Shin Splints Treatment, The Complete Guide
An extremely detailed guide to all types of shin splints for both patients and professionals, including thorough reviews of every possible treatment option, and all about the nature of the beast

Shin splints is a common and often chronic running injury, yet poorly understood by most health care professionals.
Shin splints is an extremely common repetitive strain injury in runners and running athletes. It can be impressively stubborn, because there are several possible overlapping types/causes, some more subtle and less “mechanical” than most people ever suspect. Shin splints treatment depends on what type you have.
“Many people are afraid of running because 30 to 70 percent (depending on how you measure it) of runners get injured every year.”1 As many as a third of those injuries involve shin pain,23 and at least 3% of generally active people.4
“Shin splints” is a curiously old-fashioned term — like “lumbago” or “consumption.” Why does only shin pain get called “splints”?5 Because shin splints means painful shins — sort of6 — it’s a bit silly to offer it up as a diagnosis:
“Doctor, I have shin pain.”
“Ah, you have shin splints!”
“I just said that.”
Without a more specific diagnosis, shin splints should probably just be called “anterior lower leg pain” or “tibial pain syndrome” — unexplained pain around the tibia, the big shin bone.
Shin splints treatment is 90% about "rest" (load management), but what counts for chronic cases is that last 10%. So how do you help shin splints? What works, what doesn’t, and — most importantly — why? This tutorial reviews all of the treatment options, but you cannot treat what you do not understand, so we begin with the nature of the beast (etiology).
The major types of shin splints: compartment syndrome, medial tibial stress syndrome, and stress fracture
Which shin splints is the “real” one? The term has multiple personality disorder: it might refer to nearly any of several problems that cause shin pain, depending on what you read or who you talk to. This extremely detailed tutorial aims to help readers, both professionals and patients, with all the different shin pain problems that get stuck with the same label. All of these things (at least) are the “real” shin splints:
People often mistakenly believe that the real shin splints is limited to just one of these. For instance, medial tibial stress syndrome — irritation and degeneration of the shin bone, and/or the soft tissue around it — is probably what most professionals think shin splints is these days, and it probably is the most common type of shin pain. But it is definitely not the only kind.
The confusion about the naming of shin pain probably can be traced to the truly deep and cosmic mysteries that surround shin pain. Many cases defy easy classification. Either they seem to possess the symptoms of several different problems, or they actually are more than one problem.7 Many scientific studies of shin pain have created more questions than they answered. Diagnosis and treatment can be difficult, and some cases are almost freakishly severe.
This tutorial thoroughly explores every common type of shin pain: the kinds of tissue failure involved, surprising scientific controversies and mysteries, plus the most neglected and underestimated factors in shin pain, crucial to understanding many difficult cases.
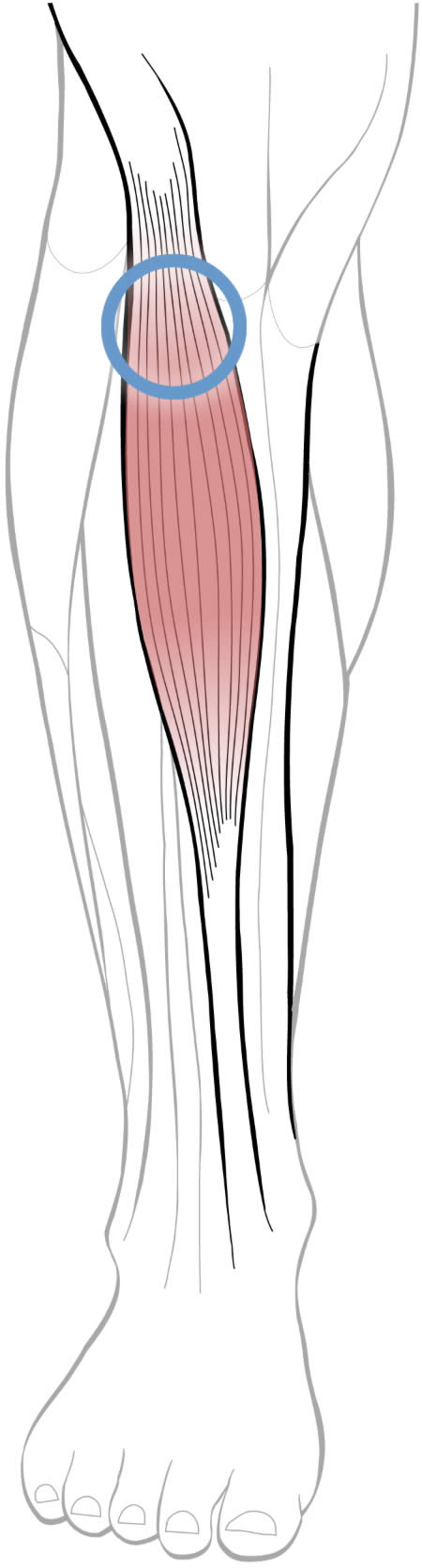
The tibialis anterior muscle of the shin usually contains significant myofascial trigger points (muscle knots) — an under-diagnosed and under-treated factor in many cases of shin pain.
Shin pain is routinely misunderstood and mistreated
Sports medicine in general is amazingly primitive considering how much potential funding it has. You’d think anything affecting elite athletes with huge audiences would be getting more attention! The situation is improving, but only recently and it still has a long way to go.8
And there are certainly no “shinologists.” Feet have entire professions devoted to them, but not shins! For most professionals, shin pain is just one of a list of hundreds of common pain problems they deal with, and they are more or less completely unaware of the finer points of the subject, particularly recent scientific research. A typical orthopedics text devotes only a paragraph to shin pain; most web pages are brief and crappy, barely scratching the surface of the topic.9 And so, in many cases the only thing professionals know is quarter-century old conventional wisdom. Such large gaps in professional knowledge make it tough for patients to find competent help for more severe and stubborn cases of shin pain. There are several issues that doctors and therapists are particularly uninformed about, and often fail to consider:
- Unfortunately, many pros do not appreciate how dangerous acute compartment syndromes are, and often fail to recognize them and give appropriate warnings to patients.
- Tissue fatigue is a critical concept, and yet the majority of professionals have rarely or never thought of it in this way, especially thinking only in terms of relatively simplistic biomechanical stresses rather than the more subtle and complicated biological vulnerabilities and the weirdness of chronic pain that are more important.10
- Progressive rehab is a sound principle — the heart of all injury recovery — but it is often rushed, and the importance of initial resting seriously underestimated and poorly handled. Often the only problem with a rehab plan is that it was started too aggressively.
- Muscle pain is probably a significant factor in many cases of shin pain, but this is almost always missed or underestimated — health care has a huge blind spot for muscle, and often just ignores the role of muscle in injuries.11
Danger! Please do not try to run through shin splints! Acute compartment syndrome can be extremely dangerous!
Until you feel confident that you know which type of shin pain you have, you should assume the worst and avoid aggravating the condition. Why?
Compartment syndrome — high-pressure swelling, fluid that’s trapped in a limb — is one kind of tissue failure that mostly afflicts lower legs.12 It’s extremely dangerous when acute. Compartment syndrome involves a vicious cycle which is not necessarily self-limiting (as many other injuries are). Once it starts, it may spiral out of control and literally kill the affected muscles, causing permanent deformity and disability at the very least, and even risk lethal infection. Triple yikes! This is absolutely serious, and unlike most other athletic injuries.
Although the pain is usually severe enough to stop people from running, some athletes may be foolhardy enough to try to keep going — if this is you, please stop! Rapidly worsening shin or calf pain absolutely must be treated like a medical emergency, and not just a cramp on your style. You are in danger of destroying your athletic career!
Ken Hildebrand of Alberta, Canada, knows just how serious compartment syndrome can be. On January 8, 2008, Mr. Hildebrand was pinned under an all-terrain vehicle in the Rocky Mountains. He survived for 96 hours by eating rotting animal carcasses, drinking melted snow, fending off coyotes with a whistle, and thinking of his grandchildren.
But compartment syndrome was his worst problem!
My leg swelled up about four times the size of normal. And in order for blood to get through they have to slice the muscle so that it can drain and then they slowly let it repair itself. The leg is good now, I’m going to be able to keep the leg, but the foot is still iffy.
Ken Hildebrand on “As It Happens,” CBC Radio One, January 23, 2008
In Mr. Hildreband’s case, compartment syndrome was the consequence of trauma, and he suffered a particularly severe case of compartment syndrome, with extreme swelling. However, equally dangerous consequences are possible in runners who try to “run through the pain.” So don’t!
Reassuring concluding note: chronic compartment syndromes, by contrast, are relatively safe — frustrating and uncomfortable, but much less dangerous. Shin or calf pain that has been around for a while and isn’t rapidly worsening is pretty unlikely to be a serious problem.

Acute compartment syndrome is no joke
To treat acute compartment syndrome, the muscle compartment is sliced open to relieve the pressure. Tissue bulges like a hot sausage spilling out of its casing. The result is a massive surgical wound that takes months to heal and leaves substantial scarring.
Part 2
Etiology
What causes shin splints?
Here are three main ways of thinking about the “cause” of shin pain (or any injury):
- the stress and risk factors that lead to injury — “I ran on hard pavement too much, and excessively pronated the whole time”
- what specific tissue fails and in what way — “my shin bone got a stress fracture in it”
- systemic vulnerability and chronic pain — “I was still hurting long after the bone should have healed”
In typical sports medicine and physical therapy, the first of these perspectives gets about 70% of the attention when it only deserves something more like 30%, and virtually all of the attention it does get is directed at alleged biomechanical problems rather than the part that actually matters: loading, loading, loading! The overall volume of loading is more important than minor variations in how you are loading. Anything will wear out if you use it hard enough and long enough, and reasons for wearing out slightly faster are not the “cause” of the problem.
The second is often neglected because no one can actually be sure of what tissue is specifically the problem. Or, even when a blatant tissue issue can be identified, it’s often not the real issue, something that commonly occurs even in healthy people. This is a vital principle for troubleshooting all kinds of stubborn injuries — plenty more about this as we go.
So what is the “real issue” in broad strokes? The third perspective is the elephant in the room, which gets about 5% of the attention but deserves more like 80%. This is where you find the difference between patients who recover just fine (or never get injured in the first place), and the patients who do poorly and end up still desperately trying to get back to running two years later.
| “splints” | just an old-timey word for “pain” |
|---|---|
| tibia | big shin bone (the sharp leading edge of the shin is the tibia) |
| fibula | little shin bone |
| tibialis anterior | the main shin muscle |
| syndrome | a pattern of unexplained symptoms |
| compartment syndrome | swelling in the “sausage wrapping” around a muscle or group of muscles |
| chronic shin splints | >3 months, increasingly “illogical”13 |
The main risk factor for shin splints: overload!
Fun fact: runners with “perfectionist tendencies” are 17 times more likely to get injured, which seems rather odd and suspiciously psychological. Stress fractures aren’t psychosomatic … right? It’s not that kind of stress! “Still, for anyone who’s been around runners,” says sports science journalist Alex Hutchinson, “it’s not hard to believe that there are some personality traits that are associated with injury risk.”14 Indeed.
Perfectionists probably push themselves harder. Perfectionism is probably a good proxy for stereotypical athletic ambition: intense, driven, a bit reckless, likely to ignore warning signs. In other words, show me a perfectionist, and I’ll show you someone who is likelier to get hurt.
There’s really only one major risk factor for any overuse injury that is known with any confidence:
- excessive loading
We know that there’s such a thing as doing too much, too soon. Especially if the load is greater and/or the body is a bit more fragile: about 10% of novice runners will get hurt, mostly the heavier, the older, and the ones who have been hurt before.15 Experience is a factor too: the more of a beginner you are, the more likely you are to hurt yourself.16 These are the obvious, general risk factors for running injuries — which includes shins splints, and that has been confirmed by studies of shins splints specifically (more on that shortly).
Once you leave the obvious behind, it gets messy and uncertain fast. We know that overuse injuries are definitely not just about loading.
Most importantly, not all loading is simple or even physical: biological and psychological stresses also contribute.17 Shin splints is routinely defined as an overload, overuse, or exercise-induced problem, and this is correct — but it’s also not the whole story. Not every case involves tissue overloading, but most probably do. And not every case only involves tissue overload.
There are deep mysteries about why shin splints happen to some people and not others, and exactly which tissues it is actually affecting and how. Tissue fatigue has clinical implications that are often underestimated (and which make up a good part of this tutorial). Despite their willingness to define shin splints as mainly a tissue fatigue problem, few professionals are willing to actually study it or treat it that way. If overload is the primary problem, then load management — carefully titrated resting and return to activity — is probably the highest priority in recovery. But rest tends to be marginalized and underestimated as a treatment option, in favour of a wide array of “fancier” theories and therapies, mostly aimed at “correcting” alleged non-obvious sources of biomechanical stress …
Introducing several other possible causes of shin splints
There is considerable scientific controversy and confusion about the other risk factors and stresses that might cause or contribute to shin splints.
Do your biomechanical quirks put you at risk? Can clues like running technique and flat feet predict who gets injured? And if a risk factor is known, does that mean it “causes” the injury? Everyone sure acts like it: fixing those risk factors is a major focus of rehab. Almost everyone who has ever sought professional help for a stubborn pain in their body has been told that they are deformed and fragile, that the root cause is some kind of “mechanical” glitch — not in such insensitive words, exactly, but that’s the take-home message. Physical therapists, massage therapists, and chiropractors in particular tend to blame pain on our “structural” problems. In the case of shin splits, the usual structural suspects are:
- excessive pronation
- varus hindfoot
- a high Q-angle, AKA genu valgum, AKA knock-kneed18
- excessive femoral anteversion
- external tibial torsion
- high vertical loading rate
Those are some the things that therapists most like to blame.19 There is certainly such a thing as a structural or biomechanical problem, but there are also some serious concerns about trying to blame injuries on factors like these. Concerns like this…
Only one of those is actually on the list of risk factors for shin splints that has been flagged by research. Just one. We don’t have a lot of amazing data on risk factors for shin splints,2021 but what we have barely overlaps with that list of usual suspects.
And even confirmed risk factors don’t necessarily confirm a cause. (Much more about to come.)
And the most significant risk factors are probably the general ones, not the specific ones. The data does unanimously confirm that heavier and previously injured runners are more likely to get shin splints — along with most other running injuries. And there’s one other vexing general risk factor, maybe:
- Being a woman? As with most athletic injuries, there is a strong theme in the scientific literature that women might get hurt more often than men, usually because they are presumed to be more structurally and/or physiologically vulnerable in some way. This sexism is more plausible in some cases than others, but mostly it’s just an obnoxious vestige of the more overt chauvinism of the past, when everyone just assumed that women were too “delicate” for manly activities. More on this later on in the tutorial.
So, what specific biomechanical risk factors for shin splints have been pseudo-identified by the research? And what are the problems with even those?
END OF FREE INTRODUCTION
Purchase full access to this tutorial for USD$1995. Continue reading this page immediately after purchase. See a complete table of contents below. Most content on PainScience.com is free.?
Almost everything on this website is free: about 80% of the site by wordcount, or 95% of the bigger pages. This page is only one of 10 that have a price tag. There are also hundreds of free articles. Book sales — over 75,500 since 2007?This is a tough number for anyone to audit, because my customer database is completely private and highly secure. But if a regulatory agency ever said “show us your math,” I certainly could! This count is automatically updated once every day or two, and rounded down to the nearest 100. Due to some oddities in technology over the years, it’s probably a bit of an underestimate. — keep the lights on and allow me to publish everything else (without ads).
Q. Ack, what’s with that surprise price tag?!
A. I know it can make a poor impression, but I have to make a living and this is the best way I’ve found to keep the lights on here.
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
| company | PainScience.com |
|---|---|
| owner | Paul Ingraham |
| contact | 778-968-0930 |
| refunds | 100%, no time limit +Customers are welcome to ask for a refund months after purchase — I understand that it can take time to decide if information like this was worth the price for you. |
| more info | policies page ❐ |
| payments |
- What do you get, exactly? An online tutorial, book-length (55 chapters). Free updates forever, read on any device, and lend it out. E-book only! MORE
- Secure payment takes about 2 minutes. No password or login: when payment is confirmed, you are instantly granted full, permanent access to this page.MORE
- Collect them all. Get an “e-boxed” set of all 10 PainScience.com tutorials, ideal for pros … or patients with a lot of problems.MORE
Q. What am I buying? Is there an actual paper book?
A. Payment unlocks access to 48 more chapters of what is basically a huge webpage. There is no paper book — I only sell book-length online tutorials. This format is great for instant delivery, and many other benefits “traditional” e-books can’t offer, especially hassle-free lending and updates. You get free lifetime access to the always-current “live” web version (and offline reading is easy too).

Read on any device. Lend it out. New editions free forever.
Q. I just don’t like reading on the computer! Is there any way around that?
A. The design and technology of the book is ideal for reading on tablets and smart phones. You can also print the book on a home printer.
Q. Can I lend the tutorial out?
A. Yes! Feel free to lend your tutorial: I do not impose silly lending limits like with most other ebooks. No complicated policies or rules, just the honour system! You buy it, you can share it. You can also give it as a gift.
Q. Is it safe to use my credit card on your website?
A. Literally safer than a bank machine. Payments are powered by Stripe, which has an A+ Better Business Bureau rating. Card info never touches my servers. It’s easy to verify my identity and the legitimacy of my business: just Google me [new tab/window].
Q. I can really get a refund at any time?
A. Yes. All PainScience.com ebooks have a lifetime money-back guarantee.
Q. Why do you ask for contact information?
A. To prevent fraud and help with order lookups. You aren’t “subscribing” to anything: I never send email to customers except to confirm purchases.
Q. Can I buy this anywhere else? Amazon?
A. Not yet. Maybe someday.
See the “fine print page” for more about security, privacy, and refunds. No legalese, just plain English.
Save a bundle on a bundle
The e-boxed set is a bundle of all 10 book-length tutorials for sale on PainScience.com: 10 books about 10 different common injuries and pain problems. All ten topics are (all links open free intros in a new tab/window): muscle strain, muscle pain, back and neck pain, two kinds of runner’s knee (IT band syndrome and patellofemoral pain), shin splints, plantar fasciitis, and frozen shoulder. (Headache coming soon, fall of 2019.)
Most patients only need one book, because most patients have only one problem. But the set is ideal for professionals, and some keen patients do want all of them, for the education, and for lending to friends and family. And, of course, you do get a substantial discount for the bulk purchase. But no rush—complete the set later, minus the price of any books already bought. More information and purchase options.
How can you trust this information?
I apply a MythBusters approach to health care (without explosives): I have fun questioning everything. I don’t claim to have The Answer for shin pain. When I don’t know, I admit it. I read scientific journals, I explain the science behind key points (there are more than 150 footnotes here, drawn from a huge bibliography), and I always link to my sources.
For instance, there’s good evidence that educational tutorials are actually effective medicine for pain.?Dear BF, Gandy M, Karin E, et al. The Pain Course: A Randomised Controlled Trial Examining an Internet-Delivered Pain Management Program when Provided with Different Levels of Clinician Support. Pain. 2015 May. PubMed 26039902 ❐ Researchers tested a series of web-based pain management tutorials on a group of adults with chronic pain. They all experienced reductions in disability, anxiety, and average pain levels at the end of the eight week experiment as well as three months down the line. The authors concluded: “While face-to-face pain management programs are important, many adults with chronic pain can benefit from programs delivered via the Internet, and many of them do not need a lot of contact with a clinician in order to benefit.” Good information is good medicine!
So all the science and all the options for shin splints treatment are here. If you’ve been struggling with pulled muscle injury, I think this tutorial will feel like a “good find” to you!
As with all the tutorials on PainScience.com, I’ve worked hard to provide you with the best information available anywhere — not just better researched and referenced, but also regularly updated, and presented in a clear, friendly style that’s just like coming to my office and having a nice long conversation about it, where all your questions get answered. For a fraction of the cost.
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
Part 2.3
Appendices
Reader feedback … good and bad
Testimonials on health care websites reek of quackery, so publishing them has always made me a bit queasy. But my testimonials are mostly about the quality of the information I’m selling, and I hope that makes all the difference. So here are some highlights from the kind words I’ve received over the years … plus some of the common criticisms I receive, at the end. These are all genuine testimonials, mostly received by email. In many cases I withold or change names and identifying details.
Thank you so much for taking the time to put this book together, and in a way that makes it feel like you wrote it just for me! You have a great writing style.
Chyna Pittman
Thanks for the great tutorial! Much more helpful than any of the professionals I’ve seen for my chronic running-induced shin pain — all the doctors, sports massage therapists, chiropractors, and physical therapists!
Cassandra Clarke
I was so sick of reading crappy little articles with the same old advice. Seems like there’s about ten thousand that all say the same useless things. Thanks for the deep dive!
Sandra Frank, Ottawa, Ontario
A year of shin pain and hardly anything but painkillers and ultrasound from doctors and physios. I was giving up! I thought I’d never have a nice long walk again. Actually I was even more discouraged after reading this book, because so many treatments are apparently bullshit. But then I started experimenting with some of the massage ideas, and bam! The nightmare ended! Unbelievable!
Alison Fromer, “just a serious walker”
My shin pain has been very stubborn. I know as well as anyone there’s no easy way to deal with this, and this book confirmed that! But I really appreciate the education. Even after a couple years of dealing with shin splints, I still had a bunch of nagging questions that this book really helped to clear up. That alone was worth the price, but there were also a couple rehab ideas I’d never come across. Totally worth it.
Andy Flaco, New York runner
One more noteworthy endorsement, with regards to this whole website and all of my books, submitted by a London physician specializing in chronic pain, medical education, and patient-advocacy (that’s a link to his excellent blog):
I’m writing to congratulate and thank you for your impressive ongoing review of musculoskeletal research. I teach a course, Medicine in Society, at St. Leonards Hospital in Hoxton. I originally stumbled across your website whilst looking for information about pain for my medical students, and have recommended your tutorials to them. Your work deserves special mention for its transparency, evidence base, clear presentation, educational content, regular documented updates, and lack of any commercial promotional material.
Dr. Jonathon Tomlinson, MBBS, DRCOG, MRCGP, MA, The Lawson Practice, London
What about criticism and complaints?
Oh, I get those too! I do not host public comments on PainScience.com for many reasons, but emailed constructive criticism, factual corrections, requests, and suggestions are all very welcome. I have made many important changes to this tutorial inspired directly by critical, informed reader feedback.
But you can’t make everyone happy! Some people demand their money back (and get it). I have about a 1% refund rate (far better than average in retail/e-commerce). The complaints of my most dissatisfied customers have strong themes:
- Too negative in general. Some people just can’t stomach all the debunking. Such customers often think that I dismiss “everything” … which I disagree with.
- Too negative specifically. Some are offended by my criticisms of a treatment option that they personally use and like. Or sell!
- Too advanced. Although I work hard to “dumb” the material down, quite a few people still just find it too dense and dorky.
- Too simple. Some people think they already know everything about the topic. Maybe they do, and maybe they don’t. I always wish I could give these readers a pop quiz. 😉 In my experience, all truly knowledegable people get that way by embracing every new persective and source of information.
Acknowledgements
Thanks to every reader, client, and book customer for your curiosity, your faith, and your feedback and suggestions, and your stories most of all — without you, all of this would be impossible and pointless.
Writers go on and on about how grateful they are for the support they had while writing one measly book, but this website is actually a much bigger project than a book. PainScience.com was originally created in my so-called “spare time” with a lot of assistance from family and friends (see the origin story). Thanks to my wife for countless indulgences large and small; to my parents for (possibly blind) faith in me, and much copyediting; and to friends and technical mentors Mike, Dirk, Aaron, and Erin for endless useful chats, repeatedly saving my ass, plus actually building many of the nifty features of this website.
Special thanks to some professionals and experts who have been particularly inspiring and/or directly supportive: Dr. Rob Tarzwell, Dr. Steven Novella, Dr. David Gorski, Sam Homola, DC, Dr. Mark Crislip, Scott Gavura, Dr. Harriet Hall, Dr. Stephen Barrett, Dr. Greg Lehman, Dr. Jason Silvernail, Todd Hargrove, Nick Ng, Alice Sanvito, Dr. Chris Moyer, Lars Avemarie, PT, Dr. Brian James, Bodhi Haraldsson, Diane Jacobs, Adam Meakins, Sol Orwell, Laura Allen, James Fell, Dr. Ravensara Travillian, Dr. Neil O’Connell, Dr. Tony Ingram, Dr. Jim Eubanks, Kira Stoops, Dr. Bronnie Thompson, Dr. James Coyne, Alex Hutchinson, Dr. David Colquhoun, Bas Asselbergs … and almost certainly a dozen more I am embarrassed to have neglected.
I work “alone,” but not really, thanks to all these people.
I have some relationship with everyone named above, but there are also many experts who have influenced me that I am not privileged to know personally. Some of the most notable are: Drs. Lorimer Moseley, David Butler, Gordon Waddell, Robert Sapolsky, Brad Schoenfeld, Edzard Ernst, Jan Dommerholt, Simon Singh, Ben Goldacre, Atul Gawande, and Nikolai Boguduk.
What’s new in this tutorial?
Regular updates are a key feature of PainScience.com tutorials. As new science and information becomes available, I upgrade them, and the most recent version is always automatically available to customers. Unlike regular books, and even e-books (which can be obsolete by the time they are published, and can go years between editions) this document is updated at least once every three months and often much more. I also log updates, making it easy for readers to see what’s changed. This tutorial has gotten 65 major and minor updates since I started logging carefully in late 2009 (plus countless minor tweaks and touch-ups).
Aug 26, 2025 — Science update: A substantive update integrating new evidence from Farquharson et al., as well as some other trials and key points. It’s “just a science update,” but a good one, a good improvement to the chapter. [Updated section: Do women really get more shin pain?]
2022 — Minor addition: Added tibiofibular pain to the list of possible causes of shin pain. [Updated section: Other causes of shin pain.]
2022 — More information: Technically this is a new section, but I’ve created it just by transplanting and elaborating on the brief dismissal of orthotics that was in the “hall of shame” section for years. It is more substantive, but it says essentially the same thing. [Updated section: Correcting pronation with orthotics or motion control shoes.]
2022 — Minor upgrade: Just a couple elaborations and refinements, based on new risk factor evidence. [Updated section: The great pronation fizzle.]
2022 — New chapter: This is a chapter that is entirely about a single citation, one interesting experiment: Napier et al. [Updated section: Does peak braking force determine when you break?]
2022 — Major upgrade: This is a huge upgrade to this section, which is now both more interesting and consequential than I expected when I started it. I’ve added significantly more detailed and referenced information about risk factors. [Updated section: The main risk factor for shin splints: overload!]
2021 — Improvements: A bit more and clearer information on the role of radiculopathy/sciatica in differential diagnosis of shin pain. [Updated section: Other causes of shin pain.]
2020 — New chapter: No notes. Just a new chapter. [Updated section: Steroid injections: a complicated mix of certain risks and uncertain rewards.]
2020 — Minor new sub-topic: [Updated section: Stripping: a popular massage techique for the shins.]
2020 — Science update: Cited Milgrom et al. on seemingly high-impact exercises actually being not so high impact, and Barton et al. on the value of running technique [Updated section: Hitting the road: shoes, surfaces, impact, and the spring in your step.]
2020 — Major improvements: Substantial editing and elaboration. The chapter is now bigger and better. [Updated section: Introducing several other possible causes of shin splints.]
2020 — Science update: Added some more recent citations, some more detail, and a photo. [Updated section: The great pronation fizzle.]
2020 — Upgraded: Added more detail, especially about trigger points and minor muscle injury, with a couple new citations. [Updated section: Strengthening can’t “fix” shin pain, but still has a vital role in rehab.]
2020 — Upgraded: More and better information, and also probably mostly complete now. There might be some other ridiculous treatments for shin splints, but probably none that are popular enough to bother writing a paragraph about. [Updated section: Hall of treatment shame: the most bogus shin splints treatments.]
2020 — Expanded: Added sub-topic: “More ways to go wrong getting strong (especially with shin pain)” [Updated section: Strengthening can’t “fix” shin pain, but still has a vital role in rehab.]
2020 — Science update: Expanded on the sub-topic of hip strength, based on three new studies. [Updated section: Strengthening can’t “fix” shin pain, but still has a vital role in rehab.]
2019 — Major upgrade: Completely rewritten and greatly expanded. Previously this chapter was just a brief dismissal of the value of corrective strength training for shin splints — which wasn’t wrong in itself, but it was inadequate, and in particular it neglected the genuinely valuable role that strength training can play in rehab, even if it can’t “fix” anything. [Updated section: Strengthening can’t “fix” shin pain, but still has a vital role in rehab.]
2019 — Expanded: Added radiculopathy, tendinopathy, and more detail about specific peripheral neuropathies. [Updated section: Other causes of shin pain.]
2019 — Big new chapter: No notes. Just a new chapter. [Updated section: The role of fascia in compartment syndrome.]
2019 — Science update: Quirky sidebar about the relationship between running softly and quietly. [Updated section: Hitting the road: shoes, surfaces, impact, and the spring in your step.]
Archived updates — All updates, including 45 older updates, are listed on another page. ❐
2007 — Publication.
Notes
- From a fascinating talk about the athletic toughness of human beings, Brains Plus Brawn, by Dr. Daniel Lieberman, evolutionary biologist of “Born to Run” fame.
- Yates B, White S. The incidence and risk factors in the development of medial tibial stress syndrome among naval recruits. Am J Sports Med. 2004 Apr-May;32(3):772–780. PainSci Bibliography 55469 ❐
Yates and White reported shin pain prevalence of 35% in naval recruits at the end of basic training — a high risk population, to be sure, and the highest figure ever reported. But other studies have also reported quite high numbers. Shin pain clearly ranges anywhere from “pretty darned common” to “rather shockingly frequent.”
More prevalence data later.
- As are all knee injuries from the knee down. Ferber et al. estimated in 2009 that about 80% of all running injuries occur in the knee and lower leg. 50% of those are in the knee, while “injuries to the foot, ankle, and lower leg—such as plantar fasciitis, Achilles tendinitis, and medial tibial stress syndrome (also known as shin splints)—account for almost 40% of the remaining injuries.”
- Farquharson E, Roberts AJ, Warland AI, Parnis N, O'Connell NE. Prevalence of medial tibial stress syndrome in the British Armed Forces: a population-based study. BMJ Mil Health. 2025 Mar:e002788. PubMed 39578017 ❐
This prevalence study of medial tibial stress syndrome (a major sub-type of shin splints) in the British Armed forces found a prevalence of 1.6% in 2018, down from 2.2% back in 2010 — much lower than a notorious older study that reported 35% (Yates & White), but their definition was looser, they relied only on symptom report, and those reports were professionally safer (having been assured that “reporting symptoms would not impact their career”). So 35% is probably a big overestimate … while 1-2% is likely a big underestimate! I’m going with “at least 3%,” but that’s being careful; honestly it’s probably three times that.
These papers come again later to help answer the question, "Do women get more shin splints?"
- Back splints, anyone? Shoulder splints? Head splints? I’ve been wondering about this little bit of language oddity for years now, but I still can’t dig up anything about the origins of “splints” and why it’s apparently exclusive to shin pain.
- Batt ME. Shin Splints — A Review of Terminology. Clin J Sport Med. 1995;5(1):53–57. “Currently the term [shin splints] is used widely and variably, with little consensus of definition. Broadly, it denotes the occurrence of exertional lower leg pain … ”
- Edwards PH, Wright ML, Hartman JF. A practical approach for the differential diagnosis of chronic leg pain in the athlete. Am J Sports Med. 2005 Aug;33(8):1241–1249. PubMed 16061959 ❐ The authors of this paper describe several common lower leg pain problems (several of which are covered by this tutorial, and including at least three types of shin splints) and then comment that “symptoms associated with these conditions often overlap, making a definitive diagnosis difficult.”
- Grant HM, Tjoumakaris FP, Maltenfort MG, Freedman KB. Levels of Evidence in the Clinical Sports Medicine Literature: Are We Getting Better Over Time? Am J Sports Med. 2014 Apr;42(7):1738–1742. PubMed 24758781 ❐
Things may be getting better: “The emphasis on increasing levels of evidence to guide treatment decisions for sports medicine patients may be taking effect.” Fantastic news, if true! On the other hand, maybe I should be careful what I wish for, since my entire career is based on making some sense out of the hopeless mess that is sports and musculoskeletal medicine …
In 2012, the The Journal of Foot & Ankle Surgery ranked 136 websites about common foot and ankle diagnoses. Expert reviewers gave each a quality score on a scale of 100. The average score? Just below fifty. Fifty! See Smith et al.
Or see Starman et al. for a review of other kinds of health care information (with nearly identical grades).
P.S. These references are aging now… but nothing’s really changed!
- Generally speaking, medical philosophy about overuse injuries is significantly bogged down by a simplistic over-emphasis on “mechanical” risk factors such as various kinds of crookedness. Shin pain is certainly blamed on a variety of common anatomical scapegoats (like excessive foot pronation), none of which have ever really been established scientifically. Much more about all this below!
- The importance of muscle dysfunction is a recurring theme throughout this website. It’s not relevant to every injury, but it is involved to some degree in most kinds of injuries, either as a root cause or a significant complicating factor. I’ll explore this in much greater detail below.
- Compartment syndromes outside of the calf are rare, because it’s all about plumbing: it’s harder to pump tissue fluid out of the lowest (most distal) large tissue compartments in the body. Once in a while there’s a compartment syndrome in the forearm, because it has the same plumbing problem to a lesser degree. Compartment syndromes elsewhere in the body probably only occur in unusual circumstances involving very specific or serious injury.
- Acute pain usually “makes sense,” in that the cause is relatively obvious: stress and strain on the tissue. Chronic pain is a bit of a vicious cycle that, to some degree, persists regardless of physical stresses. Chronic pain often seems to have a bit of a life of its own.
- OutsideOnline.com — SweatScience [Internet]. Hutchinson A. Why Perfectionists Get More Shin Splints; 2018 October 19 [cited 25 Aug 26]. PainSci Bibliography 53088 ❐
Alex speculates:
Do perfectionists simply train harder, and get injured more as a result? If so, it’s possible that their lofty goals produce faster race times despite the heightened injury risk, in which case it’s not clear this is a problem. But it’s also possible that perfectionists are more susceptible to bad training decisions—refusing to take a day off in the early stages of an injury, or ramping up training more quickly than their body can handle.
- Kluitenberg B, van Middelkoop M, Smits DW, et al. The NLstart2run study: Incidence and risk factors of running-related injuries in novice runners. Scand J Med Sci Sports. 2015 Oct;25(5):e515–23. PubMed 25438823 ❐
A giant 2015 study of almost 1700 novice runners in a “Start to Run” program found that a lot of them got hurt (almost 11%), and of those that did get hurt were more likely to be older, heavier, have a history of previous musculoskeletal problems, and less prior running experience.
- That could just be that the vulnerable have already been weeded out. But the other possibility is that it’s related to impact: beginners are probably more likely to be less graceful, hitting the pavement harder or just more awkwardly. They may also be less aware of the warning signs.
- Soligard T, Schwellnus M, Alonso JM, et al. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br J Sports Med. 2016 Sep;50(17):1030–41. PubMed 27535989 ❐ “Load” can also refer to life stress and “internal” loads, which are legion. Psychology, for instance, probably does matter, and not just perfectionism leading to pushing too hard: anything from daily hassles to major emotional challenges, as well as stresses related to sport/competition itself. These squishy, messy things almost certainly are actually risk factors for injury and — crucially — for how stubborn injuries are. These are the factors that could make the difference between someone who gets a touch of the shin splints versus someone who simply cannot shake the condition.
What is “valgum”? What is “varus”? Valgum and varus mean “twisted away/towards” the midline. So a forefoot varus is a forefoot that is twisted towards the midline, while a genu valgum is a lower leg that is bent away from the midline (knock knees).
- These are the ones I learned/heard about in my training and early in my career, and the ones that still crop up constantly in conversation with injured runners: “My physio said I’m pronating too much.” While a skilled and competent professional might know better, I’m afraid these ideas are very common and highly problematic. A lot of this tutorial is devoted to undermining the influence of these rather knee-jerk pseudo-diagnoses.
- Hamstra-Wright KL, Bliven KCH, Bay C. Risk factors for medial tibial stress syndrome in physically active individuals such as runners and military personnel: a systematic review and meta-analysis. Br J Sports Med. 2015 Mar;49(6):362–9. PubMed 25185588 ❐
- Reinking MF, Austin TM, Richter RR, Krieger MM. Medial Tibial Stress Syndrome in Active Individuals: A Systematic Review and Meta-analysis of Risk Factors. Sports Health. 2017;9(3):252–261. PubMed 27729482 ❐ PainSci Bibliography 52540 ❐
There are 136 more footnotes in the full version of the book. I really like footnotes, and I try to have fun with them.
Jump back to:
The introduction
Paywall & purchase info
Table of contents
Top of the footnotes
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help