Suffering, Disability & Pain
There’s the pain, and there’s the effect it has on lives
Anything nice or uplifting will “help” chronic pain — like good music, or puppy boops, or seeing a Nazi get punched. But that’s about easing suffering, not pain itself. At best, things like music therapy might produce some modest modulation of pain intensity. Many “treatments” for pain are essentially just … pleasant! Comforting, reassuring, encouraging, affirming. While those are good things, they aren't medicine for the actual pain that’s driving the suffering in the first place.
Pain and suffering are clearly not the same thing, but they are often confused and conflated to the detriment of patients and healthcare for pain:
- Improvements in mood after treatments are routinely mistaken for effective treatment. Reductions in suffering, even trivial and temporary ones, are a big part of “placebo” — the illusion of treatment.1 Even simple customer satisfaction is often mistaken for efficacy.
- People believe that suffering causes pain just as much as pain causes suffering, and that easing suffering will therefore ease the pain — but that probably does not work.
- Beliefs about suffering are warped by the popular idea that “suffering is optional,” which can gaslight patients by insinuating that they suffer because they aren’t tough or wise enough.
This article digs into each of these ideas in more detail.
Whoever is spared personal pain must feel himself called to help in diminishing the pain of others. We must all carry our share of the misery which lies upon the world.
Albert Schweitzer
Isn’t reducing suffering a good thing?
Reducing suffering not as important as treating the pain that’s causing it, whenever possible, but, yes, of course it’s also worthwhile to reduce suffering. People should be helped with their suffering and disability as much as possible, in every way possible.
I am on the record extolling the virtues of inherently pleasant treatments — like some kinds of massage therapy — arguing that the pleasantness is the point. In the absence of clear medical benefits,2 for instance, massage is at least a sensory treat that can improve mood and reduce anxiety, inspire, and give us a bloody break or distraction from whatever pain we have. That has real value.
As a chronic pain patient myself, I have enjoyed many an ephemeral pleasure or comfort that “helped” my pain by helping me live with it. But I’ve also never mistaken it for actually treating the pain that was causing the suffering in the first place.
Unless they are the same? Which is strongly implied by the formal definition of pain?!
Pain is formally defined as an “unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”3 The definition of pain includes our emotional experience of it.
Both pain and suffering are subjective experiences that can’t be measured. There is no pain-o-meter4 or misery-o-meter. A person with moderate pain and high psychological distress is mostly indistinguishable from someone who is calmer about much more intense pain.
And what is indistinguishable in practice is practically identical.
Pain and suffering are still different things, I pinkie swear
Identical in practice is not identical in theory. There is no formal definition of pain-related suffering, somewhat famously among pain nerds, but here’s my crack at an informal definition, cribbed from Stilwell et al. (co-authored by salamander friend Keith Meldrum of A Path Forward):5
Pain-related suffering is a subjective experience characterized by negative emotions that are related to pain but distinct from it, and which can disrupt even a “minimal” sense of self.
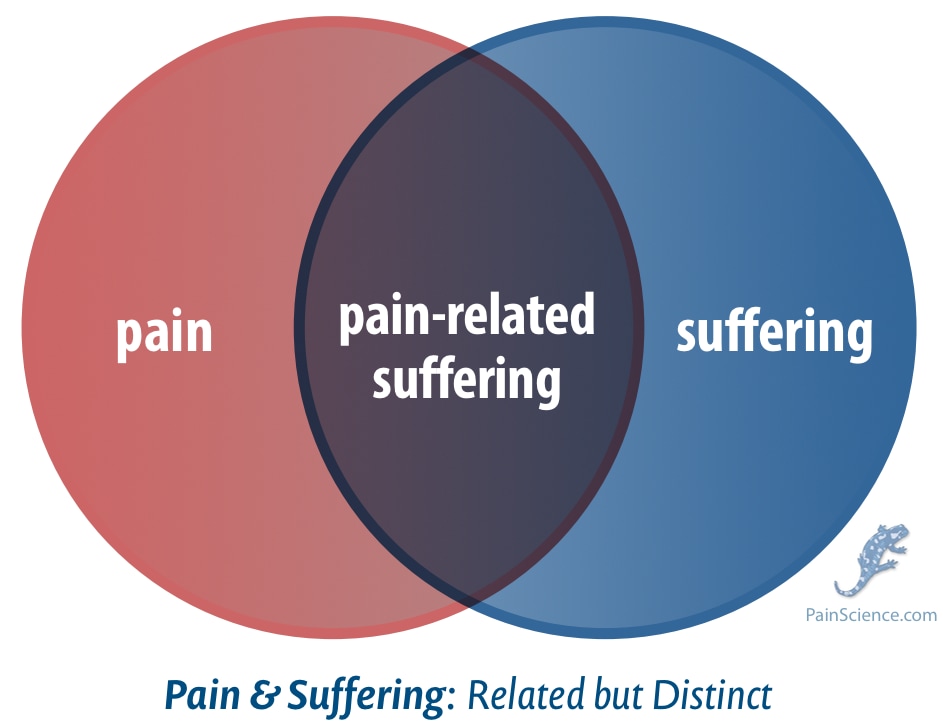
The lines between pain and suffering get blurry because they affect each other and produce similar behaviours, not because they are literally the same phenomenon. They may be hard to tease apart from the outside, but they are still neurophysiologically distinct — much like anxiety and depression, but no one thinks those are identical. Or pain and injury, or yin and yang, or burritos and tacos. This is what Venn diagrams are for!
It’s helpful to think about pain and suffering as more or less distinct for some purposes and not others. It can be useful to think of them as different sides of the same coin … but it can also be useful to think of them as truly separate things that simply have a strong interaction. Neither perspective is wrong.
So what? Why does it matter that pain and suffering aren’t the same thing?
The distinction matters because pain and suffering can be conflated in ways that can be harmful to patients. Relatively minor comforts and pleasures are often misrepresented and oversold as a form of pain treatment, even prescribed and emphasized in lieu of a dedicated pursuit of a diagnosis for pain that actually is treatable. Unfortunately, I think this happens much more than it should.
A great many kinds of chronic pain are extremely difficult to treat, if not impossible, but not all are.
For instance, when women report symptoms, they are often not taken seriously — and pathology that could be treated is never even diagnosed in the first place. And that tragedy is exacerbated when those
There’s no way to know how often this mistake is made, or how badly. But I believe this kind of healthcare malfunction happens because I’ve personally experienced it, and because I’ve heard many such stories from both my own clients (back in the day) and also from my readers (over the last 15 years). It’s also quite plausible, because “that figures,” given human nature. It is often associated with not taking pain seriously, a patronizing attitude that implies that the pain is “no big deal,” and therefore a little comfort and reassurance ought to do the trivial trick.
Even in more earnest pain treatment contexts — like trying to treat chronic pain patients with cognitive behavioural therapy — I see the worrisome and self-serving assumption that it works because suffering is supposedly causing the pain at least as much as the other way around, if not completely inverted, and so treating the suffering is seen as an indirect pain treatment. That’s an uncertain hypothesis at best, or dangerous snake oil at worst. Despite good intentions, we know that CBT doesn’t actually do much for pain.7
Thinking about pain and suffering as distinct ideas helps us navigate these troubled waters.
The closest thing we have to a formal definition of pain-related suffering
I defined pain-related suffering above by cribbing from Stillwell et al., who did it more formally. It’s worth looking at that paper in detail, because it’s essentially the only modern attempt to grok this.
Stillwell et al. argue that “pain-related suffering” remains an underdeveloped but important idea in pain science. Despite decades of emphasis on suffering in theoretical models, it has actually never been defined by the International Association for the Study of Pain. And they did not technically attempt a “definition,” but rather a preliminary step towards an “operationalization” — a bridge between theory and practice, a guide to how we might study and recognize pain-related suffering.
They built on Eric Cassell’s influential writings, and critiqued them. Cassell described suffering as a private experience of distress caused by a perceived threat to one’s integrity as a person — but his definitions were inconsistent and probably too dependent on self-reflection. If being able to think about yourself in detail (self-reflection and awareness of past and future) is necessary for suffering, that would exclude infants, animals, or people with impaired cognition.
The paper cites diverse philosophical, psychological, and clinical literature to identify the four essential attributes of suffering:
- Pain and suffering are inter-related yet distinct: one can hurt without suffering, or suffer without pain. Suffering is not reducible to nociception or sensory intensity alone; it arises when pain becomes personally meaningful as a threat to the self. Just the multiplication of intensity by duration can make a “mild” pain into a nightmare, like water torture.
- Suffering is fundamentally subjective. Like pain, it cannot be directly observed or measured by external markers; it can only be known through narrative and self-report.
- Suffering is characterized by a negative affective valence — an overarching emotional tone of distress, fear, anger, and/or despair. This clarification avoids Cassell’s circular use of the term “distress” and anchors suffering within affective terminology.
- Disruption to one’s sense of self is a major aspect of suffering. Persistent pain can fracture identity: patients report losing their former roles and values, being forcefully changed.
Stillwell et al. also explain that evidence from phenomenology and pain narratives suggests that suffering can obliterate reflection rather than requiring it. They suggest accounting for this by citing Shaun Gallagher’s “minimal self,” an alternative to the more conventional narrative self, a felt ownership of experience that exists without a “story” about who you are, where you’ve been, or where you’re going. In other words, pain can cause suffering before you have a chance to think about what it means for your hopes and dreams for the future. But then of course it can also mess with that!
The authors call for qualitative research to distinguish reflective and pre-reflective suffering, to guide better clinical recognition and relief of suffering in all creatures capable of it.
Is it bad to suffer?
Not everyone with pain thinks they are “suffering.” People with chronic pain have a wide range of responses to the idea of suffering, many of them with deep cultural roots.
While many do embrace it as validating, and would like greater recognition of it as a distinct aspect of living with pain, others reject it as inadequate or even negative, implying a lack of coping skills and resilience and a low quality of life. Some pain patients believe that it’s unhealthy to have an adversarial relationship with their pain, and so they prefer not to think of themselves as “suffering” because it emphasizes the combative relationship with pain they are trying to put behind them. If you believe that “suffering is optional” — much more on this phrase coming up next — then surely the goal is to stop choosing it?
At the other end of the spectrum, many pain patients are content to think of their pain as an adversary — and a fierce one at that — and do not believe that suffering implies any a lack of resilience, a low quality of life, or a failure to reject or transcend optional suffering.
And that is my official position: suffering does not imply inadequacy. It is normal and natural and healthy to suffer with many kinds of pain, just as it is healthy to grieve and mourn. But there is no right answer, of course — just a great human variety ways of coping with pain.
Suffering is “optional”?
This famous quote from Haruki Murakami contains both genuine wisdom and great potential for abuse in the context of chronic physical pain:
“Pain is inevitable. Suffering is optional.”
It’s not a useless idea, of course. It is mainly about psychological pain, but it certainly has infected pain care, where it is highly problematic for pain patients. Sub-topics:
- The strong harmonization between “suffering is optional” and toxic positivity.
- Many common types of pain are just too much like torture to transcend. Pain and suffering are inevitable.
- Please never risk implying that people could be suffering less with their pain if only they were somehow … wiser. Smarter. If only they could just get their shit a bit more together.
It’s a famous quote for good reason. Obviously there is some value in the idea. It is clearly useful if “pain” is defined loosely: the pain of life! Existential anguish, grief, Weltschmerz, dukkha.8
In my tortured youth, I was often stunned into paralyzed despair by all the awfulness in the world that I couldn’t look away from. I was rescued from that pattern partly by Victor Frankl’s book, Man’s Search for Meaning, which (long ago) gave me the mind-blowing idea that I could always choose my response to life’s challenges, no matter how extreme — especially since they were obviously less extreme than Frankl’s had been (in a Nazi concentration camp).910
The 2013 “Gunshow” webcomic by artist KC Green that became a meme that has been used to illustrate the pathos of countless life predicaments — and it couldn’t be more apt for this “suffering is optional” thing!
And “suffering is optional” is the pithiest expression of that principle. So yes: it can be useful.
But it’s much less useful when it comes to the pain of having a sick or hurt body. And it’s so ridiculously ripe for abuse, so easily transmogrified into gaslighting, that I consider it verboten.
It is true that we can figure out how to suffer less with some kinds of pain. Many good healthcare professionals will focus on those opportunities, healthcare of the possible, helping people achieve whatever can be achieved in some of life’s most painful and intractable medical predicaments. Good stuff, truly.
But that can all be achieved without ever leaning on any interpretation of “suffering is optional.”
The link between “suffering is optional” and toxic positivity
We shouldn’t ever actually say “suffering is optional” because it so strongly implies that pain-related suffering can be nuked from orbit by sheer force of will — an idea that angers and demoralizes millions of pain patients every day. The phrase doesn’t have to imply that, but it usually does anyway, because it harmonizes so clearly and dangerously with “toxic positivity.”
Toxic positivity is the culturally pervasive and harmful belief that even serious health problems can be greatly mitigated by the power of positive thinking. It always sounds uplifting until you turn that coin over and see … ah, yes, there’s the problem: blaming continued illness on the failure to think positively! That doesn’t sound right! Because it’s not.
“Suffering is optional” and “positive thinking heals” are practically the same idea in practice for the last twenty years.
Many common types of pain are just too much like torture to transcend
Suffering and disability might be blunted and eased — and they should be wherever possible — but they will never be “optional” with conditions like fibromyalgia or trigeminal neuralgia. Other examples:
- Cluster headaches will make a mockery of almost anyone’s best efforts to not react to the pain with suffering.
- Chronic pancreatitis is a pain Goliath that will crush the patient’s David every time — there are no unlikely victories for an underdog against an opponent that huge and fierce.
- Gout is famously disabling and dehumanizing even to the most stoic patients.
- Rheumatoid arthritis can feel like being on fire from the inside out, and in the history of human psychology no one has ever found a way to be “fine” with that.
And so on and on. This is just a few highlights from the full list of the worst imaginable chronic pains.11
Surely one cannot know such pain personally and think that suffering is “optional”? You'd be surprised! Many patients with intense pain do try to live by this principle anyway, for many reasons, chiefly desperation, of course … or because a healthcare professional convinced them of it. But it’s not a hard sell for those of us immersed in the culture that produced “toxic positivity” in the first place. And so plenty of patients earnestly believe that their suffering is indeed optional, and therefore they doggedly pursue every conceivable strategy to minimize and reject it — and I’m not knocking that. Whatever keeps your boat afloat.
But please beware of that “river in Egypt”: denial! It’s often people with less intense kinds of chronic pain that have the luxury of believing that suffering is optional. The quest to transcend suffering can easily become quixotic and unrealistic, leading only to disappointment in time.
Err on the side of never saying or even implying that suffering is optional
There are some fascinating exceptions, chronic pain patients who have found ways to suffer less than others, despite profound ongoing pain — but they are rare and mostly just prove the rule. For most people with severe chronic pain, the idea that suffering is “optional” is unrealistic at best … and fully offensive, gaslighty, and irresponsible at worst. The risk of the latter is so great that it’s best to steer clear of it completely.
Here’s a good example of a chronic pain patient being irritated by the Murakami quote:
As someone with a chronic pain disorder, while I appreciate the concept of trying to live your best life despite whatever gets thrown at you, this is hot nonsense. There is no other way to describe a decade of constant pain as anything other than suffering.
Like that person, I much prefer this adage (no clear attribution), which seems much less vulnerable to abuse:
“If you’re going through hell, keep going.”
That is an inspiring slogan I can work with!12 It captures the spirit of what I like most about occupational therapy, for instance. Good healthcare should always try to help people with pain to “keep going” with as much dignity as possible. But the suffering is not optional.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
Jan 2, 2026 — Several refinements and additions based on public feedback. Most notably, I’ve added a section acknowledging the wide range of emotional responses to the idea of suffering in pain patients — not everyone thinks it’s validating or wants to embrace it!
2025 — Added a whole bunch of content about “pain is inevitable, suffering is optional.” The new section also contains a super-footnote, a little article unto itself, about the worst imaginable kinds of chronic pain.
2025 — Publication.
Notes
- Placebo is fascinating, but its “power” isn’t all it’s cracked up to be, not even for relief of purely subjective symptoms like pain: the power of belief is strictly limited and accounts for only a little of what we think of as “the” placebo effect, which is actually a collection of diverse nonspecific effects and research artifacts. For more information, see Placebo Power Hype: The placebo effect is fascinating, but its “power” isn’t all it’s cracked up to be.
- Massage is popular and pleasant, with real benefits for mood and mental health, but little evidence for treating back, neck, or other musculoskeletal pain. Training varies widely and the field includes much pseudoscience. Even so, its psychological benefits and sensory pleasures alone make it worthwhile. For more information, see Does Massage Therapy Work? A review of the science of massage therapy … such as it is.
- IASP-pain.org [Internet]. International Association for the Study of Pain. IASP Taxonomy; 2012 May 22 [cited 19 Sep 5]. PainSci Bibliography 53250 ❐
- Objective pain-measurement is a medical fantasy that has been “five years” away for decades now. It’s either impossible in principle, and/or just hopelessly beyond our current reach. See There will never be a pain-o-meter — and maybe that’s a good thing.
- Stilwell P, Hudon A, Meldrum K, Pagé MG, Wideman TH. What is Pain-Related Suffering? Conceptual Critiques, Key Attributes, and Outstanding Questions. J Pain. 2022 May;23(5):729–738. PubMed 34852304 ❐ There's full reporting of this paper below.
- Loder S, Sheikh HU, Loder E. The prevalence, burden, and treatment of severe, frequent, and migraine headaches in US minority populations: statistics from National Survey studies. Headache. 2015 Feb;55(2):214–28. PubMed 25644596 ❐
Across large U.S. population studies, migraine and severe headache are most common among Native Americans (17%), followed by Whites (15%), Hispanics (14%), and Blacks (14%), and least common in Asians (9%). In all groups, women are roughly twice as likely to be affected, suggesting strong sex-related biological or hormonal drivers. Chronic migraine (≥15 headache days per month) is especially prevalent in Hispanic women, while White men have the lowest rates.
Healthcare data shows fewer migraine-specific medical visits among Hispanics and Blacks, implying disparities in diagnosis or access to specialized care. Limited subgroup data suggest that grouping diverse populations, such as all “Asians,” may obscure clinically relevant differences. Overall, the evidence points to both biological and systemic factors shaping racial and ethnic variations in migraine prevalence and treatment in the U.S.
This evidence does not directly support the claim that migraine is underdiagnosed in women, and there is no data for that. However, it is strongly implied, insofar as sexism and racism have similar effects on care, all migraine is underdiagnosed, and it’s particularly clear from this data that women of any race have more migraine.
- Ingraham. Cognitive Behavioural Therapy for Chronic Pain: The science of CBT, ACT, and other mainstream psychotherapies for chronic pain. PainScience.com. 5511 words.
- “Pain” gets used poetically a lot. We use it as a metaphor or analogy to describe other very strong, unpleasant emotions. We use it that way precisely because it is different, in a league of its own, so much more immediate and vivid and disruptive; it’s what we measure other strong emotions against, declaring that they are “pain-like” in their intensity and power to make us suffer.
- Frankl VE. Man’s Search for Meaning. Beacon Press (English); 1946.
Frankl’s influential 1946 book chronicles his experiences as a prisoner in Nazi concentration camps during World War II, and describes his psychotherapeutic methods, which involved identifying a purpose to each person’s life through one of three ways: the completion of tasks, caring for another person, or finding meaning by facing suffering with dignity.
As a much younger man, this book is where I got the idea that it was entirely up to me to choose my emotional response to hardship. As a Canadian in the late 20th Century, I could barely conceive of the kinds of hardships Frankl had endured, but that was all the more reason to believe that I could cope with much less dramatic life challenges. Thirty years on, pain-related suffering now connects the book to my work here on PainScience.com, especially the popular idea that “pain is inevitable, but suffering is optional,” which is under the umbrella of the very modern problem of “toxic positivity.”
A major takeaway from Frankl’s book is the claim that a positive mental attitude correlated strongly with long-term survival in the Nazi death camps, which is widely regarded as one of the most famous and compelling examples of the alleged power of positive thinking — but the book and that key claim have been criticized, and even if that correlation was real, it’s still a long way from there to the ideas that pain-related suffering is “optional” or that positive thinking is good for pain.
A more nuanced take is that Frankl distinguished between suffering with more and less meaning and dignity, and that's what made the difference — very particular ways of thinking positively. Obviously this concept could be relevant to many kinds of suffering, and perhaps pain as well. But, as one reader put it, “chronic pain is an alternative universe where normal rules of life don’t apply.”
Continuing further into the personal, there was another critical insight that spelled the end of my depressive period: there is no problem so severe that it cannot be made worse by self-pity and paralysis. 🤯
To this day, this is my best-ever example of a consequential epiphany. It changed me forever, one of the Big Three behavioural changes I’ve experienced in my life. The other two were forced marches across tipping points, achieved slowly, one desperate and determined step at a time. But that epiphany was much easier, completely irresistible. To have it was to change, no work required, really: just poof, I’m different now. But also mysterious! I have no idea how to generate another epiphany like that. I might never have another. Substantial behaviour changes are strange beasts!
Worst kinds of chronic pain
Ranking pain is seductive and misleading, and no pain can be objectively “the worst,” of course. What makes a pain terrible is extremely personal: read more for some context. That said, here is the official PainSci list of the worst kinds of chronic pain. This list is not about acute pain, even if it can occasionally turn chronic or recurrent. I’ve excluded pains that are mostly one bad experience, like a kidney stone or appendicitis. This list includes disorders that mainly cause continuous, long-term pain, or episodes that are severe/frequent/long enough to really mess with people’s lives.
List updated: December 30, 2025.
Continuous or near-continuous severe pain:
- Complex regional pain syndrome
- Central pain syndromes (post-stroke, spinal cord injury, multiple sclerosis)
- Small fiber neuropathy
- Trigeminal neuralgia (when frequent or refractory)
- Chronic pancreatitis
- Interstitial cystitis / bladder pain syndrome
- Fibromyalgia
- Advanced cancer pain syndromes
- Endometriosis
- Pudendal neuralgia
Chronic-episodic pain with extreme intensity:
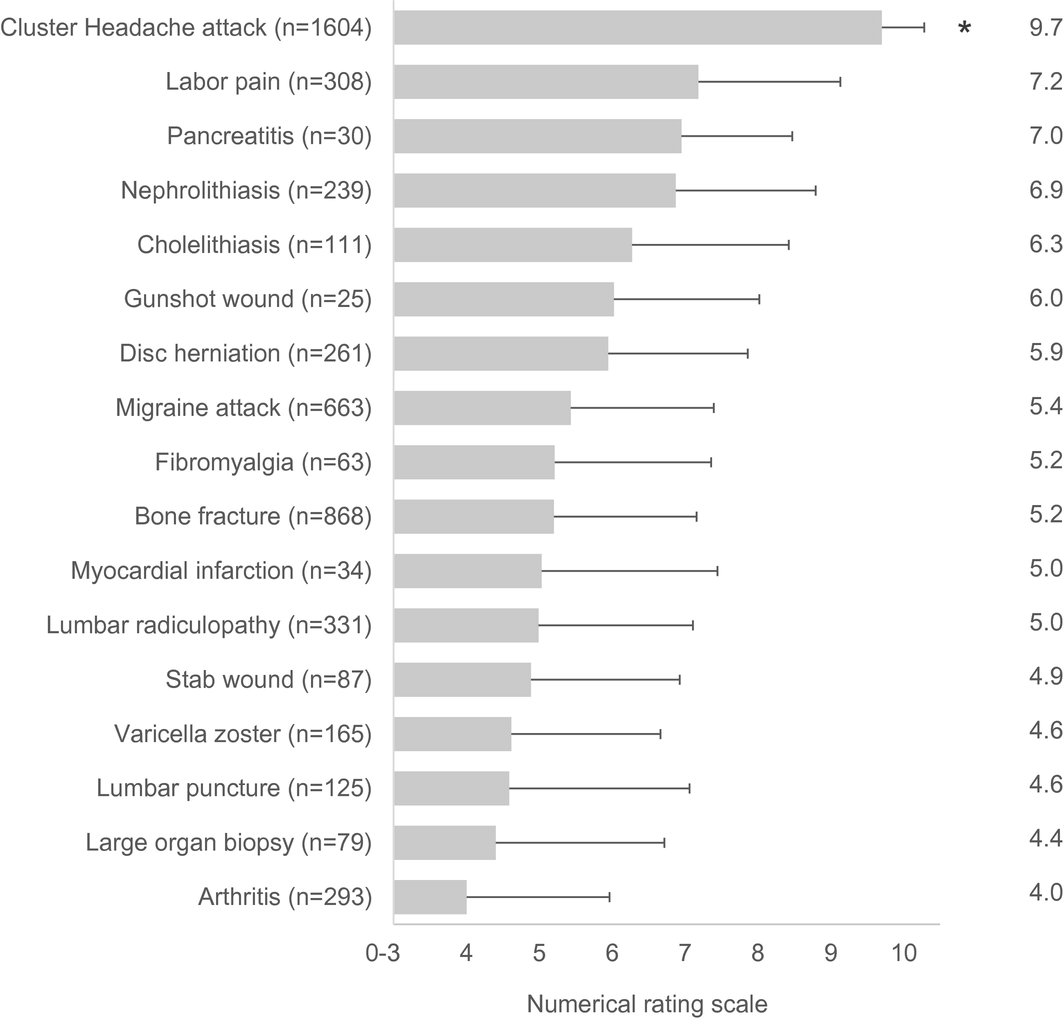
- Cluster headache (people who’ve had both cluster headaches and other kinds of severe pain all seem to agree that cluster headaches are by far the worst, see graph from Burish et al. below)
- Chronic migraine
- Hemicrania continua / SUNCT-type disorders
- Recurrent severe gout / chronic tophaceous gout
- Sickle-cell pain crises
- New daily persistent headache (a headache that starts one memorable bad day and just never stops)
- Recurrent renal colic (stone formers with frequent obstruction)
- Trigeminal autonomic cephalalgias (broader group)
![Horizontal bar chart from Burish et al. 2021 showing average pain intensity (0–10 numeric rating scale) for 17 conditions with sample sizes (n) and error bars for variability: cluster headache attacks are highest at 9.7 (n=1604, marked with an asterisk), followed by labor pain 7.2 (n=308), pancreatitis 7.0 (n=30), nephrolithiasis/kidney stones 6.9 (n=239), cholelithiasis/gallstones 6.3 (n=111), gunshot wound 6.0 (n=25), disc herniation 5.9 (n=261), migraine attack 5.4 (n=663), fibromyalgia 5.2 (n=63), bone fracture 5.2 (n=868), myocardial infarction/heart attack 5.0 (n=34), lumbar radiculopathy 5.0 (n=331), stab wound 4.9 (n=87), varicella zoster/shingles 4.6 (n=165), lumbar puncture 4.6 (n=125), large organ biopsy 4.4 (n=79), and arthritis lowest at 4.0 (n=293); axes are labeled “Numerical rating scale,” with values from 0–10, and each bar includes whiskers indicating spread/uncertainty.]()
Cluster headache patients think cluster headaches are more painful than any of those other things — based on their own experience with both cluster headaches and those other conditions! 🤯 (Exploding head emoji unusually apt here!) Graph is from Burish et al., Headache, 2020.
Intermittent-but-progressive or relapsing neuropathic/inflammatory:
- Post-herpetic neuralgia (not shingles, but pain that persists after the shingles subsides)
- Severe rheumatoid arthritis or ankylosing spondylitis
- Ehlers-Danlos with chronic pain flares
- Diabetic neuropathy
Honourable mentions, conditions that aren’t so much known for their intensity but are “special” in some other way that makes them terrible:
- Eczema, thanks to the combination of pain with itching — extremely distressing.
- Vaginismus, vulvodynia and vestibulodynia, thanks to the intense stigma.
- Phantom limb syndrome, because it is so bizarre: very psychologically unsettling!
- I’ve already mentioned MS, but the “multiple sclerosis hug” deserves a callout: a painful, suffocating spasticity of the trunk muscles.
- Pubic symphysis diastasis, probably because it feels so “core.”
- Polymyalgia rheumatica: although treatable with steroids such that it’s only a temporary horror for most patients, it is notoriously savage … and not everyone gets diagnosed and treated.
- It shifts me into a proactive, feistier, can-do mode — more assertive or even aggressive. This means war! Which is definitely better than getting stuck like a dear in the headlights, paralyzed by misfortune! Which I have allowed myself to do in the past.