Does Spinal Manipulation Work?
Spinal manipulation, adjustment, and popping of the spinal joints and the subluxation theory of disease, back pain and neck pain
![[Illustration of hands twisting a spinal column]](/assets/images/spinal-adjustment--port-280x380-10k.jpg)
Spinal manipulation: underwhelming effects on back pain since 1895.
Can your spine be “out”? Can it be “adjusted”? Adjusting the spine (spinal manipulative therapy, or SMT) is complex and controversial, largely based on the chiropractic concept of a joint “subluxation.” SMT for the back probably has modest benefits and tolerable risks, while SMT for necks involves less benefit … and the rare but real risks of paralysis and death! Nearly all medical science experts and many chiropractors reject the century-old chiropractic belief that SMT can prevent or cure diseases.
This article covers these topics thoroughly, and I particularly discuss the pros and cons of SMT as it relates to the treatment of neck pain, back pain, headaches, and muscle pain.
Meh! Overview of the most important/interesting science of spinal manipulative therapy
Although I will discuss a lot of other research below, these reviews more or less answer the title question: SMT works poorly, if it all, for most people, most of the time. There are probably exceptions for specific types of patients (that are extremely hard to identify), but the average is utterly underwhelming:
- Cochrane says: nope! The Cochrane Collaboration produces best-of-breed reviews and meta-analysis, as far as that goes, and this one concluded that “SMT is no more effective in participants with acute low-back pain” than shams and placebos.1
- No better than Advil… and side effects too! Paige et al. reported trivial benefits only, just one point up on a 10-scale at best,2 Although weirdly touted by SMT proponents as a positive study, it’s really not: they are just trying to make lemonade out of scientific lemons. It clearly damns SMT with faint praise.3 which is about the same as you’re going to get from Advil. And it gets worse! They also identified lots of treatment backfires — minor ones, but who wants to spend the time and money on spinal adjustment to get more pain?4
- Just as ineffective as everything else. Clearly contrary the hopes of the authors, a 2019 comparison of SMT to other therapies only established that SMT … is no worse than other ineffective options.5 They tried to spin this as good news, but it was a conclusion that only the researchers’ mothers might believe.
- Pick a joint, any joint? Building on this broad scientific consensus, more evidence has undermined SMT in new ways, like the 2021 review that showed that SMT outcomes are unaffected by skilled joint selection.6 If it doesn’t matter what joint you “adjust,” then it doesn’t much matter if you adjust joints at all. This data is quite damning to SMT and the practitioners who believe they are. Obviously. But the point is that it’s icing-on-the-cake data, reinforcing the bad news in an interesting new way.
- Pick a technique, any technique? If SMT is effective, then it should matter how you do it — but a 2025 review showed that there it doesn't matter how you manipulate the spine: “None of the SMT procedures were superior to others in terms of pain relief.” This is consistent with the active ingredient being caretaking interaction, not an effect on the spine. While arguably based on inadequate evidence, the result is still damning for SMT.7
If it were possible to report better news about SMT, it would be in these reviews — and I would be happy about it. But it’s not, and the topic can probably be closed by reasonable people.
It won’t be closed, of course. Historically, spinal manipulative therapy for acute low back pain has been touted as the best example of evidence-based care routinely offered by the chiropractic profession, and they are not going to stop just because the actual evidence contradicts that profitable belief. Even many fierce critics of chiropractic continue to echo it — or at least leave it alone while focusing on more glaring issues with that profession. But others have pointed out that even this “best” use of SMT has such disappointingly small benefits that it can hardly be considered effective.
My chiropractor says this is because the top of my neck attaches to my head. Is that a common problem?
from the “chiropractors say the darndest things” file, as reported by Dr. Grumpy (Only Outside Sleepy Hollow)
Spinal manipulative therapy is a very messy topic
The idea of “adjusting” the spine refers to many similar-but-different manual (hands-on) therapies: the joints of the spine may be wiggled, popped, stretched, tapped, and more. The umbrella term for these treatments is “spinal manipulative therapy” or SMT. Expert opinions on SMT range widely, with some experts — prominent doctors and medical scientists — expressing the strongest possible concern and skepticism. SMT’s origins in chiropractic are dubious, its benefits are clearly not major, and there are serious risks (including paralysis and even death with neck manipulation).
… there is a “paucity of data related to beneficial effects of chiropractic manipulation of the cervical spine” and a “real potential for catastrophic adverse events.” That’s what the science says.
Controversial it may be, but the science is clear enough to have caused a major American health insurer to stop paying for cervical spine SMT in 2010.8 There has been little high quality scientific research to determine whether or not SMT really “works,” but what little does exist is discouraging indeed. Major reviews of that literature published in recent years came to “underwhelming” and half-baked conclusions. Thus, SMT fails the “impress me” test — it might work, but it can’t possibly work particularly well. An effective therapy should have no problem passing fair tests with flying colours.
And yet spinal joint popping/cracking is a sensation that people crave. I am one of them! And most clinicians — including myself, and including serious skeptics like Dr. Homola — believe that some forms of SMT can be helpful to some of their patients, some of the time. There seems to be almost no doubt that there is something of therapeutic interest going on in SMT. In rare cases involving joint adhesions, mechanical “locking” and loss of mobility, appropriate manipulation has clear value — which is primarily why physical therapists perform spinal manipulation.
It’s a complex picture, and it’s made even more complex by the messy idea of “subluxation.” This is a chiropractic concept of some kind of spinal joint dysfunction, with many shades of meaning — too many! It’s definition has been widened again and again, to the point of absurdity, expanding beyond the spine to include any harmful “imbalance or distortion” anywhere in the body.9 And so many chiropractors still attribute great importance to subluxations, and “use spinal manipulation to treat visceral disease”10 … even if the patient has no symptoms!11 The chiropractic concept of subluxation has been both popular and controversial for many decades now, but it has never achieved medical respectability.1213 It’s problematic that SMT is usually based on such a slippery concept.
Perhaps it has too much baggage to be a useful term.
Even if you put aside all concerns about the quality of the theory, there is still not a shred of scientific evidence that any kind of spinal joint dysfunction — no matter how you define it — has any importance to your general health. In more than a century, nothing like that has ever been shown to be true.14 So do chiropractic subluxations even exist? And, even if they did, would they actually cause any problem, serious or otherwise? And how serious are chiropractors about all this anyway? I’ll address these questions over the next few sections.
Reality check: is there such a thing as a chiropractic “subluxation”?
Joint mechanics and neurology are just insanely complex, and when that complex system fails in any way, we could (and should) call it a “joint dysfunction.” Nice, safe, generic terminology. We can cram almost any kind of theory into that label — almost anything that might go wrong with spinal joints — without going too far out on a limb. There is little doubt that spinal pain often involves some kind of “joint dysfunction.”
Or maybe there is doubt: maybe the joint just feels wonky. Pain distorts body image — our mental image of our own anatomy. An odd little 2008 paper demonstrated that people with back pain think their vertebrae are deviated to the painful side.15 Simple as it is, this phenomenon may be potent and persuasive. It could be a major reason for the belief in out-of-place vertebrae.
But if it’s not just warped sensation, an anatomical illusion — if there actually is some kind of dysfunction — what kind of dysfunction? Chiropractors believe that they know, and they’ve built a profession around it: “subluxation.” A misalignment. A “spine out of line.”16
Many doctors and scientists disagree!
Chiropractors routinely push subluxation as both the main cause of back and neck pain and of disease and poor health in general.1718 The chiropractic idea of subluxation has been defined in many different ways over the years, but most definitions imply some kind of “misalignment” of the spinal joints that needs to be “adjusted” because it’s causing a disproportionate amount of trouble, both pain and poor health. This ominous definition of subluxation is both the most popular and the least defensible. Although there are other definitions — for instance, definitions that might be less controversial — they probably should not be used, because they are too easily confused with the main and original chiropractic definition.
In standard medical terminology, a subluxation simply refers to a partial traumatic dislocation of a joint. Ligaments around the joint may be painfully sprained, and cause severe pain closely coupled to movement, slowly fading over many weeks, like any other sprain. Slightly subluxed spinal joints often return to a more or less normal position immediately, like a dislocated shoulder popping back in.
Although that’s not the kind of “subluxation” that this article is about, such cases do provide important perspective, in that a true dislocation can be amazingly asymptomatic. There are many case reports of true spinal joint derangement and injury that cause little or no trouble, or certainly much less than most people expect. In the low back pain tutorial, I describe one of my own former massage therapy patients19 with a very serious lumbar dislocation — and no low back pain (she came to see me for a foot problem). Another patient with extreme scoliosis, although often uncomfortable, was generally surprisingly fine and even fit. The patient pictured here, as reported in New England Journal of Medicine, had no “pain, weakness, or parasthesia”!20
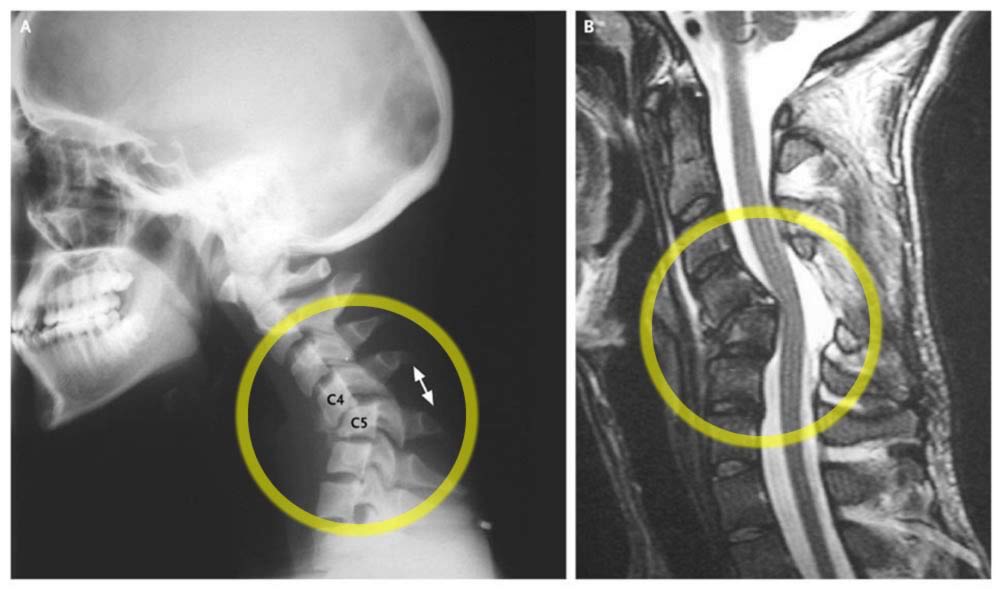
Traumatic dislocation.
For perspective, here’s an example of a spine that is genuinely “out of line.” Although this is a serious dislocation, the patient was quite healthy. See Akhaddar.
Another case report in the journal Spine describes a man who was born with part of a neck vertebra entirely missing — he also had no serious symptoms until he fell one day, and his unstable spine was dislocated “.21 After that he certainly was symptomatic: he had severe pain, but only pain.
Another fun example of congential deformity or anatomical variation is The Amazing Owl Man! You don’t see this every day. Enjoy this campy, cringe-inducing bit of news reel about a dude who can “owl” his neck — rotate 180˚ degrees! — if we can believe our eyes:
What are we to make of this? Is this anything more than an eye-popping novelty? I have no idea how he can do that, but can I extract some clinical relevance from it anyway? Natürlich! (As my high school German language teacher used to say.) Many of these examples of dramatic joint injury and dysfunction actually cause less trouble than chiropractic subluxations
If a painful or stuck-feeling neck or low back involves a “subluxation” in any sense other than partial dislocation, then, it must be something more subtle — something nowhere near so obvious as a traumatic injury — which puts it firmly in the category of the classic chiropractic subluxation.
But is there even any such thing? There is a decades-old argument between doctors and chiropractors about the existence or nature of chiropractic-style subluxations. Many chiropractors still believe in them, in one form or another, and some do not.22 Sam Homola writes:
What I read in books written by orthopedic and physical medicine specialists made more sense to me than what I was being taught in chiropractic college. I rejected the vertebral subluxation theory as a basis for use of spinal manipulation.
Sam Homola, Doctor of Chiropractic, in “Can Chiropractors and Evidence-Based Manual Therapists Work Together?”
As far as most doctors and scientists are concerned, and even for many chiropractors, the argument is long over. They believe that either subluxations do not exist at all, or they only exist in some clinically insignificant form. They argue that chiropractors still can’t prove they can even find alleged subluxations reliably, let alone treat them. They doubt that a spinal joint can be literally “out” in a clinically significant way, and the belief that it can “keeps chiropractic marginalized and subject to ridicule by the scientific community”.23 Edzard Ernst writes, “The concepts of chiropractic are not based on solid science and its therapeutic value has not been demonstrated beyond reasonable doubt.”24
In all the years that they have been talking about them, chiropractors have never been able to furnish proof of these mysterious subluxations which they alone are able to see. They may convince their clients, but never have they provided proof of their pretensions to men of science.
College of Physicians and Surgeons of the Province of Quebec in 1966 in “The scientific brief against chiropractic”25
Reality check: are spinal nerves the wellspring of all health and vitality?
Even if subluxations exist, chiropractic subluxation theory depends heavily on one premise, a conceptual bottleneck through which the entire theory must pass: that spinal nerve roots are terribly important to your health, and interfering with them spells T-R-O-U-B-L-E.
In fact, interfering with the nerve roots can only do so much harm to a person. Most of our health and vitality is regulated by mechanisms other than nerve signals travelling through nerve roots — by other kinds of nerves, and by hormones (see sidebar for details). Common trouble with nerve roots is limited to the garden-variety symptoms like pain, tingling, numbness, weakness, and so on — not organ failure and disease.29 Slightly pinched nerve roots only spell P-A-I-N and A-N-N-O-Y-A-N-C-E, at worst — no fun, no indeed, but hardly disease.
In any event, it’s also anatomically impossible for spinal joints to physically “pinch” nerve roots with anything less than extreme deformities of the spine.30
Some chiropractors go further with subluxation theory than others, and the further they go, the further out on a scientific limb they go. Most will argue that subluxations are at least responsible for chronic low back pain.
It’s extremely important to appreciate that minor variations in spinal anatomy are normal.31 Vertebrae are not Lego bricks, each one exactly like the other — they are biological and imperfect. Just because there is a slight variation in the lumps and bumps of your spine — something many of my patients worry about — does not mean that something is “subluxed.” And any such variation that is too subtle to be easily agreed upon is also unlikely to be clinically significant — and chiropractors, when tested, routinely cannot agree which joints in a given patient are actually “out.”32 One chiropractor will say it is the L3/4 joint that needs correcting, and the next will name another. This does not inspire confidence in the idea of subluxation.
There may be some truth somewhere in the chiropractic idea of subluxation, but it is clearly loaded and controversial and variable in meaning — too much so to be clinically useful. Instead, I encourage you to think in terms of the broader concept of “joint dysfunction” — that spinal joints can “misbehave,” perhaps in a variety of ways. If this sounds vague, you’re right — but that’s appropriate, because strong confidence in anything more specific than that is not really justified by the science. For instance, an intervertebral joint might move unevenly, as opposed to being out of place, and this could be clinically significant — but no one really knows.
So joint dysfunction almost certainly does not involve partial dislocation, misalignment, and serious interference with nerve root function, as implied by the traditional definition of “subluxation.” But many chiropractors have argued that this is all they really mean by “subluxation” these days anyway …
Is chiropractic subluxation theory really so different? How many chiropractors even believe it?
… we [chiropractors] have successfully distanced the concept of a chiropractic subluxation from that of an orthopedic subluxation.
A Rosner, The role of subluxation in chiropractic, 1997
I’ve heard many chiropractors scoff dismissively that “most chiropractors don’t believe subluxation theory anymore anyway.” Even if they are right, it admits that the profession is still burdened with a faction that does believe. But it’s not that small a faction. In fact, it’s probably a large one, between those who vocally defend the original, untainted theory and those who avoid the term because of its baggage but still believe it quietly, or who reject the most extreme versions but are still deeply influenced by the theory. Sam Homola:
Although many chiropractors are now backing away from the chiropractic vertebral subluxation theory, many continue to use the theory to justify treating a broad scope of health problems by “adjusting” the spine. … Some who do not use the word “subluxation” simply substitute another word or words, such as “joint dysfunction,” in support of their belief that some kind of segmental spinal “lesion” can affect overall health.
Openly defending the original chiropractic subluxation theory are many chiropractors who often call themselves “straight” chiropractors, meaning “pure.” Straights subscribe to the full, traditional “subluxation theory” more or less exactly as formulated more than a hundred years ago, they practice “subluxation-based chiropractic,” and they definitely think of a chiropractic subluxation as being fundamentally different than how a doctor would define subluxation. They believe that subluxations cause not only back and neck pain, but practically any health problem, simply by impinging or irritating spinal nerve roots.
An orthopedic subluxation, a true vertebral misalignment, or a mechanical joint dysfunction that affects mobility in the spine is not the same as a mysterious asymptomatic “chiropractic subluxation” that is alleged to cause disease by interfering with nerve supply to organs.
Chiropractic Vertebral Subluxations: Science vs. Pseudoscience, Homola (ScienceBasedMedicine.org)

A nice presented evaluation of spinal manipulation by Nick Hannah, PT.
Spinal manipulative therapy (SMT): Adjustment, manipulation and cracking of the spinal joints
The idea of “adjusting” the spine refers to many different manual therapies, usually performed by chiropractors, but also sometimes performed by other professionals.33 The knuckle-like facet joints of the low back may be mobilized (stragetically wiggled, basically34), cracked (like knuckles), tapped with a chiropractic “activator,” gently stretched or pushed on, and so on and on. Different styles may be intense or gentle — so gentle in some cases that you can hardly tell that anything is being done to you. It’s difficult to address them all at once, because there are so many different ways of going about it.
Spinal manipulative therapy is an extremely controversial topic, partly because of its connection to subluxation theory, and partly in its own right — is it safe and does it work? However, SMT for the low back joints is notably much safer and therefore less controversial than SMT for the neck. In the case of the neck, the risks are almost certainly much higher — it’s potentially lethal, in fact.35 I’ll discuss this more below. Here are the main concerns about SMT:
- Dubious provenance. SMT provided by chiropractors is largely based on the chiropractic idea of “subluxation,” which is itself a highly controversial theory that comes with a lot of baggage. To the extent that SMT is used to treat subluxations, it may be ill-conceived, over-prescribed, and inconsistent.
- Unimpressive benefits. SMT probably has some therapeutic effects on low back and neck pain, but they seem quite limited, and some methods of SMT probably don’t work at all. If SMT works at all, it certainly doesn’t work well enough to be an impressive and reliable therapy.
- Serious risks. SMT for low back pain has the potential to frighten patients and worsen their symptoms. SMT for the neck joints has the same risks, but with the chilling additional possibility that it can cause paralysis or death.
Indeed, not as many people want their spines “adjusted” as you might think. Despite the importance of the topic, only about 5% of the US population uses any kind of alternative therapy for their back pain, and only about 75% of those go to chiropractors.36 (SMT provided by physical therapists may be more common — I don’t have a statistic for that.) Still, even a small slice of the entire population is an awful lot of people.
Can SMT effectively treat neck and back pain? What does the science say?
Sam Homola points out that “there are at least 97 named antithetical adjustive techniques, all based on a nonsensical, nonfalsifiable chiropractic vertebral subluxation theory”37 — almost a hundred variations of SMT that cannot peacefully co-exist, the truth of one invalidating the others, like religions. So it’s hardly surprising that it’s difficult to determine, scientifically, what works and what doesn’t. Proponents of a flavour of SMT have a handy, comfortable defense: “my method is better than the method that was tested.”
Every published review of the literature comments on the lack of good quality evidence, making it impossible to be confident of anything.38 Even the most promising sources of research have had serious quality control problems.39 And yet plenty of that research evidence — weak though it may be — does give some hope that certain kinds of SMT might have some benefits.40 41 42 43 44
However, most of those conclusions are also qualified by various gotchas and uncertainties. Sometimes even major journals publish results that sound fabulous, but critics find flaws so major that it one wonders if it was even worth doing. There was a particularly noteworthy example early in 2011.45 Neil O’Connell:
The email from the industry was effusive. In a cock-a-hoop, caps lock-happy frenzy it bellowed “ALL MANUAL MEDICINE PROVIDERS SHOULD BE AWARE OF THIS STUDY.”
Or not? Mr. O’Connell readily identified numerous serious problems with this research in an article for Body In Mind:
It is of course possible that the results of this study are accurate and maintenance manipulations are effective, but these problems make it difficult to judge. The message from this one back pain trial might seem appealing and I can see why the email was so enthusiastic. But by focusing on one particular cherry that seems so ripe and juicy we might miss the bigger picture from the rest of the tree. And there is always the chance that the tastiest cherries contain a few artificial sweeteners. Personally I would lay off the caps lock for now.
So much for that hype.
And some studies, of course, are better quality and have had negative results. For example, in 1998, Daniel Cherkin (with medical back pain expert Richard Deyo) published a paper in the New England Journal of Medicine showing that, over the long-term, “patients receiving [chiropractic manipulation] treatments had only marginally better outcomes than those receiving the minimal intervention of an educational booklet.”46 Dr. Nikolai Bogduk weighs in with a paper stating his conclusion right in the title, “Spinal manipulation for neck pain does not work.”47 Similarly, Bronfort ostensibly found a positive result treating neck pain, but concedes that just “a few instructional sessions of home exercise with advice resulted in similar outcomes at most time points.”48
Another of the more recent experiments is a good one to zoom in on, because it damns SMT with faint praise: it is one of the official “positive” studies, but so mildly positive that one can’t help feeling disappointed by it. Is this the best SMT can do?
SMT competes with standard care … barely
In the fall of 2009, the Annals of the Rheumatic Diseases published a reasonably good test of SMT.49
The researchers took a hundred patients with nasty, fresh cases of acute low back pain, and delivered half of them into the care of chiropractors, and the other half into “standard care” — advice and ordinary pain medications, namely. Note that it has often been argued that SMT is best for acute low back pain, not chronic, so this is right in chiropractic’s strike zone: if there is anything special, anything even remotely impressive about SMT, it should have done rather well in this contest. It should actually pretty much pull out a can of whupass on “advice and meds.” One would hope.
It didn’t.
There was basically no difference between the groups. They did equally well — or equally poorly, if you prefer. All the patients had the same experience that pretty much everyone with chronic back pain has: they got better slowly but surely over the course of a few weeks, roughly exactly as they would have without any therapy at all. The researchers found that “SMT is unlikely to result in relevant early pain reduction in patients with acute low back pain.”
Now you might say, “Well, good: chiropractic was as good as drugs, so it could replace drugs. And that’s good!” But those drugs, taken in the quantities the subjects took them, are cheap and safe as houses. And their low cost was roughly appropriate for their took-the-edge-off effectiveness. Chiropractic therapy, by contrast, would have cost an order of magnitude more and required spending time on appointments with chiropractors.
So, yes, SMT “worked” — but how well? How impressed are you by SMT’s performance in this test? On a scale of ten?
Spinal manipulative therapy for migraine
Migraine is not a condition one would necessarily expect to be treatable with spinal manipulation,50 but it’s hardly surprising that people have tried. A particularly high quality test in 2016 was good enough to just about be the last word on this topic. (I’m sure it won’t actually be the last word, but high quality trials are rare in musculoskeletal medicine, and this is a particularly persuasive one.)
Chaibi et al. tested the efficacy of three months of regular chiropractic therapy for over one hundred patients with migraine, with follow-up for a year afterwards.51 Quite thorough. The patients were divided into three groups: (1) spinal manipulative therapy (SMT), (2) sham treatment consisting of irrelevant manipulations, and (3) a control group that continued with their standard medications and no other treatments. The number of migraine days per month was the main way that improvements were measured, but they also looked at migraine duration, intensity, headache index, and medication consumption.
Days with migraine went down modestly and about equally in all groups by the end of treatment. In other words, spinal manipulation for migraine was no better than the sham (on any measure, primary or secondary).
There was some minor good news for SMT: migraine intensity and headache index were modestly lower. These results are highlight by chiropractors keen to salvage scraps of good news from this study, but this is a form of cherry picking — and picking very small cherries. The effect sizes were modest, and only superior to the control group, not the sham.
Therefore, no measures, primary or secondary, produced any sign that SMT has any meaningful effect on migraine compared to a sham, and so the authors concluded that “the effect of chiropractic spinal manipulative therapy observed in our study is probably due to a placebo response.”
Formal reviews of and expert opinions on this mess
So it’s a mess. What do reviewers make of it? Better them than me! I’ll take you on a whirlwind tour of some of their older reviews, and then look more closely at the most recent and best.
Going back to 1996, Hurwitz et al. wrote that “cervical spine manipulation and mobilization probably provide at least short-term benefits for some patients with neck pain and headaches.”52 Not exactly a glowing endorsement, but others have been even less enthusiastic. Jumping to 2004, Bronfort et al. wrote that “There are few studies, and the evidence is currently inconclusive,” and that for chronic neck pain, mobilization/manipulation “offers at most similar pain relief to … rehabilitative exercise in the short and long term,”53 But that review also presented an incredible rats’ nest of conclusions, some of which were positive, some negative, all of which amounted to, “Um, it’s kinda complicated, and we’re not really sure.”54
Going from bad to worse, in 2006 the prestigious journal Spine concluded that neck adjustments are “not beneficial” when used alone.55
Does it get any better if we just look at the headache evidence? Worse, actually: even more inadequate and generally discouraging evidence. There were inconclusive scientific reviews of almost no good evidence in 200456 and 2007,57 and no improvement in 2011 in the most recent credible review:58
There are few rigorous RCTs testing the effectiveness of spinal manipulations for treating cervicogenic headaches. The results are mixed and the only trial accounting for placebo effects fails to be positive. Therefore, the therapeutic value of this approach remains uncertain.
For a more detailed analysis of the headache evidence, see The Complete Guide to Chronic Tension Headaches.
The best review so far
Although the scientific bottom line is (obviously) ambiguous and debatable due to the messiness of the data, things have been getting better. There is usually an exasperating absence of evidence about most manual therapies, but just a few years later the collective data for SMT is finally getting more substantive. And it’s still discouraging.
In 2012, an (updated) Cochrane review of SMT research was published.59 Cochrane reviews are not flawless, but they are well-regarded and are often the best available,60 and unfortunately the authors just weren’t that impressed. In their first version of the review, they came to the underwhelming conclusion that “there is no evidence that spinal manipulative therapy is superior to other standard treatments for patients with acute or chronic low back pain.” It also performed no worse, though, and was more effective than a fake intervention. A few years later, considering a bunch of new evidence,61 they still found SMT to be “no better or worse” than other therapies … which damned it again with very faint praise, of course, because no therapy has ever been shown to be all that effective for low back pain.62
A fair criticism of that review is that it lumps together too many kinds of SMT for too many different kinds of patients. Could the benefits of some SMT have been “washed out”? What if SMT works really well when done one way, with one kind of patient, but quite poorly otherwise? Real benefits in specific situations might disappear or “wash out” when mixed in with too many other scenarios where a therapy is doomed to failure.
On the other hand, any truly worthwhile benefits to SMT (in any situation) should be obvious and noteworthy. They should pull up the average.
Indeed — and this is the clincher — there is no individual study that I know of that shows any clinically substantial benefit. Not one. If any specific flavour of SMT works especially well for any particular type of patient, that combination was not studied in any of the 26 experiments covered by this Cochrane review.
And, just to bang that coffin nail one more time, all this is echoed by another major review from just a couple years before.65
What the mess of science amounts to for patients is that SMT is pretty unimpressive on average, and a bit of a crapshoot … but there are enough flickers of hope here and there that it might be worth a shot for the particularly desperate patient. Chiropractor Sam Homola sums the situation up nicely:
There is no definitive evidence that spinal manipulative therapy is more effective than other forms of treatment for patients with acute or chronic low-back pain. However, manual therapists know from experience that spinal manipulation is often more effective for providing immediate short-term relief for some types of back pain.
“Can Chiropractors and Evidence-Based Manual Therapists Work Together?”
This echoes his opinion in his 1999 book, Inside Chiropractic: A patient’s guide, that “many patients have told me that manipulation was more effective [than physiotherapeutic management] in providing immediate relief.”66 My own clients have often reported the same thing. The benefits are almost certainly there, for some people, some of the time.
But, just as clearly, SMT is not working any miracles, and thus it fails the “impress me” test completely. Some evidence may support SMT, but it doesn’t support it strongly. No one — or almost no one — is getting “cured.” After decades of study, the effectiveness of a therapy should be quite clear and significant. If it’s still hopelessly mired in controversy, how good can it possibly be? That’s an awkward question for a lot of alternative therapies.
Getting spinal joints unstuck
It’s kind of pointless to speculate about how a treatment works if we already know it doesn’t work — an axiom of science-based medicine. But speculation is fun. And if a primary, putative mechanism of action is demonstrably wrong, it adds to the evidence that the treatment doesn’t work.
So, without regard for any effect on pain, can SMT improve the function of spinal joints? There are many ideas about how manipulation helps if it helps, but this is the main one: the mechanical action and/or sensory stimulation supposedly normalizes spinal joint movement. This is a less simplistic version of supposedly putting them “back in place,” but it’s still quite simplistic: wiggle joint to unstick! “Motion is lotion.”
The unstate premise is that spinal joints can become some kind of stuck in the first place, moving inadequately or abnormally — one definition of a “subluxation” — and presumably this state of affairs is annoying, like a grain of sand in your mouth, not necessarily serious, but obvious and irritating, and probably progressively aggravating over time. It’s unclear whether or not this actually happens to spinal joints in the first place.
And, if it does, it’s probably difficult to reliably identify which joints it has happened to. The art of identifying stuck spinal joints is “motion palpation,” and in a 2015 test, two expert motion palpators could not agree on the location of joint stiffness or pain in a couple dozen patients.67 Hard to manipulate what you can’t find.
And … does SMT change spinal joint movement? A 2016 review says “no.”68 There are individual trials that show otherwise (Wong et al. is notable example69), but Aguirrebeña et al. conclude that the trial data isn’t compelling: “Evidence does not support an effect on segmental vertebral movement.” If there’s any movement dysfunction in the first place, this paper concludes that it’s unlikely that it can be put right.
But it’s more likely that the premise is just bogus, and joints just aren’t “stuck” or “out” in any kind of important way in the first place … or only so rarely, and/or in such specific types of patients, that it’s just an undetectable phenomenon without much more statistically powerful studies.
Is spinal manipulation safe?
Spinal manipulation is a very low risk trea... 😱😆😏 pic.twitter.com/ZbRZOBAO9o
— The Sp⚽️rts Physio (@AdamMeakins) December 14, 2020
If you don’t break the table… you’re not doin’ it right! Just a bit of whimsy to introduce a very serious topic. SMT is definitely not a risk-free treatment. Few treatments are completely safe, of course. Other manual therapies are also unsafe. Half of all manual therapy treatments of any kind will result in some kind of unpleasant side effect.70
Unsurprisingly, virtually any kind of neck manipulation can cause trouble — it’s a vulnerable structure. There is always some risk of life-threatening injury to the brain stem or vertebral arteries. It’s unlikely to happen, but it’s extremely serious when it does, and I’ll cover that separately in the next section. This section covers the lesser risks.
In 2010, Carlesso et al. analysed the scientific literature looking for evidence of harm from SMT for the neck.71 They found a statistically insignificant trend towards the negative, an uncertain number that leaned in the direction of bad news: increased neck pain might be 25% more likely with SMT than if you did nothing, or if you just stuck to safe and neutral treatments. The same murky data could also suggest basically the opposite: the absence of a clear signal constitutes “strong evidence that neck manipulation or mobilization does not result in an increase in neck pain,” according to the authors. Debatable,72 but noted. What about non-pain symptoms?
Much more certainly and strikingly, the same data does show that SMT patients are 100% more likely to have “transient neurological symptoms” — anything from feeling a bit woozy all the way up to serious unpleasantness, such as severe dizziness, nausea and vomiting. A typical case is described in What Happened To My Barber?
When performed intensely and/or carelessly — in the presence of undiagnosed vulnerabilities, say — SMT almost can cause direct injury. Even a completely healthy spinal joint could be mildly injured by a strong enough spinal manipulation. Most such injuries would be both rare and minor. Only extremely aggressive SMT could injure a healthy spine, and even if it did, it would probably just be a minor strain — hardly the result you want, but not that big a deal and not that common.
… the chances of injury are multiplied when chiropractic neck manipulation is routinely used many times on every patient in a misguided attempt to improve health, as opposed to occasional use of neck manipulation by physical therapists and other manual therapists who are concerned only about restoring mobility in a stiff spine.
Chiropractic Vertebral Subluxations: Science vs. Pseudoscience, Homola (ScienceBasedMedicine.org)
The risks to an unhealthy spine are obviously more serious. Most practitioners are unlikely to use aggressive SMT on a spine exhibiting symptoms of any trauma, disease or other vulnerability. However, mistakes happen — it’s unlikely, but definitely possible.
Artery tears are the most chilling and plausible example: these are not rare, and pain can be the only symptom, or by far the dominant one, with other signs and symptoms being quite subtle.73 The pain can drive patients to seek care without the foggiest idea that something ominous is going on. Although a good chiropractor is not going to miss the warning signs in most cases, a few are going to slip by even the most competent … with potentially disastrous consequences. Any strong manipulation of a neck with a torn artery is likely to worsen the tear, and greatly increase the risk of stroke. The harm might not even be obvious to the patient: just a worsening of symptoms. They think they’ve had a “bad reaction” to treatment, when in fact a serious injury has been inflicted on them.
The main common risk of SMT, however, is psychological: SMT can badly frighten patients, which is a serious risk factor for chronic neck and back pain. This is certainly not a life-threatening risk, but it’s not trivial either. The nervous patient has much to lose with SMT. Patients may be nervous because:
- they believe their spine is more fragile and vulnerable than it really is (and talk of “subluxations” usually aggravates this anxiety), and/or because
- the idea of spinal adjustment bothers them in any case (many people are “freaked out” by the idea of spinal joint cracking74).
Combining these factors — acute pain, minor potential therapeutic benefits, a high rate of harm, fear of your spine’s fragility, fear of the treatment — is all just a recipe for disaster. And so, although many clients have reported being “cured” by chiropractic treatment (sometimes even as they limp into my office still suffering from significant symptoms), many also have reported being “ruined” by a chiropractic treatment they found to be intense and terrifying and painful.
This unfortunate situation may then be more deeply aggravated by the therapist’s response: using the bad reaction as evidence of profound structural instability in the spine, and as a justification for (much) more treatment. People tend to emerge from such experiences hopelessly tangled up in the idea that they are fragile, broken and need regular SMT for the rest of their lives. It is quite tragic how one bad day can convince people that they have a really “bad back” that needs regular therapy almost forever.
Another surprising risk is that, even if all you have is back pain, chiropractors may recommend SMT for the neck even when your only symptoms are in your low back.75 And, as mentioned above, there may be substantial risks to neck adjustment. And most chiropractors don’t inform their patients about the risks.76 Let’s look at that topic now.
SMT for the neck can probably maim and kill
Hell, having your hair washed can maim and kill. Beauty parlour syndrome is rare, but common enough to be well-documented: a stroke caused by sustained neck extension while hair-washing.
SMT can probably do the same. It can cause a stroke by tearing delicate blood vessels in the neck, or cause brain stem injury in persons with undetected instability of the upper spine (atlantoaxial instability, AAI). Other injuries may be possible, including frank trauma to healthy tissues, as may have been the case with Jason Davidson, whose spine was severely injured by a physiotherapist that used “considerable” force manipulating his neck even after being asked to stop. This obviously incompetent treatment caused “severe acute injury to spinal discs which had caused blood flow to the spinal cord to cease.”77 The evidence for this will be discussed as we proceed. These hazards are certainly more likely for patients with severe and chronic symptoms. These are also therefore the patients most likely to desperately try a wide variety of treatment options, including more aggressive and frequent neck adjustments.
Disturbingly, AAI is such a complex condition that even substantial dislocation of the upper cervical spine can be clinically silent, and virtually impossible to diagnose without a specific type of X-ray (a type that chiropractors do not generally do).79 Thus, some people with AAI are walking around without so much as a headache as a warning sign … yet they are vulnerable to severe brain stem injury if they receive cervical SMT.
Less serious but extremely unpleasant consequences are also possible for patients with AAI. A light poke in the brain stem won’t kill you, but it can sure ruin your day! I knew a woman with a confirmed case of post-traumatic AAI who was treated too roughly by a student massage therapist, and she suffered about a day of severe disorientation, vertigo, and vomiting.
That’s what a poke in brain stem can do.
Incredibly, some therapists may dismiss such severe reactions with the absurdly unsafe theory that the body is just processing toxins released during the treatment. It’s difficult to imagine a more daft and irresponsible rationalization for a serious treatment mistake. For an emotionally compelling example of such dangerous incompetence, see the article What Happened To My Barber?
These dangers are, like everything else about SMT, controversial. Proof of the danger is hard to come by. Above we discussed a study by Carlesso et al. showing clear evidence that minor to moderate neurological side effects are more than twice as likely with SMT than with other neck treatments. But they did not find “smoking gun” proof that neck adjustment can kill. In fact, they didn’t even try to calculate the relative risk — the data just wasn’t up to the task. That doesn’t mean that the phenomenon doesn’t exist.80
Considering the relatively minor benefits and the high stakes, is any risk acceptable? This has been a subject of fierce debate for many years, with the chiropractic profession consistently on the defensive,81 but even key sources like the infamous Cassidy paper are weak sauce.82 Credible experts continue to publish evidence that concern about this issue is justified. For instance, in recent years the journal Physical Therapy concluded that “the literature does not demonstrate that the benefits of manipulation of the cervical spine outweigh the risks,”83 and the journal Spine concluded that “adverse reactions to chiropractic care for neck pain are common.”84 The value of a treatment must be weighed against the potential harm. As a group of Canadian neurologists ask, “Is a headache worth dying for?” Their concerns are outlined in a detailed document, “Statement of Concern to the Canadian Public from Canadian Neurologists Regarding the Debilitating and Fatal Damage Manipulation of the Neck May Cause to the Nervous System.”85
Even the most dire risks to treatment are not necessarily unacceptable, however. The chances of dying in an accident on the way to the dry cleaner is probably much greater. For the chronic neck pain patient, the risks may be acceptable if there’s a reason to believe the treatment might actually work. Some cases of neck pain and crick are extremely severe — and such patients may literally feel they have little to lose.
Unfortunately, the rationale and scientific evidence to support the use of SMT for neck pain is poor, and some methods of SMT are almost certainly useless. In chiropractic offices with a traditional view (the majority), most of the point of SMT is to treat “subluxation” -- which, as we’ve discussed, is an idea so under siege that many chiropractors themselves have denounced it. If SMT is largely supposed to treat a problem that is poorly defined and highly controversial at best, and maybe doesn’t exist at all, how good can it possibly be?
Ineffective variants of SMT
There is a problem with SMT methods that are particularly kooky. According to Dr. Homola, responsible chiropractic therapy for back pain should mostly be limited to mobilizing (wiggling) the lumbar intervertebral joints. However, there are numerous other methods, and some are particularly far out in left field.
A good example is the common use of an “activator” — a little tool that gently taps the skin and muscle over the joint. The rationale for the use of the activator is super thin, and there is no credible evidence whatsoever that it actually does anything — it’s virtually unstudied, nor is there much reason to study it. It’s just not a good enough idea!
Considering that even standard SMT isn’t working any miracles, you need to be skeptical of obscure variations on it, especially the “subtle” ones that hardly seem to be doing anything.
Scratching the itch you can’t reach: why joint popping feels good and possibly relieves pain
Here’s Dr. Homola again, still making the case for manipulation about as well as I think it can be made in a 2015 article:86
Patient satisfaction coupled with the “possible” benefits of spinal manipulation is reason enough to support inclusion of spinal manipulative therapy as a treatment option in the armamentarium of any therapist or practitioner who treats back pain. It has been my observation that manipulation can be more effective than most forms of physical treatment in providing dramatic, albeit temporary, relief of mechanical-type back pain. Although acute back pain is usually a self-limiting condition, the symptomatic relief provided by spinal manipulation can be a welcome effect.
I think it’s mostly based on how nice it can feel. There’s probably overlap between “symptomatic relief” and something that just feels pleasant. And joint popping and cracking can feel downright great. I know. I’m a crack addict, a joint popping junkie: many of my joints snap easily (often spontaneously) and pleasantly. I find it as hard to imagine life without joint popping as a life without back scratches.
Many people get relief from these little spinal “adjustments.” It seems like “scratching an itch you can’t reach.” Why does joint popping feel so good? If SMT works, why does it work, and does it have anything to do with this relieving sensation?
Whatever you have been told before, the nature of joint popping is not well understood.87 It is firmly in that category of trivial mysteries for which there is simply no research funding, and as such it will probably remain unexplained for a long time.
We do know that joint pops involve a slight increase in range of motion. Pops occur when pushing up against the limits of a joints range of motion. When the pop occurs, the joint moves just a little further.
And we also know that we can feel cracks as well as hear them. Sometimes they are even painful.88
The main skeptical take on cracking/SMT is that it’s a blast of novel sensory input that has a transient, minor effect analogous to finally getting to stretch your legs after getting off a long flight, or scratching an itch. When you really want to move, when you feel stiff, even a teensy bit of extra joint movement can feel very welcome. A better-than-nothing effect.
This interpretation is often intended to be a bit derogatory and dismissive. The punchline is that the effect is “just” a change in how the joint feels, and not a change in how it works or in the state of its tissues. But I wouldn’t want to live without scratching! Since living systems seem to thrive on sensory input, and suffer quickly without it, the sensation of relief may be quite important to us. And how joints feel might have something to do with how the work. Although Aguirrebeña et al. don’t think SMT changes joint motion, they did conclude there’s evidence of pain-killing and “improved muscle function” after manipulation.89
The “scratching an itch” can account for the satisfied feelings many people report, but it doesn’t promise the moon, either. The relief often don’t last long, and soon the “itch” needs to be “scratched” again — a notorious problem with SMT.90
It also probably explains another common problem with SMT: why the results are all over the map. Exactly what the nervous system does with novel sensory inputs depends on many factors. Some people, some of the time, seem to be able to enjoy and “exploit” such sensations and get a therapeutic effect. Other patients seem to largely ignore it — it just doesn’t make much of an impression on them. And still others are actually afraid of it! For that not-so-minor minority who find joint popping kind of alarming, popping/SMT won’t seem refreshing and relieving, but more like a bitter medicine (at best) or just a bad idea. Such an unpleasant psychological context is probably more severe in the case of low back pain, where structural problems are so feared by patients.
A significant change in the tissue state and function of the joint is conceivable — as opposed to just how it feels — but exactly what changes is unclear, and it’s unlikely that it matters much or lasts long in most cases. Most likely, popping doesn’t affect spinal facet joint function any more than it affects knuckle function.
Minimizing the risks of SMT
What you almost certainly want to avoid is the worst-of-both-worlds scenario in which you take the risks for the sake of a treating mild neck pain or — yeeks — only as a preventative treatment (as chiropractors often recommend).91 Don’t do that! There is simply no justification for SMT for the neck unless you have a problem that is worth the risk.
Here are some guidelines that may improve your chances of getting benefit from this approach, and minimizing risk. Evidence published by Manual Therapy shows that, if neck manipulation works at all, it may be more likely to work for people with these signs and symptoms.92 Perhaps to some extent this is also true of low back pain. Check all that apply to you:
- the severity of your case is mild or moderate, not severe (yes, this contradicts what I said above93)
- your neck pain is on both sides some or all of the time
- your neck feels better with movement and exercise
- you aren’t stuck in a chair more than 5 hours a day
- tipping the head back isn’t a problem
- you have no sharp, shooting pains into the arms
And here are few more guidelines for safety of my own:
- Avoid cervical adjustment if you have a history of nausea and/or vomiting associated with your neck pain, or with neck movement. Please be aware that not all physical therapists will recognize these symptoms as warning signs!
- Avoid extremes of treatment intensity. Strong neck adjustments may be dangerous, subtle ones may be useless. There is obviously less potential harm in a gentler treatment (except to your pocket book, perhaps).
- Avoid overprescription. (How much is too much?94) If you sense that a chiropractor or other health care professional wants to set you up for long term regular therapy, find someone else to help you.
- Avoid rationalizing of adverse effects. If neck mobilization/manipulation is going to help you, you should not experience any severe side effects — a little soreness or increased symptoms at the worst. Avoid any practitioner who tries to explain away significant side effects (i.e., “it’s just the toxins being cleared out”).
- Trust your instincts! Many people feel uncomfortable with the idea of neck adjustment. That concern could be the wisdom of your body talking to you (or it could also be irrational). But consider listening to that little voice!
- Inquire about the possibility of treating the neck by adjusting the thoracic spine. Thoracic spinal adjustment may help with neck pain,95 but feels safer because it almost certainly is safer. This is a particularly worthwhile option to consider if you feel nervous about neck adjustments.
If you discover, or already know, that cervical spine adjustment is helpful for you, make an effort to find a chiropractor you trust, and establish a long term relationship, confident that most of the risks discussed here will be eliminated. “Good science-based chiropractors who do not subscribe to the vertebral subluxation theory and who use manipulation appropriately can offer a service of value,” Sam Homola writes. “Unfortunately, such chiropractors are not easy to find.”
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Related Reading
- Your Back Is Not Out of Alignment — Debunking the obsession with alignment, posture, and other biomechanical bogeymen as major causes of pain
- Extraordinary Health Claims — A guide to critical thinking, skepticism, and smart Internet reading about health care
- The Complete Guide to Low Back Pain — An extremely detailed guide to the myths, controversies, and treatment options for low back pain
- The Complete Guide to Neck Pain & Cricks — An extremely detailed guide to chronic neck pain and the disturbing sensation of a “crick”
Here are some books I recommend:
- Inside chiropractic: a patient’s guide (book), by Samuel Homola. Amazon.com ❐ Dr. Homola is a chiropractor, and the most prominent critic of his own profession. His book is an essential patient guide to a profession that is so full of controversy that consumers need a guide before going to a chiropractic office. If you like getting your spine cracked, or you think you need to be “adjusted,” read this book before making your next chiropractic appointment!
- Trick or Treatment: The Undeniable Facts About Alternative Medicine (book), by Simon Singh and Edzard Ernst. Amazon.com ❐ A thorough examination and judgement of more than thirty of the most popular “alternative” treatments, such as acupuncture, homeopathy, aromatherapy, reflexology, chiropractic and herbal medicine. The ultimate verdict on alternative medicine is delivered for the first time with clarity, rigour and authority.
- Spin doctors: the chiropractic industry under examination (book), by Paul Benedetti and Wayne MacPhail. Amazon.com ❐ I include this selection as much for its Canadian content as because it is a good book. Canadians visit chiropractors about thirty million times a year, and surveys show that patients are generally satisfied with their treatment. But studies also show that as many as two hundred Canadians a year may suffer strokes brought on by neck manipulation. Spin Doctors takes a hard, dramatic, and spine-chilling look into the world of chiropractic medicine. You will be surprised to learn what chiropractors treat and why — and how much it costs you as a taxpayer. Most important, you'll learn how to protect yourself and your family from dangerous adjustments, practice-building tactics, bogus treatments, and misleading information. Paul Benedetti is an award-winning journalist who, for more than a decade, has written investigative stories about alternative medicine and health fraud. Wayne MacPhail is a journalist who has written about AIDS, alternative medicine and other health, science, and social issues for twenty-five years.
And some more immediately accessible resources:
- “Can Chiropractors and Evidence-Based Manual Therapists Work Together?,” Homola, Journal of Manual & Manipulative Therapy, 2006. Dr. Sam Homola covers the topics of subluxation theory and spinal manipulative therapy in this 2006 article, managing to be precise and thorough without losing his amiable tone (exactly what I aim for on PainScience.com). It’s still a bit heavy going for patients, but it’s worthwhile for anyone who’s really keen to understand the subject matter, and it’s still completely relevant more than a decade later.
- Chirobase: Your skeptical guide to chiropractic history, theories, and practices (chirobase.org). One of the first substantial chiropractic skepticism resources available on the Internet, and it remains the largest (although perhaps SBM is catching up now). Chiropractors everywhere must have strong opinions about this site. Operated by Stephen Barrett, MD, and ScienceBasedMedicine.org’s regular guest author and chiropractic insider, Samuel Homola, DC. Most articles remain relevant despite their age. The site is a bit old school, however, and its vintage is starting to show.
- Vertebral Subluxation on Wikipedia.com. An emotionally neutral evaluation of the chiropractic idea of intervertebral subluxation. I can save you some reading time: the bottom line of the article is that a century of debate has failed to produce any clear answers. Subluxations remain elusive.
- “Subluxation: Chiropractic's Elusive Buzzword,” Stephen Barrett, ChiroBase.org. Dr. Stephen Barrett’s take on chiropractic subluxation theory. This is one of the most prominent anti-chiropractic articles available on the Internet.
- “Undercover Investigations of Chiropractors,” Stephen Barrett, QuackWatch.org. In a series of informal but devious and persuasive tests, physician Stephen Barrett contrived to challenge the diagnostic skills of a number of chiropractors. The results were inconsistent, and make for some fascinating and disturbing reading.
- “Chiropractic Vertebral Subluxations: Science vs. Pseudoscience,” Samuel Homola, ScienceBasedMedicine.org. An excellent, expert treatment of a tricky subject by skeptical chiropractor and writer Sam Homola. No matter how much I learn about the subject, I can always learn something new from Sam.
What’s new in this article?
2025 — Science update, the first in a while: added an interesting result from Nim et al. showing that SMT technique is irrelevant.
2022 — Substantial improvements and updates to the introduction.
2019 — Science updated, added Rubinstein et al. to the evidence review.
2018 — Like-new section, heavily revised and updated: “Scratching the itch you can’t reach: why joint popping feels good and possibly relieves pain.”
2018 — New section: “Getting spinal joints unstuck.” Miscellaneous edits.
2017 — Added an example of SMT injury and a footnote about fearmongering.
2017 — Added information about artery tears with pain as the only symptom.
2017 — Significant science update to the introduction based on Paige et al.
2016 — New section: “Spinal manipulative therapy for migraine,” based mainly on Chaibi et al.
2016 — Minor update to references related to SMT for headache.
2016 — Added reference to body perception, Moseley 2008.
2011 — Added scientific cases studies, examples, pictures and video of true dislocation and abnormal anatomy to help drive home the point that even significant spinal joint dysfunction can be surprisingly harmless … never mind subtle joint problems.
2011 — Added footnote to “Minimizing the risks of SMT”, explaining how much SMT is too much.
2011 — Added reference to article in The Guardian about chiropractor disclosure of risk to patients.
2010 — A good thorough editing and cleanup. There was a bit of a mess in the aftermath of the upgrades a few days ago. 😜
2010 — Major upgrades inspired by a new scientific paper about the dangers of spinal manipulative therapy, and by Dr. Sam Homola’s new article at ScienceBasedMedicine.org, Chiropractic Vertebral Subluxations. I revised and improved content and referencing throughout the article in this update.
2009 — Publication.
Notes
- Rubinstein SM, Terwee CB, Assendelft WJJ, de Boer MR, van Tulder MW. Spinal manipulative therapy for acute low-back pain. Cochrane Database Syst Rev. 2012;9:CD008880. PubMed 22972127 ❐ PainSci Bibliography 54694 ❐
Despite this, the rest of their conclusions seem crafted to prolong the controversy. They explain to clinicians why they should still refer patients for SMT (“preferences” and “costs”); they say that more research is needed to “examine specific subgroups.” (This is based on the faint hope that SMT might work so well for an unknown subcategory of patients that they can pull up the average; see Saragiotto 2016, Saragiotto 2017.) And they say there’s a need for “an economic evaluation,” but if a treatment is not effective, it can’t be “cost effective.”
- Paige NM, Miake-Lye IM, Booth MS, et al. Association of Spinal Manipulative Therapy With Clinical Benefit and Harm for Acute Low Back Pain: Systematic Review and Meta-analysis. JAMA. 2017 Apr;317(14):1451–1460. PubMed 28399251 ❐
Paige et al. do seem to present a positive conclusion at first glance: the benefits of SMT are disingenuously summarized as “statistically significant” in the abstract, with no mention of clinical significance (effect size). So the abstract sounds like good news to all but the most wary reader, while deep in the main text the same results are conceded to be “clinically modest,” and even that seems excessively generous. Personally, I need a 20% improvement to consider it “modest”!
- Although fortunately “no RCT reported any serious adverse event,” it seems that minor harms were legion: “increased pain, muscle stiffness, and headache were reported 50% to 67% of the time in large case series of patients treated with SMT.” That’s a lot of undesirable outcomes.
- Rubinstein SM, de Zoete A, van Middelkoop M, et al. Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain: systematic review and meta-analysis of randomised controlled trials. BMJ. 2019 Mar;364:l689. PubMed 30867144 ❐
This review in the British Medical Journal continues the tradition of damning spinal manipulative therapy with extremely faint praise. It has a putatively positive conclusions, and so it will be widely cited by chiropractors as evidence of the efficacy of SMT for back pain. However, even trying to spin the data in favour of SMT, the conclusions seem tepid at best: they not some short term benefits, and declaring that “SMT produces similar effects to recommended therapies for chronic low back pain.” But chronic low back pain is notoriously untreatable, and all treatments produce minor short term benefits and no long term benefits (see Artus, Cashin). The evidence has been available for many years that SMT is just as ineffective as everything else. These conclusions are disingenuous nonsense.
There are other serious methodological concerns here, summarized by Mary O'Keeffe & Neil O'Connell in a letter to the editors of the British Medical Journal. Their conclusions are far more in tune with the evidence reviewed:
These results demonstrate no convincing evidence for the superiority of SMT over sham SMT and a lack of clinically important benefit of SMT when compared with any other treatment. The lack of a benefit of SMT over sham therapy indicates that SMT is unlikely to have any direct benefits and observed improvements are the result of contextual and other effects. It is likely that the apparent equivalence with both ‘recommended’ and ‘non-recommended’ therapies tells us more about the disappointing effectiveness of those approaches than it does about the benefit of SMT.
- Nim CG, Downie A, O'Neill S, et al. The importance of selecting the correct site to apply spinal manipulation when treating spinal pain: Myth or reality? A systematic review. Sci Rep. 2021 Dec;11(1):23415. PubMed 34862434 ❐ PainSci Bibliography 52169 ❐
This 2021 study shows that it doesn’t much matter which joints are manipulated in spinal manipulative therapy… which is not a great look. More specifically, it showed that there’s no benefit to SMT based on skilled joint selection, which is a nifty angle.
Nim et al. evaluated tests of SMT where adjustment of “clinically relevant joints” was compared to SMT applied “elsewhere” to “non-candidate” joints. Obviously the expertly selected joints should have produced better results. But they didn’t.
That result was based on data from 10 studies “all of acceptable quality” (SMT has been studied quite a bit). Nine reported no statistically significant differences, and the tenth reported only a small difference.
- Nim C, Aspinall SL, Cook CE, et al. The Effectiveness of Spinal Manipulative Therapy in Treating Spinal Pain Does Not Depend on the Application Procedures: A Systematic Review and Network Meta-analysis. J Orthop Sports Phys Ther. 2025;55(2):1–14. PubMed 39869665 ❐
SKEPTICS: Spinal manipulation is a big ol’ nothing burger.
SPINAL ADJUSTMENT FANS: It’s all in the wrist. Got to do it right. You just suck at it.
BIG NEW SCIENTIFIC REVIEW: Nope, doesn’t matter how you manipulate the spine. “None of the SMT procedures were superior to others in terms of pain relief.”
Sooo much energy has been poured into spinal manipulation “technique” over the years … without much to show for it. Nim et al. is now the go-to citation for “it does not matter how you do it.”
That quick sassy take on the review was popular on social media, and controversial, of course — spinal manipulation always is. My post was “workshopped” quite heavily in the comments. Some highlights:
“Yup, saw that paper via McMaster’s pain research newsletter thing and the conclusions were like ‘good news it doesn’t matter, so go ahead’ and I couldn’t help but leave a comment on that to indicate that if something actually works by a specific mechanism then IT SHOULD MATTER HOW YOU DO IT. Otherwise how is this different from standard massage or mobilization?”
“Just reminding everybody that this is another one in a row of studies showing lack of specificity (doesn’t matter which technique you use, just touch your patient).”
“Indicating that the only active ingredient is caretaking touch. So optimize for THAT. 🙂”
A popular soft criticism was that this paper gives us a non-conclusion, rather than an actual strike against manipulation, because it was based on low-quality evidence only. But that’s not strictly the same as an absence-of-evidence …
It is reasonable to infer evidence-of-absence from a posse of junky little studies that fail to produce a signal even when most of the researchers are almost certainly trying to p-hack their way to a happy ending. Is that inference as good as a high quality RCT that “proves” that manipulation technique is trivial or completely irrelevant? Of course not. But it’s also not nothing! It’s genuinely informative when a bunch of high-risk-of-bias trials cannot even cough up a convincing false positive, let alone the real deal.
If it’s really hard to detect any difference attributable to technique, it’s probably because it just doesn’t exist.
- In August 2010, Kaiser Permanente cut neck manipulation from their chiropractic coverage. Their revised policy states: “Given the paucity of data related to beneficial effects of chiropractic manipulation of the cervical spine and the real potential for catastrophic adverse events, it was decided to exclude chiropractic manipulation of the cervical spine from coverage.” Dr. Hall reported on the decision in detail.
- Chiro.org [Internet]. Rosner A. The Role of Subluxation in Chiropractic; 1997 November 6 [cited 19 Nov 6]. PainSci Bibliography 52685 ❐
By the late 90s “through consensus of the chiropractic college presidents under the auspices of the Association of Chiropractic Colleges in July of 1996,” subluxation was defined as:
a complex of functional and/or structural and/or pathological changes that compromise neural integrity and may influence organ systems function and general health
So, anything that can go wrong with a joint, causing any kind of health problem. Gotcha. And yet, as broad as it is, note that pain isn’t even mentioned — it went straight to organs and general health. And then, much more recently (in 2014), the official definition is broader still! In fact, this definition widens the scope so far that we’re no longer even just talking about the spinal joints, but any harmful “imbalance or distortion” anywhere in the body:
Subluxation is a neurological imbalance or distortion in the body associated with adverse physiological responses and/or structural changes, which may become persistent or progressive. The most frequent site for the chiropractic correction of the subluxation is via the vertebral column.
- Homola S. Finding a Good Chiropractor. Archives of Family Medicine. 1998;7(1):20–23. PainSci Bibliography 56032 ❐
- Dr. Sam Homola: “The treatment protocol of subluxation theory requires that all chiropractic patients have a spinal adjustment, whether they are symptomatic or not.”
- Mirtz TA, Morgan L, Wyatt LH, Greene L. An epidemiological examination of the subluxation construct using Hill's criteria of causation. Chiropractic & Osteopathy. 2009 Dec;17(1):13. PubMed 19954544 ❐ PainSci Bibliography 55783 ❐ A classic paper. Four chiropractors analyze subluxation theory and tear it out by the roots, finding that it fails to meet any of (Hill’s) criteria of causation: “No supportive evidence is found for the chiropractic subluxation being associated with any disease process or of creating suboptimal health conditions requiring intervention. Regardless of popular appeal this leaves the subluxation construct in the realm of unsupported speculation.” And yet it’s been there for more than a century, I’d like to add! Dr. Harriet Hall explained the significance of the paper in an article for ScienceBasedMedicine.org, The End of Chiropractic.
- Ingraham. Organ Health Does Not Depend on Spinal Nerves! One of the key selling points for chiropractic care is the anatomically impossible premise that your spinal nerve roots are important to your general health. PainScience.com. 4736 words. Are the little bundles of nerves that exit your spine the wellspring of all visceral vitality? Will your organs wilt like neglected house plants if those nerve roots are slightly impinged? No: cut a nerve root completely, and you’ll certainly paralyze something, but not an organ, because organs simply don’t depend on spinal nerve roots. And yet this is what many chiropractors believe, and would like their customers to believe, after a century of contradictory evidence.
- This conclusion was published in 1995 by a PhD and another chiropractor criticicizing his own profession: see Nansel and Szlazak.
- Moseley GL. I can't find it! Distorted body image and tactile dysfunction in patients with chronic back pain. Pain. 2008 Nov;140(1):239–43. PubMed 18786763 ❐
In this small, unusual study, six patients with low back pain were asked to draw their perceptions of their back and spine. For comparison, a group of ten patients with no recent back pain were asked to do the same exercise. They were encouraged to “draw what it feels like” rather than how it actually looked.
“All the patients, and none of the controls, showed disrupted body image of the back” on the same side and level as the pain. For instance, they did not have a clear sense of the outline of their trunk.
Most intriguingly, patients with back pain on just one side illustrated vertebrae deviated towards the painful side (without any obvious actual deviation).
- This is a very well-used bit of chiropractic marketing language. The rhyme and the simplicity have been used to sell chiropractic services for a century.
- In “Finding a Good Chiropractor”, Sam Homola writes, “With the development of osteopathy in 1874 and the appearance of chiropractic in 1895, spinal manipulation gave birth to a new theory. D. D. Palmer, the founder of chiropractic, a grocer, and a magnetic healer who healed by touch, announced his discovery that ‘ … 95 percent of diseases are caused by displaced vertebrae; the remainder by luxations of other joints.’”
- Swain MS, Gliedt JA, de Luca K, Newell D, Holmes M. Chiropractic students' cognitive dissonance to statements about professional identity, role, setting and future: international perspectives from a secondary analysis of pooled data. Chiropr Man Therap. 2021 Feb;29(1):5. PubMed 33526067 ❐ PainSci Bibliography 51712 ❐
An analysis of survey data from almost 2400 chiropractic students showed that 45% embrace subluxation-based or “straight” chiropractic, strongly emphasizing that this view of chiropractic continues to define the profession well into the 21st Century. Specifically, they agreed that it is important for chiropractors to hold strongly to the traditional chiropractic theory that adjusting the spine corrects “dis-ease.”
- I was a Registered Massage Therapist with a busy practice in Vancouver, Canada, from 2000–2010. I quit the profession in disgust before I could be “fired” for being critical of pseudoscience and alternative medicine. I changed my professional focus to science journalism and anti-quackery activism, writing mostly about massage-adjacent topics in the early years, but then spreading out into anything relevant to any kind of chronic pain or injury rehab — an effectively infinite list of topics. Even fifteen years after my last hands-on work, I still think of myself as a massage therapist. That said, I don’t exactly feel like an “insider” either, and I’ve branched out a lot in that time. See my bio.
- Akhaddar A, Boucetta M. Dislocation of the Cervical Spine. N Engl J Med. 2010 May 20;362(1920). PainSci Bibliography 55145 ❐
A case report (and disturbing X-ray) of a traumatic cervical spine dislocation, notable for being mostly asymptomatic: just torticollis and limited motion, but no pain, weakness or altered sensation. That such a serious injury can have so little impact on a person is quite interesting!
Paper abstract:
A 22-year-old man presented with a 10-day history of torticollis. Two months before presentation, he had fallen from standing height but did not report subsequent cervical pain, weakness, or paresthesia. On examination, there was a reduced range of movement of the cervical spine without other neurologic deficits. Radiography of the cervical spine showed a marked reversal of the cervical lordosis, anterior displacement of 60% of C4 on C5, anterior callus formation, bilateral facet dislocation, and increased posterior interspinous distance (double arrow) (Panel A). Magnetic resonance imaging was performed. Sagittal T2-weighted imaging revealed a spinal cord angulation with mild compression but without intramedullary edema or hemorrhage (Panel B). The patient was admitted for surgery. With the use of an anterior approach, diskectomy, tricortical bone grafting, and insertion of a cervical plate were carried out, with a good outcome.
- Moon SJ, Lee JK, Seo BR, Kim SH. Traumatic subluxation associated with absent cervical pedicle: case report and review of the literature. Spine. 2008 Aug;33(18):E663–6. PubMed 18708921 ❐
This paper describes the case of a man who developed severe neck and shoulder pain after a fall. It turned out that a part of one of his neck vertebrae was entirely missing, since birth (“a relatively uncommon developmental anomaly”). The fall subluxed the joint substantially. Although painful, the lack of neurological symptoms is surprising — and more evidence that nerve roots are not easily pinched.
Paper abstract:
STUDY DESIGN: Case description.
OBJECTIVES: To describe a case of traumatic subluxation in association with a congenitally absent cervical pedicle, and review the pertinent medical literature.
SUMMARY OF BACKGROUND DATA: The congenital absence of a cervical pedicle is a relatively uncommon developmental anomaly that is frequently mistaken for a unilateral facet fracture-dislocation in the context of acute trauma. Because there is little evidence of recovery after surgery, and the symptoms are usually not disabling, surgery is not recommended for most cases.
METHODS: A 62-year-old man presented with severe neck and right shoulder pain after falling. Plain radiographs and computed tomography of the cervical spine showed the typical features of a congenitally absent pedicle at C6 with anterolisthesis of C6 on C7. We performed anterior interbody fusion at C6-C7 because of persistent neck pain and progressive instability.
RESULTS: Complete restoration of the C6-C7 subluxation was achieved with resolution of the presenting symptoms. At 18 months follow-up, flexion and extension dynamic radiographs demonstrated good alignment with solid fusion at C6-C7.
CONCLUSION: Although conservative treatment is the primary treatment for this clinical entity, surgery is an alternative option for those patients who fail to achieve recovery after conservative treatment or exhibit instability.
- Good examples of those who do not include chiropractor Dr. Sam Homola, author of Inside Chiropractic; Dr. Edzard Ernst, author of Trick or Treatment: The Undeniable Facts About Alternative Medicine (and who is not quite a chiropractor, but close enough); and Dr. Murphy , one of five research-oriented chiropractors who have bared their profession’s shortcomings in a 2008 article that calls for “dramatic changes” and states that chiropractic “finds itself in a situation in which it is rated dead last amongst healthcare professions with regard to ethics and honesty.”
- ScienceBasedMedicine.org [Internet]. Homola S. Chiropractic Vertebral Subluxations: Science vs. Pseudoscience; 2010 Sep [cited 16 Feb 13]. PainSci Bibliography 54979 ❐
- Ernst E. Chiropractic: a critical evaluation. J Pain Symptom Manage. 2008 May;35(5):544–62. PubMed 18280103 ❐
- Yes, this an old source. However, “men of science” (and women) remain unconvinced. The spirit of this statement is just as valid as it was more than forty years ago.
- There is an exception, but it does not compromise the point: sympathetic nerves emerge from the spine and have an indirect and non-critical functional connection with organs. However, organs work just fine even when this connection is broken.
- This fascinating and terrible phenomenon has been well-documented in medical journals only relatively recently, although patients and doctors were likely aware of it all along. See Hagen 2015.
- After complete loss of spinal nerve supply, organs continue to function quite well in the short term, even as movement and sensation are completely destroyed (paralysis). But the irritation to the spinal cord causes autonomic dysregulation over time, which slowly wreaks havoc on organ function. In other words, organs don’t depend on the spinal cord, but they do partially depend on smooth operation of the autonomic nervous system … and the ANS gets twitchy in response to an injured spinal cord.
- Nansel and Szlazak explain that pain and other symptoms referred from a spinal segment can “create overt signs and symptoms that can mimic, or simulate (rather than cause), internal organ disease.” This fact undermines vertebral subluxation theory in another interesting way — it explains a fairly straightforward mechanism by which chiropractors may have been fooled into believing subluxation theory in the first place.
- Sam Homola describes in detail a scientific experiment in which a dissected spine is mangled by machinery in the attempt to discover just how far you have to bend a spinal joint before its nerve roots are impinged. The answer? Really damned far — you have to take the spine way beyond its normal anatomical limits. The fact is that the holes through which nerve roots exit the spine are quite generous, not at all a tight fit, and that only major injuries or disease processes can result in a pinched nerve root in this way.
- Minor variation in any anatomy is normal! See You Might Just Be Weird: The clinical significance of normal — and not so normal — anatomical variations.
- QuackWatch.org [Internet]. Barrett S. Undercover Investigations of Chiropractors; 2003 [cited 12 Mar 9]. PainSci Bibliography 57171 ❐
In a series of informal but devious and persuasive tests, physician Stephen Barrett contrived to challenge the diagnostic skills of a number of chiropractors. The results were inconsistent, and make for some fascinating and disturbing reading.
- Doctors (especially osteopaths, physiatrists, and sports medicine specialists), physiotherapists, and massage therapists also practice forms of SMT, but typically do so for quite different reasons than many chiropractors. Despite the widespread use of SMT, it is primarily associated with chiropractic in the public imagination, and chiropractic is certainly defined by it: “The chiropractic profession, which began with a founding father in 1895, is identified primarily by its use of manipulation” (Homola).
- “Joint mobilization” is the formal term for a type of passive movement of a skeletal joint. When applied to the spine, it is known as spinal mobilization.
- This is a complex issue. I deal with it in the free article, What Happened To My Barber?, and in more detail in the neck pain tutorial. An excellent overview of medical concerns about SMT for the neck can be found in this statement of concern by a group of Canadian neurologists.
- Kanodia AK, Legedza ATR, Davis RB, Eisenberg DM, Phillips RS. Perceived benefit of Complementary and Alternative Medicine (CAM) for back pain: a national survey. J Am Board Fam Med. 2010 May-Jun;23(3):354–62. PubMed 20453181 ❐ PainSci Bibliography 54984 ❐
- ScienceBasedMedicine.org [Internet]. Homola S. Chiropractic Vertebral Subluxations: Science vs. Pseudoscience; 2010 Sep [cited 16 Feb 13]. PainSci Bibliography 54979 ❐
- Fernández-de-Las-Peñas writes “There are few published randomized controlled trials analyzing the effectiveness of spinal manipulation and/or mobilization … in the last decade.” Bronfort: “There have been few high-quality trials distinguishing between acute and chronic patients, and most are limited to shorter-term follow-up.” The 2006 Cochrane review of SMT found only 39 experiments to analyze, and most of those had small sample sizes.
- Ernst E, Posadzki P. An independent review of NCCIH-funded studies of chiropractic. Clin Rheumatol. 2011 Jan. PubMed 21207089 ❐
Dr. Edzard Ernst is a highly qualified critic of sloppy researchers in alternative medicine. In this review of The National Center for Complementary and Integrative Health (NCCIH) studies of chiropractic therapy, he finds that “their quality was frequently questionable. Several randomized controlled trials failed to report adverse effects and the majority was not described in sufficient detail to allow replication.” But if NCCIH cannot produce the best quality studies of alternative medicine, who can? No organization has ever been better funded (or motivated) to validate alternative therapies.
Ernst concludes: “It seems questionable whether such research is worthwhile.”
- Hadler NM, Curtis P, Gillings DB, Stinnett S. A benefit of spinal manipulation as adjunctive therapy for acute low back pain: a stratified controlled trial. Spine. 1987;12:702–6. PubMed 2961085 ❐
From the abstract, “In the first week following [spinal] manipulation, these patients improved to a greater degree ... and more rapidly ....”
- Hoehler FK, Tobis JS, Beurger AA. Spinal manipulation for low back pain. JAMA. 1981;245:1835–8. PubMed 6453240 ❐
This study supports the usefulness of spinal adjustment for acute pain only. From the abstract: “Patients who received [spinal] manipulative treatment were much more likely to report immediate relief after the first treatment.” However, “at discharge there was no significant difference between the two groups because both showed substantial improvement.”
- Vernon H, Humphreys BK. Chronic mechanical neck pain in adults treated by manual therapy: a systematic review of change scores in randomized controlled trials of a single session. Journal of Manipulative & Physiological Therapeutics. 2008;16(2):E42–52. PubMed 19119388 ❐ PainSci Bibliography 56158 ❐
“There is moderate-to-high quality evidence that immediate clinically important improvements are obtained from a single session of spinal manipulation. The evidence for mobilization is less substantial, with fewer studies reporting smaller immediate changes.”
- Swenson R, Haldeman S. Spinal manipulative therapy for low back pain. Journal of the American Academy of Orthopaedic Surgeons. 2003 Jul-Aug;11(4):228–37. PubMed 12889861 ❐
From the abstract: “Most reviews of these trials indicate that spinal manipulative therapy provides some short-term benefit to patients, especially with acute low back pain.”
- Zaproudina N, Hänninen OOP, Airaksinen O. Effectiveness of traditional bone setting in chronic neck pain: randomized clinical trial. Journal of Manipulative & Physiological Therapeutics. 2007;30(6):432–7. PubMed 17693333 ❐
This seems to a straightforward “thumbs up” study showing that “traditional bone setting” (chiropractic adjustment, spinal manipulative therapy) has a good effect on chronic neck pain. I admit to being skeptical for no clear reasons (meaning, I see no obvious flaws with the paper). The conclusions seem too strong, too much at odds with a lot of other very mixed evidence on this topic. I can’t reject it outright, but I suspect the risk of researcher bias is high, and a careful reading of the whole paper would probably turn up concerns.
- Senna MK, Machaly SA. Does maintained Spinal manipulation therapy for chronic non-specific low back pain result in better long term outcome? Spine (Phila Pa 1976). 2011 Jan. PubMed 21245790 ❐
- Cherkin DC, Deyo RA, Battie M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med. 1998;339:1021–9. PainSci Bibliography 57062 ❐
- Bogduk N. Spinal manipulation for neck pain does not work. J Pain. 2003;4(8):427–428. I take Bogduk’s opinion very seriously, as he is one of a small group of elite pain scientists in the world today whose opinions are relentlessly well-informed and sensible (see Jackson for an intriguing example, or his short and readable editorial, “What’s in a name? The labelling of back pain”). In spite of everything I know myself, when I encounter an opinion from someone like Dr. Bogduk, I’m inclined to just go with “what he said.” Of course, guess I can’t quite give up thinking for myself … 😃 But seriously, this guy is smart, and if he says it doesn’t work, he’s got good reasons for it.
- Bronfort G, Evans R, Anderson AV, et al. Spinal manipulation, medication, or home exercise with advice for acute and subacute neck pain: a randomized trial. Ann Intern Med. 2012 Jan;156(1 Pt 1):1–10. PubMed 22213489 ❐
This reasonably well-designed, big, 12-week NCCIH trial of spinal manipulative therapy (SMT) for neck pain concludes with an important disclaimer: although SMT “won” and chiropractors cite this study as evidence that adjustment works, the authors acknowledge that just “a few instructional sessions of home exercise with advice resulted in similar outcomes at most time points.” And so SMT is damned, damned, damned with (extremely) faint praise yet again, as it always is, every time it gets studied: it costs vastly more and performs barely better than sending someone home to do a few simple exercises! Now that hurts.
- Jüni P, Battaglia M, Nüesch E, et al. A randomised controlled trial of spinal manipulative therapy in acute low back pain. Ann Rheum Dis. 2009 Sep;68(9):1420–7. PubMed 18775942 ❐
- There are two broad types of plausible mechanisms: trigger treating, or reflex effects on migraine biology. It’s possible that migraines, although quite neuro/bio in character, are triggered by fairly ho-hum spinal irritation — “cervicogenic” like many tension headaches probably are. Treat the trigger, fewer migraines. And it’s conceivable that there’s some complex neuro/sensory relationship between migraine and the stimulation of neck joints.
- Chaibi A, Benth JŠ, Tuchin PJ, Russell MB. Chiropractic spinal manipulative therapy for migraine: a three-armed, single-blinded, placebo, randomized controlled trial. Eur J Neurol. 2016 Oct. PubMed 27696633 ❐
- Hurwitz EL, Aker PD, Adams AH, Meeker WC, Shekelle PG. Manipulation and mobilization of the cervical spine: A systematic review of the literature. Spine. 1996 Aug 1;21(15):1746–1759. PubMed 8855459 ❐
- Bronfort G, Haas M, Evans RL, Bouter LM. Efficacy of spinal manipulation and mobilization for low back pain and neck pain: a systematic review and best evidence synthesis. Spine. 2004;4(3):335–356.
The complexity of this experiment’s results must be seen to be believed! Here’s a sampling:
There is limited to moderate evidence that SMT is better than physical therapy and home back exercise in both the short and long term. There is limited evidence that SMT is superior to sham SMT in the short term and superior to chemonucleolysis for disc herniation in the short term. However, there is also limited evidence that mobilization is inferior to back exercise after disc herniation surgery. Mix of acute and chronic low back pain: SMT/mobilization provides either similar or better pain outcomes in the short and long term when compared with placebo and with other treatments, such as McKenzie therapy, medical care, management by physical therapists, soft tissue treatment and back school. Acute neck pain: There are few studies, and the evidence is currently inconclusive.
Uh, yeah. That really clears things up! I’m not saying this is a bad review — I’m just saying it’s mired in the poor quality of the body of literature, and the complexity of the problem.
- Gross AR, Hoving JL, Haines TA, et al. A Cochrane review of manipulation and mobilization for mechanical neck disorders. Spine. 2004;29(14):1541–1548. The review does report evidence that neck adjustments may work when combined with exercises, but that doesn’t exactly flatter SMT. If it doesn’t have a benefit on its own, then any benefit when combined with exercise probably has little or nothing to do with the SMT itself.
- Lenssinck MLB, Damen L, Verhagen AP, et al. The effectiveness of physiotherapy and manipulation in patients with tension-type headache: a systematic review. Pain. 2004 Dec;112(3):381–388. PubMed 15561394 ❐ PainSci Bibliography 56057 ❐
- Fernández-de-Las-Peñas C, Alonso-Blanco C, San-Roman J, Miangolarra-Page JC. Methodological quality of randomized controlled trials of spinal manipulation and mobilization in tension-type headache, migraine, and cervicogenic headache. JOSPT Open. 2006;36(3):160–169.
- Posadzki P, Ernst E. Spinal manipulations for cervicogenic headaches: a systematic review of randomized clinical trials. Headache. 2011;51(7):1132–9. PubMed 21649656 ❐
- Rubinstein SM, Terwee CB, Assendelft WJJ, de Boer MR, van Tulder MW. Spinal manipulative therapy for acute low-back pain. Cochrane Database Syst Rev. 2012;9:CD008880. PubMed 22972127 ❐ PainSci Bibliography 54694 ❐
The Cochrane Collaboration publishes comprehensive reviews of what the science can tell us so far about medical treatments, and they promote and facilitate evidence-based medicine. Although not perfect — in recent years their quality control has slipped a little, in my opinion — they still generally produce the most authoritative reviews available of pain and injury science.
Now, if only they weren’t so infamous for never drawing any conclusion other than “more research is needed.”
- Rubinstein et al. “identified 26 randomised controlled trials (represented by 6070 participants) that assessed the effects of SMT in patients with chronic low-back pain. Treatment was delivered by a variety of practitioners, including chiropractors, manual therapists and osteopaths. Only nine trials were considered to have a low risk of bias. In other words, results in which we could put some confidence.”
- Cashin AG, Furlong BM, Kamper SJ, et al. Analgesic effects of non-surgical and non-interventional treatments for low back pain: a systematic review and meta-analysis of placebo-controlled randomised trials. BMJ Evid Based Med. 2025 Mar:bmjebm–2024–112974. PubMed 40101974 ❐
This big new review of common non-medical back pain treatments is bad news. It’s a sequel to a 2009 version, and, like any good sequel, it delivers more of what made the first one good: the most rigorous science, a meticulous and sensible review of placebo-controlled trials only, a high bar to clear. And it seems to be just about as discouraging as it could possibly be. But tilt your head like a curious doggo for a different view, and maybe it’s not as bad as it seems? Here’s some good news about the bad news:
- Given the amount of garbage out there, getting some relief from 1 in 10 treatments doesn’t actually strike me as being all that bad. And the winners are: NSAIDs, exercise, spinal manipulation, taping, antidepressants, and TPRV1 antagonists (like capsaicin in spicy rubs).
- There’s a lot of “garbage in, garbage out” here, and it mostly confirms that we have inadequate rather than negative evidence. The review had such high standards that there weren't enough high quality studies for many conclusions. (And yet consumers are spending billions of bucks on those not-clinically-proven treatments. 😬) But the silver lining here is that there could be good treatments that simply haven’t been tested enough yet.
And now the bad news about the bad news. Unfortunately, if tilt your head the other way, the bad news looks even worse than it seemed at first. Quite a bit worse.
- The lucky handful of treatments that are being touted as effective here are offering really minor relief, all very damned-with-faint-praise.
- And some of those small benefits are likely illusory — evidence that registered as a thumbs up in this review, but likely won’t stand up to scrutiny/replication.
- And the reems of “inconclusive” evidence here? Most of that is extremely unlikely to ever get conclusive.
The bottom line is clear: back pain is largely immune to treatment. See also Wang et al., another 2025 review focusing on interventional medicine — with similarly high standards, and disappointing results.
- This view is supported explicitly with regards to SMT and every other low back pain treatment by Cashin et al.
- He was writing about the original 2009 version of the same review, see Machado et al. The 2025 version has very similar conclusions about SMT.
- Bronfort G, Haas M, Evans R, Leininger B, Triano J. Effectiveness of manual therapies: the UK evidence report. Chiropr Osteopat. 2010;18:3. PubMed 20184717 ❐ PainSci Bibliography 55168 ❐
This review of manual therapies focusses on spinal manipulative therapy and massage therapy for low back and neck pain, with predictably mixed results ranging from inconclusive to underwhelming to suspiciously positive. Both are judged “effective” for some conditions but not impressively so, and mostly no different from other therapies that are notoriously unimpressive. For instance, the authors write that SMT is effective but “similar in effect to other commonly used efficacious therapies such as usual care, exercise, or back school.” How nice for SMT that it can hold its own against “back school.”
The “effective” conclusions about SMT for various conditions seems strange to me, because the actual data is consistent with the much more negative conclusions of other major reviews, most Rubinstein et al. I suspect these authors are keen to say nice things about SMT.
- Homola S. Inside chiropractic: a patient’s guide. Prometheus Books; 1999. p150
- Walker BF, Koppenhaver SL, Stomski NJ, Hebert JJ. Interrater Reliability of Motion Palpation in the Thoracic Spine. Evidence-Based Complementary and Alternative Medicine. 2015;2015:6. PubMed 26170883 ❐ PainSci Bibliography 54242 ❐
Two examiners, using standard methods of motion palpation of the thoracic spine, could not agree well on the location of joint stiffness or pain in a couple dozen patients. Simplifying the diagnostic challenge did not improve matters. Therefore, “The results for interrater reliability were poor for motion restriction and pain.” This does not bode well for manual therapists who use motion palpation to identify patients who might benefit from spinal manipulation.
The study only used two examiners, which might be a serious flaw. More raters would certainly be better. Nevertheless, even a small data sample can produce meaningful information if the effect size is robust enough (any two people can agree on, say, fire hydrant locations; see It's the effect size, stupid), which it probably is here. Even just two examiners should generate more similar results, unless someone is grossly incompetent. If they differ greatly, more examiners probably isn’t going to change that.
- Aguirrebeña IL, Newham D, Critchley DJ. Mechanism of Action of Spinal Mobilizations: A Systematic Review. Spine (Phila Pa 1976). 2016 Jan;41(2):159–72. PubMed 26751060 ❐
- Wong AYL, Parent EC, Dhillon SS, Prasad N, Kawchuk GN. Do participants with low back pain who respond to spinal manipulative therapy differ biomechanically from nonresponders, untreated controls or asymptomatic controls? Spine (Phila Pa 1976). 2015 Sep;40(17):1329–37. PubMed 26020851 ❐
- Carnes D, Mars TS, Mullinger B, Froud R, Underwood M. Adverse events and manual therapy: a systematic review. Man Ther. 2010 Aug;15(4):355–63. PubMed 20097115 ❐
The sound bite in this study is that 20-40% of all manual therapy treatments — massage, chiropractic, physiotherapy — will cause some kind of unpleasantness, side effect or “adverse event” in medicalspeak.
In a word: yikes!
Perspective cuts both ways here. On the one hand, it’s not as bad as it sounds: these “events” are minor and moderate in severity; only 1 or 2 per thousand visits causes a serious problem; and drugs are actually relatively worse. That is, you are modestly more likely to have an “adverse event” if you are given a pill. This just refers to typical side effects, such as ibuprofen’s tendency to cause indigestion.
But when you take a pill, the side effect is usually unrelated to the problem (i.e. it doesn’t make the problem you’re treating worse), you are generally trading those side effects for some pretty clear benefits, and it’s usually cheap. In manual therapy, most adverse events are backfires — that is, you go for a neck adjustment at the chiropractor, and you come out with more neck pain instead of less. Other data shows this is 25% more likely than if you did nothing at all (see Carlesso). And you pay through the nose for this! Manual therapy is much more expensive than most drug therapy.
Manual therapists routinely claim that their services are much safer and more effective than drug therapies. Yet this data pretty clearly shows that the difference is really not great. Depending on how you look at it, drugs are only a little worse in some ways, or maybe a little better in other ways. But no matter how you slice it, 20-40% is a pretty unpleasant rate of harm — especially at $60–120/hour!
- Carlesso LC, Gross AR, Santaguida PL, et al. Adverse events associated with the use of cervical manipulation and mobilization for the treatment of neck pain in adults: A systematic review. Man Ther. 2010 Oct;15(5):434–444. PubMed 20227325 ❐
- I’m not sure I agree that a statistically insignificant number constitutes “strong evidence” of the absence of harms so much as just generally low confidence in the results. There are just too many ways the data could be missing the truth entirely here (see the other note about this, about statistical dragons). And Carlesso acknowledges this in the paper as well (practically in the next sentence: “However, the limitations of the Strunk study and the low GRADE rating remain, affecting confidence in the estimate.”) She’s also authored three other papers about how difficult it is to study this stuff! See 2010, 2011, 2013.
- See Arnold 2006, Kerry 2009, Maruyama 2012. This is the stuff of hypochondriac nightmares, because it’s a serious problem that can almost perfectly mimic an ordinary, common one. But it’s not a perfect mimic: the pain is usually dramatically bad and weird, and there are some other common clues that something serious has happened, such as a throbbing or constrictive pain quality. For more information, see When to Worry About Neck Pain … and when not to!.
- Spinal cracks and other chiropractic manipulations — like traction — are downright frightening to a significant portion of the population. Hardly a day goes by without a client telling me they are “freaked out” by the idea of being cracked, and many people with back pain are also uneasy about traction (another common chiropractic treatment method).
- Chiropractors do this because many of them either subscribe to a belief that the whole spine is greatly affected by the condition of the cervical joints, particularly the top one. So chiropractors may well throw in a little neck adjusting, with varying degrees of conviction about its importance. But the idea is as controversial and questionable as any idea in all of chiropractic.
- Chiropractors have an ethical duty to tell their patients about risks: A survey suggests fewer than half of chiropractors always discuss the risks of cervical manipulation with patients. The Guardian. July 12, 2011. Accessed July 14, 2011.
- This may be have been misunderstood and misreported. It’s not clear exactly how Mr. Davidson’s neck was injured, except that it followed overzealous treatment.
“Fearmongering” is the deliberate and unjustified arousal of public concern, usually to serve an ulterior motive. I am often accused of fearmongering because I express concerns about potentially dangerous treatments. I plead “not guilty”: I aim for nuance and balance whenever I write anything that might spook anyone, and I make a point of weighing risks and benefits. Raising awareness of legitimate risks is not fearmongering — it’s valuable public health education. It would be fearmongering if I was making an issue out of nothing, but it’s never about “nothing.”
“You’re not paranoid if they’re really after you,” and it’s not fearmongering if concern is rational.
In the case of spinal manipulative therapy, for instance, we’re talking about a nearly mainstream treatment, provided by countless physical therapists as well as all chiropractors, received by millions of patients who have little or no awareness of the potential hazards, risks, or rewards … and the hazards include maiming and death, even if the risk is low. That’s a mountain, not a molehill!
- Swinkels RA, Oostendorp RA. Upper cervical instability: fact or fiction? J Manipulative Physiol Ther. 1996 Mar-Apr;19(3):185–194. PubMed 8728462 ❐
This 1996 paper found that “there is no correlation between the measure of hypermobility and the presence of clinical symptoms. Also, the validity of the upper-cervical stability tests is questionable.”
- Here be statistical dragons. At first glance, the lack of a smoking gun might seem to indicate that such serious harms are unlikely — wouldn’t a problem show up if it were serious? And that is exactly how I would spin my analysis if I were a chiropractor! But that signal would show up only if the research were actually designed to detect it in the first place. These authors were simply going through data from many small studies of neck adjustment, in which some rotten reactions were noted, while many other studies were disqualified for not tracking harms at all and — this is interesting — for “notable ascertainment bias.” Translation: some of the studies were written by authors likely to ignore, deny and minimize evidence of harm
In the end, only 32 studies could be analyzed. So it remains entirely possible that the phenomenon of severe neck injury from SMT is real but rare, and simply didn’t occur in any of those 32 studies, or wasn’t observed and tracked. Similarly, you could analyze dozens of studies of the health effects of hiking, but probably none of them would have data about bear attacks — yet bears do attack hikers!
- National Chiropractic Mutual Insurance Company [Internet]. Triano JJ, Kawchuk G, Gudavalli MR, et al. Current Concepts: Spinal Manipulation and Cervical Arterial Incidents 2005; 2005 [cited 23 May 15]. PainSci Bibliography 56048 ❐
Like the infamous Cassidy et al. paper, this document is often cited by chiropractors when they are trying to allay fears about serious complications of cervical adjustment. (The document isn’t readily available online anymore, but a PDF might crop up in a Google search.) Although the athors make an effort to be scientifically sound, they obviously have a conflict of interest, stating outright that they wish to make the case that cervical manipulation is not dangerous. Consider this excerpt from the executive summary: “In addition, as part of our ongoing commitment to giving NCMIC doctors the best defense possible should the need arise, we are providing this information to our network of chiropractic defense attorneys. We expect this latest research will be an important tool for our defense attorneys to use in presenting the most contemporary findings from recent research and to help overcome common biases held by judges and juries.” So, whatever else this document might be, it’s not objective. Note: Allan Terrett originally wrote a monograph for the National Chiropractic Mutual Insurance Company in 2001. The 2005 version is not written by him, but by Triano and Kawchuk “with grateful appreciation” to him.
- Cassidy JD, Boyle E, Côté P, et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study. Spine. 2008 Feb;33(4 Suppl):S176–83. PubMed 18204390 ❐
Since its publication, “the Cassidy paper” has been the defensive citation used by chiropractors to respond to accusations that neck adjustments involve a risk of stroke, and therefore should not be conducted without proven benefit and informed consent. The abstract seems to strongly exonerate chiropractors: “We found no evidence of excess risk of VBA stroke associated with chiropractic care compared to primary care.”
“But abstracts are like movie trailers,” as Dr. Mark Crislip wrote. “They give a flavor of the movie, but often leave out many important plot devices and characters. … If you were to read this article in its entirety, you would not be so sanguine about the safety of chiropractic.” He goes on to explain exactly why in one of the earliest popular posts on ScienceBasedMedicine.org, Chiropractic and Stroke: Evaluation of One Paper.
What chiropractors take from the paper is that the strokes that follow cervical spinal manipulation were already in progress, causing the symptoms that inspired the appointment. That is possible, but it is only one possibility, and the paper’s abstract emphasizes this hypothesis like it’s a conclusion (and most people stop reading when they are told what they want to hear). That hypothesis is not supported by the data Cassidy et al. pulled together (which has some key flaws). And there are other ways to explain the data. Dr. Crislip’s conclusion “from reading the paper in its entirety, rather than the abstract”:
A population that should not have a stroke, the young, has a marked increase association with stroke 24 hours after visiting a chiropractor and that given the rarity of a vertebral artery dissection as a cause of stroke in the elderly, the elderly is not a group that one could easily find an increase in stroke after chiropractor visit.
- Di Fabio RP. Manipulation of the cervical spine: risks and benefits. Phys Ther. 1999;79(1):50–65. PainSci Bibliography 56049 ❐
- Hurwitz EL, Morgenstern H, Vassilaki M, Chiang LM. Frequency and clinical predictors of adverse reactions to chiropractic care in the UCLA neck pain study. Spine. 2005;30(13):1477–1484. PubMed 15990659 ❐
- Neck911.com [Internet]. Statement of Concern to the Canadian Public from Canadian Neurologists Regarding the Debilitating and Fatal Damage Manipulation of the Neck May Cause to the Nervous System; 2009 [cited 09 Jul 19]. PainSci Bibliography 55499 ❐
We Canadian neurologists hereby express our strong concern and thereby issue this warning to Canadians. The public must be made aware that the neurological damage that can result subsequent to upper neck manipulation can be debilitating and fatal.
We make the following recommendations for the attention of the Canadian public, the practitioners of manipulation, the medical community, the provincial Ministries of Health and the health care professional regulatory bodies.
Our concerns are significant. Stroke and death due to neck manipulation has been reported in the scientific literature for over 50 years. New deaths, in the past few years, have been reported to the Canadian Stroke Consortium. The Canadian Stroke Consortium recently published a major prospective study. The latest data from the Stroke Consortium indicates that “more than 100 cases of dissection per year are associated with neck manipulation.” The resulting stroke and debilitation from such a large number is very significant.
A recent study by the Institute of Clinical Evaluative Sciences (ICES Ontario) indicates that patients with posterior circulation strokes under the age of 45 are 5 times more likely than controls to have visited a chiropractor within one week of the event.
- Sciencebasedmedicine.org [Internet]. Homola S. Opposing Chiropractic: Persecution or Justified Criticism? – Science-Based Medicine; 2015 Feb 1 [cited 19 Oct 24]. PainSci Bibliography 52726 ❐
- The dominant theory of joint popping depends on the concept of “cavitation” — the rapid formation and explosive collapse of bubbles in a liquid due to pressure changes. This is widely accepted, but it doesn’t explain some features of joint popping, most notably the “recharge” phenomenon, wherein joints that supposedly cavitated nicely just a moment ago need to be left alone for seconds, minutes or hours before they can cavitate again. Also, the cavitation hypothesis does not explain why there is such dramatic variation between individuals, or why cracking seems to be extremely prevalent in the aftermath of trauma. It is almost certainly only partially correct.
- Rare cracks, in joints that don’t usual crack — like the sternum — are often more uncomfortable. Joint pops do involve movement at the edge of normal range of motion. Where there’s sudden, strong movement, there’s potential for pain. It could indicate that the joint itself is actually irritated/vulnerable — injured or arthritic, say — but definitely not necessarily. The forces involved in the pop can be intense, and the sudden change in the state of the joint can be dramatic. I bet those can hurt much like a toe stub hurts — like any sudden, strong stimulation of healthy tissue.
- Aguirrebeña 2016, op. cit.
- Regardless of how you feel about being “adjusted”, the therapeutic “message” of a joint wiggle or crack can really only be repeated, not significantly modulated: a crack is a crack is a crack, and one traction or joint wiggle is pretty much like another. There is only so much novel sensory input these techniques can provide. If the body doesn’t “get it” after a few tries on a few different days, it’s probably not going to “get it” later. This may explains why the effectiveness of SMT treatment tends to lessen over time (a well-known characteristic of chiropractic therapy). By contrast, I have always been grateful for the large number of ways that massage therapy can be used to manipulate tissues in the low back, creating a rich variety of fresh sensory experiences for clients for an hour at a time, week after week. This is certainly one of the advantages of massage therapy as a therapy.
- Homola S. Finding a Good Chiropractor. Archives of Family Medicine. 1998;7(1):20–23. PainSci Bibliography 56032 ❐
- Tseng YL, Wang WTJ, Chen WY, et al. Predictors for the immediate responders to cervical manipulation in patients with neck pain. Man Ther. 2006;11(4):306–315.
From the abstract: “The presence of four or more of these predictors increased the probability of success with manipulation to 89%. We concluded that using favourable predictors to identify treatment responders before administering cervical manipulations could significantly increase the probabilities of a successful treatment.”
- On the one hand, according to this study, SMT is likely to be more effective for mild neck pain (and that’s a pretty reasonable idea). On the other hand, the milder the problem, the less you should want to take the risks of SMT for the neck! It’s a messy decision, no doubt about it.
- A chiropractor who recommends anything more than a dozen appointments for back pain is probably pushing the limits. Remember that most cases of back pain resolve on their own within three weeks! However, only a dozen treatments is actually on the low end of what I’ve heard about chiropractic treatment recommendations. For instance, one of my massage therapy clients was told by a chiropractor that he could only get relief from back pain if he made a commitment to two years of weekly appointments — at a cost of at least $2000! Another client faced down a chiropractor who was demanding that he sign a contract for a “two-year, $7,000 treatment plan.” Such prescriptions constitute a serious conflict of interest. Health care professionals are ethically obliged to be conservative in their treatment recommendations. Clients must be informed and presented with a range of options and allowed to make their choices with an absolute minimum of interference — not threatened with the consequences of failure to adhere to the most expensive therapeutic option available! Especially when the condition may be aggravated by the perception that it is problematic! These chiropractors were way out of line, and the chiropractic profession must take collective responsibility for such blatantly excessive treatment prescriptions.
- Cleland JA, Glynn P, Whitman JM, et al. Short-term effects of thrust versus nonthrust mobilization/manipulation directed at the thoracic spine in patients with neck pain: a randomized clinical trial. Phys Ther. 2007;87(4):431–440.