The Complete Guide to IT Band Syndrome
An extremely detailed guide to iliotibial band syndrome (runner’s knee), with detailed reviews of every treatment option

Iliotibial band syndrome (ITBS) — also misleadingly known as iliotibial band friction syndrome — is a common1 repetitive strain injury that causes pain mainly on the side of the knee, especially when descending stairs and hills. It is often maddeningly stubborn. The injury mainly plagues runners — roughly one in 60 marathoners2, probably the second most common running injury3 — but a few unlucky cyclists and hapless hikers will get it too, and it may even be common in inactive people in the aftermath of a knee surgery, or other unknown causes of vulnerability.
Pain on the side of the knee is notably different from the other common kind of runner’s knee, patellofemoral pain, which causes pain on the front of the knee and often gets mixed up with ITBS. Another common point of confusion: contrary to popular belief, ITBS is not a hip or thigh problem — that’s something else (more below).
Although IT band syndrome is common, there are no clearly effective treatments for it, just a mess of options ranging from imperfect to completely bogus. Most popular approaches — like stretching — have major problems. Like almost everything else in physical medicine, ITBS is surprisingly neglected by science and poorly understood,4 but there are many persistent and simplistic myths about — like calling it a “friction” syndrome, which is still just a contested theory.
Bogus ideas about bad treatments: IT Band syndrome myths are common

Here are some examples of wrong and obsolete IT band treatment that patients constantly encounter. (More support for these points later — this is just a debunking sampler.)
- IT band stretching is the king of the conventional wisdom, in spite of good evidence that stretches don’t work, especially the basic ones usually seen in the wild.
- “Elongating” your iliotibial band with intense massage strokes is one of the most popular alternative treatments for ITBS, but it works about as well as it would on a truck tire. Meanwhile, better targets for massage are often neglected.5
- Quadriceps training is a therapy for another kind of knee pain, but — weirdly— it often gets prescribed as treatment for ITBS. This is a simple case of mistaken identity, but you’d be amazed how often it happens.6
- Most doctors are barely aware of IT band syndrome,7 and often neglect (or overemphasize!) the medical options, like cortisone injections or IT band release surgery. Those might help a few people, but they shouldn’t be your first, second, or even third line of defense. Even specialists — sports medicine doctors and orthopedic specialists — often don’t know enough to guide you in these choices. They are usually too preoccupied with other medical priorities to be very knowledgeable about a “minor” condition like ITBS.
This video goes into more detail about some of those points, and introduces several key concepts — all of which can also be found in the text below.
IT band syndrome symptoms
The classic ITBS symptoms are just lateral knee pain when exercising, especially walking or running downhill. That’s enough to clinch a diagnosis for many people, but there’s definitely more to know:
- The epicentre of the pain is mainly sharp or hot pain on the outside of the knee. There might be some discomfort nearly anywhere else around the entire knee, particularly in severe cases, but the worst spot must be on the outside of the knee for an ITBS diagnosis (see the next section for even more location detail). That spot will also be sensitive to poking pressure.
- ITBS is an overuse injury and usually starts with a bigger-than-usual workout run, hike, or walk, especially if there’s a lot of descent (stairs, hills, mountains). The classic onset scenario is going down a big hill when you’re already tired.
- ITBS usually starts quite quickly, often without much warning, within minutes or perhaps an hour or two. But it’s never going to be sudden like a sprain.
- For some people, the pain starts after knee surgeries or other knee traumas. For these more vulnerable patients, ITBS can be triggered by much lighter activity than a classic overuse case, but there’s often still an activity trigger.
- Many patients with chronic ITBS feel fine most of the time, but suffer exasperating flare-ups whenever they walk or run for too long. They also usually learn to beware of going down stairs or hills. Hikers with ITBS may be completely fine with virtually any activity except coming down a mountain.
- However, some severe cases do cause continuous pain, or pain with virtually any use of the knee. But even those cases are still obviously aggravated by activity — especially going down stairs.
Later on, I’ll go much further into the topic of diagnosis: whether or not to get an MRI, the role of hip and thigh pain, conditions that get confused with ITBS, some all-too-common misdiagnosis horror stories, and much more.
Are you in the right place? Patellofemoral versus IT band pain

“Runner’s knee” can be either IT band syndrome or patellofemoral pain.
“Runner’s knee” is not one condition. There are two flavours of it (at least). Let’s make sure you’re reading the right tutorial, because ITBS is often confused with the other common runner’s knee injury: patellofemoral pain syndrome. Although the two conditions may seem quite similar, usually you can tell the difference just by the location of the pain.
Iliotibial band pain is truly a side of the knee condition (the side facing out), and the epicentre of the symptoms is always there, by definition.8 More specifically:
- the outward-facing side of the knee
- at or just above the prominent bump of bone (lateral epicondyle)
- well-defined pain location, an epicentre you can point to with precision
- fairly superficial — on the side of the knee joint, not in it
Patellofemoral pain syndrome (PFPS): mostly about anterior pain, not lateral
Which condition is “runner’s knee” — ITBS or PFPS? Trick question: they both are. They are constantly mixed up because they are both common repetitive strain injuries of the knee, causing pain in locations that are right beside each other. But while ITBS causes focal pain on the side of the knee, PFPS is all about more diffuse pain on the front of the knee — so much so that it is also often called “anterior knee pain.”
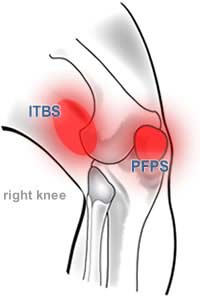
Front or side?
The epicentre of iliotibial band pain is always on the outside of the knee. The pain of patellofemoral pain syndrome is more variable, but usually dominates the kneecap.
PFPS is a bucket diagnosis that covers several of the possibilities, a condition of many conditions. If you have knee pain with a location that isn’t quite right for an ITBS diagnosis, its may be worth looking at PFPS as a possibility.
Despite the clear side vs. front distinction, confusion about the difference between these conditions abounds. For a more detailed comparison, see Diagnosing Runner’s Knee. Or, if you obviously have pain that dominates the front of your knee, then you should just switch right now to my guide to patellofemoral pain.
Is hip pain a type of IT band syndrome?
No. Pain on any part of the thigh or hip is something else — even if the IT band is involved in some way, it’s still not “IT band syndrome.” Greater trochanteric pain syndrome (GTPS) is the most common kind of unexplained hip and thigh pain. This guide covers hip pain as well as knee pain, because it might be a complication or partial cause of ITBS.

This kind of pain is never “IT band syndrome.” Despite the fact that the IT band does exist there.
Runner’s knee without running: post-surgical lateral knee pain
Lateral knee pain can crop up in many people who’ve recently had a total knee replacement. This does not seem to be a widely known fact, and I’ve become aware of it only because so many readers of this guide have emailed me to ask: “I am not a runner, but I had surgery and now I seem to have runners’ knee. Is that possible?”
Almost any amount of activity may be like “overuse” if your knee has been disturbed by surgery.
Sure it is! In 2020, Takagi et al. reported four examples of such cases, each one caused by “an obstruction just under the IT band”: two cases of extruded cement, one bone spur, and one case of a “sharp-edged bearing,” which is the polyethylene insert that serves as the “artificial cartilage” in the artificial knee.9
None of those cases responded well to non-surgical treatment, but these surgery-caused problems were all relieved in these cases by surgically removing the obstruction, which is both unsurprising and ironic. If you’ve got a bulging bit of cement, bone, or plastic “stuck” under your IT band, it’s going to cause trouble until it’s removed.
There might be an obstruction in every case of post-replacement ITBS — that might be the only way that it works, or the main way — but I doubt it.
I suspect that knees are sometimes quite easily irritated for quite a while after surgery — a natural physiological reaction that varies widely in severity. Some knees may be so vulnerable that almost any amount of activity constitutes “overuse.” For a healthy young runner, it takes a bunch of running to do this to their knees. For an older person after knee surgery, normal non-running, non-athletic activity might do the same. It is still fundamentally an overuse condition, just with an absurdly low threshold for the amount of activity required to cause trouble.
Once you have ITBS, how it works and how to treat it are probably quite similar … but not identical. This guide isn’t ideal for post-surgical, non-runner cases: it may be relevant to many patients, but misleading/irrelevant for some.
Still, regardless of where the threshold for overuse is, the rehab challenge is similar in principle: mostly it’s just about reducing knee stress until it’s under that threshold, wherever it is … but that can be difficult to embrace when you’ve seriously underestimated how low it is.
Some post-surgical lateral knee pain is probably not an IT band problem at all
In my exasperated experience, many cases of ITBS are diagnosed carelessly by surgeons, with a bit of a shrug, just tossing out an idea that’s a rough fit for lateral knee pain. Most of them probably don’t know much about ITBS. Surgery is notoriously prone to puzzling complications and many patients will struggle with a slow recovery. Maybe some post-surgical patients are being diagnosed with IT band syndrome simply because their symptoms superficially resemble it.
But no one knows, there’s no data on this. As you’ll learn below, even runner’s knee for runners is poorly understood. For post-surgical patients, the nature of lateral knee pain is even more inscrutable. Except for the cases that involve an obvious bump under the IT band! And maybe that’s most of them .
An orphan injury: IT band syndrome neglected by science
We can put a man on the moon … but we routinely can’t treat IT band syndrome. Here’s some important basic context for anyone setting out to learn more about their case: musculoskeletal medicine is a bit of a backwater.10
No wonder therapy often bombs: it’s just not studied enough,1112 and treatment for it is not taught to physical therapists and doctors.13 I have a big sports injuries text that coughs up only a few short sentences, breezily concluding that “the prognosis is good with appropriate treatment” — without even saying what the treatment is!14

“Further Study Is Needed” … for virtually all sports injuries and musculoskeletal pain problems. But ITBS is unusually bad: very common, amazingly unstudied.
Sports medicine in general is amazingly primitive considering how much potential funding it has. You’d think anything affecting elite athletes with huge audiences and deep-pocketed would be getting more attention! The situation is improving, but only recently and it still has a long way to go.15
I have suffered from IT band syndrome myself — see my own IT band story in Appendix A below (grizzly bears included). I have also seen many stubborn cases of it in my own patients (I was a massage therapist for a decade in one of the runningest cities in the world, Vancouver). The prognosis for iliotibial band syndrome is not always good, and many common treatments are ineffective.16 Many people recover with a little rest, icing, and stretching, but not everyone. And probably not you, or you wouldn’t be reading this.
Let’s get into it …
Part 2
Nature of the Beast
What causes iliotibial band syndrome?
When it’s not as obvious as surgical detritus stuck under the IT band, What causes ITBS? is not as easy a question to answer as you probably thought. In fact, it turns out that it’s not as easy as anyone thought. Overuse injuries of all kinds — once seen as basically mechanical, like brake pads wearing out — have proven to be scientifically messy and bizarre. No one can even seem to agree on whether or not they are “inflamed,” for instance. And chronic pain of any kind tends to involve some degree of neurological voodoo (“sensitization”). Much that was once considered “obvious” or “common sense” has proved to be either embarrassingly wrong or at least sketchier than anyone saw coming back in simpler times, when musculoskeletal medicine was still underestimate as a “simple” sub-field of medicine.
Researchers have only just begun to try to find out what’s really going on. Maybe.
On the face of it, iliotibial band syndrome is still a simple condition, caused by excessive knee usage and mostly treated by resting. But to anyone who can’t get rid of it just by resting, it is equally obvious that there must be more to it than that …
The conventional wisdom about IT band syndrome
Iliotibial band syndrome is mainly a running injury, responsible for about one in twenty lower limb injuries in long-distance runners.17 Probably at least a quarter of all long-distance runners will be stricken eventually. It is as common as dirt, and roughly one in twenty-five people who do any kind of vigorous physical training will get a case of it.1819 So basically it’s mainly (though not exclusively) an overuse injury.
Homo sapiens may be good at running, but that doesn’t mean it’s easy or risk-free.
Throughout hominid history, if you’re running 26 miles in a day, you’re either very intent on eating someone or someone’s very intent on eating you.
Why Zebras Don’t Get Ulcers, by Robert M Sapolsky, 123
Just to put this in perspective, iliotibial band syndrome is probably not much less common than ankle sprains, which are generally regarded as the most common of all athletic injuries.20
Iliotibial band syndrome is also prominent in cyclists21 — even though each stroke of the pedals is probably much less irritating to this knee condition than running, sheer repetition can certainly make up for it. Hiking, backpacking, orienteering, and frequent long walks can also cause the syndrome.22
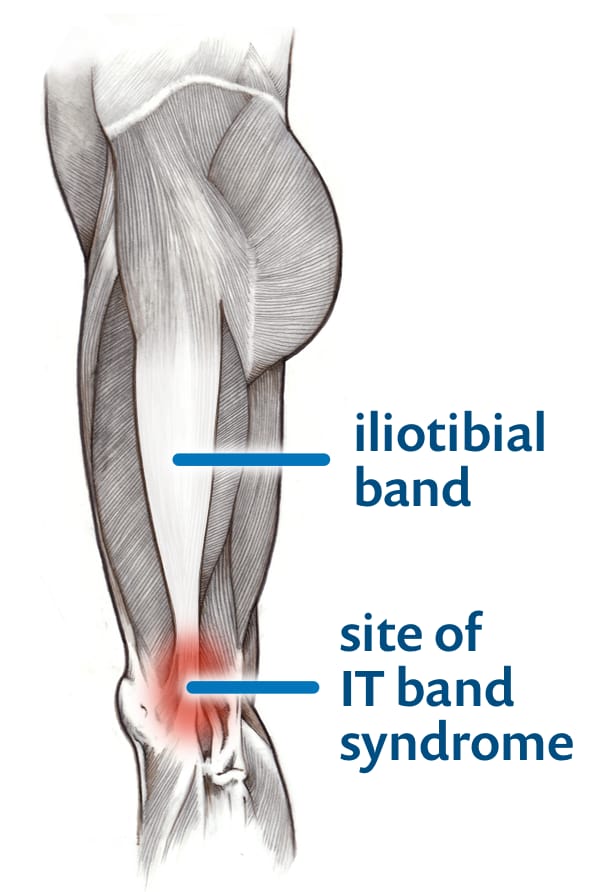
The conventional wisdom says that iliotibial band syndrome (ITBS) is a kind of tendinitis. The iliotibial band is a large tendon running down the side of the leg from the hip. If it gets too tight, it rubs painfully over a bump of bone on the side of the knee, the lateral epicondyle. For this reason — the alleged rubbing — it is also commonly called iliotibial band friction syndrome (ITBFS).
Makes sense. Right? Well, not anymore. Iliotibial band friction syndrome may not be a “friction” syndrome after all, or not always — and it may not even be a “tendinitis.” The irritated structure is probably often not the iliotibial band. Nor is the IT band “too tight” — which particularly fascinates me, because the world of physical therapy is obsessed with trying to loosen IT bands.
There are a lot of awkward problems with the conventional wisdom.
Friction syndrome? So where’s the rub? Is the IT band even “tight”?
I think IT band syndrome probably can be caused by IT band tightness and/or friction — that seems obvious when you look at the cases that crop up after a surgery, where there’s an actual foreign body stuck under the IT band and irritating it.23 But that’s not how most ITBS works; most people don’t have that blatantly problematic knee situation. And meanwhile there are major scientific concerns about the validity of the ideas of “friction” and “tightness” in ITBS.
In 2007, John Fairclough of University of Wales Institute, with seven coauthors, issued a major challenge to the classic definition of iliotibial band syndrome, and even of the iliotibial band itself, in a paper published in the Journal of Science and Medicine in Sport.2425 They make a strong case, concluding that “the perception of movement of the ITB across the epicondyle is an illusion.” They’re saying the function, dysfunction and actual anatomy of the IT band has been misunderstood all along.
It’s a charming example of how primitive medical science still is. Can we really still be learning anatomy this late in history? Oh, hell yes!26 Of course.
We’re not only still learning, but still arguing about it. A few years after Fairclough’s work on this, Jelsing et al. came along and used ultrasound to show that the IT band does move back and forth, maybe — even though they agree that the IT band really is firmly anchored to the side of the knee. There is no good solution to this paradox, but for a few reasons I still think it’s best to think of friction as an mostly obsolete idea. Much more about Jesling’s fly-in-the-ointment evidence below.
A 2024 study of the microscopic anatomy of the iliotibial tract shows complex layer and fibre orientations and tortuosity across layers, consistent with the idea that IT band syndrome involves complex internal strain and inter-layer shear, much more complex than just “rubbing” over the lateral femoral epicondyle (much more on this paper in the anatomy chapter coming soon).

The author’s knee. The forward edge of my IT band is prominent at the level of the knee, but doesn’t even particularly appear to move across the epicondyle, let alone actually do it. It just pops out. Fairclough et al.: “The perception of movement of the ITB across the epicondyle is an illusion.”
And as for the common wisdom that the iliotibial band is “too tight”?
In 2004, a research group at University of Connecticut led by Michelle Devan decided to try to figure out the effect of “structural abnormalities” on overuse knee injuries like iliotibial band syndrome.27 So they measured a bunch of stuff in a group of athletic young women, looking for structural problems that every therapist in the world “knows” are risk factors for various knee problems, including the tightness of iliotibial bands … and then they waited to see who got what kinds of knee injuries. Based on the conventional wisdom, you would fully expect the women with tight iliotibial bands to get more ITB syndrome. In fact, it’s “obvious”!
But of course that’s not what happened — and this is what makes IT band syndrome such an interesting subject. Now, here’s what did happen …
Several of these young women athletes did get iliotibial band syndrome that season. It was the most common injury in the group.28 But these expert assessors determined that not one of them had tight iliotibial bands. Not even one!
All the athletes with iliotibial band friction syndrome had a negative bilateral Ober test [their IT bands were not tight].
It was just a few athletes, and the Ober test isn’t a good test,29 but it doesn’t detract from the main message: it’s not safe to assume that a tight ITB matters.
The conventional wisdom was such a nice, straightforward picture of the condition that no one was apparently motivated to question it — after all, ITBS is a relatively minor problem. Most cases resolve spontaneously or with conservative treatment, and the others respond pretty well to a simple surgery. Why rock the boat by challenging the very definition of the problem?
Because that simple picture is almost certainly wrong! “Minor” or not, many consumer dollars have been wasted on therapies based on that wrong picture. What little research there is has been undertaken under the influence of bogus basic assumptions about how ITBS works. If we understand the condition as it truly is, maybe someday it can be treated more efficiently and conservatively, without surgery (or more effective surgeries).
So, if not generally a problem with friction and/or tightness … what then? What exactly is iliotibial band syndrome? To answer that, we need to talk anatomy. Hang on, you’re about to learn some Latin. You will be able to amaze your running buddies with your knowledge. Your authoritative command of ITB anatomy will blow them away!
So is it a tendon or what? IT bands are special
The iliotibial band is usually described as a tendon — a big one. (Quick refresher: tendons connect muscles to bones, while ligaments connect bones to bones.) The IT band is so big that it’s also called the iliotibial tract: no other tendon is known as a “tract”! It is often called the largest tendon in the body, which is sort of true, but it’s clearly not just any tendon. It’s a rather special and complicated one …
- This tendon is also technically a ligament: that is, a connective tissue structure that connects bone-to-bone, rather than muscle-to-bone. The ITB is attached to the pelvis as well as the knee. It’s the only major example of a ligament-tendon hybrid in the human body.
- Most tendons are dwarfed by the muscle they belong to, but the iliotibial band is much more massive than its tiny tensor fasciae latae muscle (TFL) — several times longer and much wider.
- Although the gluteus maximus also partially uses the iliotibial band as a tendon, the connection is at an odd angle: the job of the gluteus maximus is probably not to pull directly on the iliotibial band (like most muscle-tendon relationships), but to increase the tension on it by pulling on it laterally (like drawing a bowstring).
- The IT band blends seamlessly into the capsule around the knee (which is why your knee seems to “cinch up” during a good iliotibial band stretch30).
- Most tendons have clear edges and are well separated from other tissues. The IT band is more of a reinforced section of the connective tissue container for the whole thigh — like a tough part of a sausage wrapping.31
- It’s an energy storage device, a leg battery. It stores some elastic energy during part of our stride, and then releases it to give us a little boost, just like the Achilles tendon. It’s a minor effect, much less than the Achilles tendon, but it’s one of the things that makes it an eccentric bit of anatomy.32
- In addition to blending with the connective tissue wrappings of the thigh and the knee joint capsule, the IT band is quite well-connected with many discrete deep attachment points (“insertions”) on the femur, the tibia, and the patella.33 A couple of these have been discovered surprisingly recently, and one of them is especially relevant to runner’s knee …
- Most importantly, the IT band is tightly anchored to the full length of the femur, from hip to knee — especially just above the knee.
- Oddly, the upper reaches of the IT band also penetrate all the way into the hip, from the bottom of the tensor fasciae latae (TFL) muscle to the lateral surface of the hip joint, which it entirely covers.34 This feature of the IT band was first clarified in 2017. It has no direct relevance to IT band syndrome, but it’s interesting anatomy that’s really at odds with the conventional picture of the IT band as a superficial strap running down the outside of the thigh.
- There’s a “new” knee ligament, the re-discovered anterolateral ligament, which was mostly unknown to science until 2013.35 It probably doesn’t matter much to ITBS, but “new” anatomy is always interesting, and this example emphasizes how much we probably still have things to learn about knees and IT bands.
- A fancy “3D microstructural analysis” of the IT band in 2024 was clearly cool science,36 but does it matter? It does, actually: they showed region-specific thickness, layering, fibre orientation, and tortuosity … all of which directly challenges the common simplification of the IT band as a uniform, linear, strap-like structure. More specifically, it suggests that IT band syndrome could involve complex internal strain and inter-layer shear … and not simple “rubbing” over the lateral femoral epicondyle.
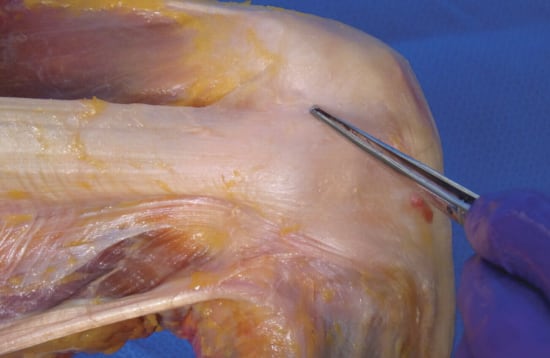
Superficial dissection of the knee, highlighting the iliotibial band. Notice how it widens and spreads out as it nears the knee.
All that anchoring to deep structures is important. Most people still think of the IT band as being free to move relative to the femur, like any other self-respecting tendon: a strap that lies under the skin, separated from the femur by a thick layer of quadriceps muscle. But the iliotibial band is not free to move relative to the femur, or so little that it doesn’t count. It is anchored to the femur between the big muscles of the front and back; it clings to it like a barnacle to a rock,37 even right where it slides back and forth over the side of the knee.
This is why Fairclough et al. suggested that “the ITB cannot actually create frictional forces by moving forwards and backwards over the epicondyle during flexion and extension of the knee.” The anatomy only creates the illusion of a slide over the side of the knee.3839
That mental image of the IT band snapping over the side of the knee is prevalent and misleading, the reason for some futile treatment strategies. This is an advanced and obscure anatomy puzzle; many pros will never learn more about this than they did in school, which was probably still really basic even if they graduated this year, even 19 years after Fairclough et al.’s paper. The state of anatomical knowledge in general is cringe-inducingly poor.40
But the truth is out there! The ITB is a unique connective tissue structure with some properties of a tendon, others of a ligament, and an unusual tension control system consisting of a couple of hip muscles at the upper end, and it probably does not slide significantly over the side of the knee .
What’s actually irritated? Not the IT band …
Fairclough et al. argued that the iliotibial band itself is not the irritated structure in ITBS. If not, what is? Something under the IT band is the simplest answer at this time…
END OF FREE INTRODUCTION
Purchase full access to this tutorial for USD$1995. Continue reading this page immediately after purchase. See a complete table of contents below. Most content on PainScience.com is free.?
Almost everything on this website is free: about 80% of the site by wordcount, or 95% of the bigger pages. This page is only one of 10 that have a price tag. There are also hundreds of free articles, including several about IT band pain. Book sales — over 75,500 since 2007?This is a tough number for anyone to audit, because my customer database is completely private and highly secure. But if a regulatory agency ever said “show us your math,” I certainly could! This count is automatically updated once every day or two, and rounded down to the nearest 100. Due to some oddities in technology over the years, it’s probably a bit of an underestimate. — keep the lights on and allow me to publish everything else (without ads).
Q. Ack, what’s with that surprise price tag?!
A. I know it can make a poor impression, but I have to make a living and this is the best way I’ve found to keep the lights on here.

Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
| company | PainScience.com |
|---|---|
| owner | Paul Ingraham |
| contact | 778-968-0930 |
| refunds | 100%, no time limit +Customers are welcome to ask for a refund months after purchase — I understand that it can take time to decide if information like this was worth the price for you. |
| more info | policies page ❐ |
| payments |
- What do you get, exactly? An online tutorial, book-length (84 chapters). Free updates forever, read on any device, and lend it out. An audio version of this book is included. E-book only! MORE
- Secure payment takes about 2 minutes. No password or login: when payment is confirmed, you are instantly granted full, permanent access to this page.MORE
- Collect them all. Get an “e-boxed” set of all 10 PainScience.com tutorials, ideal for pros … or patients with a lot of problems.MORE
Q. What am I buying? Is there an actual paper book?
A. Payment unlocks access to 73 more chapters of what is basically a huge webpage. There is no paper book — I only sell book-length online tutorials (and audio). This format is great for instant delivery, and many other benefits “traditional” e-books can’t offer, especially hassle-free lending and updates. You get free lifetime access to the always-current “live” web version (and offline reading is easy too).

Read on any device. Lend it out. New editions free forever.
Q. I just don’t like reading on the computer! Is there any way around that?
A. The design and technology of the book is ideal for reading on tablets and smart phones. You can also print the book on a home printer. Or listen to the audiobook!
Q. Can I lend the tutorial out?
A. Yes! Feel free to lend your tutorial: I do not impose silly lending limits like with most other ebooks. No complicated policies or rules, just the honour system! You buy it, you can share it. You can also give it as a gift.
Q. Is it safe to use my credit card on your website?
A. Literally safer than a bank machine. Payments are powered by Stripe, which has an A+ Better Business Bureau rating. Card info never touches my servers. It’s easy to verify my identity and the legitimacy of my business: just Google me [new tab/window].
Q. I can really get a refund at any time?
A. Yes. All PainScience.com ebooks have a lifetime money-back guarantee.
Q. Why do you ask for contact information?
A. To prevent fraud and help with order lookups. You aren’t “subscribing” to anything: I never send email to customers except to confirm purchases.
Q. Can I buy this anywhere else? Amazon?
A. Not yet. Maybe someday.
See the “fine print page” for more about security, privacy, and refunds. No legalese, just plain English.
Save a bundle on a bundle
The e-boxed set is a bundle of all 10 book-length tutorials for sale on PainScience.com: 10 books about 10 different common injuries and pain problems. All ten topics are (all links open free intros in a new tab/window): muscle strain, muscle pain, back and neck pain, two kinds of runner’s knee (IT band syndrome and patellofemoral pain), shin splints, plantar fasciitis, and frozen shoulder. (Headache coming soon, fall of 2019.)
Most patients only need one book, because most patients have only one problem. But the set is ideal for professionals, and some keen patients do want all of them, for the education, and for lending to friends and family. And, of course, you do get a substantial discount for the bulk purchase. But no rush—complete the set later, minus the price of any books already bought. More information and purchase options.
You can also keep reading more without buying. Here are some other free samples from the book, and other closely related articles on PainScience.com:
- EXCERPT IT Band Stretching Does Not Work
- EXCERPT Does the IT Band Move After All?
- EXCERPT The Causes of Runner's Knee Are Rarely Obvious
- EXCERPT Do IT Band Straps Work for Runner’s Knee?
- IT Band Pain is Knee Pain, Not Hip Pain
- Is IT Band Tendinitis Really a Tendinitis?
- Diagnosing Runner’s Knee
- Is Running on Pavement Risky?
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
The ITBS misinformation explosion and why this book matters
In the many years since I’ve been writing about IT band syndrome, there has been an explosion of shabby information about it available on the Internet. Shockingly, this has not resulted in patients or health care professionals being better informed. Most of the information that you can find out there repeats the same oversimplified conventional wisdom … much of which is just wrong.+If the road to Hell is paved with good intentions, nothing has helped more people drive there than the Internet. For many years, if you Googled “iliotibial band syndrome,” the abominable www.itbs.info was the #1 result: an incomplete, scientifically illiterate tour of stale conventional wisdom. Untouched since 2000, it finally dropped off the first page of results sometime in 2013, and then disappeared at last, after at least fifteen years of attracting tens of thousands of readers per year. The demise of itbs.info didn’t improve the Google search results much. Scientists have actually proven that “Dr. Google” is incompetent — just in case you needed any convincing. In 2012, the The Journal of Foot & Ankle Surgery ranked 136 websites about common foot and ankle diagnoses. Expert reviewers gave each a quality score on a scale of 100. The average score? Just below fifty. Fifty! See Smith et al. Or see Starman et al. for a review of other kinds of health care information (with nearly identical grades). P.S. These references are aging now… but nothing’s really changed!
I’ve been obsessively updating this tutorial for about 26 years, and it’s the largest and best of its kind as far as I know. The limited competition has serious “trust issues.”+I once noticed a new book about ITBS on Amazon. Had someone finally written something that might compete with this tutorial? Er, no — it contained exactly zero actual information about ITBS, a fraudulent non-book filled with irrelevant advice on things like how to find a doctor and research nutrition. Hilariously, this non-book was actually recommended on www.itbs.info, the awful but high-ranking website I mentioned in the last note. After years of neglect, a tiny update was posted recommending this “book.” That was the “update”! •facepalm •
There is no cure for IT band syndrome. Of course not! Wouldn’t it be great if there were a proven treatment with minimal cost, inconvenience, or side effects? But we’re nowhere close to this for IT band syndrome. This book wouldn’t need to exist if there were.
So what can I do for you?
What I can do is explain and review all the imperfect options so that you can prioritize them. I can help you confirm your diagnosis and debunk bad ideas. Some people will finally enjoy a breakthrough after reading this tutorial, and get partial or complete relief of their symptoms, sometimes temporary, sometimes lasting. And maybe that is kind of miraculous!
It’s also actually evidence-based, at least a little. Online tutorials may actually be able to help people with chronic pain.+Dear BF, Gandy M, Karin E, et al. The Pain Course: A Randomised Controlled Trial Examining an Internet-Delivered Pain Management Program when Provided with Different Levels of Clinician Support. Pain. 2015 May. PubMed 26039902 ❐
Researchers tested a series of web-based pain management tutorials on people who had been suffering for more than six months. No matter how much (or little) help they had from doctors and therapists, they all experienced significant reductions in disability, anxiety, and average pain levels, for at least three months. Basic knowledge is fine for basic cases, but more and better information is important for the tough ones. And even if you only recently developed IT band pain for the first time, how long do you want to spend following poor quality advice or muddling about with partial understanding? Get started on the right foot.
All of that is hopefully worth more than several sessions of physical therapy, at a fraction of the cost.
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
Part 2.5
Appendices
Appendix A: My own iliotibial band syndrome story … grizzly bears included

Rawr! Not the actual grizzly I met — this one looks much friendlier — but there is a resemblance.
Note: this is the condensed version of this story. If you find me particularly amusing, you can also read a more long-winded version.
I was struck down dramatically by iliotibial band syndrome in both knees at once, on a solo backpacking trip in the Monashee Mountains in the spring of 1998. But that makes me sound more adventurous than I am.
In reality, I am a big chicken, and being in the woods alone spooked me but good. I got injured because I pushed too hard, too fast, and ended up deep into the mountains late in the day, with the trail ahead lost in snow. I decided to rush back to the trail head even if I had to hike in the dark for a while. So I practically ran down the mountain with a fifty-pound backpack — big mistake! After just an hour, both my knees started to scream.
The rest of the hike was a nightmare, certainly one of my most painful experiences. There were times when I felt certain I couldn’t take another step … yet somehow I did.
I was almost at the trailhead when a momma grizzly found me. I’d seen a warning sign about her before starting the hike. In fact, I had gotten quite paranoid about crossing paths with her as I neared the trailhead!
It didn’t work.
It was deep twilight, and there was nowhere to run, and I couldn’t run anyway, and no one outruns a grizzly anyway. She charged me on the trail, and I heard her before I saw her. I thought the following two thoughts, in this order, I swear:
- I guess I’m going to be maimed and killed now. Damn. This is going to hurt.
- At least I won’t have to walk any further!
Grizzlies are fast! (Up to 34 mph, 55 kph.) She came at me like I was lying at the bottom of a cliff and she was falling on me. The idea of unlatching my bear spray from its “quick” release, pulling the safety pin, aiming, and firing … absolutely ridiculous! She was simply way too fast and intimidating.
And she did what grizzlies almost always do when they charge people: she veered off at the last second. Grizzlies aren’t particularly predatory, but they certainly take their cubs seriously, and her main goal was to intimidate me … and that she surely did.
And that’s my entertaining bear story! It’s given me years of dinner party material, and it will for the rest of my life. Now, back to iliotibial band syndrome …
The next day, I quite literally could not get down stairs — which was problematic, because I lived in a 3rd-storey walk-up — both due to the worst case of delayed onset (post-exercise) muscle soreness I have had in my life, and the napalm attacks on the sides of my knees. I have seen some nasty cases of iliotibial band syndrome in my career, but I feel comfortable claiming that I’ve had it worse than anyone else I’ve ever met.
I was in school at that time, and we hadn’t learned diddly-squat about iliotibial band syndrome yet, nor did we later — that’s partly how I know just how poorly informed most massage therapists are about this condition. I never would have learned more than the basics if I hadn’t been forced to learn more by my own injury. It took me one year to recover, and to this day I still suffer occasional flare-ups if I run for more than a couple hours … which I do.

That’s me, getting ready to flick the disc.
I am an enthusiastic ultimate player — that’s me there in the picture, getting ready to flick the disc — so the injury was deeply frustrating to me, and, just like every serious runner I’ve ever treated, it was nearly impossible to keep me from re-injuring myself. I simply would not stay off the field. Every return to play was premature. This was where I first made the observation that, in all likelihood, runners (and ultimate players) are more of a problem than their knees. Iliotibial band syndrome isn’t stubborn — we are!
For me, the best treatments were probably rest, megadoses of well-timed icing (controlling inflammation at the times when it was most likely to start), and discovering that one of the t’ai chi moves I did was particularly good at stretching the iliotibial band and associated musculature. How did I know? Because it hurt like hell! With my ultra-sensitive knees, it was really quite easy to evaluate how strongly different positions pulled on my iliotibial band — given that I was studying anatomy intensively at the time, I was in ideal circumstances to experiment. So this is how I first learned the importance of knee flexion in stretching the iliotibial band, a difference that was as clear to me as flicking a light switch: just add knee flexion to any of the standard stretches, and the iliotibial band pulls much tighter over the side of the knee. To this day, I don’t know if the stretching actually helped, but it certainly felt like a “real” stretch of the IT band, more so than any other stretch I could do.
All of this was good preparation for helping other people with iliotibial band syndrome, of course. Today, I know many things that I really wish I had known when I first hurt myself! And that’s why this very, very long tutorial exists.
Contradiction Addendum: So do I think stretching is pointless or effective? Sharp-eyed readers will notice a contradiction: I’ve written many things about stretching in general, and stretching for ITBS especially, that sound like I think it’s pointless. And yet I have also credited it with seeming to contribute to my own recovery, and I still actually recommend trying it. What gives? What is it, thumbs up or down?
For my most positive take on ITB stretching, basically I’m grading on a curve 😜 and assuming good technique (which is rare). It’s also cheap, easy, plausible, and safe enough to be worth a shot. And my own personal experience has some weight (not much, but some). These factors upgrade what would otherwise be a negative opinion up to a “cautiously optimistic” one.
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
Reader feedback … good and bad
Testimonials on health care websites reek of quackery, so publishing them has always made me a bit queasy. But my testimonials are mostly about the quality of the information I’m selling, and I hope that makes all the difference. So here are some highlights from the kind words I’ve received over the years … plus some of the common criticisms I receive, at the end. These are all genuine testimonials, mostly received by email. In many cases I withold or change names and identifying details.
I am a mostly retired ER doc in Oregon who just finished reading your ITBS tutorial. Impressive. I enjoy something medical from a non medical person's perspective — refreshing, in your case. A very nice job.
Arnold Donstain
Very interesting to read! Thanks for all the research and clearing up a lot of mysteries that I’ve tried over the years. I wish I’d bought it the first time I came across your book instead of scouring research myself and drawing no conclusions…
Angela Talbot
Anyway, once I realized it is probably ITBS, I read at least 50 websites about it. Yours was one of the first few I came across, but I figured among all the information that exists I could find enough that wouldn't warrant me to buy your e-book. I'm all for supporting people for the good work they do, but I'm also a grad student and times are tough! But it turns out that most of those websites were clearly unsubstantiated by any real science. So I bought your book today! And have spent the last two hours reading it. As personally frustrating as it is, I seriously love the thorough debunking that you do. I kind of want to buy a copy for all the authors of the articles I've read.
Sam Hollands
I really appreciate the thoroughness and research you put into these resources. I previously purchased your book on IT band syndrome and it was by far the best investment I made in recovering from the injury myself. I was back running in less than 2 months. Even though there’s no single cure, it’s a big help knowing what foolish treatments to avoid based on the research.
Alan Crane
Thank you for the clear, well-written, highly researched, and logical information you provide. I’ve read an awful lot about knee injuries and about sensitization. Much of it seems to fall into one of two camps: anti-science praise for alternative therapies, or dismissive “it’s all in your head” claims from doctors who aren’t sure what’s wrong. I deeply appreciate the time you’ve taken to explain what is known, what is not known, and how standard therapies have evolved (sometimes even in opposition to scientific evidence). Your writing resonates with my own experience of injury and pain as well as my experience of doctors who are guessing, trying things that don’t work, and then trying those same things again while hoping for better results.One more thing: I’m a fellow writer/editor type, and I appreciate your style. It’s straightforward, clear and light, skimmable but rewarding to dive into, smart and funny--everything that this type of writing should be.
Livia Neale
First off, I previously purchased two of your e-books for my wife and I. Thank you for your diligent research. Thank you for taking the initiative to get this information out there. I have suffered with a chronic case of runner’s knee that the physical therapists & orthopaedists couldn’t fix. After reading your book, it’s no wonder - these ‘experts’ know very little about the situation to begin with. After researching relevant material, including your e-book, I am finally on the road to recovery.
Dainton Sears
I purchased your ITBS book and just wanted to say thank you: every other word of advice I had gotten about the injury either didn’t help, or made things worse. Your tutorial was the only guide to the injury that was consistent with my experience and symptoms. It’s helped me understand the issue better, and I hope, a few weeks after having read through the tutorial thoroughly, that I’m on my way to recovering fully.
Dennis Tower, Boston
I appreciate what appears to be a well-researched, sobering, humble but hopeful approach to this complex condition.
Frankie Koch
I really appreciate your objectivity.
Dr. Bryan Allf, MD, North Carolina
I love your IT band tutorial. Is there any way that I can keep it forever, or maybe order a hard copy? This information is very valuable to me — I would like to be able to refer to it permanently.
Marilyn Anderson, Aspen, Colorado
Of course I hope it will be a book someday! Meanwhile, customers are welcome to electronically preserve and/or print my tutorials. ~ Paul
One more noteworthy endorsement, with regards to this whole website and all of my books, submitted by a London physician specializing in chronic pain, medical education, and patient-advocacy (that’s a link to his excellent blog):
I’m writing to congratulate and thank you for your impressive ongoing review of musculoskeletal research. I teach a course, Medicine in Society, at St. Leonards Hospital in Hoxton. I originally stumbled across your website whilst looking for information about pain for my medical students, and have recommended your tutorials to them. Your work deserves special mention for its transparency, evidence base, clear presentation, educational content, regular documented updates, and lack of any commercial promotional material.
Dr. Jonathon Tomlinson, MBBS, DRCOG, MRCGP, MA, The Lawson Practice, London
What about criticism and complaints?
Oh, I get those too! I do not host public comments on PainScience.com for many reasons, but emailed constructive criticism, factual corrections, requests, and suggestions are all very welcome. I have made many important changes to this tutorial inspired directly by critical, informed reader feedback.
But you can’t make everyone happy! Some people demand their money back (and get it). I have about a 1% refund rate (far better than average in retail/e-commerce). The complaints of my most dissatisfied customers have strong themes:
- Too negative in general. Some people just can’t stomach all the debunking. Such customers often think that I dismiss “everything” … which I disagree with.
- Too negative specifically. Some are offended by my criticisms of a treatment option that they personally use and like. Or sell!
- Too advanced. Although I work hard to “dumb” the material down, quite a few people still just find it too dense and dorky.
- Too simple. Some people think they already know everything about the topic. Maybe they do, and maybe they don’t. I always wish I could give these readers a pop quiz. 😉 In my experience, all truly knowledegable people get that way by embracing every new persective and source of information.
Acknowledgements
Thank you to Dr. Michels and his colleagues for their important, evidence-inspired work in pioneering a new surgical treatment for ITBS, with its fascinating implications. Thank you as well to Dr. Fairclough and his research colleagues who also deserve special mention for their seminal 2007 paper on IT band syndrome, which was a game-changer and instantly made this topic much more interesting to continue writing about.
Thanks to every reader, client, and book customer for your curiosity, your faith, and your feedback and suggestions, and your stories most of all — without you, all of this would be impossible and pointless.
Writers go on and on about how grateful they are for the support they had while writing one measly book, but this website is actually a much bigger project than a book. PainScience.com was originally created in my so-called “spare time” with a lot of assistance from family and friends (see the origin story). Thanks to my wife for countless indulgences large and small; to my parents for (possibly blind) faith in me, and much copyediting; and to friends and technical mentors Mike, Dirk, Aaron, and Erin for endless useful chats, repeatedly saving my ass, plus actually building many of the nifty features of this website.
Special thanks to some professionals and experts who have been particularly inspiring and/or directly supportive: Dr. Rob Tarzwell, Dr. Steven Novella, Dr. David Gorski, Sam Homola, DC, Dr. Mark Crislip, Scott Gavura, Dr. Harriet Hall, Dr. Stephen Barrett, Dr. Greg Lehman, Dr. Jason Silvernail, Todd Hargrove, Nick Ng, Alice Sanvito, Dr. Chris Moyer, Lars Avemarie, PT, Dr. Brian James, Bodhi Haraldsson, Diane Jacobs, Adam Meakins, Sol Orwell, Laura Allen, James Fell, Dr. Ravensara Travillian, Dr. Neil O’Connell, Dr. Tony Ingram, Dr. Jim Eubanks, Kira Stoops, Dr. Bronnie Thompson, Dr. James Coyne, Alex Hutchinson, Dr. David Colquhoun, Bas Asselbergs … and almost certainly a dozen more I am embarrassed to have neglected.
I work “alone,” but not really, thanks to all these people.
I have some relationship with everyone named above, but there are also many experts who have influenced me that I am not privileged to know personally. Some of the most notable are: Drs. Lorimer Moseley, David Butler, Gordon Waddell, Robert Sapolsky, Brad Schoenfeld, Edzard Ernst, Jan Dommerholt, Simon Singh, Ben Goldacre, Atul Gawande, and Nikolai Boguduk.
Warm thanks also to reader John J, who reported more typografic errors and other miner glitches in onelarge batch than I would ever have Dramed posssible so many years into the the lyfe of this documint. Many readers have helped out with such reporting, but John’s effort was truly remarkable.
What’s new in this tutorial?
This document was originally published as a much simpler article in 2002, based on keeping notes I’d been keeping on the topic since my own experience with ITBS in the late 90s. It was then expanded and republished as a book-length tutorial in April of 2007, and has been updated and revised regularly since then. An unusually large batch of improvements were made in 2012 in preparation for recording an audiobook.
Regular updates are a key feature of PainScience.com tutorials. As new science and information becomes available, I upgrade them, and the most recent version is always automatically available to customers. Unlike regular books, and even e-books (which can be obsolete by the time they are published, and can go years between editions) this document is updated at least once every three months and often much more. I also log updates, making it easy for readers to see what’s changed. This tutorial has gotten 158 major and minor updates since I started logging carefully in late 2009 (plus countless minor tweaks and touch-ups).
Mar 17, 2026 — New audiobook version: About a third of the chapters in the audiobook have now been replaced with fresh versions, following several waves of updates to chapters.
March — Editing: An all-over light editing while recording a new audio version. [Updated section: Steroid injections: a complicated mix of certain risks and uncertain rewards.]
March — Editing: A few minor improvements and one correction (I now know that it’s a bit of a myth that pill colour drives placebo). [Updated section: Some important things to keep in mind about placebos.]
March — More and better: Added some missing summaries of treatments, cleaned up some others, and quite a bit of general revision and modernizing. [Updated section: Treatment: What can you do about iliotibial band syndrome?]
March — Science updated: Updated the chapter with a discussion of Serighelli et al., who reported a correlation between hip joint noise and trouble. [Updated section: The noise, noise, noise! The significance of knee snaps, crackles, and pops.]
March — Editing: Cleaned up and modernized for new audio version. [Updated section: A new surgery works without ‘loosening’ anything.]
March — Science update: Cleaned up the chapter a bit and added a new citation to a case series of surgeries combining both old and new approaches (Arnal-Burró). [Updated section: The new surgery: excision of tissue from under the IT band.]
March — New chapter: No notes. Just a new chapter. [Updated section: Tendon failure as a drug side effect.]
February — Science update: A same-day update as the re-write of this chapter, but logged seperately because it was very much its own thing, complementary but seperate: a drop-in citation based on a lot of analysis of Yao. Click through to the bib page for the details on that paper. [Updated section: IT band syndrome may be more about physiological vulnerability than knee stress.]
February — Rewrite: Total revision of this chapter. It still discusses “failed healing” like the original, but almost everything else is different. Before: a minor chapter musing about some of the more medically mysterious cases. After: a substantial, evidence-based chaper that sheds some genuine light on the problem. [Updated section: IT band syndrome may be more about physiological vulnerability than knee stress.]
February — Science update: Added a citation to Sanchez-Gomez et al., justifying a recommendation to at least consider orthotics to limit supination. [Updated section: Orthotics for IT band syndrome: a worthwhile long shot.]
February — Science update: Added a citation to Sanchez-Gomez et al., as a good fresh example of very weak science about the role of the TFL in IT band syndrome. [Updated section: A “dysfunctional” tensor fasciae latae: one of the classic usual suspects.]
February — Science update: Cited He et al. on the state and history of ITBS research, and the most cited papers; Taunton et al. and Marais et al. on prevalence. [Updated section: Introduction.]
February — Science update: Added a discussion of ITBS induced by surgery, with a couple relevant new citations. Also added a citation to Manon on IT band microanatomy and its layering and fibre directions. General polish and editing. [Updated section: The old surgery: snipping the band.]
February — Science update: Cited Manon on the IT band microstructure (a cool study). [Updated section: So is it a tendon or what? IT bands are special.]
February — Editing: [Updated section: Friction syndrome? So where’s the rub? Is the IT band even “tight”?]
February — Science update: Cited Takagi et al., a very illuminating paper about four case studies of ITBS after knee replacement. [Updated section: Runner’s knee without running: post-surgical lateral knee pain.]
February — Science updated: Filled in an old blank, a much-cited 2010 paper by Powers that should have been here since at least 2015 just because it was so popular. And now it is, better late than never. I also added a much fresher citation to Leppänen et al., which is actually more important, and I'll probably make more of a meal of it soon. But for now it is acknowledged as a scientific point against my own bias on this topic. [Updated section: Hip strengthening is badly over-hyped.]
February — Science updated: Added big footnotes for Yao, a good example of very fancy-but-bad research (trying to make the case for hip weakness as a cause of ITBS); and Jahanshahi, another good example of a bad study (of functional motor control exercises). [Updated section: Hip strengthening is badly over-hyped.]
February — Science update: Cited and discussed two experiments showing reduced knee loading with shorter, quicker steps. [Updated section: Why does IT band pain gets so nasty so fast? A vicious cycle related to running pace.]
Archived updates — All updates, including 117 older updates, are listed on another page. ❐
2002 — Publication.
Notes
- “Many people are afraid of running because between 30 to 70 percent (depending on how you measure it) of runners get injured every year.” And many of those are IT band syndrome cases. That quote is from a fascinating talk about the athletic toughness of human beings, Brains Plus Brawn, by Dr. Dan Lieberman, evolutionary biologist of “Born to Run” fame.
- Marais JV, Jansen van Rensburg A, Schwellnus MP, Jordaan E, Boer P. Risk factors associated with a history of iliotibial band syndrome (hITBS) in distance runners: a cross-sectional study in 76 654 race entrants - a SAFER XXXIII study. Phys Sportsmed. 2024 Dec;52(6):568–578. PubMed 38618688 ❐
Marais et al. report that 1.63% of ~100,000 marathoners reported having ITBS over the previous year.
- Taunton JE, Ryan MB, Clement DB, et al. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med. 2002;36(2):95–101.
This report on two year’s worth of injuries among Vancouver runners — many of whom I probably run with routinely on Vancouver’s famous sea wall, or the Arbutus corridor Greenway — found that “patellofemoral pain syndrome was the most common injury, followed by iliotibial band friction syndrome, plantar fasciitis, meniscal injuries of the knee, and tibial stress syndrome.”
This is one of the top ten most cited papers about ITBS (according to He et al.).
- He F, Chen Y, Zeng S, et al. Research hotspots and current status of iliotibial band studies: A bibliometric analysis (1934-2023). Medicine (Baltimore). 2025 Jul;104(29):e43088. PubMed 40696678 ❐ PainSci Bibliography 49326 ❐
This unusual “bibliometric analysis” isn’t terribly informative, but it is a useful citation to emphasize the shabby state of the science, and a good overview of the ideas in the field. “The pathogenesis, prevention, and treatment of ITB-related diseases are controversial,” they write.
The entire ITBS literature consists of about about 1200 papers, most of that them published since 2000, peaked in recent history with just over a hundred papers in 2018 — very little for a condition that affects so many athletes. The selection is dominated by American research, with the UK, Germany, and Canada trailing far behind. He et al. also produced a useful top-ten list of the most cited papers in the field, which overlaps partially with the top 4 “high-quality” papers. They are all cited in this book. Unfortunately, and weirdly, fully half of them have almost nothing to do with ITBS (they are mostly about taking pieces of the ITBS for use in knee surgery for ACL injuries).
- The muscles that actually control the tension on the iliotibial band, such as the tensor fasciae latae and gluteus maximus.
Quadriceps strengthening is a standard treatment option for patellofemoral pain syndrome — another common overuse injury of the knee (more on this below). It doesn’t necessarily work even for that condition, or not for the reasons people think it does, but it is a nearly universal rehab choice for that condition, for better or worse. Not for ITBS, though! Although strengthening some muscles (hip and gluteals) has been proposed as a treatment for ITBS, and might work, quadriceps training has almost no relevance to ITBS. I assume that it gets prescribed anyway simply because these two knee pain conditions are often confused, even by pros who should know better — a simple case of mistaken identity.
Also, physical therapists just love to prescribe strength training. Like stretching, it’s dogmatically included in most rehab, regardless of whether it actually makes any sense.
- As they are of most musculoskeletal problems. Most doctors lack the skills and knowledge needed to care for common aches, pains, and injury problems, especially the chronic cases, which they tend to underestimate the complexity of. This has been shown by many studies, like Stockard et al., who found that 82% of medical graduates “failed to demonstrate basic competency in musculoskeletal medicine.” It’s just not their thing, and people with puzzling or stubborn pain should take their family doctor’s advice with a large grain of salt, and even lower their expectations of specialists (who tend to be too specialized). See The Medical Blind Spot for Aches, Pains & Injuries: Most physicians are unqualified to care for many common pain and injury problems, especially the more stubborn and tricky ones.
![Cartoon of a man sitting in a doctor’s office. The doctor is holding a clipboard with a checklist with just two items on it: stress related and age related. The caption reads: “An extremely general practitioner.”]()
There’s nothing formal or authoritative I can cite to support this position; there is no international standards organization defining minor musculoskeletal injuries; IT band syndrome isn’t even in the Merck Manual (a famous medical dictionary) or the Medline/Merrian Webster medical dictionary.
All obscure definitions are somewhat arbitrary and a product of social concensus, and so my position is based on the definition used in most academic writing and research on the topic. My strong impression after many years of writing about ITBS is that discussions and articles that talk about IT band syndrome as anything but a lateral knee pain condition are mostly amateurish, with ignorance of the condition prominently on display.
- Takagi K, Inui H, Taketomi S, et al. Iliotibial band friction syndrome after knee arthroplasty. Knee. 2020 Jan;27(1):263–273. PubMed 31883856 ❐
- Ingraham. A Historical Perspective On Aches ‘n’ Pains: Why is healthcare for chronic pain and injury so bad? PainScience.com. 3899 words. We can put a man on the moon, but we can’t fix most chronic pain. The science and treatment of pain was neglected for decades while medicine had bigger fish to fry, and it remains a backwater to this day. The seemingly simpler “mechanical” problems of musculoskeletal health care have proven to be surprisingly weird and messy. The field is dominated by obsolete conventional wisdom and the speculations of desperate patients and opportunistic cure purveyors. Ignorance is widespread thanks to professional pride and tribalism, ideological momentum, screwed up incentives, and poor critical thinking skills. But the worst single offender? The pernicious oversimplification of treating the body too much like it’s a complex mechanical device that breaks down: (“structuralism”).
- As of 2021, only just over 350 search results in PubMed! Compare that to 7700 for frozen shoulder, or 11600 for carpal tunnel syndrome. Also, more so in the case of iliotibial band syndrome than other conditions, a great number of those papers are tutorials for professionals, not primary research. To an amazing degree, they all tend to repeat conventional wisdom and reference each other and clinical experience instead of original science.
- Ellis R, Hing W, Reid D. Iliotibial band friction syndrome — A systematic review. Man Ther. 2007. PubMed 17208506 ❐
This 2007 scientific review paper makes it extremely clear that there is a “paucity in quantity and quality of research” about iliotibial band syndrome. They also conclude that what information exists is not particularly helpful! “There seems limited evidence to suggest that the conservative treatments that have been studied offer any significant benefit in the management of ITBFS.” Yet it is absolutely routine for therapists and doctors, and even so-called experts, to make claims of therapeutic effectiveness! What are they basing that optimism on? The truth is, they simply don’t really know what they are talking about. They can’t — no one does!
- In my own 3000 hours of training — three full years of nothing but studying aches and pains and how to treat them — ITBS was barely even mentioned. Unless a massage therapist has gone out of his or her way to study the condition, he or she knows no more than anyone else who spends twenty minutes looking it up on the Internet … and perhaps less!
- This is not a joke. It’s an impressive-looking, conventional sports injury textbook — but its inadequate coverage of ITB syndrome is typical for the subject. The text is Clinical Guide to Sports Injuries.
- Grant HM, Tjoumakaris FP, Maltenfort MG, Freedman KB. Levels of Evidence in the Clinical Sports Medicine Literature: Are We Getting Better Over Time? Am J Sports Med. 2014 Apr;42(7):1738–1742. PubMed 24758781 ❐
Things may be getting better: “The emphasis on increasing levels of evidence to guide treatment decisions for sports medicine patients may be taking effect.” Fantastic news, if true! On the other hand, maybe I should be careful what I wish for, since my entire career is based on making some sense out of the hopeless mess that is sports and musculoskeletal medicine …
- Falvey EC, Clark RA, Franklyn-Miller A, et al. Iliotibial band syndrome: an examination of the evidence behind a number of treatment options. Scand J Med Sci Sports. 2010 Aug;20(4):580–7. PubMed 19706004 ❐ “Our results challenge the reasoning behind a number of accepted means of treating ITBS.”
- Sutker AN, Barber FA, Jackson DW, Pagliano JW. Iliotibial band syndrome in distance runners. Sports Med. 1985;2(6):447–451.
- Almeida SA, Williams KM, Shaffer RA, Brodine SK. Epidemiological patterns of musculoskeletal injuries and physical training. Med Sci Sports Exerc. 1999 Aug;31(8):1176–82. PubMed 10449021 ❐ PainSci Bibliography 56967 ❐
In a study of 1300 US Marine Corp recruits in training, nearly 40% got hurt, and 78% of them got repetitive strain injuries, and those injuries tended to happen during the weeks with the most training. “The most frequent site of injury was the ankle/foot region (34.3% of injuries), followed by the knee (28.1%). Ankle sprains (6.2%), iliotibial band syndrome (5.3%), and stress fractures (4.0%) were the most common diagnoses.” The findings suggest that “[vigorous] training, particularly running, and abrupt increases in training volume may further contribute to injury risk.”
- In Clinical Guide to Sports Injuries, on p340, iliotibial band syndrome is listed as a “less common” cause of knee pain, after the “most common” conditions of patellofemoral syndrome, patellar and quadriceps tendinopathy, meniscus injuries and knee instability … all of which contradicts my own experience. I saw more iliotibial band syndrome in my decade of clinical practice than all of those other “more common” conditions combined. This may reflect the nature of my practice more than reality for the rest of the world, but I’m just sayin’ — it was quite a lot.
- This is surprisingly hard to prove, because the vast majority of ankle sprains are minor and go unreported and untreated. However, clinical experience and many years of personal experience playing ultimate (a Frisbee team sport with an intensity like soccer) indicates that ankle sprains are probably more common than any other significant injury.
- Some papers that mention cycling: Ellis, Fairclough, Fredericson, Martens, Farrell.
- Linde F. Injuries in orienteering. Br J Sports Med. 1986;20(3):125–127.
From the abstract: “Medial shin pain, Achilles peritendinitis, peroneal tenosynovitis and iliotibial band friction syndrome were the most frequent overuse injuries [in 42 orienteers].”
- Takagi 2020, op. cit. This is discussed in both the post-surgical ITBS chapter, and the surgery chapter.
- Fairclough J, Hayashi K, Toumi H, et al. The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome. J Anat. 2006 Mar;208(3):309–316. PubMed 16533314 ❐ PainSci Bibliography 56738 ❐
ABSTRACT
Iliotibial band (ITB) syndrome is a common overuse injury in runners and cyclists. It is regarded as a friction syndrome where the ITB rubs against (and 'rolls over') the lateral femoral epicondyle. Here, we re-evaluate the clinical anatomy of the region to challenge the view that the ITB moves antero-posteriorly over the epicondyle. Gross anatomical and microscopical studies were conducted on the distal portion of the ITB in 15 cadavers. This was complemented by magnetic resonance (MR) imaging of six asymptomatic volunteers and studies of two athletes with acute ITB syndrome. In all cadavers, the ITB was anchored to the distal femur by fibrous strands, associated with a layer of richly innervated and vascularized fat. In no cadaver, volunteer or patient was a bursa seen. The MR scans showed that the ITB was compressed against the epicondyle at 30 degrees of knee flexion as a consequence of tibial internal rotation, but moved laterally in extension. MR signal changes in the patients with ITB syndrome were present in the region occupied by fat, deep to the ITB. The ITB is prevented from rolling over the epicondyle by its femoral anchorage and because it is a part of the fascia lata. We suggest that it creates the illusion of movement, because of changing tension in its anterior and posterior fibres during knee flexion. Thus, on anatomical grounds, ITB overuse injuries may be more likely to be associated with fat compression beneath the tract, rather than with repetitive friction as the knee flexes and extends.
- Fairclough J, Hayashi K, Toumi H, et al. Is iliotibial band syndrome really a friction syndrome? Journal of Science & Medicine in Sport. 2007 Apr;10(2):74–76. PubMed 16996312 ❐
ABSTRACT
Iliotibial band (ITB) syndrome is regarded as an overuse injury, common in runners and cyclists. It is believed to be associated with excessive friction between the tract and the lateral femoral epicondyle-friction which 'inflames' the tract or a bursa. This article highlights evidence which challenges these views. Basic anatomical principles of the ITB have been overlooked: (a) it is not a discrete structure, but a thickened part of the fascia lata which envelops the thigh, (b) it is connected to the linea aspera by an intermuscular septum and to the supracondylar region of the femur (including the epicondyle) by coarse, fibrous bands (which are not pathological adhesions) that are clearly visible by dissection or MRI and (c) a bursa is rarely present, but may be mistaken for the lateral recess of the knee. We would thus suggest that the ITB cannot create frictional forces by moving forwards and backwards over the epicondyle during flexion and extension of the knee. The perception of movement of the ITB across the epicondyle is an illusion because of changing tension in its anterior and posterior fibres. Nevertheless, slight medial-lateral movement is possible and we propose that ITB syndrome is caused by increased compression of a highly vascularised and innervated layer of fat and loose connective tissue that separates the ITB from the epicondyle. Our view is that ITB syndrome is related to impaired function of the hip musculature and that its resolution can only be properly achieved when the biomechanics of hip muscle function are properly addressed.
The science of anatomy was slow to develop historically, and remains surprisingly half-arsed. One good example from 2015 is the somewhat embarrassing discovery of lymphatic vessels in the central nervous system. Oops, how’d we miss that?
My Heart Will Go On, by Robert Krulwich & Adam Cole, explores the goofiness of historical beliefs about anatomy, especially the heart. The influential Roman physician Galen made many declarations about human anatomy without ever doing a human dissection, and then no one else checked his work for another 1000 years, and so everyone thought that the liver was a pump just like the heart. Those crazy Romans! And everyone who trusted them for a millenium!
Don’t be too quick to laugh, though. Modern people still have many odd misconceptions about anatomy (albeit less glaring that “the liver is a pump”). The significance of anatomical variations is chronically underestimated by everyone but surgeons. And it’s amazing how many people swear by treatments with anatomically dubious or impossible premises. Such as wrong IT band anatomy! And the significance of variations is chronically underestimated by everyone but surgeons.
- Devan MR, Pescatello LS, Faghri P, Anderson J. A Prospective Study of Overuse Knee Injuries Among Female Athletes With Muscle Imbalances and Structural Abnormalities. J Athl Train. 2004;39:263–267. PubMed 15496997 ❐ PainSci Bibliography 56601 ❐ For a more detailed analysis of this research, see The Causes of Runner's Knee Are Rarely Obvious.
- Followed, predictably, by patellofemoral pain syndrome.
- I’ll cover this in more detail below, but basically there’s good evidence that the Ober test is not a good way to judge the tightness of IT bands (see Willett).
- Anyone who has felt that knows exactly what I mean, but the sensation eludes many people, because it’s difficult to apply enough tension to the IT band to achieve it. Many people will simply never feel it. More about this in the stretching section.
- More detail: most tendons could be snipped at either end and then tied in a bow. They are mostly disconnected from other tissues, except at the ends where they are attached to muscle and bone. In contrast, the iliotibial band is simply a massive thickened section of the sausage wrapping of connective tissue that surrounds the whole thigh.
- Eng CM, Arnold AS, Lieberman DE, Biewener AA. The capacity of the human iliotibial band to store elastic energy during running. J Biomech. 2015 Sep;48(12):3341–8. PubMed 26162548 ❐ This paper presents the abstract and speculative “results” of a thought experiment aided by a fancy model of the leg, so it can’t be taken too seriously, and in particular it has no clear clinical implications. But it is interesting! Mostly it purports to show that the IT band stores elastic energy, much like the achilles tendon, just a lot less: “1J of energy per stride during slow running and 7J during fast running,” which is “approximately 14% of the energy stored in the Achilles tendon at a comparable speed.” If that’s how it actually works, it’s a handy biological adaptation that makes running a little more efficient: more evidence that we are “born to run.”
- Vieira ELC, Vieira EA, da Silva RT, et al. An anatomic study of the iliotibial tract. Arthroscopy. 2007;23(3):269–274.
- Putzer D, Haselbacher M, Hörmann R, Klima G, Nogler M. The deep layer of the tractus iliotibialis and its relevance when using the direct anterior approach in total hip arthroplasty: a cadaver study. Arch Orthop Trauma Surg. 2017 Dec;137(12):1755–1760. PubMed 29032422 ❐ PainSci Bibliography 53147 ❐
- Claes S, Vereecke E, Maes M, et al. Anatomy of the anterolateral ligament of the knee. J Anat. 2013 Oct;223(4):321–8. PubMed 23906341 ❐ PainSci Bibliography 49986 ❐
Clearly “new” anatomy is interesting to people, and so — despite its dubious relevance to ITBS — this is one of the top ten most cited papers about ITBS (according to He et al.).
Addendum: There are seven more papers on that list of most-cited ITBS papers! Getgood, Getgood, Dodds, Vincent, O'Brien, Beynnon, Kvist … these are all mostly about ACL injuries and their surgical management, which sometimes uses pieces of the IT band like a patch. They offer no insight into ITBS at all, so it’s not clear why they are being widely cited in the ITBS literature! I’m only including them here because they’re being cited so much, and not because they’re actually relevant.
- Manon J, Gallant L, Gérard P, et al. 2D and 3D microstructural analysis of the iliotibial tract. J Anat. 2024 Nov;245(5):725–739. PubMed 39213384 ❐ PainSci Bibliography 49324 ❐
Connective tissue helps link the skin, muscles, and deeper structures of the body, but its fine structure varies by location and remains poorly understood. This study examined the iliotibial tract, a huge tendon-like structure on the side of the thigh, to describe how its internal structure changes along its length.
Manon et al. used both standard microscopy and a high-resolution 3D imaging technique, cryogenic contrast-enhanced computed tomography: tissue samples are frozen to preserve their natural structure, then soaked in a contrast agent that makes soft tissues visible to X-rays. They are then scanned with micro-CT, producing very high-resolution 3D images of the tissue without cutting it into slices. This is a way to see the internal structure of soft connective tissue intact and in three dimensions, with much higher fidelity than standard histology alone.
They measured IT band thickness, layering, and fibre direction in different regions. Overall thickness varied by location, with the upper portion tending to be thicker and the lower portion showing the greatest variation from front to back. The IT band usually consisted of two layers, though some regions had one or three.
The middle layer was generally the thickest and contained fibres running mostly along the length of the band, while the outer and inner layers had fibres running more across it. The 3D imaging confirmed these distinct fibre patterns and showed that fibres running across the band were straighter, while lengthwise and angled fibres were more wavy.
These findings show that the IT band is not a uniform structure but varies in thickness, layering, and fibre organization depending on location. The use of advanced 3D imaging provides a clearer and more accurate picture of IT band structure, supporting future biomechanical and clinical research.
This paper is fundamentally descriptive, and any clinical implications are necessarily indirect. But there are a few non-hand-wavy clinical implications:
- Refined biomechanical model of IT band syndrome — The data challenges the common simplification of the IT band as a uniform, strap-like structure. More realistic models of load transmission, strain distribution, and shear between layers could help explain why symptoms localize preferentially (e.g., distal–lateral femur) and why certain movements provoke pain.
- Supports strain-based rather than friction-based mechanisms of ITBS — Distinct fibre orientations and differential tortuosity across layers is consistent with the idea that IT band syndrome involves complex internal strain and inter-layer shear, much more complex than just “rubbing” over the lateral femoral epicondyle.
- Informs surgical planning and tissue handling — For release procedures, knowing that the ITT is multilayered with region-specific fibre orientations could help surgeons choose where and how to cut, avoiding indiscriminate releases/resections that disrupt load-bearing layers.
- Constrains expectations for physiotherapy techniques — The finding that fibres are highly organized, layered, and region-specific places realistic limits on what manual therapies (e.g., “fascial release”) can plausibly alter at the microstructural level. While this does not invalidate physiotherapy, it suggests effects are more likely neuromodulatory or load-management–related than structural “remodelling” of fibres.
This study gives us a good refinement of current biomechanical understanding of the iliotibial tract, demonstrating region-specific microstructural organization, which may help explain localized strain patterns implicated in iliotibial band syndrome and inform both surgical approaches and conservative load-management strategies.
- How is this possible? Fairclough et al. explain that “our cadaveric dissections confirm that the ITB is simply a thickened, lateral part of the fascia lata. It completely surrounds the thigh, is anchored to the femoral shaft by the lateral intermuscular septum.” In general, muscle sheaths are no more free to move relative to the muscle they contain than a sausage wrapper is free to move relative to the sausage. In this case, the wrapping is even more fixed, because it actually penetrates to the bone, attaching to the femur along most of the length of the femur (on the linea aspera). This was backed up by another dissection study in 2009, which also found that the IT band is “uniformly” and “firmly” attached to the thigh bone, “from greater trochanter up to and including the lateral femoral condyle” — in other words, the full length of the thigh. This thing does not slide around.
- As the knee bends, tension on the IT band shifts from the front to the back. That is, it “pops out” a bit, first a little ahead of the knee, then further back — which can look an awful lot like movement. But it’s just parallel fibres tightening in sequence, like a wave, as the knee changes position. Other tendons actually do slide around and snap over other structures, but the IT band is not free to do this.
- Although this has been contradicted by other evidence — Jelsing 2013 — for now I’m working with the assumption that any movement is probably trivial and not a sliding at all, like the slight swaying of seaweed anchored to rocks in shallow water. That is, it’s not “rubbing” back and forth so much as flexing to and fro.
I often hear athletes, trainers, and therapists talking about the anatomy of injuries with great ignorance and confidence — a nasty combination. They believe pain is coming from a part of them that literally doesn’t exist, or not in that neck of their woods.
Many lesser-trained professionals make so many mistakes with basic anatomy that it’s clear that they could not pass an anatomy exam … like the massage therapist I saw once who tried to base his treatment of me on an entirely imaginary muscle — a weird hybrid of two or three others, like the quadriglutator or the sternobiceptoid. (I would have laughed, if he hadn’t been carelessly handling my fairly badly injured shoulder at the time, trying to find my … whatever he thought he was looking for.) It may sound absurd, but we live in a world where some people believe that ketchup is a vegetable — and anatomy is much harder than food classification. It’s one thing to be wrong, but the overconfidence of these anatomical fantasies really tickles my funny bone.

{kind=link}
There are 233 more footnotes in the full version of the book. I really like footnotes, and I try to have fun with them.
Jump back to:
The introduction
Paywall & purchase info
Table of contents
Top of the footnotes
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help