The 3 Basic Types of Pain
Nociceptive, neuropathic, and “other” (and then some more)
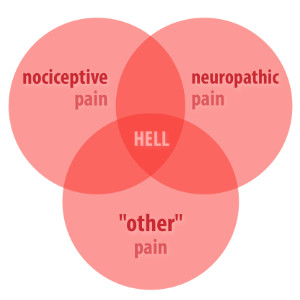
There are two well-recognized broad categories of pain:
- pain from damage — the common sensical sort, but sometimes surprisingly weird
- pain from damage to the pain system itself, the nervous system, which produces weird pain by default
That’s roughly the difference between alarms and false alarms, or actual engine trouble versus malfunction of the light on your dashboard that says there’s engine trouble. Again with more technical detail:
- Nociceptive pain arises from various kinds of trouble in tissues, reported to the brain by the nervous system.1 This is the type of pain everyone is most familiar with, everything from bee stings and burns and toe stubs to repetitive strain injury, nausea, tumours, and inflammatory arthritis. Nociceptive pain typically changes with movement, position, and load.
- Neuropathic pain arises from damage to the nervous system itself, central or peripheral, either from disease, injury, or physical irritation2 (e.g. pinching and snagging3). The simplest neuropathies are mechanical insults to nerves, like hitting your funny bone (ulnar nerve) or various kinds of irritation of the sciatic nerve. But this is a big category, including anything that damages neurons in any way, from multiple sclerosis to chemotherapy to alcoholism to phantom limb pain. The pain is often stabbing, electrical, or burning, but nearly any quality of pain is possible. Unfortunately, it’s also more likely to lead to chronic pain: nerves don’t heal well.4
Obviously these kinds of pain can and do overlap. Some medical problems, like injuries, can affect both nerves themselves and other tissues, causing both kinds of pain. However, it’s surprising how little obvious overlap there is: look at any list of the most painful conditions , or the great variety of pain causes, and they mostly fit into one category or the other. But “under the hood,” most pain does involve elements of both types.7
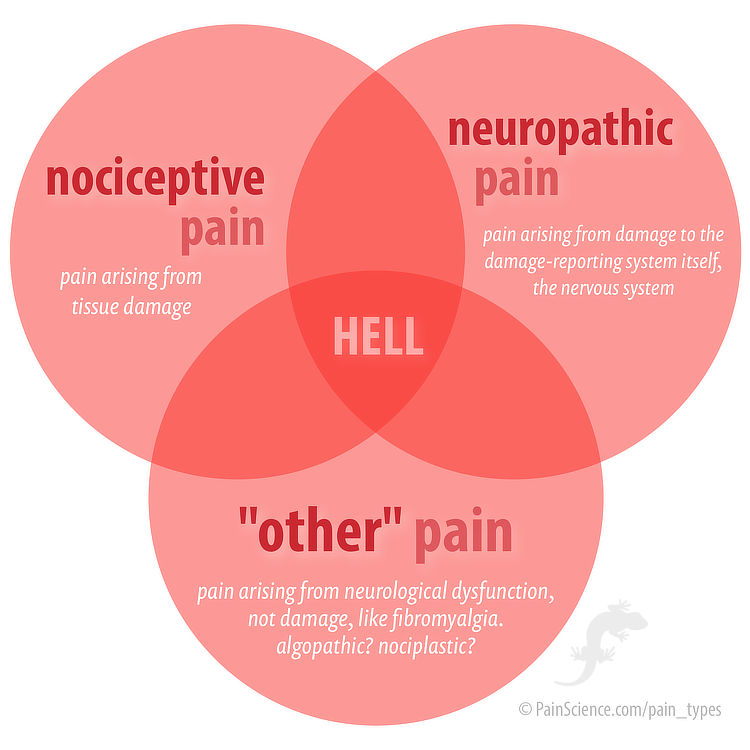
Although the different kinds of pain certainly can overlap, mercifully it’s relatively rare to end up in “hell” at the centre of this Venn diagram. Unfortunately, the “other” category often does arise from a history of other kinds of pain.
File under “other”: pain problems for which we might need a new word
Some common kinds of pain are not a great fit for either of the two official categories, like the canonical example of the pain of fibromyalgia. Historically these kinds of pain have often been called “functional pain disorders,” which is a terrible name with a lot of baggage.10 Other major examples:
- complex regional pain syndrome (CRPS)
- amplified pain syndome
- nonspecific chronic low-back pain
- primary (unexplained) headache
- irritable bowel syndrome and other chronic visceral pain disorders
- conditions that begin as nociceptive pain, like osteoarthritis, but then go into a hellish downward spiral of sensitization11
Fibromyalgia is probably a pain system dysfunction, a poorly understood multi-system failure causing widespread body pain (and more12), but “dysfunction” of the nervous system is specifically excluded from neuropathic pain, by decree, as of 2011.13 Dysfunction means that fibromyalgia isn’t caused by any (known) damage to the nervous system, but by its misbehaviour, and so it’s not welcome at the neuropathy club. It was before 2011! But not anymore.
Maybe there are unknown lesions? Maybe someday we’ll know that fibromyalgia is caused by some kind of subtle damage to the nervous system.14 There are at least two theories of subtle lesions of this type.15 That would make it just another neuropathy after all, ho hum. But for now it’s still more plausible that it’s a dysfunction, arising from widespread problems in a complex system, and no clear point of failure will ever be discovered.1617 But who knows. Science is not finished with fibromyalgia.
Meanwhile, what do we call it? And other miserable pain problems that arise from what seem to be complex organic dysfunction?
“Is that a fresh injury?” “Not really. But it’s tormenting me. Do you have any herbs capable of soothing the pain?” “That all depends on the class of pain,” the barber-surgeon said, smiling slightly. “And on its causes.”
The Witcher (Baptism of Fire), Andrzej Sapkowski
Possible names for this other kind of pain
“Other” is a bit vague, so experts have proposed some more descriptive names for this category. There are issues with all of them. (The first three here all come from the same source.18)
- Nocipathic pain: abnormal nociception. This is basically a fancy way of saying “other” pain, and I don’t think it adds much.
- Nociplastic pain: like nocipathic, but a little more descriptive, implying specifically that the problem arises from changes in how nociceptive pain works.
- Algopathic pain: pathological perception/sensation. This is the Greek way to say “pain disease.”
- Centralized pain19 or maladaptive central processing20 or central sensitivity syndrome:21 pain driven by the spinal cord and brain, regardless of what’s going on in the tissues.
- Primary pain, as proposed by Schechter,22 which simply implies that pain is the main problem.
The “noci” terms seem a little misguided to me, because the pain of a misbehaving nervous system is so much closer kin to neuropathic pain.23 Centralization is an important concept and element, but clearly not the whole story24 (and “maladaptive” might be too blamey25). Algopathic is pretty good: suitably neutral and formal, while saying just enough to be better than “other.”
But my vote is for primary pain: tidy, apt, and neutral. Why try to express mechanism for this kind of pain in the term when we so clearly don’t understand it? Or, even if we did, it would obviously be too complex to capture with a single term anyway? “Keep it simple, stupid!”
Do sensitization and centralization belong in the “other” category?
Sensitization is the amplification of danger signalling in any part of the system (which can be driven by both peripheral and central neurology, while centralization is referring only to the latter). It seems like a slam dunk to put these in the “other” category, but not so fast: the nervous system is not being dysfunctional just because it overestimates some danger. Many of us experience normal, healthy centralized sensitization every time we go to the dentist, because our nervous system is not an idiot and is very suspicious of dentists based on past experiences. Our brains think the dentist is a threat, and although they are technically wrong — the dentist is actually there to help — the judgement is not “dysfunctional.”
Sensitization is clearly part of the normal function of the pain system — it’ s not a dumb system where pain is always exactly proportionate to tissue danger. It’s more subtle. Sensitization/centralization is only dysfunctional when it’s chronic and seriously disproportionate. And of course there’s a grey zone a mile wide between normal and dysfunctional. It’s a spectrum.
File under “unknown”: many pain problems can’t be categorized… yet
Sometimes we just don’t understand a problem well enough to classify it. The best example of this is the sensitive spots in soft tissue that so many people have — “trigger points,” the things that motivate most massage therapy appointments. There is a popular hypothesis that they are caused by a problem with muscle tissue, which would make it a clear case of nociceptive pain from a fairly subtle lesion … but it’s just a hypothesis, and some experts have suggested that trigger points are caused by a problem with nerves themselves, which would make them neuropathic.26 No one actually knows, and it’s not likely to be settled for a long time.
The “official” causes of all kinds of chronic pain (another way to talk about “types” of pain) break down into three roughly equally large categories, plus one small “other” category:27
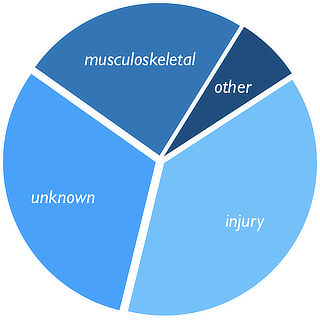
- injury (38%)
- unknown (31%)
- musculoskeletal (24%), a vague category dominated by arthritis, the rheumatic diseases, and headache
- other (7%), which is mostly cancer and abdominal pain plus “everything else” (mostly pain related to major physiological systems)
But I suspect these are pretty meaningless categories, and it should be more like 80% unknown. Misdiagnosis is routine, of course. Arthritis and the rheumatic diseases should probably be in their own major category, and almost everything else filed under “unknown.” Pain after injury is surprisingly murky: sure, it might have started with an injury, but two years later is that still the “cause”? It has usually transmogrified into something else, and exactly how that works is much more about the “unknown” than “injury.” Many cases of chronic pain are hard to put in just one of these categories (or they only seem easy to place). Most causes of pain are hard to fit into these categories. See: 38 Surprising Causes of Pain: Trying to understand pain when there is no obvious explanation.
A key deep thought: nociception isn’t pain, and there are no “pain nerves,” but muscles can still be sore
Nociceptors are the nerves that detect potentially noxious stimuli, and nociception is what they do for a living: they send reports about tissue state, not pain.Pain is a brain-generated experience based on many factors, including but not limited to nociception. If nociception is the major trigger that leads to a pain experience, it’s reasonable to call it “nociceptive pain.” But nociception is one thing, and pain is another.
Example: If you step on a Lego piece, the nerves send that information to the brain (nociception), and the brain always decides that this information means you’re in a lot of danger. Stepping on Lego is something the brain takes very seriously! So it always hurts! But it isn’t “pain” until the brain says so, and a lot of routine, boring nociception never becomes pain — like the slight discomforts that provoke us to change position, before it becomes a problem.
So, “ackshually,” nociception and pain are not the same thing, and nociceptors are not “pain fibres.”28
So what? Life is a reification fallacy
“Reification” is treating an abstraction as if it were a real thing, making it concrete. We do this constantly, of course. It’s a really basic feature of being human.
As we have come to understand how pain is surprisingly independent of tissue state — you can hurt without tissue problem and vice versa, to an amazing degree — some experts have started to object to statements like “my muscles are sore.” Why? Because, technically, it’s your brain that hurts, not your muscles. Muscles can’t feel! That’s reification! “Reification fallacies” like this are pedantically asserted during shop talk on social media often enough that it has gotten on my nerves.
It is important to be able to deconstruct pain like this, even for patients — it’s a big part of pain science — but it is not a requirement, and it’s mostly way too clunky and technical for all but the most formal and delving discussions.
Literally everything that exists (not just what we sense) is a mental construct, a brain-made story. Life is a reification fallacy and refusing to tolerate reification is impractical. The entire point of sensation is to treat abstractions as if they were real.
Example: this delicious muffin I’m eating does not technically possess deliciousness or any blueberry flavour — those experiences really are all in my mind, like everything else — but “this blueberry muffin is delicious” is still a useful, meaningful statement for basically anyone who isn’t specifically trying to explain the neurology of it.
And so is “my muscles are sore.”
Pain is whatever the person experiencing it says it is, existing whenever and wherever they say it does.
Margo McCaffery, Specialist Pain Nurse
Another way of categorizing pain: visceral and somatic
Somatic pain is experienced in the skin, muscles, bones, and joints.
Visceral pain is the pain of organs, in the thoracic or abdominal cavities.
Both somatic and visceral pain can be nociceptive, neuropathic, or algopathic. The two classification systems have full overlap.
The somatic/visceral distinction isn’t just about location and depth: visceral and somatic pain have very different characteristics, reflecting different priorities. For instance, much of somatic pain neurology is all about localization: the brain is very concerned with where somatic pain is occurring, the better to avoid external sources of danger. Visceral pain is notoriously “diffuse,” difficult to isolate, and is often felt in remote locations, because the brain basically can’t tell where the pain is coming from and starts making it up, referred pain.29
For much of medical history, no one even thought organs could hurt, which seems a bit quaint now — just what did they think was going on with the pain of a heart attack? Organs are largely impervious to the things that the somatic pain system is tuned to detect, like lacerations or burning, but they are very sensitive the kinds of things that are more likely to go wrong with organs, like stretch (a swollen gut), ischemia (a heart deprived of oxygen during a heart attack), and inflammation (inflammatory bowel disease). Hence the confusion. Now it’s obvious not only that viscera can hurt, but that they can hurt excessively and stubbornly: algopathic visceral pain, or visceral hypersensitivity, which is at the root of functional gastrointestinal disorders (gut trouble without an obvious cause, mainly irritable bowel syndrome).
Fast and slow pain, acute and chronic: yet another way to categorize
Fast pain gets all the press, the kind of pain that makes you jerk your hand away from a hot stove. Pain is basically a threat detection system intended to get you to move away from danger, and you can’t read about pain science anywhere without encountering this idea… which always seems a bit nuts to people with cpj, because where’s the threat there? Which way do you run? What do you jerk away from when your back has been killing you for six months?
Pain protects from two kinds of threats in two very different ways. And it’s the other way that matters to most people with persistent pain.
Of course, acute pain drives rapid movement away from immediate, external threats, mediated mainly by nociception via speedy “A” type nerve fibres.
But chronic pain — with threat information delivered via the sluggish “C” fibres — is trying to protect us by discouraging movement, by forcing us to hunker down for rest and healing! That’s a really different scenario.
These modes are strongly analogous to fight/flight and rest/digest. One system is optimized for emergencies, the other is optimized for recuperation.
Most chronic pain is not trying to tell us about external threats we need to get away from, but about the need to stay put until we feel better. Just as with acute pain, the warning is not necessarily accurate, and in most cases of longer term chronic pain we are too shut down and need to get moving despite the warning.
The complexity of persistent pain is generally underestimated by everyone. Most clinicians do understand that there is an important distinction, but they still underestimate it! Pain chronicity exists on a spectrum of severity and weirdness, and the transition from one end to the other can be fast and ferocious.
Did you find this article useful? Interesting? Maybe notice how there’s not much content like this on the Internet? That’s because it’s crazy hard to make it pay. Please support (very) independent science journalism with a donation. See the donation page for more information & options.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Related Reading
- A Painful Biological Glitch that Causes Pointless Inflammation — How an evolutionary wrong turn led to a biological glitch that condemned the animal kingdom — you included — to much louder, longer pain
- 38 Surprising Causes of Pain — Trying to understand pain when there is no obvious explanation
- Sensitization in Chronic Pain — Pain itself can change how pain works, resulting in more pain with less provocation
- Insomnia Until it Hurts — The role of sleep deprivation in chronic pain, especially muscle pain
- Neuropathies Are Overdiagnosed — Our cultural fear of neuropathy, and a story about nerve pain that wasn’t
- Pain & Injury Survival Tips — Dozens of ideas (and links) for evidence-based rehabilitation and self-treatment for common pain problems and injuries
- Chronic, Subtle, Systemic Inflammation — One possible sneaky cause of puzzling chronic pain
- Chronic Pain as a Conditioned Response — If pain can be learned, perhaps it can be unlearned
- “Gate Control Theory of Pain for Manual Therapists and Patients,” Nick Ng, www.massagefitnessmag.com. A detailed and accessible primer on gate control theory, with plenty of history and perspective too.
Appendix: Neuropathic versus nociceptive pain
If pain is unexplained, can we at least narrow it down to a type? Can we put it in one of the two main pain categories, neuropathic or nociceptive? Sometimes! Not always! These types of pain overlap and often the only clues are the quality of the pain and the messy stories and ideas we have about it: how it started, what makes it worse or better, and so on. We can’t just say that neuropathic pain is “electrical,” because not everyone’s sciatica feels that way.
But we can usually make an educated guess, at least.
Neuropathic pain is mostly more distinctive and specific than nociceptive pain, so it’s best to think in terms of whether pain is or is not neuropathic.
It is usually burning, electrical, or stabbing. The better these words seem to fit, the more likely it is to be neuropathic pain.
Neuropathic pain is sometimes associated with other sensory disturbances like tingling (parasthesia) and numbness, or weakness.
More exotically, neuropathic pain may cause odd effects like exaggerated pain (hyperalgesia), or even pain from stimuli that shouldn’t hurt at all (allodynia), or pain “echoes.” If any of these other non-pain neurological symptoms are present, it’s nearly a diagnostic slam dunk: the pain is probably neuropathic.
Unfortunately, plenty of neuropathic is not conveniently packaged with other obvious neurological effects. So how else can we judge it?
Extent. Neuropathic pain is often more widespread. A damaged nerve can cause symptoms in many locations “downstream” from the damage. Nociceptive pain is mostly more isolated.
Location, location, location. Although it’s hard for patients to judge this, neuropathic pain often occurs in specific locations associated with nerves or nerve roots. And yet this can fool pros too: these patterns aren’t nearly as clear-cut as the tidy diagrams in the textbooks.
Neuropathic pain is also more likely to occur in some locations. For instance, a very broad rule of thumb is that neuropathic pain is more common in the limbs, and the further you go out towards the tips the more likely it gets, simply because the limbs of are full of long and relatively exposed nerves.
Response to medication. Neuropathic pain is rarely responsive to over-the-counter pain killers; nociceptive pain is much more so, especially when it’s still fresh.
Duration. This is perhaps the roughest rule of thumb of them all — there are lots of exceptions to it — but neuropathic pain tends to last longer and is strongly associated with chronic pain.
So, if you have stubborn, widespread, burning pain in your limbs that defies acetaminophen … that’s probably neuropathic pain. And yet it’s still not a sure thing!
What’s new in this article?
Ten updates have been logged for this article since publication (2016). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
2023 — Added a footnote about whether it’s okay to call nociceptors “pain fibres.”
2019 — Added clearer acknowledgement of the odious term “functional pain,” and adopted a new preferred term for that tricky “other” category of pain: primary pain, as proposed by Schechter. Hat tip to Rachel Z. for inspiring this line of thinking.
2018 — New section: “Fast and slow pain: yet another way to categorize.”
2018 — New section: “Another way of categorizing pain: visceral and somatic.”
2018 — New section: “A key deep thought: nociception isn’t pain, and there are no ‘pain nerves,’ but muscles can still be sore.”
2017 — New section — “Appendix: Neuropathic versus nociceptive pain.”
2017 — Added an important point to the definition of neuropathy: it tends to be more chronic.
2016 — Added a nice new Venn diagram depicting the intersection of all three kinds of pain in “hell.” Added section “Do sensitization and centralization belong in the “other” category?”
2016 — Added sidebar about migraine, and converted section about the influence of the brain to a sidebar. Elaborated on overlapping pain problems.
2016 — Extensive next day revisions.
2016 — Publication.
Notes
- IASP-pain.org [Internet]. International Association for the Study of Pain. IASP Taxonomy; 2012 May 22 [cited 19 Sep 5]. PainSci Bibliography 53250 ❐ The formal definition: “Pain that arises from actual or threatened damage to non-neural tissue and is due to the activation of nociceptors [nerve endings that detect tissue damage].” The next definition is also based on this reference.
- Formally: “Pain caused by a lesion or disease of the somatosensory nervous system.” You get a gold star if you notice that “dysfunction” isn’t included there. Neuropathic pain is the pain of physical or pathological stress on nerve tissue, not physiological nerve “glitching.” More on this below.
- Compression of nerves is unquestionably a thing. “Snagging” probably is too, but it’s a bit more hypothetical, a reference to nerves getting adhered to the walls of their sheaths. One of the goals of neurodynamic stretching is to free those nerves, but no one knows if that actually works.
- Cohen SP, Mao J. Neuropathic pain: mechanisms and their clinical implications. BMJ. 2014;348:f7656. PubMed 24500412 ❐
- Chakravarty A, Sen A. Migraine, neuropathic pain and nociceptive pain: towards a unifying concept. Med Hypotheses. 2010 Feb;74(2):225–31. PubMed 19765908 ❐ “Migraine, neuropathic pain and nociceptive pain are the three commonest pain syndromes affecting human.”
- Biondi DM. Is migraine a neuropathic pain syndrome? Curr Pain Headache Rep. 2006 Jun;10(3):167–78. PubMed 18778570 ❐
- Cohen SP, Mao J. Neuropathic pain: mechanisms and their clinical implications. BMJ. 2014;348:f7656. PubMed 24500412 ❐ There’s so much overlap between the mechanisms of neuropathic and nociceptive pain that “many experts view them as different points on a chronic pain continuum, rather than distinct entities.” As a simple example, all acute nociceptive pain — every toe stub — involves an immediate ramping up of sensitivity of nerve endings in the area. That sensitizing process shares a lot of biology with neuropathic pain.
Pain is an output of the brain.
Pain is the end result. Pain is an output of the brain designed to protect you. It’s not something that comes from the tissues of the body.
Lorimer Moseley, from his surprisingly funny TED talk, Why Things Hurt
![]() 14:33
14:33The formal definition of pain emphasizes its subjective, experiential nature: “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” (IASP Taxonomy). This experience is based on many “inputs,” not just nerve signals about tissue damage.
- Although the brain takes data from tissues seriously, it also regularly minimizes, exaggerates, and misinterprets. The brain thinks minor things are serious, or serious things are minor. It’s poor at locating the sources of internal pain. If the nervous system itself is damaged, the brain can really get thrown off (as with phantom limb pain). The brain’s pain policies are warped by moods, anxieties, fatigue, and much more. For much more about this, see Pain is Weird: Pain science reveals a volatile, misleading sensation that comes entirely from an overprotective brain, not our tissues.
- Schechter NL. Functional pain: time for a new name. JAMA Pediatr. 2014 Aug;168(8):693–4. PubMed 24887181 ❐
When a comprehensive search to explain a particular symptom or cluster of symptoms does not identify an organic disease, those symptoms are often described as representing a functional disorder. When that symptom is pain, the patient is diagnosed with a functional pain disorder.
Schecter describes the history of the term “functional pain disorder,” describes several problems with it, and particularly highlights its strong and inappropriate connotation of mental illness in modern use.
- Ingraham. Sensitization in Chronic Pain: Pain itself can change how pain works, resulting in more pain with less provocation. PainScience.com. 7995 words. Pain itself often modifies the way the central nervous system works, so that a patient actually becomes more sensitive and gets more pain with less provocation. This is called “central sensitization.” (And there’s peripheral sensitization too.) Sensitized patients are not only more sensitive to things that should hurt, but also to ordinary touch and pressure as well. Their pain also “echoes,” fading more slowly than in other people.
- Poor quality sleep, fatigue, memory and mood issues — the infamous “fibrofog.”
- Jensen TS, Baron R, Haanpää M, et al. A new definition of neuropathic pain. Pain. 2011 Oct;152(10):2204–5. PubMed 21764514 ❐
IASP has recently [2008] published a new definition of neuropathic pain according to which neuropathic pain is defined as ‘pain caused by a lesion or disease of the somatosensory system.’ This definition replaces the 17-year old definition that appeared in the Classification of Chronic Pain published by IASP in 1994, which defined neuropathic pain as ‘pain initiated or caused by a primary lesion, dysfunction, or transitory perturbation of the peripheral or central nervous system’. Even though the definition has not been changed dramatically, there are two important changes in the new version: (1) the word ‘dysfunction’ has been removed and (2) a lesion or disease affecting the nervous system has been specified to be a lesion or disease of the somatosensory system.
The whole paper is excellent, but skipping to the cogent conclusion:
A definition of neuropathic pain is only useful if it distinguishes conditions in a clinically meaningful way. If the definition does not provide additional benefit in terms of understanding and treating the condition(s), then there is no reason to keep it. Hopefully, the new definition of neuropathic pain will act as a stimulant to discuss the definition in more detail and provide input for studies that can be used to test the value of the definition.
- Multiple sclerosis attacks nerves in quite a dramatic way, which we could see in autopsies, but the lesions were invisible in living patients until the invention of MRI. It’s plausible that there are still plenty of biological “lesions” that we haven’t yet learned to detect, because they are just too small and transient. Despite all of our modern technological wizardy, most of the action in biology happens at the nanoscale, cells moving molecules and atoms around at dazzling speeds through the chaos of the molecular storm (brownian motion). There are probably nanoscale lesions.
- Both small fibre peripheral neuropathy and positional cervical cord compression are candidate neuropathic etiologies: both hard to detect, both capable of explaining at least some of the symptoms of fibromyalgia, both associated with people who have been diagnosed with fibromyalgia. See the main fibromyalgia article for more information about these.
- Lyon P, Cohen M, Quintner J. An evolutionary stress-response hypothesis for chronic widespread pain (fibromyalgia syndrome). Pain Med. 2011 Aug;12(8):1167–78. PubMed 21692974 ❐ “Drawing on diverse findings in neurobiology, immunology, physiology, and comparative biology, we suggest that the form of central sensitization that leads to the profound phenomenological features of chronic widespread pain is part of a whole-organism stress response, which is evolutionarily conserved, following a general pattern found in the simplest living systems.”
- BetterMovement.org [Internet]. Hargrove T. A Systems Perspective on Chronic Pain; 2014 Oct 23 [cited 16 Sep 12]. PainSci Bibliography 53866 ❐
This deep but beautifully readable article explains, with many pictures and apt examples, how “chronic pain is often driven by dysregulation of a ‘supersystem’ that coordinates defensive responses to injury. The supersystem results from dynamic interaction between different subsystems, most notably the nervous system, immune system, and endocrine system.” The article also manages to make this information seem quite practical, believe it or not.
- Kosek E, Cohen M, Baron R, et al. Do we need a third mechanistic descriptor for chronic pain states? Pain. 2016 Jul;157(7):1382–6. PubMed 26835783 ❐ PainSci Bibliography 53276 ❐
- Clauw DJ. Fibromyalgia: a clinical review. JAMA. 2014 Apr;311(15):1547–55. PubMed 24737367 ❐
- Topical Issues in Pain (https://giffordsachesandpains.com/topical-issues-in-pain-relaunch-2013/)
- Yunus MB. Central sensitivity syndromes: a new paradigm and group nosology for fibromyalgia and overlapping conditions, and the related issue of disease versus illness. Semin Arthritis Rheum. 2008 Jun;37(6):339–52. PubMed 18191990 ❐
- Schechter 2014, op. cit.
Therefore, a new neutral name is proposed for this category, primary pain disorders. This term arises from the headache field, where headaches are categorized as primary (the head pain itself is the central problem) or secondary (the headache is due to other factors such as increased intracranial pressure or infection, for example). The term primary pain disorder implies that the pain itself is the disease.
- Even if this kind of pain does involve an exaggeration of nociception (which it probably does), it still seems to me that nociception itself is innocent. It’s not nociception’s fault! The focus should be on the mechanism of sensitization — that is what makes the problem what it is.
- Quintner, J. “Why “Centralized” Is Unacceptable As A Descriptor For The Pain Of Fibromyalgia.” Aug 23, 2016. “Not only does the word itself not imply a mechanism but also it creates potential for confusion with conditions such as ‘central post-stroke pain’ (which is technically ‘neuropathic’) and quite different from the phenomena that underlie fibromyalgia.”
- This term has some strong negative connotations. I think it could strongly stigmatise the patient’s condition, implying that they have “adapted badly” to things that other patients had no problem with. Even if that is technically true from one perspective, it’s not where the emphasis should be. Most patients with these problems have already had a lot of difficulty being heard, understood, and respected — let’s not make it harder with a blame-y label.
- Quintner JL, Bove GM, Cohen ML. A critical evaluation of the trigger point phenomenon. Rheumatology (Oxford). 2015 Mar;54(3):392–9. PubMed 25477053 ❐ Quintner, Cohen, and Bove argue that the common picture of trigger points as lesions in muscle and soft tissue, spelled out most formally in Gerwin 2004, is “flawed both in reasoning and in science.” But not even these critics of trigger points deny that people have pain that seems to come from their muscles. But if it’s not coming from the muscle, where is it coming from? They briefly discuss the possibility of inflamed nerve fibres, which would be a clear case of neuropathy. Neuritis is undoubtedly worth investigating, but it requires us to believe that nerve axons are routinely inflamed for no apparent reason. And the evidence cited to support it is actually much more limited than the evidence for a lesion in muscle.
- Painaustralia. The cost of pain in Australia. Deloitte Access Economics. 2019 Mar. PainSci Bibliography 52620 ❐
The labeling of nociceptors as pain fibers was not an admirable simplification, but an unfortunate trivialization under the guise of simplification.
The relationship of perceived pain to afferent nerve impulses, by Patrick Wall and SB McMahon, 254–255
The common casual conflation of nociception and pain is a favourite bugaboo of pain science dorks, and there’s about a 90% chance that we’ll quote Drs. Wall and McMahon at you if you dare to make this mistake. It exasperates us like “I seen” or “literally” makes an English teacher groan — but with less justification. For most people, most of the time, pain and nociception and the nerves involved are effectively synonymous. And so the use of “pain fibres” mostly does not make me cringe, or actually tempt me to say, “Akshually…” 🙂 It’s usually a harmless simplification, a perfectly reasonable shorthand — especially for pros talking to patients.
That all said, it is indeed an simplification, and the distinction between nociception and pain is real and legitimate, and speaking more precisely about that distinction is appropriate and sensible in some contexts. Sometimes we need to speak more precisely, and so we do. Jargon has its uses. And so our conflation consternation is more justified when it is spotted in, say, a scientific paper… where the authors
- The brain is somewhat inept at precisely locating internal pain and so sometimes we experience pain in a broad area around or near the cause, or even further afield. This is the same phenomenon as heart attack pain felt mainly in the arm: the brain just can’t figure out where the pain is coming from, and the arm pain is a bad “guess.” Patterns of referral from the musculoskeletal system are somewhat predictable, and most referred pain spreads away from the centre and the head (laterally, distally). By contrast, visceral referral is much more erratic.