Icing for Injuries, Tendinitis, and Inflammation
Become a cryotherapy master
Not sure when to use ice or heat? Get a quick overview in Ice versus Heat for Pain and Injury, or a detailed look at why you should (almost) never ice low back pain. In general, heating is better for almost anything that isn’t a fresh injury.

Icing — “cryotherapy” for therapy geeks — is an essential injury management skill. Everyone should understand icing the same way everyone knows how to put on a Band-Aid, because it is a cheap, effective, drugless method for taking the edge off the pain of fresh injuries. Safe application of ice to your skin can relieve symptoms from sprains, strains, bruises, and tendinitis — virtually any situation in which superficial tissues are inflamed by recent trauma or pathology. Even brief pain relief can be precious.
There are also hazards and complications to icing that anyone with chronic pain should know. This article is full of tips and insights about icing that will take you way beyond the basics.
For instance, icing might also assist recovery from repetitive strain injuries like tendinitis or iliotibial band syndrome, but that is much more speculative. Doubts about cryotherapy as a healing stimulant are reasonable, and have been spun into excessive skepticism about icing in general. This guide starts out by pushing back against that.
And what about cryotherapy for your whole body? Cold immersion therapy is a completely different bucket of ice cubes. For the science of shivery showers, ice baths, and cold-water swimming, see Whole Body Cryotherapy for Pain. And there are several other articles on the site about therapeutic temporary tinkering:
Isn’t inflammation healthy? A brief response to a popular argument against icing
It has been fashionable lately to scoff at icing as a treatment because it allegedly interferes with natural healing. The physician who first proposed the well-known RICE rehab protocol back in 1978 has actually recanted the I-for-ice part, declaring in 2015 that “icing delays recovery,” and his opinion is now cited almost everywhere this topic is discussed. (He doesn’t seem to have written anything else about it since then.)
Dr. Mirkin’s article is brief and only tackles the claim that ice promotes healing. That is a popular idea, and it’s an important one to think critically about, but there’s much more to the topic of icing, and most icing is not done to “promote healing.” The much more common goal is just to control pain cheaply and safely, and that is not a baby I want to throw out with the bathwater: pain relief can be precious!
Ironically, after devoting a few hundred words to discouraging people from icing, Dr. Mirkin actually concludes his article by recommending small doses of early icing for pain relief — which most people citing the article don’t seem to have noticed.1
Since applying ice to an injury has been shown to reduce pain, it is acceptable to cool an injured part for short periods soon after the injury occurs. You could apply the ice for up to 10 minutes, remove it for 20 minutes, and repeat the 10 minute application once or twice.
The question of whether ice promotes or impedes healing is mostly just irrelevant to the value of ice for temporary pain control. But there are at least two problems with the argument that icing actually impedes healing:
- It’s entirely speculative2 and actually contradicted by the clinical evidence, which shows that icing appears to have no effect on recovery at all, good or bad. What few studies we have of this just show no difference.3
- The inflammation associated with fresh injuries is indeed mostly biology business as usual, a normal “side effect” of healing. But not all of it! Not everything “normal” in biology is wise and good and never needs to be controlled or treated.4 Diarrhea is natural, too, but it can get out of hand. Inflammation can too, and we know that at least some of it is actually “bad” biology, an evolution-powered error.5
What ice is for
Ice is for injuries. We hope. Science, alas, is not quite so sure.67
If it works, it is useful mainly where tissue are damaged and/or “inflamed.” (Although some things that we think of as “inflamed” may not actually be inflamed. And vice versa! More about this below.)
Icing is primarily an analgesic — a pain-reliever — and not an actual treatment. That is, it doesn’t “fix” anything. Use it like you use ibuprofen. It may help to resolve chronic problems (much more about this below), but it’s mostly intended to simply numb painfully inflamed or other hurting tissues.
The most commonly iced acute injuries are fresh injuries — ligament sprains, muscle strains, and severe bruises. (When the skin is broken, things get a little trickier.) And what’s a “fresh” injury? Any time tissue has been physically damaged, it will be inflamed for a few days, give or take, depending on the seriousness of the injury. If superficial tissue is sensitive to touch, if the skin is hot and red, if there is swelling, these are all signs that your injury is still fresh, and should definitely not be heated. Heat will increase the circulation and significantly facilitate the immune system activity.
Ice is also often helpful with chronic overuse or tissue fatigue injuries like carpal tunnel syndrome, tennis elbow, supraspinatus or Achilles tendinitis,8 iliotibial band syndrome, patellofemoral syndrome, shin splints, and plantar fasciitis. There are others, of course, but these are the most common.
Ice may also be useful for garden-variety “wear and tear” arthritis, and sometimes the nasty inflammatory arthritides (rheumatoid arthritis, ankylosing spondylitis).
What ice is not for (mostly back pain)
Ice can aggravate muscle pain, which is routinely mistaken for an “iceable” injury, especially in the low back.
Back pain is rarely caused by an injury — that is, the pain is rarely caused by inflammation which might be helped by ice. Even in cases where inflammation is present, it is mostly going to be deep in the back under a thick layer of insulating muscle where ice cannot “reach” it.
Meanwhile, back pain almost always does involve muscle pain in the form of muscular trigger points (muscle knots)9 — a small patch of acutely sensitive soft tissue, a poorly understood little patch of sensory misery10 — which are more likely to be aggravated by ice and helped by heat. And so most people with back pain seem to prefer heat, and some have negative reactions to ice. (The situation is similar for neck pain.)
Although experiments have shown that both ice and heat are modestly and equally helpful for low back and neck pain,11 that evidence isn’t exactly bulletproof,12 and here are some good reasons to err on the side of heat in any case.13
But the main reason is that ice is more likely to aggravate the trigger points that are so common in neck and back pain. I recommend that ice should only be used in back and neck pain cases where …
- you clearly prefer it (for whatever reason)
- there is definitely a fresh injury (a clear mechanism of injury, and obvious inflammation: heat, swelling, redness)
And those cases are surprisingly rare, because the back is much tougher and immune to injury than people think, and also much more prone to painful trigger point activity than most people realize. Indeed, many garden variety aches and pains, especially in younger people, are probably caused not by arthritis and injury as people tend to assume, but by ordinary muscle pain — which tends to be irritated by ice and soothed by heat.
In case of inflammation, apply ice
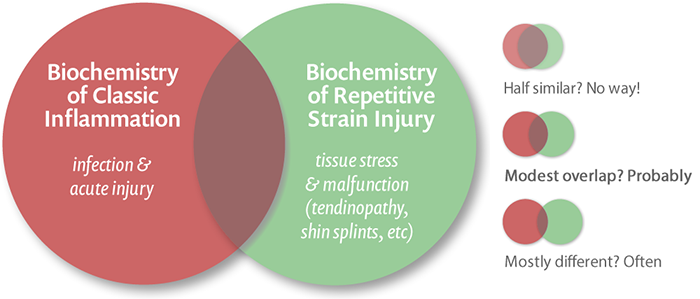
Icing is traditionally used wherever people suspect inflammation. However, that includes at least three common and surprisingly different biological situations … and different reasons for icing, or not icing.
- true inflammation, where you want an immune system reaction (lacerations)
- “sterile” injury, with no chance of infection and an unnecessary/excessive immune response (bruises, muscle and ligament tears)
- connective tissue degeneration, with little or no acute inflammation (repetitive strain injuries)
The third one in particular is a bit of a revelation for a lot of people. More below.
Classic inflammation is pretty well understood, and it’s mainly an immune system reaction. When tissue is damaged, the body responds with a complex array of chemical and neurological changes collectively known as inflammation. For instance, the capillaries widen in a big way to bring extra oxygen and nutrients to the area. They also “loosen,” becoming more permeable, to give immune system cells easy access to the injury.14 Most of the pain and discomfort of inflammation is due to this immune system activity.
If the skin is broken (septic injury), there is a risk of infection, and the immune system reaction is essential — a pure physiological goodness. Inflammation in that context is a machine finely-tuned by evolution to optimize recovery, just as a fever is an effective physiological process for fighting infection (indeed, they are closely related processes). Strictly speaking, if you to want to heal well, don’t interfere with inflammation! For broken-skin wounds, use ice only a little to “take the edge off.” And of course it’s best to use it in a sterile way, so that you don’t add to the infection risk!
If the skin isn’t broken (sterile injury), things are really quite different! In this context, inflammation is an absurd overreaction that causes collateral damage and excessive pain for no good reason at all — a genuine glitch in biology,
The important point here is that inflammation of sterile injuries is truly worse than it needs to be — and it’s quite reasonable to try to suppress it with ice, and anti-inflammatory medications like ibuprofen or Voltaren. Bet you didn’t know that. Very few people do — this is based on surprisingly new science about that glitch! This treatment logic was unavailable until quite recently.
Of course, the immune system reaction is not the only reason injuries hurt. Damaged cells put out many kinds of distress signals. As with most biological processes, our comfort is not really a priority. In fact, quite the opposite — injury and inflammation have partly evolved to be painful. Cavemen didn’t have ibuprofen and ice, nor did they have the benefit of understanding inflammatory chemistry. In the big picture, super painful inflammation was good for our species: victims were encouraged to stay relatively still while inflammation ran its course like a fever!
But for modern humans, inflammation is … well, it’s overkill. We can afford to “turn it down.” We can ignore the warning of the inflammation, to a point, and especially if we’re confident that we don’t really need an immune system reaction (for a sterile injury). Ice can only turn it down so much anyway, so there’s no risk of missing the pain alarm entirely!
In theory, cold slows metabolic activity, numbs nerve endings, constricts capillaries. It limits and controls inflammation. It makes it hurt less. It helps us get through the day. And that’s an especially good thing for the common sterile injuries, where the inflammation is largely pointless.
There’s yet another kind of “inflammation”…
Chronic “inflammation”? Not so much, actually
Do you have a chronic overuse injury? Shin splints for two years? Plantar fasciitis for five? Then you are probably thinking, “Inflammation is not @#!!$% a valuable warning signal!” It’s more like an annoying car alarm.
Right you are. Sorta.
What’s going on in a repetitive strain injury like runner’s knee or tennis elbow or Achilles tendinitis is not really inflammation, per se, except perhaps in the earliest stages,16 but erratically painful degeneration1718 — tissue rot, which has more in common with arthritis than inflammation. The chemistry of these situations is very different than classic acute inflammation, and involves little immune system activity. This has led the popular idea that tendinitises are not inflamed, and many a smug phsyiotherapist (and my own past self) has “mansplained” that fun fact.
To the extent that it’s true, the most obvious implication of this is that medicines intended to suppress immune system activity — the anti-inflammatories — are probably not going to work well if there’s not much activity to suppress. And indeed they don’t seem to.
But of course it’s all more nuanced than that.
The idea that RSIs aren’t inflamed is based mainly on the absence of classic, acute inflammation: the clinical and pathological signs of a vigorous immune response. But there’s almost certainly more to inflammation than redness and white blood cells swarming the tissue like police trying to control a riot.19
So
But that is starting to change. Just because you can’t see it doesn’t mean it’s not there, or wasn’t there earlier. Maybe you just have to look better. And Dakin et al. looked better in 2017. They looked for more subtle signs of inflammation in Achilles tendinitis … and found them, seemingly without much ambiguity. Their paper in British Journal of Sports Medicine reported that painful and ruptured Achilles tendons “show evidence of chronic (non-resolving) inflammation.”20
Looking at Dakin et al.’s results, it’s tempting to just concede that inflammation has made a comeback — it was never absent after all, it was just more subtle than the experts thought. Those goofy experts! Always changing their story!
But — and this is important — the busting of the myth of inflamed RSIs remains valid in spirit, because plantar fasciitis is clearly not inflamed as most people understand it, or in ways that can be treated with typical anti-inflammatories, which are effective only for the acute inflammation that really does not exist in RSI.
So here’s the adjusted bottom line: If there’s no (acute) fire, stop hosing it down (with treaments for acute inflammation)! But maybe there are things that can be done for a bed of smoldering coals, and that idea will come up again and again for the rest of the tutorial.
So what of ice, then? The most basic of all anti-inflammatory treatments? Ice can relieve many kinds of pain temporarily by numbing nerve endings, of course. But does it do anything else?
Benefits beyond numbing?
If ice can help a repetitive strain injury in any way beyond brief numbing, no one has ever actually proven it or shown how it might work.
But it is reasonable to speculate that icing could stimulate miscellaneous minor tissue healing processes. Most stimulation and stress, up to a point, can provoke a healthy and adaptive response — the use-it-or-lose-it principle. Stress a tissue, and it will probably get a bit tougher. Maybe.21 In broad strokes, that is probably the only plausible therapeutic mechanism of icing. Ice may simply be one of the easiest delivery systems for a bit of stimulation (while simultaneously getting some temporary pain relief from numbing).
It’s worth doing.
Bad icing news based on new data
What if ice actually doesn’t do anything for inflammation? What if it actually made it a little worse? Could you even tell? There is actually research that shows this.
A small 2013 study for severe muscle soreness had “unexpected” results, according to the researchers: it seemed to do more harm than good.22 The icing victims had higher blood levels of molecules associated with muscle injury and they felt more fatigued. Icing had no effect on recovery of strength, or any biochemical sign of inflammation. A small study, to be sure, but how good can icing be if it can generate this kind of data?
That study was specifically focused on post-exercise muscle soreness, a very specific biological situation that is essentially impossible to treat.23 Even if this data is right, it doesn’t necessarily mean that ice is bad news for other kinds of pain and injury. Icing probably has different effects depending on the situation (which should be very clear after the last couple sections), and it’s particularly clear that it has useful effects on severe inflammation following trauma.
But this is sobering news for ice enthusiasts. It is possible that the main effect of ice is temporary numbing, which just makes it difficult to tell if you’re actually a little better or a little worse an hour later. It’s hard to judge a subtle change after a big one!
Kooky new pain treatment: smart ice implants?

Imagine if you could ice a nerve directly. Like right on it. Implanted. Ice almost literally in your veins. And then tinker with the temperature.
Pretty cool! (🙄)
So this is now a thing (though not yet a product). Reeder et al. report that they have cooked up a strange new high-tech treatment for pain: soft, bioresorbable coolers for a reversible block of peripheral nerves.34 So we’re talking about nerve blocks with a little freezer instead of anaesthetic, basically — and you can fiddle with the temperature.
The branding, obviously, would have to be “Smart Ice.” (It’s not literally ice, of course. But it’s definitely therapeutic icing in spirit.)
This is weird, but it’s not crazy. The principle is sound — and the fact that it works is a vivid validation that ice can indeed be analgesic. Extremes are often instructive. Ice absolutely can shut down nerves, and that is potentially useful.
Is an implanted ice pack actually a good idea though? The devil will be in the details, as with most medical technology, and there are certainly some problems.35 But this is a fascinating new technique, and I imagine it could be quite useful in some cases. Reeder et al. may well get rich.
Use raw ice
An excellent method of therapeutic icing is to use bare or “raw” ice — that is, ice applied directly to the skin, with no layer of plastic or fabric between you and your ice.
Raw ice delivers more of an icy punch! This is due to the spreading of melt water into every crevice, which conducts heat more efficiently away from the skin both directly into the ice, and via evaporation.
In comparison, gel packs and bean bags are comparitively wimpy cryotherapies (although they have their place, as you’ll see). They tend to warm up too quickly (especially where the skin is hottest and needs the most icing), and they sometimes cannot shape themselves well (or gently) to the contours of the injured body part. There are times when they are handy or easier when the stakes are low, but for serious icing of acute injuries or a stubborn tendinitis, you really need an ice cup.
A styrofoam cup is an elegant delivery system for raw ice …
How to make an ice cup
The humble styrofoam cup is the cheapest and most effective injury management tool in my office and in my own home. It’s not the cup itself that’s so useful, of course, but its contents — ice! Don’t wait until you’re hurt to do this — have them ready and waiting.
Illustration of how to make an ice cup. It shows two images, before an after: a Styrofoam cup full of ice with a dotted line about an inch below the lip of the cup, and then the same cup again with the top cut off, exposing the ice.
- Get yourself some styrofoam cups.
- Fill a few cups with water, and freeze them.
- Cut off the top inch of the cup, exposing the ice but leaving the rest of the cup as an insulating “handle.”
If you hold it in a towel while applying, that often helps control the drippings (depending on location).
Or just use an ice cube
In a pinch, with no cups around, just use an ice cube directly held in a dishtowel — almost as good! Less convenient for larger areas, but nearly as effective for most uses. Over the years I’ve found that, 9 times out of 10 I need an ice cup, I haven’t actually got one ready in the freezer, and I end up using ice cubes at first.
Commercial ice cups
One of the downsides of the styrofoam cup option is that it’s a tiny bit wasteful. Wouldn’t it be better to have a re-usable plastic cup designed for the same purpose? There are several brands of ice cups, like the CRYOCUP™ and the Pro-Tec Ice-Up Portable Ice Massager. I’ve never used one personally, but they seem like a great idea, especially for anyone who lives on the edge and brings home new sports and adventure injuries on a regular basis.
In fact, there are even insulated icing tools designed to be taken to the field or the mountains or wherever you think you might need ice.
An alternative worth mentioning is a simple chemical ice pack — the kind you crush to activate. They aren’t as cold as ice, and won’t last as long, but they are very convenient.
The art of icing: when you’re numb, you’re done
Slide the ice over the inflamed area in a slow but steady pattern. It’s important to keep moving, as long as you don’t try to ice such a large area that tissue gets a chance to warm up before you return to the starting point.
Continue ice massaging for 1–3 minutes, or until it is numb, whichever comes first — no more. “When you’re numb, you’re done,” is the rule of thumb for safety (see next section). Areas with thick tissue, like the top of the thigh, will take longer to get numb. Thin areas, like the side of the knee, will usually go numb quickly.
What does numb feel like? Just close your eyes and lightly touch the skin. If you can’t feel it at all, or if you can feel only pressure, that’s numb enough. Stop icing and let the tissue warm up.
Can raw ice “burn” you?
Yes! You may have heard that bare ice is too cold to use directly on the skin in this way. That’s untrue for short periods. Although a cold-sensitive person may find raw ice too uncomfortable, tissue damage can only occur after sustained icing — well after you have gone completely numb, at least 3 minutes. Stopping roughly when you get numb pretty much guarantees that you won’t hurt yourself.
An ice treatment will feel like it is burning or stinging at first, and that’s okay. Icing this way can feel a bit nasty, especially at first in certain locations, but stick with it: the powerful anti-inflammatory effect is worthwhile. In many situations, this is a much better solution than an anti-inflammatory medication.
Ice repeatedly
Once your tissues warm up again, you can repeat the treatment. In fact, you can apply the ice as often as you like, as long as your tissues have a chance to mostly warm up between treatments. In the case of tendinitis, you can continue doing a lot of icing — many applications per day — as long as you still have symptoms, and even when you are feeling better.
In the case of injuries, icing is mostly just useful while the injury is still hot, red, swollen or painful — this phase may last for a few hours or several days. When these signs begin to fade, you may be certain that you would have been stuck with them for a lot longer if you had not been icing.
Power icing
Used properly and safely — being careful not to “burn” yourself — there’s really no limit to how much icing you can do, and more of this good thing might be better. If ice works at all, as a general tissue stimulant, then the benefits might be cumulative. Even if the effect is minor, it might add up.
This is, of course, pure speculation.
People often tell me that they have “tried icing” for an overuse injury like iliotibial band syndrome. A little quizzing usually reveals that this means that they have occasionally applied ice once or twice in a day, only when the need felt greatest. That is not really enough to know whether or not icing is going to help you.
Power icing is the name I’ve given to icing in megadoses — 20–50 applications of ice per day for 3–20 days at a time. As long as each dose is no more than three minutes, and if you allow sufficient opportunity for tissue to warm up between applications, this is not risky — the worst-case scenario is that you’ll waste your time.
I prescribe power icing only for seriously chronic overuse injuries, especially the common tendinitises (mostly tennis elbow), plantar fasciitis, some cases of carpal tunnel syndrome, iliotibial band syndrome, patellofemoral pain syndrome, and some kinds of shin splints.
This is all based on speculation, not science. It seems to make a certain amount of sense, and I seem to have had some success with it with my own clients and readers over the years, the occasional story of amazing recovery with just a few days of power icing. There is mostly no good excuse for prescribing self-treatments that lack even a clear rationale, let alone research evidence that they work. However, this one can be justified by its low costs and risks — worth a shot! Just don’t give yourself frostbite.
The inevitable question with power icing is “how much?” One way of clarifying is simply to say that it should be so much icing that you start to get sick of it. If you’re not thinking, “Wow, geez, this is really a lot of icing!” then you should probably do more.
If it doesn’t seem to be working within 3-5 days, it’s probably not going to do the trick for you. But I strongly recommend that you give it at least three days, so that you can be certain that you really have “tried icing!”
Use an ice cup with an ice gel for stronger, icier cooling
You can definitely enhance the effect of icing by using an ice gel afterwards. This is different than the gel-packs — it’s a goopy blue paste in a jar that feels very cold when you rub it into your skin. A variety of brands are available at any larger drugstore. There is one downside to this technique: if your goal is to do many sessions of icing, your skin tissue takes much longer to warm up between sessions when you’ve applied an ice gel.
When to use gel packs instead of raw ice (the tissue depth issue)
If you want to try to chill deeper, thicker tissues, you need gentler, slower cooling. Raw ice is just too cold to leave on for longer periods. Ice packs to the rescue! Raw ice can probably chill the skinny joints of the hands and feet thoroughly and fairly quickly, and even knees and elbows, but hips or shoulders and spinal joints are deep.
You can also use fabric or towels to further ease the intensity of a gel pack, so that it can be used safely for even longer periods.
How cold, how deep? The effect of ice on tissue temperature
Thermoregulation of our tissues is extremely efficient: reflex responses in microvasculature can compensate quite a lot for changes in surface temperature. So what happens to the tissue temperature under ice? How cold does it get? At 1 centimetre? At 3? Can you chill a knee through and through?
Turns out you can! Most joints are less insulated and have more metabolically quiet tissues, so they can’t adapt to temperature changes as well, and therefore they can be cooled or heated much more easily. In experiments on arthritic knees, Oosterveld et al. demonstrated that hot wax (ligno-paraffin) could raise deep knee temperatures by 1.7–3.5˚C … and the effect of cooling was even more dramatic, dropping the temperature as much as 9˚C.36 Brrr! That’s likely to have some effect on biology.
The effect on muscle is probably much less, but to date I’m unaware of any data that shows it.
To go deeper into this topic, see Icing, Heating & Tissue Temperature.
Did you find this article useful? Interesting? Maybe notice how there’s not much content like this on the Internet? That’s because it’s crazy hard to make it pay. Please support (very) independent science journalism with a donation. See the donation page for more information & options.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
Seven updates have been logged for this article since publication (2004). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
2023 — New section: “Kooky new pain treatment: smart ice implants.”
2022 — Added a bunch of important detail to the RSI section about acute versus chronic inflammation.
2022 — Added a small but useful cautionary tale about the consequences of accidentally icing excessively — by falling asleep with an ice pack on!
2017 — Rewrote “What ice is not for (back pain, usually)” for clarity and thoroughness.
2017 — Upgraded rebuttal to the argument that icing impedes healing.
2016 — Minor revision. Some more commentary about the popularity of debunking icing lately.
2016 — Added evidence of efficacy of NSAIDs for common injuries.
2016 — A series of substantial upgrades, details unlogged.
2004 — Publication.
Notes
- I routinely see this article cited on social media to support the broad assertion that “icing is useless.” The impulse to debunk popular ideas is powerful. Some skeptics — my “tribe,” so I know them all too well — can be so eager to bust a myth that they miss that crucial below-the-fold detail. This is an interesting example of how information is used and abused by all kinds of people, including some of my favourite ones. I suspect that Dr. Mirkin would be startled to learn just how much his article is being used to discourage anyone from icing at all, ever, for any reason.
- It’s based mostly on indirect evidence and the common sensical idea that we shouldn’t interfere with normal healing processes. This relies on assumptions that ice can actually interfere significantly, and that inflammation is always a good thing (see next point). None of the evidence Dr. Mirkin presents is empirical evidence of what actually happens when people ice or don’t ice. The views he expresses are reasonable speculation, but just speculation.
- See Collins and Malanga, both cited and described in some detail at the start of the next section.
- It’s a common misconception that “biology knows best,” but that’s only true in some ways and definitely not in others. Evolution is a wondrous but peculiar process that leads to many compromises, tradeoffs, sacrifices, and truly absurd unintended and irreversible consequences (like the recurrent larygneal nerve in giraffes — look it up, it’s one of the premium examples of how evolution can get backed into a corner). Biology is optimized for reproduction early in life, which only partially aligns with our interests. Not everything natural is good in every context! See the naturalistic fallacy.
- Research has shown that immune cells unnecessarily “swarm” sterile injury sites, causing damage and pain — a biological glitch with profound implications about why some painful problems are so severe and stubborn. For more information, see A Painful Biological Glitch that Causes Pointless Inflammation: How an evolutionary wrong turn led to a biological glitch that condemned the animal kingdom — you included — to much louder, longer pain.
- Collins NC. Is ice right? Does cryotherapy improve outcome for acute soft tissue injury? Emerg Med J. 2008 Feb;25(2):65–8. PubMed 18212134 ❐
Bafflingly, therapeutic icing (cryotherapy) is one of really those basic things that you’d think modern medical science would have mastered by now, but no — not even close!
This is a 2008 review of the inadequate evidence: just six experiments, and only two of them any good, one with slightly positive results and the other showing nothing at all. So that’s two studies that showed little or no benefit, which is leaning towards bad news, but it’s not enough data to clinch it.
Four animal studies have showed that icing reduced swelling (and too much is harmful, duh!). That evidence is mildly encouraging, but of course we can’t take animal studies to the bank.
This really just isn’t enough data, and the bottom line is that we don’t know, which is what Collins concluded: “there is insufficient evidence.” A 2015 review (with a broader scope, see Malanga) had a similar non-conclusion, mostly confirming the absence of evidence.
- Malanga GA, Yan N, Stark J. Mechanisms and efficacy of heat and cold therapies for musculoskeletal injury. Postgrad Med. 2015 Jan;127(1):57–65. PubMed 25526231 ❐
Although it’s 2015, “most recommendations for the use of heat and cold therapy are based on empirical experience,” not evidence, because the only evidence we have is still “limited.” Malinga, Yang, and Stark review the alleged benefits of heat and cold: pain relief for both, of course, plus ice reduces “blood flow, edema, inflammation, muscle spasm, and metabolic demand,” while heating increases “blood flow, metabolism, and elasticity of connective tissues.” Even these aren’t well-tested, and there are other possibilities that haven’t been tested at all.
Based on a handful of relevant trials, they concluded that “heat-wrap therapy provides short-term reductions in pain and disability in patients with acute low back pain and provides significantly greater pain relief of DOMS than does cold therapy.”
But the main take-home message from this paper is just “much more study needed.”
“Tendinitis” versus “tendonitis”: Both spellings are acceptable these days, but the first is the more legitimate, while the second is just an old misspelling that has become acceptable only through popular use, which is a thing that happens in English. The word is based on the Latin “tendo” which has a genitive singular form of tendinis, and a combining form that is therefore tendin. (Source: Stedmans Electronic Medical Dictionary.)
“Tendinitis” vs “tendinopathy”: Both are acceptable labels for ticked off tendons. Tendinopathy (and tendinosis) are often used to avoid the implication of inflammation that is baked into the term tendinitis, because the condition involves no signs of gross, acute inflammation. However, recent research has shown that inflammation is actually there, it’s just not obvious. So tendinitis remains a fair label, and much more familiar to patients to boot.
- This is a pet theory of mine that I have examined and re-examined constantly for a decade. Although no evidence directly supports it — no convenient citation — I’ve based it on a lot of indirect evidence and many other considerations. I summarize the arguments in Back Pain & Trigger Points, and I’ve written (very) extensively on the topic in my low back pain tutorial.
- Trigger points are probably contracted, stagnant, swampy, irritated patches of muscle tissue — a minor soft tissue lesion — but that’s just a controversial theory (see Trigger Point Doubts). No one doubts that these sensitive spots in muscle are common, however. They can cause anything from stiffness and dull aching to show-stopping agony. The pain often spreads in confusing patterns, and they grow like weeds around other painful problems and injuries, making them interesting and tricky and incredibly common.
- Garra G, Singer AJ, Leno R, et al. Heat or cold packs for neck and back strain: a randomized controlled trial of efficacy. Acad Emerg Med. 2010 May;17(5):484–9. PubMed 20536800 ❐
What’s better for neck and back pain — ice or heat? This experiment, conducted at a university-based emergency department, compared the effectiveness of these two common treatments. Everyone studied received 400mg of ibuprofen orally and then thirty patients were given a half hour of either a heating pad or a cold pack.
The researchers concluded that adding heat or cold to ibuprofen therapy did not change the result. Both heat and cold resulted in “mild yet similar improvement in the pain severity.” They recommend that the “choice of heat or cold therapy should be based on patient and practitioner preferences and availability.”
This study has major limitations. These were patients with pain so strong they went to the hospital, so many of them may have been well beyond the help of a hot pack or ice pack. And the ibuprofen was a significant confounding factor.
- The research just cited probably isn’t the last word on the topic: it’s findings were based on a comparison of ice and heat for acute back pain in a hospital setting, where whatever the doctor prescribes — ice or heat — is extremely likely to have a major effect on how you feel about it. The evidence is interesting, but not really much of a guide, because “it depends” too much on too many contextual factors.
Some reasons heat is probably better for back and neck pain:
- Some evidence does suggest heat is a more effective analgesic for back pain (see French; it’s far from decisive, but the results do favour heat a little).
- Heat is much more emotionally “reassuring,” and people with back and neck pain often need reassurance more than anything else (the “mind game” in neck and back pain is huge). Excessive and unwelcome temperature in either direction is going to seem like a threat to your nervous system, but cold is more neurologically menacing than heat on average.
- It’s unlikely that either ice or heating actually facilitates healing, but if one of them does even a little, my money is on heat.
- The tiny capillaries are made of cells that are shaped into a tube, like children making a tunnel from their legs to crawl through. The cells literally just pull apart a bit, enlarging the spaces between them. The circulation becomes like a stream tumbling down a rocky mountainside — it mostly follows the path of least resistance in a loose channel, but there’s lots of spilling. That’s what circulation is like in an inflamed area: wet and sloppy, with some cells staying in the capillaries and others coming and going constantly.
- Ingraham. A Painful Biological Glitch that Causes Pointless Inflammation: How an evolutionary wrong turn led to a biological glitch that condemned the animal kingdom — you included — to much louder, longer pain. PainScience.com. 6608 words. Research has shown that immune cells (neutrophils) unnecessarily “swarm” sterile injury sites, causing damage and pain with no known or likely benefit as a tradeoff. It’s just a clear error: they appear to have mistaken mitochondria for a foreign organism, a legacy of ancient evolutionary history, and a biological glitch with profound implications about why some painful problems are so severe and stubborn.
- Millar NL, Hueber AJ, Reilly JH, et al. Inflammation Is Present in Early Human Tendinopathy. Am J Sports Med. 2010 Jul. PubMed 20595553 ❐
- Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med. 2009 Jun;43(6):409–16. PubMed 18812414 ❐
A well-written and important bird’s eye view of the subject of tendinopathy, presenting an updated way of thinking about the problem. Highly recommended, required reading for professionals.
- Khan KM, Cook JL, Taunton JE, Bonar F. Overuse tendinosis, not tendinitis, part 1: a new paradigm for a difficult clinical problem (part 1). Phys Sportsmed. 2000;28(5):38–48. PubMed 20086639 ❐
From the abstract: “If physicians acknowledge that overuse tendinopathies are due to tendinosis, as distinct from tendinitis, they must modify patient management … ”
- Medzhitov R. Origin and physiological roles of inflammation. Nature. 2008 Jul;454(7203):428–35. PubMed 18650913 ❐
Medzhitov explains that “although infection-induced inflammation is vital, it might be a special case.” Indeed, classic inflammation seems to be an oddball, and has relatively little in common with lots of other “inflammation” — the immune response to infection is dramatic and conspicuous, but perhaps exceptional and distinctive within the broader context of the biology of healing and adaptation … which is so diverse that it really doesn’t fit comfortably under one umbrella term like “inflammation.”
- Dakin SG, Newton J, Martinez FO, et al. Chronic inflammation is a feature of Achilles tendinopathy and rupture. Br J Sports Med. 2017 Nov. PubMed 29118051 ❐
This paper now stands as the best available evidence so far that rumours of inflammation’s demise in tendinopathy are exaggerated/oversimplified. There are no other important sources I’m aware of so far (as of early 2020), and Dakin et al. cite only their own evidence on this.
- Many treatments are based on the idea of “toughening up” tissues. It has always been a reasonable enough idea, but it’s ripe for abuse, and what’s the “right” amount and kind of stress? Results vary widely, but some of the most popular “provocation therapies” just don’t work, like scraping masssage and prolotherapy. Icing counts as one of these dubious approaches to stimulating tissue healing, but is generally much safer, cheaper and easier to try. For more about tissue adaptation, see Tissue Provocation Therapies in Musculoskeletal Medicine.
- Tseng CY, Lee JP, Tsai YS, et al. Topical cooling (icing) delays recovery from eccentric exercise-induced muscle damage. J Strength Cond Res. 2013 May;27(5):1354–61. PubMed 22820210 ❐
ABSTRACT
It is generally thought that topical cooling can interfere with blood perfusion and may have positive effects on recovery from a traumatic challenge. This study examined the influence of topical cooling on muscle damage markers and hemodynamic changes during recovery from eccentric exercise. Eleven male subjects (age 20.2 ± 0.3 years) performed 6 sets of elbow extension at 85% maximum voluntary load and randomly assigned to topical cooling or sham groups during recovery in a randomized crossover fashion. Cold packs were applied to exercised muscle for 15 minutes at 0, 3, 24, 48, and 72 hours after exercise. The exercise significantly elevated circulating creatine kinase-MB isoform (CK-MB) and myoglobin levels. Unexpectedly, greater elevations in circulating CK-MB and myoglobin above the control level were noted in the cooling trial during 48-72 hours of the post-exercise recovery period. Subjective fatigue feeling was greater at 72 hours after topical cooling compared with controls. Removal of the cold pack also led to a protracted rebound in muscle hemoglobin concentration compared with controls. Measures of interleukin (IL)-8, IL-10, IL-1β, and muscle strength during recovery were not influenced by cooling. A peak shift in IL-12p70 was noted during recovery with topical cooling. These data suggest that topical cooling, a commonly used clinical intervention, seems to not improve but rather delay recovery from eccentric exercise-induced muscle damage.
- Ingraham. A Deep Dive into Delayed-Onset Muscle Soreness: The biology & treatment of “muscle fever,” the deep muscle soreness that surges 24-48 hours after an unfamiliar workout intensity. PainScience.com. 17437 words.
- There are four kinds: acetaminophen/paracetamol (Tylenol, Panadol), plus three non-steroidal anti-inflammatories (NSAIDs): aspirin (Bayer, Bufferin), ibuprofen (Advil, Motrin), and naproxen (Aleve, Naprosyn).
- Science Based Pharmacy [Internet]. Gavura S. How risky are NSAIDS?; 2015 Jul 25 [cited 16 Aug 18]. PainSci Bibliography 54751 ❐
- Hung KKC, Graham CA, Lo RSL, et al. Oral paracetamol and/or ibuprofen for treating pain after soft tissue injuries: Single centre double-blind, randomised controlled clinical trial. PLoS One. 2018;13(2):e0192043. PubMed 29408866 ❐
In a test of ibuprofen vs paracetamol for hundreds of soft tissue injuries, there was no significant difference in the modest benefits or side effects, contrary to some past evidence and the widely held medical belief that ibuprofen is better for injuries (inflammation). It’s possible that placebo is powering the effects of both medications, and that's why they were equal, but it's impossible to know without a control group for this study. Note that the superiority of these medications is probably variable and not as clearly established as you might think.
- FDA.gov [Internet]. Acetaminophen and Liver Injury: Q & A for Consumers; 2009 Jun 4 [cited 16 Aug 31]. PainSci Bibliography 53431 ❐
“This drug is generally considered safe when used according to the directions on its labeling. But taking more than the recommended amount can cause liver damage, ranging from abnormalities in liver function blood tests, to acute liver failure, and even death.”
- Machado GC, Maher CG, Ferreira PH, et al. Efficacy and safety of paracetamol for spinal pain and osteoarthritis: systematic review and meta-analysis of randomised placebo controlled trials. BMJ. 2015;350:h1225. PubMed 25828856 ❐ PainSci Bibliography 54220 ❐
- Bally M, Dendukuri N, Rich B, et al. Risk of acute myocardial infarction with NSAIDs in real world use: bayesian meta-analysis of individual patient data. BMJ. 2017 May;357:j1909. PubMed 28487435 ❐ PainSci Bibliography 53592 ❐
Taking any dose of common pain killers for as little as a week is associated with greater risk of heart attack, according to this meta-analysis, and the risk is greatest in the first month of use. This is probably primarily of concern for people already at risk for heart attack, but this data doesn’t address that question, and it’s a lot of people regardless.
- Derry S, Moore RA, Gaskell H, McIntyre M, Wiffen PJ. Topical NSAIDs for acute musculoskeletal pain in adults. Cochrane Database Syst Rev. 2015;6:CD007402. PubMed 26068955 ❐
- Nieman DC, Henson DA, Dumke CL, et al. Ibuprofen use, endotoxemia, inflammation, and plasma cytokines during ultramarathon competition. Brain Behav Immun. 2006 Nov;20(6):578–84. PubMed 16554145 ❐
This experiment tested the effect of ibuprofen on hard-core marathoners. There were 29 ultra-marathoners on high doses of ibuprofen and 25 controls that completed the race without meds. There was no measurable difference in muscle damage or soreness between the two groups. Lead researcher David Niemen: “There is absolutely no reason for runners to be using ibuprofen.”
For some good mainstream journalism about this research see Convincing the Public to Accept New Medical Guidelines, by Aschwanden. For a good plain language tour of the topic in a major medical journal, see Warden.
- Bittermann A, Gao S, Rezvani S, et al. Oral Ibuprofen Interferes with Cellular Healing Responses in a Murine Model of Achilles Tendinopathy. J Musculoskelet Disord Treat. 2018;4(2). PubMed 30687812 ❐ PainSci Bibliography 52446 ❐
- Wheatley BM, Nappo KE, Christensen DL, et al. Effect of NSAIDs on Bone Healing Rates: A Meta-analysis. J Am Acad Orthop Surg. 2019 Apr;27(7):e330–e336. PubMed 30260913 ❐
This is a meta-analysis of 16 trials, showing that common over-the-counter pain-killers interfere with bone healing. Chronic overuse roughly doubles the risk that a fracture will heal slowly or not at all (“non-union,” a very serious complication).
The effect was not evident in children or in lower doses or temporary usage — this bad news applies only to adults taking too much of the stuff for too long. Unfortunately, a lot of people do that! The pain-killers in question are the non-steroidal anti-inflammatory drugs or NSAIDs like aspirin, ibuprofen, and naproxen — already notorious for several other significant side effects, and yet still widely overused.
- Reeder JT, Xie Z, Yang Q, et al. Soft, bioresorbable coolers for reversible conduction block of peripheral nerves. Science. 2022 07;377(6601):109–115. PubMed 35771907 ❐
- It’s invasive, obviously, so that just automatically means that there’s some risk, no matter how good it is.
- You can only block what you can locate, so this will fail in most cases of pain without a clear origin of the pain. Which is many kinds of chronic pain.
- We know that even trying to destroy nerves often fails, for many reasons. If destroying them fails, so will chilling. I discuss this issue in my nerve block article.
- Oosterveld FG, Rasker JJ, Jacobs JW, Overmars HJ. The effect of local heat and cold therapy on the intraarticular and skin surface temperature of the knee. Arthritis Rheum. 1992 Feb;35(2):146–51. PubMed 1734903 ❐