Heat for Pain and Rehab
A detailed guide to using heat as therapy for acute and chronic pain and recovery from injury

This article is about 14,000 words and covers therapeutic heating like a small book. About 60% of it is free, and there’s a members only section that dives deep into the science spice therapy, using capsaicin to (hopefully) treat pain.
Therapeutic heating — “thermotherapy” for therapy geeks, the opposite of its trendier cousin, cryotherapy — is more useful than most people realize, mainly because muscle is a source of more and worse pain than most people realize, and muscle pain seems to respond well to heat. Muscle pain caused by over-exertion, muscle cramps and spasms, and especially trigger points (muscle “knots”) are all common and sometimes severe, but often mistaken for other kinds of problems.
This therapeutic staple has mostly been ignored by science: its benefits are far from proven, and obviously it’s no miracle cure.1 Nevertheless, it’s probably doing more than “just” relieving symptoms. (Not that we should knock symptom relief.2) Everyone should understand heating the same way everyone knows how to put on a Band-Aid: it is a cheap, drugless way of taking the edge off an amazing array of common painful problems, especially neck and back pain, and maybe more.
What heat is for: mostly non-inflammatory body pain
Heat is primarily for relaxation, comfort, and reassurance … and maybe taking the edge off several kinds of body pain, mostly duller and persistent pains associated with stiffness, cramping, and/or sensitivity, which can be loosely categorized:
- Acute soreness from over-exertion: the pain you get after the first ski trip of the season. (Interestingly, not only is heat likely helpful for this kind of pain, it’s almost the only thing that is! More about this below.)
- Stiffness and pain in specific areas related to osteoarthritis, muscle “knots” or trigger points, and many kinds of cramping/spasm3 (menstrual, neuropathic, restless leg syndrome, for example, or even just stiffness from postural stress).4 But not, of course, cramps from heat exhaustion! Or even ordinary exercise-induced cramps.5
- “Hurts all over” pain and sensitivity. There are many kinds, but primarily: fibromyalgia, the rheumatic diseases, drug side effects,6 vitamin D deficiency, and sleep deprivation.
There are many other kinds of pain, of course, but these are the ones most likely to benefit from heat. No one with appendicitis or a 2nd degree burn wants a nice hot water bottle.

Everyone loves a heating pad. But some love them even more.
What heat is not for
Heat will make some conditions much worse. Never apply heat to an infection or fresh injury! Or any other acute inflammation, like a flare-up of arthritis. Just don’t do it! That’s what ice is for: soothing inflamed tissue.
And what’s a “fresh” injury? Any time tissue has been physically damaged, it will be inflamed for a few days, give or take. If superficial tissue is sensitive to touch, if the skin is hot and red, if there is swelling, these are all signs that your injury is still fresh, and should not be heated.7
If there’s no obvious/severe injury or infection, it’s okay to try a heat treatment. But it can be surprisingly unclear!
It’s often really tough to tell how much inflammation is involved in pain. There are many kinds of pain, especially chronic pain, that exist in a grey area between “acutely/specifically inflamed” and “something else.”
An excellent example: muscle strains versus muscle “knots,” two common ways for muscles to hurt. A strain is an actual rip in the muscle — physical damage, definitely inflamed — while a “knot” or trigger point (TrP) is an irritable patch of tissue, probably a micro-spasm (more about this below). The difference between a minor strain and a bad trigger point can be subtle.8 And yet you probably want to heat the knot, but not the strain! Fortunately, if the strain is mild enough that you can’t tell if it’s a strain, it’s probably not a big deal one way or another: just try some heat and see what happens.
But there are many situations where this kind of ambiguity is a challenge, like low back pain.9
If you suspect a muscle strain, but you’re not sure, here’s a good tutorial for helping you sort it out: The Complete Guide to Muscle Strains If back pain is your issue and you’re not sure what’s causing it, get thee to another tutorial: The Complete Guide to Low Back Pain And I have an article specifically devoted to helping people understand why heating back pain is usually better than icing it: (Almost) Never Use Ice on Low Back Pain!

The hot water bottle: The classic original source of therapeutic heat.
How does heat therapy work?
The next several sections explore different mechanisms and details of how heating might be helpful to people in pain:
- Heat is reassuring, and reassurance is analgesic. (This is applied neurology, not just a psychological effect.)
- Heat can penetrate a few centimetres into tissue, and cells and biochemistry speed up when the tissue temperature rises, which might have therapeutic implications. For instance …
- Heat may have an effect on the common painful phenomenon known as “trigger points.”
- Heat may help soreness after exercise.
- Tiger Balm and similar products are “spicy” not warm, but they might tinker usefully with sensation: a neurological distraction.
Heat is reassuring, and reassurance is analgesic
Our comfort zone is a warm place. And so, almost no matter what kind of pain you have, “To reduce pain, we need to reduce credible evidence of danger & increase credible evidence of safety.” (Moseley)
The brain may interpret a safe source of warmth as good “credible evidence of safety,” for basic psychological reasons related to the environmental and social conditions we evolved in. Cold kills! Hypothermia has been at or near the top of the list of threats to our safety throughout all of prehistory and most of history.10 And we also associate warmth with contact and intimacy — another powerful goodness.
So a nice controlled source of warmth is probably just about the most basic reassuring thing there is. And that’s always good for pain … at least indirectly.
Comfort vs analgesia
Heat definitely is comforting, and people will invariably report that they enjoy their favourite thermotherapy, and most people do have a favourite … but enjoyment is not analgesia. We see this a lot in the world of pain treatment: things that feel nice, and therefore reduce the “suffering” that goes with pain … but they don’t reduce the actual pain.
Reduced suffering is inherently valuable, and — if you cannot get relief from the pain — it is still highly desirable to soften its impact on your psyche. Suffering and pain aren’t the same thing, but they do overlap and interact. It’s like wearing wool in wet weather: you won't be any less wet, but you will be better protected from its consequences.11
It’s all-too-easy to mistake sedation, euphoria, and/or a pleasant sensory experience for meaningful pain relief — and heat therapy is one of the most classic examples. For instance, in a 2024 study of electrically heated mittens for hand arthritis compared them to “cold” mittens — the same thing, sans power.12 The people who got the hot hands reported “a pleasant experience,” but even so they didn’t have less pain or more function. Heat, I am sorry to say, simply showed no real potential in that case. (It may well be different for pain of different kinds, of course.)
The heat works wonders on my lower back, which has been out for days from sleeping in the box.
Jason Dessen, Dark Matter, Blake Crouch
Heating time: how long does it take?
About fifteen minutes. There's actually a citation for this: Kominami et al. showed that it takes about that long for the skin to get as hot as possible at a reasonable, typical heating pad temperature.13 They also confirmed the relatively obvious: a hot pack alone cannot increase core temperature, regardless of location or body composition.
But surely the heat does get deeper than the surface? Yes, but not all that much …
Heating depth: how far does it go?
Roughly a degree Celsius or two at a couple centimetres depth, give or take, depending on how and where it’s done.
Scientists have tested this. For instance, in 1998, Draper et al. heated subjects’ triceps muscles with hot packs for fifteen minutes, and then checked their temperature with a needle probe — like a very thin meat thermometer (don’t worry, they were anaesthetized).14 They found an average increase of 3.8˚C at a depth of one centimetre, and .78˚ at three centimetres.
I think this data clearly shows that superficial heating is an easy way to modestly increase tissue temperature up to a couple centimetres — which is most of the volume of most muscles — for whatever that’s worth. The 3.8˚C increase in the muscle shallows is something, but .78˚ change at 3cm depth — and a lot of muscle is that deep — is clinically trivial, well within the range of healthy variations in core body temperature.
Heat for trigger points
A trigger point is a small patch of acutely sensitive soft tissue, a poorly understood little patch of sensory misery. They are probably contracted, stagnant, swampy15 sections of muscle tissue — but that’s just a theory.16
However they work, no one doubts that these sensitive spots in muscle are common. They can cause anything from stiffness and dull aching to show-stopping agony. The pain often spreads in confusing patterns, and they grow like weeds around other painful problems and injuries, making them interesting and tricky and incredibly common.
And heat seems to be a particularly good therapy for trigger points. Never formally tested! But plausible.
Pure speculation about why heat might be good for trigger points
Trigger points are probably aggravated by stress, and (as noted above) being warm is a pleasant and comforting sensation, as long as we aren’t overheated to begin with. But it probably goes beyond that …
Relaxation reduces resting muscle tone. You can have “tight” muscles without actually being in frank spasm. There are many degrees of muscle tone between deep relaxation and a charlie horse. Many otherwise healthy people live in a state of uncomfortably high muscle tone, their muscles always a little clenched and exhausted, probably with some specific areas even worse from awkward working postures. This state is inherently uncomfortable, like being tired from exercise — but without the endorphins — and it may be fertile ground for trigger points. If so, any reduction in muscle tone may be quite helpful.
Electric heating pads have been around for as long as we’ve have any kind of electric appliances.
Heat for soreness after exercise
Perhaps the most popular therapeutic reason to get into a hot tub is to try to beat the pain of DOMS (delayed-onset muscle soreness) — that nasty 24–28 hours of muscle pain you get after unfamiliar exercise. But DOMS is mostly invincible. Researchers have proven over and over again that there really is no effective treatment for it.
Except, maybe, heat?
For a long time, “warm underwater jet massage” — hot tub jets — was the only treatment that had ever shown any potential, in a 1995 study.17 But it was a small and flawed piece of research — and most people know from personal experience that a soak in a hot tub may “take the edge off,” but hardly constitutes a miracle cure for DOMS. I mostly ignored that evidence.
In 2006, we got some good science news: more persuasive data, surprisingly good results in treating DOMS in the low back with a “heat wrap,” a wearable device that applies heat for hours at a time.18 Another small study, but this time a more persuasive one. Eureka? Proof needs more data, but this makes it well worth trying heat on your sore muscles after exercise. Happy heating!
Is Tiger Balm hot?
Ointments and balms like Tiger Balm19, RUB A535, and Deep Heat are not truly hot, but “spicy” — some of them literally, because they contain capsaicin, the active ingredient in chili peppers.
Other ingredients also stimulate and irritate in a variety of ways, many of them reddening the skin, which is why they are generally known as rubefacients (and there’s your word-of-the-day).
The product name “Deep Heat” always makes me roll my eyes, because a more truthful name would be Shallow Irritation! “Chemicals that are mild skin irritants may make a patient feel warm,” wrote Borrell et al., “but they will not produce any in vivo temperature rises or any of the physiological effects of heat.”20
Capsaicin stimulates precisely same nerves that detect scalding heat, creating an effective illusion of a burn — a mild one at small doses, or a full-blown nasty one at high doses. Sounds awful! But this has many fascinating and potentially therapeutic implications. This topic is explored in great detail below in the members-only area, but here’s a high-level overview. There are four ways that capsaicin might be therapeutic, which correspond roughly to dosage and the intensity of burning pain produced:
- 🌶 Mild — Small doses of capsaicin can feel pleasantly warm, simulating a heating pad with biochemistry. This is the most basic rationale for spicy body rub products: they just feel nice, and it’s convenient. That’s it!
- 🌶🌶 Medium — Capsaicin in a dose high enough feel to like a mild burn may be a particularly effective "sensory distraction" from pain due to the unique combination of safe but intense sensation.
- 🌶🌶🌶 Hot — Capsaicin in substantial and repeated doses may “burn out” TRPV1 receptors, reducing their ability to respond to other noxious stimuli (like inflammation).
- 🌶🌶🌶🌶 Insane! — High-concentration capsaicin is a mild neurotoxin, which may produce a more profound effect, actually pruning the nerves.
High-concentration capsaicin is serious business and requires medical supervision. Do more tolerable doses achieve anything for typical aches and pains? Alas, no one actually knows. Despite these remedies being among the most common and oldest of all medicines, the evidence is “very low quality and typically limited to single studies or comparisons with sparse data.”21 It’s clear that they don’t work any miracles, of course. But it’s equally possible that they actually are helpful for many people. A 2018 review was slightly more optimistic, concluding that capsaicin seems to be roughly as good for as common over-the-counter medications, but also noted the “limited and poor quality evidence.”22
If you don’t mind feeling burned, capsaicin is probably worth a shot, and real harm is unlikely if you exercise any caution at all — capsaicin’s bark is way worse than its bite. But it’s also not likely to deliver much relief, and I’ll wager it’s just going to be a clean miss with lots of types of pain.
Note that many rubefacients also have touted other medicinal and pain-killing ingredients and mechanisms. For instance, garlic is supposed to be good for all kinds of things, and salicylates are definitely medicinal in some applications. But of course any such benefits are just bonus prizes that have nothing to do with heating or rubefacients, and it’s a rogues’ gallery of mostly unexciting possibilities.
That’s the basics of spice therapy. But there is so much more to know it’s almost unbelievable…
The next part of the article is a members-only deep dive into a major sub-topic, spice therapy. There are about two dozen sections devoted to it, about 6,500 words or 25 minutes of extra reading. It begins with a major digression into some basic science about receptor proteins, and then comes back around to a detailed exploration of using spicy heat to treat pain. Much of this is well beyond the scope of any typical article about therapeutic heat, but this is exactly the kind of intense exploration of the dorky details that PainScience.com is all about. But free reading about heat therapy continues below, for a total article size of 15,000 words.
Most PainScience.com content is free and always will be.? Membership unlocks extra content like this for USD $5/month, and includes much more:
Almost everything on PainScience.com is free, including most blog posts, hundreds of articles, and large parts of articles that have member-areas. Member areas typically contain content that is interesting but less essential — dorky digressions, and extra detail that any keen reader would enjoy, but which the average visitor can take or leave.
PainScience.com is 100% reader-supported by memberships, book sales, and donations. That’s what keep the lights on and allow me to publish everything else (without ads).
- → access to many members-only sections of articles +
And more coming. This is a new program as of late 2021. I have created twelve large members-only areas so far — about 40,000 words, a small book’s worth. Articles with large chunks of exclusive content are:
- Quite a Stretch
- Does Epsom Salt Work?
- Heat for Pain and Rehab
- Your Back Is Not Out of Alignment
- Trigger Point Doubts
- Does Fascia Matter?
- Anxiety & Chronic Pain
- Does Massage Therapy Work?
- Does Posture Matter?
- A Deep Dive into Delayed-Onset Muscle Soreness
- Does Ultrasound or Shockwave Therapy Work?
- A Painful Biological Glitch that Causes Pointless Inflammation
- Guide to Repetitive Strain Injuries
- Chronic, Subtle, Systemic Inflammation
- Vitamins, Minerals & Supplements for Pain & Healing
- Reviews of Pain Professions
- Articles with smaller members sections (more still being added):
- → audio versions of many articles +
There are audio versions of five classic, big PainSci articles, which are available to both members and e-boxed set customers, or on request for visually impaired visitors, email me. See the Audio page. ❐
I also started recording audio versions of some blog posts for members in early 2022. These are shorter, and will soon greatly outnumber the audio versions of the featured articles.
- → premium subscription to the PainSci Updates newsletter +Sign-up to get the salamander in your inbox, 0–3 posts per week, mostly short, sometimes huge. You can sign-up for free and get most of them; members get more and their own RSS feed. The blog has existed for well over a decade now, and there are over a thousand posts in the library. ❐

Change or cancel plans any time. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism. For more information, see the membership page. ❐
PREVIEW: Headings in the members-only area…
- Proteins! How do they work?
- Dr. David Julius versus the spice
- A protein for every stimuli
- Piezo1 and Piezo2 use the force
- Spice therapy
- Slow-motion capsaicin craziness: my strange first experience
- The proteins of danger!
- Threatening heat
- But “some like it hot”
- Where are all these receptors anyway?
- Abused term #1: “pain receptors”
- Abused term #2: “noxious stimuli”
- Threatening spice: TRPV1’s spicy side effect
- Why the sensitivity to something that isn’t actually much of a threat?
- With spice, context is the whole enchilada
- Yeah, but what can we do with all this beautiful knowledge?
- Heat in a tube: mild spice therapy 🌶
- Red rub, red rub! The rubefacients
- Counterstimulating with capsaicin: medium spice therapy 🌶🌶
- Potent but safe? Premium counter-irritation
- Down-regulation station: hot spice therapy 🌶🌶🌶
- An example: how capsaicin might help a problem like tendinitis
- Barfing interlude: what does capsaicin have to do with violent vomiting?
- Insane spice therapy (actually a thing) 🌶🌶🌶🌶
- Post-herpetic neuralgia as the perfect target for high-dose capsaicin
- Capsaicin as a neurotoxin
- Clinical efficacy of non-insane spice therapy
The proteins of pain, scalding heat, and spicy heat —
And how we might be able to exploit them therapeutically
How do physical stimuli turn into sensations? How exactly do we turn what’s around us into nerve impulses? “Transduction” is one of my favourite concepts in biology: the conversion of forces into electricity. We are all familiar with transduction in outline. For instance, we know that photons strike cells in our retina and trigger nerve impulses. But exactly how does that kind of thing work?
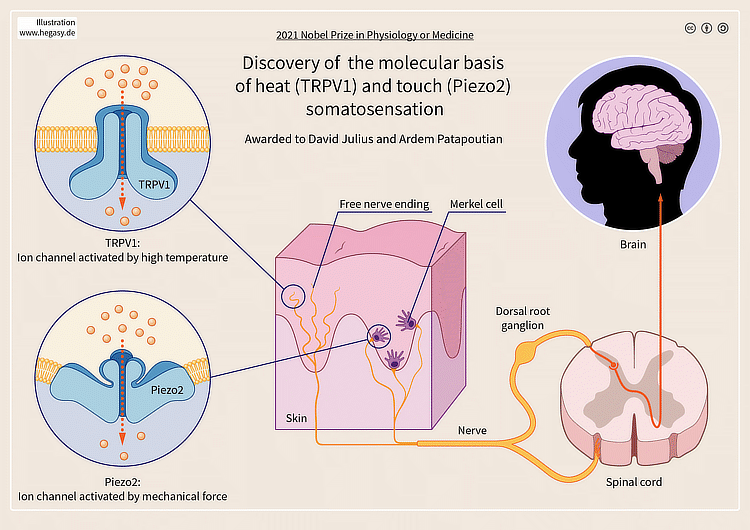
Some of these mechanisms remain unsolved mysteries of molecular biology, but others are now almost well understood. David Julius and Ardem Patapoutian just shared the Nobel for Medicine or Physiology for their discovery of proteins that transduce some basic stimuli into nerve impulses. It’s all dizzyingly complex, of course, but it can be oversimplified down to this: they enable us to detect heat, cold, and pressure.
And this all about pain, too. Because extremes of temperature and force are dangerous! So these proteins are also the most basic components of our alarm systems.
These discoveries are only about ten to twenty years old, and have been followed by many more like them, the dawn of a much more detailed science of sensation.
Let the digression begin…
Proteins! How do they work?
The most specific explanation possible for most biological marvels is proteins. One way or another, it’s usually about the proteins. But how does a protein help us feel anything? Proteins are mind-bendingly complex little nanomachines, effectively black boxes with intricate clockwork-like guts we can barely comprehend. But we know some things about what they react to and how.
The Nobel proteins are “receptors,” embedded in cell membranes with their heads and antennae sticking out, and their tails on the inside. They are “pores” in the cell of the skin that can open or close. When exposed to the right stimulus, they warp and wiggle in an instant, opening a channel for a flood of ions (atoms with a charge). This why you can also call them “ion gates,” which sounds very sci-fi. If enough ion gates open at once, they triggers a nerve impulse — a signal about something happening around the cell, like “heat!” or “mechanical deformation!” or “Klingons on the starboard bow!”
Or “spice!”
Dr. David Julius versus the spice
The first of the Nobel proteins is often called the “capsaicin receptor,” because it reacts to the active ingredient in chili pepper. It was discovered by looking for the genes that cells need to make that receptor. His lab tested many genes, until they found one that could, when expressed in cultured cells, make them sensitive to capsaicin.23 It was 1997, and this was all much more difficult and tedious back then.
This protein’s true and full name is Transient Receptor Potential Cation Channel Subfamily V Member 1, or TRPV1 for short. And it doesn’t just respond to spice. It also responds to scalding heat — which is why “spicy” and “hot” are literally the same sensation, just with different significance. The day that was noticed, someone in that lab surely said, loudly, “Holy shit!” Probably all of them. That’s how scientists say “eureka” these days.
It’s weird and fun that this one receptor detects two kinds of heat.
And TRPV1 has more tricks up its intricately folded sleeve. It’s a gifted protein that also reacts to the active ingredients in mustard and wasabi, to acidic conditions, to inflammatory molecules, and to some cannabinoids, like anandamide (which is quite similar to THC). (Detail: Capsaicin is called a vallinoid, which is a cool word for a family of molecules related to, yes, that vanilla.)
So what does TRPV1 do? Lots.
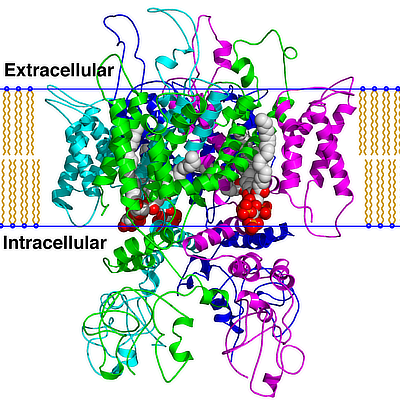
A diagram of the structure of the TRPV1 protein, which contains about 800 amino acids. Imagine how many different ways there are to arrange a chain with 800 links. This is large for a protein in a human cell, but not the largest. The mean is 431, and the top of the scale is about a thousand (excluding a few freaks like titin at ~30,000).
A protein for every stimuli
Before the ink was dry on their original report, Dr. Julius and his team were already looking for a protein that transduces the feeling of a cool spring day — a cold receptor, a protein that lets the ions flow at a much lower temperature. Meanwhile, Ardem Patapoutian was doing the same thing! Both labs then independently and simultaneously discovered TRPM8, an ion gate opened by temperatures of 20˚C, give or take a few, instead of TRPV1’s 40˚C.
And there are still other proteins that open like flowers in different temperatures, each one covering a section of the thermometer. And the discoveries of TRPV1 and TRP8 triggered a research rush to identify other kinds of receptors. The basic mechanisms of touch were still unknown at the time, and especially tantalizing.
How does squishing tissue turn into the perception of pressure?
Papoutian’s team pursued this, earning the other half of the Nobel. Charmingly, they started out by identifying natural cells that were sensitive to touch by poking them, microscopically. I am not joking: they literally poked cells with a microscopic stick until they found ones that responded with a little “spark” of electricity.
They finally found that spark, and then they “just” had to identify the spark plug: the protein that was reacting to the poke. They found two: Piezo1 and Piezo2 were announced in 2010.24 And that is why Patapoutian is sharing a prize with Julius.
Piezo1 and Piezo2 use the force
Piezo1 and Piezo2 both react to the flexing of the cell membranes in which they are thickly embedded, like rhinestones on an Elvis impersonator. The deformation of the cell membrane is a microcosm of a thumb pressing into your skin, which bends the membranes of the nerve cells in the area, opening millions of Piezo1 and Piezo2 proteins, so that kajillions of ions can pass through them, triggering nerve impulses.
This is scientific reductionism at its most dazzling, revealing the exotic nano-scale engines that power familiar human experiences, the answer at the end of a chain of child’s “but why” questions.

The thumb bends the skin, flexing the membranes of every cell in the area. Proteins embedded in the cell membranes, Piezo1 and Piezo2, transduce the flexion into nerve impulses.
But they also power un-familiar human experiences! What we consciously feel thanks to the Piezo proteins is the tip of a mighty iceberg of subtle sensation. The biological power and utility of these engines is breathtaking. They are responsible not just for the pressure component of touch, but a truly staggering variety of other biological signals, from knowing when your bladder is full to the position of your limbs are in space to which direction your eyes are pointing.
Piezo1/2 are not just the engines of touch, they are also the engines of the greatly under-appreciated “sixth sense,” proprioception, the sense of position and movement. If all your Piezo receptors vanished, it would probably kill you in seconds or minutes — that’s how much your physiology depends on knowing when tissues are stretching, flexing, twisting, and compressing.
Spice therapy
Recently I bought this capsaicin product for the first time:
I was oblivious to the long history of this brand’s cultural appropriation, going back to the mid-2000s. But I wanted to test capsaicin on my Achilles tendinitis — another problem with a history going back to the mid-2000s. But this was the only product on the shelf that actually had capsaicin (the Tiger Balm and A535 did not).

Slow-motion capsaicin craziness: my strange first experience
The first time I used this product on my poor tendons, nothing at happened at all for a whole afternoon — no sensation! I might as well have applied moisturizer. A second modest dose produced only a slight tingling that evening. I went to bed with mildly toasty heels… and then woke up with over-toasted heels.
They felt like they had actually been burned. It was awful. I did not sleep well that night. “Therapy.”
The strange delay was not a fluke. When I dared to try again a week later, it all happened again. A single small dose midafternoon was undetectable for the rest of the day, but then I was awoken by pain at 2AM that blasted a three-hour hole in my night. Oops. Not worth it!
So what the heck is up with these capsaicin receptors, and what was I hoping to achieve by spicing my heels? This experience “inspired” me to dive even deeper into this topic again. It synchronizes perfectly with the protein science that got me thinking about spicing my heels in the first place, which is all about threat detection: dangerous extremes of heat and pressure.
The proteins of danger!
Being an organism is perilous. Every living thing needs to know when it’s being poked, specifically and especially whether or not it is being done too hard. We also have to know when it’s too hot or too cold. Pressure and temperature detection are about as elementary as sensation gets. Many simple organisms can do as much, even the ones that have only a single cell.
Extremes of pressure and temperature are usually experienced as an alarm — as pain — ideally before any damage is done.
Of course we also need to know when it’s too late and we’ve actually been damaged — nothing is more dangerous than already being hurt (because it involves serious vulnerability to getting hurt even more). And these receptors are partially involved in that too. For instance, TRPV1 also reacts to inflammation.
Almost everything biology has eighteen jobs.
TRPV1 also detects … spice. Which is not threatening, but absolutely can feel like it. But spiciness is not for the birds… which is why the plants use it! An explanation of that weird sentence below.
Also: How hot can you take your bath? How can the same pressure be bliss for one person and torture for another? Finally I will track the biological oddity of spicy heat to a cool clinical question: can we exploit the nature of TRPV1 receptors to treat pain?
Threatening heat
What is “scalding” heat? 40˚ Celcius is the low end. That’s the temperature, roughly, that opens TRPV1 ion channels — a temperature right on the edge of what’s tolerable.
How do hot do you like your hot tub? 40˚ is about as high as most people want to go, and some don’t even want that (my wife again). I am fine at 40˚, wincing at 41˚ but still loving it, and I start to struggle at 42˚. In the space of 3 degrees, my reaction goes from “meh” to “ack!” All thanks to more and more TRPV1 receptors getting triggered.
Note that 40˚ is also the temperature a high fever. Curious that we have a protein dedicated to detecting our maximum tolerable temperature — inside or out. Curious & a bit profound.
Hot tap water ranges from 38–45. My home’s tap water is at the high end, and I can barely wash my hands in it — I can only do it fast, saying “Ooh ooh ooh!” My wife won’t touch it.
But “some like it hot”
Whether there’s enough heat to feel painful is partially just a matter of literal degrees. More degrees means more TRPV1 reacting. On a cold day, your TRPV1 proteins are mostly still and quiet. In a scalding hot shower, billions of them are getting busy. If you are actually scalded and burned… trillions.
But it’s not just quantity, it’s also context. If someone aggressively rushed up to you on the street and threw a bucket of 41˚ water on you, you’d scream like you were being burned alive — even though that cannot actually damage you. On the other hand, you can slip into a 46˚ steam room and think it’s bliss, at least at first… but that actually can burn you.
That’s the brain getting involved in interpreting the potential meaning of all that TRPV1 signalling, and modulating our perception accordingly. And aside from the temperature itself, the most important contextual clues are the area of skin exposed to scalding heat and how quickly that exposure happens.
Rapid full-body immersion in 42˚water is brutal — most people just can’t do it. But slowly inserting just your hands into a sink at 44˚ is no problem at all for most people. The rate and extent of the activation of TRPV1 receptors are valuable clues about potential threats that the brain takes super seriously.
Where are all these receptors anyway?
Receptor proteins are sprinkled everywhere in human physiology, but they are clustered the most thickly on nociceptors — the nerves most specialized for detecting potentially dangerous stimuli. And they are the thickest of all where they are most likely to encounter the stimuli they exist to detect — so there’s a lot of them in the skin.
Piezo1 and Piezo2 are also dense in the walls of hollow organs. To detect stretch. How else will you know when it’s time to pee?
Abused term #1: “pain receptors”
Some people will call these proteins and their host nerves “pain receptors,” but that’s definitely oversimplifying things dramatically, to the point of error (even more so than my “proteins of pain” title).
Pain is not a thing in the world to be detected. Even the output of nociceptors is not yet pain, let alone the input.
Proteins transduce the stimuli, they don’t interpret it. The nerve cells pass the message along, but they don’t editorialize.
Abused term #2: “noxious stimuli”
The term “noxious stimuli” is similarly abused, as if it was the same thing as pain. But these stimuli are not inherently noxious — they are only threatening in excess or depending on what caused them. Both heat and pressure can easily be excessive and dangerous, but usually these stimuli are minimal and completely safe… and yet still extremely useful.
For instance, squirming is inspired by the information we get from pressure receptors. We are bombarded by constant low-priority data about the need to shift position because there’s been some pressure on this or that spot for too long. It’s nowhere close to “dangerous” yet — but if we didn’t move, those spots would become pressure sores.
Threatening spice: TRPV1’s spicy side effect
TRPV1 is also a capsaicin detector… by accident. It responds to capsaicin, the active ingredient in all kinds of chili peppers. The response is proportionate to the dose, and it can be potent indeed, but we can detect even teensy traces of capsaicin in places that have many TRPV1 receptors, like tongues.
And eyeballs.25
Good as we are at detecting capsaicin, it’s mostly harmless. It feels much more toxic than it is. Even large doses of capsaicin are surprisingly harmless — even people who get pepper sprayed right in the eyes can fully recover.
Why the sensitivity to something that isn’t actually much of a threat?
It’s probably a bug, not a feature — our branch of the tree of life is just good at detecting this stuff by accident, a side effect of how our heat transduction works. But nature has made good use of it anyway, as explained by Nature in 2001.26 Plants probably produce capsaicin because it “selectively discourages vertebrate predators” — they mean us, because we happen to be sensitive to the stuff — but “without deterring more effective seed dispersers,” like birds, who happen not to be sensitive to capsaicin.
You cannot irritate a bird with spice. Like honey badger, they just do not care.
So here’s a thing that can cause pain — not because it’s a threat, but because it sets off the same receptor that does detect dangerous heat. That makes it really interesting. It means that it feels a lot more harmful than it is, and therefore that context is a major factor in how we experience it.
With spice, context is the whole enchilada
Your brain is aware that the “scalding” heat on your arm is actually just Tiger Balm, and not a burning hot ember from a campfire. It doesn’t need to warn you about Tiger Balm nearly as urgently. And so literally the same signal, starting with TRPV1, causing nerve impulses in nociceptors, may or may not be painful depending on… the situation.
But if you pop a whole Carolina Reaper chili into your mouth — 200 times hotter than a jalapeno — and the absurd amount of capsaicin will jam open every TRPV1 ion channel you have, generating more impulses from those nerves than your brain has ever seen… and you’re going to freak out.
I mean really freak out. The effect is harsh.
A large overdose of capsaicin is effectively indistinguishable from a serious burn, as far as the brain is concerned. While no direct harm will come of it — capsaicin is quite safe — people will suffer extreme pain, reacting as if they had actually swallowed boiling water: tremors, nausea, vomitting… for days. The pain is so intense that it probably causes panic attacks in many people (and panic attacks can often make people think they are dying).
And yet people still flirt with this experience! Because context is that powerful, and pain can literally be fun when you know it’s safe.
There’s an entire fascinating book about that: Hurts So Good. I look forward to reading and reviewing that one.
Yeah, but what can we do with all this beautiful knowledge?
There’s some lovely science here, but is it useful? Can we apply it? Can any of this knowledge help pain as well as tickle your brain? Maybe.
There are, of course, many possible clinical implications of the “proteins of pain.” But for our purposes here we’ll focus on one of the big ones, spice therapy, the use of capsaicin to manipulate sensation mediated by TRPV1 receptors.
The general idea here is that capsaicin can trigger TRPV1 receptors with a strong but relatively harmless stimulus. That main idea breaks down into four more specific ones that have been used to explain capsaicin as a pain medication. They correspond roughly to dosage and the intensity of burning pain produced:
- 🌶 Mild — Small doses of capsaicin can feel pleasantly warm, simulating a heating pad with biochemistry. This is the most basic rationale for spicy body rub products like A535: they just feel nice. Heat you can apply wherever you like and walk around with easily is just more convenient that stuffing a hot water bottle into your shirt.
- 🌶🌶 Medium — Capsaicin in a dose high enough feel to like a mild burn — and we know that this is literally what it feels like — may be a particularly good way to “distract” the nervous system because of the unique combination of safe but intense sensation.
- 🌶🌶🌶 Hot — Capsaicin in substantial and repeated doses may “burn out” TRPV1 receptors, reducing their population and sensitivity, which in turn reduces the amount of signalling they can produce in response to other noxious stimuli — like inflammation.
- 🌶🌶🌶🌶 Insane! — Capsaicin in large doses is a mild neurotoxin, which may produce a more profound effect, shrivelling TRPV1-containing nerve endings like salted slugs.
All of these mechanisms have been used to justify spice therapy over the years, but they all have the same basic form: applying capsaicin to the skin.
The capsaicin in chili peppers stimulate TRPV1 receptors. So does heat. So do some molecules of inflammation. This overlap produces some fascinating implications.
Heat in a tube: mild spice therapy 🌶
Ointments and balms like Tiger Balm, RUB A535, Deep Heat, Zostrix and many others are not actually hot, but literally feel like it, because they stimulate the TRPV1 receptors that also respond to scalding heat.
Other than contextual clues, our nervous systems literally have no way of telling the difference. A little capsaicin feels like a mild burn, like the early stages of a sunburn.
That can feel “nice” to us.
These burning sensations are widely regarded as therapeutic! The rationale for this is not immediately obvious, and the popularity of these remedies precedes our comprehension of TRPV1 ion channels by most of human history. But it’s also still not clear that we understand if or why they are helpful.
They can feel nice though. They are indeed “warming.” And humans do like a bit of that. Heat rarely works miracles for any kind of pain… but I would also never want to give it up as an option. Mild spice therapy is perfectly justifiable in that spirit.
Red rub, red rub! The rubefacients
These nostrums are sometimes classified as “rubefacients” (and there’s your word-of-the-day) because many of them cause reddening of the skin. Not all them. In fact, this is not actually due to capsaicin, which — surprisingly — does not actually turn the skin red.27
However, many of these products contain other compounds that do increase superficial circulation, for whatever it’s worth.28 It’s also worth noting that many of them do not actually contain capsaicin at all, including classic Tiger Balm (although the company does make other products that contain it).
Counterstimulating with capsaicin: medium spice therapy 🌶🌶
“Sensory distraction” is another classic rationalization for how therapy works (much like increasing circulation). It’s probably more legitimate, however.
One sensation can “pre-empt” another to some degree. This is known as counterstimulation, and it is certainly a real thing — it is firmly based on the well-known neurological principle of “gate control.”29 The canonical example is the way we instinctively rub tissue around acute minor injuries.
If we counterstimulate one noxious stimuli with another, it’s counter-irritation.
Counterstimulation is a real thing, but not an especially potent thing. You could call it another tool for the pain treatment toolbox, but it’s not an impressive tool. Maybe just like a small screwdriver or a tack hammer.
But counterstimulation with capsaicin might be different.
Potent but safe? Premium counter-irritation
There are lots of potent but hazardous sources of counter-irritation. Hitting your hand with a hammer would also be an impressively effective counter-irritant, but I don’t recommended it.
The discomfort of capsaicin overdose can be shockingly intense while remaining almost perfectly safe (another weird thing about capsaicin, discussed in more detail in the last post). That combo of a strong source of sensation that is also actually safe might make capsaicin a more premium counter-irritant than other options — more irritating! More countering!
If capsaicin is a good counter-irritant, it strongly suggests a promising usage strategy: don’t just apply capsaicin to the body part that hurts. Apply it in patches nearby, as well as other patches distributed around your body. Give your body multiple “burns” to process. I think it’s quite likely that this strategy would be more efficacious. Naturally this hypothesis has never been tested.
Down-regulation station: hot spice therapy 🌶🌶🌶
We can become more or less sensitive to stimuli by a variety of mechanisms. Nerves fire in response to specific chemicals. The number of receptors they have for specific chemicals is “regulated,” and they can be regulated “up” or “down.” If you flood a nerve with too much with a specific chemical, it will get “numb” to it — by downregulating the number of receptors for it.
Clever system.
TRPV1 receptors can be downregulated if persistently drenched in capsaicin. Nerve cells exposed to lots of capsaicin start reacting to it less over time. And if the nerve cells have downregulated their populations of TRPV1 receptors… then they have also become numb to scalding heat. And that works, which we have known for decades.30 But it’s also not very useful.
But if that works, then they may also get numb to inflammatory triggers — and that might be extremely useful (but has never been demonstrated, as far as I know).
It’s not clear how long it takes, but it’s quite a while.
And it’s not clear how much capsaicin this takes, but it’s more than just a little. Simone et al. used 0.075%, three times more than the concentration I struggled with. And low-dosages might actually backfire and cause sensitization — an effect that has been demonstrated!31
And there are probably many unknown and unknowable variables affecting all of that in different ways for different people at different times.
But the general principle is sound: it’s almost impossible not to downregulate TRPV1 receptors if you just throw enough capsaicin at them.
And there’s another interesting mechanism that’s probably at work: a lot of capsaicin probably also changes how the TRPV1 protein behaves, making it less responsive to more capsaicin — just pure biochemistry, a quirk in how the protein changes in response to a lot of capsaicin. So they can probably be downregulated and desensitized.
An example: how capsaicin might help a problem like tendinitis
This is how I rationalized using capsaicin on my own Achilles tendinitis:
- My tendons are persistently inflamed. (Yes, they are! Inflammation has been demonstrated in chronic tendinitis, despite the popular contrary view that they are “not inflamed.”32)
- At least part of the reason that they hurt is that my TRPV1 receptors are responding to the presence of molecules of inflammation. (There is undoubtedly more to it, of course.)
- If I flood that superficial tissue with capsaicin, I might reduce the population of TRPV1 receptors and desensitize the remainder — and so I might also not feel the inflammation as intensely.
But the burning of the capsaicin was just too severe — and too weird with it’s timing, surging in the middle of the night — so I gave up after only a couple of days. I probably didn’t get to the “downregulated” and “desensitized” part. 🤷🏻♂️
Barfing interlude: what does capsaicin have to do with violent vomiting?
Cannabis can cause a severe and surprisingly non-rare violent vomiting problem called “cannabinoid hyperemesis syndrome.”33 It probably does this by “burning out” TRPV1 receptors (downregulation again)… which are sensitive to cannabinoids! (In addition to scalding heat, capsaicin, and inflammation!) No one knows for sure, but that’s the most likely reason. Widespread downregulation of TRPV1 receptors causes vomiting! Maybe. The details are hazy.
These tragic patients — it really is an awful thing — habitually self-treat with the hottest showers and baths they tolerate. They may be trying to compensate for the lack of TRPV1 receptor activity with a different and strong source of stimulation for them.
So… how about capsaicin? That’s another source of strong stimulation for TRPV1 receptors! Gold star if you saw this coming. See Moon et al. for a good technical summary of the rationale (there’s a nice diagram I can’t use, because copyright).34
The logic is simultaneously based on some seriously advanced biology … and yet it kinda boils down to “well, let’s try to give those TRPV1 receptors a good kick,” like Fonzi bashing an appliance.
Alas, it doesn’t seem to work terribly well, despite the clever rationale.35 But it is, at least, a really interesting idea.
Insane spice therapy (actually a thing) 🌶🌶🌶🌶
“I say we take off & nuke the entire site from orbit. It’s the only way to be sure.”
Earlier I called over-the-counter topical capsaicin a tool, but an unimpressive one, “maybe a small screwdriver.” But the dosage makes the poison. If the dose is small enough dose to feel mild, it’s probably not doing much; and if it’s doing something, it probably doesn’t feel mild! So, how much capsaicin to make it into a crowbar?
High-dose capsaicin has actually gotten some high fives and thumps on the back from science, specifically for treating neuropathic pain with disturbingly high doses36 How much are we talking about?
8% capsaicin. Eight! Percent! Compare that to .025% capsaicin in a typical over-the-counter product — like the one that I put on my Achilles tendinitis. 8% is three hundred and twenty times more.
Even far saner dosages can be extremely intense sensory experiences. It’s important to understand that this will make you feel as if you’ve been badly burned. This isn’t user-friendly medicine. It isn’t something you can do for yourself, or would want to: “It must be applied under highly controlled conditions, normally under local anaesthetic, due to the initial intense burning sensation it causes.” For pity’s sake, why?
You have to be desperate.
Post-herpetic neuralgia as the perfect target for high-dose capsaicin
Shingles is notoriously painful, but do you know what’s worse? Shingles pain that keeps going, long after the rash and blisters are gone: post-herpetic neuralgia, one of the most vicious of all chronic pain syndromes. Of course it varies in severity, but for some patients it really is just like the shingles never really ended. 😱
Despite all the misery I have endured from fibromyalgia (unexplained chronic widespread pain), I know that it’s nothing compared to “infinite shingles.” People with post-herpetic neuralgia are willing to do almost anything to try to shut those nerves up. Including a third degree burn. “Kill it with fire”!
Or at least something that feels like that. Like high-concentration capsaicin.
Capsaicin as a neurotoxin
The idea with high-concentration capsaicin is to shoot past mere “downregulation” and have a more profound effect on the neurons — downright neurotoxic in fact, poisoning them, actually making their tips shrivel and retreat from the insane stimulus. This does happen.37 Interesting stuff.
But does it work clinically? Does poisoning those nerve endings translate into a reduction of neuralgia?
It actually does for a select few. According to Derry et al., some people do quite well with this approach — while most do not.38 There’s probably some genetic or biological x-factor, something we can’t identify in advance.
This is not promising for the average mediocre pain problem. But, if I had post-herpetic neuralgia, I’d probably roll that dice.
Do tolerable doses achieve anything for typical aches and pains?
Clinical efficacy of non-insane spice therapy
We’ve discussed multiple plausible and interesting mechanisms for pain relief from mild, medium, hot, and insane dosages of spice therapy. But we have half decent efficacy data only for the insane dosages.
Welcome to the science of pain, where hardly anything that normal people actually do for their pain is ever properly tested.
The same folks who reviewed high-concentration capsaicin also reviewed low-concentration and found the evidence to be “very low quality and typically limited to single studies or comparisons with sparse data” (Derry et al. again).
Notably, even low concentration capsaicin caused lots of adverse events and withdrawals of study subjects compared to placebo. That’s what happened to me with my heels. If I’d been in a study, I would’ve dropped out, because yikes. And that was with .025% capsaicin.
A 2018 review was slightly more optimistic, concluding that capsaicin seems to be roughly as good for as common over-the-counter medications, but also noted the “limited and poor quality evidence.”39
If you don’t mind risking feeling a bit burned, capsaicin is probably worth a shot, and real harm is unlikely if you exercise any caution at all — capsaicin’s bark is way worse than its bite. But it’s also not likely to deliver much relief, and I’ll wager it’s just going to be a clean miss with lots of types of pain.
•
And that concludes this tour of protein-inspired spice therapy science.
For many years, this article had only very basic coverage of the topic, and yet I have always known that it was biologically intriguing subject matter — and the whole point of PainScience.com content is to delve into stuff like this. Really wrapping my head around this topic was long overdue, and the Nobel prize finally pushed it to the top of my writing list.
I “grok” TRPV1 proteins, sorta, finally! Achievement unlocked.
Sort of? Writing this took about 20 hours of studying and writing and processing shower brainstorms. I looked at dozens of scientific papers. I estimate that I now know at least three percent of everything there is to know about the TRVP1 and Piezo1 and Piezo2 receptors, their many cousins, and how they relate to pain experiences and treatments.
As detailed as this is, it really is only the tip of the spiceberg.
↑ MEMBERS-ONLY AREA ↑
Local heating versus systemic heating
There are many ways to heat yourself up, but two broad categories: local and systemic.
Local heating means specific heating: applying a hot water bottle, heating pad, heated gel pack or bean bag to a specific place on the body.
Systemic heating means raising the entire body temperature with a bath or jacuzzi, steam bath, or piping hot shower — basically creating an artificial fever!

For most local heating, I recommend seeking out a large-sized (14 × 27) Thermophore, the Rolls Royce of heating pads: large, heavy, thick, and moist. Yes, moist — they produce a moist heat with “a special tightly-woven fleece blend cover which retains moisture from the air.” If you leave a Thermophore on a plastic surface, there will be beads of water under it five minutes later. The moisture captured from the air by the Thermophore conducts heat far more effectively than a dry heating pad. Luxurious! Both genuine Thermophores (roughly USD $50-100) and cheaper knock-offs (and probably nearly as good) can be ordered online from Relaxus.com, and are also available in some medical supply stores. Of course, Amazon.com has them, too.
Full-body heating in hot tubs, showers, saunas and steam rooms is also often a helpful factor with conditions where emotional stress and/or knots in your muscles are the cause of your troubles, or a significant complicating factor — low back pain is the most obvious example. See Hot Baths for Injury & Pain for tips on getting the most out of your bathtub or Jacuzzi. Believe it or not, many people do not really know how to take a bath! There are several simple tips that can definitely wring more therapeutic value out of the experience. (Adding Epsom salts to a bath is not one of them, however — it’s popular, but probably useless.40)
Even more localized heating + the relevance of climate and context
A reader question:
Is there a product that heats a very small area, like the size of a trigger point (which I’d say is ~ U.S. dime sized)? I could imagine something, kind of ball shaped at the end ... (b) Would heating just that small an area be of some value? I ask because roughly one third of the year (that includes right now), I don’t want to heat a big part of my body, except in the shower. It’s too hot! But I’d heat a very small area.
A home remedy version of this could be heating up a stone, which is easy enough.
Other than hot stone therapy (which usually involves many stones), there is no such product that I am aware of. (I was going to add “probably because it wouldn’t be efficacious,” but we live in a world of holographic bracelets and detox foot baths; efficacy isn’t exactly a prerequisite for selling something.)
If your environment is too hot for heat to be comforting and reassuring, then it’s unlikely to be helpful, and could even backfire to the extent that it’s actually perceived as a significant threat (although it takes quite a lot of heat to tip over into the threat zone). But it’s a highly idiosyncratic thing. There are people who love to bake themselves in direct sunshine, which I find intolerable. My wife will put a heating pad on under the blankets even in summer, which I cannot imagine tolerating, and her craving for heat surges even higher for treating aches and pains. But I too have suddenly found myself craving the heating pad in warm weather when trying to ease an unusually savage aching.
The threshold between pleasing and annoying definitely moves around!
I am confident that a tiny heater wouldn’t be very “comforting” or “reassuring,” though I find myself hard-pressed to say exactly why. It’s just not big enough to have much of a sensory impact, I suspect.
Although, if you’re cold enough to begin with, even a small source of heat is a comfort! Consider the context of an extremely cold environment — like, say, Canada (my home). Little glove and boot heaters are standard in the stores here, little chemical hot packs that fit in the palm of your hand. They feel great on a cold day, quite pleasant indeed. And those could conceivably be used with a therapeutic intent in a warmer environment.
Bottom line: very localized heating might be worth tinkering with if it seems appealing, but the uses and value are probably quite limited.
Warming with infrared radiation: infrared saunas, especially “far” infrared saunas
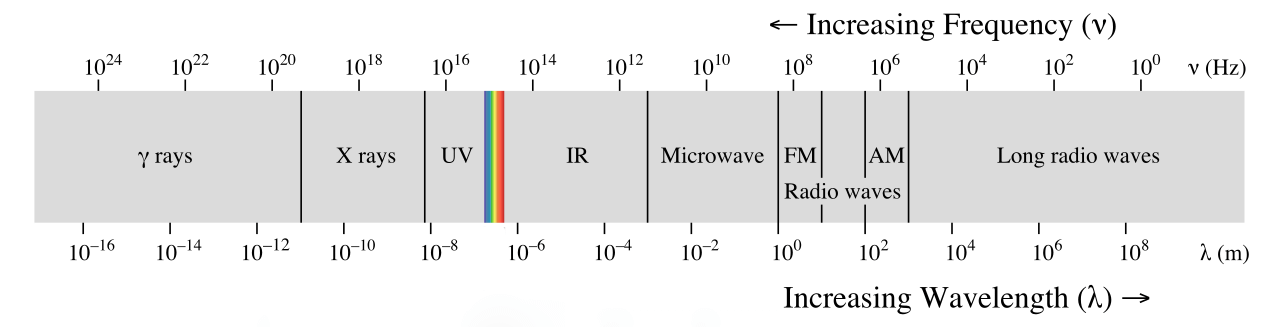
Infrared radiation is almost light — so close that it is often called infrared “light,” even though it is actually beyond the part of the electromagnetic spectrum that we can normally see. It has a longer wavelength than any visible light. And infrared is radiation is warming — it jostles our molecules — which is why it is also often called heat radiation.
Infrared saunas sound fancy, like they are emitting some kind of special radiation, not just heating rays but healing rays. In fact, an infrared heater is just a … heater. All heaters are infrared heaters, because all radiative heating is infrared. Calling it an “infrared radiation” heater is kind of like calling a lamp a “visible radiation” lamp. If you were to put a space heater in a small cedar panelled room, you would have yourself an infrared sauna.
If any infrared radiation is a healing ray, it’s “far” infrared radiation (farther from visible light, the longest infrared wavelengths). More expensive saunas use far infrared, and it is a bit different. The main advantage of using far infrared is entirely practical: they require minimal shielding, because the heating elements themselves stay almost magically cool while still heating up whatever they paint with their radiation (like you). So they can be built into the walls of the sauna without scorching them (or you). And that’s quite useful.
Manufacturers and resellers universally tout the penetrating quality of far infrared heating. Supposedly longer wavelengths “shine” right through superficial layers of tissue, heating deeper tissues directly, while sunlight heat is almost all in the near infrared that supposedly heats only the outer layer. (And we all know how unsatisfying warm sunshine is. 🙄)
In general, all infrared radiation penetrates tissue to some degree, just like visible light. But heat is heat, and all heat “penetrates” — via conduction. It’s just how it works. If far infrared can shine deeper into tissues — if — then those deeper tissues will get a head start. But those deeper tissues will get warm in a normal sauna too — it just takes slightly longer, via conduction. This is much like the difference between a microwave oven and a conventional oven: either way, food gets heated all the way through, it’s just a matter how efficiently it happens.
But it’s specifically far infrared heating that is usually touted as being particularly penetrative, and I have been unable to find a good source for this claim. The only widely cited source is a 2012 paper that makes the same claim but does not support it in any way,46 making it a classic example of a bogus citation. Even if it true, it is not actually supported by that reference.
Meanwhile, I have found precisely the opposite claim from other more credible experts, who say that far infrared is actually the least penetrative, and even shorter wavelengths don’t penetrate very far, only a few millimetres.47 (They don’t actually cite a source for their statement either, ugh, but the paper is much calmer and more trustworthy overall. If any of my readers can shed any light on this — a better source, perhaps — I’d be grateful.)
If that’s the best I can learn after a lot of searching, then the average sauna-shopper cannot possibly be expected to know what to believe. But for the sake of argument, let’s just say that far infrared is penetrative and then ask the really important science question here: so what if it does? There might be a subtle qualitative difference: that penerating radiative heat is just a little nicer than an intense conductive heating, which often involves temporarily over-heating the skin so that it will “soak in” quicker.
You want microwaves with that?
Far infrared heating is, in fact, almost microwave heating: they are immediately adjacent to each other on the EM spectrum.
Healing rays: is far infrared radiation special?
The only reason to think that “penetrating” heat matters is the idea that there’s something about far infrared radiation that is actually helpful to our biology in some way. And while there is endless speculation and belief that effects like this exist — for instance, there are very closely related beliefs about lasers, infrasound, ultrasound, and electric current — even though most enthusiastic experts concede that we don’t actually know. For instance, Vatansever and Hamblin (cited above) conclude their over-excited review like this:
If it can be proved that non-heating FIR has real and significant biological effects, then the possible future applications are wide ranging.
If. If! I can think of an awful lot of things that would be wonderful if they could be proved! The fact is, no one really has any idea, because not nearly enough good quality research has been done on this topic.
And there’s a more practical problem: claims about far infrared are generally paired with the idea that it has to be “pure” far infrared, exclusively limited to a specific, narrow range of wavelengths. As with tanning beds, these heaters can be made well and deliver the type of radiation that was promised — for whatever it’s worth — but the consumer has no way of knowing. And these are expensive products. The potential for corruption and abuse is obvious, and of course regulation is effectively nonexistent.
Finally, a safety note: it’s not like a high-tech person-warming oven is completely risk-free. Pure thermal injury is possible on the mundane end. But there are more exotic risks, too: if you accept the possibility of positive biological effects, then you have to embrace the possibility of negative ones too. Amateur and overexcited biophysicists often forget this.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
Five updates have been logged for this article since publication (2007). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
Like good footnotes, update logging sets PainScience.com apart from most other health websites and blogs. It’s fine print, but important fine print, in the same spirit of transparency as the editing history available for Wikipedia pages.
I log any change to articles that might be of interest to a keen reader. Complete update logging started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
2025 — Two small new sections, “Comfort vs analgesia” and “Heating time: how long does it take?” There’s actually more new content tucked away in a footnote about Bartholdy et al. on heated mittens.
2021 — Major upgrade to information on capsaicin and “spice therapy.” A huge new members-only area has been added with extremely detailed information on this fascinating sub-topic, almost doubling the length of the article, and longer itself than most independent articles. But even the freely available summary is substantially upgraded, much more detailed and accurate.
2020 — New section: “Even more localized heating + the relevance of climate and context.”
2020 — Added substantial section about infrared heating.
2016 — Added evidence of efficacy of NSAIDs for common injuries.
2016 — A series of substantial upgrades, details unlogged.
2007 — Publication.
Notes
- Garra G, Singer AJ, Leno R, et al. Heat or cold packs for neck and back strain: a randomized controlled trial of efficacy. Acad Emerg Med. 2010 May;17(5):484–9. PubMed 20536800 ❐ This 2010 study showed quite clearly that both ice packs and hot packs were only a little bit beneficial for neck and back pain, and about equally so. But a small therapeutic effect is still valuable, and there are almost certainly situations where it works even better — after all, these were people with acute pain bad enough that they went to the hospital. They may have been a bit beyond the help of a hot pack!
- Ingraham. Masking Pain is Under-Rated: “Masking” symptoms is often scorned, but sometimes symptoms need masking — especially pain! PainScience.com. 1106 words. “Masking symptoms,” especially with medications, is often maligned because it doesn’t “treat the root cause.” But masking symptoms can be a good idea, and it should not be eschewed just because it doesn’t have a real healing effect … because there are very few real healing effects! “Healing” is mainly about removing impediments to natural recovery, like stress on tissues. It’s not dictated by some mythical power to speed healing, but by a strong understanding of the nature of the problem and what pisses it off and impedes recovery. Focus on facilitating natural recovery, and don’t knock a little “symptom relief” along the way.
Muscle tension can cause a surprising amount of pain. A leg or foot cramp is a common and extreme example, where no one has any doubt of the cause of pain. But imagine a muscle spasm much less strong, but lasting for days and days — or years! Although superficially a simple concept, there are actually several physiological mechanisms by which muscle can become shortened and painful, acutely or chronically, some well understood and straightforward (spasticity from neurological diseases), while others are quite mysterious (like spasms people are born with, as in torticollis or wry neck).
One excellent example of neuropathic spasticity is the “MS hug”: a symptom of multiple sclerosis that feels like a painfully tight band around the chest, often experienced long before diagnosis. Although the feeling of constriction is the classic symptom, many patients also just experience widespread pain in the chest wall.
- There is zero direct scientific evidence that heat is effective for any kind of cramping, but it is something that many cramp sufferers are obviously naturally drawn to.
- Indeed, exertional cramping are much more strongly linked to heat than to dehydration. That is, you’ll cramp if it’s hot, whether you hydrate adequately or not. This was quite well-established by a terrific 2011 experiment: see Schwellnus et al.
- Several drugs make muscles hurt, but the most notorious are the statins (cholesterol-reducing drugs) and bisphosphonates (for osteoporosis). In some people, these seem to act like muscle poisons.
- Here’s an example of what can happen when you heat an inflamed injury: When I was still in school, and my father had not yet learned to call me before asking a doctor about his aches and pains, he went to a drop-in clinic following a traumatic knee injury. The physician on duty prescribed heat! That was wrong, and the results spoke loud and clear: my dad’s knee swelled dramatically, outrageously, causing severe pain and immobility.
- Some rips aren’t as sudden and obvious as you might expect, and trigger points can flare up faster than you expect. They also probably occur together: a TrP may be why the muscle tore in the first place, or it could crop up in the aftermath, or it could simply feel like a tear.
- In low back pain — infamous for being frustratingly chronic — strains and trigger points are both common, but there are also many other potential sources of pain. So it’s much more difficult to know if heat is a good idea than it is with, say, thigh pain.
- Obviously heat kills too, but much, much less frequently. Humans can survive almost any amount of heat as long as we can get some shade and water and don’t have to overexert ourselves. Cold kills relatively effortlessly!
- Is this suffering vs. pain thing a distinction without a difference? Anyone in pain will take the comfort and call it a win! But there is a difference: no one thinks that the pain of appendicitis is being relieved by a cool cloth on your forehead, however, much it might be appreciated. Still, these are deep waters, and there is no right answer.
- Bartholdy C, Døssing A, Stisen ZR, et al. Effect of heated mittens on physical hand function in people with hand osteoarthritis: randomised controlled trial. BMJ. 2024 Dec;387:e078222. PubMed 39689944 ❐ PainSci Bibliography 50081 ❐
The British Medical Journal gave us a weird Christmas gift! This is a study I didn't think I’d ever see in one of the big, general medical journals: not just a study of heat for hand arthritis, but the unusually practical and folksy option of electrically heated mittens. Power mittens.
Mittens with inbuilt battery driven heat elements are now commercially available and offer an easy means of delivering heat therapy to patients with hand osteoarthritis in an accessible manner outside of clinics.
The goal of Bartholdy et al. was to give us some evidence on this topic that’s actually good for once, and I think they more or less did it. It’s biggish, rigorous, well-planned. The paper is also open-access and quite readable.
Obviously hand osteoarthritis is just about as common as painful problems get. It makes life harder for hundreds of millions of people. Although heat is a staple treatment, the evidence is of course super lame — as usual for this field, as my first post of 2025 explained. It’s rare but nice to see a study like this in a top-tier journal, because they often immediately become the best evidence available for many years to come, out-ranking a bunch of junkier studies.
And sometimes they don’t.
This one does have a huge flaw: Bartholdy et al. compared hot mittens them to cold ones. Which begs a burning question: who did they think they were fooling? How exactly is a unheated mitten an effective sham for a hot one? Wouldn’t people be rather disappointed to get the cool ones? Or perhaps too enthusiastic about the niceness of the hot ones? Isn’t that a glaring confounder?
Yes, and they knew it:
It was not possible to mask the participants throughout the trial, which is a major limitation. This is not surprising as heated mittens would become warmer shortly after switching on the heating element, and the control mittens would not, despite the LED lights being active. Unsuccessful masking and use of patient reported outcomes could have led to an overestimation of effects, which is an inherent weakness and challenge when assessing effects of physical treatments in clinical trials.
But science is messy, flawed data is better than none, and everything else was done quite well. And so let’s crack on…
![An infographic showing the design of heated mittens used in an experiment. The mitten has labeled components, including a “Heating element” winding through the mitten, a “Battery pack” attached near the wrist, and a “Heat control and intensity indicator” with three settings: Low (green), Moderate (yellow), and High (red). A box labeled “Control mittens” explains that the heating elements in the control mittens were disconnected, but the heat control and indicator light remained connected. The background is gradient blue and orange, suggesting warmth.]()
The heated mittens were far from perfect: "more concentrated heat around the joints would have been preferable. … Developing mittens specifically for people with hand osteoarthritis, with a better, possibly customised fit and easier battery recharging system, might help to enhance the effect of heated mittens. Image by Bartholdy et al. & BMJ, CC BY-NC 4.0.
They measured pain and function in a couple hundred older Danish patients with bad hands. Everyone got a pair of mittens, with or without power, and were asked to wear them for at least 15 minutes/day for six weeks, “preferably when symptoms were worst (typically in the morning).” Another study by Kominami et al. showed that it takes about that long to fully heat up. Actual wear times were somewhat longer.
But of course everyone knew what they got! The researchers made a diligent effort to conceal allocation up until the start of the trial, but the jig was up as soon as anyone put them on.
The results
Hot mittens didn’t help. Boooo.
There was no important difference between the groups in pain or function, and what little difference there is probably attributable to the frustrebo effect, more negative reporting from the “frustrated” cold-mitten group … and a more standard enthusiasm-powered placebo for the hot-mitten group.
Many participants expressed a positive experience from use of heat. It is therefore reasonable to assume that participants allocated to the intervention group were more enthusiastic about the mittens, which also could have contributed to an overestimation of the true effect.
P.S. Just one adverse effect reported: itching. 😜
- Kominami K, Sato K, Takahashi N. Relationship between body composition indices and changes in body temperature due to hot pack use. J Physiol Anthropol. 2022 Nov;41(1):40. PubMed 36369123 ❐ PainSci Bibliography 50086 ❐
- Draper DO, Harris ST, Schulthies S, et al. Hot-Pack and 1-MHz Ultrasound Treatments Have an Additive Effect on Muscle Temperature Increase. J Athl Train. 1998 Jan;33(1):21–4. PubMed 16558479 ❐ PainSci Bibliography 54111 ❐
- Shah JP, Danoff JV, Desai MJ, et al. Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Arch Phys Med Rehabil. 2008;89(1):16–23. PubMed 18164325 ❐
This notable study showed that the biochemical milieu of trigger points may be strongly acidic and “polluted” with pain-causing metabolites. For much more information about this, see Toxic Muscle Knots.
- “Trigger points” are controversial, although published expert opinions criticizing the concept remain relatively scarce. This article does not get into the controversy, but it’s important to acknowledge it. The bottom line is that people do suffer from a painful phenomenon (very sensitive spots), and no one disputes that — they just dispute what to call it, how it works, and how to treat it! If you want to learn more about the controversies, see: Trigger Point Doubts: Do muscle knots exist? Exploring controversies about the existence and nature of so-called “trigger points” and myofascial pain syndrome
- Viitasalo JT, Niemela K, Kaappola R, et al. Warm underwater water-jet massage improves recovery from intense physical exercise. Eur J Appl Physiol Occup Physiol. 1995;71(5):431–8. PubMed 8565975 ❐
- Mayer JM, Mooney V, Matheson LN, et al. Continuous low-level heat wrap therapy for the prevention and early phase treatment of delayed-onset muscle soreness of the low back: a randomized controlled trial. Arch Phys Med Rehabil. 2006 Oct;87(10):1310–7. PubMed 17023239 ❐
- Ironically, tigers really hate Tiger Balm.
- Borrell RM, Parker R, Henley EJ, Masley D, Repinecz M. Comparison of in vivo temperatures produced by hydrotherapy, paraffin wax treatment, and Fluidotherapy. Phys Ther. 1980 Oct;60(10):1273–6. PubMed 7443789 ❐
- Derry S, Rice AS, Cole P, Tan T, Moore RA. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database Syst Rev. 2017 01;1:CD007393. PubMed 28085183 ❐ PainSci Bibliography 52172 ❐
Persson MSM, Stocks J, Walsh DA, Doherty M, Zhang W. The relative efficacy of topical non-steroidal anti-inflammatory drugs and capsaicin in osteoarthritis: a network meta-analysis of randomised controlled trials. Osteoarthritis Cartilage. 2018 12;26(12):1575–1582. PubMed 30172837 ❐ PainSci Bibliography 52173 ❐
- Caterina MJ, Schumacher MA, Tominaga M, et al. The capsaicin receptor: a heat-activated ion channel in the pain pathway. Nature. 1997 Oct;389(6653):816–24. PubMed 9349813 ❐
ABSTRACT
Capsaicin, the main pungent ingredient in 'hot' chilli peppers, elicits a sensation of burning pain by selectively activating sensory neurons that convey information about noxious stimuli to the central nervous system. We have used an expression cloning strategy based on calcium influx to isolate a functional cDNA encoding a capsaicin receptor from sensory neurons. This receptor is a non-selective cation channel that is structurally related to members of the TRP family of ion channels. The cloned capsaicin receptor is also activated by increases in temperature in the noxious range, suggesting that it functions as a transducer of painful thermal stimuli in vivo.
- Coste B, Mathur J, Schmidt M, et al. Piezo1 and Piezo2 are essential components of distinct mechanically activated cation channels. Science. 2010 Oct;330(6000):55–60. PubMed 20813920 ❐ PainSci Bibliography 52196 ❐
- My father, a Vietnam veteran, has a great story about a wild pepper he encountered in the jungle. He used it to liven up his C-ration, which it sure did. But after chopping the mystery chili, he rubbed an eye … and was effectively blind in that eye for about a day.
- Tewksbury JJ, Nabhan GP. Seed dispersal. Directed deterrence by capsaicin in chilies. Nature. 2001 Jul;412(6845):403–4. PubMed 11473305 ❐
- I tested a good dose of pure capsaicin on my arm just to make sure. It’s completely invisible. I can feel it, but I cannot see it. Higher concentrations will certainly do it (photo), but not OTC products.
- Is red skin worth anything? Probably not. “Increasing circulation” is tediously overused explanation for why all kinds of treatments work (like massage), but a lack of circulation is rarely the problem, and increasing circulation to a meaningful degree is rarely possible in any case.
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965 Nov;150(3699):971–9. PubMed 5320816 ❐
This is Melzack and Wall’s seminal paper arguing that (emphasis mine) “pain perception and response is triggered after the cutaneous sensory input has been modulated by both sensory feedback mechanisms and the influences of the central nervous system. We propose that the abstraction of information at the first synapse may mark only the beginning of a continuing selection and filtering of the input.” Among other things, this is the paper that described the mechanism of gate control and ultimately gave rise to the highly influential concept of the neuromatrix (Melzack).
- Simone DA, Ochoa J. Early and late effects of prolonged topical capsaicin on cutaneous sensibility and neurogenic vasodilatation in humans. Pain. 1991 Dec;47(3):285–294. PubMed 1784499 ❐
- LaMotte RH, Lundberg LE, Torebjörk HE. Pain, hyperalgesia and activity in nociceptive C units in humans after intradermal injection of capsaicin. J Physiol. 1992 Mar;448:749–64. PubMed 1593488 ❐ PainSci Bibliography 52165 ❐
- Dakin SG, Newton J, Martinez FO, et al. Chronic inflammation is a feature of Achilles tendinopathy and rupture. Br J Sports Med. 2017 Nov. PubMed 29118051 ❐
- An alarming side effect of THC/CBD usage is cannabinoid hyperemesis syndrome (CHS): escalating episodes of chills, nausea, and painful projectile vomiting. Takakuwa et al.:
As cannabis becomes more widely available with the adoption of state medical cannabis laws, ED-related cannabis visits will likely rise. While cannabis has historically been considered a relatively safe drug, increased legal and illegal access to newer formulations of higher potency products and consumption methods have altered the management and approach to ED patient care and forced physicians to become more vigilant about recognizing and treating some new cannabis-related life-threatening conditions.
CHS tends to be worse in the morning, and patients often alternate between vomiting and self-treating the chills with hot baths and showers.
For more information, see Marijuana for Pain: The hype versus the science! What does the evidence actually show about cannabis and chronic pain?. - Moon AM, Buckley SA, Mark NM. Successful Treatment of Cannabinoid Hyperemesis Syndrome with Topical Capsaicin. ACG Case Rep J. 2018;5:e3. PubMed 29379817 ❐ PainSci Bibliography 52210 ❐
- McConachie SM, Caputo RA, Wilhelm SM, Kale-Pradhan PB. Efficacy of Capsaicin for the Treatment of Cannabinoid Hyperemesis Syndrome: A Systematic Review. Ann Pharmacother. 2019 11;53(11):1145–1152. PubMed 31104487 ❐
- Derry S, Rice AS, Cole P, Tan T, Moore RA. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database Syst Rev. 2017 01;1:CD007393. PubMed 28085183 ❐ PainSci Bibliography 52172 ❐
- Kennedy WR, Vanhove GF, Lu SP, et al. A Randomized, Controlled, Open-Label Study of the Long-Term Effects of NGX-4010, a High-Concentration Capsaicin Patch, on Epidermal Nerve Fiber Density and Sensory Function in Healthy Volunteers. J Pain. 2010 Jun;11(6):579–587. PubMed 20400377 ❐
- Derry S, Rice AS, Cole P, Tan T, Moore RA. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database Syst Rev. 2017 01;1:CD007393. PubMed 28085183 ❐ PainSci Bibliography 52172 ❐
- Persson MSM, Stocks J, Walsh DA, Doherty M, Zhang W. The relative efficacy of topical non-steroidal anti-inflammatory drugs and capsaicin in osteoarthritis: a network meta-analysis of randomised controlled trials. Osteoarthritis Cartilage. 2018 12;26(12):1575–1582. PubMed 30172837 ❐ PainSci Bibliography 52173 ❐)
- Epsom salt in your bath is cheap and harmless and it makes the water feel “silkier,” but it’s unlikely that it has a therapeutic effect on aches and pains. It definitely doesn’t “detox” anything. Magnesium supplementation might be helpful for some people with deficiency and chronic pain, but it probably can't soak through the skin. The soothing heat of a nice bath is probably the main source of health benefits. The case for the healing powers of Epsom salt is mostly made by people selling the stuff, or recommending it as casually and imprecisely as an old wives’ tale. See Does Epsom Salt Work? The science and mythology of Epsom salt bathing for recovery from muscle pain, soreness, or injury.
- There are four kinds: acetaminophen/paracetamol (Tylenol, Panadol), plus three non-steroidal anti-inflammatories (NSAIDs): aspirin (Bayer, Bufferin), ibuprofen (Advil, Motrin), and naproxen (Aleve, Naprosyn).
- Science Based Pharmacy [Internet]. Gavura S. How risky are NSAIDS?; 2015 Jul 25 [cited 16 Aug 18]. PainSci Bibliography 54751 ❐
- Hung KKC, Graham CA, Lo RSL, et al. Oral paracetamol and/or ibuprofen for treating pain after soft tissue injuries: Single centre double-blind, randomised controlled clinical trial. PLoS One. 2018;13(2):e0192043. PubMed 29408866 ❐
In a test of ibuprofen vs paracetamol for hundreds of soft tissue injuries, there was no significant difference in the modest benefits or side effects, contrary to some past evidence and the widely held medical belief that ibuprofen is better for injuries (inflammation). It’s possible that placebo is powering the effects of both medications, and that's why they were equal, but it's impossible to know without a control group for this study. Note that the superiority of these medications is probably variable and not as clearly established as you might think.
- FDA.gov [Internet]. Acetaminophen and Liver Injury: Q & A for Consumers; 2009 Jun 4 [cited 16 Aug 31]. PainSci Bibliography 53431 ❐
“This drug is generally considered safe when used according to the directions on its labeling. But taking more than the recommended amount can cause liver damage, ranging from abnormalities in liver function blood tests, to acute liver failure, and even death.”
- Machado GC, Maher CG, Ferreira PH, et al. Efficacy and safety of paracetamol for spinal pain and osteoarthritis: systematic review and meta-analysis of randomised placebo controlled trials. BMJ. 2015;350:h1225. PubMed 25828856 ❐ PainSci Bibliography 54220 ❐
- Vatansever F, Hamblin MR. Far infrared radiation (FIR): its biological effects and medical applications. Photonics Lasers Med. 2012 Nov;4:255–266. PubMed 23833705 ❐ PainSci Bibliography 52578 ❐
This is a lousy paper. The authors clearly have rose-coloured glasses on when it comes to infrared radiation. They repeat the assertion that far infrared radiation can “penetrate up to 1.5 inches (almost 4 cm) beneath the skin”… but, appallingly, provides no additional detail or source, even though it’s a very important point. And yet it appears that their statement has been taken as gospel by most everyone in the infrared sauna business. This is a familiar scenario, and there have been quite a few cases where publication of a paper like this was arranged by an industry specifically so that it can be cited in marketing materials. Just sayin’.
- International Commission on Non-Ionizing Radiation Protection. ICNIRP statement on far infrared radiation exposure. Health Phys. 2006 Dec;91(6):630–45. PubMed 17099407 ❐
The three infrared spectral bands roughly distinguish between different penetration depths into tissue, which are strongly dependent upon water absorption. IR-A radiation [near infrared] penetrates several millimeters into tissue. IR-B penetrates less than 1 mm, and at the penetration depth (1/e) is least (approximately 1 m) at wavelengths near 3 m, where water has its highest absorption peak. IR-C [far infrared] does not penetrate beyond the uppermost layer of the dead skin cells, the stratum corneum.
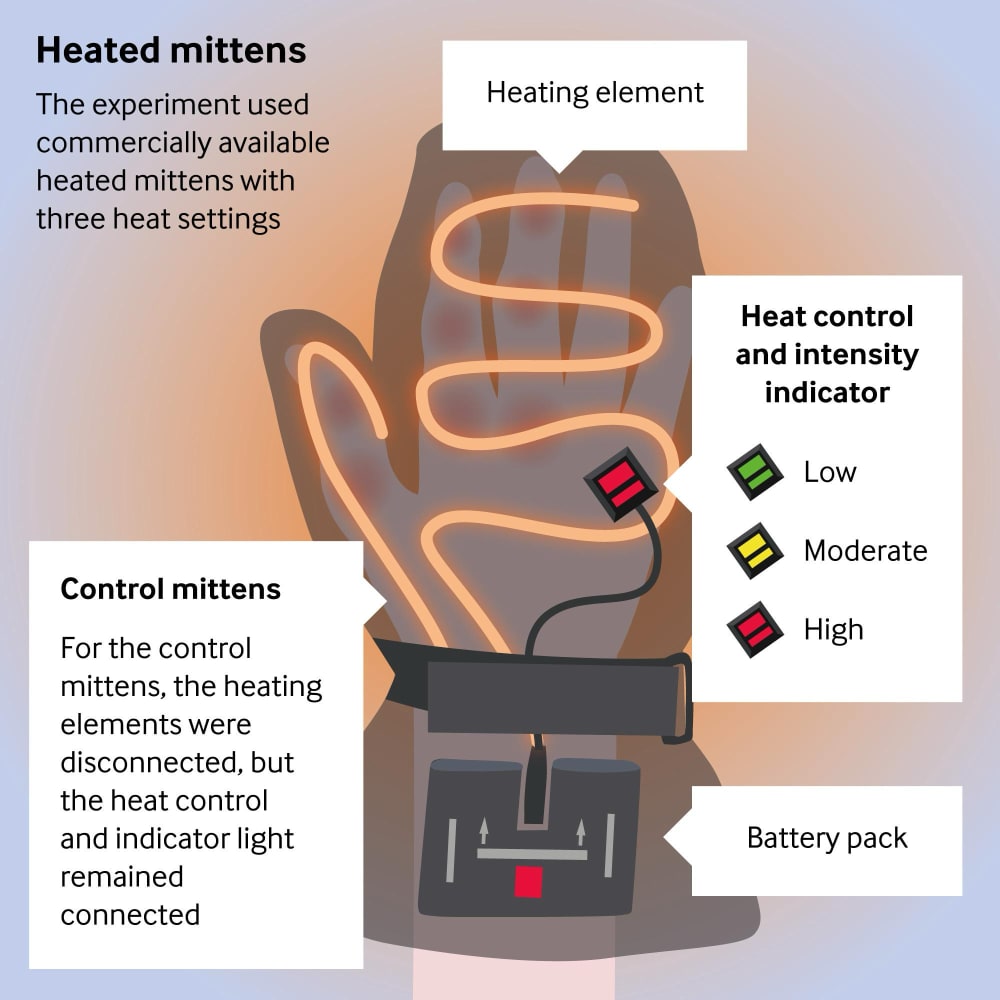
{kind=link}
{kind=link}