What Works for Chronic Pain?
A skeptical roundup of all the disappointingly small selection of effective chronic pain treatments (or the least bad ineffective ones)

Chronic pain is hard to treat — as profound an understatement as I can imagine. Treatments are notoriously underwhelming.1 “What works?” is one of the most unanswerable questions in all of medicine because “it depends,” always, on so many things. Pain is the king of It Depends. My confidence in what I think I know about pain has actually decreased over more than twenty years in this field.
Like cancer, pain is not one thing. It has literally thousands of possible causes. Nothing can possibly work for everyone or in every situation, and perversely even short-term success can lead to long-term failure.2 Pain is also so integrated into our “wiring” and identity that it is nearly impossible to suppress it without numbing the person (or critical subsystems) at the same time — which is why the only total analgesia is anaesthesia.3
Removing a definite cause of the pain is the ultimate treatment, like Androcles removing the thorn from a lion’s paw. Unfortunately, the metaphor of the thorn only fits some cases of chronic pain. It is startling and terrible how often no “thorn” can be found — and how many more can be found but not removed. And strange how many things look like thorns but aren’t actually the problem, and cause long wild goose chases. It’s a thorny problem!
What then for the rest of us?
The problem is immense. As of the early 21st Century, what are the best solutions for the most common problems? What is the most evidence-based and plausible? What actually works in at least some specific way, for well-defined groups of suffering people?
Anything? 😬
Yes, a few things do work well enough for that.
Since 2001, I have been debunking the pseudoscience and quackery that dominates the options for pain patients. I have been very “negative.” I believe that only the most marketable ideas dominate treatment and therapy for pain, with disastrous results.4 Since 2015, I have ironically been a chronic pain patient myself, seeking answers as desperately as any of my readers over the years.
This page is a long overdue optimistic collection of what definitely works for pain.5
It’s not a long enough list, obviously — especially because it excludes many experimental therapies and speculative strategies that are genuinely “worth a shot” due to their lower costs and risks and somewhat higher plausibility (see Pain & Injury Survival Tips). This article is not about what might work for a few people, it’s about what definitely works for quite a few people.
But never everyone, and always with caveats.
“Is that a fresh injury?” “Not really. But it’s tormenting me. Do you have any herbs capable of soothing the pain?” “That all depends on the class of pain,” the barber-surgeon said, smiling slightly. “And on its causes.”
The Witcher (Baptism of Fire), Andrzej Sapkowski
It’s a myth that “nothing works” — despite the difficulties, relieving pain is probably easier than coping with it
The idea that nothing works for pain seems extreme, but some professionals seem to have embraced it so completely that they have “given up” on treating pain, and shifted the focus to helping people with the fallout from pain: disability and suffering. The hope is that this is easier than actually treating pain.
Is it really wiser to try to treat disability and suffering rather than pain? Does it help people more? It sounds crazy to many patients, but is it actually just pragmatic, the “art of the possible”?
Saragiotto et al. pooled a lot of data and reported that pain is actually the outcome most affected by treatment attempts.6 Relieving disability and suffering is not obviously easier, and in fact it is probably harder — especially if pain remains!
The evidence suggests the obvious: relieving pain is the shortest path to relieving disability and suffering. That doesn’t mean it’s easy, and it doesn’t mean it isn’t also worth trying to relieve disability and suffering (and good luck trying to treat one without the other in any case, which would be like trying to flip one side of a coin). But pain relief should still be the focus, if for no other reason than it’s what patients want, and that matters (a lot). Giving the goal of pain relief short shrift can seriously piss patients off.7
Modern thorn removal: not “what works” exactly, but the greatest source of hope
That is, the power to identify and remove obscure causes of persistent pain — “thorns” — that we couldn’t find and remove before.
Nothing beats actually identifying a treatable problem that is the unambiguous cause of the pain. My favourite simple example is my friend with intractable back pain who was finally cured by the removal of a small tumour from a nerve root — after years of wrong theories, failed therapy, and escalating misery. One day his nightmare was just over, because the tumour was identified by the right expert looking in the right place in the right way (the right kind of MRI).
“Well, there’s your problem.”
This is the single best thing that modern medicine has to offer to anyone with unexplained chronic pain: a deep catalogue of hard-to-diagnose pathologies that cause pain, and the power to actually diagnose them (despite the difficulties). Not all such things can be treated, of course, but many can. The search for such a diagnosis remains the single best hope for many chronic pain patients. The failure to find a thorn — a persistent source of nociception (noxious stimuli) — even after many years, does not mean it isn’t there.
This isn’t a “treatment” per se, and it barely even counts as a strategy. You can’t even go to one doctor to hunt a tricky diagnosis, because there is no such thing as a specialist in all possible causes of pain. And medicine clearly still has more to learn. But! There is much more relevant knowledge out there today than there was a hundred or fifty or even twenty years ago. This is a legitimate cause for hope, the single best good news I can think of.
To help you get started on the search, I have compiled a fairly large list of diverse examples of surprising causes of pain.
Now for some more specific things that work…
- Opioids work (for some things, and with major risks)
- Over-the-counter analgesics work (not amazingly well, but reliably for a lot of things)
- Counterstimulation works (a little bit for a lot of people)
- Icing and heating work (not dramatically, but accessibly and comfortingly in many painful situations)
- Exercise and fitness work (if you don’t overdo it, and for some people it’s tragically easy to overdo it)
- Progressive loading works (where the problem is tissue overload)
- Drugs for neuropathy work (for a very lucky few)
- Neurostimulation with implants works, especially spinal cord stimulation (for those that qualify)
- Actually using best practices in musculoskeletal medicine works (for pretty much everyone, but also no one in particular)
- Treating insomnia works (for some people with insomnia)
- “Prehab” works (for preventing pain after surgery … or before accidents)
- Pain relief in the future
- Notable exclusions
Opioids work (for some things, and with major risks)

Ripening seed head of an opium poppy.
Opioids are the “nuclear option” in pharmacological analgesia — and perhaps the ultimate perfect example of something that works especially well in a specific context only. Most notably, they are ideal for dying people, because their grim side effects cannot menace a person who won’t exist in a few weeks or months. The existence of this option is one of the least appreciated greatest hits of modern medicine, arguably as big a deal as anaesthesia, vaccination, antibiotics, and so on. For the dying especially, opioids are a really big deal.
For everyone else? It’s more complicated and fiercely controversial, but opioids are also effective for many not-dying-yet chronic pain patients, for whom the risks are often very much the lesser of evils. The politicized and simplistic demonization of opioids — always a problem, but particularly disastrous right now in the middle of the Opioid Crisis/War — has disastrously limited access for many patients who truly can benefit from them. It has also stigmatized them, such that non-addicts who actually need the drugs routinely have to fight being treated like “drug-seekers” — which is often almost synonymous with being treated like criminals.
Obviously there’s a ton of bad news about opioids — not just the addiction problem, but the disturbing truth that they aren’t as potent as we’d like to think. They can be surprisingly ineffective for some people (genetics!) and for many kinds of chronic pain.
Over-the-counter analgesics work (not amazingly well, but reliably for a lot of things)
For every chronic pain patient who sneers at this option — and they do sneer! — there are two more who can’t imagine life without it. For instance, my own father has had impressively good results treating rheumatoid arthritis with naproxen (though not, of course, without side effects). The OTC pain-killers absolutely can work quite well for many conditions — and in some cases they are even amazingly safe (most notably acetaminophen within recommended dosages).
The over-the-counter analgesics mostly work by inhibiting various aspects of inflammatory signalling, in contrast to the narcotics which alter perception of pain regardless of how it’s being produced. So they can only do so much… but they definitely do something.
Menstrual cramping is one of worst pain plagues suffered by humans — and it can often be treated surprisingly effectively by a specific type of pain-killer, the non-steroidal anti-inflammatory drugs (like ibuprofen and aspirin).9 It’s a great example of something truly effective for a very specific context, but also an extremely common one. This is not to say that it always helps, but it’s a revelation for many women to learn that the NSAIDs specifically will often succeed where other common pain killers fail.
Another modern standout is topical diclofenac (Voltaren), one of the NSAIDs. Absorbing diclofenac through the GI tract is madness, rife with serious side effects. But in much smaller doses through the skin, right where it’s needed? •chef’s kiss• It is a truly good option for many, many kinds of pain.
Counterstimulation works (a little bit for a lot of people)
Counterstimulation is a basic neurological mechanism for minor temporary pain relief, a sensory “distraction” from pain. It’s not a potent thing, but it is a real thing, and it is probably responsible for the modest efficacy of many, many pain treatments that supposedly work some other way, but actually work this way.
You could call it another tool for the pain treatment toolbox, but it’s not an impressive tool — maybe just like a small screwdriver or a tack hammer.
It’s also why many kinds of chronic pain can and probably should be routinely treated with all manner of minor sensory pleasures and self-grooming: routinely, cheaply, and slightly fighting pain with other sensations, from the “spicyness” of a hot lotion, to the luxury of hot tub jets, to squirming around on a foam roller.
Like the OTC pain killers, counterstimulation is rarely going to work any miracles — but it will always be at least a little bit useful for many people.
It is probably the reason that massage and other manual (hands-on) therapies are perennially popular — which is both good news and bad. The good news is that it’s part of a legitimate explanation for why we like those treatments. The bad news is that it props up many bogus narratives about how they work, which in turn fuels a staggering amount of false hope. I explain this in more detail here:
Icing and heating work (not dramatically, but accessibly and comfortingly in many painful situations)
Icing and heating almost did not make the cut, because their powers are quite limited and perhaps they are just another source of counterstimulation (see previous section), and am I going to include every popular source of counterstimulation? But I think icing and heating stand out from that crowd for two reasons:
- Familiarity and accessibility. Nearly everyone has cheap, convenient access to these modalities.
- Their familiarity is psychologically significant. Both ice and heat have a comfort aspect that is probably critical for generating contextual (“placebo”) effects that drive up their value. The comfort factor is particularly huge for heat.
- Icing has some minor but real physiological effects that go beyond the “sensory hack” of counterstimulation. First, nerves can actually get numbed, their function genuinely suppressed, analgesia temporarily achieved. Second, ice may suppress the activity of receptors in the heat-detecting TRP family; this is definitely why ice is a genuinely potent pain-killer for burns, but TRP receptors are also triggered by inflammation (which isn’t a burn, but feels burn-like, and that’s not a coincidence).
So while there’s no major analgesia here, ice and heat do seem a little more truly useful than your garden variety source of counterstimulation.
I had a personal experience that convinced me that ice matters, a flare-up of calcific tendinitis of the shoulder that was by far the worst pain I have ever endured — like a rotting tooth that kept me awake and nauseous for days. In that situation, ice felt like a precious resource. (And heat was unthinkable, like the idea of putting a hot water bottle on a fresh burn.) I never thought I was actually fixing anything — the only goal was to blunt the pain, but that it did, and I would have been even more miserable without it. If anyone had tried to tell me in the middle of that experience that ice was useless for pain, I would have wanted to slap that naysayer.
Without that experience, I probably wouldn’t have included ice here. As it is, I cannot exclude it in good conscience.
People just cannot resist suggesting their favourite remedies to people who say they are in pain. But nearly everything casually suggested is a clean miss for most patients with serious pain, if not all of them.
Exercise and fitness work (if you don’t overdo it, and for some people it’s tragically easy to overdo it)
It has been said that exercise is the closest thing there is to a miracle cure. There’s plenty of truth to that, It doesn’t mean that exercise is a pain treatment specifically, but it is relevant. What exactly makes exercise such a wonder drug? For those who can do it, exercise has many complex benefits that are both inherently analgesic10 and protective over the long term, a great investment in long-term “health insurance.”111213 It even seems to help injured brains.14
If you are persistent, and sensible about not overdoing it, exercise almost cannot go wrong.
The big caveat is that quite a few people with chronic pain are also exercise intolerant — their threshold for “overdoing” it is really low — and simply cannot exercise enough to reap the rewards. Fibromyalgia patients are highly variable in their response to exercise, ranging from “very helpful if cautious” to “backfires almost every time,” probably because they have a wide variety of underlying conditions driving similar-ish symptoms.
But for many, many people with chronic pain, exercise works because it is biologically “normalizing,” pushing complex systems to work the way they are supposed to work. Biology is all about clever homeostatic mechanisms that nudge tissue state back to average. Those systems all rely on negative feedback loops based on molecular signalling (hormonal, neurological, etc), and exercise produces a lot of raw “data” to feed into those loops. Exercise cannot normalize everything. But it does stimulate an incredible array of adaptive and homeostatic mechanisms — way more than any medicine, supplement, or superfood.
Increased fitness is probably the ultimate way to reduce systemic vulnerability to pain, mostly through the mechanism of reduced inflammation. Poor fitness correlates strongly with an array of disease risks which are mostly all about chronic, subtle systemic inflammation, and fitness is the antidote.
Progressive loading works (where the problem is tissue overload)
A lot of chronic pain is caused by failure of recovery from tissue overload — repetitive strain injury — usually because the source of tissue stress is never reduced enough. Basically, people just keep re-injuring themselves: poor “load management.”
The body can recover from almost anything if you give damaged tissue an adequate rest and then slowly give it more functional challenges, starting very easy and working your way back up (“progressive training”). Baby steps, wisely executed, rarely fail to take a person back to normal. When this strategy does fail, it’s usually because the problem wasn’t tissue overload to begin with … which does happen, because an underlying biological vulnerability can easily create the appearance of a conventional injury. This is a one of the all-time best examples of how nothing works for everyone: progressive rehab is a fantastic principle where applicable.
This is a basic principle of rehab that has no direct evidence, because the strategy is too complex to meaningfully test, but it is supported by powerful “circumstantial” evidence and high biological plausibility. In my opinion, it doesn’t get enough credit because of a strong culture of excessively aggressive rehab strategies that routinely doesn’t allow enough recovery time to be successful. When done methodically, and carefully avoiding overload, it’s highly effective. But there is no citation for that: it’s a modest and logical extrapolation from the extremely powerful evidence that exercise in just-right doses is a powerful adaptive stimulus.
Drugs for neuropathy work (for a very lucky few)
Neuropathy is a malfunction of the nervous system itself: pain caused by dysfunction of the pain system. Many drugs that tinker with neurological function, often suppressing it in some way, are helpful for some of these patients. However, it generally takes rather a lot of experimentation to find the right drug — something that works well enough, with tolerable side effects.
Arguably, we do not have effective enough drug therapy for neuropathy to put it on any list of “what works for pain,” and some of the drugs generally touted as efficacious for neuropathy probably don’t deserve their reputation. However, it’s equally clear that drug therapy does work well enough for some patients that the world would be a much more desperate place without it. It’s far from a silver bullet for neuropathy, but many people have been saved by just the right drug.
Neurostimulation with implants works, especially spinal cord stimulation (for those that qualify)
The modern era of electrical therapy began when deep brain stimulation was introduced in 1987, and it has been steadily improving since then, thanks to better surgical techniques and a greater understanding of the neurology of pain. In just the last decade, I think it has improved enough to qualify for this list.
There are many types of neurostimulation, and many of them are bogus. But I’m referring mainly to spinal cord stimulation (SCS). Peripheral nerve stimulation is much too mediocre, and brain stimulation — while extremely promising — is not quite ready for prime time. Even other kinds of spinal stimulators are ineffective, like spinal muscle stimulators.16 For now, the smart money is on SCS — although even that is hardly perfect.
Any invasive treatment has major risks, of course, and it’s usually only a wise choice for specific kinds of patient with particularly great need. But SCS can be almost miraculous for some patients. Interestingly, it’s largely based on the somewhat underwhelming principle of counterstimulation (discussed above) — but the “potency” appears to be amped up by stimulating the spinal cord directly.
Actually using best practices in musculoskeletal medicine works (for pretty much everyone, but also no one in particular)
Pain is too complex and multifactorial for one-size-fits-all solutions, which makes it very difficult to say “what works.” But if many factors contribute to pain, then many factors are probably involved in treatment, complex care for a complex problem: medicine that includes many best practices, wisely and skilfully applied.
And what does that look like, pray tell?
It’s not a mystery. A 2019 paper distilled several key best practices in musculoskeletal medicine from eleven recent, high quality, English clinical practice guidelines.17 See that footnote for the formal language. Here is a translation of those best practices into plain English:
- Care should be customized to the patient’s situation — and the only way you can do that is to know the patient’s situation. Which means a lot of good listening and making decisions together about what makes sense. (Patient-centered care.)
- How the patient feels is one of the most important parts of the clinical equation: their emotional state and the things going on in their life that are most likely to affect pain and be affected by it. Pain is emotional; psychology matters.
- Put a strong focus on helping people continue or return to work — and or sport/play if it’s unusually important to them.
- Pain involves so many potentially serious causes that it’s really important to be aware of the red flags, and to screen for them.
- MRI and X-ray (radiological scanning) is a bad idea in the early stages of assessment unless it has a good chance of changing care, or of course if a serious pathology is suspected (because of the red flags already mentioned).
- Ideal care really needs to be a physical exam. Actual touch required! Neurological screening tests are one of the best examples of the kind of hands-on examination that is often needed.
- Progress should be measured and logged as objectively as possible.
- Patients need educational materials. Information is empowering, and empowerment is particularly valuable for pain. (Pro tip: Send them to PainScience.com!)
- An emphasis on fitness and exercise (basically reflecting the fact that “exercise is the closest thing there is to a miracle cure,” see above).
- Surgical options should usually be deferred until after more cautious options have been tried.
And saving the best for last, the one that is the most challenging to so many professionals, and so different from what most patients actually get:
- Manual therapy — mostly massage therapy and spinal “adjustment” — can be a part of the equation, but it shouldn’t be the centrepiece, because so many manual therapy techniques either have never been tested, or have been and failed (no clinically significant specific effects). They should be treated like the experimental medicine that they are.18
This isn’t a perfect list, of course (and exactly how it falls short is a much longer conversation). But it certainly does describe a kind of care that is miles better than what most patients are actually getting. Many of these best practices are bizarrely neglected by — or even at odds with — the common beliefs and practices of healthcare professionals who should know better.19
Much of the list is just the biopsychosocial model of care, which has always basically boiled down to being more humble and engaged with patients20 — but it’s unclear and difficult, and professionals tend to talk the BPS talk a lot more than they walk the BPS walk… especially in musculoskeletal medicine,21 where structuralism seduces so many professionals away from the nuances of BPS.
If every patient with a stubborn painful problem got care that ticked all of these boxes, I think a lot more of those problems would get meaningfully helped. There’s no citation for that, of course: it’s impossible to standardize complex care (almost a paradox, really). But each individual component is to some extent based on good science, and I think they undoubtedly add up to something that “works.”
Treating insomnia works (for some people with insomnia)
Sleep deprivation plays a major role in some cases of chronic pain, and makes a bad situation worse for many others. There are a lot of systemic stresses that contribute to vulnerability to pain, but sleep deprivation is one of the most obvious common ones that can often be solved or significantly mitigated. Although insomnia has as many causes as chronic pain, we understand many of them quite well, and several types can now be easily treated or even outright cured.
Even total recovery from insomnia isn’t going to actually cure much chronic pain — but it’s indisputably an upgrade, a complex and indirect but reliable way to reduce the impact of chronic pain for some patients.
“Prehab” works (for preventing pain after surgery … or before accidents)
In addition to “rehab” after surgery, one should prepare by being as fit as possible before surgery: “prehab,” AKA preoperative physical therapy. Prehab is one of the best evidence-based things anyone can do to prevent pain.
And prehab for surgery is also prehab for injury. So that’s a nice perk.

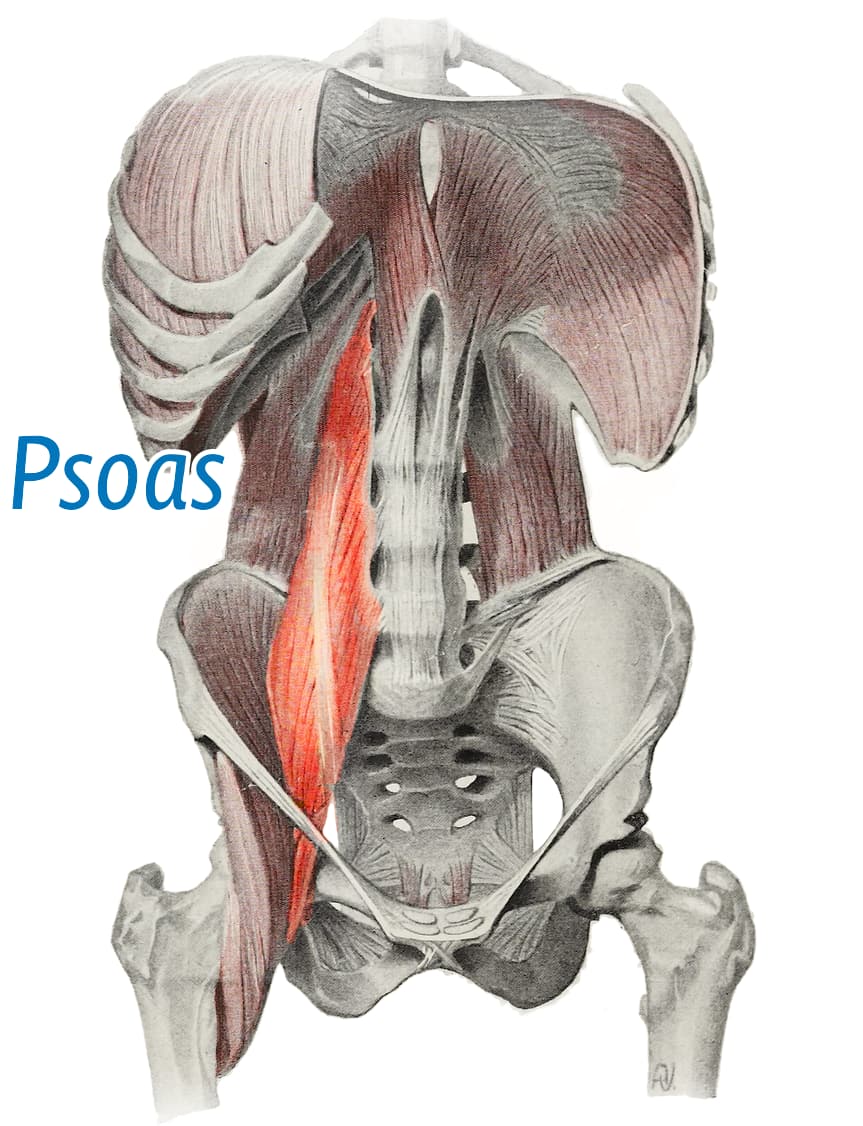
Your core muscles are not just for crunches — their size predicts how well you bounce back from spine surgery. Yet another reason to stay strong.
A 2024 study showed that stronger people got much better results from surgery to correct scoliosis.22 Specifically Hirase et al. compared recovery in patients with more or less cross-sectional area of an obscure but large spinal muscle, the psoas (pronounced “so ass”).23
How much better was recovery for patients with supersized psoases? Pso much!
- about one third less time in hospital (and prehab had more effect on this than any other factor)
- almost doubled walking distance in the three days after surgery
- almost half the adverse events
That’s good stuff! And there are quite a few other studies of prehab with similarly impressive results. It is not a subtle effect!
Importantly, this probably isn’t a core strength thing, nor is about the “power” and mystique of the psoas — it’s just that you find big psoas muscles in people who are more fit in general.24
•
Pain relief in the future
There are three areas of major promise in the future of exciting, high-tech and advanced pain medicine:
- Deep brain stimulation. We already have spinal cord stimulation and some brain stimulation that is at least somewhat effective (see above). But the future is bright for more advanced neurostimulation, as we push further into the mysteries of the brain, stimulating neural pathways with much greater precision. Consider a 2021 study that demonstrated substantial pain relief with a mini-computer implanted in rat brains, modulating pain in real time, as needed.25 Amazing, and quite likely to help people in time. (And there’s also a substantial what-could-possibly-go-wrong factor as well.2627)
- Regenerative medicine. Genuine regenerative medicine is legitimately promising, and someday it may effectively cure many painful pathologies and injuries that we can’t do anything about today — cure in the same way that vitamin C cures scurvy, pulling pain out by the roots on a large scale for the first time in history. But for now it remains primitive… and a magnet for profiteering charlatans. The proliferation of bogus “stem cell clinics” is particularly appalling.
A new generation of pain-killers. Like fusion power, safe and strong pain-killers have been thirty years away for decades. But they probably will eventually get here. Consider VX-548, likely being brought to market in 2025, which works roughly as well as opioids (hydrocodone) without being addictive — and that is in itself quite an accomplishment, and genuinely cool. But it’s also no better than opioids, and only at high doses and it is definitely going to be more expensive, and therefore less accessible, and therefore not exactly a game-changer either. See Plug your sodium channels with VX-548. Despite the slow progress, I think we will someday have some new drugs are very helpful to some patients.
But the greatest potential in health care is always with the boring basics, and that applies as much to pain as any other medical issue. The “root causes” of most chronic pain go deep: poor health and inadequate care, which are in turn driven by poverty, social injustice, and dysfunctional institutions and governance. Improving these things is not a “pain treatment,” per se, but it’s as important to pain as sanitation is to public health. Systemic changes have by far the greatest potential to relieve pain… and, of course, they are also the least likely to actually happen. Because, as basic as these things are, they can only be produced by a more advanced and better-organized society: progress, the hardest thing there is.
Notable exclusions
Some things will get added to the list above in time. But not many, and not these, not for now: several exclusions that many people will ask about if I don’t mention them.
- Acupuncture has been studied to death, with consistently negative or damned-with-faint-praise results in every higher quality study. Even if I conceded that it has some efficacy (which I do not), it would be no better than conventional pain-killing drugs…and dramatically more expensive, and not entirely safe.
- Massage therapy has great untapped potential, but disappointing preliminary results for major specific indications like back pain and trigger points, and such a complex mess of confounding factors and mythology that it makes no sense to endorse it as a generally efficacious therapy.
- Chiropractic generally, and spinal manipulative therapy specifically, for so many reasons.
- No, sorry, definitely not cannabis: the evidence on THC for pain is thoroughly discouraging, and the CBD science barely exists at all.
- Psychotherapy in generally, represented mainly by cognitive behavioural therapy, is completely damned with faint praise. Idealized CBT might be effective in theory, but in practice people cannot get that.
- Lifestyle medicine, including and especially treatment for stress and anxiety, has the potential to reduce systemic vulnerability to many mechanisms of chronic pain. It has extremely high general plausibility, but it is extremely messy and virtually untestable … and thus too experimental. I extracted one critical element for the list above: exercise and fitness.
- Meditation, mindfulness, and yoga for pain are just “meh” — fine for a few people who like their “vibe,” tedious and disappointing for many more.
- Low-dose naltrexone is very interesting, certainly seems to work for some folks with chronic widespread pain, but not exactly a solid evidence-based option … yet.
- Regeneration therapies in general, but most notably autologous chondrocyte implantation and platelet-rich plasma. Regeneration therapies may get there someday, but these are weak early options. Regenerative medicine just hasn’t panned out … yet.
- Several more popular and therapies that seem promising but are particularly disappointing:
There are, of course, many many more that I could mention. But these are the ones that people are most likely to ask about if I don’t mention them.
Is there something you think should have made the cut, but you don’t see anywhere on this page? Feel free to ask.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
Ten updates have been logged for this article since publication (2021). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.
I log any change to articles that might be of interest to a keen reader. Complete update logging of all noteworthy improvements to all articles started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
Oct 29, 2025 — Minor improvements to the spinal cord stimulation section.
2025 — Improved the new section “‘Prehab’ works (for preventing pain after surgery),” including new information, images, and perspective.
2025 — Added a new section: “‘Prehab’ works (for preventing pain after surgery).”
2024 — Added “a new generation of pain-killers” as a third category of legitimately promising “advanced” approaches to pain.
2023 — Science update. Beefed up the exercise section with four fresh good-news studies.
2022 — Added section: “Icing and heating work (not dramatically, but accessibly and comfortingly in many painful situations).”
2022 — New sidebar: “The price of honesty and humility.”
2022 — Added some comic relief: the dead-or-pretending meme, the you-keep-using-that-word meme, plus a sidebar, “What people think I do for a living….” (which is fun, but also goes a little deeper).
2022 — New section: “Actually using best practices in musculoskeletal medicine,” plus a bunch of editing throughout the article. Almost ready for prime time!
2021 — New section: “Pain relief in the future.”
2021 — Publication.
Notes
Pain medicine has been slowly choking to death on “evidence” that shows minor transient benefits to virtually all treatments for most patients. For instance, it’s a given these days that most manual and passive therapies can be shown to have statistically significant but clinically trivial effects, modest and temporary at best.
In most cases, even that much is probably just a research artifact, wishful thinking powered by methodological and statistical jiggery pokery (e.g. p-hacking).
In the remainder, it’s probably attributable to non-specific effects that weren’t adequately controlled for.
And so we have endless “promising” results that rarely, if ever, amount to anything more — if they are even legit in the first place, which they often aren’t, because there are so many ways to warp a little study so that it confirms a bias (see Cuijpers). Literally no manual or passive therapy — like massage, spinal traction, ultrasound, or cartilage debridement — has ever been shown to have an unambiguously impressive effect on recovery from pain/injury. See Cook.
Even some of the most highly regarded champions of rehab fail to stand up to scrutiny. I spent an hour re-reviewing the research on heel drops for Achilles tendinitis in the hopes of including it in this article as a fine example of something that works, because it is so widely embraced as an effective intervention. But it is actually not that impressive. It does not clearly “work.”
And so it goes, all the way down virtually the entire mighty list of options for virtually everything that hurts.
- I am referring specifically to the paradox of downregulation of opiate receptors. Any artificial stimulation of the firing of inhibitory nerve pathways — one of the most potent ways to relieve pain — also desensitizes those pathways, crippling them for your future self.
The pain system is a necessary part of us, like a vital organ that’s everywhere. It’s one of the main reasons we have a nervous system in the first place. Half our biochemistry is devoted to dealing with threats, and most components have other critical jobs. Anything potent enough to really shut pain up is also going to shut you down: anaesthesia, opioids, steroids, tetrahydrocannabinol, Botox … everything that is to some degree useful also tends to have a substantial price tag, usually the loss of some kind of function. And so pain treatment is always going to be some kind of compromise. When the reward is total pain relief, the cost is the temporary but total obliteration of consciousness by anaesthesia.
- It’s just impossible to overstate how much marketing, hype, and clickbait have defined pain and injury treatment. This has been happening since the patent medicine era, more and worse with every decade. No bad idea ever dies — not if you can still sell it! The grift goes on and on. For a more detailed rant on this theme, see You’ve only heard of marketable pain treatments.
This article was about twenty years in the making. As badly overdue as it is, I don’t think I could have written it much sooner in my career than this. I just wasn’t ready! I didn’t really have good answers to the question “What works for pain?” I had to figure out how to write it without good answers. I had to cook up several genuinely nice things to say about a field that is a bit of a dumpster fire of quackery, bullshit, fraud, wishful thinking, self-serving delusions, and even extreme ignorance and irrationality.
So it was a tall order, and quite a departure for me.
I have been delivering the bad news for a long time. I have been infamously “negative.” PainScience.com had a strong focus on debunking in the early days. The funk of curmudgeonry was overwhelming for many readers. Why so negative? The annoying reality is that musculoskeletal and pain medicine are surprisingly primitive, and the huge gaps in our knowledge are mostly filled with pseudoscience, much of which actually passes for “mainstream.” There’s an army of well-intentioned hacks and quacks out there selling their wares to chronic pain patients, eager to tell them exactly what’s wrong with them and how to fix it.
And so I have told readers what’s not worth their time, their money, or the risk to their health. And I like to think I have saved tens of thousand of people from unnecessary expenses, false hope, and side effects.
But clearly I have been a disappointment to many more, millions of website visitors over the years who couldn’t get past being offended by the mean things I say about stretching, acupuncture, platelet-rich plasma, or therapy taping. I could have sold so many more books if I just hadn’t been such a buzz-killing skeptic.
Finally putting out an article about what does work is not going to turn this grumpy ship around. My good news is too heavily qualified, too obviously diplomatic. But it is sincere. This is what I actually believe. For whatever it’s worth, this is the best news that I can ethically deliver.
- Saragiotto BT, Maher CG, Traeger AC, Li Q, McAuley JH. Dispelling the myth that chronic pain is unresponsive to treatment. Br J Sports Med. 2017 Jul;51(13):986–988. PubMed 27797740 ❐
“The view that pain is not the best measure of treatment success for chronic pain is not evidence-based. The assumption that behavioural or psychological therapies mainly reduce disability but not pain is not consistent with the data from Cochrane reviews on chronic LBP. Pain intensity should be measured in chronic pain research and clinical practice. Considering pain intensity to be the wrong metric for chronic pain hampers treatment selection and does our patients a great disservice.”
Consider this quote:
“Our duty to patients with chronic pain is not to reduce pain intensity, but to improve their quality of life.”
That sentiment makes a poor impression on patients. One of my most popular tweets expressed a little outrage about it:
“Putting my patient hat on here. Speaking as a chronic pain patient, not even trying to look at this from a clinical perspective… I want the intensity of my pain reduced. Just that. Pretty 🤬 sure THAT would ‘improve quality of life.’”
- Bastian H. "They would say that, wouldn't they?" A reader's guide to author and sponsor biases in clinical research. J R Soc Med. 2006 Dec;99(12):611–4. PubMed 17139062 ❐ PainSci Bibliography 51373 ❐
The full quote:
“A promising treatment is often in fact merely the larval stage of a disappointing one. At least a third of influential trials suggesting benefit may either ultimately be contradicted or turn out to have exaggerated effectiveness.”
- Menstrual cramping is triggered by prostaglandin, a signalling molecule produced by the womb during menstruation, and also an important part of inflammation. NSAIDs inhibit the production of prostaglandin, which suppresses inflammation … and menstrual cramps specifically and especially. It’s a very specific biochemical effect, making the NSAIDs truly effective muscle relaxants for this one specific kind of muscle cramping. Other over-the-counter pain-killers, most notably acetaminophen, do not have this effect.
- Weng Q, Goh SL, Wu J, et al. Comparative efficacy of exercise therapy and oral non-steroidal anti-inflammatory drugs and paracetamol for knee or hip osteoarthritis: a network meta-analysis of randomised controlled trials. Br J Sports Med. 2023 Jan;57(15):990–996. PubMed 36593092 ❐ PainSci Bibliography 51421 ❐
This enormous meta-analysis concludes that exercise is a modestly effective treatment for hip/knee arthritis in the short term:
Exercise has similar effects on pain and function to that of oral NSAIDs and paracetamol. Given its excellent safety profile, exercise should be given more prominence in clinical care, especially in older people with comorbidity or at higher risk of adverse events related to NSAIDs and paracetamol.
The data also shows diminishing returns over time, dwindling to a trivial benefit.
But this data shows that exercise is quite safe and somewhat helpful — and therefore also obviously not harmful.
Read more about this paper.
- Klasson CL, Sadhir S, Pontzer H. Daily physical activity is negatively associated with thyroid hormone levels, inflammation, and immune system markers among men and women in the NHANES dataset. PLoS One. 2022;17(7):e0270221. PubMed 35793317 ❐ PainSci Bibliography 51450 ❐
This is a good trial linking long-term daily physical activity to clear reductions in systemic inflammation (as measured by major biomarkers). They found “evidence for both systemic metabolic effects via thyroid hormones and in specific systems via reduced inflammation and immune cell counts.”
- Ahmadi MN, Clare PJ, Katzmarzyk PT, et al. Vigorous physical activity, incident heart disease, and cancer: how little is enough? Eur Heart J. 2022 Oct. PubMed 36302460 ❐
This is of those morbid mortality studies, a big one cross-referencing deaths with fitness gadget data for tens of thousands of people. People died less if they did frequent small doses of vigorous exercise — less than 2-minute sessions, and only one or two per day. Intense and regular, but just little blasts of action. The benefits became measurable at 15-minutes per week, and continued to improve up to a total of an hour per week (or 4 mini workouts per day).
Note that “all-cause mortality” definitely overlaps with the “reduced systemic inflammation” measured by Klasson et al. Taming inflammation was probably partly how mortality was reduced.
- Webber BJ, Piercy KL, Hyde ET, Whitfield GP. Association of Muscle-Strengthening and Aerobic Physical Activity With Mortality in US Adults Aged 65 Years or Older. JAMA Netw Open. 2022 Oct;5(10):e2236778. PubMed 36251297 ❐ PainSci Bibliography 51392 ❐
Webber et al. studied the effect on all-cause mortality of muscle strengthening specifically — an emphasis on wearing out muscles relatively quickly by lifting heavy things, as opposed to huffing and puffing aerobically. They identified a robust drop in mortality, about 20% lower in people who did 2–6 weekly sessions compared to none or just one.
- Leddy JJ, Haider MN, Ellis M, Willer BS. Exercise is Medicine for Concussion. Curr Sports Med Rep. 2018 Aug;17(8):262–270. PubMed 30095546 ❐ PainSci Bibliography 52267 ❐
This is a positive review of moderate exercise as “medicine” for brain injury, concluding that it probably normalizes concussed brains, even in cases of persistent post-concussion syndrome.
- I am highly critical of “corrective” exercise — the alleged use of specific, technical exercises to “fix” allegedly clinically significant weakness and asymmetries. See “The Corrective Exercise Trap”.
And I even have awkwardly mixed feelings about progressive training — we know that overloading is a risk factor for injury, especially spikes (see Soligard et al.), and so it just seems to make sense that “managing” load would be an important part of both prevention and recovery. And that may be true in some ways. But the evidence is mixed and conflicted. There is encouraging evidence, but also evidence that gives me reasonable doubts that carefully load managed exercise really “works” for many injuries (Hopewell et al. is a good example).
- Schwab F, Mekhail N, Patel KV, et al. Restorative Neurostimulation Therapy Compared to Optimal Medical Management: A Randomized Evaluation (RESTORE) for the Treatment of Chronic Mechanical Low Back Pain due to Multifidus Dysfunction. Pain Ther. 2025 Feb;14(1):401–423. PubMed 39812968 ❐ PainSci Bibliography 49289 ❐
This is a clinical trial of the ReActiv8 “neuromodulation” implant, which is related to the simple electrical stimulators you can buy at any drugstore, but surgically implanted. The principle of the device is implied by the name: it “re-activates” the deep multifidus muscle around your spine. ReActiv8 could be efficacious, but it was not convincingly shown by this very badly flawed trial — mostly just poorly controlled — despite the apparently positive results. It is of interest mainly as an unusually good example of a bad trial. Gilligan et al. was far better, but mostly negative.
Read more about this paper.
- Lin I, Wiles L, Waller R, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med. 2019. Here are the recommendations quoted verbatim:
- Care should be patient centred. This includes care that responds to the individual context of the patient, employees effective communication and uses shared decision-making processes.
- Screen patients to identify those with a higher likelihood of serious pathology/red flag conditions.
- Assess psychosocial factors.
- Radiological imaging is discouraged unless:
- Serious pathology is suspected.
- There has been an unsatisfactory response to conservative care or unexplained progression of signs and symptoms.
- It is likely to change management.
- Undertake a physical examination, which could include neurological screening tests, assessment of mobility and/or muscle strength.
- Patient progress should be evaluated including the use of outcome measures.
- Provide patients with education, information about their condition and management options.
- Provide management addressing physical activity and or exercise.
- Apply manual therapy only as an adjunct to other evidence based treatments.
- Unless specifically indicated (e.g. red flag condition), offer evidence-informed non-surgical care prior to surgery.
- Facilitate continuation or resumption of work.
“Manual therapy” refers mainly to massage, spinal manipulation, and many other methods of assessing and treating common musculoskeletal problems and injuries with hands and/or tools, from Rolfing to acupuncture to ultrasound. Most of this is done *to/for* patients, so it is also sometimes called *passive* therapy as opposed to *active* (mainly exercise therapy). It is largely the domain of massage therapists, chiropractors, and physical therapists, but also much smaller populations of osteopaths, acupuncturists, and a few doctors. Manual therapy is the jewel in the crown of alternative medicine, exemplifying the best it has to offer: the time, compassion, and touch that medicine often neglects. Done wisely, it can deliver great patient-centered care and valuable medical screening Unfortunately, even at its best, manual therapy is time-consuming therefore expensive and mostly inaccessible to people most affected by chronic pain due to poverty and systemic inequality. And it is *often* not at its best. Much of that expensive time is used poorly. Manual therapy also showcases some of the worst of alternative medicine; it is a pseudoscientific dumpster fire. Despite the great variety of technique, there are only a few major, simplistic themes. It is mostly fueled by faith that tissue can be fixed or improved by just the right kind of physical manipulation or force, and often a lot of force, such that the no-pain-no-gain hubris of several methods involves some risks … which cannot be justified by evidence. What little good research exists shows modest medical benefits at best, and the handful of journals dedicated to manual therapy are disdained by the scientifically literate. Instead of evidence and scientific plausibility, manual therapy is largely based instead on authority, tradition, and whatever sells. To a shocking degree, it is dominated by the branding and commercialization of simplistic ideas like “alignment” or “fascia release.” The field has a hall of shame the size of Grand Central Station, exhibiting some of the nastiest snake oils in history (e.g. infant chiropractic), as well as the silliest (vitalism is so influential in the world of manual therapy that it cannot be dismissed as a fringe belief). But even its more mainstream methods are something of an embarrassment: physical therapists are notorious for quackery that passes for good medicine, including many manual and similar therapies (probably most notably dry needling). And yet! There probably is a signal somewhere in all that noise. Rational manual therapists can ethically offer more plausible techniques, minimize the risks and costs, and create pleasant sensory and social experiences that are both inherently valuable *and* probably have some complex systemic benefits — such as a proven power to reduce anxiety/depression. The potential of touch, compassion, and novel sensations to inspire, encourage, comfort, reassure, and ease suffering and disability should not be underestimated. For more information, see Manual Therapy: What is it, and does it work? The science of "fixing" tissue with hands-on treatments like massage and spinal manipulation.
- For instance, the importance of psychosocial factors is either entirely neglected or hotly contested by many; or it is paid lip service but given short shrift in practice. There is an immense gap between theory and practice in musculoskeletal medicine, with vast numbers of professionals perpetually indulging in pet theories of pain and wildly overestimating the value of passive therapies — the power of gadgets, tools, and hands — while underestimating and neglecting everything else.
- Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977 Apr;196(4286):129–36. PubMed 847460 ❐
This paper is the origin of the now famous biopsychosocial model of healthcare, advocating for a kinder, more nuanced and artful medicine, as opposed to the rather cold, clinical, and technical profession it had become in the middle of the 20th Century thanks to its immense science-powered successes.
Engel argued that the dominant biomedical model inappropriately reduced too many complex health concerns to biology and pathology alone (reductionist), excessively separated body and mind (dualist), and left “no room within its framework for the social, psychological, and behavioral dimensions of illness.” In short, he believed medicine had become dehumanizing, excluding the patient and their “…attributes as a person, a human being.”
Engel proposed that the BPS model could provide a “…blueprint for research, a framework for teaching, and a design for action in the real world of health care.”
Ever since publication of this landmark paper, the BPS model has been extensively interpreted and misinterpreted, used and abused and co-opted and perverted. Cormack et al. describe many of the problems that emerged over the years, and I explored that topic in detail, see: BPS-ing badly! How the biopsychosocial model fails pain patients.
- Ben Cormack, Peter Stilwell, Sabrina Coninx, Jo Gibson. The biopsychosocial model is lost in translation: from misrepresentation to an enactive modernization. Physiotherapy Theory and Practice. 2022:1–16. PubMed 35645164 ❐ PainSci Bibliography 52047 ❐
- Hirase T, Lovecchio FC, Allen MRJ, et al. Preoperative Physical Therapy is Associated With Decreased Length of Stay and Improved Postoperative Mobility in Patients With Sarcopenia Undergoing Adult Spinal Deformity Surgery. Spine (Phila Pa 1976). 2024;50(3):172–178. PubMed 38809100 ❐
The psoas pair is a lot like the columns of muscles flanking the spine in the back, except that they are in the front, deep in the belly.
![Simple anatomical diagram in a vintage style, showing the abdomen with the viscera removed and the psoas muscle highlighted, originating on the sides of the lumbar vertebra and descending, prominently labelled “psoas.”]()
- There’s a surprising amount of silliness about the psoas in manual therapy. But even without a weird fetish for the psoas, many professionals will leap to the assumption that this study shows that it’s the psoas specifically and core strength that made the difference.Not pso fast! It’s more likely that this is about strength in general, thanks to the substantial metabolic benefits of having more muscle anywhere at all. People don’t get thick psoas muscles from just sitting around. If you’ve got big psoases (and you cannot lie) it’s probably because you’re all kinds of healthy, and it’s the fitness that matters.See a deep dive on how this works (members only), or just get a taste from one key citation.
- Zhang Q, Hu S, Talay R, et al. A prototype closed-loop brain-machine interface for the study and treatment of pain. Nat Biomed Eng. 2021 Jun. PubMed 34155354 ❐
This study advances the science of brain-machine interfaces with a test of an implanted computer chip in rat brains, designed to treat chronic pain. The chip reads the rat’s minds: it detects patterns of brain activity in the cingulate gyrus that are consistent with pain, and then stimulates part of the frontal lobe to mute pain: specifically, to “exert top-down nociceptive regulation.” Obviously this is very invasive, and even if it works there’s a risk of adaptation and dependence, and human applications are many years off.
Doing this for humans is probably still many years away. But if it works? It’s extremely precise, responding in real-time, only working when there’s pain to treat — completely unlike the continuous, always-zapping approach that has dominated the field so far.
And it really did work amazingly well. The treated rats withdrew from painful stimuli about 40% slower, and greatly preferred spending time in a chamber where the implant was functional to one where it wasn’t. These were strong results, and a very promising demonstration of the principle.
This kind of approach is likely to improve as we continue to improve brain-machine interface technology, and knowledge of brain circuity gets more precise.
See neurologist Dr. Steve Novella’s more detailed explanation of this experiment.
Science fiction is full of cautionary tales about a brain interface tech that is still decades away (if ever). Yes, you might get used as a battery by our robot overlords. Meanwhile, back in the early to mid 21st Century…
The obvious problem with a technique like this is that it’s about as invasive as invasive can get — it’s a brain implant. There are going to be complications.
Technological glitches aren’t out of the question either. This is not a simple device. “Have you tried rebooting it?” is not what patients want to hear when they call tech support for their brain implant.
Here’s a less obvious and more interesting concern: this could cause adaptation and dependence just like opioids. Any time you overstimulate an inhibitory neurological function, there’s a chance that it will get a bit numbed to the input… and no one wants a pain inhibition system that isn’t working at full power. Understatement.
We know this phenomenon extremely well from opioid dependence, but the inexorable logic of “downregulation” applies to anything that tinkers with nerves to kill pain. Pick a pathway that inhibits pain, any pathway, give it a boost with some kind of artificial stimulation, and gosh darn it if it doesn’t start downregulating and become less responsive to natural stimulation… et voila, you become either dependent on the artificial stimulation, or seriously sensitized without it.
But “it’s complicated,” of course. This will just have to be studied over time to find out if that happens.