Tissue Provocation Therapies in Musculoskeletal Medicine
Can healing be forced? The theme of hormesis in pain and injury medicine

Adapting? Or failing?
How tissue copes with stress is still remarkably mysterious.
“What doesn’t kill you makes you stronger.” Except, it doesn’t always! We can only adapt to so much stress so quickly — but it’s almost miraculous when we do adapt. How does tissue adaptation work? How good at it are we really? And can it be exploited for a treatment effect? Several popular therapies for pain and injury are based on this idea. Popularity, unfortunately, is no guarantee that they are actually useful. These are the most notorious examples of provocation therapies, and they are all a bit sketchy:
- Prolotherapy — Injecting an irritant to provoke scar tissue formation.
- Eccentric loading — A type of contraction often prescribed treat tendinitis.
- Trigger point therapy and dry needling — Applying strong pressure to “muscle knots,” or even lacerating them with needles.
- Shockwave therapy — An intense cousin of ultrasound that uses much slower but stronger pressure waves — enough to physically damage tissue. Its biological effects are putatively regenerative.
- Scraping massage — The IASTM modalities like Graston, Astym, gua sha.
Tough love and hormesis: the logic of provocation therapies
You gotta be
Cruel to be kind in the right measure
Cruel to be kind it’s a very good sign
Cruel to be kind means that I love you
Baby, you gotta be cruel to be kindNick Lowe, Cruel To Be Kind
Many treatment strategies for chronic pain and injury are based on the dubious idea of forcing tissues to adapt, and the hope that they can be “toughened up.” These are the provocation therapies (my own term). They claim to cure with small doses of stress and damage — and sometimes much larger doses. It’s an emotionally compelling treatment idea, based on a genuine seed of truth. It’s pervasive in our culture, an idea that has been expressed many ways:
- No pain, no gain.
- What doesn’t kill you makes you stronger.
- What hurts the most, helps the most.
- You have to break some eggs to make an omelette.
- Pain is a sign of weakness leaving the body.
Maybe it’s right, or half right. Maybe it’s a cliché for good reason … or maybe that just makes it a terrific engine for placebo.
A closely related technical term is “hormesis”: a beneficial effect of a small dose of something that would be dangerous at a high dose. “The dose makes the poison” — but a low dose of some things may not just merely harmless, but actually therapeutic. Exercise is the classic simple example: it is well known to force healthy adaptation as a response to minor damage. Take it too far, though, and you will definitely get hurt.
But can that effect be harnessed by your physical therapist? Can it be applied to passively with a tool? Will the body respond adaptively to an entirely artificial, contrived stimulus?
And — most important — is that stimulus going to be clinically useful for tissues that are already in some kind of trouble? That’s a much more profound interpretation of the significance of hormesis, which benefits from the aura of legitimacy from its simpler interpretation. Maybe hormesis is just another “deepity”: an idea with a simple interpretation that is true but trivial, or a deeper and more sensational interpretation that’s bullshit.
Obey the (tissue adaptation) law — you really have no choice!
This is all about how tissue adapts to stimuli and stressors. So how do they?
There are two “laws” of tissue adaptation, one each for hard and soft tissue. Wolff’s law is that bone will adapt to loading. This was first noticed by Julius Wolff in the 19th Century, who got the naming rights. It was greatly refined in the mid 20th century by Dr. Harold Frost, an American surgeon who studied bone biology (and published scientific papers more often than I change my socks). The full details of how bone responds to stress are described in his Mechanostat model.1 A great example of Wolff’s law at work is found in pro tennis players: the humerus in their dominant arm is bigger by 16–21%.2
Bones serve as the Federal Reserve for the body’s calcium, constantly giving and collecting loans of calcium to and from other organs. And part is for the sake of bone itself, allowing it to gradually rebuild and change its shape in response to need. How else do cowboys’ bow-legged legs get bowed from too much time on a horse?3
Robert M Sapolsky, Why Zebras Don’t Get Ulcers, 2004, p. 115.
But bone cells are trapped deep in rigid bone. As biologist Dr. Sheldon Weinbaum put it, they “live in caves.” How do they know what’s going on? How can bone adapt to anything? There are several mechanisms. It’s worth going over a couple of them.
- Bone uses microscopic fluid-filled tubes to detect bone stress. The moving fluid tugs on incredibly fine cellular feelers in the tube, and the signals tell bone cells how much bone to make or dissolve. This system fails in zero gravity … which is how we figured it out. The system fails in astronauts.4
- Equally cool is the way bone uses piezoelectric effect as a signalling mechanism. This was discovered by an orthopedic surgeon, Robert Becker, way back in the 70s, and described in his fascinating book, The Body Electric (this website has a salamander logo because of that book). Piezoelectric effect is a tiny electrical current produced by deformation of a crystal. Bone, as it happens, has a crystalline structure. As the structure is ever-so-slightly flexed by stresses, it lights up with tiny electrical signals to the cells, telling them exactly where the stress is being felt. Clever!
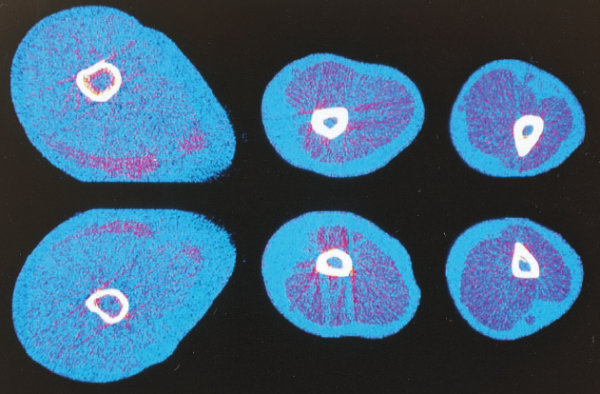
Cross-sections of a former pro tennis player’s dominant upper arm (top row) compared to his other arm (bottom row). The bone in the dominant arm is about 18% bigger. That’s Wolff’s law at work. Source: Haapasalo 2000
Going soft: Davis’ law
The corollary of Wolff’s law for soft tissue is the obscure and much less developed Davis’ law.5 Although there’s no question soft tissue does adapt to stress, the responses of muscles, tendons, ligaments, and intervertebral discs are much more complex and less well understood. Bone is one tissue, but “soft tissue” is a whole spectrum of tissues, with diverse functions and properties, as varied as the inhabitants of a zoo.
In its mildest form, Davis’ law is simply the “use it or lose it” principle: the growth of muscles in response to exercise, say. At the other extreme of stress — trauma — scarring is a fairly obvious soft tissue “adaptation.” An intermediate example would be the way we can “seize up” — everything from minor transient sticky adhesions between layers of tissue, to significant shortening of structures. Heavily used tendons go through a complex progression of responses to stress that leads to repetitive strain injury if pushed too far.
Flexibility is a wonderfully complex example. On the one hand, it’s obvious that the soft tissues of extremely flexible athletes like dancers, gymnasts and martial artists have been changed by years of stretching regimens — often brutal and injurious. For most of the rest of us, however, there’s good evidence that flexibility changes are all in the mind: a neurological adaptation, and not a change in the tissue.6 Does a difference in the behaviour of physical unchanged soft tissue count as an example of Davis’ law? Your guess is as good as mine — it’s an almost philosophical question.
The Twa people of Africa provide another great example. A lifetime of climbing trees leads to amazing ankle mobility:7
These guys have a huge range of motion into dorsiflexion. They can get their foot almost forty five degrees to the shin. (The normal range of motion for a westerner is about ten to twenty degrees.) This allows them to get their body weight closer to the tree which makes climbing much easier.
Barefoot Running, Squatting Like a Baby, and Pygmy Feet, Hargrove (BetterMovement.org)
Finally, the best example of all: we now know, thanks to first evidence of its kind published in 2017, that intervertebral discs do adapt to exercise.8 These structures have always been considered one of the least adaptable soft tissues. For decades, almost everyone has assumed that the jarring impact of running constitutes a source of relentless wear and tear on the spine, and that the discs in particular probably cannot keep up with the onslaught, and aren’t able to adapt and recover — a slow losing battle. Specifically, data on “turnover rates” — how quickly tissue is replaced — have “lead to the assumption that positive adaptation in the mature intervertebral disc is unlikely to occur during the normal human lifespan.”
But that’s all wrong: the lumbar intervertebral discs actually adapt well to the forces involved in running. They get fatter and juicier! Tellingly, not just any old running will do, and it’s not a straightforward more-is-better relationship. It’s quirky. There is a sweet spot, but it’s in the pacing, not the volume: regardless of distance, the discs adapt best to a moderate speed, a just-right amount of impact found in slow running and fast walking. Only careful research will elucidate exactly what it takes to coax adaptation out of tissues.
The SAID principle: another basic concept in adaptation
The Specific Adaptation to Imposed Demand (SAID) principle is a very basic concept in sports science and physiology, almost as basic and general as “use it or lose it.” When the body is placed under any form of stress, it starts to prepare to deal with that kind of stress better in the future — if it can. Many kinds of adaptation fit under this umbrella. As put by Todd Hargrove, “it is a general tendency of the body which is played out in innumerable separate mechanisms.”
The most basic implication of SAID is that you will get better at whatever you practice. It also implies that you will mainly or only get better at what you practice. Push-ups are a classic example of an exercise that is mostly good for getting better at push-ups and enlarging pectoral muscles, but not much of anything else, because there aren’t many athletic or occupational activities that benefit significantly from that kind of strength.
Here’s a more detailed example: you can improve your balance with conventional strengthening of the trunk (sit‐ups and back extensions) or trunk stabilization exercises (plank, quadruped exercise, and back bridging)… but the latter works better, because it involves more actual balancing.9 And SAID principle says that the best way to get a good score on the Star Excursion Balance Test is to … do the test a lot. 🙂
The potency bias
Provocation therapies might be effective. But it’s more likely that the strong sensations they produce are rocket fuel for robust placebo effects. This is an important perspective on any treatment that supposedly works because of its intensity.
People equate strong sensations in a medical context with therapeutic potency. In short, we really believe that there is no gain without pain, and we assume that pain is justified by gain.
A funny example: people love to love Buckley’s cough syrup, a notoriously foul-tasting Canadian “medicine” with no conventional active ingredients, just gross ones like lots of camphor and pine needle oil, advertised with the slogan, “It tastes awful. And it works.” That slogan taps directly into the pro-potency bias! It’s practically an explanation for it. People can’t love Buckley's because it’s actually effective, because it cannot possibly be, so they love it simply because the taste is horrifying … and they think intense medicines must be more potent. Surely no one would sell such diabolical swill if it wasn’t good medicine?! Right?
It’s a bit of a myth that placebo can be enhanced by factors as subtle as pill colour. However, it remains generally true that patient expectations are inflated by how "serious" or dramatic a treatment seems. This why we see stronger placebo effects from needles than pills, and why surgery is the ultimate placebo, because it is a very dramatic medical intervention, and that extremity is equated with efficacy to an astonishing degree (see Surgery: The ultimate placebo).
I see this in the world of manual therapy and rehab constantly, in many forms.
And nowhere is the potency bias more obvious than with the provocation therapies! So now let’s look at some specific examples…
Prolotherapy
Prolotherapy is the ultimate, classic provocation therapy in orthopedic and musculoskeletal medicine. A portmanteau of “proliferative therapy,” it was invented by a charismatic doctor decades ago to treat back pain by toughening up ligaments by injecting them with an irritant.10 These days we know that “weak ligaments” are not why people get back pain,11 and so it’s not too surprising that the direct evidence for prolotherapy has always been inconsistent and unimpressive at best. Prolotherapy’s earnest founder got great results in his own clinic … but his results couldn’t be reproduced under controlled conditions, by anyone else, ever again. It did not even begin to stand the test of time.
And yet it will not die. It continues to be tried for many conditions. There are promising-but-unconvincing shreds of evidence here and there.12 An allegedly evidence-based comeback in the 2010s was not impressive. The method is so notoriously sketchy and persistent that it’s an easy target for satire:
The patient who was randomized to the prolotherapy had a 0.4 improvement in their pain on the Wong-Baker scale after taking motrin. The Kool-Aid recipients had worse pain scores after the injections, so clearly we proved that prolotherapy works. No point doing any more research!
“Sports Med Doc Performs RCT Comparing Koolaid vs Prolotherapy,” GomerBlog.com (“The Onion for doctors”)
I have a much more detailed review of prolotherapy for back pain in my low back pain tutorial.
Eccentric loading
A modern and ordinary example of provocation therapy is eccentric loading (contracting while lengthening) for tendinitis.13 This is most often seen in the form of a heel drop exercise for Achilles tendinitis.
Eccentric contractions are (curiously) a more challenging stimulus than regular contractions — they do consistently make people much more sore after exercise (delayed-onset muscle soreness). And, to the extent that eccentric loading makes us sore, it’s obviously a provocative stimulus, causing minor damage and then adaptation in the muscle and tendon — just like other strength training!
Eccentric loading can be considered a provocation therapy insofar as it is often performed with the intention to deliberately cause that soreness, to generate a “stronger signal” for the body to adapt to. But is the soreness produced by eccentric exercise actually physiologically different? Or is it just that you cause it a little more efficiently? Is there are any difference between achieving that soreness with eccentric contractions versus regular concentric contractions?
Not really, no. Many experts are just not impressed by eccentric exercise therapy, despite a sprinkling of positive studies: “There is no convincing clinical evidence to demonstrate that isolated eccentric loading exercise improves clinical outcomes more than other loading therapies.”14 If exercising eccentrically is actually useful in rehab, it is not clearly established yet.15
Scraping massage: instrument-assisted soft tissue mobilization (IASTM) modalities like Graston, Astym, gua sha)
In January 2026 this section got too big for its britches, and I condensed it to a summary of a complex topic. But I’ve written much more about it now! If you’d like all the details, especially a full science review, see Scraping massage with tools: gua sha and Graston (Member Post) (temporarily members-only, until later this year).

{kind=link}
Care for a little scraping massage? The steel massage tools of Graston Technique®.
Gua sha literally means scraping and bruising massage therapy, an ancient folk medicine practice in Asia. Like acupuncture, gua sha is used in the West, powered by Asian fetishism, but it has also been re-branded with vague pseudoscientific justifications and “advanced” scraping tools and methods. It is now best known as the eponymous Graston Technique (GrastonTechnique.com), but there are others — mainly Astym® and HawkGrips (Hawk IASTM) — the “clinical” brands, known as instrument-assisted soft tissue mobilization (IASTM).
And you can’t get much more “provocative” than the faddish FasciaBlaster! This consumer product is pitched mainly as a cosmetic self-treatment for cellulite — also routinely recommended as a treatment for painful conditions. Bruising is common in practice (sometimes severe), regardless of whether it is endorsed by the manufacturer.
All kinds of scraping massage uses rigid tools — plastic, ceramic, steel, stone, bone, often with a sharp edge — and has goals like “breaking down scar tissue” and “releasing” speculative fascial restrictions.16 IASTM is uncomfortable (at least) when used for those purposes; it is mostly aimed at tissues that are themselves chronically painful and possibly fragile. Treating painful tissues with painfully stressful treatments is truly in the spirit of all the provocation therapies, and so IASTM also always a little risky. It is broadly impossible to achieve the routinely stated goal of releasing fascial restrictions without also breaking some muscle cells. Skin infections are also more of a risk that most people would guess.
Scraping massage is probably not very dangerous on average for health patients in a clinical context. But a surprising number of people aren’t healthy (see “tissue fragility” sidebar). And even safe discomfort and unpleasantness are only justified by strong evidence of efficacy. Without that, then it’s just mild, expensive torture.
So what does the science say? Hardly anything! It is thin and very “pseudo.” Some minor benefits for some people are conceivable, but not particularly plausible; it’s much likelier that this is just another manual therapy ritual that is more therapy theatre than healthcare.
And of course the many claims of high success rates are almost nonsense by definition. As of early 2026, Astym.com claims a 96.5% success rate — a huge red flag for any thinking person.17 It’s just more marketing — which is what drives most of this industry rather than science.
Are trigger point therapy and dry needling “provocative”?
Trigger point therapy refers to a diverse group of treatments methods for the sore spots or “muscle knots” associated with stiffness and aching. While no one disputes that such pesky spots exist and are common and occasionally quite fierce, they are controversial in almost every other way: how they work, how important they are clinically, and whether and how they can be treated in any case. Trigger point therapy was massively popularized by Dr. Janet Travell in the 1980s and 90s, and has been a staple of massage therapy ever since. As I have explained in great detail elsewhere,18 I consider trigger point therapy to be a legitimate experimental therapy, ethically defensible and potentially useful if delivered with humility, informed consent, in modest doses.

Most trigger point therapy boils down to trying to destroy them with pressure, like popping zits.
Unfortunately, people rarely get their trigger point therapy like that. Most massage therapists don’t know much about the messy and limited science of sore spots, and rationalize their efforts simplistically, with a tendency to get a bit brutal when they believe they are hunting evil spots in your muscles. Out, damn spot! And so trigger point treatment is routinely delivered in a style that amounts to a provocation therapy: basically trying to beat trigger points into submission. In some cases, that is the actually stated intent: to “break” the trigger point in one sense or another!
But that’s nothing!
Dry needling
“Dry needling,” widely practiced by physiotherapists, is the practice of literally stabbing trigger points with acupuncture needles. The rationale for this practice is sloppy and is often just a lightly jargonized version of “kill it with needles.” As with massage, dry needling for trigger points as often practiced is a kind of provocation therapy.
You can find lots of information online about dry needling, but basically none of it is (a) detailed, (b) skeptical, and (c) referenced. But you can find that kind of information about dry needling in my book about trigger point therapy.
Shockwave therapy
Shockwave therapy is the ultimate example of a therapy that is not only provocative, but in a way that is specifically touted to be regenerative, with at least superficial support from a lot of research into its biological effects.
Shockwave is a cousin of ultrasound that uses high-intensity pressure waves to slap tissues: much bigger and faster than ultrasound's waves, and also at much lower frequencies (infrasonic). Weirdly, it’s a lot like a massage “gun” that produces more potent and penetrating vibrations.
Shockwave therapy is also more painful than ultrasound or massage guns because … it actually does damage. Not a lot, of course. It’s “microtrauma”: minor, diffuse damage, which is sometimes obvious due to minor bruising, but mostly only visible in a microscope.
Cells react to practically any stimulus … but is it a useful reaction?
And the point, of course, is that a little damage will “kickstart healing” — the inevitable metaphor. Stated more grandiosely, the core hypothesis of shockwave therapy is that microtrauma hormetically stimulates cellular regenerative processes? Oooh, that’s more like it! Talk nerdy to me, baby!
Cells will respond to many stimuli in some way, so it’s not surprising that shockwave therapy has measurable effects on tissue. But all those intriguing biological effects are meaningless noise if they don’t translate into meaningful clinical benefits.
And they don’t.
There is seemingly positive research, of course, and it is constantly touted by the people selling shockwave therapy, but it all follows the usual depressing pattern in this business: just junky little studies showing unimpressive effects, contradicted by a handful of higher quality ones that show little or nothing.19
I discuss the details thoroughly in my full guide to ultrasound and shockwave therapy.
What could possibly go wrong?
It’s not hard to imagine! Clearly there is a risk of hurting instead of helping. The physiology of adaptation may be impressive, but it’s just as clear that too much stress is injurious. And one person’s “just right” may well be the next person’s “too much.”
We also now know, thanks to the last 20 years of pain science, that chronic pain may often be due to a failure of nervous system itself. Many people with serious chronic pain problems — the same desperate patients who might try something riskier — are probably pathologically oversensitive. Pain can make us more sensitive to more pain.20 What happens if you “stress” a nervous system in that condition? The problem could get worse, not better.
And, finally, brand new research has shown quite conclusively (and graphically, on video!) that inflammation can be actively destructive to tissues: like a gang of insane firefighters, immune cells deliberately over-react and destroy healthy cells just in case there might be an infection.21 This response is exactly what we want for open wounds, but overkill for all minor internal injuries — like tendinitis. Indeed, it may be a major reason for the stubbornness of conditions like tendinitis. Any provocative, intense treatment unquestionably has the potential to provoke exactly this reaction.
Potentially dangerous treatments should never be sold to patients on the basis of scant data. We shouldn’t take risks without proven potential for benefit. There is no reason to think that it will necessarily go well to provoke tissue, and I just spelled out at least two theoretical reasons it could go badly.
The safety of an aggressive treatment is something that should be tested thoroughly, to find out if the potential rewards outweigh the risks. Patients should be wary of overconfidence about these treatments.
Provocative recommendations
Therapy based on provoking an adaptive response has always been a reasonable hypothesis to experiment with, both clinically and scientifically. Unfortunately, there is a lot of devil is in the details: what constitutes the “right” amount and kind of stress is extremely hard to determine — it probably depends on some genetics, for instance — and consequently the results of such therapies have generally always been inconsistent and mostly underwhelming… especially the popular ones. Probably some conditions/people benefit from “toughening up” while others don’t. Your mileage will vary!
Meanwhile, the potential for abuse — for overzealous, irrational, and misguided provocation — is just off the charts. Patients even collaborate and facilitate their own abuse because so many of them come into therapy with the pre-existing idea that there is no gain without pain.
Provocation therapies are inherently risky, some of them much more so than others. They are also usually among the more expensive therapeutic choices.
Unreliable, a bit risky, and expensive is not a good combination — provocation therapies should be low on your list of treatments to try. And if you’re a professional who is using these methods, it might be time to reconsider your choices.
Did you find this article useful? Interesting? Maybe notice how there’s not much content like this on the Internet? That’s because it’s crazy hard to make it pay. Please support (very) independent science journalism with a donation. See the donation page for more information & options.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
Ten updates have been logged for this article since publication (2012). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
Apr 6, 2026 — Editing and polishing.
January — Refinement of the new condensed version of the scraping massage section. Added a substantial new sidebar, a safety PSA about massage injuries.
January — The scraping massage section has been condensed to a summary here for now — it was just getting too big for this space. The detail and citations that were removed here will return in the form of dedicated article in the future.
2024 — Substantial revision and expansion.
2024 — Minor editing. Added a more or less complete list of “provocation therapies,” also serving as a partial table of contents.
2024 — I shared a quote from this article about scraping massage, and it was extremely popular, so I decided to do a wave of updates to this article for the first time in several years. I upgraded the summary, added detail and citations to the eccentric loading section, and added two whole new sections: “The SAID principle: another basic concept in adaptation” and “Is trigger point therapy “provocative”? I also added a more detailed description of the “potency bias.”
2017 — Added a great visual example of Woolf’s law at work on the arm bones of tennis players (Haapasalo).
2017 — An especially neat science update about changes in intervertebral discs in runners (Belavý).
2017 — Science update. Cited a new review of all relevant research so far (Cheatham et al.). Also clarified the example of eccentric loading.
2016 — Science update. Cited a high quality new study of Graston technique, Crothers et al.
2012 — Publication.
Notes
Dr. Dr. Robert Zapolsky summarizes the hormonal dimension of it with flair:
Bones serve as the Federal Reserve for the body’s calcium, constantly giving and collecting loans of calcium to and from other organs. And part is for the sake of bone itself, allowing it to gradually rebuild and change its shape in response to need. How else do cowboys’ bow-legged legs get bowed from too much time on a horse?
- Haapasalo H, Kontulainen S, Sievänen H, et al. Exercise-induced bone gain is due to enlargement in bone size without a change in volumetric bone density: a peripheral quantitative computed tomography study of the upper arms of male tennis players. Bone. 2000 Sep;27(3):351–7. PubMed 10962345 ❐
- And, interesting additional point from the same passage: “the hormones of stress wreak havoc with the trafficking of calcium, biasing bone toward disintegration, rather than growth.”
- Fritton SP, Weinbaum S. Fluid and Solute Transport in Bone: Flow-Induced Mechanotransduction. Annu Rev Fluid Mech. 2009 Jan;41:347–374. PubMed 20072666 ❐ PainSci Bibliography 52978 ❐
Astronauts lose about 20% of their leg bone mass in a three-month stay in space, no matter how hard they work out on the Stair Master®. Why? To figure it out, scientists needed to crack a century-old mystery. We’ve known since the late 1800s that bone’s microscopic structure is perfectly adapted for the stresses it has to endure — but how does it do it? Bone cells are trapped deep in rigid bone. How do they know what’s going on? Sheldon Weinbaum is one of the scientists who cracked the bone code; he was interviewed by Robyn Williams on Australia’s excellent The Science Show in 2009:
“Bone cells live in caves. The mystery has always been how a tissue that’s as stiff as bone can communicate that it’s being loaded to the cells that live within it.”
And the solution to the mystery is “tiny little tubes.” Just like your inner ear uses fluid-filled tubes to detect motion, bone uses (much, much smaller) microscopic tubes to detect forces on bone: “a flow-induced system of mechanotransduction.” Under stress, fluid in the teensy tubes triggers a reaction in the bone cells. This process was identified only in the 90s, and Sheldon Weinbaum has been trying to figure out exactly how it works ever since. They made a major breakthrough: “we showed that the bone cell processes were actually tethered along their length and attached to these rigid canalicular walls.” It is these “tethers” that are responding to the fluid motion, tugging ever-so-slightly on the cell in response to gravity.
No wonder it took a hundred years to figure it out.
So, astronauts lose bone mass because the tube system simply doesn’t work in zero-G: the fluid floats randomly in the tubes! Precisely the same reason that astronauts get dizzy in zero-G, and have to learn how to orient themselves visually.
- No one seems to know who Davis was. Whoever he was, I was only dimly aware of his law before preparing this post. The Wikipedia entry for Davis’ law is anemic.
- If not entirely, at least substantially. It seems like some physical adaptation must be occurring in the examples of gymnast, contortionists and martial artists. But for most people, most of the time, simple stretch tolerance is a strong candidate theory to explain modest increases in flexibility with stretching. I cover this in considerable detail in the second half of my main stretching article, Quite a Stretch.
- Venkataraman VV, Kraft TS, Dominy NJ. Tree climbing and human evolution. Proceedings of the National Academy of Sciences of the United States of America. 2012 Dec. PubMed 23277565 ❐ PainSci Bibliography 54672 ❐
The Twa people of Africa and you will earn amazingly limber calves that allow your ankles to bend half way (45˚) to the shin — two to four times greater than the average urban person! A good video of this flexibility has unfortunately disappeared from YouTube.
- Belavý DL, Quittner MJ, Ridgers N, et al. Running exercise strengthens the intervertebral disc. Scientific Reports. 2017 Apr;7:45975. PubMed 28422125 ❐ PainSci Bibliography 53606 ❐
- D'souza CJ, Santhakumar H, Bhandary B, Rokaya A. Immediate effect of stabilization exercises versus conventional exercises of the trunk on dynamic balance among trained soccer players. Hong Kong Physiother J. 2022 Jun;42(1):23–30. PubMed 35782693 ❐ PainSci Bibliography 51683 ❐
From a prominent description of prolotherapy by The American Osteopathic Association of Prolotherapy Regenerative Medicine:
Prolotherapy works by stimulating the body’s natural healing mechanisms to lay down new tissue in the weakened area. This is done by a very directed injection to the injury site, “tricking” the body to repair again. The mild inflammatory response which is created by the injection encourages growth of new, normal ligament or tendon fibers, resulting in a tightening of the weakened structure. Additional treatments repeat this process, allowing a gradual buildup of tissue to restore the original strength to the area.
- For instance, low back pain does not correlate at all with the “looseness” of ligaments, and therefore logically it cannot in general benefit from “tightening” them.
- Yelland MJ, Sweeting KR, Lyftogt JA, et al. Prolotherapy injections and eccentric loading exercises for painful Achilles tendinosis: a randomised trial. Br J Sports Med. 2011 Apr;45(5):421–8. PubMed 19549615 ❐
This is a trial of 40 patients, comparing eccentric loading exercises and prolotherapy, or a combination of the two. It looks like a win, and the evidence is worth noting, particularly about prolotherapy, but there are several caveats and the results must be taken with a grain of salt: it’s a small study with no control group, the short-term effect size is modest, and the long-term results were scarcely distinguishable. With a control group, for all we know, untreated individuals would have done just as well, or even better.
“Tendinitis” versus “tendonitis”: Both spellings are acceptable these days, but the first is the more legitimate, while the second is just an old misspelling that has become acceptable only through popular use, which is a thing that happens in English. The word is based on the Latin “tendo” which has a genitive singular form of tendinis, and a combining form that is therefore tendin. (Source: Stedmans Electronic Medical Dictionary.)
“Tendinitis” vs “tendinopathy”: Both are acceptable labels for ticked off tendons. Tendinopathy (and tendinosis) are often used to avoid the implication of inflammation that is baked into the term tendinitis, because the condition involves no signs of gross, acute inflammation. However, recent research has shown that inflammation is actually there, it’s just not obvious. So tendinitis remains a fair label, and much more familiar to patients to boot.
- Couppé C, Svensson RB, Silbernagel KG, Langberg H, Magnusson SP. Eccentric or Concentric Exercises for the Treatment of Tendinopathies? J Orthop Sports Phys Ther. 2015 Nov;45(11):853–63. PubMed 26471850 ❐
- Murphy MC, Travers MJ, Chivers P, et al. Efficacy of heavy eccentric calf training for treating mid-portion Achilles tendinopathy: a systematic review and meta-analysis. Br J Sports Med. 2019 Sep;53(17):1070–1077. PubMed 30636702 ❐
- Fascia is widely considered an exciting frontier in manual therapy, and is particularly embraced by massage therapists. The big idea is that fascia — sheets and webs of connective tissue found throughout the body, literally the gristle in our meat — can get tight and needs to be “released” by pulling on it forcefully and/or artfully. Unfortunately, although fascia biology is interesting, the stuff has no properties that are relevant to hands-on therapy. Fascia research is plentiful but mostly amateurish and pseudoscientific and clearly fails to support “fascial therapy.” Enthusiasm about fascia is an unjustified fad. See Does Fascia Matter? A detailed critical analysis of the clinical relevance of fascia science and fascia properties.
I’m often asked what I think of a treatment that supposedly has an extremely high success rate, and it’s the same answer, every time: it’s absurd, and a huge red flag.
“Success rates” are not something individual clinicians can actually know, and it wouldn’t constitute validation of the methodology even if we could — there are way, way too many confounding factors.
But self-serving claims in healthcare are common, especially in fee-for-service manual therapy — self-employed “freelance” therapists tend to overpromise — and they are almost entirely based on conflating customer satisfaction with actual efficacy: “I know my treatments work because my clients are so happy,” basically. But people can be satisfied completely independently of whether or not they’re actually getting healthier. Satisfaction is easy to achieve. People want to be satisfied. They want to feel like they’re getting their money’s worth—so it’s pretty easy to get them there. And they also avoid admitting dissatisfaction! The combination is powerfully misleading, and most clinicians grossly underestimate it.
But many freelancer manual therapists go hyperbolic and claim perfection, or close to it: 98, 99, or 100% success rates! This is a delusion of grandeur, a sign of profound incompetence, and invariably part of a sales pitch. Perfection in most things is impossible in principle, but especially in healthcare. Most painful problems are the tip of an etiological iceberg. Genetic differences alone would make it impossible to treat every case successfully.
For a classic example of this problem discussed in more detail, see Overestimating “success rates” (for dry needling).
- People experience muscle pain and acutely sensitive spots in muscle tissue that we call “muscle knots.” What’s going on? The dominant theory is that a trigger point is an isolated spasm of a small patch of muscle tissue. Unfortunately, it’s just a theory, trigger point science is half-baked and controversial, and it’s not even clear that trigger points are even a problem with muscle. Meanwhile, people keep hurting, and massage — especially self-massage — is a safe, cheap, reasonable way to try to help. That’s why I have a large tutorial devoted to how to self-treat “trigger points” — whatever they really are. See Trigger Point Doubts: Do muscle knots exist? Exploring controversies about the existence and nature of so-called “trigger points” and myofascial pain syndrome.
- Modern pseudoscience is quite sophisticated, and rests on all the inadequacies and exploited vulnerabilities of science and scientific publication. Above all, a high volume of poor-quality evidence is systematically misrepresented as "promising," a careless but optimistic interpretation of inadequate literature. The research itself also exaggerates its mediocre results, usually by emphasizing biological effects instead of medical benefits, and conflating statistical significance with trivial clinical significance … and even that is usually distorted, because statistical significance is unreliable when measuring implausible claims. All these ways of making the science seem better than it is actually leads to almost inevitable cycles of escalating enthusiasm that is eventually curbed, slightly, when someone finally publishes a trial that's actually good quality, with an inevitably negative result — but that by that time, countless clinicians and scientists have spent 10-20 years talking like it’s already a done deal, and the bad news can easily be dismissed in what looks like a credible way by a citation dump of all the putatively "positive" evidence.
- Woolf CJ. Central sensitization: Implications for the diagnosis and treatment of pain. Pain. 2010 Oct;152(2 Suppl):S2–15. PubMed 20961685 ❐ PainSci Bibliography 54851 ❐
Pain itself often modifies the way the central nervous system works, so that a patient actually becomes more sensitive and gets more pain with less provocation. That sensitization is called “central sensitization” because it involves changes in the central nervous system (CNS) in particular — the brain and the spinal cord. Victims are not only more sensitive to things that should hurt, but also to ordinary touch and pressure as well. Their pain also “echoes,” fading more slowly than in other people.
For a much more detailed summary of this paper, see Sensitization in Chronic Pain.
- McDonald B, Pittman K, Menezes GB, et al. Intravascular danger signals guide neutrophils to sites of sterile inflammation. Science. 2010 Oct;330mcd(6002):362–6. PubMed 20947763 ❐
Researchers at the University of Calgary Faculty of Medicine are using an innovative new imaging technique to study how white blood cells (called neutrophils) respond to inflammation, and have revealed new targets to inhibit the response. Basically this research explains why neutrophils unnecessarily “swarm” sterile injury sites, causing damage and pain with no direct benefit — a biological glitch with profound implications. Collateral damage!
- Davidson CJ, Ganion LR, Gehlsen GM, et al. Rat tendon morphologic and functional changes resulting from soft tissue mobilization. Med Sci Sports Exerc. 1997 Mar;29(3):313–9. PubMed 9139169 ❐
This small study of rats attempted to demonstrate the possible relevance of Graston Technique to tendon healing. It is cited as the sole example of scientific research supporting the clinical use of Graston Technique. Although it does provide some interesting and positive findings, it is a small study of rats, so it has major limitations. Rat tendons were injured with a collegenase injection, allowed to heal for three weeks, and then some were treated with Graston Technique. Their gait allegedly improved more quickly than in the untreated rats. The authors claim that the results “suggest” that scraping “may promote healing via increased fibroblast recruitment.” Such cautious phrasing is appropriate: although promising, the effect of treatment on five rats is hardly conclusive.
- A 1% rate adverse effect rate is high — but you could do five human studies, using treatment groups of 20 each, encounter only a single example, and you still wouldn’t have a clue about the real statistical risk. Graston Technique poses a real potential danger, yet its safety hasn’t been studied at all. This is precisely the kind of thing that makes peoples heads explode about drugs — foisting serious side effects on the public, no matter how rare, is the stuff of scandal!