BPS-ing badly! How the biopsychosocial model fails pain patients (Member Post)
A fanciful note from an abstraction to the healthcare professionals of the world:
Dear Healthcare Professionals:
Which part of “be nicer” was not clear to you? Did we stutter back in 1977? Is it really too much to ask you to actually treat patients more like people? People with complicated, relevant stories? Stop just saying you get it and start acting like you get it!
Sincerely,
The Biopsychosocial Theory of Health/Care
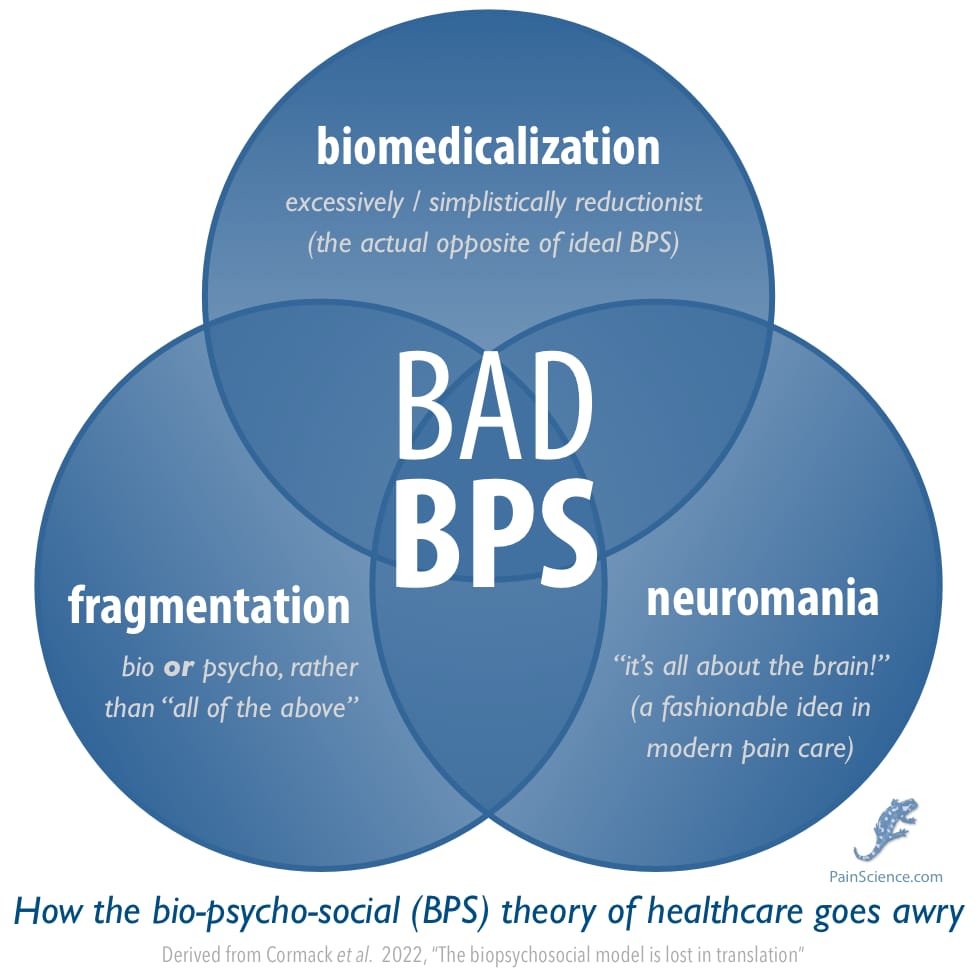
A sneak peak at how BPS goes awry. Much more detail below.
This post is a blend of my own thoughts with highlights from a paper by Cormack et al. about the troubling failures of the biopsychosocial (BPS) theory of healthcare.1 The paper is published in the journal Physiotherapy Theory and Practice, so it focusses on the care of patients with complex physical rehab and chronic pain challenges — problems that we know (or should know) are often more biological and less “mechanical” than anyone used to think, and so it’s particularly important to consider the entire messy patient … literally including their life story.2
So what seems to be the BPS problem?
BPS has always been more fashionable than functional. Clinicians have a tendency to talk the BPS talk, but not so much walk the BPS walk… and this has been going on for decades now.
Cormack et al. offer some ideas about what has gone wrong, and what might be done about it — some BPS upgrades. It’s a fancy paper full of five-dollar words for things that most patients understand easily as the components of good bedside manner: healthcare that treats people not just with compassion, but like it matters who they are, like they have complex lives that are actually relevant to their care. 🤯
No one disagrees with that vision of healthcare. No one would dare! It sounds too wholesome and wise. But it does seem to go rather poorly in practice…
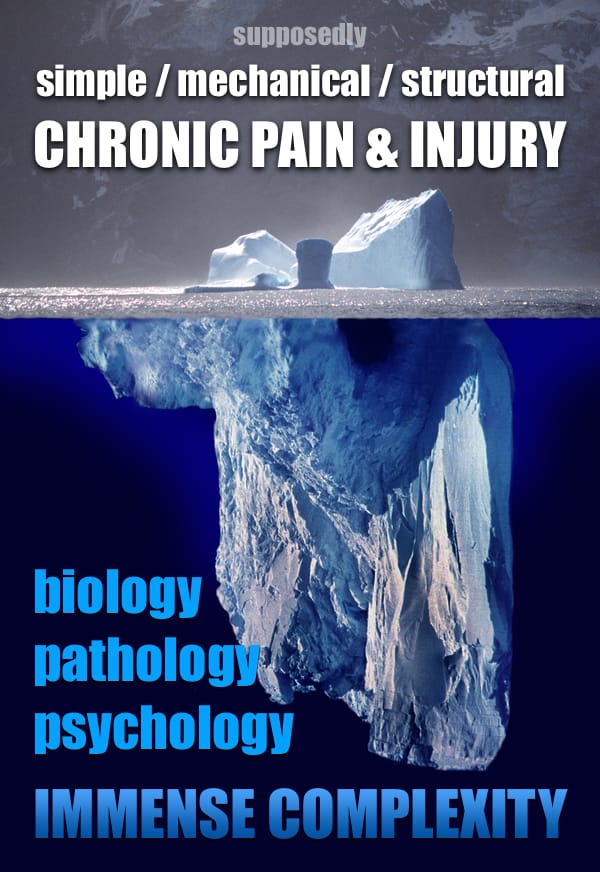
In theory, the biopsychosocial theory of healthcare is all about grappling with the complexity that underlies seemingly “simple” health problems. Complex problems require complex care. But they have to be recognized as complex in the first place! And that routinely doesn’t happen with pain.
Image created by Uwe Kils (iceberg) and User:Wiska Bodo (sky), CC BY-SA 3.0, via Wikimedia Commons.
Most PainScience.com content is free and always will be.? But the rest of today’s post about BPS-ing badly is for PainSci members only. Membership unlocks an additional 2400 words — it’s a big one — and an audio version, plus all past member posts, plus many extra sections all over PainScience.com.
Almost everything on PainScience.com is free, including most blog posts, hundreds of articles, and large parts of articles that have member-areas. Member areas typically contain content that is interesting but less essential — dorky digressions, and extra detail that any keen reader would enjoy, but which the average visitor can take or leave.
PainScience.com is 100% reader-supported by memberships, book sales, and donations. That’s what keep the lights on and allow me to publish everything else (without ads).

Change or cancel plans any time. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism.

{kind=link}
1977: BPS is born
American psychiatrist George Engel cooked up the “biopsychosocial” theory of illness and healing, pushing back against a medical paradigm in the middle of the 20th Century that had become excessively technical, impersonal, and paternalistic. Too many doctors acted as if patients could be treated without knowing anything about them at all other than their test results.
George L. Engel, father of the biopsychosocial perspective.
Some doctors were always wiser than that, of course! Engel was no radical (although no doubt we could probably dig up examples of doctors who scoffed at him as if he were). He just explained, in an academic way, why medicine should climb down off its high horse a bit and take patients seriously as people rather than walking pathologies. He explained that for the first time in his classic 1977 paper.3
BPS was the original “holistic” medicine (before that term was largely co-opted and corrupted by alternative medicine). It meant nothing more (or less) than “the whole person matters.” Another good catch-all term for this is just “humanistic” medicine. The same values are also quite well-known today under the rubric of “patient-centered care.” Cormack et al.:
[Engel] argued that the biomedical model was: reductionist (i.e. complex health concerns inappropriately reduced to biochemical or pathoanatomical processes); dualist (i.e. separated body and mind); and that it “…leaves no room within its framework for the social, psychological, and behavioral dimensions of illness”. He recognized the need for a new approach, moving away from the dehumanizing biomedical model as it does not include the patient and their “…attributes as a person, a human being.”
…
Engel sought to broaden the scope of the clinician’s perspective to include self-reflection on one’s approach to patient assessment and treatment… He also aspired to transform the patient’s role from a passive recipient of care to an active participant in the process of recovery.
Bravo! Reading Engel decades later, it all seems to be a bit of a no-brainer, like he was obviously ahead of his time. We might quibble (endlessly) about exactly what BPS is all about and how to apply it, but good luck finding anyone who objects to the spirit of the thing these days. That would just be weird.
And yet BPS is arguably a failure.
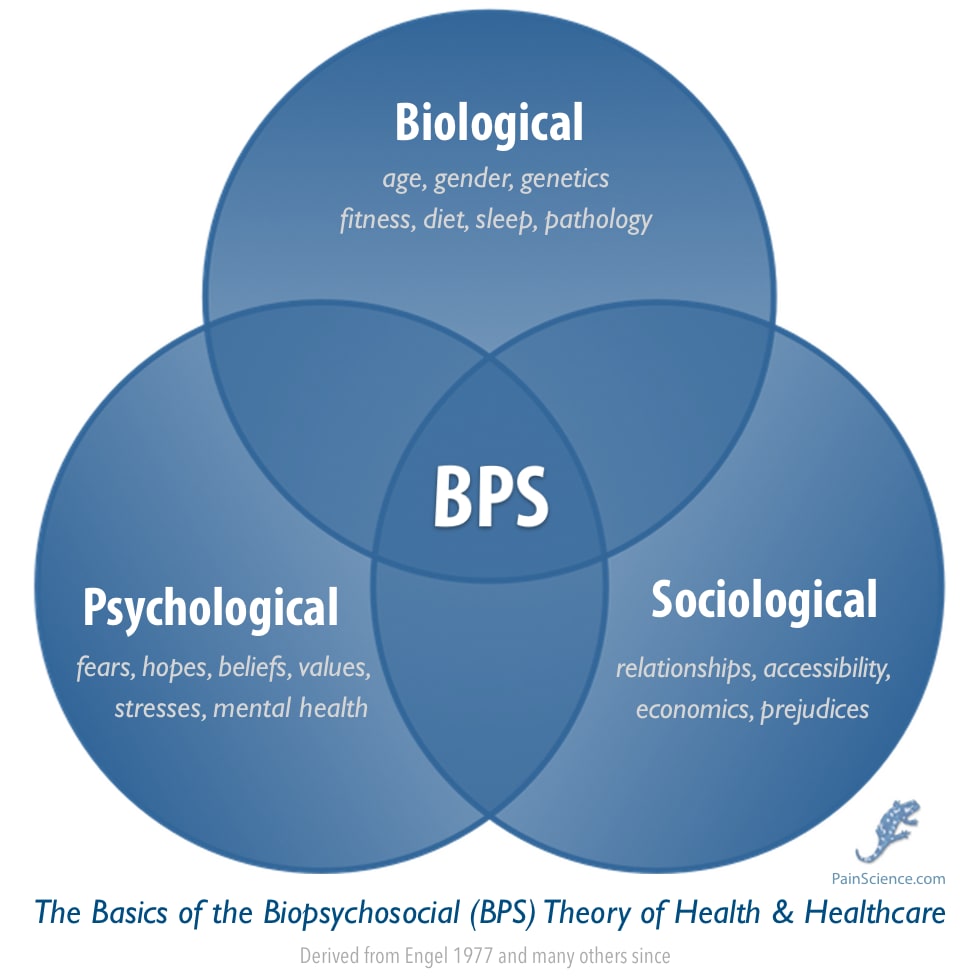
Yet another Venn of the BPS framework of health/care; this one has a bit of my own special sauce. Most won’t mention “prejudices,” for instance — but racism and sexism are huge social factors in healthcare, especially for chronic pain patients.
How BPS fails pain patients
Obviously it’s not all bad news, and there are notable exceptions — occupational therapy stands out as positive example, for instance4 — but the trend is discouraging. There are serious problems. People have noticed! Many patients have learned to hate BPS (even if they don’t know the term). Consider this take from @OnlyEnnui on Twitter:
“BPS model has been fucking people with myalgic encephalomyelitis for years.”
If you’re not familiar with “myalgic encephalomyelitis,” just substitute any poorly understood or hard-to-diagnose illness that causes malaise and pain (e.g fibromyalgia, Ehlers–Danlos syndrome, post-Lyme disease syndrome, endometriosis, celiac disease, and many more). Healthcare providers, often oblivious to the great diversity of “bio” possibilities, shift the diagnostic burden onto the easier scapegoat of the “psychosocial,” and pat themselves on the back for doing it. Worse, they often do this in an insidiously gaslighting way, e.g. “You’ve stressed yourself into chronic illness, it’s self-inflicted burnout, you poor self-sabotaging thing!”5
Or it swings the other way: oversimplification of the bio, rather than overemphasis of the psychosocial. Many patients not only still get treated too much like biological machines that have a glitch, but also in an amateurish way that leads to extreme over-diagnosis of many familiar and simplistic scapegoats for common pain problems: asymmetry, inflexibility, weakness and countless more technical and specific variations on these themes, from glutes or quads that don’t “fire” when they should to subtle spinal subluxations to bad q-angles in your knees.
Biomedicalization, fragmentation, and neuromania
There are (at least) three main ways that BPS has gone wrong in the last couple decades. Cormack et al. explain that the BPS model is “often biomedicalized, fragmented, and used in reductionist ways, thereby deviating from the original model proposed by Engel.”
- Biomedicalization — Professionals are paying lip service to humanism and holism, but still being really rather biomedical. And if you’re biomedicalizing when you’re supposed to be BPS-ing, “U R doin’ it wrong.” The whole idea is not to be excessively or simplistically biomedical! (A moderate and nuanced biomedical approach is not just okay, it’s the goal.)
- Fragmentation — A tendency to see patients’ complaints in terms of this or that (e.g. bio or psycho or social), instead of this and that (it’s always all of the above). Even when BPS is applied more assiduously, often only one major facet of it is emphasized, at the expense of the other.6
- Neuromania — It all boils down to the 🧠! Reducing too many problems to “the brain” — the ultimate scapegoat for symptoms, especially in the world of persistent pain, where there’s often nothing but subjective perception to try to interpret (no objective medical signs). “Reductionism” could have gone other ways, but Cormack et al. flag this specifically as a trend in the last twenty years. It’s not that it’s wrong to consider the role of the brain, of course, but many clinicians do seem to have gone a bit overboard in this direction. I am guilty of a little neuromania myself, circa 2014–2018.7
In other words, it’s not just that providers aren’t BPS-ing right: it’s more just that they aren’t really doing care the BPS way at all. They’re really just making a few token BPS noises while carrying on mostly doing healthcare the old way, making the exact mistakes that Engel wanted to fix.
Result? “Suboptimal musculoskeletal care,” presumably — although that is not a consequence that Cormack et al. substantiate, and it’s interesting to consider the fact that we do not and cannot actually know if good BPS-style care is actually better care. It’s just too hard to standardize for useful testing. It would be like trying to do a clinical trial of charisma. Or fabulousness.
“This is why you fail” — why is BPS-ing so hard?
If the BPS perspective is so attractive and wise, why are patients still so often being treated like relatively simple machines that break down? Or psychosomatic cases?
Life is full of answers that are simple but wrong, and complex but right, and guess where most people go? (I wish I could include the classic Non Sequitur comic strip here, but… copyright.) The biomedical perspective on pain and injury is widely dumbed down to an excessively “mechanical” perspective, what I have called structuralism. That paradigm is appealing and dominant because it is oversimplified: it far easier to understand, and has much clearer clinical implications than BPS. Routinely wrong! But clear. Structuralism is “actionable.”
It also drowns out other ways of looking at health and pain. The more mired a clinician is in structuralism, the more limited their BPS perspective will be. That happens even to smart professionals, but many more clinicians get sucked into the sillier fantasies of alternative medicine: meridians! fascia! vibrations! homeopathic! quantum! And much worse. Such fairy tales are even more seductive because they are even more “magical” in their promises, and even harder to falsify. No one can tell you that you are doing fascial therapy or Reiki wrong, because there are no standards, no right way to fall short of. Convenient.
To compete with such beguiling simplicity, BPS would need an extremely clear vision of a better way to do things. But the complexity of the real problem makes that almost impossible. Cormack et al. point out that “much of Engel’s writings are vague and without a strong underlying theory” and “lack philosophical coherence.” In other words, perhaps it just never clear in th first place exactly what to do with BPS or why. Engel may not have even been all that good at it himself!
It is also important to note that the tone of Engel’s writings reflect the era his papers were written in, as well as what appears, at times, a lingering affinity to aspects of the biomedical paradigm.
Is BPS busted? Nope, it’s just hard
There’s quite a lot wrong with healthcare for people with chronic pain. It’s not just that it’s hard: the difficulties are also chronically underestimated, and so the great need for the skilful application of BPS well is also underestimated.
Rocket science is hard, but that doesn’t mean there’s anything wrong with rocket science, and I don’t think there's anything wrong with BPS itself. It’s a vision of really great healthcare; it would be weird if it was gracefully, consistently implemented across the land. It’s aspirational. Here's Engel from a paper published the year after The Big One, about “the education of health professionals”:
“The key to optimal patient care is collaboration, communication and complementarity among all branches of the health professions… To buttress collaboration, communication, and complementarity, the fourth indispensable attribute of health care professionals must be competence.”
BPS-ing well takes competence, and competence is a rare and precious commodity. “Good help is hard to find” may be one of the most justified clichés of the human condition.
↑ MEMBERS-ONLY AREA ↑
Notes
- Ben Cormack, Peter Stilwell, Sabrina Coninx, Jo Gibson. The biopsychosocial model is lost in translation: from misrepresentation to an enactive modernization. Physiotherapy Theory and Practice. 2022:1–16. PubMed 35645164 ❐ PainSci Bibliography 52047 ❐
- Not every patient’s life story in every situation, of course. While the whole patient is never un-important, you can see how the patient’s life story matters quite a bit less to the ER doc treating a broken nose, or to the oncologist trying to kill someone’s breast tumour. Healthcare needs to be efficient as well as compassionate! It’s a juggling act.
- Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977 Apr;196(4286):129–36. PubMed 847460 ❐
Occupational therapy is probably the closest thing there is to a profession that is really all about trying to help “the entire messy patient.” It’s their main idea. Here’s occupational therapist Dr. Bronnie Lennox Thompson, regarding another paper critiquing the way the BPS framework has been applied over the last 40 years (Nicholas):
There is much I agree with in [Nicholas'] analysis, but I do hold some frustration at the almost complete omission of the contextual work occupational therapists do in pain management. I’m saddened by this omission because it continues the neglect of a profession with a total focus on the person within their own context and with training across the “physical” and “mental” health space."
- That sounds outrageous, but in most cases it either actually that bad or is far too easily mistaken for it. Healthcare professionals really can be that obnoxious (especially with a bit of prejudice). And so most “difficult” patients are sensitized to that subtext… and most compassionate clinicians underestimate how hard it is to avoid sending the wrong message when you talk about psychological factors in pain/illness, how extraordinarily clear and careful you have to be to defuse the “all in your head” implications. Patients can smell that bullshit a mile away, no matter how artfully it is presented. In many if not most cases, I think it’s wiser to just not talk about the psychosocial dimensions of pain at all, rather than risking it sound anything like the actual gaslighting that nearly all patients are sick of.
Cormack et al. argues that two different aspects of BPS are often emphasized at the expense of each other:
When there is an emphasis on lived experience or the relational and communication elements in Engel’s BPSM, we call this focus the “humanistic” version of the BPSM. When there is an emphasis on factors or mechanisms contributing to a person’s health concern, we call this the “causation” version of the BPSM. Historically these two versions of the BPSM with their particular focus (i.e. humanism or causation) have been running mostly in parallel in the literature and rarely integrated in meaningful ways.
- I may have run too far with the idea that pain is “always an output of the brain,” and I’m probably even guilty of pushing some receptive clinicians into neuromania with my writing. That is still evident in some of my published work today. In my defense, I started to retreat from that almost immediately (and you can see that in my writing too).