Knee Replacement Surgery Doubts
Is it legit? Knee replacement is extremely popular, but it (still) isn’t evidence-based medicine
{kind=link}
Various types of knee replacement surgeries (arthroplasties) are a popular choice for people with intractable knee pain caused by osteoarthritis. Both partial and total knee replacement (PKR, TKR) are common. As the technology improves, it’s also becoming available to younger patients. This is a huge industry, delivering hundreds of thousands of knee replacements annually in the US, and millions globally.
That’s a lot of bionic knees.
This short article raises a few key concerns about the efficacy of knee replacement. Only you and your surgeon can decide if it’s a good idea for you, but I hope some of these points will contribute to that conversation.
Just a single almost good TKR study
There’s a great deal of research on this topic, but almost none of the kind that we actually need to determine the efficacy of any treatment: a truly controlled trial. There’s just one trial that gets us halfway there! Just one prominent study that has directly compared surgery to doing nothing, as well as higher quality non-surgical care.1 The New England Journal of Medicine reported in 2015 that surgery TKR got clearly better results, but also had a lot more complications.
That’s roughly a tie between the pros and the cons, which is not an encouraging outcome for people considering surgery.
High-quality evidence to support the effectiveness of the procedure, as compared with nonsurgical interventions, is lacking.
Skou et al., 2015, New England Journal of Medicine
That trial isn’t definitive. It’s the wrong design. The needed to compare real surgery to fake surgery — not non-surgical treatment.
Still no placebo-controlled trials! For one of the most profitable procedures in the history of medicine
What if the pain relief reported by Skou et al. wasn’t actually caused by the surgery? What if a fake surgery had the same effect? Just putting someone under, cutting them open, and then closing them up again? When they wake up, congratulate them on a successful surgery?
No one has checked. And they really should.
There’s a real possibility that the pain relief may have been entirely or substantially driven by placebo. Surgery can be an extremely powerful generator of placebo effects, because of the strong hopes it generates. It sounds bizarre, but it has already been demonstrated about many other popular surgeries.2345 It would be foolish to assume that knee replacement is any different. It might be different. Some procedures, for some patients, clearly have value. But it’s not a safe assumption, not by a long shot.
The active ingredient of surgery is often faith, not what the surgeon actually does. And yet there are no placebo-controlled trials of knee replacement at all yet, despite the existence of many of these studies for other popular orthopedic surgeries… most of which have demonstrated that pain relief still occurs with sham surgery!
This excellent 2016 book by Ian Harris, an orthopedic surgeon, explores the shameful history of untested surgeries in detail. It’s fascinating and mostly easy enough reading for patients. Highly recommended. Start with an excerpt.
Total versus partial knee replacement: Is more surgery better? Is less worse?
We don’t have enough research comparing knee replacement to nothing or a sham — and we really need that — but how about total versus partial? A PKR, in a way, a partial sham of TKR. What if researchers asked the question, “Is doing half as much surgery just as good as doing the whole thing?”
They did. And they got an answer. After collecting data for five years, Beard et al. reported in Lancet that TKR and PKR get results that are … about the same!6
“Both TKR and PKR are effective, offer similar clinical outcomes, and result in a similar incidence of re-operations and complications. Based on our clinical findings, and results regarding the lower costs and better cost-effectiveness with PKR during the 5-year study period, we suggest that PKR should be considered the first choice for patients with late-stage isolated medial compartment osteoarthritis.
Less surgery can routinely be just as good as more. Partial absolutely competes with total. Good to know. This strong suggests that a great deal of TKR has been (at least) more than those patients actually needed, more than they could benefit from.
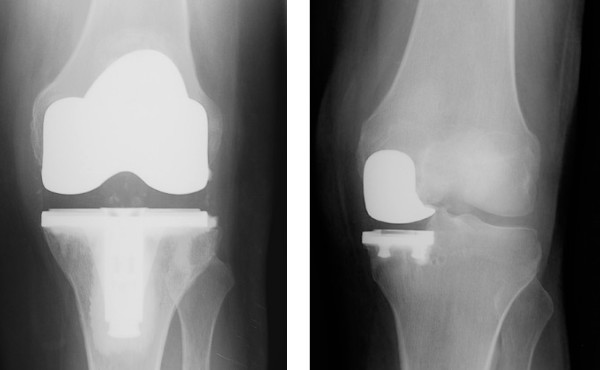
Total versus partial knee replacement implants
There’s just a lot less titanium in a partial knee replacement—it’s more like a “patch” of metal. And yet both types of surgery have remarkably similar outcomes.
So why does everyone seem to act like knee replacement is evidence-based?
If you browse scientific paper conclusions casually, it would be easy to think that everything in Knee Replacement Land is pretty great. Start reading more carefully, however, and the caveats are everywhere.
Even patient satisfication scores — which are grossly inadequate and misleading evidence even when done right7 — have been measured with a valid method in only 13% of more than 200 studies.8
It’s all much ado about nothing without the right studies: fair tests comparing to real surgery to a sham. Without those tests, we cannot even know if knee replacement is efficacious. This is unambiguously true, science 101.
Orthopedic surgery as a profession has much to be ashamed of: decades of much lower standards for evidence-based care than have been considered normal in virtually every other part of health care, even long before evidence-based medicine got more rigorous in the 90s.9 They have been working in a little bubble of authority-based medicine, where RCTs have been considered unnecessary or impossible, both of which are absurd.10 It will probably take a new generation of surgeons to move beyond this.
It is difficult to get a man to understand something when his job depends on not understanding it.
Upton Sinclair
Persistent post-surgical pain: a complication, or a normal side effect?
About 20% of patients who undergo knee replacement suffer from moderate to severe pain six months after the operation, and 16% were still in trouble at 12 months.11 The patients who suffered this unpleasant outcome were more anxious by nature (“trait” anxiety as opposed to “state”), had more pain before surgery than average, and expected more pain after. Just as optimism and faith may drive good surgical results, fear and pessimism can drive terrible outcomes.12
And the mind is surely not the only reason for persistent post-surgical pain.
A lot of patients with pain after surgery are told by their surgeon that it’s “normal.” This can be completely correct and fine in the short term… or incompetent evasion later on.
Increased persistent pain is always considered a complication. However it’s a bit complicated by the fact that some degree of post-surgical pain is normal — but exactly how much and for how long? At what point do you say that post-surgical pain is a complication rather than an expected side effect? There’s such a wide grey zone in there that, in general, pain levels in the first few months are rarely measured (or considered definitive). Instead, you measure pain levels many months or years after surgery. Increased pain at 3 months? Ambiguous. At 6 months? Starting to look like an adverse effect, but still ambiguous. A year? Definitely a complication.
Confidence and optimism versus the truth
Fearing the worst from a knee surgery is at least partially a self-fulfilling prophecy: the more worried you are, the worse things tend to go. Dr. Gary J Macfarlane, regarding his paper on knee replacement results:13
“We identified 3 distinct response trajectories in patients undergoing knee replacement. Expectations of pain/limited function and poor coping strategies differentiated the trajectories, suggesting a role for preoperative psychosocial support in optimizing the clinical outcome.”
And so it also seems likely that anything at all that increases patient optimism and confidence would probably help. This is consistent with a large body of relevant evidence on the power of mind-over-pain — which is not an easily controlled power, but a power nevertheless.14
It’s also a dilemma for health science reporting and clinicians: truth may be harmful! The discouraging reality about side effects, poor outcomes, and other bad science news may make patients more pessimistic and fearful, and actually cause worse outcomes. But we cannot lie or conceal the truth, either! Awkward. 🎵 The truth may be problematic, but it’s also unavoidable and essential. There is no easy solution to this dilemma.
But consider this: the same confidence and optimism that helps surgical patients almost certainly also applies to outcomes for patients who do not get surgery. •head explodes•
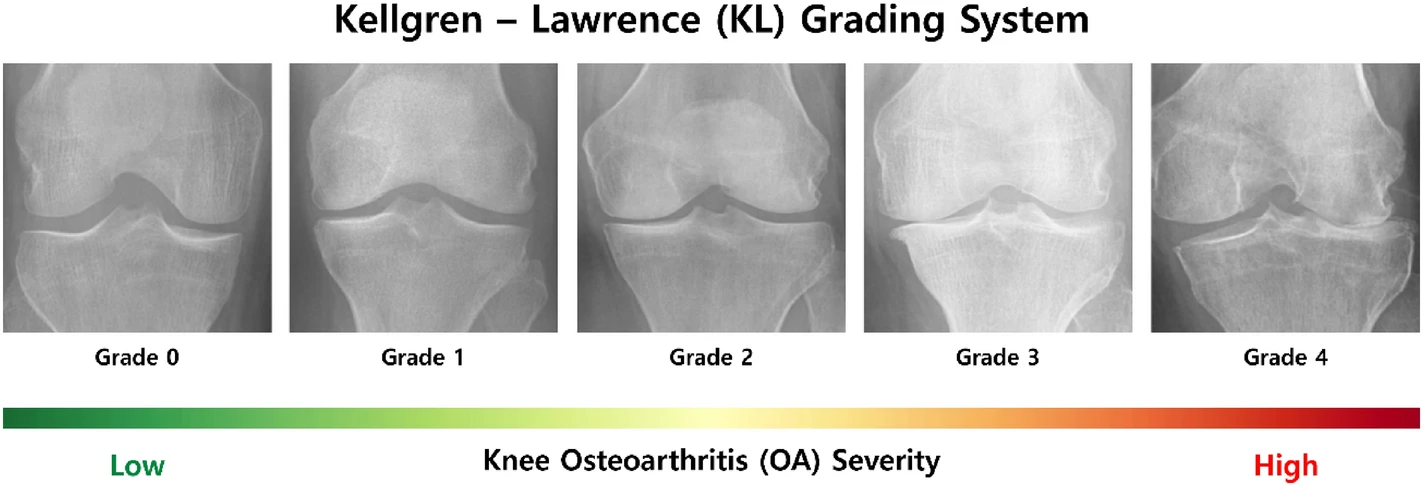
Knee joint X-rays for each KL grade according to OA severity. The KL grade system categorizes grades according to two aspects of OA: the extent of joint space narrowing, and the size of osteophytes (spurs). From Ensemble deep-learning networks for automated osteoarthritis grading in knee X-ray images, by Pi et al., CC BY 4.0.
Severe arthritis: does “bone-on-bone” mean you need surgery? You should be more worried about surgeons who say BOB than your arthritis
Most people assume that BOB means that arthritis is severe and surgery is either imminent or inevitable. That notorious pseudo-diagnosis is almost synonymous with the belief that some kind of drastic action is required!
But how often is BOB actually true? It is routinely an exaggeration of the state of the joint (which often cannot even be known with any precision). I think many orthopaedic surgeons, especially in America, have a tendency to deploy BOB to close the deal when patients are waffling:
PATIENT: Well, maybe … but the risks are real. Maybe it’s too soon?
SURGEON: Maybe. But we are talking bone-on-bone here, so …
PATIENT: I guess it can’t get much worse than that! Shut up and take my money.
Even when BOB is accurate (severe arthritis certainly does exist), it’s often not nearly as bad BOB makes it sound, and surgery may well still be premature. For instance, my father — who has a very dramatic case of arthritis induced by a 50-year-old gunshot wound acquired in Vietnam — was told almost thirty years ago that his knee was “shot,” ha ha, and already bone-on-bone. But he has lived remarkably well with his objectively “severe” arthritis ever since. He has rough patches, but they aren’t too bad, and they end, and then he’ll go month without anything more than minor aggravation. He is a more or less perfect example of how bone-on-bone is not necessarily mean that symptoms are severe or that surgery is necessary. I know my father's case the best, but I also know of many other like this.
Not only does BOB tend to provoke premature surgery, it also — even more disastrously — scares people away people from exercise, for fear of wear and tear that is not actually a problem for arthritis. But inactivity actually does make arthritis worse, along with much else. Beware of BOB!
BOB is a big topic, which I cover in much more detail in a separate article:
Bottom line
Does knee replacement work? No one really knows, period — there simply isn’t enough of the right kind of evidence. It is effectively an experimental treatment.
Meanwhile, there is now substantial evidence that several similar orthopedic surgeries cannot help people more than a sham.
If your surgeon reacts defensively to these concerns, seek a second opinion.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Related Reading
- Knee Debridement is a Completely Ineffective Procedure — Evidence that arthroscopic knee surgery for osteoarthritis is about as useful as a Nerf hammer
- Should You Get A Lube Job for Your Arthritic Knee? — Reviewing the science of injecting artificial synovial fluid, especially for patellofemoral pain
- Bone on Bone — How often are those dirty words about arthritis a harmful exaggeration? And should we ever use them, even when it’s accurate?
- MRI and X-Ray Often Worse than Useless for Back Pain — Medical guidelines “strongly” discourage the use of MRI and X-ray in diagnosing low back pain, because they produce so many false alarms
- Placebo Power Hype — The placebo effect is fascinating, but its “power” isn’t all it’s cracked up to be
- Surgery: The ultimate placebo (book), by Ian Harris (book review). What if a fake surgery had the same effect as a real one, because the “active ingredient” in surgery is just the dramatic ritual? What if surgery delivers a huge placebo effect? This often appears to be case, as shown in a few well-known examples, and a steadily growing list of new ones. But many common orthopedic surgeries have still never been subjected to the gold standard of evidence-based medicine, the randomized controlled trial. Instead, they are based mainly on tradition, authority, and the “common sense” of surgeons, who have been slow to embrace the need to subject their methods to trials, citing a list of typical reasons — none of which stand up to scrutiny, and sound more like turf-defending excuses every year (like a strong example as recently as 2025, see Block and burn for backs and necks bombs a big test, doctors bluster). In this superb book, orthopedic surgeon Dr. Ian Harris explores the shameful history of untested surgeries in detail. It’s fascinating, and mostly easy enough reading even for patients. There’s a free excerpt from the book that you can read to get started. Many scientific papers before and since publication of the book have supported Harris’ position. See Louw et al. and Blom et al.
- Does Cartilage Regeneration Work? — A review of knee cartilage “patching” with autologous chondrocyte implantation (ACI).
What’s new in this article?
Five updates have been logged for this article since publication (2019). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
Like good footnotes, update logging sets PainScience.com apart from most other health websites and blogs. It’s fine print, but important fine print, in the same spirit of transparency as the editing history available for Wikipedia pages.
I log any change to articles that might be of interest to a keen reader. Complete update logging started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
2024 — New section: “Severe arthritis: does ‘bone-on-bone’ mean you need surgery? You should be more worried about surgeons who say BOB than your arthritis.”
2021 — New section based on Hamilton et al.: “Confidence and optimism versus the truth.”
2021 — Some editorial polishing and three new images.
2021 — Science update and new section: “Total versus partial knee replacement: Is more surgery better? Is less worse?” Also cited more evidence on the role of the anxiety and fear in post-surgical pain. Updated Skou 2015 with data from Skou 2018 and added a full description of that research. Clarified the importance of sham-controlled surgical trials.
2019 — New section: “Is pain after surgery a complication or a normal side effect?”
2019 — Publication.
Notes
- Skou ST, Roos EM, Laursen MB, et al. A Randomized, Controlled Trial of Total Knee Replacement. N Engl J Med. 2015 Oct;373(17):1597–606. PubMed 26488691 ❐
(See also Skou 2018, a follow-up study that basically extended the trial, adding more data: “Combined reporting of the two trials allowed more in-depth comparison of available treatment options.”)
Skou et al. found a lots of people who weren’t eligible for surgery for various reasons. Some of those were virtually ignored (just given educational pamphlets, the “basically nothing” group), and the rest were given the best possible care, basically everything medicine could throw at them that wasn’t surgery: exercise, education, dietary advice, use of insoles, and pain medication, and all with regular guidance from physicians and physical therapists. And then those groups were compared to patients who did get TKR. The results of high quality non-surgical care were definitely better than nothing, literally, but nowhere near as good as the TKR results.
- Louw A, Diener I, Fernández-de-Las-Peñas C, Puentedura EJ. Sham Surgery in Orthopedics: A Systematic Review of the Literature. Pain Med. 2016 Jul. PubMed 27402957 ❐ PainSci Bibliography 53458 ❐
A review of a half dozen high quality tests of four popular orthopedic (“carpentry”) surgeries, all showing a lack of efficacy compared to placebos. This review is an excellent academic citation to support the claim that sham surgery has shown to be just as effective as actual surgery in reducing pain and disability. It’s also an eyebrow-raiser that Louw et al. could find only six good (controlled) trials of orthopedic surgeries, and all of them were bad news.
- Thorlund JB, Juhl CB, Roos EM, Lohmander LS. Arthroscopic surgery for degenerative knee: systematic review and meta-analysis of benefits and harms. BMJ. 2015;350:h2747. PubMed 26080045 ❐ PainSci Bibliography 53297 ❐
A review of nine studies presenting strong collective evidence that meniscectomy is a futile surgery for most patients, and with significant risk of harms to boot. For a good plain language overview of this topic, see Kolata.
- Siemieniuk RAC, Harris IA, Agoritsas T, et al. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. BMJ. 2017 May;357:j1982. PubMed 28490431 ❐ PainSci Bibliography 52778 ❐
These guidelines “make a strong recommendation against the use of arthroscopy in nearly all patients with degenerative knee disease … ” regardless of “imaging evidence of osteoarthritis, mechanical symptoms, or sudden symptom onset.” The authors believe this is the last word on the subject: “further research is unlikely to alter this recommendation.”
- Blogs.BMJ.com [Internet]. Jevne J. The sexy scalpel: unnecessary shoulder surgery on the rise; 2015 Jan 27 [cited 19 Feb 20]. PainSci Bibliography 53852 ❐
An excellent short opinion piece by Jørgen Jevne in the British Medical Journal about unnecessary shoulder surgeries, with broad applicability to other orthopedic surgeries.
- Beard DJ, Davies LJ, Cook JA, et al. The clinical and cost-effectiveness of total versus partial knee replacement in patients with medial compartment osteoarthritis (TOPKAT): 5-year outcomes of a randomised controlled trial. Lancet. 2019 08;394(10200):746–756. PubMed 31326135 ❐ PainSci Bibliography 51798 ❐
- Satisfaction measures are basically formalized anecdotal evidence, a popularity contest for treatments. It is practically the opposite of rigorous evidence. Human beings are routinely “satisfied” with treatments for a thousand reasons other than actual treatment efficacy, and have proven this again and again throughout medical history with astonishing examples of enthusiastically endorsing treatments that were actually hurting them, even killing them. See Popular but Weird & Dangerous Cures.
- Kahlenberg CA, Nwachukwu BU, McLawhorn AS, et al. Patient Satisfaction After Total Knee Replacement: A Systematic Review. HSS J. 2018 Jul;14(2):192–201. PubMed 29983663 ❐ PainSci Bibliography 52400 ❐
- Harris I. Surgery: The ultimate placebo. NewSouth Publishing; 2016.
This excellent book by an orthopedic surgeon explores the shameful history of untested surgeries in considerable detail. It’s fascinating and mostly easy enough reading even for patients.
- Wartolowska K, Judge A, Hopewell S, et al. Use of placebo controls in the evaluation of surgery: systematic review. BMJ. 2014 May 21;348:g3253. PubMed 24850821 ❐ PainSci Bibliography 53841 ❐ From the abstract: “Placebo controlled trial is a powerful, feasible way of showing the efficacy of surgical procedures. The risks of adverse effects associated with the placebo are small. In half of the studies, the results provide evidence against continued use of the investigated surgical procedures. Without well designed placebo controlled trials of surgery, ineffective treatment may continue unchallenged.”
- Rice DA, Kluger MT, McNair PJ, et al. Persistent postoperative pain after total knee arthroplasty: a prospective cohort study of potential risk factors. Br J Anaesth. 2018 Oct;121(4):804–812. PubMed 30236242 ❐
- Sorel JC, Veltman ES, Honig A, Poolman RW. The influence of preoperative psychological distress on pain and function after total knee arthroplasty: a systematic review and meta-analysis. Bone Joint J. 2019 01;101-B(1):7–14. PubMed 30601044 ❐ “Preoperative pain catastrophizing, mental distress, symptoms of anxiety and/or depression, and somatoform disorders appear to adversely affect pain and function after TKA.”
- Hamilton DF, Shim J, Howie CR, Macfarlane GJ. Patients follow three distinct outcome trajectories following total knee arthroplasty. Bone Joint J. 2021 Jun;103-B(6):1096–1102. PubMed 34058868 ❐
- Pain is a volatile, unpredictable experience that might get amplified by an overprotective brain. If the brain produces all pain — and technically it does, just like everything else we experience — maybe that means we can think pain away? Probably not with pure willpower or an attitude adjustment. But perhaps we can influence pain, indirectly, if we understand it — a few Jedi pain tricks. This isn’t about treating the root causes of pain, but the potential to tinker with the perception of it. Pain is fundamentally an alarm, and maybe we can convince our brains that it doesn’t need to be so loud, with methods like increasing confidence through education about pathology and pain itself (“Explain Pain”), avoiding nocebo, limiting “pain talk,” and many more. These are not easy or proven paths to pain relief, but all of them have some potential. See Mind Over Pain: Pain can be profoundly warped by the brain, but does that mean we can think the pain away?