Manual Therapy: What is it, and does it work?
The science of "fixing" tissue with hands-on treatments like massage and spinal manipulation
“Manual therapy” refers mainly to massage, spinal manipulation, and acupuncture for common musculoskeletal problems and injuries, provided mainly by massage therapists, chiropractors, osteopaths, acupuncturists, and (more surprisingly) physical therapists.
This article is balanced between a bleak and cynical review of an industry with serious problems, and a love letter to a way of trying to help people that I am still faithful to despite those problems. I was a massage therapist myself for many years,1 and I still believe in the power of compassionate touch and novel sensations to inspire, comfort, and reassure. If nothing else, manual therapists particularly provide a lot of what medicine often cannot: time.
But time is also expensive, and it is often used poorly. Although popular despite the cost, manual therapy is badly polluted with pseudoscience and treatment methods that are corrupted by commercialization and branding: the “modality empires.” At its best, it’s not very affordable and the benefits are uncertain; at its worst, it is just actively wasteful and harmful.2
What exactly are we talking about? An unfamiliar term for a family of very familiar treatment methods
“Manual therapy” is mentioned almost two thousand times on this website, and yet it’s an unfamiliar term for many visitors3 — even though all major examples are well-known. It is a broad and fuzzy category of many therapeutic methods or “modalities,” countless branded and improvised variations on the major themes of poking, kneading, scraping, jostling, wiggling, zapping, and so on.

A major theme in manual therapy is hands-on “manipulation” — of spinal joints especially, but virtually any tissue is up for “grabs.” There are even manual therapists who claim to tinker with organs (“visceral” manipulation) and the brain (craniosacral therapy).
Hands-on is the soul of manual therapy, and the reason for calling it “manual,” but tools-on methods are closely related. Many tools are substitutes for hands — like attacking “muscle knots” with needles instead of thumbs — while many others bring something else to the table, usually some form of energy. Ultrasound/shockwave, laser therapy, dry needling [book chapter], and hydrotherapy are all mostly provided by the same professionals for all the same kinds of reasons.
Manual therapy even includes methods with no hands or tools at all, based on the delivery of imaginary energy: therapeutic touch and Reiki are also generally considered part of the manual therapy family (albeit an embarrassing one4). So there’s a broader definition of manual therapy that goes beyond “hands” on, and is based mainly on the intent:5
Manual therapy is any therapy that tries to directly and immediately produce pain relief and/or facilitate healing by doing things to patients’ tissues with hands or tools, and mostly without breaking the skin.
Most manual therapy is done to/for patients, so it is also sometimes called passive therapy as opposed to active therapy, which of course mainly refers to exercise therapy. While exercise and manual therapies are often combined, they are not the same thing. But some ideas really blur the lines between them, especially strength training (because it’s often another way to try to “correct” the same alleged defects), stretching, and therapy taping.
The good news about manual therapy
I believe that manual therapy has more to offer than most skeptics gives it credit for, most controversially trigger point therapy,6 and a few others, but mainly it’s just the value of touch and time. A particularly good use of the time and attention is screening and triage that is often neglected by other kinds of healthcare professionals.
And the allegedly progressive replacements for the much-maligned old ways haven’t exactly won me over.78910
Testimonials abound! We shouldn’t make too much of it — there are plenty of testimonials for all kinds of things that don’t deserve them, even dangerous things — but people really love to love the hands-on therapies, especially massage. Why? What earns that enthusiasm?
I often feels great. Manual therapy often produces many strong “scratching an itch” sensations, which can seem profound.
I’m not saying those experiences are placebo-powered, but they might be, and perhaps the lines between placebo and treatment are uniquely blurry in manual therapy. Certainly pleasant, intense, interesting, and meaningful sensations are rocket fuel for placebo!11 So much so that it may go beyond what we normally think of as placebo, what I call a “sensation-enhanced” placebo. While placebo may not actually “fix” much — the power of placebo is often exaggerated for ideological reasons12 — it can blunt pain at least as well as an ibuprofen, and maybe more under the ideal (and unstudied) conditions that manual therapy at is all about creating. Manual therapy may be a refined form of “therapy theatre,” treatment optimized for placebo in many ways.
That may be a bit of a backhanded compliment, but it’s better than no compliment at all!
Good therapy theatre likely has value, maybe even for the same reasons as actual theatre. I think manual therapy is a good enough show to pay for sometimes, if you can afford it — and I can, and I do, albeit somewhat sparingly. The older I get, the less willing I am to risk spending $150 just so I can listen to someone tell me that my glutes aren’t activating; or, if they fancy themselves progressive, lecture me about how “pain doesn’t equal damage.”13
Manual therapy can be comforting and supportive and empowering … and that’s a big deal
Many kinds of manual therapy are inherently pleasurable and/or satisfying, independently of whether they actually have any specific medical effects, and that can probably go well beyond “nice”: for instance, we know massage does ease depression and anxiety,14 and that should not be underestimated. That is a heavy clinical lift. That’s real power.
Manual therapy is a great context for coaching, encouragement, and education in other rehab tactics and strategies, like exercise or better sleep hygiene.
And so hands-on therapy is a unique position to deliver some relief from suffering and disability, if not actual pain — and it’s hard to even tell the difference. A little of one might give us some of the other, or at least a very persuasive illusion of it.15
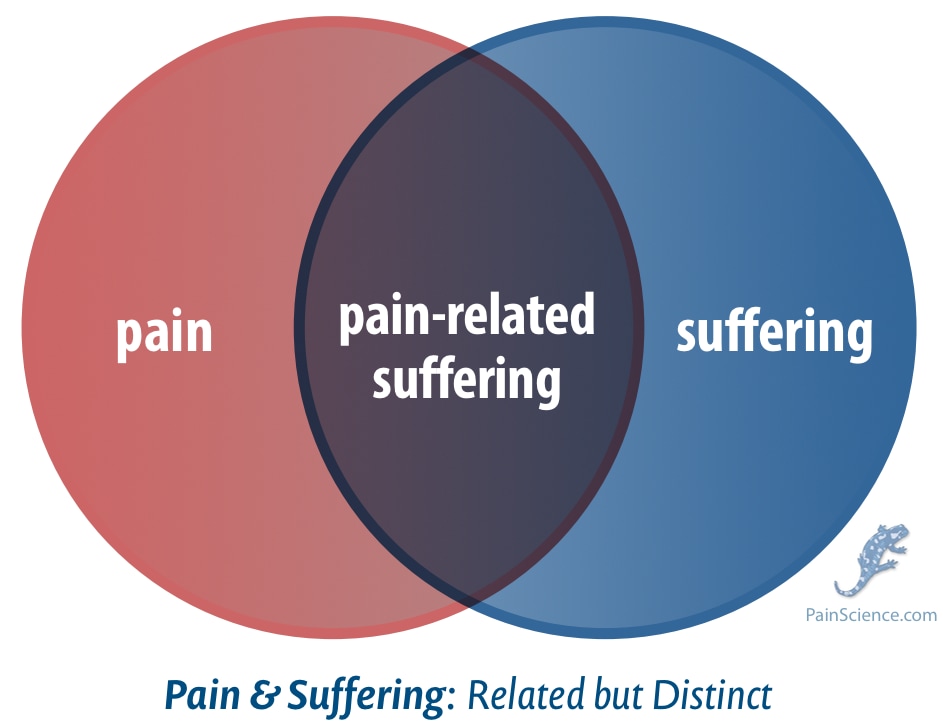
Although pain and suffering are different things, relief from one is indistinguishable from the other up to a point. And manual therapy can (and should) ease the suffering. It’s one of the best things about it.
And to whatever extent manual therapy can also relieve some pain, even just a bit for just a while, it is probably also disproportionately reassuring and inspiring — even without any major analgesia. But imagine if there was also some real pain relief!
All that general satisfaction, relief, encouragement, and education — and, yes, some analgesia too — may create some significant “windows of (rehab) opportunity” for optimization of healing. Perhaps too much has been made of this idea,16 but it’s not nothing.
For all of these reasons, I have somehow managed to hold on to a little optimism about manual therapy, despite all the of the bad news still ahead in this article. I’ll return briefly to the positive perspective at the end. But first, some more basics…
Who provides manual therapy? The major examples
Massage therapists and chiropractors are the two most familiar professions that are almost entirely devoted to manual therapies. Massage therapists practice countless styles of massage, but the field is dominated by trigger point therapy and fascia-inspired therapy, with everything else falling under the heading of “other.” Chiropractors are largely defined by spinal manipulation and being anti-medicine — despite the best efforts of the best chiropractors, who have always fought a losing battle to be well-known for anything else.
Osteopaths are much less well known, but also practice manual therapy extensively (though not exclusively), and are best-known to the public for their widespread, embarrassing use of craniosacral therapy. (Note that the character of osteopathy varies dramatically around the world, much more like chiropractic in some places, and more like physical therapy and orthopaedic medicine in others.)
Physical therapists (AKA physiotherapists) used to do a lot more hands-on manual therapy, especially spinal manipulation, but as the profession became increasingly mainstream, they (notoriously and unfortunately) started to provide much more “modern” and technological therapies like ultrasound, transcutaneous electrical nerve stimulation, and laser therapy, which substantially differentiated them from chiropractors and massage therapists.
But the manual therapy that PTs are most strongly associated with in the 21st century is, weirdly, dry needling — which looks almost exactly like acupuncture (same needles), but is much more closely related to trigger point therapy, because the point (ha) is to treat muscle knots by stabbing them. If you’re not familiar with this, I promise it’s more popular than you would guess! Physical therapists tend to be the main source of dry needling, because in many jurisdictions they are the only non-doctors who can legally needle anyone (and the doctors are much less interested, although some of them also do it).
What about doctors? It’s a very rare physician that stoops to offer the more conventional kinds of manual therapy. Perhaps they steer clear of it because of the strong stink of “alternative” on it. Also, touching, ew!
Those are all the major examples of manual therapy providers, but there’s plenty more around the edges.
Acupuncture is one of the stranger members of the manual therapy family, and some people might exclude it. But it is so in sync with the intention and sensibilities of manual therapy that I think it belongs.
Other sources of manual therapy
Acupuncture, of course, is almost exclusively the domain of the acupuncturists — odd members of the manual therapy family, but too popular not to include.17
Hydrotherapy was a major part of manual therapy historically, and has never fully gone away — and still has faddish revivals, like ice baths in the 2020s — but it is no longer associated with any particular profession.
Finally, there are millions of “body workers” and “energy workers” and various and sundry other self-identified “healers.” The majority are just unlicensed massage therapists, providing mainly massage, but a great many of them are also vitalists at heart, convinced that they are massaging your chakras and acupuncture points and meridians. Much of this nonsense still counts as manual therapy: the intent is the same, even if the “tissue” they are targeting is your aura. But many of these “professionals” get very weird indeed, and get up to all kinds of methods that are more like psychic healing and traditional folk medicine (e.g. ear candling, crystal therapy, iridology).
And it’s not clear that any kind of manual therapy is actually therapeutic…
Is manual therapy effective? The bad news, pulling no punches
The shortest simple answer: probably not very effective, but no one really knows thanks to the lack of (good) science. Unfortunately, much of it isn’t even plausible, let alone evidence-based.
Manual therapy contains much of the worst of alternative medicine. It is thoroughly dominated by pseudoscientific and simplistic nonsense. The field has a hall of shame the size of Grand Central Station, exhibiting some of the nastiest snake oils in history, as well as the silliest. However, even if we ignore all of that, there are still major problems!
Despite the practically infinite variety of technique, there are only a few major, simplistic themes. Manual therapy is mostly fueled by faith in the rather implausible idea that tissue can be fixed or improved by just the right kind of physical manipulation or force.
Sometimes that force is implausibly subtle, relying on extraordinary claims of the therapist’s ability to detect and/or “adjust” something in the body. And sometimes that force is intense, and so the no-pain-no-gain hubris of many methods involves some medical risks … which cannot be justified by evidence.
Much of the problem can be traced to the industry’s obsession with the pathologization of misalignment and things that are “tight” or “out of balance” — especially f*cking fascia! The entire focus of fascial therapy is on completely imaginary “distortions” in our gristle. And then there's “increasing circulation,” used to justify countless treatment methods. Or “kick-starting” healing … often almost violently, because you have to “break some eggs to make an omelette.”
All of these themes and ideas are shallow and at odds with the evidence, no matter how dressed up in jargon and pseudoscience, and yet they are clearly at the heart of all the major manual therapy modalities. And so literally all of the well-known ideas and methods of manual therapy are of dubious value, and several are particularly problematic — like spinal manipulation, especially when performed on infants, a shockingly common bit of chiropractic quackery (of which there is plenty).
The state of the science of manual therapy
The only popular manual therapy exclusively offered by physical therapists, dry needling, is sketchy as hell, with real risk of harm and clear evidence-of-absence.18 And that’s from the most mainstream of the providers in this category.
We have half decent evidence that neither massage nor spinal adjustment are helpful for the average back pain patient.1920
Manual therapists also widely use (and abuse) the Functional Movement Screen,21 a pseudo-diagnostic tool that harmonizes strongly with manual therapy because it’s based on the largely discredit idea that pain and injury are caused by subtle movement dysfunctions that only sufficiently skilled professionals can detect (or fix).
TENS and ultrasound and shockwave therapy, the major gadget-based modalities, have all been quite well-studied with extremely disappointing results: not entirely negative in every case, but thoroughly unimpressive. TENS is the canonical example of a therapy that is “clinically proven” … to be only ever-so-slightly helpful.
Those modalities probably account for three quarters of all manual therapy. And most other techniques are barely studied and range from implausible to inane, and what little science we do have invariably shows no benefit at all, or damns with the faint praise of tiny benefits that are more likely illusory than just trivial.
But mostly the science is just inadequate.
Evidence-based manual therapy cannot really exist, because it is plagued by small, junky little studies that cannot actually answer the questions they are trying to answer. Barely positive results are common, but probably almost always the product of bias-powered p-hacking. Those “positive” studies are barely worth mentioning, and yet they are routinely spun as “promising” by the minority of practitioners that look at the science at all.
The handful of journals dedicated to manual therapy are of poor quality and held in contempt by the scientifically literate. Their editors and contributors are supposedly the best and brightest that manual therapy has to offer, and of course some of them actually are — but the overwhelming impression their work makes on a scientifically literate outsider is that it’s an amateurish mess. As a science journalist specializing in this field, I actually just gave up regularly reading some of the key journals that I originally focused on. The juice just isn’t worth the squeeze!
It’s all rather weak sauce for services that cost most patients at least a buck a minute (and often double that). Quite disheartening!
Claims of high and even perfect success rates
I’m often asked what I think of a treatment that supposedly has an extremely high success rate, and it’s the same answer, every time: it’s absurd, and a huge red flag.
Such claims in health care are common in for-profit healthcare generally, but especially in manual therapy. Fee-for-service and self-employed “freelance” therapists tend to overpromise.
They are almost entirely based on conflating customer satisfaction with actual efficacy: “I know my treatments work because my clients are so happy,” basically. But people can be satisfied completely independently of whether or not they’re actually getting healthier. Satisfaction is easy to achieve. People want to be satisfied. They want to feel like they’re getting their money’s worth—so it’s pretty easy to get them there. And they also avoid admitting dissatisfaction! The combination is powerfully misleading, and most clinicians grossly underestimate it.
But many manual therapists go hyperbolic and claim perfection, or close to it: 98, 99, or 100% success rates! This is a delusion of grandeur, a sign of profound incompetence, and invariably part of a sales pitch. Perfection in most things is impossible in principle, but especially in healthcare. Most painful problems are the tip of an etiological iceberg. Genetic differences alone would make it impossible to treat every case successfully.
For a classic example of this problem discussed in more detail, see Overestimating “success rates” (for dry needling).
Ending on a high note
Despite my cynicism, despite all the problems, I still suspect that there are at least a few useful manual therapies, a little signal in all that scientific static, unpredictable but genuine medical benefits that have yet to been confirmed. They are probably modest on average, but I believe that they are occasionally profound.
Shhh! Don’t tell my skeptical colleagues!
Massage therapy in particular still has a piece of my heart, and I have tried hard in the last few years of my career to walk back some of my cynicism and reassure massage therapists that they can be proud of what they do. The message — now for any kind of rational manual therapist — is that it’s always possible to offer more plausible techniques, minimize risks and costs, and create valuable sensory and social experiences. Manual therapists can humbly and conservatively dabble in experimental treatments with informed consent instead of overconfidently pushing them on patients. They can, if nothing else, deliver the time, compassion, and touch that medicine routinely neglects — and not spoil the show with pseudoscience.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
Nov 19, 2025 — Another batch of substantial edits and upgrades, especially a full audio version of the article.
2025 — Many minor improvements and corrections.
2024 — Substantial editing, with particularly meticulous improvements to the article summary, which is widely reproduced wherever relevant around the site. “Integration” with the rest of the library is a standard production step for all articles — linking to and from other articles — but it was particularly extensive here, because the topic is so important to PainScience.com as a whole. There are many dozens of appropriate places to summarize manual therapy, or some aspect of it, and link to more information, so it was very important to have a highly polished summary.
2024 — Publication.
Notes
- I was a Registered Massage Therapist with a busy practice in Vancouver, Canada, from 2000–2010. I quit the profession in disgust before I could be “fired” for being critical of pseudoscience and alternative medicine. I changed my professional focus to science journalism and anti-quackery activism, writing mostly about massage-adjacent topics in the early years, but then spreading out into anything relevant to any kind of chronic pain or injury rehab — an effectively infinite list of topics. Even fifteen years after my last hands-on work, I still think of myself as a massage therapist. That said, I don’t exactly feel like an “insider” either, and I’ve branched out a lot in that time. See my bio.
Time is both valuable and costly, and so unfortunately the best of what manual therapy has to offer is also out of reach to many of the people who need it the most — poverty and prejudice are constant bedfellows of chronic pain, for complex socioeconomic reasons. To a surprising degree, it is a service for the privileged, much less affordable than a cleaning service. This is almost never highlighted by manual therapy’s enthusiastic, idealistic practitioners! And yet the worst of manual therapy is persuasively marketed and amazingly popular, and that drives many people to pay more than they can comfortably afford — even if they are a bit skeptical — to give it a chance to help with their serious problems. I have heard countless rather tragic stories of people who have nearly bankrupted themselves to pay for a “package” or “course” of expensive treatments that are of dubious value at best. Caveat emptor!
Weirdly, there isn’t really a good word for all the kinds of professionals that try to help people with injury rehab and pain. What do you call them, if you have to write about them constantly? Every option is flawed, and it sure gets tedious listing them every time: physical therapists, massage therapists, osteopaths, chiropractors, occupational therapists! I don’t want to think about how many times I’ve had to type that list in a quarter century of doing this.
It’s a real annoyance, for instance, that you can’t conveniently abbreviate them all, a mental hangnail. Chiros and osteos and physios are all concise and tidy and even rhyme … but then there’s the massage and occupational therapists! The massas and occus? Ugh.
And, no, never “masseurs”!
Nor do you dare abbreviate “pedorthists.” 😏
By about 2020, I had more or less settled on “manual therapists” as the most useful catch-all terms for the professions I
pick onwrite about the most. It’s the least bad option I’ve come across.It’s clearly not perfect. For instance, a lot of patients have no idea what I’m talking about if I say “there’s a lot of bullshit in manual therapy.” That's mainly why I am writing this article: to define and explore a term and a family of ideas that, despite it’s imperfections, is actually fairly useful.
- They are pure “vitalism” — a childish belief in an undetectable energy system in biology, like the Force in Star Wars. It’s on the same level as believing in psychic powers, and I do not apologize for holding it in contempt.
- This is my own definition. It is not a formal or widely accepted definition — those exist, but they aren't particularly formal or widely accepted either!
- I think it’s an interesting and legitimate experimental therapy than can be ethically, cautiously explored with informed consent. I also think it is horrifically abused and overconfidently oversold by many manual therapists. See The Trigger Points Index.
- Taylor AJ, Kerry R. When Chronic Pain Is Not “Chronic Pain”: Lessons From 3 Decades of Pain. J Orthop Sports Phys Ther. 2017 Aug;47(8):515–517. PubMed 28760092 ❐
This paper tells the story of a patient who had “sciatica” for thirty-five years and was misdiagnosed many times until finally getting not only a definitive diagnosis but a cure. He had a narrowed artery (arterial stenosis causing “claudication,” the pain of impaired circulation). That’s it! Not even a difficult diagnosis in the end, really. There were some pretty glaring clues there that got ignored by a lot of people who should have known better.
Not only was he misdiagnosed many times over more than three decades, he was misdiagnosed fashionably: that is, each misdiagnosis neatly fit a paradigm in physical therapy, better than it fit his symptoms. This carried on right up to and including the present day fascination with psychosocial factors and sensitization (which served him no better than any of the other paradigms had).
Interestingly, the patient’s belief that something ‘was actually wrong’ had remained with him throughout the journey. This, of course, had been explained away to him (more recently) by current research and evidence-based thinking on central sensitization and pain.
Just fascinating. The authors thoughtfully explore the implications of this rather shameful episode (definitely aimed at pros, some jargon, but readable enough for anyone — and behind a paywall, unfortunately). The bottom line? Good diagnostic skills are never out of fashion. Or shouldn’t be, anyway!
There are criticisms of this paper from a couple of my favourite experts and writers, pointing out in a letter to the journal that one of the “fashionable” paradigms impugned here, the biopsyschosocial model, “includes the considerations [the “bio” part] that eventually cured the patient’s pain.” I like the criticism and I like the authors’ response — I see only healthy debate here
Accuracy disclaimer: It’s always possible that a case study like this has been misrepresented to make a point. Maybe it didn’t really go down this way. But based on my own professional, I think things like this definitely do happen (and based on my personal experience, I know they do). I am referring both to fashionable misdiagnosis in general, and to problematic overemphasis on psychosocial factors and sensitization in particular. The omission of the “bio” from the “biopsychosocial” model should not happen in theory, but it certainly does in practice.
- Breedt E, Tichenor E, Barlott T. Diagnosing the body in physiotherapy: the passage from discipline to control. Physiother Theory Pract. 2025 Nov:1–25. PubMed 41215734 ❐
This paper is a strong indictment of some of the fashionable trends in physical therapy. The authors argue that modern “holistic,” “patient-centred,” “pain-science informed” physiotherapy is not actually humane or liberating, even though many clinicians obviously sincerely believe it is. Instead, they suggest that it quietly extends physiotherapy’s reach into more intimate aspects of life, and that that expansion conveniently aligns with unrealistic neoliberal expectations to self-optimize, self-manage, stay productive, and keep adapting forever.
In other words, progressive physio tends to put the burden of pain relief on the patient. Although that is obviously a major oversimplification, and it doesn’t capture the authors' entire argument, it does express a major key point.
For patients, we could boil it down even further to just a single word: gaslighting.
Breedt et al. think today’s “progressive” approaches encourage people to:
- reinterpret their own pain,
- reframe their beliefs,
- regulate their emotional responses,
- build self-efficacy,
- pursue meaningful activity despite symptoms,
- and continually upgrade themselves.
The horror! What’s wrong with those things? They can seem (and even be) meaningfully supportive, but the authors see them as part of a broader social dysfunction where individuals are expected to manage their own suffering through self-regulation rather than relying on (for instance) healthcare providers to, you know, provide. Provide what? Clinically important diagnosis and/or treatment! Which may well be neglected! See Taylor for important documentation of a representative example of that neglect.
Breedt et al. are critiquing an ideology that wraps around this newer style of care. Progressive physiotherapy can have a shiny, benevolent surface while still carrying hidden problems — just different ones than the old biomechanical paradigm. Out of the frying pan, into the fire. From simplistic biomechanics to simplistic biopsychosocialism. The are concerned about the social-political machinery that offloads responsibility for structurally produced harm onto individuals in the first place. Rather than refining techniques of self-regulation, they urge us to examine how our economic and political orders generate the very injuries, illnesses, and debilities people are then told to manage on their own.
I notice a striking similarity between this thesis and that of one of my favourite books, Ron Purser’s brilliant McMindfulness. This statement in the abstract jumped out:
“We contend that ‘holistic’ movements in physiotherapy, despite their progressive appearance, serve control societies and perpetuate state and corporate power.”
That may sound strangely political/philosophical to many readers' ears, but it’s practically an echo of the point of Purser’s book, which is that corporations have co-opted meditation and mindfulness “as a technique for social control and self-pacification.”
- Cognitive Functional Therapy (CFT) promises a modern, biopsychosocial alternative to conventional back-pain care, but the RESTORE trial — widely promoted as a breakthrough, strong evidence that CFT works — delivered only modest benefits with plenty of caveats. RESTORE had numerous serious flaws: it wasn’t placebo-controlled, was fully unblinded, used self-reported outcomes, and showed small effect sizes that are common to almost any active intervention, and that was even with some serious statistical jiggery-pokery favouring the results. A three-year follow-up claims durable gains, but heavy attrition undermines confidence. CFT may still be “less wrong” than old-school manual therapy, and it may be valuable as compassionate coaching, but evidence for a specific therapeutic effect still does not exist even as CFT teeters on the brink of being corrupted by (well-intentioned) commercialization. See Reluctantly Reconsidering RESTORE: An in-depth analysis of the RESTORE trial of Cognitive Functional Therapy for back pain.
- Riley SP, Ware E, Pitre Z, Russell N, Flowers DW. Pain neuroscience education combined with any singular form of physical therapy intervention is not more effective than the single intervention itself: a systematic review. J Man Manip Ther. 2025 Nov:1–11. PubMed 41262073 ❐
This review of pain neuroscience education (PNE) concludes that trials are a bit of a mess, with studies leaning heavily on statistical significance while paying little attention to effect size, uncertainty, or clinical meaning. Seemingly “positive” findings rest mainly on dubious methods and biased interpretation rather than strong evidence.
After strict screening for trial quality and research integrity, the authors found only a handful of studies worth taking seriously — and those do not show that adding PNE to a single physical therapy intervention improves pain or function. The evidence base is thin and varied, and cannot justify good-news conclusions. PNE is somewhere between absence of evidence and evidence of absence: not disproven outright, but doesn’t produce a clear positive signal even when bias is presumably warping results in favour of PNE.
Riley et al. do not claim that PNE is useless in all contexts, but they do conclude that it cannot be defended as an effective add-on treatment for improving pain or functional outcomes. Some secondary measures — such as pain knowledge, self-efficacy, and fear of movement — show limited signals in specific cases, but these effects do not translate into meaningful clinical benefit. Overall, this is quite damning review: the literature is not just “inconclusive,” it’s unimpressive.
The “meaning” is a tricky ingredient. People easily own their own pleasant experiences: they know it’s pleasant, and you can’t really convince them otherwise. But what the sensations “mean” is much easier to influence, and it is often dictated by the clinician, by the stories they tell about what’s happening, the “narrative” that justifies or explains the sensation (often potent). Left to their own devices, people may assign their own meaning to a sensory experience — but in practice, they are usually prompted, guided, and even bullied into believing that it means something specific. That belief is problematic. People can easily have their minds poisoned with harmful and even dangerous ideas about what’s going on, like false beliefs about their “alignment” or their vulnerability/fragility. And manual therapists have a lot of stories like this.
- Placebo is fascinating, but its “power” isn’t all it’s cracked up to be, not even for relief of purely subjective symptoms like pain: the power of belief is strictly limited and accounts for only a little of what we think of as “the” placebo effect, which is actually a collection of diverse nonspecific effects and research artifacts. For more information, see Placebo Power Hype: The placebo effect is fascinating, but its “power” isn’t all it’s cracked up to be.
- Chronic pain is indeed quite “weird” and janky at times … but it’s not at all clear that pain neuroscience education is any better than the manual therapies it purports to replace, and meanwhile simplistic “pain ‘splaining’” is both common and obnoxious. See Mind Over Pain.
- Moyer CA. Affective massage therapy. Int J Ther Massage Bodywork. 2008;1(2):3–5. PubMed 21589715 ❐ PainSci Bibliography 54758 ❐
Pain and suffering are closely related but distinct. In this context, “suffering” is the emotional distress and disability caused by pain. There is no formal definition of pain-related suffering (somewhat famously among pain nerds), but here’s my crack at a thorough and precise one, paraphrasing Stilwell et al.: “Pain-related suffering is a subjective experience characterized by negative emotions that are related to pain but distinct from it, and which can disrupt even a ‘minimal’ sense of self.”
It’s unlikely that suffering actually drives pain … but that is what some professionals do believe, and so they “target” the psychological distress in the hopes that it’s easier than diagnosing and treating whatever is causing the pain (this is most obvious in the example cognitive behavioural therapy.
But it is indisputable that relieving suffering is inherently valuable, and also hard to distinguish from pain relief. Up to a couple points of change on a scale of ten, there’s just no clear difference between feeling better about your pain and actually feeling less pain. Read more: Suffering, Disability & Pain: There’s the pain, and there’s the effect it has on lives.
- A “window of opportunity” (WOO) in therapy is a period of minor pain relief or boosted confidence that facilitates normal activity/exercise, which in turn is what delivers the true rehab value. This is exemplified in some cases of frozen shoulder. A placebo can also generate a bit of WOO, but a good WOO is a little more substantive. The idea of WOOs is also often used as a self-serving justification for ineffective methods that only produce trivial, transient benefits. See “Windows of Opportunity” in Rehab: The importance of WOO in recovery from injury and chronic pain (using frozen shoulder as a major example).
- On the other hand, it isn't nearly as popular as they'd like us to think. Most people do not go to an acupuncturist for that case of frozen shoulder that has been dragging on — certainly not in the West, and quite possibly not even in China.
- Stieven FF, Ferreira GE, Wiebusch M, et al. No Added Benefit of Combining Dry Needling With Guideline-Based Physical Therapy When Managing Chronic Neck Pain: A Randomized Controlled Trial. J Orthop Sports Phys Ther. 2020 Apr:1–21. PubMed 32272030 ❐
This is a rare good quality trial of dry needling of trigger points as a treatment for chronic neck pain. It had a clearly negative result, and it’s a bit of a nail-in-coffin study for dry needling, as much as any one study ever could be.
The researchers compared standard “guideline-based physio” — as garden-variety as possible — to a combination of that with dry needling in more than a hundred patients, with follow-up at 1, 3, and 6 months. It seems like a fair comparison to me, and I agree with the authors that it is effectively testing and “mimicking the clinical decision-making process seen in daily practice.” Their conclusions:
Adding dry needling to guideline-based physical therapy resulted in a small, not clinically meaningful, reduction in average neck pain intensity at one-month post-randomization, but not at 3 and 6 months in participants with chronic neck pain. Clinicians should not consider dry needling in addition to physical therapy as an approach to managing chronic neck pain.
I will keep following the evidence on needling, but after this data, I know where I am placing my bets on the long-term outcome of this controversy.
This is probably the best single citation for this, but there’s a great deal more detail about dry needling in my weirdly skeptical trigger points book (weird because most people who write entire books about trigger points are boosting it, not giving it the side eye).
- Furlan AD, Giraldo M, Baskwill A, Irvin E, Imamura M. Massage for low-back pain. Cochrane Database Syst Rev. 2015 Sep;9:CD001929. PubMed 26329399 ❐
Previous versions of this meta-analysis of massage therapy for back pain (Furlan 2002 and Furlan 2008) are among the most cited scientific papers about massage therapy. This one is unlikely to wear that crown, because it has a pessimistic conclusion — a change of tune from the optimism of the previous versions. In 2008, the authors concluded that “massage might be beneficial.” In 2015, based on 25 studies instead of a thirteen, they wrote, “We have very little confidence that massage is an effective treatment.” This is a reasonable change, considering that the evidence available is that they “judged the quality of the evidence to be ‘low’ to ‘very low’, and the main reasons for downgrading the evidence were risk of bias and imprecision.” Every study of this topic has serious flaws, even the biggest and most rigorous (eg Cherkin). The evidence is inconclusive at best.
See Does Massage Therapy Work? for much more detailed discussion of this and related studies.
- Rubinstein SM, de Zoete A, van Middelkoop M, et al. Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain: systematic review and meta-analysis of randomised controlled trials. BMJ. 2019 Mar;364:l689. PubMed 30867144 ❐
This review in the British Medical Journal continues the tradition of damning spinal manipulative therapy with extremely faint praise. It has a putatively positive conclusions, and so it will be widely cited by chiropractors as evidence of the efficacy of SMT for back pain. However, even trying to spin the data in favour of SMT, the conclusions seem tepid at best: they not some short term benefits, and declaring that “SMT produces similar effects to recommended therapies for chronic low back pain.” But chronic low back pain is notoriously untreatable, and all treatments produce minor short term benefits and no long term benefits (see Artus, Cashin). The evidence has been available for many years that SMT is just as ineffective as everything else. These conclusions are disingenuous nonsense.
There are other serious methodological concerns here, summarized by Mary O'Keeffe & Neil O'Connell in a letter to the editors of the British Medical Journal. Their conclusions are far more in tune with the evidence reviewed:
See Does Spinal Manipulation Work? for much more detailed discussion of this and related studies.These results demonstrate no convincing evidence for the superiority of SMT over sham SMT and a lack of clinically important benefit of SMT when compared with any other treatment. The lack of a benefit of SMT over sham therapy indicates that SMT is unlikely to have any direct benefits and observed improvements are the result of contextual and other effects. It is likely that the apparent equivalence with both ‘recommended’ and ‘non-recommended’ therapies tells us more about the disappointing effectiveness of those approaches than it does about the benefit of SMT.
- The Functional Movement Screen (FMS) is a pseudo-diagnostic physical test of coordination and strength, especially “core” strength, invented in 1997 and now used (and abused) by manual therapists healthcare professionals. It was originally conceived of as a trouble-detection system, which is baked into the name: it’s just a “screen,” in theory. In practice, it also unwisely used like diagnostic tool to “explain” injury (“well there’s your problem,” pointing to a slight deficit “revealed” by the FMS). Although it’s at least somewhat reliable (practitioners can generally produce the same results), it has failed many tests of its validity, its ability to predict or even detect injury. Multiple scientific reviews since the mid-2010s have concluded that it is not useful. It’s extremely unlikely that anyone can figure out who is going to get injured, or what’s wrong with people who already have been injured, just by watching them move. The FMS is both a product of, and a contributor to, the common but dubious belief that injury is a function of subtle movement dysfunctions. See The Functional Movement Screen (FMS) Reviewed: The powers of the popular screening system for athletic injury risk may be over-hyped.