The Causes of Runner's Knee Are Rarely Obvious
The science shows that you usually can’t blame IT band pain or patellofemoral pain on the structural quirks that seem like “obvious” problems
I love science that surprises. And even though I should know better by now, I’m still surprised by all the evidence that biomechanical issues aren’t nearly as much of a problem as it seems like they should be.
In 2004, a research group at the University of Connecticut let by Michelle Devan decided to try to figure out the effect of “structural abnormalities” on repetitive strain injuries of knee like iliotibial band syndrome (ITBS) and patellofemoral syndrome (PFPS).1 In particular, they wanted to study women.2
So, they did one of my favourite kinds of studies: they measured a bunch of stuff that every therapist in world “knows” is a risk factor for various knee problems, the usual structural suspects. In fifty young women athletes, they checked:
- the tightness of iliotibial bands
- the angles of knee joints
- the strength of their hamstrings and quadriceps
And then they waited to see who got what kinds of knee injuries over the course of the season.
Most health care professionals would fully expect the women with tight iliotibial bands to get more ITB syndrome, and the ones with some wacky knee angles to get patellofemoral pain syndrome.
But that’s not what happened!
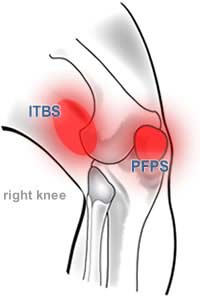
IT band pain & patellofemoral pain are the two common types of runner’s knee, both routinely blamed on bad running form or biomechanical issues.
The surprising results for IT band syndrome
Several of these young women got iliotibial band syndrome that season, and one even got it in both knees. But these experts determined that not one of them had tight iliotibial bands! “All the athletes with iliotibial band friction syndrome had a negative bilateral Ober test.”
The Ober test is a test of IT band tightness, supposedly. Actually, it mostly detects hip muscle and joint capsule tightness.3 Regardless of why, these women didn’t have restricted hip movement, not one of them. That is some strongly counter-intuitive evidence! Which makes it hard to hang onto the nice, simple, dogmatic idea that tight ITBs cause ITB syndrome, eh? Or that IT band stretching will help.
And the same surprising results for patellofemoral pain
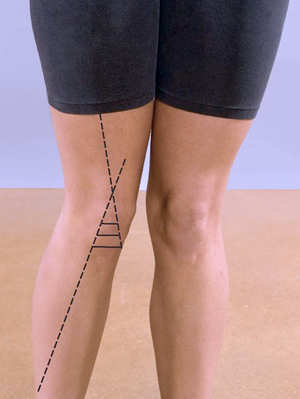
Wicked Q-angle!
It is more or less gospel that a steep, womanly Q-angle like this one is a risk factor for patellofemoral pain … but not one of the women who got symptoms had a big Q-angle.
Exactly the same kind of results were found with regards to knee angles and patellofemoral pain syndrome: no connection at all with the measurement that is supposedly bad news for knees.
The knee angle of concern is the “Q” angle — Q for quadriceps — and the conventional wisdom is that a steep, womanly Q-angle is a risk factor for PFPS. (Wide hips increase your Q-angle.) However, the researchers found that “none of the 9 athletes who sustained an overuse knee injury had an excessive Q-angle.” Not one.
Once again, wow. So much for the conventional wisdom.
Caveats about Devan et al.
So far I’ve just been reporting on a single study. It involved a fairly small number of young female athletes — hardly a good cross-section of the population. And did find some suggestive evidence of a connection between knee injuries and the relative strength of the hamstrings and quadriceps. And there is some other evidence of connections between these injuries and structural abnormalities. So let’s broaden the view …
The bigger picture and other research
There’s a strong theme in pain and injury research: most of the classic biomechanical factors are probably much less important than we used to think.4 For instance, a 2016 study followed 89 healthy runners over 12 weeks, monitoring for new injuries, and although 24 of them did get injured in those twelve weeks — which is a lot — they were not the runners with classic biomechanical scapegoats.5 It would seem that there’s no relationship between running injuries and the “mechanics” of running at all, or it’s too subtle to detect easily.
There’s a lot more evidence about this, some of it going one way,67 some the other.89 But it’s clear that knees aren’t just “mechanical,” and we can’t assume — or do therapy based on the assumption — that a tight IT band is necessarily a big deal, or that a steep Q-angle dooms runners to anterior knee pain. And even if you could be sure that they are important, half the time you can’t do anything about them anyway: just trying changing your Q-angle! You might as well try to change your height.
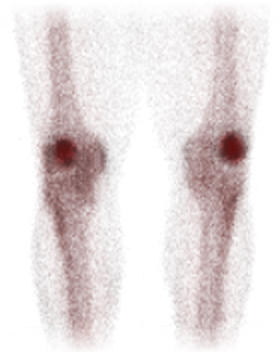
Bone scan of “hot,” metabolically active kneecaps — a good example of how injuries may be more about biochemistry than biomechanics.
So what then, if not biomechanics?
Injuries probably have much more to do with things like training volume and intensity,10 body weight,11 or dynamic factors like coordination and strength.12 Happily, these factors are also easier to work with than funky anatomy. And the stubbornness of injuries — which may be much of the problem — probably often has a lot to do with the biology of inflammation,1314 and neurological issues like sensitization.15
In other words, it’s messy: more biochemistry than biomechanics.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Related Reading
PainScience has extremely detailed guides to iliotibial band syndrome, patellofemoral syndrome, and shin splints, and many other related articles:
- Massage Therapy for Your Quads — Perfect Spot No. 8, another one for runners, the distal vastus lateralis of the quadriceps group
- Is Knee Pain More Common in Women? — The relationship between sex and knee pain, especially runner’s knee (IT band syndrome, patellofemoral pain)
- What Can a Runner With Knee Pain Do at the Gym? — Some training options and considerations for runners (and others) with overuse injuries of the knee
- Patellofemoral Pain Diagnosis with Bone Scan — If you have anterior knee pain, should you bother x-ray, MRI, CT scan, or bone scan?
- Does Cartilage Regeneration Work? — A review of knee cartilage “patching” with autologous chondrocyte implantation (ACI)
- Diagnosing Runner’s Knee — It usually starts with lateral knee pain during and after runs, but there are two major types
- Should You Get A Lube Job for Your Arthritic Knee? — Reviewing the science of injecting artificial synovial fluid, especially for patellofemoral pain
- Does Hip Strengthening Work for IT Band Syndrome? — The popular “weak hips” theory is itself weak
- Patellofemoral Pain & the Vastus Medialis Myth — Can just one quarter of the quadriceps be the key to anterior knee pain?
- Patellofemoral Tracking Syndrome — The beating heart of the conventional wisdom about patellofemoral pain is mostly nonsense
- Knee Debridement is a Completely Ineffective Procedure — Evidence that arthroscopic knee surgery for osteoarthritis is about as useful as a Nerf hammer
- Is Running on Pavement Risky? — Hard-surface running might be a risk factor for running injuries like patellofemoral pain, IT band syndrome, shin splints, and plantar fasciitis
- IT Band Stretching Does Not Work — Stretching the iliotibial band is a popular idea, but it’s very hard to do it right, and it’s probably not worth it
- Does the IT Band Move After All? — An ultrasound study says it does indeed slide across the lateral epicondyle, debunking my debunkery and prolonging the controversy
- Do IT Band Straps Work for Runner’s Knee? — The science of knee straps for iliotibial band syndrome (runner’s knee)
- IT Band Pain is Knee Pain, Not Hip Pain — Pain in the hip and thigh is something else, I promise
- Is IT Band Tendinitis Really a Tendinitis? — Research has clearly shown that the IT band itself is probably not the anatomy that gets inflamed … which has significant implications for treatment
What’s new in this article?
2016 — Added new images. Beefed up final section about non-biomechanical explanations. Several edits for clarity.
2016 — Long overdue revision, upgrades, updating. Added much more scientific context and several citations.
2007 — Publication.
Notes
- Devan MR, Pescatello LS, Faghri P, Anderson J. A Prospective Study of Overuse Knee Injuries Among Female Athletes With Muscle Imbalances and Structural Abnormalities. J Athl Train. 2004;39:263–267. PubMed 15496997 ❐ PainSci Bibliography 56601 ❐
- Some evidence suggests that women get more knee pain like this, but it’s controversial, and the authors wanted to try to clear it up a little — and try to find out why there is a difference, if there is a difference.
- Willett GM, Keim SA, Shostrom VK, Lomneth CS. An Anatomic Investigation of the Ober Test. Am J Sports Med. 2016 Mar;44(3):696–701. PubMed 26755689 ❐
This cadaver study confirmed something fairly obvious: the iliotibial band doesn’t restrict hip movement (adduction), but hip muscles do.
The IT band is the huge, complicated, tendon-like structure running down the side of the thigh from hip to knee.
The “Ober test” is a physical test to detect IT band tightness. I learned it in school. It’s been performed a bazillion times by health care pros helping athletes with knee rehab.
But this experiment showed that the Ober test does not actually detect IT band tightness per se, but rather the “tightness of structures proximal to the hip joint, such as the gluteus medius and minimus muscles and the hip joint capsule.”
In three years of training, the Ober test is really the only thing I learned about the IT band, and it’s probably all I ever would have known about it if I hadn’t gotten serious about my post-graduate education.
- Ingraham. Your Back Is Not Out of Alignment: Debunking the obsession with alignment, posture, and other biomechanical bogeymen as major causes of pain. PainScience.com. 21878 words. “Structuralism” is the excessive focus on crookedness and “mechanical” problems as causes of pain. It has been the dominant way of thinking about how pain works for decades, and yet it is a source of much bogus diagnosis. Structuralism has been criticized by several experts, and many studies confirmed there are no clear connections between biomechanical problems and pain. Many fit, symmetrical people have severe pain problems! And many crooked people have little pain. Certainly there are some structural factors in pain, but they are generally much less important than messy physiology, neurology, psychology. Structuralism remains dominant because it offers comforting, marketable simplicity. For instance, “alignment” is the dubious goal of many major therapy methods, especially chiropractic adjustment and Rolfing.
- Hespanhol Junior LC, De Carvalho ACA, Costa LOP, Lopes AD. Lower limb alignment characteristics are not associated with running injuries in runners: Prospective cohort study. Eur J Sport Sci. 2016 Jun:1–8. PubMed 27312709 ❐ This was the right kind of study for this, but perhaps a bit underpowered, and I wish I could see the same data for a couple hundred runners over six months. Nevertheless, you would expect runners with clearly identified biomechanical issues to be the ones who get injured, and yet “we did not find significant associations between lower limb length discrepancy, Q-angle, subtalar angle and plantar arch index and injury occurrence.”
- Lun V, Meeuwisse WH, Stergiou P, Stefanyshyn D. Relation between running injury and static lower limb alignment in recreational runners. Br J Sports Med. 2004 Oct;38(5):576–80. PubMed 15388542 ❐ PainSci Bibliography 53470 ❐ “In recreational runners, there is no evidence that static biomechanical alignment measurements of the lower limbs are related to lower limb injury except patellofemoral pain syndrome.”
- Salata MJ, Gibbs AE, Sekiya JK. A Systematic Review of Clinical Outcomes in Patients Undergoing Meniscectomy. Am J Sports Med. 2010 Jun;28(9):1907–16. PubMed 20587698 ❐
Meniscectomy is a common surgery (and a fairly useless one, see Thorlund). And almost everyone believes that loss of meniscal tissue — a loss of “padding” — leads to knee osteoarthritis. These researchers looked for evidence of it in research done up to 2010.
The data is a bit of a mess and they found a lot of lower level evidence of not much use (“garbage in”). However, they did detect some interesting patterns, a few factors that were clearly associated with either more or less osteoarthritis five or more years after surgery. For instance, they identified several factors that were not associated with more arthritis: gender, age, activity level, and poor mechanical alignment of the knee. Most of those are a bit surprising (all but gender). Surely poor alignment would spell trouble? That’s a common assumption! But apparently it doesn’t.
And since when does age not correlate with arthritis? And wouldn’t the association be even stronger after having some meniscal tissue trimmed away? How odd!
So what did make arthritis more likely? Fairly obvious things: weight, getting more meniscus removed, and crappy genes (inferred from osteoarthritis in other joints). The researchers pointed out that there are likely quite a few other variables that just aren’t represented in this data at all, like smoking and other injuries. “More research needed,” of course.
This is complicated review with many findings, but it included one conclusion that is particularly relevant here: poor mechanical alignment of the knee is not clearly a factor in the development of arthritis after a loss of meniscal tissue. Some studies show a connection, some do not! - Nakagawa TH, Moriya ÉTU, Maciel CD, Serrão AFV. Frontal plane biomechanics in males and females with and without patellofemoral pain. Med Sci Sports Exerc. 2012 Sep;44(9):1747–55. PubMed 22460471 ❐
Research on the biomechanics of patellofemoral pain syndrome (PFPS), and almost any knee issue, has focused on movement in the "sagittal plane" (looking at someone from the side). This study decided to investigate the "frontal plane" (looking at someone from the front) movements and how they may change in someone with PFPS during a stepping task.
People with PFPS tended to have increased knee abduction (knock knees) throughout the motion, and greater trunk, pelvis and hip motion during the step down. Females were also a little weaker in the hips than males.
Interestingly, this study seemed to show that PFPS does involve altered frontal plane biomechanics. No effect sizes were reported, however, so "how much different" remains a question, but the differences certainly exist. It's not surprising — if your knee hurts, you move differently!
- Noehren B, Shuping L, Jones A, et al. Somatosensory and Biomechanical Abnormalities in Females with Patellofemoral Pain. Clin J Pain. 2015 Nov. PubMed 26626291 ❐ “These results suggest that patellofemoral pain is characterized by an increase in both localized and centralized pain sensitivity which is related to movement mechanics. Thus, patellofemoral pain has both biomechanical, nociceptive components as well as inferred aspects of altered central sensitization.”
- van Gent RN, Siem D, van Middelkoop M, et al. Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review. Br J Sports Med. 2007 Aug;41(8):469–80; discussion 480. PubMed 17473005 ❐ PainSci Bibliography 54668 ❐
After reviewing 11 high quality studies (mostly prospective cohort studies) of how frequently long-distance runners injure themselves, this report found “a large range” of 19% to 79%, mostly in the knee (7-50%), followed by the lower leg and then foot. There was strong evidence for only two risk factors — a history of other injuries and lots of running every week for men (>64km/week) — and nothing else. There was only limited or conflicting evidence for practically every other imaginable risk factor: age, sex, leg length differences, alcohol consumption, or training factors like experience, shoe age, and running surfaces and many more.
Curiously, the authors also found “strong evidence that increased training distance per week was a protective factor, although only for knee injuries” but they caution that it’s not clear why, and “the relation between distance and injury may not be simple and there may be a fine balance between overuse and underconditioning among long distance runners.” Understatement.
- Messier SP, Legault C, Schoenlank CR, et al. Risk factors and mechanisms of knee injury in runners. Med Sci Sports Exerc. 2008 Nov;40(11):1873–9. PubMed 18845979 ❐
What are the risk factors for knee injury while running, if any? This small study looked at behavioural and physiological risk factors. 20 patients were questioned, analyzed for their gait, and knee joint loads were calculated. Hamstring and quadricep flexibility was assessed. Their conclusion: “The results of this study relate larger knee joint loads to poor hamstring flexibility, greater body weight, greater weekly mileage, and greater muscular strength. Most of these risk factors could potentially be modified to reduce joint loads to lower the risk of injury.”
- Ferber R, Hreljac A, Kendall KD. Suspected Mechanisms in the Cause of Overuse Running Injuries: A Clinical Review. Sports Health: A Multidisciplinary Approach. 2009;1(3):242–246. PubMed 23015879 ❐ PainSci Bibliography 55475 ❐
- Näslund J, Näslund UB, Odenbring S, Lundeberg T. Comparison of symptoms and clinical findings in subgroups of individuals with patellofemoral pain. Physiotherapy Theory and Practice. 2006 Jun;22(3):105–18. PubMed 16848349 ❐
Researchers bone scanned and x-rayed 80 patients diagnosed with PFPS and with many common similar diagnoses eliminated, a nice “pure” selection of unexplained knee pain patients. They divided them into three groups: 17 with pathology, 29 with “hot” kneecaps (metabolically active), and 29 without any findings (5 dropped out). All patients and 48 healthy subjects without any knee pain were then interviewed and examined by a surgeon and a physical therapist.
They could not diagnose the pathologies without the scans — all patients with pain tested about the same, and their symptoms were indistinguishable. Q-for-quadriceps angles were about 4˚ bigger in the afflicted, but the authors carefully explain that 4˚ too small to be reliably detected. The most interesting result of the study is that almost half the PFPS patients had kneecaps throbbing with metabolic activity — that’s a fairly strong pattern.
- Research has shown that immune cells unnecessarily “swarm” sterile injury sites, causing damage and pain — a biological glitch with profound implications about why some painful problems are so severe and stubborn. For more information, see A Painful Biological Glitch that Causes Pointless Inflammation: How an evolutionary wrong turn led to a biological glitch that condemned the animal kingdom — you included — to much louder, longer pain.
- Noehren et al., cited above, connected sensitization with biomechanics, but sensitization is a powerful phenomenon that undoubtedly can also occur regardless of any biomechanics. Pain itself can change how pain works, so that patients with pain actually become more sensitive and get more pain with less provocation. See Sensitization in Chronic Pain.