The Complete Guide to Patellofemoral Pain Syndrome
An extremely detailed guide to rehab from patellofemoral pain syndrome (aka runner’s knee), with thorough reviews of every treatment option

Patellofemoral pain syndrome (PFPS), also known as runner’s knee, is the most common of all kinds of knee pain, causing pain around and under the kneecap. Almost anyone can get it, but it particularly affects runners, cyclists and hikers, and also office workers or anyone else who sits for a living. It’s also common in teens, and more than twice as common in women.1 Almost 40% of pro cyclists will get anterior knee pain in any given year,2 but runners are by far the most numerous victims, and PFPS is the most common of all runner’s knee injuries.3
Most people recover from PFPS with a little rest and then slowly working their way back to normal activity, but not everyone. This kind of runner’s knee can be extremely resistant to treatment, and sometimes becomes a seriously style-cramping chronic pain problem. Surgery for such cases is much more popular than it should be.
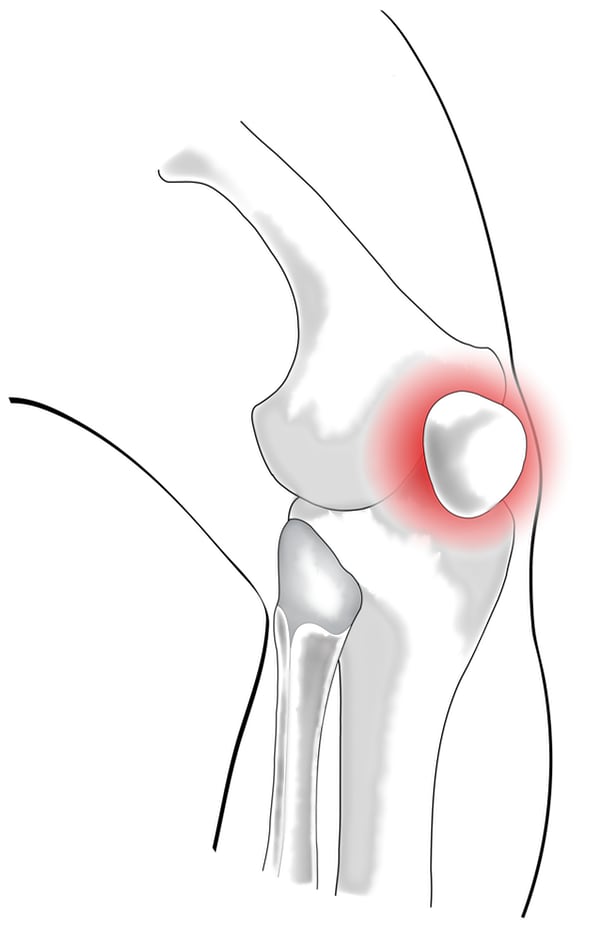
Patellofemoral pain is mostly felt directly around and under the kneecap, but there are exceptions due to knees and chronic pain being ridiculously complicated.
This deep-dive tutorial is for patients with serious and stubborn patellofemoral pain, and the professionals trying to help them. The main goal is to explore treatment and rehab, of course, but also diagnosis and the nature of the beast. It’s important to know your enemy. The book has a broad scope and is really about almost a variety of flavours of anterior pain — but “patellofemoral pain” is what people search for!
I survived a brain tumor. Knee rehab has been worse.
actual reader quote (no really, he did say that!)
An overview of patellofemoral pain
Patellofemoral syndrome is a problem with pain — and you’d be surprised how many people suspect this diagnosis and yet have no pain. The pain feels like it is mainly on the front of the knee, specifically under or around the kneecap, usually at its worst with activities like squatting, climbing, and during and after sitting. The formal definition also includes the possibility of joint noise, mild swelling, and a tender patellar facet.4
There will be (much) more detail about all of this later in the guide, but here are some quick answers to the most frequently asked questions about PFPS…
How painful is patellofemoral pain syndrome? PFPS can be painful enough to seriously interfere with walking, sitting, and sleeping, but even severe cases are usually limited to about a 5 or 6 on a scale of 10. It’s not in same league as kidney stones or gout.
Does patellofemoral syndrome cause swelling? Not often, and never severe.
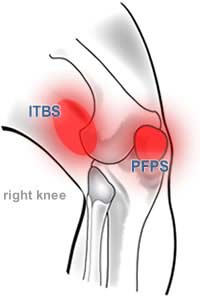
PFPS affects the kneecap and surrounding area. Don’t confuse it with iliotibial band syndrome (ITBS) which definitely affects primarily the outside of the knee (the lateral or outward-facing side of the knee). This picture is of a right knee.
Does patellofemoral syndrome ever go away? Average cases usually back off within a few months with basic taking-it-easy therapy and some basic rehab exercising.5 “Basic rehab exercising” probably isn’t particularly effective, but recovery proceeds anyway because the body is mostly quite good at healing.6 Unfortunately, some cases do worsen and persist indefinitely. If it has already been going on for several months, the sky’s the limit.
How do you treat patellofemoral pain? Mostly with “load management,” especially more initial rest than most people realize they need — simple in theory, but challenging in practice, and it won’t work with all causes of anterior knee pain. Many doctors and therapists buy into the conventional wisdom that the problem is essentially “mechanical” and they try to fix it — with corrective exercise, stretching, and surgery, for instance — but this is a simplistic view of what’s wrong in the first place.
What happens if patellofemoral pain isn’t treated? Since there is no proven or reliable treatment, there is also none to neglect. If untreated — which is effectively all most people do — it probably won't get any worse … unless you obviously push you’re your luck by overdoing it with your knees.
What exercises can I do with patellofemoral syndrome? It’s not so much “what” exercise you can do as “how soon” and “how hard” you can do them. You can do any exercise that doesn’t irritate the knee, at first, but nothing that does. As rehab progresses, you reintroduce more activities that load the knee, and eventually anything’s fair game.
Do you need surgery for patellofemoral syndrome? Very rarely. Some relatively minor procedures can become realistic options for a few severe, chronic cases.
Does patellofemoral pain affect teens more than adults? The incidence of patellofemoral pain in adolescents is only a little bit higher than it is in the general population, and it is mostly less serious. Patellofemoral pain in teens isn’t specifically covered in this guide, but it may still be useful for young patients.7Getting good care for patellofemoral pain is a challenge
Anterior knee pain may be common, but it’s surprisingly hard to find good self-help information for it. Dr. Google is always a bit sketchy, obviously.8 Even medical journals tend to be shallow and just repeat the same dubious conventional wisdom,9 and this will only get worse as AI-generated content starts to take over. A 2020 scientific paper warns specifically that online information about PFPS specifically is not good, and patients and clinicians “should not rely on general web-based information.”10 Maybe you should close this tab right now? Fortunately, this information doesn’t have any of the flaws they expose!
It’s also harder than it should be to get help from professionals. A great many of those low quality webpages about patellofemoral pain are written by clinicians promoting their practices who — how can I say this nicely? — just don’t know how much they don’t know. Few doctors or physical therapists are prepared to treat tough cases. Sports medicine in general is surprisingly primitive for a field with so much potential funding. You’d think anything affecting elite athletics would be getting more scientific attention. The situation is improving, but only recently and it still has a long way to go.11 Major deficiencies in the research as of the late 20th Century have still barely been addressed well into the 21st.12
And so, many popular treatments for PFPS are of dubious value:
- Correcting muscle imbalances and poor patellar alignment and movement is by far the most common prescription for PFPS. The idea is to teach muscles to pull more evenly on your kneecap — which good science has shown to be difficult at best, possibly impossible, and quite likely irrelevant. The science of this controversial claim will be discussed in detail below, but it’s much too uncertain for this to be a popular approach.
- Quadriceps massage and intense “fascial release” of the lateral thigh and IT band is a popular alternative treatment, but massage — while good medicine for many painful conditions — is really not very helpful for any common kind of knee pain.
- “Stay active” is one of the most common recommendations — but it can be the worst therapy of all for patellofemoral pain. While activity and exercise certainly can be useful, simply “staying active” is overly simplistic advice that can easily backfire simply by doing too much, too soon.
- Treating PFPS like arthritis is a common basic misunderstanding of the condition. Family doctors usually do this, because they are poorly informed about PFPS.13 It’s an understandable mistake — the distinction between PFPS and arthritis is complex — but it’s bad news for the patient with serious chronic pain.
- Knee surgery is rarely a good option and often prescribed prematurely. Specialists14 and orthopaedic surgeons cannot be counted upon to provide good advice for PFPS.15 Debridement in particular is a very low quality prescription16 and the research on all kinds of surgical approaches is quite discouraging. Some things just cannot be fixed with scalpels.
You should try to find good professional help, but that can be difficult — so it’s always a great idea to be as well informed as possible when you do it, or you can easily waste a lot of time and money on dubious therapies — even if this guide can’t give you “the answer,” I hope it can at least help you avoid wasting time and money on ineffective treatments.
Actual medical referral text, shared with an implied eyeroll by (highly competent) sports medicine specialist, Dr. James Noake. Just one of many clues that half of all healthcare professionals are below average.
What’s in a name? The many labels of patellofemoral pain
“Patellofemoral pain syndrome” is a surprisingly meaningless name. It basically means “strange kneecap pain,” but in Latin. “Anterior knee pain syndrome” is another common name with an even broader meaning, and it’s a little more direct and honest: it’s pain, and it’s on the front of your knee, ‘nuff said.
![A humourous graphical definition of patellofemoral pain syndrome, showing the meaning of the root “patello” means “kneecap,” the word “pain” means “ow,” and “syndrome” means “kinda mysterious.”]](/assets/images/pfps-graphic-definition--land4-500x120-10k.png)
Sometimes the “pain” part is dropped and it is just called “patellofemoral syndrome” or PFS. Sometimes syndrome is swapped out for “disorder.” And sometimes pain is replaced with “stress,” emphasizing that it’s usually a repetitive strain injury: “patellofemoral stress syndrome.” Sometimes the femur is shunned, and people just talk about patellar pain — and it probably often is the kneecap itself, and not the femur under it.
And the misspellings! No musculoskeletal condition is trickier. The number of poorly spelled Google searches for this condition is off the charts.17
“Patellofemoral pain syndrome” is the most common term. A syndrome is never a “diagnosis,” or not a good one anyway: it’s an unexplained distinctive pattern of symptoms. In the case of pain on the front of the knee, especially where overuse is a factor, we assume that those problems are coming from the patellofemoral joint, and the odds do favour that — but it’s hardly guaranteed. The patellofemoral joint is the prime suspect in most cases, but it’s not the only one. I will get into much more detail about other possibilities later in the guide.
Sometimes you’ll hear therapists or doctors call this condition “patellofemoral tracking syndrome” (PFTS) or even chondromalacia patellae (definitions and detail ahead), but these are blatantly in error: these are things that might be causes of the condition, but they are not the condition itself.

Do you live in a chair?
“Chair warriors” who spend more than 4–6 hours per day suffer as much from knee pain as many runners. Woe to runners who also work all day in a chair.
“Runner’s knee” is a popular description among runners, of course, and they do get it more often than anyone else. But it is not a great term to use, because there are at least a half dozen other conditions that term could refer to, especially iliotibial band syndrome. And then there are all those people with cyclist’s knees and hiker’s knees!
Calling it “runner’s knee” particularly leaves out people whose knees hurt while sitting and because of sitting. Office workers and other chair-bound workers really do suffer from PFPS in droves. In fact, another name for this condition is moviegoer’s knee because of the tendency of the condition to cause pain after sitting for a long time. This also explains the use of the term “theatre sign” among professionals, as in, “He’s got theatre sign — must be a case of movie-goer’s knee.” In my professional experience, however, you could just as well say, “He’s got desk job sign — must be a case of office worker’s knee.”
Part 2
Nature of the Beast
The (many) possible causes of patellofemoral syndrome
Officially, no one knows what causes it. There are many ideas, but none confirmed. Here are some typical disclaimers from scientific papers dating going back decades:
- In 1988 Potter et al. summed it up like this: “Ironically, as simple as its presentation is, lack of consensus on the fundamental factors associated with PFS remains. No agreement exists on the exact pathophysiology … .” Spoiler alert: that’s basically still the situation more than thirty years later.
- In 1993, the Clinical Journal of Sports Medicine published an editorial called “The myth, mystic and frustration of anterior knee pain,”18 a title that showed some medical uncertainty on the subject.
- But in 1998 the Journal of Orthopaedic & Sports Physical Therapy published the opinion that “there is no consensus on the most effective method of treatment … the indications and contraindications of each approach have not been well established … [and] there is no generally accepted classification scheme for patellofemoral disorders.”19
- Not long after, in 1999 in the journal American Family Physician: “Managing patellofemoral pain syndrome is a challenge, in part because of lack of consensus regarding its cause and treatment,” and “no single biomechanical factor has been identified as a primary cause of patellofemoral pain.”20 (Probably because there isn’t one.)
- You would hope for progress by 2006, but, with resounding negativity, Näslund et al. declared that “no consensus on the definition, classification, assessment, diagnosis, or management has been reached.” So, no consensus on anything — wow — and that is still true to this day.
Not much has changed. We have now at least had a formal definition since 2016.21 But in 2019, an updated physician's tutorial in American Family Physician reguritated just a couple of the clichés about causes with no disclaimers or even explanations!22
Any honest doctor or therapist should be happy to admit that PFPS is mostly still a mystery. But in practice, too many professionals think and act like the conventional wisdom is adequate.
The kneecap is all about leverage — we have kneecaps so that we can extend the knee more powerfully, as shown by this really nice little model (source unknown). But that leverage has a cost: the loading on the joint is perpetually more extreme, making the patellofemoral joint more vulnerable to fatigue and failure. More on this soon.
The conventional wisdom
In 2007 Dixit et al. declared that the mystery of PFPS was solved! In a tutorial for physicians, they confidently declared the cause of PFPS, and it was a pitch perfect rendition:
[Patellofemoral pain syndrome] is caused by imbalances in the forces controlling patellar tracking during knee flexion and extension, particularly with overloading of the joint.
Well, thank goodness! That’s nice and clear, isn’t it? The conventional wisdom says that patellofemoral pain syndrome is painful degeneration of the cartilage on the underside of the kneecap, caused by a “mechanical” failure of that joint. What kind of failure? A “tracking” problem: the patella doesn’t slide evenly in its groove or “track” on the femur.
This idea is so entrenched that many professionals consider a “tracking” syndrome to be synonymous with PFPS.
Unfortunately, the idea that tracking problems cause patellar pain has not been proven beyond a reasonable doubt. In fact, as I will show, it’s tough to even prove that tracking and pain coexist at all, let alone how much how strongly they correlate, or that tracking issues cause pain rather the other way around. Even stranger, it turns out that tracking problems are extremely difficult to even identify, let alone blame for anything.
And as if this wasn’t enough trouble for the conventional wisdom, the other really big idea about patellofemoral pain is even emptier: degeneration of the kneecap’s cartilage seems to have little or nothing to do with patellofemoral pain syndrome, despite being an obvious culprit. But that fits with a very strong theme throughout musculoskeletal medicine: structure is overrated.
Wow. That’s a lot of myths.
The evidence that tissue pathology does not explain chronic pain is overwhelming (e.g., in back pain, neck pain, and knee osteoarthritis).
Teaching people about pain — why do we keep beating around the bush?, by Lorimer Moseley, 2–3
Assault on the conventional wisdom about patellofemoral pain syndrome
Joints wear out, right? Comedian Louis CK:23
The doctor shows me an x-ray of my ankle and he’s like, “Yeah, your ankle’s just, uh … worn out.”
“What do you mean? I injured my ankle?”
He’s like, “No, it’s just shitty now.”
And yet! Pain in the patellofemoral joint mostly does not appear to be associated with any identifiable tissue degeneration or damage, dysfunction or malfunction, asymmetry or weakness.2425 Sometimes it just hurts, even though the knee — indeed, the whole leg — seem to be healthy in every way that we can measure knee health. And if that seems a bit odd, you ain’t seen nothing yet!
Even when the joint is degenerating…
END OF FREE INTRODUCTION
Purchase full access to this tutorial for USD$1995. Continue reading this page immediately after purchase. See a complete table of contents below. Most content on PainScience.com is free.?
Almost everything on this website is free: about 80% of the site by wordcount, or 95% of the bigger pages. This page is only one of 10 that have a price tag. There are also hundreds of free articles, including several about patellar pain. Book sales — over 75,500 since 2007?This is a tough number for anyone to audit, because my customer database is completely private and highly secure. But if a regulatory agency ever said “show us your math,” I certainly could! This count is automatically updated once every day or two, and rounded down to the nearest 100. Due to some oddities in technology over the years, it’s probably a bit of an underestimate. — keep the lights on and allow me to publish everything else (without ads).
Q. Ack, what’s with that surprise price tag?!
A. I know it can make a poor impression, but I have to make a living and this is the best way I’ve found to keep the lights on here.

Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
| company | PainScience.com |
|---|---|
| owner | Paul Ingraham |
| contact | 778-968-0930 |
| refunds | 100%, no time limit +Customers are welcome to ask for a refund months after purchase — I understand that it can take time to decide if information like this was worth the price for you. |
| more info | policies page ❐ |
| payments |
- What do you get, exactly? An online tutorial, book-length (104 chapters). Free updates forever, read on any device, and lend it out. E-book only! MORE
- Secure payment takes about 2 minutes. No password or login: when payment is confirmed, you are instantly granted full, permanent access to this page.MORE
- Collect them all. Get an “e-boxed” set of all 10 PainScience.com tutorials, ideal for pros … or patients with a lot of problems.MORE
Q. What am I buying? Is there an actual paper book?
A. Payment unlocks access to 97 more chapters of what is basically a huge webpage. There is no paper book — I only sell book-length online tutorials. This format is great for instant delivery, and many other benefits “traditional” e-books can’t offer, especially hassle-free lending and updates. You get free lifetime access to the always-current “live” web version (and offline reading is easy too).

Read on any device. Lend it out. New editions free forever.
Q. I just don’t like reading on the computer! Is there any way around that?
A. The design and technology of the book is ideal for reading on tablets and smart phones. You can also print the book on a home printer.
Q. Can I lend the tutorial out?
A. Yes! Feel free to lend your tutorial: I do not impose silly lending limits like with most other ebooks. No complicated policies or rules, just the honour system! You buy it, you can share it. You can also give it as a gift.
Q. Is it safe to use my credit card on your website?
A. Literally safer than a bank machine. Payments are powered by Stripe, which has an A+ Better Business Bureau rating. Card info never touches my servers. It’s easy to verify my identity and the legitimacy of my business: just Google me [new tab/window].
Q. I can really get a refund at any time?
A. Yes. All PainScience.com ebooks have a lifetime money-back guarantee.
Q. Why do you ask for contact information?
A. To prevent fraud and help with order lookups. You aren’t “subscribing” to anything: I never send email to customers except to confirm purchases.
Q. Can I buy this anywhere else? Amazon?
A. Not yet. Maybe someday.
See the “fine print page” for more about security, privacy, and refunds. No legalese, just plain English.
Save a bundle on a bundle
The e-boxed set is a bundle of all 10 book-length tutorials for sale on PainScience.com: 10 books about 10 different common injuries and pain problems. All ten topics are (all links open free intros in a new tab/window): muscle strain, muscle pain, back and neck pain, two kinds of runner’s knee (IT band syndrome and patellofemoral pain), shin splints, plantar fasciitis, and frozen shoulder. (Headache coming soon, fall of 2019.)
Most patients only need one book, because most patients have only one problem. But the set is ideal for professionals, and some keen patients do want all of them, for the education, and for lending to friends and family. And, of course, you do get a substantial discount for the bulk purchase. But no rush—complete the set later, minus the price of any books already bought. More information and purchase options.
You can also keep reading more without buying. Here are some other free samples from the book, and other closely related articles on PainScience.com:
- EXCERPT Patellofemoral Pain Diagnosis with Bone Scan
- EXCERPT Patellofemoral Pain & the Vastus Medialis Myth
- EXCERPT Patellofemoral Tracking Syndrome
- Does Cartilage Regeneration Work?
- Diagnosing Runner’s Knee
- Is Running on Pavement Risky?
- What Can a Runner With Knee Pain Do at the Gym?
- The Causes of Runner's Knee Are Rarely Obvious
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
I guarantee only education, not “results”
This book does not spell out a treatment “plan,” per se. There is no secret cure that will be revealed when you pay the fee. The entire reason the book exists is that there is not a good, reliable treatment for patellofemoral pain. It’s very important to state this clearly. Wouldn’t it be great if there were a proven treatment with minimal cost, inconvenience, or side effects? But medical science is nowhere close to this for most chronic pain conditions, and especially for patellofemoral pain.
However, there are good reasons for optimism.
What I can do is explain all the options, help you to confirm your diagnosis, and debunk bad ideas. It may or may not lead to a “cure,” but it will get you as close as you can get. Some readers will finally break free of their patellar pain. Others will make progress after ditching a counter-productive therapy, or trying an option they didn’t know about before. And maybe that is kind of miraculous.
Mostly what’s for sale here is simply a deep understanding of the subject and your options. For some people, it’s worth $20 just to feel like they aren’t overlooking something. In general, if it’s not in this tutorial, it probably doesn’t matter.
And $20 is lot cheaper than even a single appointment with most healthcare professionals. And you might just get more out of it.
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
Answers to more of your frequently asked questions about patellofemoral pain
I covered some of the most common questions earlier in the introduction, and here are several more: the questions people are actually asking in large numbers (taken straight from Google searches). The answers are basic — they represent the truth, but not the whole truth. They are quick notes extracted from the more detailed answers in the full book.
Will a knee brace help patellofemoral syndrome? Bracing is no cure, but a soft and comfy brace may limit knee use while also making the knee feel a bit “safer,” which can provide some short term pain relief.
Is cycling good for patellofemoral syndrome? No and then yes. All forms of exercise that aggravate patellofemoral pain are bad for it in the early stages of rehab, and then slowly become good for it later on as your load tolerance increases.
Can I walk with patellofemoral pain syndrome? Yes, but less in the early stages of recovery, and it may make sense to avoid altogether for a while. Walking on stairs/hills should be treated as a much more significant source of knee stress than flat walking.
Can patellofemoral pain be cured? In rare cases, a specific cause can be identified and fixed to completely resolve the pain. But those cases are quite rare.
How do you sleep with patellofemoral syndrome? Avoid any joint position that seems to irritate it. Slight flexion is usually the safest and most comfortable position.
What is the best painkiller for knee pain? Topical anti-inflammatory drugs based on either salicylates or diclofenac.
Does patellofemoral syndrome lead to arthritis? Patellofemoral pain can probably contribute to the development of arthritis, but only a little, and only in the long-term.
How do you test for patellofemoral syndrome? You don’t. As a “syndrome,” patellofemoral pain is defined almost entirely by its symptoms; no objective sign is definitive.
How do you know if you have a torn meniscus in your knee? Damaged menisci are usually associated with excessive joint noise, erratic locking, instability, and giving way.
Can just the patella be replaced? It’s technically possible, but never actually done. The cartilage can be replaced, however.
Why does my knee hurt when I get up from sitting? Sitting is more stressful to the knee than most people realize. Simply bending the knee applies considerable pressure to the patellofemoral joint surfaces.
How do you fix a tilted kneecap? Odd patellar angles are common and not a cause of patellofemoral pain, and usually cannot be changed in any case. They are one of the “biomechanical bogeymen” of patellofemoral pain.
What is patellofemoral friction syndrome? It’s not a real name or concept, except as a common misunderstanding. It’s probably based on confusion with IT band friction syndrome (which is itself a misleading label, but one that referes to a well-known idea about how IT band syndrome allegedly works).
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
Part 2.3
Appendices
Reader feedback … good and bad
Testimonials on health care websites reek of quackery, so publishing them has always made me a bit queasy. But my testimonials are mostly about the quality of the information I’m selling, and I hope that makes all the difference. So here are some highlights from the kind words I’ve received over the years … plus some of the common criticisms I receive, at the end. These are all genuine testimonials, mostly received by email. In many cases I withold or change names and identifying details.
I just finished your e-book about patellofemoral pain syndrome and wanted to say that it was very helpful! As a chronic sufferer of PFPS, I have personally experimented and learned the hard way about almost all of the experiences you mentioned and found most of them to be spot on. I wish I had found this information 15 years ago, but it was helpful to confirm that I'm not alone and reinforce what I learned through personal experience.
Jerry Taylor
Thanks for a well written, humorous and informative piece. Your book helped me understand what I did to my knee running and how to treat (and not treat!) stubborn injury. Might see you jogging through Stanley Park or water front, on one of our visits to daughter, love Vancouver.
Matt Randlett
I wanted to write a short thank you email for all the help you have brought me. Im a recently graduated medicine student from Argentina, and i have been getting knee pain for almost 8 months. I have been to the best traumatologists in the country, none who could explain correctly what was going on with my knee. They did exactly the kind of mistakes you constantly mention all along your book.By reading the tutorial i have at last fully understood what im up against, how to correctly fight it, and hopefully beat the crap out of this horrible pain.Just wanted to write this short thank you email, you should know your amazing work helps people all around the globe.
Petra Fellows
My name is Lexy, I’m a 23-year-old with patellofemoral syndrome. For the past six months. I don’t have any questions really, but I wanted to reach out and let you know how valuable your writing has been to me. I’m just an occasional visitor of painscience.com, but when I get those mental waves of dread that tell me my injury is going to last forever, your writing style has been super helpful in putting things in perspective, and helping me be realistic, yet hopeful about my recovery. I’ve seen PTs, acupuncturists, orthopedic surgeons and doctors, many of which have given me shit advice and left me feeling upset and angry, or like my pain wasn’t being taken seriously. I thank you for creating a forum where I feel a sense of solidarity with other humans/athletes, and most importantly where I don’t feel like I have to pay a ridiculous amount of money to feel like a factory-line patient. I really appreciate that.
Shakil Irvine
I wanted to send you a quick email to deeply thank you for all your work. I grappled for 18-months with horrible knee pain that threw my life into a tailspin. Your books were critical for getting me on the path to healing. I have spent much of my career in health research and policy and really admire your ability to distill evidence and then present it clearly and accurately to a general audience. Thank you.
Franco Sargent
Your tutorial on patellarfemoral syndrome really cut through a lot of misinformation I’ve received from MDs and PTs.
Alastair Rosario
Given what I have learned about patellofemoral pain syndrome over the last two years through personal experience, your tutorial is probably the best summary of everything I have seen.
anonymous
This has already served as a massive eye opener for me. It makes a huge amount of sense where previously there was only confusion.
Greg Bruce, “struggling masters athlete”
Just reading tutorial has already given me hope that I can finally get some relief from my chronic patellofemoral pain syndrome. Why didn’t I find this 2 years ago?! It has been so frustrating, both physically and emotionally, as I’m sure you already know from your patients. Your eBook is very enlightening and well written. Please feel free to use my comments as a testimonial. I was glad to see other testimonials, too — it’s nice to know that I’m not the only one who is struggling with this.
Melanie Caldwell, Yonkers, NY
Finding this information was a huge relief for me. I really did think I had “tried everything.” But I found pages and pages of stuff in your article that no other doctor or therapist had ever even mentioned.
Jared Foster, long-distance runner
One more noteworthy endorsement, with regards to this whole website and all of my books, submitted by a London physician specializing in chronic pain, medical education, and patient-advocacy (that’s a link to his excellent blog):
I’m writing to congratulate and thank you for your impressive ongoing review of musculoskeletal research. I teach a course, Medicine in Society, at St. Leonards Hospital in Hoxton. I originally stumbled across your website whilst looking for information about pain for my medical students, and have recommended your tutorials to them. Your work deserves special mention for its transparency, evidence base, clear presentation, educational content, regular documented updates, and lack of any commercial promotional material.
Dr. Jonathon Tomlinson, MBBS, DRCOG, MRCGP, MA, The Lawson Practice, London
What about criticism and complaints?
Oh, I get those too! I do not host public comments on PainScience.com for many reasons, but emailed constructive criticism, factual corrections, requests, and suggestions are all very welcome. I have made many important changes to this tutorial inspired directly by critical, informed reader feedback.
But you can’t make everyone happy! Some people demand their money back (and get it). I have about a 1% refund rate (far better than average in retail/e-commerce). The complaints of my most dissatisfied customers have strong themes:
- Too negative in general. Some people just can’t stomach all the debunking. Such customers often think that I dismiss “everything” … which I disagree with.
- Too negative specifically. Some are offended by my criticisms of a treatment option that they personally use and like. Or sell!
- Too advanced. Although I work hard to “dumb” the material down, quite a few people still just find it too dense and dorky.
- Too simple. Some people think they already know everything about the topic. Maybe they do, and maybe they don’t. I always wish I could give these readers a pop quiz. 😉 In my experience, all truly knowledegable people get that way by embracing every new persective and source of information.
Acknowledgements
Thanks to Dr. Scott Dye for helping me to understand and believe in my own unconventional ideas about patellofemoral pain syndrome, and by extension every other joint problem.
Extra special thanks to Tony Ingram, for substantial contributions of expertise and writing to this book in 2014 — the book is much better for it.
Thanks to every reader, client, and book customer for your curiosity, your faith, and your feedback and suggestions, and your stories most of all — without you, all of this would be impossible and pointless.
Writers go on and on about how grateful they are for the support they had while writing one measly book, but this website is actually a much bigger project than a book. PainScience.com was originally created in my so-called “spare time” with a lot of assistance from family and friends (see the origin story). Thanks to my wife for countless indulgences large and small; to my parents for (possibly blind) faith in me, and much copyediting; and to friends and technical mentors Mike, Dirk, Aaron, and Erin for endless useful chats, repeatedly saving my ass, plus actually building many of the nifty features of this website.
Special thanks to some professionals and experts who have been particularly inspiring and/or directly supportive: Dr. Rob Tarzwell, Dr. Steven Novella, Dr. David Gorski, Sam Homola, DC, Dr. Mark Crislip, Scott Gavura, Dr. Harriet Hall, Dr. Stephen Barrett, Dr. Greg Lehman, Dr. Jason Silvernail, Todd Hargrove, Nick Ng, Alice Sanvito, Dr. Chris Moyer, Lars Avemarie, PT, Dr. Brian James, Bodhi Haraldsson, Diane Jacobs, Adam Meakins, Sol Orwell, Laura Allen, James Fell, Dr. Ravensara Travillian, Dr. Neil O’Connell, Dr. Tony Ingram, Dr. Jim Eubanks, Kira Stoops, Dr. Bronnie Thompson, Dr. James Coyne, Alex Hutchinson, Dr. David Colquhoun, Bas Asselbergs … and almost certainly a dozen more I am embarrassed to have neglected.
I work “alone,” but not really, thanks to all these people.
I have some relationship with everyone named above, but there are also many experts who have influenced me that I am not privileged to know personally. Some of the most notable are: Drs. Lorimer Moseley, David Butler, Gordon Waddell, Robert Sapolsky, Brad Schoenfeld, Edzard Ernst, Jan Dommerholt, Simon Singh, Ben Goldacre, Atul Gawande, and Nikolai Boguduk.
About the 2nd Edition
The 2nd “edition” of the PFPS tutorial was launched on July 28, 2014, after months of collaboration with Tony Ingram, a Physical Therapist who did his Masters thesis on anterior knee pain. Tony was officially a co-author for a while, but retreated to focus on pursuing a PhD and a career in science.
Like all my books, this one was updated many times over the years, but changes were too small and spread out to constitute an “edition”: that had to wait for this, by far the largest ever major change to the book. It has several new sections, a lot of new science, and a strong (and overdue) new emphasis on the evidence-based value of exercise — reversing my grumpy anti-exercise position. It’s also much less exclusively about a single theory of knee pain than it was.
A new position on exercise
Exercise for patellofemoral pain syndrome is a good example of a treatment that works, but probably doesn’t work how most people think it works. I was anti-exercise before because the evidence just wasn’t there for it yet, and too many professionals fancied that they were prescribing exercise to change biomechanical parameters (e.g. patellar tracking) that correlated poorly with the condition. Such prescriptions tended to be overzealous: too much exercise, too soon for patients suffering from what is fundamentally an overuse condition.
Now there is good evidence that exercise is effective — hallelujah, some much-needed good news — but dosage and timing are key, and the biomechanical rationale still needs to be taken out with the trash.
Not just one guy’s theory any more
The previous version of the book had a significant weakness, a major idea about the nature of the beast (basically the whole “it’s the homeostasis, stupid,” ). The idea was plausible and elegant, but lacked adequate scientific support for an important basic point of the book. One advanced reader complained:
I didn’t buy your book so I could get one guy’s theory about how patellofemoral pain syndrome works.
Fair enough. She went on to say that it was probably a pretty good idea, just painfully unsupported. Simple as it is, that’s one of the best single constructive criticisms I’ve ever received. On the one hand, I unapologetically offer my take on these complex subjects. They are my books, and this is not a medical journal. On the other hand, I don’t want my take to be based solely on private speculation — if my opinion is to have much value, it should be clearly based on a diversity of expert and scientific sources. And so this is one of the major repairs in the 2nd edition. My basic point was sound, but badly needed some scientific and more diverse expert support — and now it has that.
Further Reading
- “The pathophysiology of patellofemoral pain: a tissue homeostasis perspective,” Dye, Clinical Orthopaedics & Related Research, 2005. This article by Scott F. Dye, MD, an orthopaedic surgeon from San Francisco, was by far the most influential source for this article. I do not normally recommend scientific articles to my readers, most of whom are ordinary people with knee pain, and not especially interested in slogging through medical jargon. However, in this case, I have to make an exception: although Dr. Dye’s writing is certainly intended for a professional audience, patients should still be able to get something out of it. It’s clear (for a scientific paper) and sensible, and even somewhat visionary in tone. Despite the fact that it’s certainly harder reading than this article, and despite the cost — the article will set you back US$10 to access — I still think it’s worth it. If you really want a good depth of understanding of PFPS, it’s required reading.
- Massage Therapy for Your Quads will add to your understanding of the quadriceps muscle group and its relationship to the kneecap.
- There are other kinds of knee pain, and it’s not always easy to tell which kind you’ve got. In particular, the two main types of runners knee are often confused. Tell them apart with this quick guide and checklist: Diagnosing Runner’s Knee.
- The journal American Family Physician publishes free tutorials for doctors which may also be useful for patients. I have come to trust those tutorials as one of the best sources available when I am trying to understand conventional medical opinion. They are usually well-written and beautifully illustrated, and determined patients can often get plenty of value out of them despite the jargon. See “Patellofemoral pain syndrome: a review and guidelines for treatment” for a 1999 tutorial for doctors, and “Management of patellofemoral pain syndrome” for their 2007 article on the subject. Bear in mind that these articles present only the conventional wisdom, however, and primarily discuss structural explanations for knee pain. As such, I do not think that they are useful to my patients and readers except as the best available representation of conventional wisdom.
- One of the hottest and most controversial treatment ideas for patellar pain is the idea that strengthening your hips will help. I explore the controversy here: Does Hip Strengthening Work for IT Band Syndrome?
A few more articles about patellofemoral pain syndrome and related topics:
- Should You Get A Lube Job for Your Arthritic Knee? — Reviewing the science of injecting artificial synovial fluid, especially for patellofemoral pain
- Is Knee Pain More Common in Women? — The relationship between sex and knee pain, especially runner’s knee (IT band syndrome, patellofemoral pain)
- Is Running on Pavement Risky? — Hard-surface running might be a risk factor for running injuries like patellofemoral pain, IT band syndrome, shin splints, and plantar fasciitis
- What Can a Runner With Knee Pain Do at the Gym? — Some training options and considerations for runners (and others) with overuse injuries of the knee
- The Dubious Science of Kinesiology Tape — The origin story and science of therapy tapes like Kinesio Tape, KT Tape, Spider-Tech, RockTape
- Knee Debridement is a Completely Ineffective Procedure — Evidence that arthroscopic knee surgery for osteoarthritis is about as useful as a Nerf hammer
What’s new in this tutorial?
The original publication date of this tutorial has been lost, but I think it was in 2004. It was quite rudimentary until 2007, when significant upgrades began. This change log was started in May 2007, along with many major improvements. As you can see, the tutorial has been updated many times since, and remains a live document.
Regular updates are a key feature of PainScience.com tutorials. As new science and information becomes available, I upgrade them, and the most recent version is always automatically available to customers. Unlike regular books, and even e-books (which can be obsolete by the time they are published, and can go years between editions) this document is updated at least once every three months and often much more. I also log updates, making it easy for readers to see what’s changed. This tutorial has gotten 147 major and minor updates since I started logging carefully in late 2009 (plus countless minor tweaks and touch-ups).
Mar 3, 2026 — New chapter: No notes. Just a new chapter. [Updated section: Tendon failure as a drug side effect.]
2024 — Science update: At last, some long-awaited new patellar circulation evidence, plus significant revision and other improvements, especially the addition of a new discussion about the therapeutic implications (does exercise improve circulation, mainly). [Updated section: Blood-starved kneecaps.]
2024 — Editing: Just editing, but a noteworthy batch of edits to several chapters. I made minor corrections and adjustments to every recently added or revised chapter, and some small but (I hope) meaningful clarifications to how “resting” is presented as a treatment strategy.
2024 — New sub-topic: Added a substantial discussion of patellofemoral joint replacement, and made a number of other modest improvements to the surgery chapter. [Updated section: Surgery is only a last resort.]
2024 — Minor upgrades: After publishing part of this chapter as an excerpt, I made several minor improvements, and added one simple diagram. [Updated section: Under pressure.]
2024 — New chapter: No notes. Just a new chapter. [Updated section: Self-examination of patellofemoral joint tenderness: prodding under the kneecap.]
2024 — New section: No notes. Just a new chapter. [Updated section: Simple gait retraining: softer and/or quicker running may improve patellofemoral pain.]
2023 — New content: Added a fascinating and extreme case study that perfectly illustrates the potential relationship between ITBS and patellofemoral pain (though still exasperatingly unclear). Includes audio version. [Updated section: Tight IT bands.]
2023 — Revised and expanded: The section had been short and basic for many years, and many readers would never have guessed how much more I’ve written about this topic. It’s now more thorough and more in tune with the times, including the modern skeptical pespective on trigger points, and a more nuanced discussion of what role they might or might not have in patellofemoral pain. [Updated section: And what about trigger points?]
2023 — Minor editing: Just a few little improvements, especially harmonizing with the IT band tightness chapter. [Updated section: ITBS vs. PFPS (in detail).]
2023 — Many improvements: After greatly expanding this chapter in 2022, it was a bit of a mess: thorough but disorganized. I eliminated some egregious rambling (was I drunk?). [Updated section: 16 other causes and diagnoses of anterior knee pain.]
2023 — New topic: Added a small section: “Be careful what you wish for: pain relief can be problematic.” [Updated section: You and “vitamin I”: anti-inflammatory meds, especially Voltaren® Gel.]
2023 — Major revision: I pretty much just started from scratch and re-wrote this chapter. It’s now better in all the ways, I think. [Updated section: Diagnosis: How do I know I’ve got patellofemoral syndrome?]
2023 — New section: No notes. Just a new chapter. [Updated section: Who should be encouraged to stop running? Four not-so-rare “exceptions” to the rule runners should rarely be discouraged.]
2023 — New sub-topic: Added a substantive new sub-topic: “Built for pressure: How thick is the patellofemoral joint cartilage? And the patella?” [Updated section: Under pressure.]
2023 — Evidence update: Updated several references throughout the introductory sections, along with many related edits and improvements.
2023 — Science update: Added an important footnote with a bunch of detail about exactly what kind of strength training was tested by Hansen et al. [Updated section: Does exercise work for patellofemoral pain? Treating the knee with strength.]
2023 — Science update: After almost a decade without a meaningful update, new evidence from Hansen et al. has forced a rewrite of this chapter! [Updated section: Does exercise work for patellofemoral pain? Treating the knee with strength.]
2023 — Science update: Cited a case study about mistaking Parkinsonian dystonia for a knee injury. [Updated section: 16 other causes and diagnoses of anterior knee pain.]
2023 — Reorganization: Just a bit of housekeeping: rearranged the content and edited for clarity. Probably not enough, but it’s a start. [Updated section: 16 other causes and diagnoses of anterior knee pain.]
Archived updates — All updates, including 111 older updates, are listed on another page. ❐
2003 — Publication.
Notes
- Boling M, Padua D, Marshall S, et al. Gender differences in the incidence and prevalence of patellofemoral pain syndrome. Scand J Med Sci Sports. 2010 Oct;20(5):725–30. PubMed 19765240 ❐ PainSci Bibliography 53958 ❐
Following over 1000 army recruits (once again) for 2.5 years, Boling et al. found women to be 2.23 times more likely to develop and report patellofemoral pain than men. The study design and analysis seems to be of pretty high quality. Maybe there’s something peculiar about the knees of women interested in a military career — but that seems unlikely.
- Clarsen B, Krosshaug T, Bahr R. Overuse Injuries in Professional Road Cyclists. Am J Sports Med. 2010 Sep. PubMed 20847225 ❐
- Taunton JE, Ryan MB, Clement DB, et al. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med. 2002;36(2):95–101.
This report on two year’s worth of injuries among Vancouver runners — many of whom I probably run with routinely on Vancouver’s famous sea wall, or the Arbutus corridor Greenway — found that “patellofemoral pain syndrome was the most common injury, followed by iliotibial band friction syndrome, plantar fasciitis, meniscal injuries of the knee, and tibial stress syndrome.”
- Crossley KM, Stefanik JJ, Selfe J, et al. 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 1: Terminology, definitions, clinical examination, natural history, patellofemoral osteoarthritis and patient-reported outcome measures. Br J Sports Med. 2016 Jul;50(14):839–43. PubMed 27343241 ❐ PainSci Bibliography 52793 ❐
The definition is formal and official insofar as it was agreed on by a bunch of experts who got together to hammer one out, and that’s surprisingly recent: 2016!
“The core criterion required to define patellofemoral pain is pain around or behind the patella, which is aggravated by at least one activity that loads the patellofemoral joint during weight bearing on a flexed knee (eg, squatting, stair ambulation, jogging/running, hopping/jumping).”
They also included some “maybe” signs and symptoms: joint noise, mild swelling, pain after sitting, and a tender patellar facet.
The patellar facets are the joint surfaces on the underside of the kneecap. It’s hard to feel them, but when the knee is straight and relaxed you can basically pry it up and get the tip of a finger under there to see if it’s hurty. It often is with patellofemoral pain.
- Dixit S, DiFiori JP, Burton M, Mines B. Management of patellofemoral pain syndrome. Am Fam Physician. 2007;75:194–202. PubMed 17263214 ❐ PainSci Bibliography 56699 ❐ “ … although management can be challenging, a well-designed, non-operative treatment program usually allows patients to return to recreational and competitive activities.”
- Most “basic” physical therapy for PFPS consists of minor interventions of dubious value — mostly corrective exercises, stretching, ultrasound, taping and strapping — yet the clinical impression of most professionals is that mild patellofemoral pain does go away with conservative advice. The most likely explanation for this — and it’s a common “problem” in physical therapy — is simply that most of those cases would have gotten better regardless of the therapy. Of course, in some cases, some good advice may be mixed in with bad advice, and that may help. And there may be some placebo effect: being therapized really does help a lot of people to feel better, regardless of whether or not the therapy makes any sense, and yes this phenomenon can occur even with something as seemingly un-psychological as knee pain! See Moseley.
- It is mostly a temporary condition: they recover from or grow out of more easily than adults do. Although serious cases certainly can and do occur in teenagers, their age is not particularly relevant to those cases. A serious case in a teenager has to be handled in pretty much the same way that you would handle a serious case in an adult. So although age is a factor I haven’t focused on, everything that I have focused on should be of interest to teens with persistent knee pain.
- Starman JS, Gettys FK, Capo JA, et al. Quality and content of internet-based information for ten common orthopaedic sports medicine diagnoses. J Bone Joint Surg Am. 2010 Jul;92(7):1612–8. PubMed 20595567 ❐
Researchers evaluated the accuracy of top Internet sources of information about common orthopedic conditions, such as knee injuries and low back pain, reporting that “the quality and content of health information on the Internet is highly variable for common sports medicine topics.” Brought to you by the Department of Duh! That conclusion is just a bit of an understatement: there are lots of prominent sites peddling the most astonishing nonsense.
As of 2023, this remains the most recent paper about the quality of online sports medicine content, and obviously the Internet has changed a lot since 2023 … but not generally for the better!
Dr. Steven Novella wrote about this study, commenting specifically on privately run health information sites like PainScience.com:
It is also not surprising that individual sites also scored relatively low on average. An individually run site is only as good as the individual running it, so there is bound to be a great deal of variability. Also, individuals are more likely to make mistakes or have missing information than groups.
Amen!
- Petersen W, Ellermann A, Gösele-Koppenburg A, et al. Patellofemoral pain syndrome. Knee Surg Sports Traumatol Arthrosc. 2014 Oct;22(10):2264–74. PubMed 24221245 ❐ PainSci Bibliography 51593 ❐
This paper is a general review of patellofemoral pain and is a fine example of all the best in conventional wisdom. On the one hand, it is a generally credible mainstream scientific publication with plentiful citations providing at least some support for its key points. On the other? Most of those points remain controversial and have been credibly challenged by various experts, some of the support is weak to the point of being bogus.
As one example, the authors acknowledge, barely, that patellar maltracking is controversial, but they wave it away: “Recent studies, however, show that maltracking of the patella probably plays a key role.” But their citations are not persuasive, and they do even attempt to address any of the standard rebuttals.
The whole paper is quite rudimentary. But, for the sake of balance, if you wanted one scientific paper that represents the conventional wisdom, this is the citation you’re looking for!
- de Oliveira Silva D, Rathleff MS, Holden S, et al. Patients and clinicians managing patellofemoral pain should not rely on general web-based information. Phys Ther Sport. 2020 Sep;45:176–180. PubMed 32810696 ❐
This citation is so perfect for my purposes here that it’s like de Oliveira Silva et al. wanted to write a paper just for me. These authors read 40 webpages about patellofemoral pain and judged how well they harmonized with current expert consensus (as reported in papers like Crossley 2016, which is well known to me).
Almost half the articles they looked at did not mention their sources, and half of those that did. This page is littered with hundreds of obviously peer-reviewed citations. With summaries. And often detailed analysis.
The most common misinformation was broken definitions of patellofemoral pain (20% of pages), and about clinical examination (15%). This page goes into extraordinary detail about the official definition and where it comes from, and accurately reports the issues with clinical exams and tests, citing multiple sources.
22% of pages recommended surgery, which is bonkers — I downvote surgery in my second paragraph, and have a chapter titled “Surgery is only a last resort.”
Oliveira Silva et al. conclude:
Due to the commonality of PFP and potential for improving self-management, there is an urgent need to develop more accurate and comprehensive web-based patient education resources for PFP.
Or people could just read this one. 🙂
- Grant HM, Tjoumakaris FP, Maltenfort MG, Freedman KB. Levels of Evidence in the Clinical Sports Medicine Literature: Are We Getting Better Over Time? Am J Sports Med. 2014 Apr;42(7):1738–1742. PubMed 24758781 ❐
Things may be getting better: “The emphasis on increasing levels of evidence to guide treatment decisions for sports medicine patients may be taking effect.” Fantastic news, if true! On the other hand, maybe I should be careful what I wish for, since my entire career is based on making some sense out of the hopeless mess that is sports and musculoskeletal medicine …
- Thomeé R, Augustsson J, Karlsson J. Patellofemoral pain syndrome: a review of current issues. Sports Med. 1999 Oct;28(4):245–62. PubMed 10565551 ❐
A review of “current” patellofemoral pain issues in 1999. Given the sad pace of progress in this field, it’s fair to say that, even a great many years later, we still don’t have a “clear consensus in the literature concerning the terminology, aetiology and treatment for pain in the anterior part of the knee.”
Two major general explanations for PFPS, “malalignment” and “muscle balance,” were unsupported by evidence then … and are still that way now.
Thomeé, Augustsson, and Karlsson also called for treatments to be studied with “prospective, randomised, controlled, long term studies using validated outcome measures.” Do those exist today? Nope.
This is not to say that no progress has been made whatsoever, but it is not great, and this 1999 paper strongly remains depressingly “current” more than 20 years after its publication.
- Most doctors lack the skills and knowledge needed to care for common aches, pains, and injury problems, especially the chronic cases, which they tend to underestimate the complexity of. This has been shown by many studies, like Stockard et al., who found that 82% of medical graduates “failed to demonstrate basic competency in musculoskeletal medicine.” It’s just not their thing, and people with puzzling or stubborn pain should take their family doctor’s advice with a large grain of salt, and even lower their expectations of specialists (who tend to be too specialized). See The Medical Blind Spot for Aches, Pains & Injuries: Most physicians are unqualified to care for many common pain and injury problems, especially the more stubborn and tricky ones.
![Cartoon of a man sitting in a doctor’s office. The doctor is holding a clipboard with a checklist with just two items on it: stress related and age related. The caption reads: “An extremely general practitioner.”]()
- Sports medicine specialists are probably the least of all evils — although no professional category seems generally well-informed about PFPS, you probably stand a somewhat better chance of getting competent help from a sports medicine doctor than from any other kind of health care professional. Although they are more or less as prone to the toeing the line of conventional wisdom as any other health care professional, at least their expertise is directly concerned with non-surgical management of conditions like PFPS — and so there is at least some respectable chance that a doctor in this speciality will have paid some attention to the scientific controversies.
- Orthopaedic surgeons are surgeons — not only do surgeons strongly tend to perceive musculoskeletal problems only in terms of surgical solutions, but they are (quite correctly) professionally preoccupied with their surgical expertise and professional development, which means that they are typically not knowledgeable about conservative physical therapy methods for relatively minor overuse injuries like PFPS. Many of them certainly try to make a professional point of avoiding the overprescription of surgery, but that doesn’t necessarily make them experts in what to do instead of surgery. And PFPS is a particularly bad problem to take to a surgeon for the simple reason that, among knee injuries, PFPS is just about the last one that you’d want to operate on. This will be fully explained as we continue with the tutorial.
- Surgeons often oversimplify patellofemoral pain syndrome as simply a case of “arthritis” of that joint, and recommend a debridement (filing or smoothing) of the knee cartilage, either of the patellofemoral joint, or of the main joint between the tibia and femur (which is particularly irrelevant to patellofemoral pain). However, debridement has been proven to be ineffective even for arthritis (let alone PFPS, which isn’t arthritis), originally and most spectacularly by Moseley in 2002, then most authoritatively by The Cochrane Collaboration in early 2008 (see Laupattarakasem), and most recently by New England Journal of Medicine in September 2008 (see Kirkley). This is one of the most straightforward scientific slam dunks in surgery research in recent history — surgical debridement doesn’t work!
- There are more misspelled searches for this than any other topic on this huge website. A lot more. Femoral patella syndrome, patellar femoral, patellafemoral, femoropatellar syndrome! Those are the actual four most common, and there are many more, and much worse: patel, patlofemal, patalafremerol, fermopaltela, etcetlero! Both “petalla” and “femoral” are easy to get wrong independently, and when people try to merge them… well, it’s a spelling meltdown.
- Reid DC. The myth, mystic and frustration of anterior knee pain. Clin J Sport Med. 1993;3:139–43. PainSci Bibliography 56702 ❐
- Wilk KE, Davies GJ, Mangine RE, Malone TR. Patellofemoral disorders: a classification system and clinical guidelines for nonoperative rehabilitation. JOSPT Open. 1998;28(5):307–322.
- Juhn MS. Patellofemoral pain syndrome: a review and guidelines for treatment. Am Fam Physician. 1999;60(7):2012–2022. PainSci Bibliography 56687 ❐
- Crossley 2016, op. cit.
- Gaitonde DY, Ericksen A, Robbins RC. Patellofemoral Pain Syndrome. Am Fam Physician. 2019 Jan;99(2):88–94. PubMed 30633480 ❐ The paper contains almost no information about etiology at all. There are just two paragraphs, barely more content than this footnote: one common idea is dismissed because it has “not been shown to be a clear contributing cause,” another is simply presented as something that “is believed” … with a single indirectly related citation to “support” it.
- A one-minute excerpt from his 2008 stand-up show Chewed Up is embedded below, but you can also watch the full segment (2:30) on YouTube. Funny stuff!
- Näslund J, Näslund UB, Odenbring S, Lundeberg T. Comparison of symptoms and clinical findings in subgroups of individuals with patellofemoral pain. Physiotherapy Theory and Practice. 2006 Jun;22(3):105–18. PubMed 16848349 ❐ In this study of 80 patients with a diagnosis of PFPS, with all other likely diagnoses already eliminated from consideration, signs of pathology were found in only 17 of 75 patients, and the authors conclude that even these “cannot be detected from ... commonly used clinical tests.” That’s quite a few mysteriously painful knees.
- Piva SR, Fitzgerald GK, Irrgang JJ, et al. Associates of physical function and pain in patients with patellofemoral pain syndrome. Arch Phys Med Rehabil. 2009 Feb;90(2):285–95. PubMed 19236982 ❐
Researchers tested 74 patients diagnosed with patellofemoral pain syndrome for the presence of several factor that are commonly suspected to be associated with that condition, the “usual biomechanical suspects”: muscle weakness and tightness, coordination, and postural and anatomical abnormalities. They also considered psychological factors, which is quite unusual for a study of knee pain.
They found no correlation at all with between the biomechanical factors and chronic anterior knee pain.
Interestingly, the researchers did find that “psychologic factors [anxiety and fear-avoidance beliefs about work and physical activity] were the only associates of function and pain in patients with PFPS.”

There are 351 more footnotes in the full version of the book. I really like footnotes, and I try to have fun with them.
Jump back to:
The introduction
Paywall & purchase info
Table of contents
Top of the footnotes
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help