IT Band Stretching Does Not Work
Stretching the iliotibial band is a popular idea, but it’s very hard to do it right, and it’s probably not worth it

What’s wrong with this picture?
She’s not doing much with this classic IT band stretch — even if her technique was good (it’s not). Read on to find out why.
Iliotibial band stretches don’t work? Really?! So why does it seem like they are prescribed for iliotibial band syndrome — runner’s knee — by practically every physical therapist in the world?
IT band stretching is just another obsolete bit of simplistic conventional wisdom, like countless other shabby old ideas that have been repeated ad nauseam on the Internet. At best, stretching your iliotibial band is probably only slightly helpful. At worst, IT band stretching is just wastes your time and reinforces misconceptions about the cause of IT band pain.
And that’s all assuming you are actually even applying tension your IT band in the first place — which is biomechanically tricky.
Most people never succeed in pulling firmly on their iliotibial bands. All the commonly prescribed stretches are mechanically ineffective.1 There is research available that shows how to apply tension to the IT band effectively, but almost no one seems to know about it.
Prefer video? Here’s a video tour of basic IT band myths, including the stretching myth:
Stretching is over-rated in general, but especially so for runner’s knee
Stretching has a much better reputation than it deserves,2 and an especially so in this case. Stretching is by far the most common advice given to people with lateral knee pain. Most ITBS patients are told to stretch by a doctor, physical therapist, or massage therapist. But there is no evidence that stretching will prevent3 or fix4 IT band pain. No researchers have studied the problem properly, and the preliminary data is underwhelming. Not only is the IT band a difficult structure to stretch, but it is doubtful that IT band tightness is even a problem that needs solving.
It is not safe to assume that stretching works just on the say-so of your physiotherapist, or running mates who swear by it, or because it’s recommended by almost every article on the Internet about IT band syndrome.
Applying strong tension to the IT band is just really tricky
It’s not easy to stretch the iliotibial band. Not easy at all. In fact, it’s possible that it’s impossible.
The most common kind of stretches recommended for the iliotibial band are also the least likely to be effective, simply because they are focused on stretching the iliotibial band and the tensor fasciae latae muscle, and there is no good way of applying any significant amount of stretch to these structures. Not everything in the body can be stretched, just like not every muscle can hoist a heavy barbell.5 There are biomechanical difficulties with stretching some anatomy, like all three of the structures most relevant to IT band syndrome:
The hip joint and shorter hip muscles are the structures that limit range of motion in an idealized stretch of the iliotibial band. This was competently demonstrated in 2016 by Willett et al.,6 Their point was to test a test: the Ober test, the test supposedly used to measure the tightness of the IT band. What they found was that it did no such thing. Instead, it was measuring the “tightness of structures proximal to the hip joint, such as the gluteus medius and minimus muscles and the hip joint capsule.”
If you can’t test the tightness of the IT band that way, then you can’t stretch it therapeutically either. The Ober test is a theoretically ideal stretch, and it’s not actually stretching the IT band (or not primarily). Other structures get in the way, and the structures we want to stretch — the IT band and the muscles that pull on it — are hard to apply tension to …
- The iliotibial band itself is just too tough to be stretched. Even smaller tendons that are easy to pull on are extremely difficult to elongate, requiring long hours of painful stretching such as dancers and gymnasts do. But the ITB is the longest and most massive tendon in the human body. It’s also not free to move like most tendons: it’s anchored along the length of the femur.7 Imagine bolting a 2-foot strip of thick tire rubber to a plank of wood in several places. Now try to “stretch” it! You might be able to apply some tension to it, but it’s certainly not going to elongate significantly.
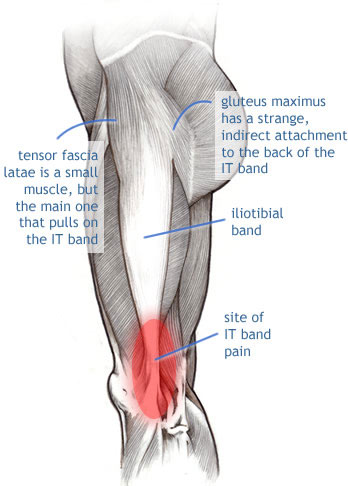
- The tensor fasciae latae, the muscle that most directly controls tension on the iliotibial band, is the most promising target for stretch. It is a hip abducting muscle, so to stretch it you primarily have to adduct the hip: that is, the leg must move towards the midline. But there is not much movement available in that direction: the other leg is in the way. The best that anyone can do is to cross the (stretch-side) leg over the other leg, and push the pelvis out. It is possible to stretch the TFL and IT band in this manner … but not strongly.
- The gluteus maximus is mostly unstretchable: a surprisingly long muscle, it is just impossible to flex the hip enough to apply much tension to it, because the thigh meets the belly too early … even in a skinny person. In someone with a bit of belly fat, it’s hopeless.
- In addition to its extraordinary toughness, the IT band is also probably more elastic than most tendons, as a functional feature.8 This is not a contradiction: things can be both extremely tough and elastic (like these super rubber bands — unbreakable, but still elastic). Whatever elongation you can get out of an IT band is only what it allows by nature — you can’t stretch it past that point, and by nature it will snap back to its resting length effortlessly, as though you never did anything.
Two things missing from standard iliotibial band stretches
The usual IT band stretches are missing a crucial component: knee flexion. For any hope of stretching this structure, you simply have to include knee flexion. And yet almost no one does.
As discussed above, the iliotibial band does not have a well-defined attachment point on the knee, the way most tendons do. Instead, it spreads out and blends into the capsule of connective tissue that surrounds the knee. Thus, knee position clearly affects tension on the iliotibial band — and it has long been recognized that the iliotibial band is tightest around 30˚ of flexion,9 though some evidence shows than flexion beyond 90˚ may apply even more tension.10
And there’s more.
Another element that is important but often overlooked is “anchoring” the pelvis. The IT band “hangs” from a “hook” on the front of the pelvis called the anterior superior iliac spine (ASIS). If you want to stretch something attached to the ASIS, the ASIS has to be held still, or pulled the other way. Just lean your torso away from that corner of the pelvis. This takes up the slack in the lateral and anterior abdominal muscles, pulling up on the front of the pelvis. Raising the arms too: that takes up a lot of slack in the very long latissimus dorsi muscles, which tightens the broad thoracolumbar fascia like a girdle, which helps to anchor the pelvis.11
No elongation: you can’t make your IT band “longer”
Even if you do everything right, even if you perform the ideal stretch and manage to pull firmly on your IT band for a couple minutes — which is longer than most people ever bother — how much would you actually change the length of your IT band? How far would it move?
Roughly 2 millimeters — an overall change in length of less than half a percent.
You still won’t actually change its length, any more than you can make a leather belt longer by pulling on it. This is the most important thing IT band stretchers need to understand.
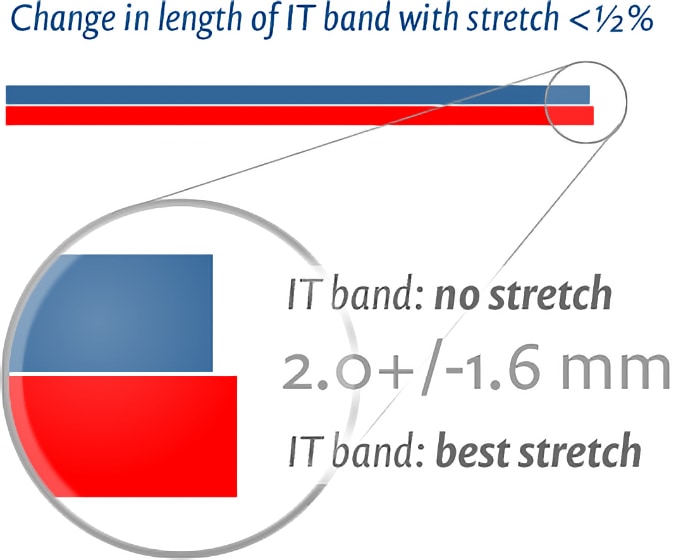
In 2010, Irish researcher Dr. Eanna Falvey and her colleagues measured the mechanical effect of a basic IT band stretch (like the standard one illustrated at right) plus a more sophisticated stretch, and found virtually no difference: the IT band was effectively unaffected. And that was including knee flexion, in a stretch carefully applied to corpses by anatomists!1213 In an even more aggressive experiment in 2017, the IT band was completely excised, washed, frozen, thawed, and machine-stretched … and it still stretched only a few millimetres.14
If those tactics can’t elongate the IT band, runners don’t stand a chance.
And so, unfortunately, conventional iliotibial band stretches, prescribed and described practically everywhere — even the better ones — are simply not able to do the job. Assuming it’s even a job worth doing.
Some stretching hope: a better iliotibial stretch?
There are better IT band stretches than the conventional stretches — primarily adding knee flexion, though some other refinements are also possible — and there are some reasons to suspect that applying tension might still be a little bit therapeutically useful even if actual elongation is impossible. As with most therapies, the neurology of sensation is probably more important than any alleged tissue change: stretching the IT band may change how the brain “feels” about the knee.15 I have seen stretching appear to help IT band syndrome.
But there are better treatment options for IT band syndrome than stretching. Practically everyone who is looking for IT band stretching information would be better off learning much more about IT band syndrome first, because the subject is a minefield of myths and misconceptions (not just about stretching):
- Most physiotherapists still prescribe ITB stretches without any evidence that they work, and many reasons to believe they won’t … and they aren’t even the best ITB stretches.
- Most massage therapists still try to “elongate” your iliotibial band with long deep strokes — which works about as well as it would on a truck tire — while usually ignoring the muscles that actually control ITB tension, the all-important tensor fasciae latae and even your gluteus maximus.
- Most chiropractors still waste your money on wild goose chases to treat crooked pelvises and short legs, which have never been shown to have anything to do with ITBS.
- Most doctors still call it a “friction” syndrome even though the scientific evidence now strongly suggests that “friction” has nothing to do with it. They also rarely know much about medical options like cortisone injections or IT band release surgery.
Some health professionals have taken the time to study ITB syndrome properly, of course. But it’s usually impossible to luck out and find one before your training schedule is blown to smithereens.
There are no miracle cures for IT band syndrome
So do I think stretching is pointless or effective? Sharp-eyed readers will notice a contradiction: I’ve written many things about stretching in general, and stretching for ITBS especially, that sound like I think it’s pointless. And yet I have also credited it with seeming to contribute to my own recovery, and I still actually recommend trying it. What gives? What is it, thumbs up or down?
For my most positive take on ITB stretching, I’m grading on a curve 😜 and assuming good technique (which is rare). It’s not completely implausible that it could be effective, if done properly. It’s also cheap, easy, and quite safe to experiment with. Also, my own personal experience has some weight (not much, but some). These factors upgrade what would otherwise be a negative opinion up to a “cautiously optimistic” one, making it one of the least-terrible options available.
Learn much more
This article is an excerpt from a much larger tutorial for both patients and professionals. The whole thing contains basically everything there is to know about ITB syndrome. There is no foolproof system for beating iliotibial band syndrome, or even a reasonably reliable one (and please do not believe anyone who says there is). But if you read the full tutorial, I can guarantee that you will know the condition better than most doctors, and you will understand the imperfect options and how to prioritize them.

Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
| company | PainScience.com |
|---|---|
| owner | Paul Ingraham |
| contact | 778-968-0930 |
| refunds | 100%, no time limit +Customers are welcome to ask for a refund months after purchase — I understand that it can take time to decide if information like this was worth the price for you. |
| more info | policies page ❐ |
| payments |
- What do you get, exactly? An online tutorial, book-length (84 chapters). Free updates forever, read on any device, and lend it out. E-book only! MORE
- Secure payment takes about 2 minutes. No password or login: when payment is confirmed, you are instantly granted full, permanent access to this page.MORE
- Collect them all. Get an “e-boxed” set of all 10 PainScience.com tutorials, ideal for pros … or patients with a lot of problems.MORE
Q. What am I buying? Is there an actual paper book?
A. Payment unlocks access to 73 more chapters of what is basically a huge webpage. There is no paper book — I only sell book-length online tutorials. This format is great for instant delivery, and many other benefits “traditional” e-books can’t offer, especially hassle-free lending and updates. You get free lifetime access to the always-current “live” web version (and offline reading is easy too).

Read on any device. Lend it out. New editions free forever.
Q. I just don’t like reading on the computer! Is there any way around that?
A. The design and technology of the book is ideal for reading on tablets and smart phones. You can also print the book on a home printer.
Q. Can I lend the tutorial out?
A. Yes! Feel free to lend your tutorial: I do not impose silly lending limits like with most other ebooks. No complicated policies or rules, just the honour system! You buy it, you can share it. You can also give it as a gift.
Q. Is it safe to use my credit card on your website?
A. Literally safer than a bank machine. Payments are powered by Stripe, which has an A+ Better Business Bureau rating. Card info never touches my servers. It’s easy to verify my identity and the legitimacy of my business: just Google me [new tab/window].
Q. I can really get a refund at any time?
A. Yes. All PainScience.com ebooks have a lifetime money-back guarantee.
Q. Why do you ask for contact information?
A. To prevent fraud and help with order lookups. You aren’t “subscribing” to anything: I never send email to customers except to confirm purchases.
Q. Can I buy this anywhere else? Amazon?
A. Not yet. Maybe someday.
See the “fine print page” for more about security, privacy, and refunds. No legalese, just plain English.
Save a bundle on a bundle
The e-boxed set is a bundle of all 10 book-length tutorials for sale on PainScience.com: 10 books about 10 different common injuries and pain problems. All ten topics are (all links open free intros in a new tab/window): muscle strain, muscle pain, back and neck pain, two kinds of runner’s knee (IT band syndrome and patellofemoral pain), shin splints, plantar fasciitis, and frozen shoulder. (Headache coming soon, fall of 2019.)
Most patients only need one book, because most patients have only one problem. But the set is ideal for professionals, and some keen patients do want all of them, for the education, and for lending to friends and family. And, of course, you do get a substantial discount for the bulk purchase. But no rush—complete the set later, minus the price of any books already bought. More information and purchase options.
If you choose to buy, thanks in advance for your business, and please feel free to write to me about something unusual or interesting about your case. I routinely make improvements to the tutorial as a result of feedback from runners and readers and health care professionals around the world.

Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
And you can also keep reading for free. The book page has a substantial free introduction, and there other free samples from the book and closely related articles:
- EXCERPT Does the IT Band Move After All?
- EXCERPT The Causes of Runner's Knee Are Rarely Obvious
- EXCERPT Do IT Band Straps Work for Runner’s Knee?
- IT Band Pain is Knee Pain, Not Hip Pain — Pain in the hip and thigh is something else, I promise
- Is IT Band Tendinitis Really a Tendinitis? — Research has clearly shown that the IT band itself is probably not the anatomy that gets inflamed … which has significant implications for treatment
- Diagnosing Runner’s Knee — It usually starts with lateral knee pain during and after runs, but there are two major types
- Is Running on Pavement Risky? — Hard-surface running might be a risk factor for running injuries like patellofemoral pain, IT band syndrome, shin splints, and plantar fasciitis
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
What’s new in this article?
2017 — Cited and discussed the implications of Eng 2015, which purports to show that the IT band uses elastic energy to enhance running efficiency.
2017 — Added important new point about why the IT band is hard to stretch, based on Willett et al.
2017 — Added a new citation to Umehara et al. on the effect of knee flexion on stretching, added an important point about the relevance of sensitization, updated the footnote about stretching being overrated overall, added a related reading section.
2017 — Major update. Comprehensive editing and modernization, added a key new reference to Wilhelm et al., several clarifications and a new (and more optimistic) ending, and corrected minor errors that had accumulated over time.
2012 — Publication.
Notes
- Not universally, of course. Some therapists will know this stuff. But let me put it this way: I worked with ITBS patients routinely for a decade, and in that time the number of patients I saw who’d been taught to stretch properly by another therapist … I can count them on one hand. The huge majority were given the standard, inadequate stretch.
- Research has clearly shown that conventional stretching isn’t good for much, and may even be harmful (minor harm to perform, some risk of injury). Although it can increase flexibility, that has no inherent value if you don’t actually need it (martial arts, gymanstics, etc), and flexibility can also be achieved by full ROM strength training — and why wouldn’t you want to get stronger at the same time you’re building flexibility? Stretching certainly feels good and the movement and stimulation is probably good for us in subtle ways, but it’s value is much less clear than most people believe. See Quite a Stretch: Stretching science has shown that this extremely popular form of exercise has almost no measurable benefits.
- Brushøj C, Larsen K, Albrecht-Beste E, et al. Prevention of overuse injuries by a concurrent exercise program in subjects exposed to an increase in training load: a randomized controlled trial of 1020 army recruits. Am J Sports Med. 2008 Apr;36(4):663–670. PubMed 18337359 ❐ This study showed “no significant differences in incidence of injury” in soldiers doing preventative exercises for commmon overuse knee injuries, especially iliotibial band syndrome and patellofemoral pain syndrome (two kinds of runner’s knee). The authors concluded that the exercises “did not influence the risk of developing overuse knee injuries or medial tibial stress syndrome in subjects undergoing an increase in physical activity.” The exercise regimen certainly included static stretching, and it certainly did not work any prevention miracles for iliotibial band syndrome.
- Khaund R, Flynn S. Iliotibial Band Syndrome: A Common Source of Knee Pain. Am Fam Physician. 2005 Apr 15;71(8). PainSci Bibliography 56763 ❐ From the article: “ … studies have not demonstrated that stretching hastens recovery from [iliotibial band] syndrome.”
- Ingraham. The Unstretchables: Eleven muscles you can’t actually stretch hard (but wish you could). PainScience.com. 5105 words.
- Willett GM, Keim SA, Shostrom VK, Lomneth CS. An Anatomic Investigation of the Ober Test. Am J Sports Med. 2016 Mar;44(3):696–701. PubMed 26755689 ❐
- Fairclough J, Hayashi K, Toumi H, et al. The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome. J Anat. 2006 Mar;208(3):309–316. PubMed 16533314 ❐ PainSci Bibliography 56738 ❐ Many therapists don’t believe this at first — it doesn’t jibe with the anatomy they learned in school. But this anchoring arrangement was discovered (or clarified) by researchers many years ago now. The attachment is not through the big thigh muscles, but behind them. Attachment is more direct in the distal femur. Here’s the relevant sentence from the paper: “This layer of deep fascia completely ensheathed the thigh and was continuous with the strong lateral intermuscular septum, which was firmly anchored to the linea aspera of the femur.”
- Eng 2015, op. cit. Briefly recapping: this study shows that the IT band “may contribute to energy savings during locomotion,” an elastic energy storage structure like the Achilles tendon. Although all tendons are extensible to a point, not all of them are equally elastic, and most don’t use their elasticity to actively put energy back into the system (it might only be these two that have that trick).
- As early 1979, Noble wrote that, “Tenderness over the lateral epicondyle associated with pain at 30 degrees of flexion on compressing the iliotibial band against the lateral epicondyle is diagnostic.” In 1996 Orchard shows the practical, painful reality of this in the biomechanics of running. In 2006, Fairclough confirmed that tension on the iliotibial band is greatest at 30˚ of flexion.
- Umehara J, Ikezoe T, Nishishita S, et al. Effect of hip and knee position on tensor fasciae latae elongation during stretching: An ultrasonic shear wave elastography study. Clin Biomech (Bristol, Avon). 2015 Dec;30(10):1056–9. PubMed 26388173 ❐ “…investigate the effects of hip rotation and knee angle on tensor fasciae latae elongation during stretching in vivo using ultrasonic shear wave elastography…”
- Fredericson M, White JJ, Macmahon JM, Andriacchi TP. Quantitative analysis of the relative effectiveness of 3 iliotibial band stretches. Arch Phys Med Rehabil. 2002;83(5):589–592. “Adding an overhead arm extension to the most common standing ITB stretch may increase average ITB length change … in elite-level distance runners.” Not that we can actually change the length of the IT band …
- Falvey EC, Clark RA, Franklyn-Miller A, et al. Iliotibial band syndrome: an examination of the evidence behind a number of treatment options. Scand J Med Sci Sports. 2010 Aug;20(4):580–7. PubMed 19706004 ❐
- Many people will reasonably question the value of a dissection study — so different than the living body! However, the clinical relevance of studies on corpses varies with context. Certainly many things can and have been learned from dissection. In this case, we’re looking exclusively at whether or not an anatomical structure can be elongated when pulled on. It’s not a test of stretching effectiveness in the real world, but of the mechanics and anatomy of the stretch. If a well-executed passive stretch does not elongate the IT band in a corpse, is it likely that a living person could do any better? Do live IT bands respond very differently to being pulled on? I doubt that.
The result is also consistent with a lot of other evidence and with other aspects of the anatomy of the structure, established in this and other studies, particularly that it is anchored to the femur along most or all of its length. It is not an “elongatable” structure. This can be established as well on a corpse as in the living — probably better.
We then can decide what to make of that — that is, what clinical implications arise — but the biomechanical facts are difficult to dispute here. The response that “it’s just a dissection study” is a convenient way to dispose of inconvenient, myth-busting evidence. But dissection studies have their place and are very good at determining things just like this, and that’s why we do them. - Wilhelm M, Matthijs O, Browne K, et al. Deformation Response of the Iliotibial Band-Tensor Fascia Lata Complex to Clinical-Grade Longitudinal Tension Loading in-Vitro. Int J Sports Phys Ther. 2017 Feb;12(1):16–24. PubMed 28217413 ❐ PainSci Bibliography 53506 ❐
This is an in vitro study of the effect of pulling on a dissected IT band, removed from a corpse. This is not necessarily a pointless thing to do (in vitro experiments have their uses), but in this case the IT band was aggressively harvested: completely removed from its complex anatomical context, cleaned, frozen, warmed up to 20˚ C, and then machine-stretched … although we can learn things from this, it’s important to emphasize that the differences from biological and clinical reality are piled high here.
The abstract of the paper “advertises” a statistically significant effect of machine stretching on an excised IT band … but not a clinically significant effect. They report an elongation of just a few millimeters. In the main text, they concede that “the current study’s findings are in agreement with those of Falvey et al. demonstrating minimal stretching of the ITB”! (Falvey et al. is the paper most cited to argue that the IT band cannot be meaningfully stretched, and this paper is “in agreement” with it, demonstrating “minimal stretching.”)
They also write: “it is unlikely that … ‘clinical stretching’ produces permanent ITB deformation.” So despite superficial appearances to the contrary, this paper clearly actually reinforces the point that IT band stretching is futile (to the extent that stretching a completely dissected IT band can tell us anything at all).
I got a chuckle out of this:
“While the tissue used for the present analysis was harvested from a specimen sample that was older than those individuals who would likely develop ITB pain, it is difficult to obtain cadaveric tissue samples from a younger population for testing.”
Indeed.
- By far the clearest result of 21st Century pain science so far is that chronic pain is aggressively multifactorial, and routinely has a strong component of sensitization: an over-reactive, paranoid central nervous system that is producing a louder, longer alarm (pain) in reaction to less and less actual trouble in the tissue. Anything that “reassures” the brain and convinces it that there’s no actual danger, and therefore no need for pain, may be quite helpful. There’s no direct evidence that stretching can help ITBS by this mechanism, but the phenomenon of sensitization is very well-etablished, and it’s much more plausible than the idea that stretching causes a helpful change in the IT band itself.
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help