Quite a Stretch
Stretching science has shown that this extremely popular form of exercise has almost no measurable benefits

Stretching is a pleasant ritual for many people. It’s simple, it feels good, and we all believe — or at least hope — that something that feels that good must be good for preventing or treating injuries and aches and pains in some way. But for many athletes and couch potatoes alike, stretching can also be a bit of a drag: a duty that weighs on the conscience, one more thing to make time for. And yet they still do it!
Can all these people be barking up the wrong tree? Yes.
The goal of this huge article is to persuade you, with lots of science, that stretching is not an important part of fitness and wellness.1
- Stretching is not a good warm up. It can’t prevent or treat soreness or injury in general, or enhance performance — but it certainly can cause injuries, and it can actually slow you down!
- Stretching will boost flexibility, yes, but so can strength training,2 which is arguably much more valuable to fitness than flexibility alone, which isn’t very useful on its own… even for most athletes.
- Stretching has almost no value in treating any common kind of chronic pain. It cannot even fix poor posture, which is often blamed for pain (and much too often3).
There may be some minor benefits, and surely “every little bit helps”?4 Maybe. Or maybe almost all stretching is just a waste of time, its reputation for being therapeutic or “good for” anything almost completely undeserved.
But stretching feels good!
You bet it does! (Unless it doesn’t — there are rare exceptions.5) But clearly most people do think it feels good, even great — and it’s worth doing just for the pleasure.
Which is why I stretch almost every day — hamstrings, lumbar erector spinae, and especially the deep gluteals are my favourites. I do it because it feels nice, but I don’t believe the habit is doing much more for me than a daily back scratch. I am just as stiff and inflexible and full of “knots” as I have ever been. I play sports the same way with or without it. I still get just as sore, whether I stretch or not.
I am hardly the only person to notice that stretching for fitness goals may not be all it’s cracked up to be,6 and there’s plenty of science on this.7 This free online book — yes, this is a short online book, about 38,000 words — is a readable review of the key arguments and concepts and some of the most interesting evidence, actively maintained since the mid-2000s. Warning: you may not enjoy stretching quite so much once you realize how many myths there are about its benefits.
This isn’t just about static stretching! Types of stretching
This book is not just about the inadequacies of static stretching: just lengthening muscles and then holding still for a while. Many stretching fans are happy to join me in criticizing simple, old-school static stretching. They are happy to do that because most of them decided long ago that some other method of stretching actually does work, and that’s where their allegiance lies.
Unfortunately, there is no clear evidence that any method of stretching is a clear winner for any important therapeutic goal. All stretching is either a trivial variation on one of the basic themes, or too different to really be considered stretching in the first place (e.g. there are other “active ingredients,” like in yoga). Here’s an introduction to the members of the stretching family:
- Static Stretching — Just elongating muscles for a while, mainly varying in the intensity and duration.
- Neurodynamic Stretching — A noteworthy sub-type of static stretching devoted to stretching nerve tissue.
- Dynamic Stretching — Stretching with movement. Essentially all branded methods of stretching are some variation of dynamic stretching. Some major sub-types:
- Ballistic Stretching — Using momentum to repeatedly, briefly push past the end of your comfortable range of motion.
- Contract-relax Stretching — Alternating stretches with contractions. Also rather grandiosely known as “proprioceptive neuromuscular facilitation” (PNF).
- Dynamic Joint Mobility Drills — Rhythmic, repetitive movement through a full range of motion than usual (i.e. swinging your arms in a circle or walking lunges).
- Mixed — Complex exercise practices that include some stretching, but also much else. Yoga is the ultimate example, but virtually any activity that by nature requires range of motion — like martial arts — can be considered a complex dynamic stretching exercise.
- Pandiculation — Spontaneous brief stretches, often combined with yawning, that most vertebrate animals seem to do routinely and reflexively after a period of stillness. It’s unclear if this has anything in common with the deliberate stretching humans do.
So what is “advanced” stretching?
There are no special members of the stretching family. For instance, PNF is nothing fancy, despite the high-falutin’ name: the contract-relax approach just adds contraction.8 And it doesn’t increase flexibility any more than static stretching.91011 At best, PNF might have subtle advantages for specific situations — and good luck guessing what those are.
There’s also the whole thing about how a major presumed neurological mechanism for PNF’s alleged superiority was mostly debunked in 2009. See the “reciprocal inhibition invalidated” sidebar below.
So PNF is not so advanced after all.
And neither is anything else that has ever been touted as an advanced stretching method.
There have been countless trademarked stretching methods, probably thousands of them over the decades, most of them distinguished more by their marketing than by the details, all claiming to be advanced. For all that variety, they are all tediously similar, mostly just variations on dynamic stretching, which all integrate so much movement that they are more about movement than “stretching.” To the extent that they work, they probably work because they are just exercise — and would still work if you stripped out the stretching.
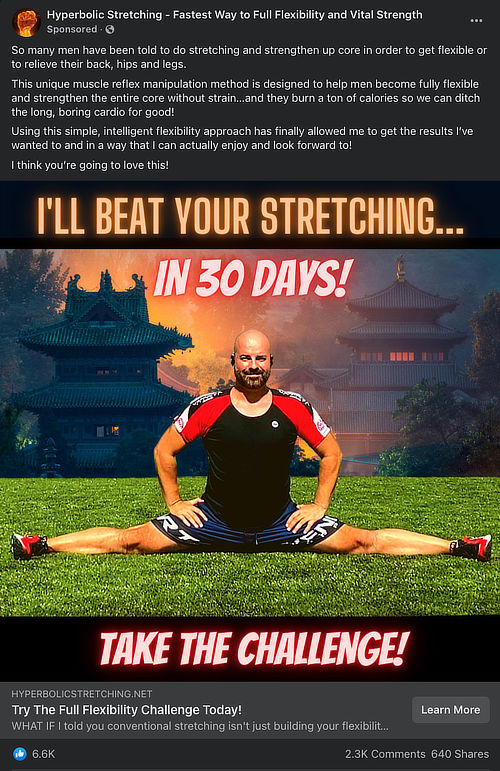
This is a fine example of an advertisement for an advanced stretching method that not only supposedly improves flexibility quickly, but helps men “strengthen the entire core with strain” and, LOL, “burn a ton of calories.” How plausible is it that there is a secret method of exercise that can improve cardio, strength, and flexibility quickly and without strain? Even if it worked, how could it possibly be just “stretching”? Also note the absurd level of social media engagement…on an advertisement.
So “advanced” it’s not even stretching anymore. A few of the most distinctive methods of stretching have earned their own identity only because they are thoroughly mixed up with other concepts (again, yoga being the most obvious example). They have fallen so far from the stretching tree that they cannot really be considered stretching anymore. There are only so many things that you can change about stretching before it really becomes something else.
I don’t really think there is any such thing as “advanced” stretching — just basic stretching with delusions of grandeur, like a Volvo with racing stripes. This book is about everything that can reasonably be considered stretching, and all those methods are quite similar — and it is not about anything else. The operational definition of stretching for this book is:
Stretching is any exercise that involves elongating muscles to the point of feeling significant tension for at least several seconds, and which may include some minor embellishments (but nothing that’s likely to be a major active ingredient in its own right).
The unstretchables: some muscles are biomechanically impossible to stretch
I will begin tipping over stretching’s sacred cows with this extremely controversial statement: anatomy has limits.16 Strict limits!
For instance, an owl can rotate its head as much as 270° and you can’t! Owl spines and people spines are different. I am not making this up.
Although anatomy is amazingly variable (for some interesting examples, see You Might Just Be Weird) it still works about the same for most people, and there are anatomical boundaries on all stretches… and some more than others.

Not as much of a stretch as it looks (or feels) like
Some muscles are just biomechanically impossible to stretch. For instance, stretching your quadriceps is about 85% futile — because most of them are just not actually stretched in this position (or any other position). Do you know why? Most people do not.
Tensile force can’t be applied equally to all muscles. Some muscles are just biomechanically awkward to stretch. I call them “the unstretchables” — a bit of hyperbole, but true in spirit. Although these muscles can be elongated, they can’t be elongated enough to create the satisfying sensation of good stretch. When we try to stretch them, most of us will hit the end of our natural range of motion long before we’ve stretched anywhere near as hard as we can stretch other muscles.
There are several noteworthy muscles and muscle groups that are just mechanically impossible to stretch much, including ones (like the quadriceps) that people think they are stretching.17 Even if stretching actually had the benefits that people believe in — which it clearly does not — those benefits would still not actually be available for large masses of muscle.
This biomechanical reality is spread over the whole topic of stretching like a large, wet blanket. Whatever stretching can do for us, if anything, it must do it within the significant constraints of our anatomy, like a suntan lotion that we can’t apply to our own back. As you read, bear this broad limitation in mind.
For much more detail, see: The Unstretchables: Eleven muscles you can’t actually stretch hard (but wish you could)
Part 2
5 Main Reasons Athletes Stretch… All Flawed
Stretching science shows that it doesn’t do most of what we hope it does

Athletes stretch mostly to warm-up, prevent and treat injuries, and to boost performance mainly through flexibility. Only one of those popular reasons for stretching has ever held up to scientific scrutiny, and even that one is only half true: stretching will indeed make most people more flexible, if you work hard enough at it, but flexibility is mostly worthless to the average athlete, and even most elite ones.
Stretching has a place of honour in athletics, sports medicine, and fitness — it is an activity everyone loves to love — and yet it is arguably the most over-rated thing you can do with a body.
But for the science of stretching in sports and fitness… just keep scrolling.
What a sensible article, and about time somebody exploded the stretching myth! I remember as a schoolboy in South Africa forty years ago always being told to run slowly to warm up for our various rugby, cricket, and soccer games — nobody ever told us to stretch, and over the past ten or so years I’ve been puzzled to see this come in as dogma. As a runner of marathons for years and a GP with injured patients, I’ve never been able to figure out how on earth stretching the heck out of muscles, ligaments, and nerves could (a) warm them up or (b) do the slightest bit of good, and have sometimes been given “the jaundiced eye” when I’ve suggested such to my patients.
Peter Houghton, MD, Vancouver (reader feedback)
An overview of the five reasons (plus one bonus reason)

Barking up the wrong tree! Literally none of the common reasons people stretch are actually good reasons (except that it feels good).
When challenged, stretching enthusiasts — both casual and hardcore — have a surprisingly hard time explaining why they are stretching. Everyone just “knows” that it’s a good thing, and they haven’t really thought about why. It’s dogma, practically a religion.
When pressed for reasons, most people will cough up a few predictable stretching goals. Here are the four hopeful reasons for stretching that I hear every day:18
- flexibility, of course
- warm up and injury prevention
- prevention/treatment of exercise soreness
- treatment of sports injuries and chronic pain
And a fifth which I only hear occasionally, but it’s still out there:
- “performance enhancement” (e.g. faster sprinting)
All of these overlapping goals for stretching have serious problems. Either they have long ago been proven to be impossible,19 or they never made sense to begin with, or both, or worse. Certainly none of them is a slam dunk. They will all be critically analyzed below.
Bonus reason to stretch!
It feels good, obviously. This is the neglected bonus reason for stretching I can get behind.
Reason #1: Stretching as a warm up (which can actually backfire)
You cannot “warm up” your muscles by stretching them: it’s like trying to cook a steak by pulling on it. Instead, the best way to warm up is probably to start by doing a kinder, gentler version of the activity you have in mind (i.e. walk before you run). The metabolic activity involved in muscle contraction does literally warm up your muscles, an inevitable side effect of all the activity that actually makes warm up effective for injury prevention.

Warmup works
A large study of girls’ soccer teams showed warming up can cut injury rates by about a third. Notably, the warmup that was studied, FIFA’s “11+” warmup, did not include stretching!
Nothing about static stretching is more clear than this failure. Your basic quick (static) stretch warmup is one of the most studied topics in all of musculoskeletal health care and exercise science. For instance, a huge 2011 review of all the research found “overwhelming evidence that stretch durations of 30-45 seconds … imparted no significant effect” and even some evidence of harm.20
Um, harm? Slight harm, yes: stretching may actually reduce performance. Probably not much, but also probably not what anyone wants. More on this shortly.
Metaphorically, “warming up” also refers to readiness for activity or body awareness. You are “warm” in this sense when you are neurologically responsive and coordinated: when your reflexes are sensitive and some adrenaline is pumping. Warmup for its own sake (i.e., without following it up with more intense exercise) is fairly pointless — the goal is to prevent injury and enhance performance. And those goals may be realistic. For instance, research has shown that a warmup routine focused on these goals actually does provide decent insurance against the number and severity of both accidents and over-use injuries.2122
So, warmups in this second sense are probably helpful … but does stretching warm you up in this sense? No, probably not much — certainly no more than a bunch of other exercises you could do — and quite possibly not at all. One of the most-studied warmup regimens (including one of the studies just cited), FIFA’s “The 11+” programme, notably does not include stretching.23 The most compelling evidence that stretching doesn’t warm you up is the evidence that shows that it doesn’t prevent injury or enhance performance (discussed below)… but it can actually cause some injuries, and might even impair some kinds of performance! Much more on those backfire effects in the sections ahead.
Static stretch is somewhat stimulating to tissue, but in ways that are quite different from most actual activities.
Because of all this, stretching to warm up does not even qualify as “official” exercise dogma anymore — most professionals actually gave up on it many years ago, and it is passé even in the opinion of a great many more informed joggers and weekend warriors. It simply doesn’t work, and it’s hard to imagine a common fitness practice more thoroughly contradicted by the evidence and by many professionals. And yet …
And yet I still see it all the time in the wild. I live and play on Vancouver’s famous “sea wall” — one of the best and most popular running routes in the world. And so I can constantly observe runners in their natural habitat, doing what runners do. A great many of them participating in structured training programs and running groups, instructed and led by experts and coaches… and they stretch to warm up. In droves. So despite the evolution of professional opinion, this practice clearly still needs to be discussed and debunked.
I am also an avid ultimate player,24 and so I also routinely see seriously athletic people stretching to warm up (and often hear their justifications for it, too, which are always bog standard stretching dogma).
Clearly there are still far too many people out there stretching before they run and play sports, trying to “warm up” almost exclusively by standing still and elongating muscles!
Once again, the best way to prepare for an activity is probably just to start it slowly.
Reason #2: Stretching to prevent soreness (or speed recovery from it)

The evidence strongly suggests that stretching does not prevent DOMS
Another extremely popular idea about stretching is that it prevents a specific type of soreness: the deep soreness that follows a hard workout. That phenomenon is called “delayed-onset muscle soreness” (DOMS) or sometimes just “post-exercise soreness.” Many people believe that stretching can help DOMS. Some seem to believe it like it’s their religion, and it’s amazing how determined people can be to ignore evidence that contradicts it.25
Recently (2016), decades after this faith first got entrenched, science finally coughed up a specific reason why it might be based on something: evidence that stretching reduces inflammation in connective tissue.26 This isn't particularly surprising; exercise in general is anti-inflammatory.27 Surely this is relevant! It sure sounds like a great science factoid to explain why people think stretching helps soreness after exercise. Practically a slam dunk! It is interesting evidence for sure, and I’ll return to it later.
But there are many problems with leaping to that conclusion.28 It’s a classic mistake to assume that a scrap of biological relevance translates into a clear benefit in the real world. Unfortunately, the evidence strongly suggests that stretching does not prevent DOMS. Many studies have shown that nothing short of amputation can prevent DOMS293031 — and certainly not stretching.32 Whatever effect stretching has on inflammation in connective tissue, it does not add up to a DOMS cure — or any other clearly identified biological benefit of stretching.
Reason #3: Stretching to prevent injury
The commonly accepted idea that increased ROM and stretching prior to activity prevents injuries has been challenged and found to be on the shakiest of scientific foundations, or to come from such a paucity of data that no reasonable conclusions can be drawn.
Flexibility, by William Sands, p. 389

The evidence does not show that injuries are prevented by stretching. Indeed, stretching may be more likely to cause injuries — especially because too many people try too hard.
According to the evidence to date — which isn’t everything we could hope for, but there certainly is some — stretching probably does not prevent injury. As I mentioned above, this has been suggested by a combination of recent literature reviews and large clinical studies, some of which I have already cited. Here’s some more…
In 2005, the Clinical Journal of Sports Medicine published a review of the scientific evidence, and found that “showed stretching had no effect in reducing injuries.”33 Neither poor quality nor higher quality studies reported any injury prevention effect. Regardless of whether stretching was of individual muscles or entire groups, there was no reduction in injury rates.
A 2008 study published in the American Journal of Sports Medicine showed “no significant differences in incidence of injury” in soldiers doing preventative exercises.34 Half of them participated in an exercise program including 5 exercises for strength, flexibility, and coordination of the lower limbs, and 50 of those soldiers sustained overuse injuries in the lower leg, either knee pain or shin splints. The other 500 soldiers were doing nothing at all to prevent injury in the lower limbs — no specific stretching, strengthening or coordination exercises — and only 48 of them had similar injuries. There were “no significant differences in incidence of injury between the prevention group and the placebo group,” and the authors concluded that the exercises “did not influence the risk of developing overuse knee injuries or medial tibial stress syndrome in subjects undergoing an increase in physical activity.”
However, what is clear is that the exercise regimen certainly included static stretching, and it certainly did not work any prevention miracles for some of the most common athletic injuries from the knees down. If stretching performs that poorly in such an experiment, how good can it possibly be at preventing other injuries? Probably not very.
Here in Vancouver — a running Mecca — researchers at Simon Fraser University have done an unusually large study of pre-run stretching, with more than 2700 participants. They found “no statistically significant difference in injury risk between the pre-run stretching and non-stretching groups.”35 Injury rates for all kinds of injuries were the same, with or without stretching. It’s almost as though stretching made no difference at all. But make up your own mind!
I’m never surprised by such findings, because I’ve never heard a sensible explanation for how stretching can prevent most of the sorts of injuries it is intended to prevent. Usually, advocates have a vague notion that “longer” muscles are less likely to get strained: even if garden-variety stretching made muscles longer (which is doubtful in itself), and even if we knew exactly what kind of stretching to do (we don’t), and even if we had the time to stretch every significant muscle group, the benefits would still be relevant to only a small fraction of common sports injuries. An ankle sprain, for instance, or a blown knee — two of the most common of all injuries — probably have nothing to do with muscle length.
Not convinced yet? A 2014 review of exercise therapy for injury prevention in the British Journal of Sports Medicine was completely negative about stretching36 — even though the authors were obviously a bit too optimistic about everything else!37 “Consistently favourable estimates were obtained for all injury prevention measures except for stretching.” Ouch.
Stretching as injury prevention for runners and other endurance athletes has always been a little bit more of a reach. A detailed 2017 review adds yet another well-defended expert opinion that stretching isn’t useful for runners in any way.38
In 2020, the British Journal of Sports Medicine published a review in infographic form that declares that the research “definitively” shows that the belief in stretching as injury prevention for runners is wrong.39 I can’t use the infographic here because copyright, but you can easily find it with a search.
Any good news?
All those reviews and expert opinions based of imperfect evidence could be wrong: there might be some injury prevention powers to stretching, which simply haven't been confirmed yet. Muscle strains seem like the most likely candidate for a couple reasons40. Any benefits that do exist may be quite specific and missed by many basic, general pre-event stretching regimens,41 but they might exist.
And I am aware of at least one clear example of a study that certainly seems like good news. A 12-week customized stretching program initially did not initially prevent any injuries in about sixty high school soccer players, compared to another sixty in a no-intervention control group — there was no effect during the dozen program. But there was a clear reduction in injuries over the next forty weeks, so that’s interesting.42
Instructed stretching exercises, personally designed by physical therapists to address muscle tightness, improved the range of motion and trunk flexibility, with a positive effect on the injury rate in male high school soccer players, especially for non-contact disorder injuries during training.
But it’s just one study, and all studies have flaws. It is interesting, but it’s not enough to turn the debunking tide.
Reason #4: Stretching to recover from injury

Most of injury rehab is (or should be) just “load management”… but stretching doesn’t have much to contribute to that.
That which prevents injury often also treats it, and vice versa, and that’s the basic rationale for stretching as a treatment for injury — better late than never? People believe that stretching prevents injury, and so they extend that assumption to treatment. Unfortunately, we already know that belief is wrong and stretching does not prevent injury… so it’s unlikely that it can treat it either.
There are some more elaborate rationalizations for stretching as a treatment, chiefly that it corrects something.
Exercise is the closest thing there is to a general miracle drug,4344 and strength training is one of the best types of exercise, practically like magic: healthier and more efficient than most people realize.45 It’s also widely accepted as a major part of injury rehab, and stretching goes along for that ride. Although it’s not taken anywhere near as seriously as strengthening, millions of athletes, trainers, coaches, and healthcare professionals still consider it to be a staple of rehab.
Tedious and specific “corrective” or “therapeutic” exercises are a tired cliché of rehab and physical therapy, both strengthening and stretching. It’s what everyone (athletes and non-athletes alike) imagines their training montage will look like if they are ever hurt.
Unfortunately, corrective exercise isn’t a great reason to build strength, and it’s an even poorer justification for stretching. This style of rehab is largely based on the flawed and even harmful assumption that there is something in-correct about injured patients — fragile, weak, uneven — which must be fixed by sufficiently expert and precise exercise prescription.
For instance, there is often an alleged “imbalance” that consists of both overstretched and weak muscles that need to be toughened and tightened up, and tight and overworked muscles that need to be loosened and stretched.46 It’s surprising how much that single idea has boosted the perceived importance of stretching in the rehab equation.
This kind of thinking has been called the “trap” of corrective exercise, for pros and patients.47 (You can read much more about “the trap” in my main strength training article.)
Stretching obviously doesn’t have much to contribute to load management. At best, it could be considered a form of light exercise that could be used for some stimulation in the early stages… but you could and probably should mostly just stick to dynamic joint mobility drills and very easy strength training instead.
If there’s any other justification for stretching in rehab, it has to live in the much smaller neighbourhood of rehab that isn’t all about load management.
Protecting or restoring range of motion after injury
This is the most reasonable reason to stretch for rehab: not because it helps the injury itself to heal, but to prevent any related loss of range of motion, or to restore it. As explained in detail below, there is no doubt that stretching can improve range of motion. But more ROM does not have clear value in general. Many factors restrict its importance even further in a rehab context.
Stiffness is the sensation that inspires stretching in rehab, but injury stiffness — the stiffness that typically afflicts the joints near an injury — usually has nothing to do with “tight” muscles and tendons. It’s mainly just a neurologically imposed inhibition of movement, a kind of pain, a warning about movement rather than a lack of it. To the extent that it actually does involve any shortening of muscle, it’s probably either minor and temporary and things will get back to normal on their own… or it’s more serious and cannot actually be affected by stretching in any case.48
I think there are some clinical scenarios where a little stretching to maintain or restore post-traumatic ROM is probably worthwhile, but they are minor and rare.
Specific stretching for specific injuries
If not to maintain and restore range of motion, why else would you stretch an injury? What else could stretching do for an injury? Most people imagine that it’s about restoring balance: fixing things that are “too tight” and holding back recovery in some way, probably by constantly irritating the injury. In many cases, this hypothetical restriction is considered the root cause of the injury in the first place, which must be addressed to allow healing to proceed.
Stretching itself is not generally rehabilitative, because a limited range of motion does not usually cause or sustain injuries. Every kind of injury has to be considered separately, because there are all kinds of specific ideas about why one should stretch to fix different injuries. But if you go through a list of injuries and their presumed mechanisms, most cannot be blamed on anything that stretching can fix. Maybe none.
For instance, people believe that the reason they get iliotibial band syndrome, one of the two common kinds of runner’s knee is because the iliotibial band is “too tight.” Unfortunately, that almost certainly isn’t the problem, and the IT band is much too tough a structure to stretch in any case.49
But the arguments for and against stretching for ITBS are completely different than they are for, say, muscle strains or low back pain. Different kinds of injuries, different arguments about stretching. My plantar fasciitis book goes on for three chapters about the possible role of stretching in treating that condition, but the bottom line is that it either doesn’t work, or not all that well.50
Over time, I will expand on a few other major examples. For now, suffice it to say that
There are a handful that might be in the “promising” category, where it’s probably worth giving it a try. It’s not like stretching is expensive or risky. But even in those cases, it’s always arguable that dynamic joint mobility drills and strengthening would be better choices. For instance, in the case of muscle strain (tear), stretching may help cue the healing mechanisms in your muscle to lay down new connective tissue in a tidy way, and there’s even evidence to support that51 … but so will gentle contractions. Simply using the muscle almost certainly does the same thing, or does it better.
You can go back and forth like this with almost any injury, but the bottom line is that stretching has never been found to make a significant difference in anyone’s rehab.
Ackshually, stretching can cause injuries (and other harms)

Ironically, stretching can actually cause some of the very injuries it is thought to prevent or treat. Although stretching is mostly a safe activity, especially if practiced with a modicum of caution, there are (at least) four potential types of stretching hazards:
- Stretching as a warmup may modestly impair athletic performance, as discussed above. Not a huge concern — a trivial effect — but also exactly the opposite of what people want from their stretching: a backfire in spirit, even if minor.
- Traumatic injury (sprains and strains) from over-stretching, fairly common in yoga, dance, martial arts, and so on. People just overdo it, sometimes.
- Traumatic injury to people who should never be stretching in the first place, but may not know it, because of medical vulnerabilities directly related to flexibility, mainly the hypermobility spectrum disorders and connective tissue diseases (e.g. Ehlers–Danlos syndrome, Marfan syndrome).
- Unexplained pain and illness may combine poorly with stretching — which is not really stretching’s fault, but it is stretching’s problem and a legitimate reason why stretching is a bad idea for some people. This section focusses on physical trauma, but later in the book I’ll discuss medical harms like lightheadedness, fainting, nausea, and malaise: see “Stretching doesn’t always feel good.”
Hypermobility and Ehlers-Danlos syndrome
Some people are much more flexible than average — pathologically flexible. “Hypermobility spectrum disorders” (HSD) are a group of conditions defined by joint hypermobility — unexplained joint looseness.52 Ehlers–Danlos syndrome (EDS) is a closely related group with known genetic causes53 that includes hypermobility along with fragile tissues that heal poorly, especially skin, with many consequences. All of these conditions together are quite common, and chronic pain is a routine complication.54
Most people don’t need to stretch, but people with HSD/EDS really should not stretch … and they may not know it. HSD/EDS is often undiagnosed and mistreated; it is clinically important and yet often non-obvious. So lots of people are probably suffering without having any idea why or that they shouldn’t be stretching. Consider this story from a 75-year-old reader:
Upon continued strong urging by my physical therapist, I engaged in “glute” and “quad” stretches — quickly to my detriment and horror. MRI survey confirmed gluteal minimus and medius tendinitis and partial thickness tendon tears. After a year of seeking help and ineffective treatment I was just this month diagnosed by a rheumatologist with hypermobility joint syndrome.This condition does not seem to be on the “radar” of most docs or PT’s. As a kid, I delighted in acrobatics, some said I was “double-jointed”; and in high school and college, modern dance (which included acrobatics). I was still dancing and hiking up until a year ago, but this injury has been devastating!
Now I understand the problem, so my rehab routine is strengthening within a normal range of motion. Feel-good, easy whole-body stretching only. Swimming has been a great help, along with careful exercising with weights at the gym.
It’s awful that this patient, with a long history of hypermobility, was convinced to overstretch by “strong urging” from a healthcare professional. This is a perfect example of clinical ignorance of hypermobility and the consequences of unjustified enthusiasm for stretching. Most people, even healthcare professionals, are simply oblivious to how common and serious hypermobility is — but it’s highly relevant to the value and safety of stretching.
Other soft-tissue vulnerabilities
A strong enough stretch can damage any anatomy, obviously — it’s a physical stress. If applied to tissue that is fragile in any way, harm is more likely. Hypermobile tissues are fragile in a way that is quite obviously related to stretching, but there are other ways for tissues to be vulnerable to physical damage, and I have a whole article about that: Sneaky soft-tissue fragility: Many underdiagnosed health problems reduce the resilience of muscle and connective tissue, increasing the risks of “deep” massage and stretching. This category also overlaps with other chronic illnesses that involve other kinds of vulnerability, discussed in some detail below.
For instance, back pain has many possible causes — including a wide variety of possible issues with the spine, many of which could be aggravated by stretching, even severely. And yet people routinely attempt to self-treat back pain with stretching, more or less oblivious to the possibility that it will do more harm than good in some cases.
Here’s the story of my own ill-fated attempt to treat some neck pain with stretching:
Reason #5: Stretching to enhance performance
The most flexible athletes are not necessarily the most successful.
Flexibility, by William Sands, p. 389
You don’t hear this argument for stretching as often as you hear the others. And yet it comes up, especially with runners, and with athletes who play sprinty team sports. It’s a common practice to stretch when you’re off the field. The habit is probably usually rationalized as an injury prevention method, but many of those athletes will also insist that it enhances their performance — that the muscles “spring back” from the stretch and make them run faster.55
I’ve already mentioned a huge 2011 scientific review by Kay et al. that found “overwhelming evidence” that pre-exercise stretching has “no significant effect.” That was not a surprise. What is a little surprising is that the same review showed the opposite of a benefit — that pre-exercise stretching might reduce muscle strength.56 I wouldn’t take the danger too seriously, but it certainly emphasizes the lack of benefit: if anything, it swings the other way. Yikes!
Similarly, research has shown that stretching does not improve sprinting … but it gets worse. What really happens to your sprint if you stretch first? It turns out that, all other things being equal, the athlete who didn’t stretch is actually going to leave you behind!
If you want to perform in a sprinty sport, you might not want to stretch right before getting your cleats dirty.
There are many possible mitigating factors here.58 However, the complexities only emphasize the absurdity of the legions of people who have an oversimplified faith that stretching gives them an edge. The evidence is clear that stretching is largely pointless for enhancing performance, and quite possibly worse. Scientific reviews just keep reporting the same conclusion.59 Maybe eventually this news will reach amateur athletes? But don’t hold your breath.
What was that about stretching impairing performance? MOAR SCIENCE
A 2014 test found that a nice pre-run stretch causes “a reduced capacity of the skeletal muscle to produce explosive force.”60 Yikes. It’s not a huge effect, but as Alex Hutchinson put it for Runner’s World, “I can’t see anything good about something that makes me go slower but feel like I’m trying harder.” Indeed, it’s literally the opposite of what people want. Even if the harm is too minor to be of concern, it does underline that stretching is not an effective warm-up.
There are many other studies that have shown static stretch-induced performance impairments, and I’ll summarize some of them in a moment. But why would this happen? It might be purely psychological and neurological — basically just a relatively obvious consequence of a relaxing activity right before a vigorous one. Or stretching could temporarily interfere with normal movement function; virtually any way of measuring it might be impaired in the immediate aftermath of a strong stretch, and how long does that go on? If you do a powerful stretch, it’s actually quite obvious that it takes a few moments to get back to normal after exiting the stretch; we all need to flex and squirm a bit to restore normal movement, and it’s possible or even likely — based on the evidence — that this effect lasts for quite a bit longer than is obvious. Anything more than a couple minutes would be a deal-breaker for me, and probably for most athletes.
Here are some more studies about this crappy effect:
- Musham 201061 — Researchers compared dynamic stretching with “active static stretching” (yep, that acronym is “ASS”) and a control group before sprints of over 20 metres. ASS had no effect one way or the other at first, but turned negative over repeated sprints; 65% of results showed a negative impact by the third sprint. This implies an effect on endurance.
- Wolfe 201162 — The baseline performance (V02 max) of ten elite endurance cyclists was checked on three different occasions. On the second and third occasions, some of them did static stretching first (five stretches, each one held for 30 seconds four times in a row). At the five-minute mark in their workouts, their submaximal VO2 spiked a bit. That sounds good to the untrained ear, but it’s actually a bad thing, and so: “Coaches and highly trained endurance cyclists should exclude static stretching immediately prior to moderate intensity cycling as it reduces acute cycling economy.”
- McHugh 201363 — This was a test of the effect of stretching on hamstring stretches with and without spinal flexion, which adds “neural tension” to the hamstring stretch (by pulling on the spinal cord and big nerve roots and nerves like the sciatic nerve). After stretching with neural tension, strength dropped about 12% — quite a bit actually! The effect of regular hamstring stretching was a mixed bag, with reduced strength at short muscle lengths but boosted at long muscle lengths — a fine example of how generalizations about the effects of stretching are foolhardy.
- Lowery 201464 — Pre-run stretching caused an eight percent drop in performance in a one-mile uphill run. Alex Hutchinson had plenty to say about this one, but here’s the nasty nugget: Yikes!
- Konrad 202065 Punctuating the danger of oversimplification, this review strongly emphasizes that “your mileage may vary” (very close to literally). This review reports a range of both positive and negative effects on performance, depending on what kind of stretching and how performance is measured. But, without a doubt, static stretching can impair performance in some ways in some athletes; the authors reported “detrimental effects in performance variables and metabolic variables.” In general, static stretching seems to more likely to hold you back, whereas dynamic stretching is more likely to be helpful.
None of these needs to be a deal-breaker for anyone who loves stretching. The effects are too minor and complex to be much of a concern. But they do vividly show that basic static stretching — the kind of thing almost all amateur athletes do constantly, and way too many elite athletes too — is definitely not helping consistently/much. And that directly contradicts one of the most classic reasons that people stretch.
Cramp first aid: at least one undeniable stretching benefit
Stretching may not have much of a role in treating or preventing sports injuries, but it is the only way to respond to an acute cramp — which can be injurious. The cramps encountered by most people in a fitness context are exertional or exercise-induced cramps, which is just one of many other kinds of unwanted muscle contractions. We can see how complex muscle physiology is just from the number of ways that it can glitch!
Exercise-induced cramps are intense, painful contractions that usually strike when fatigued and/or overheated. They are most common in the legs, especially the calves and hamstrings, more rarely the quadriceps. Fatigue and heat are major factors, but not dehydration and electrolyte shortage (that’s a myth).66 What actually does cause them is still unclear (shocker), along with much else about them.
Regardless of how cramps work, we have to stretch (or be stretched) when they strike: the urge to pull the other way is irresistible, like jerking your hand away from fire. It feels like we have no choice. Stretching isn’t a “treatment” for cramps per se — it’s more like urgent first aid. The only way to cope with an acute exertional muscle cramp is to directly fight the contraction with stretch.
It’s a benefit of stretching in the same sense that not bleeding is a benefit of a bandage. But why? Does a stretch actually “stop” a cramp? Or does it just make it more tolerable while we wait for it to ease? I don’t think anyone knows the answer to these questions.
Cramp first aid is a legitimate use for stretching, even if it doesn’t actually have anything to do with why people normally stretch.
Last word: Stretching is not a ‘pillar’ of fitness
A lot of stretching happens in an athletic context for the reasons discussed above, but they all have something in common. The underlying general assumption, almost always unstated, goes like this:
Stretching is a major component of fitness, on par with strength and endurance.
That idea breaks down into specific claims that don’t hold up under scrutiny, but no matter how effective that debunking, almost everyone who likes stretching will continue to assume that it’s different for “serious” athletes or athletes who seem to need more flexibility: gymnastics, dance, martial arts, circus arts, and so on. And yet it’s likely that even for those functional goals stretching is not actually anywhere near as important as we have believed, and maybe not even important at all. If all this information is taken to heart, it should be clear that a “serious” athlete might actually want to avoid stretching. They have a lot of other training to do that is definitely more important — and which will also achieve flexibility.
Until fairly recently, there were few major examples of elite athletes rejecting stretching, but that’s changing. The best recent example I know of is that the Australian Ballet has purged stretching; instead, it’s all about training for strength training throughout the full joint range. The Australian Ballet has written about their experience with this: same or better performance, fewer injuries. Wow.
Dogma is powerful. When there’s a long tradition of doing things a certain way, it can be extremely difficult for people to accept that it might not be necessary. For years, I have been getting cranky email from martial artists, sneering smugly about how I obviously know nothing because, clearly, elite martial artists know that they have to stretch. Maybe. I doubt it, and I think that doubt will be confirmed in time, but it’s officially unknown.
I do know the power of dogma. I know how many times in sports history traditional practices have been overturned and replaced by updated beliefs that were required to break new records.
And in fact I do have some personal experience with martial arts, and I know that not every martial artist is flexible or thinks they need to be. My most memorable example was a grizzled old practitioner of Aikido — the most formidable martial artist I ever met, and also the least flexible. He seemed flexible, but it was all in how he used the rather stunted range of motion he had. He worked within his limitations like an artist — a martial artist — and you would never even have guessed he was so stiff unless you spent time with him in training.67 We never stretched much in that dojo, and an MMA club — with some very competitive members — also never did any stretching.
As the years tick by, I predict that there will be more and more stories about elite athletes who no longer stretch — but still kick ass.
Why is it that many Kenyans don’t stretch? Why was legendary coach Arthur Lydiard not a fan of stretching? Why does Galloway say, “In my experience runners who stretch are injured more often, and when they stop stretching, the injuries often go away”?
Bob Cooper, Runner’s World Magazine68
I am a soccer referee, and mostly by happy accident began substituting what you call “mobilizing” for various stretches prior to my matches, and I find this does an excellent job of stimulating the muscles, whereas after only stretching I still seem to be tight for the first several minutes. Then I read this article, which corroborates what I have found in practice!
Carlos Di Stefano, soccer referee (reader feedback)
•
In the face of so much discouraging evidence, it makes sense to assume that sport itself provides all the “stretching” one needs. The late Mel Siff:
It is almost heretical to question this stretching doctrine, yet it is important to disclose that there is no research which proves categorically that there is any need for separate stretching sessions, phases or exercises to be conducted to improve performance and safety. To appreciate this fact, it is useful to return to one of the clinical definitions of flexibility, namely that flexibility refers to the range of movement of a specific joint or group of anatomical tissues. Moreover, flexibility cannot be considered separate from other fitness factors such as strength and stamina. There is no real need to prescribe separate stretching exercises or sessions, since logically structured training should take every joint progressively through its full range of static and dynamic movement. In other words every movement should be performed to enhance flexibility, strength, speed, local muscular endurance and skill, so that separate stretching sessions then become largely redundant.
Facts and fallacies of fitness, by Mel Siff, p. 123
Siff’s sensible minimalism — from 1988 — stands in stark contrast to a much more common and marketable “flexibility first” approach, an approach that just happens (coincidence, I’m sure!) to give coaches, trainers and therapists something to be expert about: the idea that athletes must make a point of increasing flexibility first (by whatever stretching method), and then train for the strength and coordination to exploit this marvelous new range of motion. That picture is quite likely to be exactly backwards.
More reading related to athletic stretching
- Why Do Muscles Feel Stiff and Tight? — Maybe your range of motion is actually limited, or maybe it just feels that way
- A Deep Dive into Delayed-Onset Muscle Soreness — The biology & treatment of “muscle fever,” the deep muscle soreness that surges 24-48 hours after an unfamiliar workout intensity
- The Tyranny of Yoga and Meditation — Do you really need to try them? How much do they matter for recovery from conditions like low back pain?
- Strength Training for Pain & Injury Rehab — Why building muscle is easier, better, and more important than you thought, and its role in recovering from injuries and chronic pain
Injuries where stretching might play some role in rehab… or where its role particularly needs debunking:
Part 3
Stretching for Pain (and Pleasure)
Is stretching a treatment for chronic pain?

Stretching has an extraordinary reputation for being good for aches and pains, but it’s not clear that stretching deserves this honour.
Stretching as therapy mostly rides on the coat-tails of stretching’s indomitable popularity for other purposes, especially the nearly universally accepted idea that flexibility is a pillar of wellness and fitness, on par with strength and endurance. Unfortunately, that claim does not hold up to scientific scrutiny. All common ideas about the benefits of stretching have been shot down by research over the last twenty years.
But if stiffness is like an itch, stretching is how we want to scratch it! And the symptom of stiffness is thoroughly tangled up with chronic pain. The pleasant sensations of stretching seem directly relevant to the symptom of stiffness, like ice on a burn. It feels inherently valuable to people, and I am not knocking “pleasure”!
But not everything that feels pleasant is actually therapeutic, and there are many, many kinds of pain. Even if stretching is good for some of them, it probably isn’t good for all or even most of them.
So what kind of pain does stretching work for? Any of them? And if so, why? I will have some good things to say about it, but there’s also plenty of debunking ahead.
Stretching as therapy for miscellaneous pain and stiffness
The anecdotal evidence that stretching “works” for miscellaneous body pain and stiff and aching muscles is substantial. (So is the anecdotal evidence that it can backfire.) There is also some scientific evidence suggesting that stretching is helpful for common stubborn pain problems, such as neck and back pain,6970 but it’s also a complicated, incomplete, underwhelming mess, like a good 2016 study of stretching for neck pain that had completely underwhelming results.71 Or a 2010 study of exercise for headache confirmed that stretching is much less effective than strength and endurance workouts72 — and yet almost everyone thinks that many headaches are caused by neck tension. Or a 2020 trial of stretching for fibromyalgia that damned stretching with very faint praise73 — a “technical” win for stretching, but not a very satisfying one.
There are also popular stretching tactics for common conditions that are clearly a waste of time. One of the best examples is the idea that tight hamstrings cause back pain, and therefore stretching them is good back pain therapy. But they really don’t, and it’s really not (there’s a whole section about this below). And yet that belief probably accounts for at least 50% of all the stretching people do for back pain!
Another good example is the passionate dedication some runners have to stretching their IT bands — a huge, tendon-like structure on the side of the thigh — to prevent/treat runner’s knee. But IT band “tightness” is not what causes iliotibial band syndrome, and you couldn’t stretch it out even if it did.74
What’s wrong with this picture?
She’s not doing much with this classic IT band stretch. Even if her technique was good. Which it’s not. More about IT band stretching.
And yet…
Stretching doesn’t seem to come close to “curing” anyone of anything, but darned if it doesn’t sometime seem to “take the edge off” enough to make it worth trying. Consider the trial of stretching for fibromyalgia mentioned above: not impressive results, but technically positive. And when your as desperate as most fibromyalgia patients, any relief is welcome — especially if it’s as cheap and safe as a bit of stretching.
So people in pain stretch, and sometimes they feel better. A little bit. For a while.
People who feel stiff and tight usually assume their range of motion is limited by literally short muscles, but this is rarely the case, despite how it feels. Stiffness isn’t the same as being inflexible; they aren’t even really related.
There are many possible causes of soreness and stiffness that stretching has little to do with: sensitization, and positional cervical cord compression and multiple level radiculopathy, vitamin D and magnesium deficiency, and non-obvious entrapment of nerves (neuropathy) and bloods vessels (claudication). Several hard-to-diagnose diseases can involve long-term excessive aches and pains as a major symptom, such as the hypermobility disorders, facioscapulohumeral muscular dystrophy (FSHD), and multiple sclerosis. And then there’s drug side effects, too!75
That is just a sampling; all of these and more are summarized in 38 Surprising Causes of Pain. If you have pain from any of these sources, stretching is quite unlikely to help. In some cases, it might be useful for symptom control, at best.
Of course, there could be reasons why stretching is good for pain that we don’t understand, or are only just barely starting to understand. In the next sections, I’ll get into some of the causes of stiffness that stretching might be more relevant to: inflammation, trigger points, and contracture. But — spoiler alert — there’s literally not one clear promising example of stretching as effective medicine for anything painful. Not one.
Stretching, inflammation, and aging

“Inflammaging” is a steamroller that stretching probably can’t touch. Nice idea, though.
Why do we so clearly get stiffer as we age? Even in people who have nothing in particular wrong with them, none of the many causes of aches and pains mentioned above?
If there’s one thing most responsible for the feeling of needing to stretch, it’s probably the most common cause of aches and pains: “inflammaging.” Chronic low-grade inflammation that gradually escalates over the years, for all kinds of poorly understood reasons.76 This kind of stiffness is basically a form of mild pain that limits range of motion basically by making it uncomfortable. Our brains are more reluctant to allow free, quick movement of sore tissues. Stiffness is probably mainly a form of inhibition, then.
Unfortunately, systemic inflammation cannot be diagnosed or treated reliably by any means: it is simply too complicated and mysterious. Nevertheless, it is a trendy bogeyman, and allegedly anti-inflammatory diets in particular are extremely popular. But the best defense is simply to be as fit and healthy as possible.
And stretching? That seems like a long shot. But it’s worth discussing, at least.
Stretch your inflammation away?
A 2016 study produced one scrap of evidence that stretching reduces inflammation in connective tissues.77 It’s not clear how much “inflammation in connective tissue” is related to inflammaging — maybe none, maybe lots — but obviously there could be a connection.
We do also have some relevant evidence that inflamed connective tissue is associated with back pain,78 which is of course the epicentre of stiffness as we age (although back pain actually backs off quite a bit on the far side of middle-age).
That evidence is all there is, and it’s too scanty to trust yet. In fact, I am confident that these isolated research clues are probably misleading, and I don’t really buy that stretching reduces inflammation any more than I believe that massage reduces inflammation (a popular idea based on one over-hyped study79). But let’s keep our minds open.
If stretching does help some inflammation resolve, obviously that would be good for us. It wouldn’t even have to be a large or consistent effect (neither are the benefits of pain meds). “Taking the edge off” sometimes would be enough to explain the reputation stretching has for relieving stiffness and soreness.
Chances are strong that inflammaging is a steamroller that stretching cannot really touch, however. There are several plausible mechanisms for inflammaging that are unlikely to be affected by stretching. The best hope is that stretching is somehow mildly anti-inflammatory, regardless of what caused the inflammation, but it’s more likely that fitness is much more “anti-inflammatory” than stretching specifically. Practically any functional stimulation of the same tissue — not just stretching — might have the same modest anti-inflammatory effect.
Stretching for fibromyalgia
Fibromyalgia is a common, unexplained, and mostly untreatable illness of chronic pain, fatigue, and mental fog affecting about 1 in a 100 people. Its non-specific symptoms are often confused with (and/or related to) many other conditions. It probably has multiple possible causes, including more severe or premature cases of the "inflammaging" discussed above. Controversy, stigma, quackery, and junky science swirl around fibromyalgia like a bad smell. Only a handful of imperfect treatment options exist, most notably scrupulous sleep hygiene and exercise in tolerable dosages.
Stretching is light exercise.
There is no other specific reason to think stretching is helpful for fibromyalgia patients, but — like most of of self-serve wellness practices, the easy things widely believed to be good for us — it’s one of those things fibromyalgia patients routinely have on their “try everything” list.
But for many people with chronic widespread pain, however, it does not even feel good. The legendary deliciousness of stretch is just not there. When I originally blogged about this, most of the feedback came from folks with fibromyalgia: “It just hurts too much. Usually too sore!”
Even light exercise may not be viable for people with severe and chronic widespread pain. And so a lot of stretching experiments for fibromyalgia patients end quickly.
For fibromyalgia patients that do like the feeling of stretch, of course there’s never anything wrong with adding some good feelings to your life. But … is it a “treatment”?
Tested: stretching for fibromyalgia
There’s barely any science specifically about stretch for fibromyalgia, and what we have is not inspiring stuff: like Støve et al., published in mid-2026, about a little experiment claiming that a mere six minutes of daily home stretching for six weeks reduced fibromyalgia symptoms by a bit over 18%.80 Not exactly “huge” if true, but good enough, and cheap, and no major flaws leap out of the abstract, so … should I put that in my skeptical pipe and smoke it?
No. It’s a terrible experiment, and no threat to my bias against stretching. If anything, this study backfires and undermines stretching as a treatment for fibromyalgia. Based on the abstract alone, Støve et al. sure looks like solid good news, but abstracts are like movie trailers: they only show you the good bits!

Støve et al.’s abstract is a perfect example of making the experiment sound much better than the full paper does. (Image source unknown to me.)
The honest conclusion — like an “honest trailer” for a bad movie [YouTube again] — is that a six-minute daily routine with weekly researcher contact improved self-reported fibromyalgia symptoms over six weeks compared to — wait for it — being on a waitlist. 🤦🏻♂️ The abstract only describes “usual care” for the control group, but what is that a notoriously untreatable disease? Well, nothing of course!
And that is in fact what they got, as revealed in the full text.
And it’s a critical flaw, a cliché of amateur science: a failure to adequately “control” major confounders, also known as the whole point of doing a clinical trial. The paper title claims it is “controlled,” but it’s just not: the “usual care” waitlist design is a what-were-they-thinking choice.81 See that footnote for a full explanation of why this is a deal-breaker.
This paper’s conclusions are implausibly inflated in favour of stretching. If anything, the absence of a better result is damning.82
Clearly stretching is not much of a treatment for fibromyalgia. But by all means do it if it feels nice to you, or just use it like a light form of better-than-nothing exercise. And ideally do it with a dog or cat, so you can at least get some validation and compassion…

Dogs are a superb source of the validation and compassion that were probably the active ingredients in the Støve et al. experiment. A good dog will provide these while you stretch (sometimes while napping).
The next five sections are set aside for members only, about 15 minutes of extra reading (9% of the whole article). Two of the topics covered are also available in the trigger points and low back pain books. The locked topics are:
- Stretching for “trigger points”
- Stretching for back pain (especially the hamstrings)
- Maybe try less stretching for back pain
- Is stretching good for tendons? Can it align their fibres?
- Scratching your inner itch: a feel-good theory
Most PainScience.com content is free and always will be.? Membership unlocks extra content like this for USD $5/month, and includes much more:
Almost everything on PainScience.com is free, including most blog posts, hundreds of articles, and large parts of articles that have member-areas. Member areas typically contain content that is interesting but less essential — dorky digressions, and extra detail that any keen reader would enjoy, but which the average visitor can take or leave.
PainScience.com is 100% reader-supported by memberships, book sales, and donations. That’s what keep the lights on and allow me to publish everything else (without ads).
- → access to many members-only sections of articles +
And more coming. This is a new program as of late 2021. I have created twelve large members-only areas so far — about 40,000 words, a small book’s worth. Articles with large chunks of exclusive content are:
- Quite a Stretch
- Does Epsom Salt Work?
- Heat for Pain and Rehab
- Your Back Is Not Out of Alignment
- Trigger Point Doubts
- Does Fascia Matter?
- Anxiety & Chronic Pain
- Does Massage Therapy Work?
- Does Posture Matter?
- A Deep Dive into Delayed-Onset Muscle Soreness
- Does Ultrasound or Shockwave Therapy Work?
- A Painful Biological Glitch that Causes Pointless Inflammation
- Guide to Repetitive Strain Injuries
- Chronic, Subtle, Systemic Inflammation
- Vitamins, Minerals & Supplements for Pain & Healing
- Reviews of Pain Professions
- Articles with smaller members sections (more still being added):
- → audio versions of many articles +
There are audio versions of five classic, big PainSci articles, which are available to both members and e-boxed set customers, or on request for visually impaired visitors, email me. See the Audio page. ❐
I also started recording audio versions of some blog posts for members in early 2022. These are shorter, and will soon greatly outnumber the audio versions of the featured articles.
- → premium subscription to the PainSci Updates newsletter +Sign-up to get the salamander in your inbox, 0–3 posts per week, mostly short, sometimes huge. You can sign-up for free and get most of them; members get more and their own RSS feed. The blog has existed for well over a decade now, and there are over a thousand posts in the library. ❐

Change or cancel plans any time. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism. For more information, see the membership page. ❐
Stretching for “trigger points”

So called "trigger points" are common sore spots of uncertain in soft tissue. Could stretching ease them?
There is one kind of soreness that is common and might be responsive to stretching: the stiffness, aching, and tightness associated with the sensitive spots in muscle commonly known as “muscle knots” or trigger points.
The story goes like this: trigger points are isolated regions of contracted muscle fibres, basically micro cramps. If that’s how they actually work, then stretching might be a viable treatment method. Unfortunately, how they work is highly debatable, and basically unknown.
Stretching as a treatment for trigger points has some expert endorsements. In the weighty text Muscle Pain, researchers Dr. David Simons and Dr. Siegfried Mense wrote that stretching “by almost any means is beneficial.” This depends on a chain of assumptions and theories about how trigger points work: the micro-cramp is metabolically exhausting, like an engine revving in the red, producing waste metabolites that pollute and irritate the surrounding tissues, causing pain and more contraction. In theory, a trigger point cannot burn fuel if it is fully elongated, which would give the energy crisis a chance to abate — a vicious cycle breaker.
If they are right, then stretching works about the same way that stretching out a calf cramp works: you win the tug-of-war with spasming muscle, just on a smaller scale. This sounds great on paper, but there are several major problems in both theory and practice. Simons and Mense also emphasize that it has “not been firmly established” that stretching trigger points is helpful, and that stretch works primarily for “newly activated, single-muscle” trigger points … leaving out a lot of trigger points that are serious problems. There are many circumstances in which you cannot realistically hope to win a tug-of-war with a strong one, because it would be too anatomically awkward and/or too painful.
How can we pull apart a powerful contraction knot — a tiny segment of muscle fibres in full spasm — with anything less than pliers, a vice, and a glass of bourbon? We almost certainly do not have the leverage or pain tolerance required, especially if the muscle fights back with a defensive contraction (which may account for the cases that backfire). That trigger point is like a knot in a bungie cord: all we’re going to do is stretch the hell out of the bungie cord on either side of the knot. If it works at all, it probably mostly only works on the milder cases that don’t matter much in the first place.
And then there’s the possibility that Simons and Mense were just wrong, and a trigger point is not like a tiny cramp at all. If there is no metabolic “revving,” no energy crisis to interrupt by pulling muscle proteins apart like kids fighting on a playground, then it’s back to the drawing board: either stretching doesn’t work at all, or we just have no idea how it works. Which is possible.
This topic is covered in much greater detail (about 10x the length of this section) in my trigger points book.
Stretching for back pain (especially the hamstrings)
There are many common types of pain that stretching might be helpful for, but back pain is the 800-lb gorilla of musculoskeletal medicine, the most ferocious problem that many people face. If stretching wants to be known for being good for pain in general, it needs to be good for back pain.
And people do believe it is.83
But it’s both under studied and badly studied. I’ll do my best, but don’t expect much data-driven enlightenment on this topic — that data is just not good enough. For instance, the literature is littered with studies that seem “promising,” but don’t stand up to any scrutiny. Here are three telling examples:
- A 2010 experiment described in the Archives of Internal Medicine comparing yoga, a stretching class, and an educational booklet.84 This study has been widely reported as “stretching and yoga work,” rather than “stretching and yoga are equally damned here with faint praise.” Not only is it not persuasive, I think it backfires and convinces me that yoga/stretching really didn’t do much.
- In 2014, Chen et al. reported “significant” benefit for nurses with back pain who stretched three times per week after work for six months.85 The results are right in line with what people optimistically expect of a stretching habit: that it’s at least as good as popping ibuprofen. Isn’t it great when Science tells us what we already believe? Unfortunately, it’s a terrible study, so bad that I only cited this paper so I could point at it and laugh before pivoting to the disappointing reality.
- In 2019, Pourahmadi et al. reviewed 12 studies and reported happy news about “slump stretching” for back pain86 — similar to a seated toe-touch, with some technical refinements. This is a fine example of a not-so-positive-after-all test in two key ways. First, it’s not actually a muscle stretch, it’s literally spinal cord stretching (neurodynamic stretching), an obscure technique that most people know nothing about. Second, even if they did, the quality of the evidence here is “very low.” So it might work… but we have no way to know based on a few scraps of shabby data.
I am unaware of any study of this question that is actually promising. Meanwhile, there is plenty of actual “evidence of absence.” Three examples:
- In 2014, Sihawong et al. showed in a roundabout way that stretching doesn’t prevent back pain, even in people with poor trunk flexibility.87 They studied hundreds of office workers who had no back pain, yet, and followed them for a year while half of did exercises and half didn’t. Good design so far, but they also combined stretching with other kinds of exercise which almost certainly accounted for all the observed benefits.
- An interesting 2021 study compared stretching unfavourably to a more elaborate exercise therapy, “motor skills training.”88 Stretching lost (and so did strength training). Not by a lot, but it didn’t have to: even with unimpressive competition, stretching was not a contender.
- A good 2020 review of studies of exercise for back pain in British Journal of Sports Medicine concluded that stretching doesn’t work.89
That’s enough science of general stretching for back pain. Let’s get more specific now.
Stretching the hamstrings to treat back pain
Can you beat back pain can by stretching tight hamstrings? This is one of the most popular specific ideas about the therapeutic value of stretching. There are a handful of other stretching targets (quads, iliopsoas), but this is the big one — if it doesn’t hold up, we can largely ignore the rest.
The relevance of hamstring stretching to back pain is a bit sketchy (understatement). The fear is that tight hamstrings will make your lower spinal joints behave differently and, presumably, suffer greater strain, ultimately succumbing to painful degenerative changes. More simply put, “tight hamstrings cause arthritis!” Dumbed down to that, it sounds kind of ridiculous, but that’s what it boils down to.
Supposedly tight hamstrings lead to the kinds of changes that are well-known to be a poor explanation for most back pain, especially in younger people.90 You can’t make back pain with one ingredient any more than you can make a stew with just carrots.
This is not a difficult scientific question to answer in principle. We need only ask:
It’s hard to even identify people with tight hamstrings. There are several simple tests of hamstring flexibility, but they are notoriously unreliable, and there’s really only one method that should be used for research.93 How often has that method actually been used in research? You get a gold star if you guessed “almost never.”
A couple more interesting studies:
- The standing torture test — How long do you think you could stand before your back started to ache? Scientists asked 20 brave volunteers — healthy folks with good backs — to stand for two hours.94 (The inhumanity! Ban human testing!) Exactly half of these folks got back pain during the test. Their hamstring flexibility was measured before and after… and there was no correlation between tight hammies and succumbing to back pain while standing. Hmmm.
- Hamstring tightness and lumbar joint movement — Is there any connection between hamstring flexibility and the amount of lumbar movement when reaching forward? People sure think so, and they’d be right … but only if you’re talking about healthy people. Not so much in back pain patients! A 2010 study was so simple that the results are hard to argue with, even if it’s hard to know what they mean: some low back pain patients use their lumbar joints when they reach, others not so much, and good luck predicting which ones based on hamstring flexibility. You’ll fail if you try, this data says.95 The lack of correlation persisted even after recovery. The point? There’s definitely no clear evidence that lumbar joint movement is wonky in back pain patients with tight hamstrings. Which is really the only plausible mechanism by which it could cause trouble in the first place.
Marshall et al.:
With no relationship to actual disability and contradictory findings in the literature for the relationship of the hamstrings to the mechanics of the low back, it is unclear whether decreased hamstring extensibility should be targeted in rehabilitation programs for axial lower back pain.96
All this keeps me from getting excited about the potential of hamstrings or any other stretch target. But, unlike so many other alleged problems, most people can easily fix hamstring tightness. So you might as well! Just don’t waste a lot of time on it: a simple stretching program will work just fine.
Maybe try less stretching for back pain
This is 2020 email exchange, an interesting anecdote about how stretching for back pain can backfire:
Reader — I have had chronic back problems, dating back nearly 30 years. After my worst episode about 6 years ago, I did not recover well and continued to experience significant ongoing pains. I was significantly debilitated and paranoid about re-injuring myself. I saw several different healthcare professionals, and they all insisted on stretching, even though it was doing no good. PT’s, chiropractors, osteopaths, etc. So I stretched! I stretched a lot. it didn’t work. Long story short…
Me — Wow. I am horrified by how much advice you got to stretch. I correspond with so many genuinely expert people that I sometimes forget how much simplistic, old-school back pain care there is out there! How much were you stretching when you knocked it off and finally got some relief? How quickly did your back pain fade after you stopped stretching?
Reader — I was stretching a ridiculous amount, probably 20–30 minutes every day just to stretch (in addition to a bunch of other exercise). I didn’t log it, but I would say after a couple of months of no stretching, my symptoms were essentially nonexistent. Like anything else, it takes the body a while to adjust, including psychological adjustment after being brainwashed that you must stretch. I was very nervous about abandoning it, but I had tried everything else. It may have contributed to my early retirement. But I have not fully recovered, and there is virtually nothing I cannot do that I did as a younger man. I feel pretty damn good for 64!
Obviously there were other variables here, and it wasn’t necessarily stretching that was “causing” the back pain, or stretching-cessation that solved it. For instance, the easing of hypervigilance could have been a decisive factor. But I do think it’s safe to say that stretching wasn’t helping him! And that it was a waste of time at best. And at worst? The fearful faith in its necessity could well have been harmful.
Is stretching good for tendons? Can it align their fibres?
Muscle and tendon, although they are distinct tissues, blend together quite seamlessly. Much of what we think of as mucle is an extension of tendinous tissue, and vice versa. It’s impossible to draw a line where tendon stops and muscle starts, and if stretching doesn’t do much to muscles, it probably doesn’t do much to tendons either.
And so most likely a positive effect of stretching on tendons is minimal or nil. Digging a little deeper …
In general, tissues are stimulated to growth and repair by the same forces that they normally have to deal with (and also the same forces that occasionally overload and overwhelm them and cause overuse injury or trauma). That stimulus is dished up far more efficiently and thoroughly by normal (and athletic) activity than by any isolated deliberate exercise therapy.
Cells inside of tendons generate collagenous fibres and absorb others as needed in response to stresses, constantly remodelling and tweaking the tendon so that it is optimized to cope with the actual stresses it encounters all day, every day. (Organisms always act on the assumption that the immediate future will probably be similar to the immediate past — that doesn’t always work out, but it’s a pretty good rule of thumb.)
However, tendons are quite static compared to other tissues, and remodelling is slow and “conservative” — they don’t do it quickly. Even a very strong stretch to a tendon constitutes an extremely brief input of stimulus relative to the context of an entire day or week of normal usage of the tendon.
For comparison, consider how bone remodels — and bone is much more dynamic and responsive than tendons are. If bones are subjected to strong new stresses, they will change, slowly but steadily getting thicker and tougher in just the right way to cope with that stress. But it takes a lot! Now, how much do you suppose you could influence that process by deliberately applying a force to the bone? Even a heroic twenty-minute application per day — far more than anyone would ever bother stretching a single tendon, or pair of tendons? And even if it could work, what are the chances that the deliberate application of force would be a good enough “simulation” of natural biomechanical stresses that it would elicit the desired, relevant adaptation? A simulation might be good enough in principle in some cases, but it’s just not much like the stresses that the tendon actually has to deal with in the real world — and therefore it’s a fundamentally inefficient way of preparing for those stresses. If it works at all.
About alignment … the specific notion that tendon stretching will “align” its fibres is a particularly dubious and overly optimistic concept. Tendons are well nigh impervious, rupture only with extreme forces (and/or when already compromised), and change only in response to long term “just right” overloading. It’s relevant to understand that they are so tough that they are the strongest link in the chain, and in many cases they will tear away from their moorings on bone (avulsion fracture) before the “rope” breaks. For a mere stretch, collagen fibres don’t line up obediently any more than they already are — and tendons have impressively well-aligned microscopic orderliness to begin with.
It’s also important to keep in mind that study after study after study has shown no injury prevention benefit to stretching … and that includes tendon injuries. Tendons are not getting injured any less frequently in people who stretch a lot. If you want to reduce the chances of your tendons rupturing, then the way to do it is to expose them to a bunch of activities. Push the envelope just a little: enough that they are challenged, but not brutalized! Just the right amount of stimulation.

Scratching your inner itch: a feel-good theory
Is food an effective therapy because it tastes good?
Is music an effective therapy because it sounds good?
Essentially every pleasant sensation and experience has therapeutic qualities. These therapeutic qualities are not unimportant, but they’re not the same thing as an effective therapy. There’s a good reason why your physical therapist never prescribes ice cream. Here’s the last big stretching mystery I’d like to cover: how can stretching be so pleasant without (apparently) doing much measurable good? Look at this pattern:
- Stretching feels great … but it’s over-rated and nowhere near as medically or athletically useful as most people think.
- Massage feels even better … but its effects on pain are notoriously mild and fleeting.
- Chiropractic “adjustments” can feel scrumptious, even addictive, especially in that cinder-block-rigid area between the shoulder blades … but in most cases you’ll be craving a re-do before long (which makes for a lovely business model for chiropractors).
The pattern is that of being “relieved” instead of “fixed.” Over many years of thinking about pain and therapy, it has been a stubborn mystery to me why these things can feel so good — really, really good — without making any large or lasting difference to most painful problems, most of the time.
Feeling good without working all that well causes no end of confusion and trouble. Wonderful and profound sensations are largely responsible for an epidemic of excessive optimism about their healing powers. It’s understandable that we would expect something that feels that good to work well, but a lot of testing has shown over and over again that stretching, massage and chiropractic are not exactly saving the world from its aches and pains.
It’s not hard to explain how something might feel good without curing pain. Sex feels great, but it does not cure pain. Back scratches, chocolate cake, sunshine, and hot baths: all wonderful, all mostly powerless to cure pain.
But stretching is where the gap between how it feels and how well it works is the most glaring, the best feeling but most useless of “treatments.” I’ve already mentioned that I do stretch regularly because I like it, but that doesn’t quite cover it: I actually stretch for pleasure almost every single day. I’m as inflexible and prone to aches and pains as ever, and I’ve never been able to justify the habit with anything except, “Because it feels good, dammit.” And that’s fine.
But why does it feel that good? “It’s stimulating” just doesn’t cut it. I can give a specific reason why each of the delicious things above feel so good. But stretching? I just don’t get it.
And then one day — while I was stretching, of course — I had an epiphany: stretching doesn’t just feel like scratching an itch, maybe it’s actually scratching an itch. A deep itch. In my experience, stretching feels best when I am sore from working out — which only deepens the mystery. Why would it feel so pleasant to pull on soft tissues that are incredibly sore?
That soreness is like an internal “rash” or any skin irritation. And we feel an incredible compulsion to scratch rashes, mosquito bites and other itchy, irritated things. Consider the mosquito bite: scratching it is certainly not going to “treat” it, and we know it. But the temporary relief of scratching is so great it almost transcends pleasure and degenerates into a nasty compulsion. As many pleasures do.
Could it be that exercise-induced soreness is kind of like a minor internal “rash”? And that stretching is just about as close as we can get to “scratching” it? To get a little fleeting relief? This is the best analogy I’ve come up with yet to describe how stretching feels to me.
There may be many reasons why stretching feels good without being particularly helpful, but this makes some serious sense to me. It’s specific and plausible. It achieves the difficult trick of simultaneously accounting for both the unusually pleasant sensation and the more or less total lack of any meaningful effect. And it nicely fits the way I like stretch best when my muscles feel the worst. And it makes even more sense if you extend the metaphor of the itch to include the even more common sensations of being stuck or stagnant, which I’ve written about in the past (guest posting for Todd Hargrove’s excellent blog, see The Bamboo Cage).
I have often said that stretching and other relieving sensations of massage or spinal adjustment feel “like” scratching an itch. But I never went that extra step and considered that maybe they feel like that because, in a way, they actually are — because we can have genuine internal “itches,” vague sensory annoyances … and very limited and indirect ways of scratching them.
↑ MEMBERS-ONLY AREA ↑
Stretching does feel good, and maybe that is a kind of pain-killer

If stretching is mostly irrelevant to pain and injury, why is it that I feel like I have to stretch or I’m going to seize up like an old piece of leather? Why do I have this compulsion to stretch, and why does it feel so good, if it’s not actually doing anything? Why is this true for so many of us?
Because it is probably actually doing something! It’s just probably not doing what you thought it was doing. And we don’t really know for sure what it is doing. If we are intellectually honest, we simply have to admit that.
Although there are exceptions — discussed below in detail — most people report that stretching feels good, that it reduces muscle soreness, or that they feel a strong urge to stretch. And I’m one of them. I have a stretching habit because it feels good, and because it feels like I’m going to “seize up” if I don’t. In particular, I stretch my hamstrings regularly and strongly, and it feels as pleasantly essential to my well-being as slipping into a hot bath — but the exact nature of the benefits are completely unclear to me, and I suspect it’s about as medically useful as a back scratch.
It’s probably a stew of genuine but mysterious and subtle physiological benefits — like the heart rate regulatory effect noted in the last section — plus almost certainly some good placebo, too. I was raised on stretching. Despite my doubt about the conventional wisdom, I tend to emotionally “believe” in stretching just like everyone else — it’s deep in our culture, and, since stretching feels good, it’s easy for my mind to jump to the conclusion that it must be good. But of course that’s not really helpful at all — lots of things feel good without having any clear physiological benefits. Stretching might be like scratching: an undeniably strong impulse, but with almost no relevance to athletic performance or overall health.
I just don’t know. And based on the research to date, no one else does either.
If people believed that feeling good was the only thing that stretching was good for, most people — especially the athletes — would drop it from their exercise routine immediately. Most of us have better things to do. However, if someone firmly declared, “I stretch just to feel good,” I would applaud and say, “Hallelujah! That is an excellent reason to stretch! And one of the few that I can defend!”
And, then again, there may actually be real physiological benefits to stretching — just not the usual ones that get tossed around.
Stretching for contracture: Thumbs down to static stretching as a treatment for seizing up

Stretching for a pathological contracture like this case of Dupuytren’s contracture is futile. This is a great example of a “technical” reason to stretch that many or most people would assume to be effective, but is not.
“Contracture” is the unlovely process of muscle and other soft tissues seizing up in response to neurological problems or prolonged immobilization. Your face can’t really “freeze like that” as your mother warned you, but if you could make an ugly face long enough — weeks — eventually contracture really would set in. This is pathology, mind. The tissue changes. For the worse.
Most people probably assume that long, intense stretches must be an effective prevention/treatment for contracture, perhaps the only viable option. It is not an assumption held with much conviction, but stretching always gets the benefit of the doubt, whether it deserves it or not, and it seems to make sense that stretching would be a cure for contracture.
Common sense fails again. As it so often does. The Cochrane Collaboration published a review of static stretch for the treatment and prevention of contractures.97 The verdict? Thumbs way down. Based on “high quality evidence” they concluded that “stretch is not effective for the treatment and prevention of contractures.” I’m shocked. Shocked, I say!
Treatments are usually more obviously valuable to those who need them more. For example, the effect of acetaminophen is more obvious to someone with a headache. This very basic principle doesn’t always apply, but it usually does. This evidence shows that stretch does not meaningfully help even for a condition where the need for tissue elongation is dramatic.
So this is (yet another) great example of a “technical” reason to stretch that many or most people would assume to be effective. But no — probably not static stretch, anyway.98
Pathologically seized up tissue cannot be meaningfully elongated. So what’s happening when healthy people seem to get flexible?
Nerve stretching (neural mobilization, neurodynamics, nerve gliding, nerve flossing, etc)
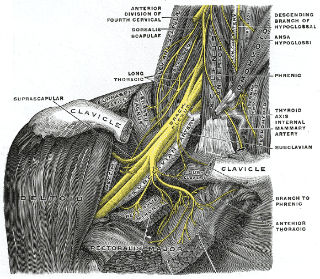
The goal of neurodynamic stretching is to stretch and stimulate nerve tissue specifically — not muscles.
Some pain is caused by physical interference with nerves — neuropathy. Neural mobilization or neurodynamics is a loose collection of experimental treatments for neuropathy based on the idea that physical stimulation through movement is good for unhappy nerve tissues.
But not just any movement! Only quite specific movements need apply. Particularly and specifically, movements that “slide” or “glide” nerves within their sheaths, perhaps breaking or preventing adhesions and stickiness between them.
This is a fine example of a (very) specialized type of stretching that could have genuine benefits for some patients. If it works, it would be an impressive partial vindication of therapeutic stretching.
But, of course no one actually knows if it works. It just hasn’t been studied well enough. It’s a tough thing to test — technical, messy, hard to standardize — and the science is threadbare.99
Subtle tunnel syndromes and the very hypothetical hope of treating minor aches and pains
One interesting possibility is that common subtle neuropathies are responsible for quite a lot of mostly trivial aches and pains. Some experts have proposed that these little micro nerve entrapments are actually the specific explanation for the “trigger point” phenomenon — humanity’s plague of unexplained sore spots.100 It is one possible explanation for why stretching might sometimes relieve pain… but inconsistently, because a lot of stretching would be the wrong kind of stretching.
Nerve tension and stretch tolerance
Hitting the natural and pathological limits of how far nerves can be pulled is one of the things that determines how intense a stretch feels. We may think we’ve stretched as far as we can not because we’ve hit the mechanical limit of the extensibility of our tissues, but because we’ve moved a nerve as far as it can be moved in its sheath. Nerve stretch may be what causes discomfort when you’re deep in a hard stretch, and it might be why some stretches are more unpleasant to hold than others.
For much more information about neurodynamics, see:
More reading related to stretching for pain
- Your Back Is Not Out of Alignment — Debunking the obsession with alignment, posture, and other biomechanical bogeymen as major causes of pain
- Does Posture Matter? — A detailed guide to posture and postural correction strategies (especially why none of it matters very much)
- Why Do Muscles Feel Stiff and Tight? — Maybe your range of motion is actually limited, or maybe it just feels that way
- A Deep Dive into Delayed-Onset Muscle Soreness — The biology & treatment of “muscle fever,” the deep muscle soreness that surges 24-48 hours after an unfamiliar workout intensity
- The Tyranny of Yoga and Meditation — Do you really need to try them? How much do they matter for recovery from conditions like low back pain?
- Strength Training for Pain & Injury Rehab — Why building muscle is easier, better, and more important than you thought, and its role in recovering from injuries and chronic pain
- Pain is Weird — Pain science reveals a volatile, misleading sensation that comes entirely from an overprotective brain, not our tissues
- The 3 Basic Types of Pain — Nociceptive, neuropathic, and “other” (and then some more)
- 38 Surprising Causes of Pain — Trying to understand pain when there is no obvious explanation
Part 4
Stretching for Flexibility
You can probably increase your flexibility by stretching, for whatever it’s worth… but what is it worth?

There is only one effect of stretching that seems to be almost completely uncontroversial: it does actually increase flexibility. Even plain old “static” stretching, and not even that much of it. Just applying tension to soft tissue will probably do the job.
The phenomenon is widely observed, and seems to have been confirmed by experiments. Many studies over many years have shown it in many ways.101 102 103 104 105
For whatever it’s worth. But what is it worth, exactly?
The American College of Sports Medicine believes that flexibility is “important in athletic performance (e.g. ballet, gymnastics) and in the ability to carry out activities of daily living.” It’s a “major component” of fitness, along with body composition, cardiovascular endurance, muscle endurance, and muscle strength. They recommend 2–3 days of stretching per week (2–4 repetitions of multiple stretches per day).106
Personal trainers sure buy into it. About 80% of American trainers prescribe static stretching — for all the reasons, but mainly for the flexibility.107
But when you try to spell out exactly why flexibility matters, it’s surprising how quickly things get a bit “um, er, well.” Obviously it’s helpful for some specialized needs — it’s the most important thing on every contortionist’s resumé. But not especially valuable to most athletes. Even many athletes who supposedly need extra flexibility. People love the idea of being flexible, but good luck defining specific benefits for most of them. Read on to watch me try and fail.
It’s possible, but how difficult is it?
Flexibility is not an easy achievement to unlock. It may depend on your genes. I really can’t seem to do it, for instance, which I established long ago with an intense personal experiment. Many other people feel defeated by the challenge as well. Here’s a story sent in by a reader who has been working on it for decades:
I have done yoga every day for more than 20 years. I’m really devoted to it. I do different sets of positions every 2 weeks, but I start my sessions every day with 5-10 minutes of breathing in simplified/easier lotus position (padmasana, where one foot is on the floor, and another is on top of the opposite thigh). It is still just as uncomfortable now as it was when I started. I can handle it for those 5-10 minutes, but more is just too hard. I can still do the full version, but only for a minute or so. One would hope after so many years, doing it daily, I would become more flexible! But not even a little bit — I do the yoga for other reasons.
Franjo M, California
However, for many people, a diligent effort over a period of weeks will probably increase your range of motion. How much of an effort? What “dosage” of stretching is required to get the flexibility effect you want? More on this shortly.
And how does flexibility work?
Once I’ve explored how difficult and pointless increasing flexibility is, I’ll wrap up one of the biggest controversies in stretching science: how the heck does flexibility increase anyway. It’s a matter of nearly pure intellectual curiosity and zero practical significance, but it is fascinating.
When someone increases their flexibility, what exactly changes? How does it work? Turns out flexibility is much more complicated than rocket science. It’s either plasticity or tolerance, or some combination, and it’s an argument that’s been raging for many years. Do we get flexible because tissues actually get physically longer, like pulling taffy? Or is it because we get used to the discomfort and “learn” to be longer, a sensory and neurological stupid-human-trick? Hint: never bet against neurology.
What does it take? Stretching dosage for flexibility: intensity, frequency, and duration
Beliefs about flexibility and the optimal means of stretching have often proceeded from assumptions that have never been tested and from an almost religious zeal regarding the perceived benefits of stretching by a few.
Flexibility, by William Sands, p. 389
Hold it right there! For how long exactly, though? And how often? How hard? What works best? Is five seconds of light stretch every other day for a couple weeks enough? Probably not. Or should it be five minutes of brutally yanking on your muscles three times a day for three months? That’s probably too much — even if it was definitely more effective, ain’t nobody got time for that. The bottom line:
- no one really knows
- a reasonable amount is probably good enough
- the returns probably diminish steadily as the dosage increases.
The battle of the experts
Here is a vivid example of how poorly understood this all is. This is an excerpt from one of the textbooks I used in school in the late 90s, a weighty and authoritative tome, a bible of therapeutic exercise (granted, out of date now, but this is the text I originally learned from):
Several authors have suggested that a period of 20 minutes or longer is necessary for a stretch to be effective and increase range of motion when a low-intensity prolonged mechanical stretch is used.
three citations listed, Therapeutic Exercise, 3rd Ed., Kisner/Colby, p157
Twenty minutes?! Almost no one is stretching for that long. No one’s recommending that. And yet “several authors” have found that it is “necessary”? Naturally that prescription is contradicted in other textbooks, by other experts, not to mention the fact that it’s extremely impractical. Imagine trying to stretch for injury prevention: 20 minutes for each of even just 10 important muscles would be more than three hours. Again, ain’t nobody got time for that.
The idea of a “correct” dosage (or any aspect of technique) is mostly a fantasy. And yet, somewhere between “not nearly enough” and “way too much” there is probably a sweet spot.
In practice, most people stretch only a small selection of tissues quite briefly, seconds only, and erratically. Only the most diligent of us can actually sustain a daily habit for long. We don’t know if that’s enough to achieve the goal. The evidence suggests that holding a stretch for 15 seconds is better than 5… but only a little bit.108
In 2011, a nicely done experiment by Marshall et al. showed that regular hamstring stretching substantially increased range of motion in normal university kids.109 Specifically, after “a 4-week stretching program consisting of 4 hamstring and hip stretches performed 5 times per week,” their range increased about 16˚ or 20%. That’s a real result from a sane stretching dosage.
But what if you’re not entirely sane? More extreme goals and methods deserve some focused attention…
Getting hard core: more extreme efforts undoubtedly do produce more extreme results
Acrobats, gymnasts, yogis, contortionists, and martial artists have clearly been pushing the limits for centuries, sometimes achieving uncanny mobility. But these are highly motivated athletes with specific and exotic performance goals and stretching regimens that would definitely intimidate the rest of us, and with good reason: they often injure themselves along the way. Indeed, it may even be necessary to injure joints — to traumatize their capsules and ligaments — in order to get them to move that far.
Even these unusual athletes are not chasing flexibility alone, and most athletes have much higher priority training goals. “Athletes usually don’t require extreme ranges of motion,” writes Todd Hargrove,110 “but rather extreme control at the end of relatively normal ranges of motion.”
Fitness and health are not equivalent. You can be fit for a particular athletic pursuit, but that doesn’t mean you are a healthier person: high performance in a narrow category often comes at great costs (such as joint stability). Flexibility is good for a few specialized tasks … and really not much else. It is obviously useful for gymnasts, for instance.

{kind=link}
Is this a good idea? This is an “oversplit.” Regularly doing this kind of thing will certainly make a person flexible … but not “healthy.” Photo of former Olympic gymnast Irina Tchachina.
There’s another photo like this that I cannot publish, unfortunately, showing a young girl gymnast doing the splits with a fat middle-aged coach literally sitting on her back. Is that young gymnast going to be more flexible? Oh, yes, I think she will be! Will she perform better? Not necessarily: she might be better off doing strength training at the limits of her range — which will not only increase her range, but improve her control at the limits of her range. Is she going to be “healthier” for it? Blatantly not. And she has a middle-aged guy sitting on her back!
Despite its reputation, ballistic stretching is not actually unsafe or even useless
A ballistic stretch is a bouncing stretch: you stretch up the end of your range (take up the “slack”), and then you “bounce” a little beyond that limit. Technically, you’re using momentum to repeatedly, briefly push into “overstretch” — stretching just past the end of your comfortable range of motion. That’s a bunch of words for something quite simple that people do almost unconsciously when stretching.
But, if you believe anything you read about it, overstretch sounds more dangerous than frayed-bungie-cord jumping.
Ballistic stretching is a notorious old-school type of dynamic stretching that is widely believed to be useless and risky — a belief that is rich with irony.
And how did it get that way when there is no compelling evidence or reason to believe that it’s dangerous?111 And when there actually is evidence that it’s just as good as static stretching for increasing flexibility?112113 It’s like the mirror image of a myth!
Many prominent sources warn people not to “bounce” your stretches, but none provide references, because (to the best of my knowledge) there simply are none to cite, no evidence at all that this style of stretching actually causes more injuries. One of the only relevant studies I have ever seen actually found that a large dose of ballistic stretching actually produced much less soreness than static stretching114 (and, yes, stretching can make you sore). All of these citationless warnings are prominent in Google search results in mid-2021:
- Healthline’s “Ballistic Stretching: Is It Safe?” says it “carries a risk of injury” and “generally not recommended.” Vague to the point of meaninglessness. No citations.
- The American Sports and Fitness Association has a blog post called The Dangers of Ballistic Stretching. “Today the very thought makes us cringe.” No citations, just their institutional authority.
- The American Academy of Orthopaedic Surgeons has a guide called “Warm Up, Cool Down and Be Flexible.” They say, “Do not bounce your stretches. Ballistic (bouncy) stretching can cause injury.” No citations — just their institutional authority.
- Well+Good publishes a page called “Stretch Pros Are Begging You To Never, Ever Do Ballistic Stretches—Here’s Why,” which reads: “Stay far, far away from ballistic stretches” seems to be the general consensus among stretch pros, who widely caution against the practice. No citations — just regurgitating expert opinions.
- ShareCare publishes three expert answers to the question, “Why is ballistic stretching bad?” No citations, and every answer is terrible, full of errors and misleading oversimplifications. I will zoom in on one of these next.
Ballistic stretching does not make muscle “fight back”
All three of the “expert” answers on ShareCare say that bouncing provokes reflexive, protective tightening of the muscle, thus “defeating the purpose.” This is incorrect. They are not expert. There is a grain of truth here, but only a grain: there is such a thing as a protective stretch reflex, but it primarily responds to rapid and unexpected stretch in the mid-range. (This is covered more below in the section about how flexibility works.) When you are voluntarily and trivial bouncing a few degrees out of your comfort zone, that’s nothing your body needs to freak out about, and it doesn’t.
I can’t cite an absence of evidence, but search PubMed and see for yourself. But we can easily infer from other evidence that it’s either not happening at all, or barely, or it doesn’t matter — because, as already noted, ballistic stretching increases flexibility just as well as static stretching. If muscles are fighting back, it isn’t getting in the way of the goal, and hitting that barrier is as harmless as the joint reaching it’s natural limits.
Defiant safety message
I know it all seems very “what could possibly go wrong?” Oh noes, you are pushing beyond your limits! Rapidly! In an “uncontrolled” way!
But I just don’t believe that any reasonably cautious person is going to hurt themselves stretching ballistically. “The dose makes the poison.” Too much of anything will hurt you, of course, and there isn’t an exercise in existence that people haven’t overdone. But no ordinary ballistic stretching intensity is hazardous enough to justify all the paranoia.
In fact, if anything, I suspect that some movement at the end of the range is a cautious thing: a way of testing and exploring how the end of the range feels, of generating more raw sensory data for your nervous system to work with.
The value of flexibility
“I want to be more flexible,” people say. Even when they have normal range of motion in every joint. What’s this about? Why are people so keen on being bendier? What is it you want to do with that super power?
There are several elastic superheroes. I think this speaks to our genuine craving for greater range of motion. We love that fantasy. But the reality is that hardly anyone actually needs to be more flexible. Most people have a normal range of motion — that’s why it’s normal! Unless you are specifically frustrated because you lack sufficient range of motion in a joint to perform a specific task, you probably don’t need to be more flexible.

What exactly are you planning to do with your flexibility?
Even abnormally poor flexibility is usually no big deal, as long as you are otherwise healthy. There aren’t many functional limitations caused by being super stiff that actually matter much. A couple examples:
- Toe touching is the ultimate in trivial flexibility goals. People can live their whole lives without being able to touch their toes without any practical consequences. Flexibility should only matter if it can help us do something that actually matters to us. For the martial artist, flexibility enables performance goals that martial artists care about! Great! But if a dude doesn’t care if he can touch his toes ... so what?
- Reaching bra hooks actually matters to women, but — unless something is truly wrong with that shoulder, like frozen shoulder — few women are so inflexible that it’s an issue. If it was a problem, they would certainly think it was well worth fixing — et voila, a job for stretching! But it’s both rare and easy to fix: it wouldn’t take much improvement in shoulder ROM.
For stretching with a flexibility goal to matter, we have to identify a common and meaningful functional limitation that can be overcome by increasing range of motion. There are lots of examples that are rare and trivial … or common and trivial … or rare and meaningful … but not both common and meaningful. And so the seemingly worthy goal of better ROM is actually quite marginalized — it doesn’t and shouldn’t matter to most people, most of the time.
If inflexibility is good enough for Eliud Kipchoge, it’s good enough for you. As of 2018, Mr. Kipchoge is the world’s fastest marathoner.115 But the man cannot touch his toes! This is an anecdote from someone who trained with him leading up to when he broke that record:
He was extremely inflexible. After an easy morning run (16km in 1hr10mins), I stretched with the group. Most of them were fairly flexible in the hamstrings (ie. standing straight legged and bending over to touch your toes with your knees straight and being able to touch your toes. Eliud was miles off). He was nowhere near touching his toes! They all found it hilarious that he couldn’t come close to touching his toes.
Matt Fox for SweatElite.co, “Training with Eliud Kipchoge – 5 Things That Surprised Me”
Flexibility and general health
When people have good aerobic capacity — when they are fit enough to efficiently distribute oxygen to all their cells — they are measurably more functional and healthier in all kinds of other ways too. If stretching is an important part of fitness, then it too should be linked to all kinds of other good stuff.
But it’s not. Stretching barely registers any effect on any measure of health and function. More flexible people do not die less or fall down less as they age. They don’t have clearly higher quality of life (a tough one to measure, but it’s been done). They don’t have less back pain or injuries, and in fact they may have more. They don’t have lower blood pressure, resting heart rate, cholesterol — those markers of fitness are much more strongly predicted by weight and endurance.116
Flexibility also isn’t linked to the other components of fitness: flexible people cannot lift more, run farther, or slip through narrower cracks. James Nuzzo: “Absence of correlations between flexibility and other fitness components indicates flexibility is a distinct trait, but not one particularly important for health and function.”
How does flexibility work?
What actually changes when we become more flexible? Almost everyone — especially non-experts, and that includes almost all clinicians — assumes that the tissue changes. The stuff that’s being stretched must change its properties: it must get longer, softer, more elastic. The muscles and tendons must be different. A few people add “fascia” for buzzword points.
Must this, must that. It sure seems like the tissue must change, but nothing is as obvious as it seems in musculoskeletal and sports medicine, and it’s probably more complicated. Even the stretching researchers and experts have oversimplified. There have been many ideas and many arguments. Here are some of the major specific candidates that have been explored over the years…
Viscoelastic transmogrification
Muscles are mostly liquid, and they act like it: they have properties of a liquid (“visco” for viscosity) and a solid (“elasticity”). Viscosity is a fluid’s resistance to changing shape depending on how quickly force is applied to it, while elasticity is how much and how fast a solid returns to normal after being deformed. The idea is that stretching tinkers with these variables.
Stretching may indeed change these properties, but only slightly and temporarily. Significant and lasting changes in viscoelasticity have not been observed.118
Change like a plastic
Connective tissue is tendons and fascia, the sheets of gristle that don’t just wrap muscles like a sausage-wrapping, but subdivide it into compartments, which are in turn subdivided. Every muscle is a honeycomb of fascia, and the stuff blends seamlessly into tendons at the ends of the muscle.
Plasticity is the mirror-image of elasticity: it’s the tendency of a solid to remain in a deformed shape, rather than snap back. We call it plasticity because plastics are the best well-known example a material that can be easily, permanently changed into a new stable shape. There are many different mechanisms for plasticity. And, yes, connective tissue has some plasticity — pull on it hard enough for long enough, you can definitely permanently change it, like pulling taffy.
But doing so usually involves either injury, or extreme patience and persistence — well beyond the reach of most stretching habits.
Connective tissue is a lot tougher than taffy. This is more like pulling steel cable. Like spider silk, many superlatives apply to the properties of connective tissue. The power to deform it in a reasonable time-frame, without injury, has never been convincingly demonstrated in an experiment.
Just add sarcomeres
Sarcomeres are the microscopic engines of muscle, the contractile “links” in the chain of a muscle fibre. It sounds kooky, but we know that animals do in fact grow new sarcomeres when muscle is immobilized in a lengthened position. Strange as it is, this certainly seems like a plausible mechanism for increasing flexibility.
There’s just several problems: The sarcomeres also shorten, so the overall length of the chain is maintained. The muscle also quickly loses the sarcomeres it gained. And sustained immobilization is extremely different from intermittent stretch, and not a very plausible source — but it’s also a hard thing to study (muscle biopsies are serious).
Reflexive relaxation
We have a reflex called the “stretch reflex” that kicks in to protect muscles from potentially dangerous elongation, such as you might experience while wrestling. Perhaps this reflex is partly what limits range of motion, and perhaps it can be trained to be less restrictive. Sounds reasonable, no?
But there’s no clear precedent for changing the sensitivity of any reflex — just try not to blink when you get a grain of sand in your eye.120 In any case, the stretch reflex doesn’t generally seem to kick in during slow stretch (no EMG activity at the end of range of motion). It primarily has a braking function: that is, it activates mainly when load is rapidly and significantly increased, something we need to do countless times per day as a part of normal activity. If the stretch reflex applied for a job controlling slow stretches, it wouldn’t get hired. But it’s complicated, and there is some contrary evidence.121
It’s the sensation, stupid! Stretching increases tolerance of stretching
The biomechanical properties of muscle do not seem to change with improvements in flexibility — which seems a bit nuts, and is a bit of a brain teaser. We have some well-established ways of measuring how a muscle responds to elongation, and it’s quite clear that those measurements do not change in people who improve their flexibility — they just go further.
Clearly something’s changing, but the tissue is not the only possibility. So what else is there?
The mind. Seriously.
Well, the brain — which doesn’t much care what your mind thinks. Brains decide when enough is enough, based on how the stretch feels. Your brain commands you to stop when it thinks the stretch is getting dangerous. And how does it enforce that? Inhibition of the muscles pulling you further into it — a kind of self-paralysis.
Yes, this is my second LoTR reference in one section. But who’s counting?
Your brain is the boss of you. The next section will dig deeper into how this actually works, and the evidence for it.
The case for sensory tolerance (and against it) in detail
In the last section, several possible ways that flexibility increases were explored and mostly dismissed, leaving only the sensory theory of flexibility. This is how Cynthia Weppler and S. Peter Magnusson explained it in their 2010 paper, framing it as the last theory standing:
Increases in muscle extensibility observed immediately after stretching and after short-term (3–8 week) stretching programs are due to an alteration of sensation only and not to an increase in muscle length. This theory is referred to as the sensory theory throughout this article because the change in subjects’ perception of sensation is the only current explanation for these results.
Note that phrasing, “the only current explanation.” That’s a Sherlock Holmesian way of putting it: “Once you eliminate the impossible, whatever remains, no matter how improbable, must be the truth.” It’s a strange, cool, and unexpected conclusion … but it also seems to be all we’ve got left, so we should probably take it seriously. And they do present considerable evidence supporting it. I’ll review some interesting highlights.
The wisdom of the body: why we can only stretch so far
Body is not stiff, mind is stiff.
K. Pattabhi Jois
If the sensory tolerance model of flexibility is correct, then it’s “just” the brain that sets the limits of our flexibility. A lot of tissue can probably be stretched much further than we think it can, but the brain decrees: you’re only going to lengthen your muscles so far, period, end of discussion. Any attempt to go further is simply shut down. It’s not a negotiation … at least not in the short term.
Your body probably has excellent reasons for strictly limiting elongation. When a stretch becomes uncomfortable, that’s your nervous system saying, “No way, sister, we don’t go there — we’ve got some sensible and firm safety rules about this.” The overprotective nervous system is a strong theme in neurology generally, and pain science particularly.)
And you can’t overrule your brain. Don’t make the mistake of thinking you could just blast through that barrier with will power. We humans do not control our own brains. Hell, we can barely keep our minds on a leash.122 But we do have some indirect influence, some levers we can pull on — quite literally in the case of stretching.
Stretching is a way of demonstrating to the brain that it’s safe to stretch a little further, just by getting used to the sensations. Familiarity breeds contempt. If your brain is concerned about you — and it always is, often more than you are — what better way to reassure it than to simply spend time at the edges of your range of motion, with nothing bad happening?
It appears that our brains can be tediously convinced to tolerate more elongation of soft tissue. To some degree.
Brain limits everywhere! Tolerance is not just for flexibility
Just as stretching has Team Tolerance, so does athletic performance in general. We are used to thinking in terms of being held back by a variety of physical limits: we can only run so far or jump so high because the spirit is willing, but the flesh is weak. The reality may be that the flesh is not as weak as we thought, that it’s often capable of doing more than we thought possible, and our spirit is irrelevant: it’s the brain that sets the limits.
What I have boiled down to a few words here, Alex Hutchinson explores for an entire book: Endure: Mind, body, and the curiously elastic limits of human performance.
The evidence is now extremely strong that brains play a major role in regulating our effort, progressively shutting us down — for our own good — as we approach the edges of what is safe, rather than what is possible. The brain uses all kinds of sensory cues and biological parameters — heat, thirst, pain — to keep us from exercising ourselves right off a cliff.123
There’s plenty of scientific controversy about this, and there has been ever since it emerged in the 1990s. But most experts accept that the only question is how much brains set limits.
If tolerance is a thing for several other aspects of performance, it probably is for flexibility too. It is part of a broad pattern of evidence converging on the potency of the brain in regulating almost everything.
Can tolerance explain extreme flexibility?
It’s probably a much better way to explain the feats of yogis and martial artists, whose hypermobility might well be dangerously dysfunctional if it were attributable mostly to plastic deformation. If you actually deformed your muscles and tendons enough to really pretzel yourself, they might get too long and loose to be useful and functional in general. Tolerance tidily accounts for how they can both allow extreme elongation, while retaining the ability to return to a normal, functional state. It sounds preferable.
Tolerance also doesn’t rule out the possibility of some plastic change at the extremes. More on this below.
Some interesting science experiments
In 2006, Folpp et al. did a nice simple experiment: they studied the effects of a month of daily 20-minute hamstring stretches in 20 people.124 The secret sauce was in exactly what they measured at the beginning and the end. They measured how far the hamstrings stretched with a specific force applied, and that barely budged: one degree more movement after a month of stretching. That doesn’t really sound worth it! But, adding more force, the subjects could tolerate eight degrees more stretch. So, to be clear, their hamstring muscles responded to the same force in exactly the same way despite lots of stretching. But if more force was applied, they could go eight degrees further than when they started.
Implication: their muscles didn’t change, but their tolerance did.
In 2014, Blazevich et al. tested calf stretching: several people stretched their calf muscles twice per day for three weeks.125 Each session consisted of 4 stretches of 30 seconds. They were compared to people who did not stretch. Measurements included changes in muscle and tendon mechanics, muscle activity, and spinal motoneuron excitability. The non-stretchers didn’t change, while stretch training “elicited a 19.9% increase in dorsiflexion range of motion (ROM) and a 28% increase in passive joint moment at end ROM.” However, the ROM improvement was not explained by changes in the muscle structure:
Increases in end ROM were underpinned by increases in maximum tolerable passive joint moment (stretch tolerance).
Here’s a neat trick: increasing the flexibility of muscles without even stretching them. If you do some upper body stretching, your lower body will get a little more flexible. Not much, but enough to measure in a controlled test.126 But that’s the only effect — which suggests that it’s due to an increase in tolerance of stretch, and that’s all. It’s one of many interesting clues suggesting that stretch tolerance is the secret sauce in flexibility.
And here’s a cool example of how increasing flexibility may be more of a nervous system “hack” than a matter of changing tissue: if you just add some vibration, even already flexible gymnasts can get a surprising boost in flexibility.127128129 Clearly that is a neurological effect on flexibility … and a very cool one. (Vibration is an interesting topic: see Vibration Therapies, from Massage Guns to Jacuzzis.)
This is not all the evidence, not by a long shot — but it’s certainly enough to establish that Team Tolerance isn’t just guessing.

Increased flexibility may simply be an increased tolerance for the discomfort of excessive muscle elongation.
Who disagrees? Team Plasticity strikes back (or just flails)
It seems unlikely that Weppler and Magnusson had the last word in 2010, although that paper seems well regarded. The sensory theory of flexibility has held up quite well, and it has many supporters. It is likely to be less wrong130 than anything else.
But Team Plasticity remains substantial and devout, and some of the objections are very “Oh yeah? Is not!” in character.
The next step up is to just cite our ignorance: there might be unconfirmed structural/behavioural changes in the muscle.131 It’s true, there could be — but we also know that there’s not much significant change in the extensibility of tissue to explain. It’s also unlikely that there is some mysterious property of muscle that makes it glow in the dark… because it does not glow in the dark.
The 2011 study of flexibility I cited above is good example of stubbornly defending plasticity in a more scholarly style. Marshall et al. clearly showed that stretching increases flexibility: when subjects were stretched with the same force (torque) applied, pushed to the same level of discomfort, they could go 20% farther.132 The data doesn’t say what changed,133 but the authors have a bad case of wishful thinking and followed their data into an overinterpretation, apparently trying to score points for Team Plasticity.134 Because range increased, but pain at the end of the range did not, they strangely concluded that a change in tolerance was not a factor. But stretching farther without hurting more is exactly what we’d expect to see with an increase in (neurological) tolerance. Although it wasn’t measured, it’s safe to assume the subjects’ pain would have been less if stretched only to the end of their original range. So their take just doesn’t make sense to me — it seems like a straightforward failure to understand the concept of sensory tolerance.
I see a lot of this kind of thing from Team Plasticity these days: weak arguments that seem to miss the point. But they are not completely without evidence to support their position. There’s not much, and it mainly seems to be from studies of hardcore stretching, but it’s something: changes in the physical properties of the tissue that we cannot explain. This is the best example I am aware of, and the only one that I consider to be a solid point against Team Tolerance:
Guissard and Duchateau observed lasting changes (a month) in torque/angle curves after five-weeks of calf stretching, five days per week, for 20 minutes135 — a huge dose compared to what is usually used in research and sports, but not necessarily unusual for rehab. We have no idea how the torque/angle curves changed, and all the candidates have major problems (see above). But change they did, and that’s a clear sign that something in that actual tissue was different.
Plasticity has almost been ruled out by a bunch of studies — here’s another fresh one136 — but not completely, and meanwhile neurological adaptation still hasn’t actually been confirmed. It just remains the best non-eliminated explanation.
This whatever-it-is can’t explain the changes observed from more typical stretching regimens. But of course it is possible that flexibility can increase in more than one way.
Part 5
Is stretching good for anything?
Responses to some common objections and ideas about stretching (and some of my own)
How about this? It’s good for your heart!137 “Enhanced vagal modulation.” That’s fairly straightforward good-news science about stretching. (And yet I’ve never heard anyone say they were stretching for heart health.)
It’s not surprising that movement would have some systemic regulatory effects, but it’s nice to see some corroboration of that common sensical notion, and it’s also nice to know that perhaps just stretching did this (to the extent we can learn anything from a single study). If true, it makes for a nice point in favour of a general stretching habit and yoga, “massaging with movement,” and probably even massage itself. It may have a lot to do with why massage feels good.
But stretching is probably not good for the reasons most people are stretching — not much good, anyway, and certainly not much in any ways anyone has figured out how to measure.
Undoubtedly, some specific stretching techniques are good for specific purposes … but quite different from the stretching goals that most people actually have in mind, if they have any clear goals at all. My concern is not that stretching itself is useless, but that people are stretching aimlessly and ineffectively, to the exclusion of evidence-based alternatives, such as a proper warm-up or mobilizations.
I don’t believe that stretching is any more generally useful for people than it is for cats — you do it when you get up in the morning for a few seconds and then you’re off to the sandbox. That feels good — it’s stimulating and enhances your body awareness, it scratches some simple physiological itch, and that’s fine and dandy. But for most people, most of the time? As a time-consuming therapeutic exercise ritual? Stretching simply has a lousy effort-to-reward ratio.
In the next few sections, I will respond to some of the common objections and questions that readers often have.
Stretching to … build muscle? It works, but there’s a catch
Yes, it’s true: stretching can make muscles bigger and stronger! Much like pumping iron, but without the pumping, or the iron.
You really have to be savage about it, though.
Since its recent discovery, this fun fact about stretching has made the rounds in social media quite a bit. And that resulted in the inevitable dumbing down and exploitation by people with a stake (financial or ideological) in making stretching sound as awesome as possible in every way, no matter what the science actually says. And so this odd little bit of physiology is getting widely used as fresh new justification for stretching as a “pillar of fitness” — like people weren't enthusiastic enough about stretching already!
But this isn’t a pillar that will be holding anything up for actual people, and probably not even elite athletes. Maybe a few obsessive-compulsive masochists?
Let’s dig into the stretching-as-strengthening science a bit…
Warneke et al. did indeed show that a large dosage of just stretching induced the same kinds of changes in muscle (hypertrophy) that we normally only expect to see from “lifting heavy things” (resistance training).138
Those results certainly are physiologically fascinating. They suggest that muscle adapts in more or less the same way to almost any kind of strong stimulus — not just exhausting it with contraction. Stress a muscle, and it will grow.
Neat, if true. Perhaps not greatly surprising, but neat. (It’s also meta-fascinating that we didn’t already know this: another good reminder that training and rehab science is still quite young in the big picture.)
How much stretching does it take to make a muscle bigger?
It may be neat, but it’s not very practical information, because the stretching protocol they used is just bonkers. For a single muscle, mind you…
- An hour per day?
- For six weeks?!
- At close to maximum stretch discomfort???!!!
Sheesh. Hard pass. Even half that intensity for half as long would still be an extremely impractical way to build any muscle. It would literally be a full-time job to do it for several of your biggest muscles.
Perhaps a more modest dosage of stretch would work? A similar study by Panidi et al. showed the same effect with less outrageous durations, but it was still impractical: “only” 9-15 uncomfortable minutes per muscle, per day, for three months.139 We’re down to a part-time job now, but “ain’t nobody got time for that.”
How about even less stretching? That is unlikely to achieve hypertrophy: a 2020 review by Nunes et al. concluded, based on review of several other studies, that lower-intensity stretch shows no clear sign of being able to get strengthening’s job done.140 It’s likely that it just requires an uncomfortable regimen.
•
This may be interesting physiology, but it’s a rather silly way to argue that stretching is healthy. Probably not one person in 10,000 has ever attempted that much stretching, let alone sustained it. And no one has ever taken up stretching because they thought it would build up their muscles, and it would be a fool’s errand if they did it now based on this news.
But now you know! Pull on a muscle hard enough and long enough, and your body will probably say, “Okay, fine, we’ll upgrade that a little.” Yahtzee.
Doesn't pandiculation demonstrate that stretching regulates physiology?
Pandiculation is the reflexive stretching that many animals do frequently when we rouse ourselves from rest or sleep. It routinely includes yawning, which can be thought of as “face pandiculation.” While pandiculation includes brief stretching, and can be considered a type of stretching, it is clearly not the stretching of our familiar fitness rituals: it’s a more complex and ephemeral mixture of contraction and stretching.
Perhaps the ubiquity of pandiculation validates stretching? Maybe it shows that stretching is physiologically important, even if it doesn't deliver the fitness and athletic benefits most people are aiming for. This hope rests on the general idea that pandiculation is “regulatory,” that it helps our bodies maintain homeostasis, and more specifically that it “resets” or “calibrates” muscle tone. This is plausible and interesting in itself, and in a way it would be surprising if a major animal behaviour was not regulatory in some way. Unfortunately, we have no evidence that confirms or illuminates it.
But even a rigorously and specifically validated “reset” phenomenon would not be much of a eureka. It would not necessarily follow that it has practical implications, that it would validate, enhance, or replace stretching, or inform manual or movement therapies — all of that is just self-serving speculation for alt-med professionals, who have always had a love affair with metaphors like “reset” and “release.” Pandiculation gets exploited to explain and justify highly speculative therapeutic techniques, and to boost reputations for being savvy about the wisdom of the body.
Without validation and clarification about the nature of the phenomenon — which we are unlikely to get — then pandiculation is definitely just a curiosity, no more (or less) interesting than yawning.
See
But doesn’t stretching have nifty benefits for general health, like decreasing arterial stiffness?
One the many well-measured benefits of aerobic exercise is softer arteries — reduced “arterial stiffness” — which is pretty much what it sounds like, and a fine and lovely thing. In contrast, resistance training may increase arterial stiffness. In 2020, Kato et al. published a meta-analysis of stretching exercises for arterial stiffness, showing that it too — just like aerobic exercise — can reduce arterial stiffness.141 🤯
Can you stretch this? A little, sure.
Stretching advocates danced in the streets.
Actually, not so much, because most stretching advocates have never even heard of this benefit. But when they do hear, they do get overexcited about how nicely it confirms their bias that stretching is a pillar of fitness. Checkmate, stretching skeptics!
There are a few other examples of physiological benefits like this, possible benefits of stretching that aren’t widely known, but are still destined to be cited by anyone trying to promote stretching with some footnotes (and there are plenty of those). Two key points apply to all them:
- Is it really a “stretching” benefit, or just a benefit of any exercise? Probably some other kinds of exercise, if not any exercises at all, can achieve the same thing … and maybe better.
- Even if true, obscure physiological benefits that no one even knows about just have nothing to do with debunking what people actually do believe about stretching. Stretching may well have some obscure benefits, but what doesn’t? I’m sure trampoline dodgeball, square dancing, and sumo wrestling all have some. That doesn’t make them pillars of fitness that everyone should be doing.
And another thing…
This particular evidence (Kato et al.) is actually just not very impressive. Meta-analysis is not magic, and it is only as good as the data that goes into it, and its conclusions can be just as flawed as any other kind of scientific paper. In this case, the abstract contains one of cardinal sins of research summary: declaring the results to be “significant” — meaning only statistically significant — without acknowledging low effect sizes. The effects of stretching here were detectable, but probably not important.
You clearly do not have to stretch to decrease your arterial stiffness. And stretching is very unlikely to be the best way to do it.
Don’t people just need to be taught how to stretch properly?
No one actually knows what a “proper” stretch is. There are no accepted standards in stretching technique (not even close), no method that is clearly superior, no way to know what’s right, no definition of success and no accepted method of achieving it.
The pretentious subtext of all preaching about stretching technique is always the same: stretching is only valuable if you “know what you’re doing.” And so a number of experts stay in business by advocating a stretching method or rationale that seems to trump all the others. Unfortunately, none of them can agree with each other.
The nice thing about standards is that there are so many of them to choose from.
Andrew S. Tanenbaum
Isn’t yoga all about stretching? And Yoga has lots of benefits, doesn’t it?
Yes, it is, and yes, it does — but probably not the benefits that people normally attribute to stretching. Even flexibility is suspect.142 Same with qigong, and the martial arts are full of stretching techniques — some of them appropriated from the modern Western fitness tradition, and others inherited from traditional practices. I advocate this kind of stretching elsewhere in my writings. So what’s the difference?
The difference is in intention. The intention of stretching in the context of good qigong, yoga or martial arts is to focus the mind, to stimulate vitality through a combination of mental and physical exercise. The intention is everything — without the intention, you might as well not bother with these activities.
Most westerners stretch without the foggiest notion of this underlying complexity. Stretching is generally stimulating to body awareness, of course: but that awareness is unsophisticated and incidental, rarely involving any insight more complex than “ooh, that muscle sure is sore.” Without education about intent — without a rich philosophical context — the value of stretching in yoga is just as uncertain as it is in any other situation.
And stretching in yoga also involves some risks. Too often people perceive yoga as an entirely wholesome and harmless activity, but in fact over-stretching injuries and muscle strains are actually common. As with dancing or martial arts, there are many ways to hurt yourself practicing yoga.
Stretching doesn’t always feel good: stretch syncope, malaise, and other collisions with pathology
Every time I’ve ever published anything that undermines bad beliefs about stretching — and there are plenty of those to undermine — I get a fresh batch of reactions like this:
“But stretching feels so good!”
And for as long as I’ve been writing about how stretching is not a pillar of fitness (since circa 2005), I have been softening the blow by acknowledging that, yes indeed, it really does feel good. Even great. That is one of the few stretching beliefs I can get behind.
But stretching does not feel good for everyone, and sometimes it can even feel bad. (And I don’t mean stretch injury — physical trauma, ripping tissue — although that is also a thing, discussed earlier. It is a more obvious thing! This section about a much less obvious kind of unpleasantness.)
Stretching just feels bland and pointless for some people, like no kind of itch is being scratched. If they bother stretching at all, it must be motivated by an abstract faith in the benefits (despite evidence to the contrary), because it doesn’t feel like it’s doing anything at all, good or bad. Emotionally that may be disappointing, frustrating, or tedious — because it doesn’t feel like it’s living up to the hype — but mostly just … boring.
I have heard from some people like that over the years. Not many; they are well outnumbered by the but-it-feels-good faction. But they exist.
And it can get worse than “boring”: imagine feeling queasy and lightheaded just because you stretched! Some people even faint.
Stretching and … fainting? Stretch syncope
“Stretch syncope” is real but truly rare. Some specific stretches — not just any kind of stretch — can collide with a rare physiological vulnerability to fainting, which may be a complete surprise to the individual (or something they have encountered before in other contexts).
The culprit in most documented cases is probably neck hyperextension, which can compress or stimulate the carotid sinus — a pressure-sensing spot in your neck that helps regulate blood pressure. This won’t happen to just anyone, or no one would ever do a yoga class. The carotid sinus has to be a bit twitchy for some reason — that’s the rare part. But when it is, and you stimulate it just so, it can trigger a reflex blood pressure drop. In many people, this probably just registers as a bit of lightheadedness. In some, it crosses over into nausea. It can freak people out, and I wouldn’t be surprised if it’s responsible for some panic attacks.
In the worst cases — in the unluckiest stretchers — the effect can cascade into presyncope (very woozy) or full syncope (out like a light).
(You can read a bunch about the carotid sinus in my article about the effect of massage on nerves, but it’s for members only because it’s nerdy extracurricular reading.)
This unpleasant nonsense is more common in people with orthostatic intolerance. [Wikipedia] There are many kinds of OI, but it is often associated with chronic unexplained illness and pain, especially the POTS sub-type (postural orthostatic tachycardia syndrome, characterized by a racing heart upon standing up). Although stretch syncope is rare, it’s probably less rare in the people using stretch to try to relieve their aches and pains.
This is less about “stretching can make you faint” and more about a perfect storm: a just-wrong posture combined with an exotic sensitivity, in someone whose autonomic regulation may already be a bit glitchy. It’s a “stupid human trick,” an edge case in a system that mostly works fine.
Unpleasant stretch has many other possible explanations
- Habitually holding your breath while stretching probably won’t cause serious symptoms, but it might make stretching feel less pleasant. And it’s probably common. Just ask a yoga instructor how often they need to remind people to breathe!
- The pleasantness of stretch can be undermined by simple overexertion. Sometimes stretching involves quite strongly held positions, especially in a yoga context, and it is piling more exercise onto a body that is already a bit worn out and run down, maybe quite sore or even borderline injured.
- Any physical activity can collide with the transient vague malaise of mild infections (mostly colds and flus that never develop clear symptoms). This would be a passing, occasional thing, but also probably quite common.
- There are many underdiagnosed health problems that reduce the resilience and increase the sensitivity of muscle and connective tissue or otherwise cause non-obvious vulnerability. For instance, some people are just too sore, always or often, due to common illnesses that cause chronic widespread pain, like fibromyalgia and Ehlers–Danlos syndrome. Many people with these conditions do like stretch, and even find it helpful — but not all.
- Many chronic health conditions also involve malaise and weakness, and stretch or common stretching positions and movements can be a trigger. For instance, POTS seems to be a component of many chronic health conditions, and could be set off just by the getting up and down (no carotid sinus trigger).
- The most serious pathology that can collide with a common stretch position is upper cervical instability, caused by trauma and a variety of diseases of the joints at the top of the spine, which can be subtle yet serious. The only symptom of erratic irritation of the spinal cord and brainstem might be vague episodes of malaise. This is not as rare as you’d think. More dire cases are rare, but they do exist, and — weirdly — still often go undiagnosed, simply because the trigger is not obvious.
- “Exercise intolerance” is exhaustion and malaise triggered by exercise. It comes standard with ME/CFS, and is also linked to several other chronic conditions. I suffer from this: I get bizarrely nauseous when I exercise my muscles strongly (resistance training). Although stretching is not a known trigger for exercise intolerance, it’s not implausible. Stretching is a kind of exercise, and we already know that other kinds of muscle stimulation can go badly …
- Even seemingly healthy people can feel a bit off after a massage: post-massage soreness and malaise, or PMSM, a weird phenomenon. Whatever it is, it could be triggered by any stimulation of muscle, either massage or stretch, making it seem like a kind of exercise intolerance. Muscle tissue is biologically lively and well-integrated into the whole system. For instance, it’s an “endocrine organ” — it produces hormones when stimulated. That’s mostly a good thing (anti-inflammatory), but maybe not in all physiological circumstances. If massage can trigger PMSM without any obvious illness in the picture, then stretching might too — but it seems even likelier if there is a chronic illness, even if it’s undiagnosed and mild. Personally, I would bet that there’s some kind of undetected vulnerability in every case, even if it’s just a weird genetic quirk with no other practical consequences.
There are a lot of ways to hurt and feel bad, and “everyone is different” is an understatement.
So stretching is good for … stretching?
We already know that stretching does not do all the basic stuff we used to hope it was doing, especially injury prevention. Is it good for anything else?
There is no known benefit to greater flexibility, except for:
- bragging rights
- dominating Twister tournaments
- making full use of Indian love manuals
In short, stretching appears to be good for … more stretching. Oh, and of course:
- yes, stretching does feel pleasant
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Part 6
Appendices
More reading
- A Stretching Experiment — What happens when you stretch your hamstrings intensely for several minutes a day in a steam room?
- The Unstretchables — Eleven muscles you can’t actually stretch hard (but wish you could)
- Stretching Injury — How I almost ripped my own head off! A cautionary tale about the risks of injury while stretching
- Cramps, Spasms, Tremors & Twitches — The biology and treatment of unwanted muscle contractions
- Sports Injury Prevention Tips — A few evidence-based ways to reduce your risk of injury
- Mobilize! — Dynamic joint mobility drills are an alternative to stretching, a way to “massage with movement”
- Basic Self-Massage Tips for Myofascial Trigger Points — Learn how to massage your own trigger points (muscle knots)
- IT Band Stretching Does Not Work — Stretching the iliotibial band is a popular idea, but it’s very hard to do it right, and it’s probably not worth it
- Some other articles that critically examine popular ideas about health: Does Epsom Salt Work? and Water Fever and the Fear of Chronic Dehydration and Does Posture Matter?
Other interesting reading relevant to stretching:
- “Stretching ‘fails to stop muscle injury’,” News.BBC.co.uk.
- “Reducing risk of injury due to exercise: Stretching before exercise does not help”. This is a superb British Medical Journal editorial, which adds about fifty kilos of credibility to this article.
- “Effects of stretching before and after exercising on muscle soreness and risk of injury: systematic review”. This is the much more technical article, to which the editorial mentioned above is referring.
- “Stretching before exercise: an evidence based approach”. Another more technical article, but also excellent and heavily referenced.
- Published since this, my article A Deep Dive into Delayed-Onset Muscle Soreness — The biology & treatment of “muscle fever,” the deep muscle soreness that surges 24-48 hours after an unfamiliar workout intensity covers the subject of preventing DOMS more thoroughly.
What’s new in this article?
This article had a long history of unlogged updates — a decade or so — before I finally started logging them in 2015. Updates shown here are the most recent only.
Jun 26, 2026 — New section: No notes. Just a new chapter. [Updated section: Stretching for fibromyalgia.]
June — New section: Major new exploration of an under-rated category of rare but notable stretching hazards for some people. [Updated section: Stretching doesn’t always feel good: stretch syncope, malaise, and other collisions with pathology.]
June — Tune-up: A minor update integrating this section with the new chapter about more exotic kinds of stretching harms. [Updated section: Ackshually, stretching can cause injuries (and other harms).]
February — Added nuance: Added minor but overdue note about opportunity cost and how “every little bit helps” is often wrong. Also added a curious anecdote about a reader who thinks stretch does not feel good for anyone. [Updated section: Introduction.]
February — Science update: Cited Warneke et al. for broad general support for the thesis of this article. [Updated section: Introduction.]
2024 — New : Substantial new sidebar, “Reciprocal inhibition invalidated,” about how a major premise for “advanced” PNF stretching was largely disproven in 2009. [Updated section: This isn’t just about static stretching! Types of stretching.]
2024 — Revised intro: Thoroughly re-wrote the introduction and summaries (which are often used when the article is cited by other articles). It’s amazing to me that I can re-visit one of my oldest and most polished articles and immediately find many ways to improve it! Revising introdutions and summaries isn't all that significant for readers, at least not consciously, but it is an art form unto itself — it takes a great deal of thoughtful work to capture as many key points as possible from the body of the article and compress them as much as possible.
2023 — New section: No notes. Just a new chapter. [Updated section: Stretching to … build muscle? It works, but there’s a catch.]
2023 — Science update: Identified some non-trivial flaws in a trial that dared to challenge my bias. 😜 [Updated section: Reason #3: Stretching to prevent injury.]
2023 — New section: No notes. Just a new chapter. [Updated section: But doesn’t stretching have nifty benefits for general health, like decreasing arterial stiffness?]
2023 — Added a pop quiz: Fun, right? [Updated section: Is stretching good for anything?: Responses to some common objections and ideas about stretching (and some of my own).]
2023 — Science update: Updated and added some citations, including one that challenges my bias (for the first time). [Updated section: Reason #3: Stretching to prevent injury.]
2023 — New section: No notes. Just a new chapter. [Updated section: Doesn't pandiculation demonstrate that stretching regulates physiology?]
2021 — New section: No notes. Just a new chapter. [Updated section: Cramp first aid: at least one undeniable stretching benefit.]
2021 — Rebooted: Over the last couple weeks, this article has been upgraded and expanded in many ways. It is now about 33,000 words long, which gives it the dubious distinction of being the first PainSci article to match the length of the shortest PainSci book. Henceforth, I will call this page a “book.”
Archived updates — All updates, including 31 older updates, are listed on another page. ❐
Notes
- Warneke K, Thomas E, Blazevich AJ, et al. Practical recommendations on stretching exercise: A Delphi consensus statement of international research experts. J Sport Health Sci. 2025 Dec;14:101067. PubMed 40513717 ❐ PainSci Bibliography 49373 ❐
There’s lots more science coming on many specific points, but this is by far the best recent single citation to show this whole article is generally in tune with the scientific consensus. Twenty stretching experts pooled their expertise for this ambitious consensus paper. It’s not a “scientific review,” exactly: it formalizes expert opinion of existing reviews, which is more clinically useful, more practical and broader in scope than a scientific review (but also less rigorous on any specific point). The clickbait headline for it would be “The Great Stretching Myth: 20 Scientists Reveal What Actually Works — and What Doesn’t.” And it doesn’t work for much.
- As detailed as this article is, it’s an article about stretching, not flexibility, so I don’t go into any detail about how strength training can improve flexibility. But it does! My colleague Nick Ng does go into detail about that: see How to Become Flexible With Strength Training.
- Poor posture is a minor factor in pain and injury, but gets far too much attention in physical therapy and rehab. Many habitual postures are adaptations to anatomical quirks that can’t be changed. Most other “poor posture” is just coping with bad ergonomics. “Posturology” is mostly misguided pseudoscience. When people seem to be vulnerable to postural stresses, the vulnerability is usually the problem. For more information, see Does Posture Matter? A detailed guide to posture and postural correction strategies (especially why none of it matters very much).
- “Every little bit helps” is sometimes a little bit true, but more often those little bits are just a waste of time we can ill afford. Low-value treatments and over-optimization of health and wellness have an opportunity cost [Wikipedia] — exactly like the non-physical harms of tame snake oils that still waste time/money/attention that people actually need for other things in life.
After twenty years of hearing literally hundreds, probably thousands of “but it feels good!” comments from readers, in 2026 someone on social media piped up with this surprising take:
“It’s an odd statement to say stretching ‘feels good.’ Stretching is quite painful!”
When I pushed back and explained my long exposure to the clear majority view, she doubled down, insisting that “it’s 100% news to me if there are people out there who don’t find that sensation to be one of mild to moderate pain.” Okaaaay. Not sure what world she’s living in! 🤔 Probably the world where many people are empathy-impaired and think struggle to imagine other people having different experiences. But usually that cuts the other way: it’s the people who love stretch who struggle to believe that some people don’t.
It’s important for us to recognize that there are people who feel underwhelmed, irritated, or even worse when they stretch. In many cases, it may be uncomfortable for pathological reasons, and in rare circumstances it can cause fainting, nausea, malaise: see below for more information.
- There are many examples — expert criticism of stretching dates back decades now — but here’s a good new one from 2022: Jonathan Jarry, writing for the McGill Office for Science and Society:
“I traipse into this minefield, fully aware that this is hallowed ground. People, after all, do not like their stretches to be criticized.”
I am proud to be quoted here. Jonathan definitely did not just “take my word for it” — he really vetted the key concepts and claims, greatly increasing the value of his endorsement of my writing on the topic.
Fortunately, he had other excellent sources to lean on. This isn’t like the early 2000s! Back in those days, mostly all I could do was point to the absence of evidence for major claims … and to the stink of wishful thinking and faith-based fitness. But these days? There’s much more data and skepticism from highly credible and credentialled experts.
- Nuzzo JL. The Case for Retiring Flexibility as a Major Component of Physical Fitness. Sports Med. 2020 May;50(5):853–870. PubMed 31845202 ❐
This is the first of many citations in this article, but it’s also one of the best and most general, and highly recommended reading for professionals. It is like a more scholarly and formal version of this article.
- Some readers will sniff at this and say that CR is still not “advanced” stretching, but it is certainly still widely used, taught, and touted as being better than humble static stretching. I see trainers using it at the gym all the time. Patients can go for physical therapy pretty much anywhere in the world, and there’s a good chance the therapist will do a whole bunch of CR stretching with them, while charging about a buck a minute.
- Azevedo DC, Melo RM, Alves Corrêa RV, Chalmers G. Uninvolved versus target muscle contraction during contract: relax proprioceptive neuromuscular facilitation stretching. Phys Ther Sport. 2011 Aug;12(3):117–21. PubMed 21802037 ❐
This well-planned experiment tested whether or not the contraction component of a contract-relax stretch actually makes a difference, and clearly found that it does not. The researchers compared a normal CR stretch of the hamstring to a modified one without any hamstring contraction (instead, some other “uninvolved, distant” muscle was contracted). The effect of both stretches was the same — “a significant moderate increase in range of motion.” In other words, it didn’t matter if the hamstring was contracted or not — with or without a contraction, the result was the same. This strongly undermines the central claim of CR-PNF stretching.
This is the only trial I’ll cite on this topic; the other two citations are both reviews.
- Hill KJ, Robinson KP, Cuchna JW, Hoch MC. Immediate Effects of Proprioceptive Neuromuscular Facilitation Stretching Programs Compared With Passive Stretching Programs for Hamstring Flexibility: A Critically Appraised Topic. J Sport Rehabil. 2017 Nov;26(6):567–572. PubMed 27632820 ❐ Based on just five eligible studies out of 195, this review concluded that there were “consistent findings from multiple low-quality studies that indicate there is no difference…when comparing proprioceptive neuromuscular facilitation [contract-relax] stretching programs to static stretching programs.” Clearly the evidence is limited, but if there is a signal in that mess, it’s awfully weak. The studies they reviewed are almost certainly being produced by people bias in favour of PNF, and yet they still found nothing despite that bias (which inevitably warps studies in subtle ways).
- Lempke L, Wilkinson R, Murray C, Stanek J. The Effectiveness of PNF Versus Static Stretching on Increasing Hip-Flexion Range of Motion. J Sport Rehabil. 2018 May;27(3):289–294. PubMed 28182516 ❐ Another review of just five studies of PNF stretching. In one study, PNF produced better results; in the other four, there was no significant difference. The authors concluded that “both static and PNF stretching effectively increase ROM; however, one does not appear to be more effective than the other.”
- Osternig LR, Robertson R, Troxel R, Hansen P. Muscle activation during proprioceptive neuromuscular facilitation (PNF) stretching techniques. Am J Phys Med. 1987 Oct;66(5):298–307. PubMed 3434629 ❐
- Condon SM, Hutton RS. Soleus muscle electromyographic activity and ankle dorsiflexion range of motion during four stretching procedures. Phys Ther. 1987 Jan;67(1):24–30. PubMed 3797473 ❐
- Etnyre BR, Abraham LD. Antagonist muscle activity during stretching: a paradox re-assessed. Med Sci Sports Exerc. 1988 Jun;20(3):285–9. PubMed 3386509 ❐
This experiment was an early test of the hypothesis of reciprocal inhibition, a key premise of proprioceptive neuromuscular facilitation. They seemed to confirm the phenomenon using wire EMG (electrodes embedded in the muscle), as opposed to skin electrodes, concluding/speculating that the negative results of other tests (like Osternig and Condon) were probably caused by the imprecise superficial electrodes. However, this conclusion was probably definitively contradicted probably definitively by a better experiment conducted by Mitchell in 2009.
- Mitchell UH, Myrer JW, Hopkins JT, et al. Neurophysiological reflex mechanisms' lack of contribution to the success of PNF stretches. J Sport Rehabil. 2009 Aug;18(3):343–57. PubMed 19827499 ❐
This 2009 experiment probably definitively invalidated the phenomena of antagonist inhibition and autogenic inhibition, contradicting Etnyre et al.’s 1988 result, which had been the most credible evidence pointing the other way, but confirming a variety of other early experiments (like Osternig et al. and Condon et al.).
They studied eighteen adult subjects doing proprioceptive neuromuscular facilitation (PNF) stretches, collecting EMG from the medial hamstring muscles via both surface and indwelling wire electrodes.
Not only was “reciprocal inhibition was not evident,” but they found an “elevated rather than an inhibited EMG during the antagonist contraction, possibly representing co-contraction.” They also could not detect autogenic inhibition (relaxation after contraction in the same muscle), and again the result was actually the opposite: EMG values were “higher than baseline.”
“Previous neurophysiological explanations for mechanisms of PNF stretching appear to be inadequate,” they concluded. “This study corroborates previous findings that a muscle’s tone increases during its antagonist’s contraction. Other explanations should be considered regarding the mechanism for the effectiveness of the CRAC and CR PNF techniques in a nonneurologically impaired population.”
- “Controversial”? That was sarcasm. It is not actually controversial that “anatomy has limits.” But you wouldn’t know it from the contents of my inbox. I never would have thought so until I published this idea. But countless readers have written to explain to me that, apparently, they can stretch whatever they want as far as they want, and it’s only my mind that’s limited.
- Other major examples include: masseter and temporalis, the suboccipitals, the thoracic paraspinals, latissimus dorsi, the gluteals, the foot arch muscles, and the IT band (of IT band syndrome fame). Some of these muscles can, sort of, be stretched. But all of them are limited to a moderate intensity stretch at best (e.g., the gluteals), in most people, most of the time, using reasonably accessible methods.
- I spent a decade in clinical practice as a massage therapist, routinely asking my patients about their stretching beliefs and habits, among many other things. These days I am a full-time writer on these topics with a global audience, so I hear vastly more about stretching from readers by email than I ever heard from my patients back in the day. I have a great bird’s eye view of popular opinions about stretch. Professionals send me a lot of mail as well, so I get a lot of exposure to their opinions. Are they more educated about stretch? You’d sure hope so, but that hasn’t really been my impression, to be honest — it really seems like everyone is just repeating things they heard other people say. Professionals just hear and repeat even more.
- More evidence on this is coming, but meanwhile there’s an interesting general principle at work here that is worth pointing out: these goals are proven to be impossible either straightforwardly by an evidence of absence, or less obviously but almost as certainly by a preponderance of evidence of minor efficacy. Proof of the existence of a trivial benefit damns with faint praise, and proving that something barely works is literally almost the same as proving that it doesn’t work at all. This is a chronic problem with many allegedly effective treatments and therapies: they may work a little, but they fail to impress. Stretching suffers from this problem in spades.
- Kay AD, Blazevich AJ. Effect of Acute Static Stretch on Maximal Muscle Performance: A Systematic Review. Med Sci Sports Exerc. 2011 Jun 8. PubMed 21659901 ❐ Researchers looked at more than 4500 studies before choosing about 100 to look at more carefully. They found “overwhelming evidence” of “no significant effect,” and that is certainly no surprise for anyone who had been watching stretching science over the years.
- Soligard T, Myklebust G, Steffen K, et al. Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. BMJ. 2008;337:a2469. PubMed 19066253 ❐ PainSci Bibliography 56160 ❐ In 2008, Norwegian researchers compared injuries in over a thousand female footballers who participated in such a warmup for a season, to another several hundred who didn’t. The athletes with the warmup had fewer traumatic injuries, fewer overuse injuries, and the injuries they did have were less severe. Static stretching was not part of the warmup. “Active stretching” was … but “active stretching” is what I would call “mobilizations” — doing moving lunges, for instance — as opposed to the kind of static or passive stretching that most people think of when they think of stretching.
- Soligard T, Nilstad A, Steffen K, et al. Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Br J Sports Med. 2010 Sep;44(11):787–93. PubMed 20551159 ❐ PainSci Bibliography 54998 ❐
Researchers found that injury rates were significantly lower in soccer (football) teams that diligently performed warmup exercises (“The 11+”, a warmup program recommended by FIFA, which notably does not include stretching). On the one hand, there was not much difference between a little warming up (low participation) and a bit more warming up (average participation). But players and teams that did an especially good job of warming up (“twice as many injury prevention sessions”) got solid results: “the risk of overall and acute injuries was reduced by more than a third among players with high compliance compared with players with intermediate compliance.” That extra enthusiasm went a long way!
- Bizzini, M. Junge, A and Dvorak, J. The 11+ Manual: A Complete warm-up programme to prevent injuries. FIFA Medical Assessment & Research Centre. Publication date unknown. Accessed 2021-05-08; no longer available in 2023. The 11+ warmup does include some “active stretching,” but not much. It also includes this specific clarification: “Why does the 11+ not include stretching exercises? Research has shown that static stretching exercises have a negative influence on muscle performance [more on this soon], and results on the preventive effect of dynamic stretching are inconclusive [more conclusive these days!]. Stretching exercises are not recommended as part of a warm-up programm…”
- Ultimate is a Frisbee team sport, co-ed and self-refereed, with soccer-like intensity and usually the vibe of a good party. Players tend to be jock-nerd hybrids: lots of engineers and scientists. Hippies invented the sport, but have mostly been displaced, and the sport is now relatively mainstream and there’s a pro ultimate league. I’ve been playing since 1997.
A related example
When I was studying to become a massage therapist, our most scientifically literate instructor dared to share a recent research paper with the class (something no other instructor ever did, which is an ugly truth about my training). The study suggested that massage therapy has no effect on the phenomenon of delayed-onset muscle soreness (Tiidus). This was heretical! Most of the class reacted angrily to this attempt to tip over one of the sacred cows of massage therapy, and the hapless instructor was nearly shouted out of the classroom.
What amazed me most about that was that the belief the students were defending was new to them, based only on what they’d heard from instructors in their first year of classes. And yet it was already essential to their self-image as budding health professionals, a “fact” that they planned to use to promote their services someday. It doesn’t take much for dogma to settle in!
This incident made quite an impression on me, and is partly responsible for my own journey from credulity to skepticism.
- Berrueta L, Muskaj I, Olenich S, et al. Stretching Impacts Inflammation Resolution in Connective Tissue. J Cell Physiol. 2016 Jul;231(7):1621–7. PubMed 26588184 ❐ PainSci Bibliography 52915 ❐
In a previous experiment, these researchers claim to have found evidence that stretching successfully treated inflammation and pain in rats. In this follow-up experiment, they looked more closely at the biology, measuring markers of inflammation: inflammatory lesion thickness, neutrophil count, resolvin (RvD1) concentration. They believe this shows a “direct mechanical impact of stretching on inflammation-regulation mechanisms within connective tissue.” It’s intriguing science for sure, but replication in humans is needed before we get too excited about it.
- Pedersen BK. The anti-inflammatory effect of exercise: its role in diabetes and cardiovascular disease control. Essays Biochem. 2006;42:105–17. PubMed 17144883 ❐
- It’s just one study. We don’t actually know that what Berrueta et al. found is for real, and we won’t know until it has been replicated. More importantly, this was a demonstration of an effect on connective tissue, not muscle — and while muscle is full of connective tissue, DOMS is much more of an issue with muscle than connective tissue, and it is far from guaranteed that an effect on connective tissue has anything to do with DOMS.
- Lund H, et al. The effect of passive stretching on delayed onset muscle soreness, and other detrimental effects following eccentric exercise. Scand J Med Sci Sports. 1998 Aug;8(4):216–21. PubMed 9764443 ❐
From the abstract: “There was no difference in the reported variables between experiments one and two. It is concluded that passive stretching did not have any significant influence on increased plasma-CK, muscle pain, muscle strength and the PCr/P(i) ratio, indicating that passive stretching after eccentric exercise cannot prevent secondary pathological alterations.”
- Cheung K, Hume P, Maxwell L. Delayed onset muscle soreness: treatment strategies and performance factors. Sports Med. 2003;33(2):145–64. PubMed 12617692 ❐
From the abstract: “Cryotherapy, stretching, homeopathy, ultrasound and electrical current modalities have demonstrated no effect on the alleviation of muscle soreness or other DOMS symptoms.”
- Weber MD, Serevedio FJ, Woodall WR. The Effects of Three Modalities on Delayed Onset Muscle Soreness. JOSPT Open. 1994;20(5):236–42. PubMed 9512831 ❐
Forty women were subjected to intense training of the biceps and brachilias muscles, until they were sore, and then treated with one of four treatments for DOMS: massage, TENS (electrical stimulation), and ergometry (basically light exercise, to stimulate metabolic activity), and rest. Treatments were given immediately after and then 24 and 48 hours after. There was no difference in the results for any of the women.
- Herbert RD, de Noronha M, Kamper SJ. Stretching to prevent or reduce muscle soreness after exercise. Cochrane Database Syst Rev. 2011;(7):CD004577. PubMed 21735398 ❐
Does stretching help either before or after exercise to reduce soreness? Nope. This large review of eleven small scientific studies, and one huge one, wrapped up with a clear thumbs down:
The evidence from randomised studies suggests that muscle stretching, whether conducted before, after, or before and after exercise, does not produce clinically important reductions in delayed-onset muscle soreness in healthy adults.
The evidence was “low to moderate,” with “moderate to high” risk of bias, which means most of the researchers were probably hoping to find that stretching does help DOMS … but even with that likely bias, they still didn’t find what they were looking for.
The big study was technically positive, finding an average drop in soreness of four points on a 100-point scale, which is basically meaningless. The variation between the results for individuals is undoubtedly greater than that.
- Hart L. Effect of stretching on sport injury risk: a review. Clin J Sport Med. 2005 Mar;15(2):113–113. PubMed 15782063 ❐
ABSTRACT
OBJECTIVE: Effect of Stretching on Sport Injury Risk: a Review To assess the evidence for the effectiveness of stretching for the prevention of injuries in sports.
DATA SOURCES: MEDLINE (1966 to September, 2002), Current Contents, Biomedical Collection, Dissertation Abstracts, the Cochrane Library, and SPORTDiscus were searched for articles in all languages using terms including stretching, flexibility, injury, epidemiology, and injury prevention. Reference lists were searched and experts contacted for further relevant studies.
STUDY SELECTION: Criteria for inclusion were randomized trials or cohort studies of interventions that included stretching compared with other interventions, with participants who were engaged in sporting or fitness activities. One author identified 361 articles reporting on flexibility, methods and effects of stretching, risk factors for injury, and injury prevention, of which 6 articles fulfilled the inclusion criteria for meta-analysis.
DATA EXTRACTION: Three independent reviewers blinded to the authors and institutions of the investigations assessed the methodologic quality of the studies (100-point scale) and reached consensus on disagreements. Details of study participants, interventions, and outcomes were extracted. Weighted pooled odds ratios were calculated for effects of interventions on an intention-to-treat basis.
MAIN RESULTS: Reduction in total injuries (shin splints, tibial stress reaction, sprains/strains, and lower-extremity and -limb injuries) with either stretching of specific leg-muscle groups or multiple muscle groups was not found in 5 controlled studies (odds ratio [OR] 0.93; 95% CI, 0.78 to 1.11). Reduction in injuries was not significantly greater for stretching of specific muscles (OR, 0.80; CI, 0.54-1.14) or multiple muscle groups (OR, 0.96; CI, 0.71-1.28). Combining the 3 ratings of methodologic quality, median scores were 29 to 60/100. After adjustment for confounders, low quality studies did not show a greater reduction in injuries with stretching (OR, 0.88; CI, 0.67-1.15) compared with high quality studies (OR, 0.97; CI, 0.77-1.22). Stretching to improve flexibility, adverse effects of stretching, and effects of warm up were not assessed by appropriate intervention studies.
CONCLUSION: Limited evidence showed stretching had no effect in reducing injuries.
- Brushøj C, Larsen K, Albrecht-Beste E, et al. Prevention of overuse injuries by a concurrent exercise program in subjects exposed to an increase in training load: a randomized controlled trial of 1020 army recruits. Am J Sports Med. 2008 Apr;36(4):663–670. PubMed 18337359 ❐
- Pereles D, Roth A, Thompson DJS. A Large, Randomized, Prospective Study of the Impact of a Pre-Run Stretch on the Risk of Injury in Teenage and Older Runners. USATF.org. 2011 Jun 15. PainSci Bibliography 55243 ❐
- Lauersen JB, Bertelsen DM, Andersen LB. The effectiveness of exercise interventions to prevent sports injuries: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2014 Jun;48(11):871–7. PubMed 24100287 ❐ PainSci Bibliography 53226 ❐
- They thought strengthening looked good, but based their very positive-sounding conclusions on only four studies of dubious quality and relevance.
- Baxter C, Mc Naughton LR, Sparks A, Norton L, Bentley D. Impact of stretching on the performance and injury risk of long-distance runners. Res Sports Med. 2017;25(1):78–90. PubMed 27912252 ❐
This paper focusses on stretching’s relationship to endurance sports. It’s somewhat muddled and poorly written, but the substance confirms my bias that stretching is pointless or even slightly harmful for runners. The authors' acknowledge the absence of adequate direct evidence, but thoroughly review what there is, plus a bunch more tangentially relevant evidence. My bias is based on much of the same evidence, so their rambling analysis didn’t add much for me, unfortunately, but I certainly agree with their conclusion that “neither acute nor chronic static stretching has clinically beneficial effects for endurance runners on performance, incidence of DOMS, or to prevent injury.”
- Alexander JLN, Barton CJ, Willy RW. Infographic running myth: static stretching reduces injury risk in runners. Br J Sports Med. 2020 Sep;54(17):1058–1059. PubMed 31694812 ❐
ABSTRACT
It is a commonly held belief that static stretching plays an important role in improving running performance and decreasing injury risk. As such static stretching, undertaken as part of a ‘warm-up’ prior to running, at the end of a run or as part of a strength training programme, is a common practice among runners of all levels. Static stretching involves lengthening a muscle to the point at which a gentle tension is felt and remaining in this position, typically for a minimum of 30seconds per stretch.
Current research evidence definitively reports that this belief is, in fact, incorrect.
- Behm DG, Blazevich AJ, Kay AD, McHugh M. Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: a systematic review. Appl Physiol Nutr Metab. 2016 Jan;41(1):1–11. PubMed 26642915 ❐ PainSci Bibliography 52916 ❐
This wide-ranging review concluded that “studies indicate a 54% risk reduction in acute muscle injuries associated with stretching.” This is at odds even with previous reviews by some of the same key authors. For instance, while McHugh et al. were optimistic in 2010, they based their optimism on speculation and characterized the evidence as limited: “For example, there is a good rationale for why stretching could impact the risk of sustaining a muscle strain injury, but the effect of stretching on muscle strain injuries has not been adequately researched in sports with a high incidence of muscle strains.” That was just six years prior, with almost no relevant new evidence in the interim.
Nearly identical evidence. One review calls it inadequate. The other says stretching prevents muscle strain.
So I guess this question is not settled. 😜
- For instance, if stretching reduces the chances of tearing a muscle, you’d need to stretch the muscles most likely to tear, which are the big muscles of the thighs: quadriceps, hamstrings, and adductors (groin). Hamstrings are likely to be included in most stretching regimens. Quadriceps are often included, but not always. Adductors are often missed or given minimal attention. If stretching reduces the risk of muscle strains, you’d have to make a point of stretching all three — and that’s only the most common strain locations.
- Azuma N, Someya F. Injury prevention effects of stretching exercise intervention by physical therapists in male high school soccer players. Scand J Med Sci Sports. 2020 Nov;30(11):2178–2192. PubMed 33463794 ❐
The abstract for this paper makes it sounds like stretching reduced injury rates. However, the researchers cherry picked their own data to arrive at that conclusion. There was no difference in traumatic injuries to report… only "disorders." There was no difference in the injury rates during competition. And there was no difference in the injury rates.
When you measure several things, there's a pretty good chance that at least one of them is going to look rosier than the others.
And finally, the effect they did detect — 32 of 64 stretchers had at least one (non-traumatic, non-competitive) injury versus 48 of 60 non-stretchers — was technically statistically significant, but also absolutely could have occurred by chance. I suspect if you studied two groups that size several times in a row you'd get quite a surprising variety of numbers.
This study could be showing a genuine injury prevention effect, unlike the body of evidence on this topic. But I doubt it. This is indeed a technically positive trial, but it’s not at all persuasive on its own.
- Academy of Medical Royal Colleges. Exercise: The miracle cure and the role of the doctor in promoting it. AOMRC.org.uk. 2015 Feb. PainSci Bibliography 53672 ❐
This citation is the primary authoritative source of the quote “exercise is the closest thing there is to a miracle cure” (although there are no doubt many variations on it from other sources over the years).
- Gopinath B, Kifley A, Flood VM, Mitchell P. Physical Activity as a Determinant of Successful Aging over Ten Years. Sci Rep. 2018 Jul;8(1):10522. PubMed 30002462 ❐ PainSci Bibliography 53004 ❐
If you want to age well, move around a lot!
We already know that physical activity reduces the risk of several of the major chronic diseases and increases lifespan. “Successful aging” is a broader concept, harder to measure, which encompasses not only a reduced risk of disease but also the absence of “depressive symptoms, disability, cognitive impairment, respiratory symptoms and systemic conditions.” (No doubt disability from pain is part of that equation.)
In this study of 1584 older Australians, 249 “aged successfully” over ten years. The most active Aussies, “well above the current recommended level,” were twice as likely to be in that group. Imagine how much better they’ll do over 20 years …
- Research shows strength training is a much more efficient form of exercise than most people realize, and almost any amount of it is much better than nothing. You can gain strength and all its health benefits fairly easily. For more information, see Strength Training Frequency: Less is more than enough: go to the gym less frequently but still gain strength fast enough for anyone but a bodybuilder.
- The “Upper-Crossed Syndrome” (UCS) sounds impressively technical. It is the apex of clinical storytelling about posture in therapy culture, and the prototypical “muscle imbalance” theory, and yet it basically just means slouching: head and shoulders forward, mostly, with several complicated assumptions about its causes and consequences. With UCS, your muscles are presumed to be like dysfunctional ship’s rigging: some are weak and loose (“inhibited”), while others are too strong and tight (“facilitated”). Viewed from the side, you can draw diagonal lines between these groups that cross. (There’s a Lower-Crossed Syndrome as well.) Dr. Janda was a pioneer and did good work with the information he had at the time, but he was probably mostly wrong about UCS; muscle imbalance theories like UCS have not done well over the last couple decades. For more information, see the upper-crossed syndrome section of my posture article.
- Tumminello N, Silvernail J, Cormack B. The Corrective Exercise Trap. Personal Training Quarterly. 2017 Mar;4(1). PainSci Bibliography 52905 ❐
The authors decisively but gently tip over the most sacred cow of personal training and therapy: corrective exercise, which is grounded in the assumption that there is something in-correct about patients — fragile, weak, or uneven — which must be fixed by sufficiently expert and precise exercise prescription. Exaggerating the importance of defect-correction is actually dangerous for the patient (nocebic): “When clients are told such things about themselves from an authority figure (as they might be during some corrective exercise evaluations), that this potentially makes one’s clients less resilient and more prone to injury and pain.” Translation sans diplomacy: stop #%&^ telling patients they are fragile and weak!
The corrective exercise trap is also about overconfidence in the value of allegedly advanced rehab exercise, when the evidence is overwhelming that corrective exercise is no better than general exercise. “The danger here” — the trap! — “is that many fitness professionals might end up making their training process more about a formalized evaluation procedure and less about good personal training.”
- If an injury causes more stubborn loss of ROM by the mechanism of contracture or derangement of the bone or cartilage in a joint, stretching is going to be futile.
- Ingraham. IT Band Stretching Does Not Work: Stretching the iliotibial band is a popular idea, but it’s very hard to do it right, and it’s probably not worth it. PainScience.com. 3664 words.
- Radford JA, Landorf KB, Buchbinder R, Cook C. Effectiveness of calf muscle stretching for the short-term treatment of plantar heel pain: a randomised trial. BMC Musculoskelet Disord. 2007 Apr;8:36. PubMed 17442119 ❐ PainSci Bibliography 52975 ❐
This trial of stretching for plantar fasciitis made an effort to blind the participants. That is, the 92 study subjects didn’t know what treatment was being tested, reducing the likelihood of bias in reporting on the results. This was achieved by adding sham ultrasound to both the treatment and control groups, a good strategy. After two weeks, unfortunately there was no difference between the groups: “a two-week stretching program provides no statistically significant benefit in ‘first-step’ pain, foot pain, foot function or general foot health compared to not stretching.”
It could have been a larger, longer study, sure, but 92 feet is quite a decent sample size for studies of this kind of thing. And although stretching benefits might ramp up over time, that’s probably wishful thinking, and you’d certainly hope to see clearer signs of progress after two weeks of diligent stretching.
- Malliaropoulos N, Papalexandris S, Papalada A, Papacostas E. The role of stretching in rehabilitation of hamstring injuries: 80 athletes follow-up. Med Sci Sports Exerc. 2004 May;36(5):756–9. PubMed 15126706 ❐
About 40 Greek athletes who stretched more intensively recovered faster than those who stretched more lackadaisically (and the effect is probably not limited to the Hellenic people). How much faster did they recover? They regained their range of motion about 22% sooner (5.6 days instead of 7.3), and their “rehabilitation period” was about 12% shorter (13.3 days instead of 15 days). The researchers reported that this was of “great importance in treating muscle strain injuries.” I’m not quite so thrilled by those numbers: getting back in the game about 36 hours sooner is not nothing, but I wouldn’t call it greatly important. One could easily argue that a wee improvement in healing time isn’t worth the risk of injury, or even the tedious routine of stretching. One could also argue that they really should have compared stretching to other kinds of rehabilitative exercise, and the difference probably would have disappeared.
- HSD is a bucket diagnosis for people with symptomatic hypermobility, but without a clear diagnosis of a connective tissue disorder, like EDS or Marfan syndrome.
- “The essential difference between HSD and hEDS lies in the stricter criteria for hEDS compared to the HSD.” But it’s very tricky, and those criteria are all very new (see the 2017 EDS International Classification). Ironically, as of 2017, the one sub-type of EDS that does not have an identified genetic cause is the hypermobile EDS (hEDS).
- Scheper MC, de Vries JE, Verbunt J, Engelbert RH. Chronic pain in hypermobility syndrome and Ehlers-Danlos syndrome (hypermobility type): it is a challenge. J Pain Res. 2015;8:591–601. PubMed 26316810 ❐ PainSci Bibliography 52758 ❐ Hypermobility is “highly prevalent among patients diagnosed with chronic pain.”
- There’s actually an entire stretching book that is largely based on this idea — but that book is conspicuously full of armchair science, and no actual evidence that the ideas are true.
- From Kay et al.: “The detrimental effects of static stretch are mainly limited to longer durations (≥60 s) which may not be typically used during pre-exercise routines in clinical, healthy or athletic populations. Shorter durations of stretch (<60 s) can be performed in a pre-exercise routine without compromising maximal muscle performance.”
- Beckett JR, Schneiker KT, Wallman KE, Dawson BT, Guelfi KJ. Effects of Static Stretching on Repeated Sprint and Change of Direction Performance. Medicine & Science in Sports & Exercise. 2009 Jan 5.
- The most obvious wrinkle is that the negative impact of static stretching on sprinting might be short term — were the runners slowed down for only ten minutes? Twenty minutes? As much as sixty? Another important consideration is that the potential therapeutic effects of stretching — still remarkably unproven at this late date in history, but still hypothetically possible — could conceivably outweigh the relatively small cost of being slowed down. For instance, if (big if) stretching significantly reduced the risk of a muscle strain, would that risk reduction be worth the cost to sprinting speed? Probably! If.
Baxter 2017, op. cit. Previously cited for their conclusion that stretching doesn't prevent running injuries, Baxter et al. also don’t think it boosts running performance, pointing to evidence of the opposite effect:
“The literature suggests that stretching poses no significant advantage to endurance runners. Acute stretching can reduce running economy and performance for up to an hour by diminishing the musculotendinous stiffness and elastic energy.”
- Damasceno MV, Duarte M, Pasqua LA, et al. Static Stretching Alters Neuromuscular Function and Pacing Strategy, but Not Performance during a 3-Km Running Time-Trial. PLoS One. 2014;9(6):e99238. PubMed 24905918 ❐ PainSci Bibliography 53972 ❐
- Musham C, Hayes PR. Effect of pre-exercise stretching on repeat sprint performance. Br J Sports Med. 2010;44(14). PainSci Bibliography 54795 ❐
- Wolfe F, Clauw DJ, Fitzcharles MA, et al. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J Rheumatol. 2011 Jun;38(6):1113–22. PubMed 21285161 ❐
- McHugh MP, Tallent J, Johnson CD. The role of neural tension in stretch-induced strength loss. J Strength Cond Res. 2013 May;27(5):1327–32. PubMed 23439335 ❐
- Lowery RP, Joy JM, Brown LE, et al. Effects of static stretching on 1-mile uphill run performance. J Strength Cond Res. 2014 Jan;28(1):161–7. PubMed 23588487 ❐
- Konrad A, Močnik R, Nakamura M, Sudi K, Tilp M. The Impact of a Single Stretching Session on Running Performance and Running Economy: A Scoping Review. Front Physiol. 2020;11:630282. PubMed 33551850 ❐ PainSci Bibliography 51822 ❐
- Minetto MA, Holobar A, Botter A, Farina D. Origin and Development of Muscle Cramps. Exerc Sport Sci Rev. 2013 Jan;41(1):3–10. PubMed 23038243 ❐ PainSci Bibliography 54733 ❐ “Dehydration (and/or cramps, motor unit action potentials, motor neurons electrolyte depletion) often is given as an explanation for muscle cramps occurring in workers and athletes, although this claim is not supported by scientific evidence.” I discuss this at greater length, with more references, in Cramps, Spasms, Tremors & Twitches.
- His wrist ROM was especially memorable: it was like his hands were welded onto the end of his forearms. He once showed me how far he could bend his wrist back, which was not at all. Aikido uses a lot of wrist locks, so his sturdy and inflexible wrists made him almost impervious to those … but with no detectable functional deficit either.
Cooper, Bob. “The Rules Revisited.” Runner’s World. September, 2009. p. 59. - Ylinen J, Kautiainen H, Wiren K, Hakkinen A. Stretching exercises vs manual therapy in treatment of chronic neck pain: a randomized, controlled cross-over trial. J Rehabil Med. 2007;39(2):126–132. PubMed 17351694 ❐
This examiner-blinded randomized cross-over trial of 125 patients found pretty promising benefits to both stretching exercises and “manual therapy” for a month, and the researchers concluded that “low-cost stretching exercises can be recommended in the first instance as an appropriate therapy intervention to relieve pain, at least in the short-term.” However, there are several reasons not to get too excited about the significance of this study, perhaps the most important of which is simply that showing some improvement over 4 weeks is hardly an impressive therapeutic accomplishment, and if the study had included a control group it might well have revealed that the “therapeutic” effects weren’t much different than the natural course of the condition — i.e. everyone might have gotten better, with and without therapy of any kind.
- Sherman KJ, Cherkin DC, Wellman RD, et al. A Randomized Trial Comparing Yoga, Stretching, and a Self-care Book for Chronic Low Back Pain. Arch Intern Med. 2011 Oct. PubMed 22025101 ❐
This experiment compared the effects of yoga, a normal stretching class, and an educational booklet on chronic low back pain. The primary findings were that both yoga and stretching seemed to be modestly effective, but neither was better than the other. Back in 2005, the same authors got similar results comparing yoga to conventional therapeutic exercise.
The research has been widely reported as “stretching and yoga work,” with a few writers emphasizing that yoga was no better. However, I haven’t seen anyone report that both stretching and yoga are equally damned here with faint praise, and quite possibly illusory praise: the effect size was modest, just 2.5 points on a scale of 11, and some or all that effect may well be attributable to bias and frustrebo (frustrated placebo) caused by a lack of blinding. Subjects deprived of either a lovely stretching or yoga experience may have reported a more negative experience.
I analyze this study in greater detail in my advanced tutorial, The Complete Guide to Low Back Pain
- Tunwattanapong P, Kongkasuwan R, Kuptniratsaikul V. The effectiveness of a neck and shoulder stretching exercise program among office workers with neck pain: a randomized controlled trial. Clin Rehabil. 2016 Jan;30(1):64–72. PubMed 25780258 ❐
A trial of stretching for neck pain, specifically “neck and around shoulder stretching exercises two times/day, five days/week during four weeks.” This study had 96 subjects and was well-controlled: stretching was compared to a control group of patients who received only an educational brochure on posture and ergonomics (which isn’t likely to do much, of course). Nevertheless, the control group did improve over three weeks, and while the stretching group improved more they did not improve much more — roughly a point on a 10-point pain scale, for instance. Nothing to write home about. On the bright side, subjects who stretched more did better.
- Ylinen J, Nikander R, Nykänen M, Kautiainen H, Häkkinen A. Effect of neck exercises on cervicogenic headache: a randomized controlled trial. J Rehabil Med. 2010 Apr;42(4):344–9. PubMed 20461336 ❐
- Gómez-Hernández M, Gallego-Izquierdo T, Martínez-Merinero P, et al. Benefits of adding stretching to a moderate-intensity aerobic exercise programme in women with fibromyalgia: a randomized controlled trial. Clin Rehabil. 2020 Feb;34(2):242–251. PubMed 31847574 ❐
This trial compared a program of endurance training with stretching to another program without the stretching. The results are characterized as a win in the abstract, but the fine print —the actual data — is disappointing. This is yet another one of those “technically positive” studies. A few dozen subjects who stretched did get better scores on four different outcome measures. However, the differences were really quite small.
- This is a topic I cover in considerable detail in an excerpt from an entire book about IT band syndrome. See IT Band Stretching Does Not Work: Stretching the iliotibial band is a popular idea, but it’s very hard to do it right, and it’s probably not worth it.
- Some drugs are notorious for causing joint and/or muscle pain as a side effect. (Other kinds of pain are possible too, but are usually more distinctive and readily identified as a drug side effect. But joint and muscle pain are often mistaken for musculoskeletal trouble, and no one suspects the drug.) The usual suspects are the statins (for lowering cholesterol), bisphosphonates (for osteoporosis and Paget’s disease), fluoroquinolones (a class of antibiotics with an extraordinary range of nasty side effects, most notoriously tendinitis), the retinoids (for skin conditions, like Accutane for acne), and Trintellix (an antidepressant). Withdrawal from benzodiazepines (Valium, Ativan, Xanax, etc) can be extremely uncomfortable and painful; unaware of the risks, many people stop taking them carelessly and suffer quite a bit without ever knowing why. For more detail on some of these, see 38 Surprising Causes of Pain.
How do we get into this mess? Inflammaging correlates with poor fitness and obesity (metabolic syndrome, the biological precursor to diabetes and heart disease). And that, in turn is linked to chronic psychological stress (and of course biological stresses too, like smoking and sleep deprivation). And then there are several other unproven but plausible reasons why inflammation escalates as we age, such as the accumulation of permanent minor infections, lasting collateral damage from past infections (essentially autoimmune disease and allergies that are too subtle or nonspecific to diagnose), and environmental poisons.
For a much more thorough exploration of these possibilities, see Chronic, Subtle, Systemic Inflammation: One possible sneaky cause of puzzling chronic pain.- Berrueta 2016, op. cit.
- Langevin HM, Stevens-Tuttle D, Fox JR, et al. Ultrasound evidence of altered lumbar connective tissue structure in human subjects with chronic low back pain. BMC Musculoskelet Disord. 2009 Dec;10:151. PubMed 19958536 ❐ PainSci Bibliography 53554 ❐
Researchers measured the thickness of lumbar connective tissues with ultrasound in 60 chronic low back pain patients and 47 health people. The fascia was about 25% thicker in people with back pain, which is quite a bit, and a surprising finding with potentially major — but unknown — clinical significance. The authors suggest that it could be related to “genetic factors, abnormal movement patterns and chronic inflammation.”
This observation has not been reproduced by other researchers, but a follow-up study in 2011 examined the flexibility of the same tissue, and found it was about 20% less in back pain patients: see Langevin for more commentary on the implications of both studies.
- Ingraham. Massage Does Not Reduce Inflammation: The making of a new massage myth from a high-tech study of muscle samples after intense exercise. PainScience.com. 5631 words.
- Støve MP, Magnusson SP, Thomsen JL, Riis A. Efficacy of a novel home-based stretching program on fibromyalgia symptoms: a randomised controlled trial. Arch Phys Med Rehabil. 2026 Jun:S0003–9993(26)00747–1. PubMed 42242521 ❐ PainSci Bibliography 49278 ❐
This trial cannot separate the effect of stretching from the effects of expectancy, novelty, and weekly contact with a caring researcher, yada yada yada — an especially glaring problem with fibromyalgia, where patients are starved for validation. Participants weren’t blinded either, so the waitlisted group results were probably deflated by disappointment (“frustrebo” effect, performance bias), widening the artifactual gap further. All of this has happened before, like with massage for fibromyalgia.
The authors acknowledge this problem, but they seriously understate how decisively it sabotages the experiment:
“the waitlist design may have induced expectancy asymmetry and limited causal inference compared with an active comparator”
This is like saying that eating potato salad left in the sun for an afternoon may induce facilitated fecal transit. The waitlist design definitely broke the experiment.
- If stretching actually did anything, it would have been added to the predictable effect of therapist attention, resulting in results that were downright impressive instead of modest. In other words, even though this study was doomed to give stretching an unfair advantage, it still couldn’t produce anything better than a modest benefit — and that’s actually a backwards form of negative evidence.
- Setchell J, Costa N, Ferreira M, Hodges PW. What decreases low back pain? A qualitative study of patient perspectives. Scand J Pain. 2019 07;19(3):597–603. PubMed 31031264 ❐ This survey of 130 Australians showed that about 40% of them believe that “stretching and therapeutic exercise” relieves back pain. I am sure that percentage varies quite a bit depending on who you ask and how you ask them, and (for instance) I wish they’d asked about just stretching. But just the fact that stretching is named (as if it’s the most important example of therapeutic exercise) is significant: faith in stretching is baked right into the question.
- Sherman KJ, Cherkin DC, Wellman RD, et al. A Randomized Trial Comparing Yoga, Stretching, and a Self-care Book for Chronic Low Back Pain. Arch Intern Med. 2011 Oct. PubMed 22025101 ❐
- Chen HM, Wang HH, Chen CH, Hu HM. Effectiveness of a stretching exercise program on low back pain and exercise self-efficacy among nurses in Taiwan: a randomized clinical trial. Pain Manag Nurs. 2014 Mar;15(1):283–91. PubMed 23266331 ❐
- Pourahmadi M, Hesarikia H, Keshtkar A, et al. Effectiveness of Slump Stretching on Low Back Pain: A Systematic Review and Meta-analysis. Pain Med. 2019 02;20(2):378–396. PubMed 30590849 ❐
- Sihawong R, Janwantanakul P, Jiamjarasrangsi W. A prospective, cluster-randomized controlled trial of exercise program to prevent low back pain in office workers. Eur Spine J. 2014 Apr;23(4):786–93. PubMed 24492949 ❐ PainSci Bibliography 51730 ❐
- van Dillen LR, Lanier VM, Steger-May K, et al. Effect of Motor Skill Training in Functional Activities vs Strength and Flexibility Exercise on Function in People With Chronic Low Back Pain: A Randomized Clinical Trial. JAMA Neurology. 2021 04;78(4):385–395. PainSci Bibliography 51820 ❐
Got back pain? Trouble bending over? Twisting this-a-way? Flexing that-a-way? Maybe just keep trying! The “just do it” school of therapy. Motor skills training is basically doing movements that are “difficult to perform because of low back pain.” From a certain perspective, you could even call MST a kind of advanced stretching — because it’s focused on pushing beyond movement limitations. (It has a lot in common with the McKenzie mentioned in the previous footnote, actually, with regards to Owen et al.) van Dillen et al. presents evidence that it’s a bit more effective than a more conventional stretching program (and combined with strengthening), but only just a bit. Meh.
In addition to damning stretching with a technical loss, and damning MST with a trivial win, this study has some other problems.
- Owen PJ, Miller CT, Mundell NL, et al. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br J Sports Med. 2020 Nov;54(21):1279–1287. PubMed 31666220 ❐ PainSci Bibliography 51736 ❐
- This is a very complex point that I have substantiated in extreme detail in other places. For one (of several) introductions to the topic, see MRI and X-Ray Often Worse than Useless for Back Pain.
- Hori M, Hasegawa H, Takasaki H. Comparisons of hamstring flexibility between individuals with and without low back pain: systematic review with meta-analysis. Physiother Theory Pract. 2019 Jul:1–24. PubMed 31317831 ❐
- Sadler SG, Spink MJ, Ho A, De Jonge XJ, Chuter VH. Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: a systematic review of prospective cohort studies. BMC Musculoskelet Disord. 2017 05;18(1):179. PubMed 28476110 ❐ PainSci Bibliography 52715 ❐
- Ylinen JJ, Kautiainen HJ, Häkkinen AH. Comparison of active, manual, and instrumental straight leg raise in measuring hamstring extensibility. J Strength Cond Res. 2010 Apr;24(4):972–7. PubMed 20300030 ❐
- Raftry SM, Marshall PWM. Does a 'tight' hamstring predict low back pain reporting during prolonged standing? Journal of Electromyography and Kinesiology. 2012 Jun;22(3):407–11. PubMed 22397821 ❐
- Johnson EN, Thomas JS. Effect of hamstring flexibility on hip and lumbar spine joint excursions during forward-reaching tasks in participants with and without low back pain. Arch Phys Med Rehabil. 2010 Jul;91(7):1140–2. PubMed 20599054 ❐
- Marshall PW, Mannion J, Murphy BA. Extensibility of the hamstrings is best explained by mechanical components of muscle contraction, not behavioral measures in individuals with chronic low back pain. PM R. 2009 Aug;1(8):709–18. PubMed 19695522 ❐ This was a small trial for cLBP patients, finding no link between hamstring extensibility and disability.
- Harvey LA, Katalinic OM, Herbert RD, et al. Stretch for the treatment and prevention of contractures. Cochrane Database Syst Rev. 2017 Jan;1:CD007455. PubMed 28146605 ❐ PainSci Bibliography 52742 ❐
- Perhaps there are other methods of stretching that do work for contracture, but the average person has no idea what those are, and therapists scatter in every direction on this point, failing to agree on which “other method” works because there is no evidence base for it — just a whole lot of guessing.
- Basson A, Olivier B, Ellis R, et al. The Effectiveness of Neural Mobilization for Neuro-Musculoskeletal Conditions: A Systematic Review and Meta-Analysis. J Orthop Sports Phys Ther. 2017 Jul:1–76. PubMed 28704626 ❐
The level of evidence for neural mobilization is “largely unknown” according to this review of forty studies (only seventeen with a low risk of bias, and with lots of variety in methods throughout). The results were mixed, and NM notably failed for relatively straightforward peripheral neuropathies like carpal tunnel syndrome — if NM is good for anything, it should be good for that, at least.
On the bright side, according to the paper, the data “reveals benefits of NM for back and neck pain,” but these are complex conditions and notoriously multifactorial, so I remain pessimistic in the absence of more and better data. As the authors understate: “Due to the limited evidence and varying methodological quality, conclusions may change over time.” I’d say it’s so likely that “conclusions may change” that the word “conclusion” isn’t really useful here.
- Quintner JL, Bove GM, Cohen ML. A critical evaluation of the trigger point phenomenon. Rheumatology (Oxford). 2015 Mar;54(3):392–9. PubMed 25477053 ❐ Quintner et al. have hypothesized that “irritated peripheral nerve trunks” are “a rich source” of pain, and may be the true cause of trigger points, rather than the more conventional idea that they are “micro cramps.”
- Freitas SR, Mendes B, Le Sant G, et al. Can chronic stretching change the muscle-tendon mechanical properties? A review. Scand J Med Sci Sports. 2018 Mar;28(3):794–806. PubMed 28801950 ❐ “Stretching interventions with 3- to 8-week duration do not seem to change either the muscle or the tendon properties, although it increases the extensibility and tolerance to a greater tensile force.”
- Behm DG, Blazevich AJ, Kay AD, McHugh M. Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: a systematic review. Appl Physiol Nutr Metab. 2016 Jan;41(1):1–11. PubMed 26642915 ❐ PainSci Bibliography 52916 ❐ “All forms of training induced ROM improvements, typically lasting <30 min.”
- Medeiros DM, Cini A, Sbruzzi G, Lima CS. Influence of static stretching on hamstring flexibility in healthy young adults: Systematic review and meta-analysis. Physiother Theory Pract. 2016 Aug;32(6):438–445. PubMed 27458757 ❐ “In all tests, the results favored static stretching compared to control group… In conclusion, static stretching was effective in increasing hamstring flexibility in healthy young adults.”
- Decoster LC, Cleland J, Altieri C, Russell P. The effects of hamstring stretching on range of motion: a systematic literature review. J Orthop Sports Phys Ther. 2005 Jun;35(6):377–87. PubMed 16001909 ❐
Results were inconclusive as to whether or not any particular type of stretching could improve knee ROM. Overall, however, “the evidence appears to indicate that hamstring stretching increase range of motion,” regardless of the technique used. “Appears to indicate” is pretty inconclusive.
- Harvey L, Herbert R, Crosbie J. Does stretching induce lasting increases in joint ROM? A systematic review. Physiother Res Int. 2002;7(1):1–13. PubMed 11992980 ❐ “The results of four 'moderate' quality studies show a convincing effect of stretching in people without functionally significant contracture.”
- American College of Sports Medicine. ACSM’s guidelines for exercise testing and prescription. 10th ed. Philadelphia: Wolters Kluwer; 2018.
- Waryasz GR, Daniels AH, Gil JA, Suric V, Eberson CP. Personal Trainer Demographics, Current Practice Trends and Common Trainee Injuries. Orthop Rev (Pavia). 2016 Sep;8(3):6600. PubMed 27761219 ❐ PainSci Bibliography 52598 ❐
- Roberts JM, Wilson K. Effect of stretching duration on active and passive range of motion in the lower extremity. Br J Sports Med. 1999 Aug;33(4):259–63. PubMed 10450481 ❐
Another (small) study to determine if stretching for five or fifteen seconds can make a difference in range of motion of the joint. It concluded: “These findings suggest that holding stretches for 15 seconds, as opposed to five seconds, may result in greater improvements in active ROM. However, sustaining a stretch may not significantly affect the improvements gained in passive ROM.” In other words, the returns diminish quickly.
- Marshall PWM, Cashman A, Cheema BS. A randomized controlled trial for the effect of passive stretching on measures of hamstring extensibility, passive stiffness, strength, and stretch tolerance. J Sci Med Sport. 2011 Nov;14(6):535–40. PubMed 21636321 ❐
- Hargrove T. Playing With Movement: How to explore the many dimensions of physical health and performance. 1st ed. self-published; 2019. p. 148
- Hard to prove a negative, of course, but if you go looking for data on this and you actually find some, you’re research fu is stronger than mine.
- Covert CA, Alexander MP, Petronis JJ, Davis DS. Comparison of ballistic and static stretching on hamstring muscle length using an equal stretching dose. J Strength Cond Res. 2010 Nov;24(11):3008–14. PubMed 20375742 ❐
This was a comparison of static versus “ballistic” (bouncing) stretching for the hamstrings, showing trivial superiority of static stretching — so trivial that they were basically identical.
- Konrad A, Stafilidis S, Tilp M. Effects of acute static, ballistic, and PNF stretching exercise on the muscle and tendon tissue properties. Scand J Med Sci Sports. 2017 Oct;27(10):1070–1080. PubMed 27367916 ❐ PainSci Bibliography 51812 ❐
This was a comparison of the effect of a single dose of static stretching, ballistic stretching, or proprioceptive neuromuscular facilitation (PNF) stretching, but very thoroughly measured (several different metrics). The comparison showed “no clinically relevant difference between the stretching groups.”
- Smith LL, Brunetz MH, Chenier TC, et al. The effects of static and ballistic stretching on delayed onset muscle soreness and creatine kinase. Res Q Exerc Sport. 1993 Mar;64(1):103–7. PubMed 8451526 ❐
- 2:01:39, which is 1:18 faster than the previous record, the greatest improvement since 1967. This dude is fast.
- That’s a lot of claims. Rather than citing to support all of them, I’ll just refer you to Nuzzo’s very detailed review, previously cited, which cites many examples and also acknowlgedes some exceptions. The exceptions, however, mostly just “prove the rule.”
- Ch W, Holzman C, Magnusson SP. Increasing muscle extensibility: a matter of increasing length or modifying sensation? Phys Ther. 2010 Mar;90(3):438–49. PubMed 20075147 ❐ PainSci Bibliography 55283 ❐
- Mizuno T, Matsumoto M, Umemura Y. Viscoelasticity of the muscle-tendon unit is returned more rapidly than range of motion after stretching. Scand J Med Sci Sports. 2011 May. PubMed 21564309 ❐
Participants stretched their calf muscle; at intervals following the stretch, the stiffness of the muscle and the range of motion of the ankle were tested. Although the stiffness of the muscle improved considerably at first, it decreased quickly; however, the range of motion of the ankle significantly increased and was retained for up to 90 minutes. That is, range of motion was retained even after a brief reduction in stiffness subsided, strongly suggesting that ROM is not limited by the viscoelasticity of the tissue.
This study, although small, is consistent with other evidence and the general trend that the impact of stretch is sensory and neurological, not mechanical — i.e. a mild warm-up, basically.
- Brunello E, Reconditi M, Elangovan R, et al. Skeletal muscle resists stretch by rapid binding of the second motor domain of myosin to actin. Proc Natl Acad Sci U S A. 2007 Dec;104(50):20114–9. PubMed 18077437 ❐ PainSci Bibliography 52656 ❐
While it is well understood that muscles have a “braking” function that kicks in with rapid increases in load, something that occurs constantly in normal activity, but the molecular mechanisms for braking has been slow . This super cool study shed quite a bit of light on that old puzzle of muscle physiology, showing that muscles brake not by “contracting” to resist the rapid elongation, but by building many extra actin-myosin bonds in an instant — becoming stiffer and less extensible in just a few milliseconds, like a rubber band that gets instantly thicker in proportion to how suddenly you pull on it.
This process is also requires very little energy. So the muscle basically solidifies efficiently.
- Optometrists have a machine that blows a puff of air into the eye. I always enjoy the silly challenge of trying to resist blinking. It’s clearly impossible. In general, humans haven’t shown much potential to resist their reflexes. When the doctor bonks your patellar tendon with a rubber hammer, your leg kicks, period — no amount of practice is going to stop that. (Although, to be fair, I’ve never tried really hard.)
- Blazevich AJ, Cannavan D, Waugh CM, et al. Neuromuscular factors influencing the maximum stretch limit of the human plantar flexors. J Appl Physiol (1985). 2012 Nov;113(9):1446–55. PubMed 22923509 ❐ This study reports some apparently reflexive contraction. “Previous research has rarely found a link between EMG activity and range of motion … In contrast, we found a moderate and statistically significant correlation between the angle of onset of muscle activity (but not EMG amplitude) and peak ROM. To our knowledge, this is the first such report…”
- In general, the brain can’t be manipulated simply by wishing, force of will, or a carefully cultivated good attitude. The brain powerfully and imperfectly controls how we experience potentially threatening stimuli, but I’m sorry to report that you do not control your brain. Consciousness and “mind” are by-products of brain function and physiological state. (Deep, eh?) It’s not your opinion of sensory signals that counts, it’s what your brain makes of them that counts — which happens quite independently of consciousness and self-awareness.
- It’s important to keep in mind that the limits aren’t highly flexible because they exist for really excellent reasons. If all the brain limits were suddenly lifted from all the world’s elite and hardcore athletes, half of them would probably be dead or severely injured within a week. It makes complete sense that it’s really hard to convince the brain to be more permissive.
- Folpp H, Deall S, Harvey LA, Gwinn T. Can apparent increases in muscle extensibility with regular stretch be explained by changes in tolerance to stretch? Aust J Physiother. 2006;52(1):45–50.
- Blazevich AJ, Cannavan D, Waugh CM, et al. Range of motion, neuromechanical, and architectural adaptations to plantar flexor stretch training in humans. J Appl Physiol (1985). 2014 Sep;117(5):452–62. PubMed 24947023 ❐
- Behm DG, Cavanaugh T, Quigley P, et al. Acute bouts of upper and lower body static and dynamic stretching increase non-local joint range of motion. Eur J Appl Physiol. 2016 Jan;116(1):241–9. PubMed 26410819 ❐
In this study, range of motion and strength were tested in the upper body after static stretching in the lower body, and vice versa. Passive range of motion was modestly improved, which is nifty, but not active ROM or strength, suggesting that “enhanced stretch tolerance was likely the significant factor,” as opposed to a mechanical or neural drive mechanism.
- Issurin VB, Liebermann DG, Tenenbaum G. Effect of vibratory stimulation training on maximal force and flexibility. J Sports Sci. 1994 Dec;12(6):561–6. PubMed 7853452 ❐
In this 1994 experiment, as described by Sands et al., gymnasts “used a vibrating ring suspended by a cable, in which the foot of the subject was placed while they stretched forward over the raised leg, targeting the hamstrings. The resulting increase in ROM was astonishing. These researchers demonstrated that vibration could enhance flexibility.” The results were replicated by Sands et al. in 2006, and Kinser et al. in 2008.
- Sands WA, McNeal JR, Stone MH, Russell EM, Jemni M. Flexibility enhancement with vibration: Acute and long-term. Med Sci Sports Exerc. 2006 Apr;38(4):720–5. PubMed 16679989 ❐
This experiment replicated the results of an intriguing 1994 experiment by Issurin et al. Ten highly trained gymnasts did forward splits with or without vibration. They stretched to the point of discomfort for 4 minutes, alternating between each leg, 10 seconds of stretching at a time. Flexibility immediately after stretching with vibration was dramatically greater; the long-term results were less striking.
- Kinser AM, Ramsey MW, O’Bryant HS, et al. Vibration and stretching effects on flexibility and explosive strength in young gymnasts. Med Sci Sports Exerc. 2008 Jan;40(1):133–40. PubMed 18091012 ❐
Replicates the findings of both Issurin and Sands — “simultaneous vibration and stretching may greatly increase flexibility, while not altering explosive strength.”
Calling an idea “less wrong” is a way to acknowledge that an idea is probably not the whole truth while also asserting that it’s closer to it than other ideas. It’s a much more realistic goal than being “right” about anything controversial or at the edges of complex fields of knowledge. We have a shot at reducing inaccuracy and imprecision, but actually eliminating it is nearly impossible — especially in the life sciences, where emergent properties bubble up through thick layers of interacting systems, shaped by countless variables, and about as comprehensible to us as a microwave is to a dog.
The LessWrong blog says that less wrong expresses two important points:
- A humble recognition that no human is ever going to attain perfectly true beliefs and be right about everything. We should always believe that some of our beliefs are mistaken, we just don’t know which ones.
- A bold recognition that notwithstanding the impossibility of being perfectly right, there is still the possibility of being less wrong. Everyone believes false things, but some believe a lot fewer wrong things than others.
- Blazevich 2012, op. cit. This study is an extremely good example of just how absurdly complex all of this is, and specifically it shows that there are variables we still don’t understand. Consider some of their conclusions:
As reported by previous researchers, subjects who were more flexible demonstrated less resistance to the stretch and were able to tolerate a greater stretch load (i.e., greater “passive” joint moment). However, for the first time, we have also shown that more flexible subjects exhibited greater fascicle rotation during stretch and a later onset of reflex muscle activity (i.e., EMG onset) than their less flexible counterparts. Nonetheless, the angle of EMG onset was not correlated with H-reflex amplitude recorded with the muscles held in a stretched position. The present results show significant differences in neural and muscular responses to stretch between the groups.
- Marshall 2011, op. cit.
- This experiment was agnostic about mechanism. It cannot actually settle the bet — it demonstrated only a reduction in stiffness, but not whether it was due to neural or structural adaptations.
- Several things in the paper suggest their bias, but it’s clearest here: although they concede that they “cannot completely rule out volitional stretch tolerance as a possible explanation for changes in extensibility,” they still conclude that “it does seem that hamstring pain elicited during a passive stretch has little involvement in explaining training related improvements.” Really? Sure seems to me like it could!
- Guissard N, Duchateau J. Effect of static stretch training on neural and mechanical properties of the human plantar-flexor muscles. Muscle & Nerve. 2004 Feb;29(2):248–55. PubMed 14755490 ❐
- Konrad A, Tilp M. Increased range of motion after static stretching is not due to changes in muscle and tendon structures. Clin Biomech (Bristol, Avon). 2014 May 9. PubMed 24856792 ❐
Another data point in the plasticity vs. tolerance debate: “The increased range of motion could not be explained by the structural changes in the muscle-tendon unit, and was likely due to increased stretch tolerance possibly due to adaptations of nociceptive nerve endings.”
- Farinatti PTV, Brandão C, Soares PPS, Duarte AFA. Acute effects of stretching exercise on the heart rate variability in subjects with low flexibility levels. J Strength Cond Res. 2011 Jun;25(6):1579–85. PubMed 21386722 ❐
… multiple-set flexibility training session enhanced the vagal modulation and sympathovagal balance in the acute postexercise recovery, at least in subjects with low flexibility levels. … The present results suggest that stretching routines may contribute to a favorable autonomic activity change in untrained subjects.
- Warneke K, Wirth K, Keiner M, et al. Comparison of the effects of long-lasting static stretching and hypertrophy training on maximal strength, muscle thickness and flexibility in the plantar flexors. Eur J Appl Physiol. 2023 Aug;123(8):1773–1787. PubMed 37029826 ❐ PainSci Bibliography 51621 ❐
- Panidi I, Bogdanis GC, Terzis G, et al. Muscle Architectural and Functional Adaptations Following 12-Weeks of Stretching in Adolescent Female Athletes. Front Physiol. 2021;12:701338. PubMed 34335307 ❐ PainSci Bibliography 51449 ❐
- Nunes JP, Schoenfeld BJ, Nakamura M, et al. Does stretch training induce muscle hypertrophy in humans? A review of the literature. Clin Physiol Funct Imaging. 2020 May;40(3):148–156. PubMed 31984621 ❐
- Kato M, Nihei Green F, Hotta K, et al. The Efficacy of Stretching Exercises on Arterial Stiffness in Middle-Aged and Older Adults: A Meta-Analysis of Randomized and Non-Randomized Controlled Trials. Int J Environ Res Public Health. 2020 08;17(16). PubMed 32764418 ❐ PainSci Bibliography 51988 ❐
- Many readers have pointed out that experienced yoga practitioners are flexible, especially the older ones. For instance, T.G. writes, “In my yoga class, the older people are way more flexible than the younger ones.” It may be that training has made them more flexible, but not necessarily. A perpetually neglected explanation for the flexible-yoga-oldster phenomenon is that people with natural gifts of flexibility like the activity and stick with it, because we humans enjoy almost anything we’re good at … and the less flexible tend to drop out. I’m not saying this is how it is — I truly don’t know — just that it’s the kind of explanation that tends to get neglected. We need to consider such counter-intuitive, inside-out explanations that are, perhaps, less comforting to our biases. Even if there is a training effect, it’s extremely likely that it’s only part of the reason those folks are more flexible, and that’s something most “huge fans” of stretching have simply never considered.