A rare good quality trial of magnesium supplementation for pain
Four pages on PainSci cite Yousef 2013: 1. The Complete Guide to Trigger Points & Myofascial Pain 2. Does Epsom Salt Work? 3. Vitamins, Minerals & Supplements for Pain & Healing 4. Magnesium supplementation as a pain killer

Magnesium crystal. Some processing required before ingestion.
PainSci commentary on Yousef 2013: ?This page is one of thousands in the PainScience.com bibliography. It is not a general article: it is focused on a single scientific paper, and it may provide only just enough context for the summary to make sense. Links to other papers and more general information are provided wherever possible.
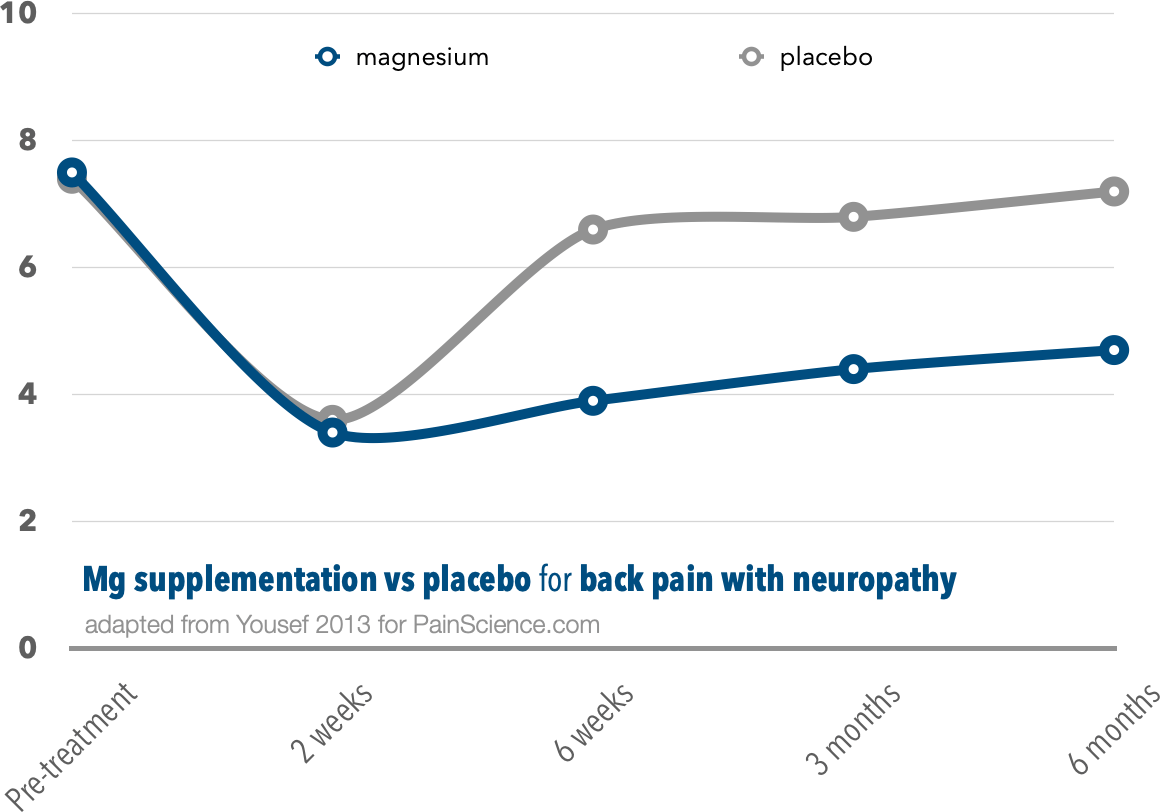
This is one of the only good quality trials of magnesium supplementation for body pain. However, crucially, they studied only back pain with a neuropathic component. 40 patients were given a placebo, and their progress over 6 months was compared to 40 more who got intravenous magnesium for two weeks, then oral for another month.
The patients who got magnesium clearly did better in the long run.
Both groups did great at first, more than halving their pain. If stopped there, the study would have shown that magnesium was no better than a placebo. But then the placebo group's numbers rebounded, while the magnesium folks stayed low… for six months. The improvement wasn’t huge, but it wasn’t small either. I wouldn’t turn it down.
This is a clearly positive result on its face — which is such a rarity in this field that it’s cause for too-good-to-be-true concern. It is “just one study,” with unknown flaws, and unreplicated.
This experiment just cannot tell us anything about the effect of magnesium on the most common kinds of pain, which are mostly not neuropathic. Back pain without neuropathy is a good proxy for many other kinds of pain; back pain with neuropathy is more about neuropathy than “back pain.”
But, for whatever it’s worth, it is indeed a properly positive result — and that’s more than we can say for a great many other trials of any intervention for any kind of back pain.
original abstract †Abstracts here may not perfectly match originals, for a variety of technical and practical reasons. Some abstacts are truncated for my purposes here, if they are particularly long-winded and unhelpful. I occasionally add clarifying notes. And I make some minor corrections.
Persistent mechanical irritation of the nerve root sets up a series of events mediating sensitisation of the dorsal roots and dorsal horns in the spinal cord. Current evidence supports the role of magnesium in blocking central sensitisation through its effect on N-methyl-d-aspartate receptors. We studied the role of sequential intravenous and oral magnesium infusion in patients with chronic low back pain with a neuropathic component. We recruited a cohort of 80 patients with chronic low back pain with a Leeds Assessment of Neuropathic Signs and Symptoms pain scale score ≥ 12, who were receiving a physical therapy programme. All patients were treated with anticonvulsants, antidepressants and simple analgesics; in addition 40 patients received placebo for 6 weeks (control group), while the other 40 patients received an intravenous magnesium infusion for 2 weeks followed by oral magnesium capsules for another 4 weeks (magnesium group). Patients were asked to rate their pain using a numerical rating scale. Lumbar spine range of motion was also determined using a long-arm goniometer. In the magnesium group, the patients' numerical rating scales revealed a significant reduction in pain intensity. The mean (SD) pre-treatment value was 7.5 (2.2) compared with 4.7 (1.8) at 6 months (p = 0.034). The reduction in pain intensity was accompanied by significant improvement in lumbar spine range of motion during the follow-up period. The mean (SD) values of flexion, extension and lateral flexion movements before treatment and at 6-month follow up were 22.2 (8.4) vs 34.7 (11.5) (p = 0.018), 11.8 (3.4) vs 16.9 (3.5) (p = 0.039), 11.4 (3.6) vs 17.2 (4.4) (p = 0.035), respectively. Our findings show that a 2-week intravenous magnesium infusion followed by 4 weeks of oral magnesium supplementation can reduce pain intensity and improve lumbar spine mobility during a 6-month period in patients with refractory chronic low back pain with a neuropathic component.
This page is part of the PainScience BIBLIOGRAPHY, which contains plain language summaries of thousands of scientific papers & others sources. It’s like a highly specialized blog. A few highlights:
- Long-Term Effects of Repeated Injections of Local Anesthetic With or Without Corticosteroid for Lumbar Spinal Stenosis: A Randomized Trial. Friedly 2017 Arch Phys Med Rehabil.
- Cannabis-based medicines for chronic neuropathic pain in adults. Ateş 2026 Cochrane Database Syst Rev.
- Effect of exercise on depression and anxiety symptoms: systematic umbrella review with meta-meta-analysis. Munro 2026 Br J Sports Med.
- Optimizing elastic band resistance training for Metabolic Syndrome components in older adults: A systematic review, meta-analysis, and meta-regression of randomized controlled trials. Saez-Berlanga 2026 Arch Phys Med Rehabil.
- Biomechanical insights into Achilles tendinopathy risk and protection in runners: a large prospective study 4HAIE. Jandacka 2026 Br J Sports Med.