A Historical Perspective On Aches ‘n’ Pains
Why is healthcare for chronic pain and injury so bad?

Jonas Salk at the University of Pittsburgh where he developed the first polio vaccine.
The 20th Century was such a scientific and technological earthquake that we all now have a tendency to assume that the human species has advanced knowledge about basically everything, but we really don’t. The state of our knowledge of anything relatively subtle, subjective, or complex in medicine is still surprisingly primitive. Chronic pain care is notoriously inadequate and difficult, and even the most “simple” and “mechanical” problems, like arthritis or tendinitis, have proven to be deeply biological in nature. Even sports medicine — with so much potential funding (and potential relevance to occupational injuries) — has been bizarrely slow to build its evidence base.1 The performance of elite athletes is worth trillions to our economy, and obsessively optimized, and yet science remains almost completely silent on the best treatment options for the most common injuries affecting those high value patients, things like muscle strain.2
For most of history, medicine had bigger, scarier fish to fry than treating mere aches and pains and injuries. And it still does. But just a few decades ago, doctors and researchers were necessarily preoccupied with much more pressing public health issues … and rewarding new treatments.
Insulin and penicillin were still changing the world, as were a string of new vaccines — diptheria, pertussis, tuberculosis, tetanus, flu, yellow fever, typhus, polio, measles, mumps! Surgery and anesthesia were finally coming into their own, with error rates plummeting.3 The first organ transplants were saving people who would be doomed without them. Dialysis! Pacemakers! Laser treatments for eyes! MRI and CT scan! Arthroscopy!
Medicine was still creating huge leaps in the length and quality of our lives.4 It was an era of low-hanging medical fruit.
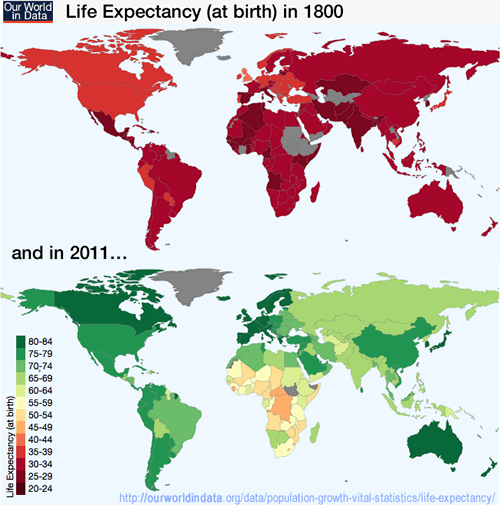
When you look at the big picture, it’s easy to see that we’ve been rather busy making an amazing amount of progress in many, many other ways. Our World In Data provides many terrific examples. So many of my worst cynical impulses are contradicted by Max Roser’s charts and data. Refreshing! As Bill Clinton said, “Follow the trendlines not the headlines.” Chart Source: Max Roser & OurWorldinData.org,
Meanwhile, physical medicine is a bit of a backwater
Chronic pain and stubborn “minor” injuries (like repetitive strain injury) were barely noticed by medical science until about the 1980s, and they remain a bit of a backwater to this day, both scientifically5 and clinically.6 Musculoskeletal medicine is still a cocky teenager, just starting to come of age and figure out that it doesn’t know everything.
Most doctors are straight up unqualified to treat chronic pain and non-traumatic injuries.7 PM&R (Physical Medicine & Rehabilitation, A.K.A. physiatry) is one of the youngest and most obscure medical specialties, and the only one that tackles most “aches and pains” head on. (Rheumatologists and orthopedists in theory deal with all forms of therapy for any kind of musculoskeletal problems, but in practice these specialities have been dominated by serious diseases and injuries, and by profitable elective surgeries that “make sense” to the surgeons who make money doing them but are amazingly unstudied to this day — or, for the few that have been properly tested, proven ineffective89 or dangerous!10)
Perhaps we do have the medical “luxury” of paying more attention to relatively minor pain problems that were overshadowed by the more critical medical issues of the past. But of course those problems aren’t really so minor — just less major than things that kill you outright.
Despite a century of rapid overall progress in medicine, there are still many common medical myths that simply won’t die: doctors and patients alike still believe things that we should drink at least eight glasses of water a day or that we only use 10% our brains.11 And that’s still a problem even where the light of science is shining most brightly.
It’s far worse in musculoskeletal medicine: for every mainstream medical myth, there are three about aches and pains and injuries. Myths and snake oil have thrived in the relative darkness of this neglected sub-category of medicine.
Chronic pain is a pretty scary fish to fry too
Non-lethal chronic pain accounts for a stupendous amount of human suffering. The economic costs of even mild to moderate problems — your garden variety low back pain guide, frozen shoulder, patellofemoral pain, carpal tunnel syndrome, and so on — are quite hair-raising. Scientific papers on these topics always begin with an accounting of their horribleness.

For most of history, medicine had bigger, scarier fish to fry than treating aches and pains. Not that pain isn’t scary too …
More severe chronic pain problems — a horrible neck pain that just won’t quit, or dreaded afflictions like fibromyalgia, complex regional pain syndrome (CRPS), and trigeminal neuralgia — are truly awful. Indeed, they can be so horrendous and untreatable12 that many victims take their own lives to escape the pain. And yet patients with chronic pain often justly feel abandoned, disbelieved, and even gaslit and blamed.13
The general neglect of pain science was most unfortunate. Turns out it’s more important, difficult, and generally weirder than anyone could imagine a half a century ago. We can put a man on the moon, but we can’t fix most chronic pain! It’s just a much trickier subject than most people think; the rabbit holes are deep, and I suspect that there is no such thing as a simple problem in all of the world of pain science. I bet it even gets weird if you start trying to really figure out toe stubs.
Part of the problem is that pain is usually “complex” while rocket science is merely “complicated.” Science has made similarly weak progress in solving other complex problems like autoimmune, metabolic and mood disorders. Evidence based treatments in areas involving complexity are barely better than folk wisdom. Which opens the door to alt med quackery.
Todd Hargrove, paraphrasing (by tweet) key concepts in his excellent article, “Is Movement Therapy Rocket Science?”
Poor quality healthcare for chronic pain and injury is still the rule
Healthcare for persistent pain and stubborn injuries remains disappointing not only because of how hard the problem has turned out to be, but because professionals treating these problems have been too free to “wing it” for too long. It is a mess professionally, a shambolic parody of good healthcare.
The bleeding edge consists not of good science, but the speculations and experiments of opportunistic cure purveyors and their desperate patients. I am referring not only to blatant quacks and cranks — plentiful, of course — but also to vast numbers of ordinary professionals who still work almost exclusively with obsolete conventional wisdom, old and simplistic ideas about what’s wrong and how to help, ideas that predate a surge of research that is late and inadequate but much better than nothing.
While there are certainly many progressive professionals out there who are leaving the old ways behind, it’s hard to overstate how bad the situation still is even in the “mainstream” (and it’s downright bizarre in the “alternative” realm).
A reader wrote to me in the grips of justifiable outrage about a string of egregiously incompetent healthcare professionals he’d encountered while trying to recover from a stubborn injury. It was all routine nonsense from my perspective — unfortunately, I see such stories frequently— but he was in a state of disbelief that so many so-called professionals could possibly be so amateurish. “Why is there so much ignorance in musculoskeletal medicine?” he asked.
So many factors! A sampling …
- Professional pride and tribalism, ideological momentum, screwed up incentives.14
- At the other extreme, and not much better, there is the love affair with “advanced” methods and technological gadgets — like laser therapy — which has generated vast amounts of pseudo-quackery: quackery that effectively masquerades as mainstream despite strong evidence that it’s ineffective.17
- Near universal ignorance of the history of science, critical thinking skills, and the cognitive distortions and limitations that blind us all … like emotional reasoning, confirmation bias, the human weakness for oversimplification and “common sense,” and looking only where the light is.
- The obscurity and difficulty of newer and better ideas, especially the major physiological factors that we’re still learning about (tip of the iceberg). Neglecting these has become unforgivable over the last twenty years.
There’s particularly embarrassing ideas and distractions, especially in chiropractic and massage: really archaic alt-med stuff, all kinds of vitalism and worse.15 Acupuncture, the darling of alt-med, a therapy even many skeptics gave a pass to for a long time, is now all washed up, the domain of cranks, flakes, and the naive.16
But I’ve saved the best for last.
Big, bad ideas
The biggest problem in the field is “structuralism”:18 a simplistic overemphasis on visible and measurable signs of abnormal anatomy, position, and movement, all of which ignoring extensive evidence that these things are not what drives injury and pain. We still see an amateurish industry-wide obsession with treating the body like a fragile machine that breaks down. No matter how technical, it boils down to blaming what we can see (structure) over anything else (like physiology), and it’s all mostly barking up the wrong tree.
We have seen laudable efforts to move beyond structuralism, but that probably isn’t working out well either: legions of “progressive” professionals are shifting the blame from visible flaws and fragility to psychology and the power of the mind — which are certainly relevant, but rarely the root of the problem.
Medical and scientific meltdown
Modern, scientific medicine has also generally failed patients with puzzling chronic pain. There is a conspicuous failure of leadership from physicians in this field. Pain clinics are the only source of specialization in chronic pain, but they are not well-loved by patients, and indeed some of the most prestigious are also the most notorious and controversial.
Meanwhile, the output of the scientific publishing industry has declined precipitously in quality since the 1990s. Always somewhat dysfunctional, it is now saddled with a number of serious new modern problems. The result? We don’t have the data we need, but we do have an avalanche of poor quality studies that are used to justify a lot of nonsense as “evidence-based” — including a great deal of what goes on in mainstream pain clinics. See 15 Kinds of Bogus Citations.
•
And so … people with unexplained chronic pain bounce around the medical system like they are in an evil pinball machine of disappointment, serially misdiagnosed and mistreated and condescended to, often never finding a single doctor or therapist who recognizes the actual problem, or — having at least recognized it — has a clue what to do about it.
There is a groan that unites men and women, rich and poor, in any nation. These [muscle] pains are “explained” in every culture, but the universal fact of this persistence must mean that no adequate therapy exists.
Professor Patrick D. Wall, FRS, DM, FRCP, in the Foreword to Muscle Pain: Understanding its nature, diagnosis and treatment
Some “getting the word out” reading
- Biology is destiny. A lot of pain is caused by obscure medical problems. For every easily diagnosed cause of pain, there are a dozen that are much trickier! See 38 Surprising Causes of Pain.
- The science is a mess. Most scientific trials in musculoskeletal medicine are junky, and a high percentage are even worse (egregious pseudoscience, fraudulent, etc). See 15 Kinds of Bogus Citations and Studying the Pain Studies. More broadly speaking, it’s shocking how primitive musculoskeletal medicine, orthopedic surgery, and pain science all still are.
- Surgery is the ultimate placebo. Most orthopedic surgeries are based on tradition, authority, and the faith of surgeons, and have not been properly tested in a well-designed clinical trials. Of those that have, many could not outperform placebo, and many more will probably fail in the future. •mind blown•
- Stretching is the king of popular-but-ineffective treatments. Practically everyone thinks they should stretch, but it’s mostly a waste of time that doesn’t do anything people hope it does, other than feel good.
- The value of “clinical experience” is over-rated. It’s deeply at odds with science and evidence, and it’s a terrible way to figure out what works. “Success rates” are not something individual clinicians can actually know, and it wouldn’t constitute validation of methodology even if we could. Clinical outcomes are affected by a dazzling number of confounding factors. Most importantly, clinicians have a badly skewed sample: patients tell them about perceived successes much more than failures.
- Posture is by far the most over-rated factor in chronic pain, and a professional preoccupation with posture is amateurish. Any therapist who starts a session with a “postural scan” should be fired. See Does Posture Matter?
- The “power” of placebo is badly misunderstood and overhyped.
- The controversy over the nature of trigger points (unexplained sore spots) is a legitimate, ongoing scientific controversy. It should not be a closed topic, as argued by some critics.
Did you find this article useful? Interesting? Maybe notice how there’s not much content like this on the Internet? That’s because it’s crazy hard to make it pay. Please support (very) independent science journalism with a donation. See the donation page for more information & options.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
2024 — General improvements and modernization. I particularly fleshed out the “new” section (from 6 years ago!) about why “poor quality healthcare for chronic pain and injury is still the rule.”
2018 — Revised to properly answer a reader question: “Why is there such ignorance in musculoskeletal medicine?” It was good cynical fun trying to explain.
2017 — Cited Grant et al. and Ramos et al. on the state of evidence-based sports medicine.
2016 — Minor edit: added a particularly good turn of phrase to the conclusion (“the speculations of desperate patients and opportunistic cure purveyors”).
2016 — Minor edit: mentioned physiatry and PM&R (a strange oversight, overdue for correction).
2016 — Added more medical and scientific context and some new citations, particularly about orthopedic surgeries and opioids. Some general editing. Removed a small section of dubious value.
2016 — New introductory paragraph, for additional historical context.
2007 — Publication.
Notes
- Grant HM, Tjoumakaris FP, Maltenfort MG, Freedman KB. Levels of Evidence in the Clinical Sports Medicine Literature: Are We Getting Better Over Time? Am J Sports Med. 2014 Apr;42(7):1738–1742. PubMed 24758781 ❐
Things may be getting better: “The emphasis on increasing levels of evidence to guide treatment decisions for sports medicine patients may be taking effect.” Fantastic news, if true! On the other hand, maybe I should be careful what I wish for, since my entire career is based on making some sense out of the hopeless mess that is sports and musculoskeletal medicine …
- Ramos GA, Arliani GG, Astur DC, et al. Rehabilitation of hamstring muscle injuries: a literature review. Rev Bras Ortop. 2017;52(1):11–16. PubMed 28194375 ❐ PainSci Bibliography 52750 ❐ Yet another “garbage in, garbage out“ review of mostly hopelessly inadequate evidence, not enough for conclusions about any of the most popular treatments for one of the most common athletic injuries. A high profile injury with a clear nature, nothing subtle or weird or obscure. That’s all we’ve got at this point in history? I’m starting to wonder if this is ever going to be fixed.
- The story of anaesthesia is incredible: fatal errors were horrifying at first, largely due to lack of standardization of equipment, and then reduced to nearly zero in one the most impressive quality control initiatives in any human endeavour. The story is marvelously told in Atul Gawande’s fantastic book, Complications.
- Visualizing the History of Improving Health around the World (https://slides.ourworldindata.org/global-health/#/title-slide)
- Don’t get me wrong: there’s a lot of research. If you do a PubMed search for most pain problems, you’ll find quite a lot. But it’s a big world, and that research is dwarfed by the scale of Big Medical Science (which has been pumping out almost unbelievable amounts of research for decades). It’s a trickle of surprisingly recent, tiny, and many amateurish studies.
- Kulich R, Loeser JD. The business of pain medicine: the present mirrors antiquity. Pain Med. 2011 Jul;12(7):1063–75. PubMed 21699650 ❐ “The practice of pain medicine is often considered a fledgling field, as are the economic, business, and related ethical issues associated with providing these services.”
- Doctors are unqualified to care properly for most common pain and injury problems, especially the stubborn ones, and this has been proven by other doctors: Stockard et al. found that 82% of graduates lacked “basic competency” in this area. For more information, see The Medical Blind Spot for Aches, Pains & Injuries: Most physicians are unqualified to care for many common pain and injury problems, especially the more stubborn and tricky ones.
- Louw A, Diener I, Fernández-de-Las-Peñas C, Puentedura EJ. Sham Surgery in Orthopedics: A Systematic Review of the Literature. Pain Med. 2016 Jul. PubMed 27402957 ❐ PainSci Bibliography 53458 ❐
This review of a half dozen good quality tests of four popular orthopedic (“carpentry”) surgeries found that none of them were more effective than a placebo. It’s an eyebrow-raiser that Louw et al. could find only six good (controlled) trials of orthopedic surgeries at all — there should have been more — and all of them were bad news.
The surgeries that failed their tests were:
- vertebroplasty for osteoporotic compression fractures (stabilizing crushed verebtrae)
- intradiscal electrothermal therapy (burninating nerve fibres)
- arthroscopic debridement for osteoarthritis (“polishing” rough arthritic joint surfaces)
- open debridement of common extensor tendons for tennis elbow (scraping the tendon)
Surgeries have always been surprisingly based on tradition, authority, and educated guessing rather than good scientific trials; as they are tested properly, compared to a placebo (a sham surgery), many are failing. This review of the trend does a great job of explaining the problem. This is one of the best academic citations to support the claim that “sham surgery has shown to be just as effective as actual surgery in reducing pain and disability.” The need for placebo-controlled trials of surgeries (and the damning results) is explored in much greater detail — and very readably — in the excellent book, Surgery: The ultimate placebo, by Ian Harris.
- Even where the need for surgical intervention seems obvious, such as stabilizing a badly fractured spine, things aren’t so simple. See Spinal Fracture Bracing and Fixation: My wife’s terrible accident, and a whirlwind tour of the science and biomechanics of her spine brace.
- Cohen D. How safe are metal-on-metal hip implants? BMJ. 2012;344:e1410. PubMed 22374741 ❐ PainSci Bibliography 53447 ❐
A scholarly analysis of the safety of MoM implants:
Hundreds of thousands of patients around the world may have been exposed to toxic substances after being implanted with poorly regulated and potentially dangerous hip devices, a BMJ/ BBC Newsnight investigation reveals this week. Despite the fact that these risks have been known and well documented for decades, patients have been kept in the dark about their participation in what has effectively been a large uncontrolled experiment.
Cobalt-chromium implants have been used successfully in orthopaedics for years—for example, in knee operations and fracture repair. They are known to release metal ions, but some metal-on-metal prostheses do so on a much greater scale than previously thought. These ions can seep into local tissue causing reactions that destroy muscle and bone and leaving some patients with long term disability.
Harris tells the (chilling) story of metal-on-metal hip implants in Surgery: The ultimate placebo, one of the best-ever (and freshest) examples of surgical overconfidence.
- Vreeman RC, Carroll AE. Medical myths. BMJ. 2007 Dec;335(7633):1288–9. PubMed 18156231 ❐ PainSci Bibliography 52815 ❐
- O’Connell NE, Wand BM, McAuley J, Marston L, Moseley GL. Interventions for treating pain and disability in adults with complex regional pain syndrome. Cochrane Database Syst Rev. 2013;4:CD009416. PubMed 23633371 ❐ PainSci Bibliography 54535 ❐
- Toye F, Seers K, Allcock N, et al. Patients' experiences of chronic non-malignant musculoskeletal pain: a qualitative systematic review. The British Journal of General Practice. 2013 Dec;63(617):829–41. PubMed 24351499 ❐
This paper reviewed qualitative research on musculoskeletal pain to shed light on what it’s like to have chronic pain. Several worrisome themes were clear. Chronic musculoskeletal pain often forces patients into the awkward position of having to prove the legitimacy of their condition: “if I appear ‘too sick’ or ‘not sick enough’ then no one will believe me.” Many end up doubting themselves and questioning their own identity and wondering who is “the real me.” Many lose hope and feel lost (or lost by) the health care system.
- Certification rackets are rampant: professionals routinely invest deeply in training and certifications of extremely dubious value. Freelance healthcare professionals are inherently biased towards whatever is emotionally appealing to their customers. Insurance is a major source of bizarre incentives: patients will seek out a specific bogus therapy, and professionals will provide it, simply because insurance will pay for it (insurance-based medicine). The profit motive is strong! Consider that orthorpedic surgeries are fantastically profitable for American orthopaedic surgeons (and there are many lesser examples). All of this stuff pulls clinicians towards “faith” in their methods, rather than the evidence.
- Both massage and chiropractic are guilty of believing and promoting an astonishing array of pseudoscientific ideas and therapies. See The Chiropractic Controversies, Does Massage Therapy Work? and 💩 Massage Therapists Say.
- Acupuncture has a good reputation that it does not deserve. Although heavily researched, its support comes only from biased junk science, while it fails all the good quality scientific tests. It does not work for pain or anything else and we shouldn’t be surprised: it’s based on mysticism and myths. It’s surprisingly modern rather than ancient and wise, for instance, and cannot actually be used for anesthesia. More study is not needed. For more information, see Does Acupuncture Work for Pain? A review of modern acupuncture evidence and myths, focused on treatment of back pain & other common chronic pains.
- Pseudo-quackery is quackery that passes for good medicine despite strong evidence that it doesn’t work. Unfortunately, not all quackery is obvious — not even to skeptics. “Pseudo-quackery” appears to be mainstream, advanced, technological, “science-y,” or otherwise legit — quackery without any sign of being way out in left field. It has enough superficial plausibility to persist in the absence of evidence against it. This subtler type of snake oil is a more serious problem in musculoskeletal health care, because it hides right in the mainstream. For instance, it’s nearly synonymous with the early history of physical therapy, and remains alarmingly prevalent in that profession. So pseudo-quackery is extremely common, and generates more false hopes and wasted time, energy, money, and harm than more overt quackery, which is relatively marginalized. See Pseudo-Quackery in Physical Therapy: A large and dangerous grey zone between evidence-based care and clear quackery in rehab and pain treatments.
- Ingraham. Your Back Is Not Out of Alignment: Debunking the obsession with alignment, posture, and other biomechanical bogeymen as major causes of pain. PainScience.com. 21878 words.