras Don’t Get Ulcers. 3rd ed. New York: Times Books; 2004. p. 164.
…the fewer social relationships a person has, the shorter his or her life expectancy, and the worse the impact of various infectious diseases. Relationships that are medically protective can take the form of marriage, contact with friends and extended family, church membership, or other group affiliations. This is a fairly consistent pattern that cuts across a lot of different settings. Moreover, these general findings are based on some careful prospective studies and are seen in both sexes and in different races, in American and European populations living in both urban and rural areas. Most important, this effect is big. The impact of social relationships on life expectancy appears to be at least as large as that of variables such as cigarette smoking, hypertension, obesity, and level of physical activity.
- Smith TO, Dainty JR, Williamson E, Martin KR. Association between musculoskeletal pain with social isolation and loneliness: analysis of the English Longitudinal Study of Ageing. Br J Pain. 2019 May;13(2):82–90. PubMed 31019689 ❐ PainSci Bibliography 52275 ❐
This study looked for a link between chronic musculoskeletal pain, and loneliness and social isolation in several thousand older adults. They found that subjects in pain were actually less likely to be socially isolated, but more likely to be lonely, an interesting apparent contradiction. However, loneliness is probably what matters: that is, social isolation isn’t a problem if you don’t feel socially isolated (lonely).
- Sapolsky, Why Zebras Don’t Get Ulcers, op. cit.
Take a rodent or a primate that has been housed alone and put it into a social group. The typical result is a massive stress-response. In the case of monkeys, this can go on for weeks or months while they tensely go about figuring out who dominates whom in the group’s social hierarchy.
Why Zebras Don’t Get Ulcers, by Robert M Sapolsky, 406
- “I was hoping it might be shiny still,” he said in an interview with CBC Radio One’s “As It Happens,” but it was badly corroded — perhaps the reason it finally caused some symptoms, but who knows.
- Athanaselis ED, Fyllos A, Stefanou N, Varitimidis SE, Giannikas D. A Tumor-Like Lump in the Palm Caused by an Inconspicuous-for 75 Years-Bullet. Case Rep Orthop. 2020;2020:8898016. PubMed 32695542 ❐ PainSci Bibliography 51622 ❐
ABSTRACT
CASE: An unusual case of a foreign body in the hand is described here. Excision of a tumor-like soft tissue mass revealed a 75-year-old World War II bullet fragment of which patient was unaware.
CONCLUSION: Differential diagnosis of hand lumps and inflammatory reaction must always include retained foreign bodies even after a very long period of posttraumatic quiescence or patient's inability to provide a relative injury case history.
- Smuck M, Schneider BJ, Ehsanian R, Martin E, Kao MCJ. Smoking Is Associated with Pain in All Body Regions, with Greatest Influence on Spinal Pain. Pain Med. 2020 Sep;21(9):1759–1768. PubMed 31578562 ❐
- Holman AJ. Fibromyalgia and Positional Cervical Cord Compression Differ Only By Autonomic Nervous System Consequences: A Double-Blinded, Prospective Study. Arthritis Rheumatol. 2015;67(suppl 10).
This paper presents evidence of “minor” irritation of the upper spinal cord may cause “potent sympathetic arousal in humans” — firing up the same branch of our nervous system that handles emergencies. Thirty-one of fifty-four patients with fibromyalgia and positional cervical cord compression showed clear signs of sympathatic arousal.
- See Sezer, Hagen, Hou, Stein.
- Konstantinou K, Lewis M, Dunn KM. Agreement of self-reported items and clinically assessed nerve root involvement (or sciatica) in a primary care setting. Eur Spine J. 2012 Nov;21(11):2306–15. PubMed 22752591 ❐ PainSci Bibliography 52894 ❐
Patient descriptions like “pain below the knee,” “radiating pain in the legs,” “pain running down the leg,” have always been considered indicators of sciatica (radiculopathy caused by nerve root compression). Do any of these common phrases actually identify sciatica? Unfortunately not: in this study of more than 500 back pain patients with pain radiating to the legs, no single self-report, or cluster of them, was clearly associated with cases of sciata identified by careful history and exam. “Pain below the knee” was the closest match, but it was still misleading: not every patient with sciatica has that symptom, and some with that symptom do not have sciatica. Similarly, a cluster of descriptions including “distribution of pain below the knee,” “leg pain that is worse than back pain,” and “feeling of numbness or pins and needles in the leg” also correctly identified many cases, but still misclassified too many.
Certain self-report indicators particularly pain radiating below, leg pain worse than back pain, and numbness, pins and needles in the leg can be useful at a very crude level. However, when accuracy in case definition is of importance, clinical examination is the recommended method.
- Brindisino F, Signorelli M, Rizzo S, Heick JD, Maselli F. Lower-Limb Pain Differentiation by a Physical Therapist in an Amateur Cyclist: A Case Report. JOSPT Cases. 2021;1(2):114–123. PainSci Bibliography 52144 ❐
Cyclists get plenty of overuse injuries and are usually referred to physical therapists for any persistent pain that doesn’t have an obvious medical cause. In this case, a 57-year-old recreational amateur cyclist had been suffering thigh and leg pain for two months. The patient failed a couple basic tests for endurance of the leg muscles — painful and weak — and had a reduced blood pressure in the lower limb. A blockage in a leg artery was identified and repaired by a surgeon, and the patient fully recovered within three months.
“Clinicians should consider vascular conditions, even in endurance sports.”
- Taylor AJ, Kerry R. When Chronic Pain Is Not “Chronic Pain”: Lessons From 3 Decades of Pain. J Orthop Sports Phys Ther. 2017 Aug;47(8):515–517. PubMed 28760092 ❐
- There are good criticisms of this paper from a couple of my favourite experts and writers, pointing out in a letter to the journal that one of the “fashionable” paradigms impugned here, the biopsyschosocial model, “includes the considerations [the “bio” part] that eventually cured the patient’s pain.” I like the criticism and I like the authors’ response — I see only healthy debate here.
- Scheper MC, de Vries JE, Verbunt J, Engelbert RH. Chronic pain in hypermobility syndrome and Ehlers-Danlos syndrome (hypermobility type): it is a challenge. J Pain Res. 2015;8:591–601. PubMed 26316810 ❐ PainSci Bibliography 52758 ❐ Hypermobility is “highly prevalent among patients diagnosed with chronic pain.”
- “The essential difference between HSD and hEDS lies in the stricter criteria for hEDS compared to the HSD.” But it’s very tricky, and those criteria are all very new (see the 2017 EDS International Classification).
- Rodgers KR, Gui J, Dinulos MBP, Chou RC. Ehlers-Danlos syndrome hypermobility type is associated with rheumatic diseases. Sci Rep. 2017 Jan;7:39636. PubMed 28051109 ❐ PainSci Bibliography 52757 ❐
hEDS patients may see multiple subspecialists without realizing a connection between their joint symptoms and multi-systemic involvement of the disease; they are often dismissed as hypochrondriacs, and report feelings of isolation from the lack of diagnosis.
Perhaps due to a lack of gravitas surrounding the hEDS diagnosis, management of the disease varies among practitioners, and clinical workup does not often extend beyond the joint and skin examination.
- Manson JE, Patsy M B, Rosen CJ, Taylor CL. Vitamin D Deficiency — Is There Really a Pandemic? N Engl J Med. 2016 Nov 10;375(19):1817–1820. PubMed 27959647 ❐
ABSTRACT
The claim that large proportions of North American and other populations are deficient in vitamin D is based on misinterpretation and misapplication of the Institute of Medicine reference values for nutrients — misunderstandings that can adversely affect patient care.
- Holick MF, Chen TC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr. 2008 Apr;87(4):1080S–6S. PubMed 18400738 ❐ PainSci Bibliography 55028 ❐
- Bone aching is caused by osteomalacia, which is bone weakening specifically caused by malfunctioning bone building biology. The Mayo Clinic describes osteomalacia symptoms like so: “The dull, aching pain associated with osteomalacia most commonly affects the lower back, pelvis, hips, legs and ribs. The pain may be worse at night, or when you’re putting weight on affected bones.”
- Mauskop A, Varughese J. Why all migraine patients should be treated with magnesium. J Neural Transm (Vienna). 2012 May;119(5):575–9. PubMed 22426836 ❐ Treating migraines with magnesium is hardly a sure thing, and some object to it, but conservative magnesium supplementation is about as low-risk an intervention as they get — far better than any migraine drug.
- Banerjee S, Jones S. Magnesium as an Alternative or Adjunct to Opioids for Migraine and Chronic Pain: A Review of the Clinical Effectiveness and Guidelines. CADTH Rapid Response Reports. 2017 Apr. PubMed 29334449 ❐
This paper concluded in 2016 that “magnesium appears to have an analgesic effect.” Great! But don’t read the fine print if you want to hang on to that good feeling. Their own summary of findings doesn’t seem to back up the optimism. They clearly state that conclusions were “not possible” for migraine … that the evidence is conflicting for a rather exotic kind of chronic pain (complex regional pain syndrome) … and they mention only a single trial showing a benefit for back pain (with intravenous supplementation, no less, and for back pain complicated by neuropathy; see Yousef).
And that’s just all they wrote about the data. If there is enough evidence to justify “magnesium appears to have an analgesic effect,” it is not reported in this paper.
- Garrison SR, Korownyk CS, Kolber MR, et al. Magnesium for skeletal muscle cramps. Cochrane Database Syst Rev. 2020 09;9:CD009402. PubMed 32956536 ❐ PainSci Bibliography 52162 ❐
This review of only a handful of existing studies concluded that “it is unlikely that magnesium supplementation provides clinically meaningful cramp prophylaxis to older adults experiencing skeletal muscle cramps.” Amazingly, the evidence for the effect of Mg on cramps caused by exertion, disease, and pregnancy is just hopelessly inadequate. You’d think someone would at least have studied exercise-induced cramping, given its importance in elite athletics. The last version of this review was in 2012, and almost nothing changed.
- Glancy B, Hartnell LM, Malide D, et al. Mitochondrial reticulum for cellular energy distribution in muscle. Nature. 2015 Jul;523(7562):617–20. PubMed 26223627 ❐
For decades, mitochondria have been described as the “power plants” of cells, and they are already fascinating and complex. (I’m particularly amazed by their role in unnecessary inflammation.) But we may need to update the simile: turns out mitochondria don’t just produce energy “like a power plant,” they also deliver it like a network of power lines. This phenomenon was identified in mouse muscles:
Researchers found that mitochondria in mouse muscles not only produce energy, but can quickly distribute it across the muscle cell through a grid-like network. The findings reveal a major mechanism for energy distribution in skeletal muscle cells, and could provide new insights into diseases linked to energy use in muscle.
What a wonderful example of how much we still have to learn about muscle tissue (and others too, I’m sure, but muscle seems to be particularly full of surprising puzzles). It seems likely that we probably can’t understand muscle pain properly if we have only just now discovered something so fundamental about muscle biology. Imagine trying to troubleshoot an electrical problem if you weren’t aware of a major feature of how power is generated and transmitted!
- Meeus M, Nijs J, Hermans L, Goubert D, Calders P. The role of mitochondrial dysfunctions due to oxidative and nitrosative stress in the chronic pain or chronic fatigue syndromes and fibromyalgia patients: peripheral and central mechanisms as therapeutic targets? Expert Opin Ther Targets. 2013 Sep;17(9):1081–9. PubMed 23834645 ❐ “Mitochondrial dysfunction has been shown in leukocytes of CFS patients and in muscle cells of FM patients, which could explain the muscle pain. Additionally, if mitochondrial dysfunction is also present in central neural cells, this could result in lowered ATP pools in neural cells, leading to generalized hypersensitivity and chronic widespread pain.”
- Filosto M, Tonin P, Vattemi G, et al. The role of muscle biopsy in investigating isolated muscle pain. Neurology. 2007 Jan;68(3):181–6. PubMed 17224570 ❐
- Jutras BL, Lochhead RB, Kloos ZA, et al. Borrelia burgdorferi peptidoglycan is a persistent antigen in patients with Lyme arthritis. Proc Natl Acad Sci U S A. 2019 Jul;116(27):13498–13507. PubMed 31209025 ❐ PainSci Bibliography 52327 ❐
- Bjornevik K, Cortese M, Healy BC, et al. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science. 2022 01;375(6578):296–301. PubMed 35025605 ❐ PainSci Bibliography 52020 ❐
This study strongly linked the endemic Epstein-Barr to multiple sclerosis by studying millions of subjects over twenty years. Unlike countless other “links” in medical science, there is so much correlation smoke here that there is almost certainly a causality fire. The risk of developing multiple sclerosis thirty-two times greater after EBV infection. And so EBV probably causes multiple sclerosis (in combination with other factors) — an extremely important discovery.
- Cui D, Wang Y, Huang L, et al. Rheumatic Symptoms Following Coronavirus Disease 2019 (COVID-19): A Chronic Post-COVID-19 Condition. Open Forum Infect Dis. 2022 Jun;9(6):ofac170. PubMed 35611349 ❐ PainSci Bibliography 52058 ❐
These are mainly just mild to moderate symptoms, fortunately. But that’s still a lot of premature arthritis for several million people.
The knees, hands, and shoulders were the most affected, and more in women and older patients. All of this happened independently of illness severity or steroid therapy.
This the first good data we’ve gotten on this topic (thirty months into the pandemic).
- Suh J, Mukerji SS, Collens SI, et al. Skeletal Muscle and Peripheral Nerve Histopathology in COVID-19. Neurology. 2021 08;97(8):e849–e858. PubMed 34099523 ❐
- Aschman T, Schneider J, Greuel S, et al. Association Between SARS-CoV-2 Infection and Immune-Mediated Myopathy in Patients Who Have Died. JAMA Neurol. 2021 08;78(8):948–960. PubMed 34115106 ❐
- We know that FSHD causes excessive delayed-onset muscle soreness, often for many years before diagnosis, and without any other symptoms. This is a well-described genetic pathology. There is nothing squishy or uncertain about the diagnosis. And yet the mechanism by which FSHD causes soreness in the absence of any other symptoms is simply unknown. No one knows how FSHD does that. If a disease like FSHD can do it without anyone knowing how, there are surely other pathological ways to be sore without a diagnosis.
- Yes, weirdly, nitroglycerin — the explosive and the pills for angina — is also occasionally used as an medicinal ointment or patch for tendinitis. It is allegedly a pain-killer but definitely a headache-causer. There are two pretty decent trials of this (which doesn’t sound like much, but it’s better than we get for most obscure treatments). Paoloni et al. reported a respectable benefit for tendinitis way back in 2004, but also quite a few headaches. In 2024, Kirwan et al. found no benefit at lower dosages … but still saw headaches! I review nitro as a tendinitis treatment in detail in my guide to Achilles tendinitis.
- Di Stasi SL, Macleod TD, Winters JD, Binder-Macleod SA. Effects of Statins on Skeletal Muscle: A Perspective for Physical Therapists. Phys Ther. 2010 Aug. PubMed 20688875 ❐
- “Rhabdo” is a nasty but also very interesting condition. I discuss it in detail in Poisoned by Massage.
- Mammen AL. Statin-Associated Autoimmune Myopathy. N Engl J Med. 2016 Feb;374(7):664–9. PubMed 26886523 ❐
- Regarding classification, professionals should take a look at a great 2004 interview with Eliot A. Brinton, MD: “There are 4 interrelated terms for muscle problems that can occur with statins. Unfortunately, they are often confused even by healthcare professionals … .” (Technical note: this document is freely available, but direct linking will hit a paywall. Medscape only reveals the whole thing to people arriving from a Google search. Simply search for do a Google search for it to get around the paywall.)
- Ganga HV, Slim HB, Thompson PD. A systematic review of statin-induced muscle problems in clinical trials. Am Heart J. 2014 Jul;168(1):6–15. PubMed 24952854 ❐
In this review of several statin trials, only slightly more patients had pain on statins than without (placebo): just 12.7%, compared to 12.4%. You could conclude from this data that there actually is no such thing as statin mylagia! But it probably is a real phenomenon, which is highly plausible based on the existence of rarer but very severe side effects on muscle (see Mammen or Statin Therapy). We don’t have very good data about it, it’s mostly not severe, and it’s hard to distinguish from the “background noise” of many other common causes of musculoskeletal pain.
- Cholesterol Treatment Trialists' Collaboration. Effect of statin therapy on muscle symptoms: an individual participant data meta-analysis of large-scale, randomised, double-blind trials. Lancet. 2022 Aug. PubMed 36049498 ❐
- Gupta A, Thompson D, Whitehouse A, et al. Adverse events associated with unblinded, but not with blinded, statin therapy in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid-Lowering Arm (ASCOT-LLA): a randomised double-blind placebo-controlled trial and its non-randomised non-blind extension phase. Lancet. 2017 Jun;389(10088):2473–2481. PubMed 28476288 ❐
This study was designed to test the existence of the phenomenon of statin myalgia. Taking statins did not increase pain in patients when they were unaware that they were taking them. This suggests that statin myalgia is something people get because they are afraid of it, not because it’s a real side effect. As the authors concluded:
These analyses illustrate the so-called nocebo effect, with an excess rate of muscle-related AE reports only when patients and their doctors were aware that statin therapy was being used and not when its use was blinded. These results will help assure both physicians and patients that most AEs associated with statins are not causally related to use of the drug and should help counter the adverse effect on public health of exaggerated claims about statin-related side-effects.
- Michalska-Kasiczak M, Sahebkar A, Mikhailidis DP, et al. Analysis of vitamin D levels in patients with and without statin-associated myalgia - a systematic review and meta-analysis of 7 studies with 2420 patients. Int J Cardiol. 2015 Jan;178:111–6. PubMed 25464233 ❐
- Lee M, Silverman SM, Hansen H, Patel VB, Manchikanti L. A comprehensive review of opioid-induced hyperalgesia. Pain Physician. 2011;14(2):145–61. PubMed 21412369 ❐
Opioid-induced hyperalgesia (OIH) is defied as a state of nociceptive sensitization caused by exposure to opioids. The condition is characterized by a paradoxical response whereby a patient receiving opioids for the treatment of pain could actually become more sensitive to certain painful stimuli.
Clinicians should suspect OIH when opioid treatment’s effect seems to wane in the absence of disease progression, particularly if found in the context of unexplained pain reports or diffuse allodynia unassociated with the original pain, and increased levels of pain with increasing dosages.”
- Burke NN, Finn DP, McGuire BE, Roche M. Psychological stress in early life as a predisposing factor for the development of chronic pain: Clinical and preclinical evidence and neurobiological mechanisms. J Neurosci Res. 2016 Jul. PubMed 27402412 ❐ “Early-life adversity increases the risk of developing a number of disorders, such as chronic pain, fibromyalgia, and irritable bowel syndrome.”
- “For me, it was almost pathological … I needed to make sense of the nonsensical.”
- “Couldn’t this desire to explain the reason for our pain come from a simpler, mammalian, instinctive place? Pain is scary. Why are we scared? Because unexplained pain could, we worry, mean impending death. So if we can give our pain an origin that’s not deadly, than we can worry a little less.”
- “I think that people need explanations. Explanations make simple and safe what’s sprawly and scary. What kind of nutcase would just ‘sit with’ raw experience without attempting to soothe via rationalization? Even if the explanation arrived at isn’t rational?”
- “Pain requiring an explanation makes sense from a evolutionary biology standpoint. The adaptive value is to change behavior, ergo, the mind must create a hypothesis. If someone has chronic pain and has NOT tried to explain it to themselves in some way wouldn’t that be the more maladaptive behavior?”