Does Craniosacral Therapy Work?
Craniosacral therapists make big promises, but their methods have failed to pass every fair scientific test of efficacy or plausibility
Craniosacral therapy (CST) doesn’t look like much: light holding of the skull and sacrum and some barely detectable manipulations. Indeed, the action of craniosacral therapy is so gentle and slight that it is the best example of the so-called “subtle” manual therapies,1 which claim to achieve profound health benefits with minor and safe hands-on tinkering. Practitioners believe that the tiny manipulations of CST affect the pressure and circulation of cerebrospinal fluid, the fluid that surrounds and cushions the brain and spinal cord.
The founder of modern CST, John Upledger, an osteopath,2 is one of the more famous personalities in complementary and alternative medicine. He built on much older ideas, of course.3 Mr. Upledger says that CST “works with natural and unique rhythms of our different body systems to pinpoint and correct source problems.”

No one can deny that craniosacral therapy is relaxing. But, then again, so is a nap. And a nap is cheaper.
Does craniosacral therapy work as advertised?
Skeptics have always had several concerns about craniosacral therapy (here’s a good CST reading list from EBM-First.com):
- CST is an alleged solution in search of a problem. CSF circulation doesn’t need to be manipulated or stimulated, because it isn’t ever meaningfully “stagnant” in the first place. There are no common or relatively minor problems that are attributed to it by any expert, and so CST is a solution to a problem that doesn’t exist.5 There is no credible evidence that CST has clinically significant effects on pain, for instance.6
- There is good, recent scientific evidence that the most important and basic assumption about how CST works is just not true: craniosacral therapists cannot actually move the bones of the skull enough to affect the pressure or circulation of the fluid surrounding the brain and spinal column.7 Although CST fluid does circulate, we know that it’s pumped almost entirely by respiration,8 not skull movement.
- The cranial bones do not even move to relieve the pressure of dangerous swelling in the cranium, so they are probably not going to move for therapist’s fingers either.9
- There is both old and new evidence that CST therapists produce conflicting diagnoses of the same patients.1011 That is, when asked to assess a patient the CST way, they come to mutually exclusive conclusions.
- Any effect that CST has on people must be a complex and subtle one, since it cannot be measured. Subtle effects of manual therapy probably do exist — just because it can’t be measured doesn’t mean it isn’t there — but it seems unlikely that any therapist is wise and knowing enough to reliably produce a therapeutic effect by leveraging a phenomenon so subtle that it can’t be measured. And there just aren’t any good quality studies showing that CST does anything to CSF circulation or helps patients. The closest is probably a 2015 study comparing CST to light touch for neck pain: it claimed to find evidence of a minor benefit, but it was quite flawed and probably got it wrong.12
Despite more than 50 years of investigation & the promotion of CST by some practitioners, there remains a void in credible evidence supporting the ability of these techniques to alter the movement of the cranial sutures or improve patient-centered outcomes. … The time is past due for advocates of CST to contribute well-designed studies evaluating the efficacy of these techniques to the peer-reviewed literature. The challenge is clear: prove that it works, or move on.
Flynn et al., 2006, Journal of Orthopaedic & Sports Physical Therapy
CST is guilty by association with the prevalent pseudoscientific claim of “increasing circulation”
The idea that craniosacral therapy increases the circulation of cerebrospinal fluid is transparently riffing on a much more quotidian myth about massage: the belief that it meaningfully increases the circulation of blood, and that this is one of the main mechanisms of helping patients. Most massage therapists claim to increase the circulation of blood; CST practitioners up the ante by claiming to increase a much more subtle and exotic type of circulation.
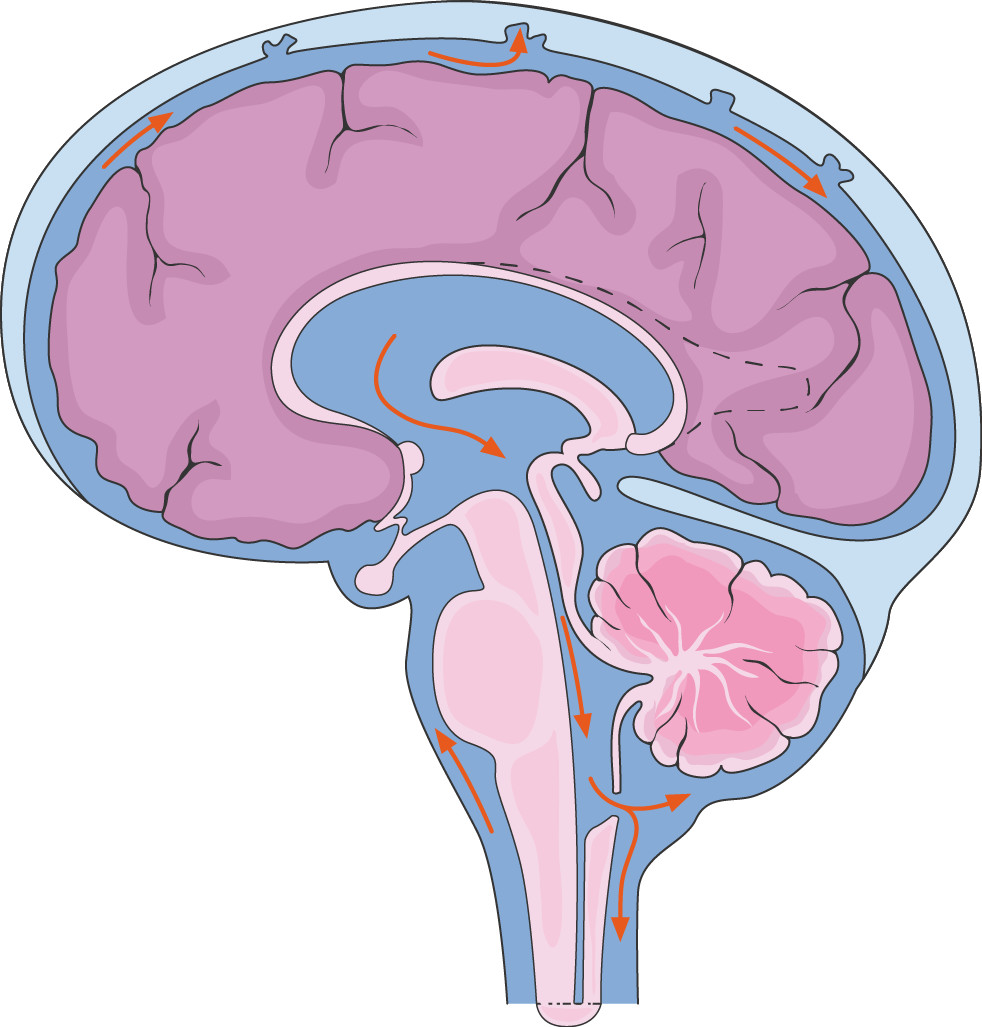
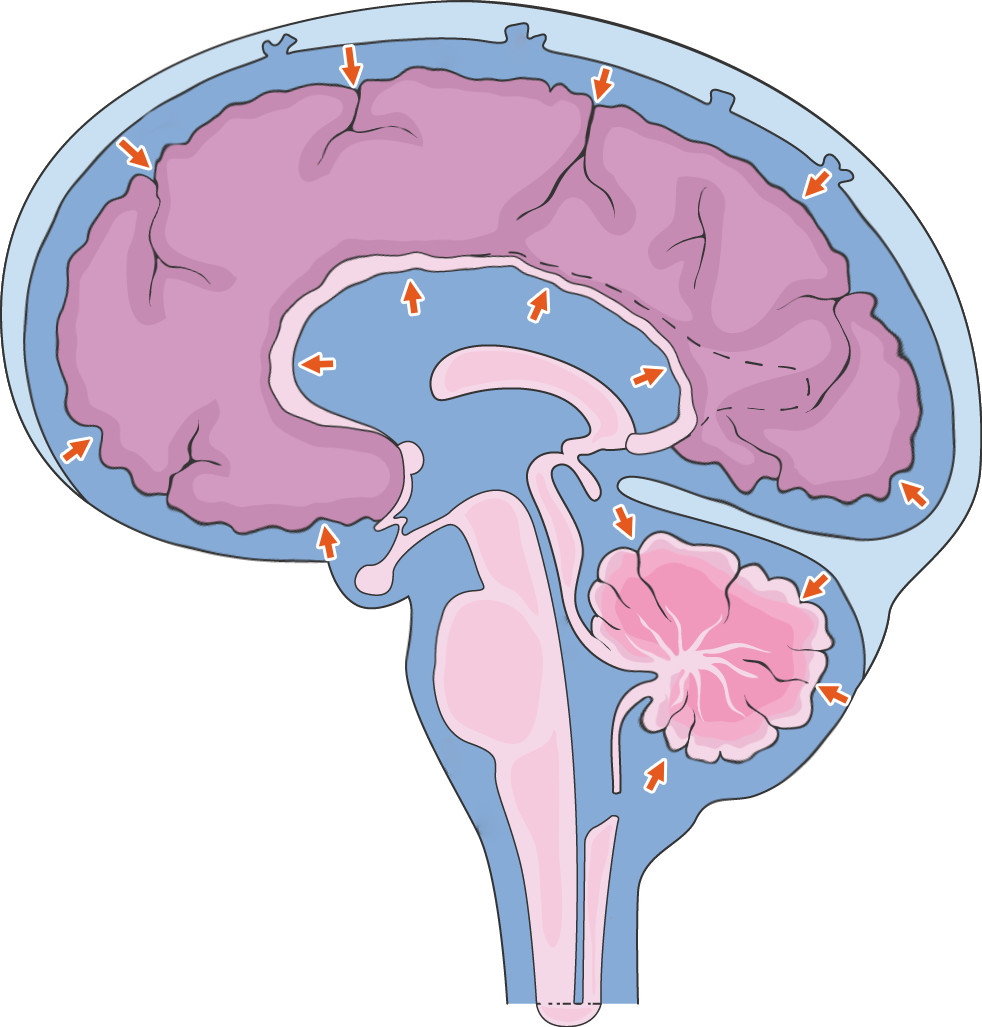
Cerebrospinal fluid flows around the brain, brain stem, and spinal cord, mainly pumped by respiratory movement of the trunk.
Massage therapy supposedly “increases circulation,” and this is one of the main mechanisms of helping patients. Although massage probably does sometimes modestly boost circulation in some ways, the scientific evidence shows that it’s too little to matter. Most importantly, light exercise is clearly a much stronger driver of circulation. Because the circulatory system is closed and blood volume is constant, circulation can only “increase” in an area at the expense of another. Also, the relaxation that we expect from any decent massage actually shunts blood into the core, away from the muscles, a robust effect that likely dominates the equation.
Blood clots broken loose by massage will be swept downstream by the circulation until they finally get trapped by the filter of the lungs, with symptoms ranging from trivial to deadly: a kind of circulatory effect, with vital safety implications. Serious examples are rare, but “minor” lung damage may be disturbingly under-reported. Clots mostly form in the calves (deep vein thrombosis), and so calf massage for a higher-risk person is like playing Russian roulette. Notably, COVID has increased clotting risks in huge numbers of people.
For more information, see Does Massage Increase Circulation? Almost certainly not in a clinically important way, and definitely not as much as even a small amount of exercise.
“Circulation boosting” of all kinds is a common concept in alternative medicine, often touted and never validated. To the extent that it’s true in some contexts, it’s probably not very important; to the extent that circulation actually matters (and of course it does), it’s not something that any therapy has much power over.
Even if boosting blood circulation with massage is definitely a myth, of course it’s possible that CSF circulation could be significantly stimulated. They are entirely different things, after all. But they are based on a shared type of motivated reasoning: imprecise and self-serving attempts to explain a treatment effect that is assumed to be true.
At least craniosacral therapy is actually relaxing
I have experienced CST. It is truly, deeply comforting to have your head held and gently manipulated for a long time by a craniosacral therapist with the best intentions to provide a soothing experience.
Also on the bright side, I have no doubt at all that there are emotional benefits to the touch therapy involved. And I am happy to admit that there might be some “interesting” neurological effects, some of which may even be therapeutic — I provide a peculiar example below. Which has nothing to do with how CST supposedly works, but still: effects! And of course they aren’t medically harmful. This is, after all, a gentle therapy.
Despite my own professional expertise, I do not begin to have the power to micro-manage such subtle and “interesting” neurological effects … assuming they exist at all. This is a simple matter of humility. Anyone who has studied physiology and neurology honestly must admit to profound ignorance. No one knows how that system really works. There are just too many blank areas on the map.
Yet, craniosacral therapists claim to “know” what is going on well enough to reliably deliver profound therapeutic effects. They believe it strongly enough to charge top dollar for it, too. That’s some serious overconfidence.
More than relaxing? Satisfaction guaranteed by autonomous sensory meridian response (weird euphoric head tingles)
Touch and close personal attention can be psychologically and even biologically profound. Mammals require touch for normal development,1314 and we don’t entirely outgrow that. But the appeal of “subtle” therapies like CST may owe a lot to something a little more specific and motivating, a strong sensory reward: the odd sensory sorcery of autonomous sensory meridian response (ASMR).
ASMR is a flush of euphoria and tingling around the head and neck. It’s triggered by things like attentiveness, a soft voice, quiet and repetitive actions, and interesting and gentle tactile stimulation (especially around the head). ASMR isn’t well understood, but it’s probably a sensory reward for grooming behaviour (in the same way that orgasms are an evolutionary incentive to reproduce).15 A CST session seems like a perfect ASMR-generating ritual, a grooming simulation fine-tuned to produce ASMR… decorated with a large superfluous narrative about cerebrospinal fluid.
Satisfaction guaranteed not by the manipulation of cerebrospinal fluid circulation, but by primate sensory neurology.
What do other osteopaths think?
Even Complementary Therapies in Medicine — a journal that is much friendlier to alternative therapies than mainstream scientific journals — published a review of the available research in 1999 and “found insufficient evidence to support craniosacral therapy.”16 Wouldn’t you expect such a journal to say just the opposite?
There hasn’t been any research supporting CST since then.
In 2006, craniosacral therapy was strongly questioned in yet another journal that you might expect to be friendlier to an alternative therapy, Chiropractic & Manual Therapies.17 Dr. Steve Hartman, a professor of anatomy at a college of osteopathic medicine, writes with much greater authority on this subject than I have:
Craniosacral therapy lacks a biologically plausible mechanism, shows no diagnostic reliability, and offers little hope that any direct clinical effect will ever be shown. In spite of almost uniformly negative research findings, “cranial” methods remain popular with many practitioners and patients.
Until outcome studies show that these techniques produce a direct and positive clinical effect, they should be dropped from all academic curricula; insurance companies should stop paying for them (and their willingness to do so is not evidence that CST works18); and patients should invest their time, money, and health elsewhere.
As a scientist in this age of evidence-based practice, I have grown frustrated in my dealings with the “cranial” faithful. As a group, evidence carries little weight with them.
Hartman, 2006, Chiropractic & Manual Therapies
Should patients buy craniosacral therapy?
Unproven therapies should never be sold to patients without acknowledging the uncertainties — it’s not ethical.19 More importantly, there’s a risk of harm: not from the therapy (in the case of CST), but from belief in a non-existent pathology.20
I can imagine a health care professional who sells CST but strictly limits her therapeutic predictions and is conspicuously humble. Such a therapist might integrate CST as one component of treatment, a relaxing touch therapy, hoping that it might have some other subtle benefits, but not promising or overselling them. The uncertainty would have to be clear to the patient.
That would be a responsible use of CST — presented with a grain of salt, and offered as just one component of therapy, not the centerpiece.
How many CST therapists actually practice in this way? In my experience, CST practitioners like this are basically unheard of. Most seem to be “true believers,” ideologically committed to the modality, unaware of the substantial scientific evidence that CST is ineffective, and not interested in it either.
CST practitioners are also extremely likely to integrate other dubious methods into treatment, especially “energy” medicine, like therapeutic touch and Reiki — pure vitalism (believe in a “life force”), and as intellectually immature as taking astrology seriously.
Can craniosacral therapy treat hydrocephalus?
Hydrocephalus is an excess of fluid around the brain, compressing it and causing all kinds of trouble, from headaches to confusion to seizures and worse. It is caused by birth defects, but it can also develop in adults. I got this question by email:
My wife has been struggling to regulate CSF flow as a result of her hydrocephalus. She has a programmable shunt and having a difficult time finding a good setting for her. A family member is “encouraging” me to pursue craniosacral therapy for her with the hope that it will improve her CSF flow. I am concerned it could have a negative effect and before asking her doctor wanted to find out more if I could. Is it possible it could help, and is there any risk that it will hurt?
While it’s unlikely to be directly harmful, the costs and any delay of legitimate treatment are significant.
And it has about as much chance of helping as I have of getting into Hogwarts.
Hydrocephalus is caused by physical obstruction of the CSF circulation, or by “relative obstruction” from having too much of the stuff (due to over-production or reabsorption failure). Many cases are complex and it’s impossible to be sure why it’s happening.
Hydrocephalus squeezes the brain. The skull cannot yield to a higher volume of increased cerebrospinal fluid, so the brain yields instead.
From a strictly evidence-based perspective, it’s theoretically plausible but extremely unlikely that hydrocephalus could be treated with CST. It’s plausible only insofar as CST manipulations are intended to have an effect on cerebrospinal fluid circulation and it’s not inconceivable that they do. But it’s extremely unlikely to be enough or the right kind of effect for this problem, because we know that by far the dominant CSF pump is respiratory,21 and we know that the effects of CST are certainly subtle (if they exist at all), and would simply be overwhelmed, like trying to stop the tide with a bucket.
And not all hydrocephalus is mechanical! There are multiple biological mechanisms by which CSF balance gets thrown off by over-producing or under-absorbing it. There’s absolutely no specific reason to believe that CST can touch those mechanisms at all, let alone therapeutically.
And so, even if CST actually does affect CSF circulation, it’s extremely unlikely to be able to compensate for the forces involved in acquired hydrocephalus.
That gives CST a lot of benefit of the doubt that it has not earned over the last few decades. If we don’t give it that, then any reasonable hope of treating hydrocephalus with CST just goes right out the window. When you consider CST’s long history of irresponsible claims that reach far beyond the science, the plausibility drops so low that I think it’s not even worth a shot — even for someone who can afford to throw money at serious long shots. CST would be peaceful and pleasant enough — little or no actual risk — but I think anyone would get more value out of good quality relaxation massage.
Do CST practitioners actually try to treat hydrocephalus?
The Upledger Institute says it’s “contraindicated” — a bad idea, potentially unsafe.22 It would be more honest to say, “It’s likely safe because it doesn’t do much in the first place, maybe nothing at all,” but alternative medicine never passes up an opportunity to imply its potency.23
A common problem with pseudoscientific therapies, however, is that practitioners are often ignorant of whatever passes for official standards and best practices. Or they just think they know better and strike out on their own, emboldened by the ahead-of-the-science vibe that filled the room, like obnoxiously strong incense, at their $3000 Level IVIXVXII certification course.
While treating hydrocephalus is not exactly a common claim, it only took me seconds of Googling to find examples of it. Is there an epidemic of it? No. Does it happen? Of course — this is a world where far more outrageous and dangerous quackery is actually common.
The good, the bad, and the ugly of craniosacral therapy
The good
- medical harm is extremely unlikely
- relaxing, pleasant, gentle
The bad
- harm to your wallet is inevitable, because it doesn’t work
- no plausible mechanism of action
- practitioners can’t agree on diagnoses
The ugly
- CST exists to solve a problem that doesn’t even exist
- practitioners tend to be “true believers” whose faith in CST is the tip of an iceberg of pseudoscientific beliefs, sometimes extending as far into the weeds as claims like the ability to treat hydrocephalus
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
Six updates have been logged for this article since publication (2008). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more
Like good footnotes, update logging sets PainScience.com apart from most other health websites and blogs. It’s fine print, but important fine print, in the same spirit of transparency as the editing history available for Wikipedia pages.
I log any change to articles that might be of interest to a keen reader. Complete update logging started in 2016. Prior to that, I only logged major updates for the most popular and controversial articles.
See the What’s New? page for updates to all recent site updates.
2021 — Explored the relevance of autonomous sensory meridian response in a small new section, “More than relaxing: satisfaction guaranteed by autonomous sensory meridian response (weird euphoric head tingles).”
2020 — New section, “Can craniosacral therapy treat hydrocephalus?” Also a science update, citing Haller.
2020 — Added a brief but important point of logic, about CST being a “solution in search of a problem.”
2019 — General editing from top to bottom.
2019 — Short new section comparing and contrasting beliefs about increase circulation of cerebrospinal fluid versus blood.
2016 — Added summary and good/bad/ugly points. Added a good new related reading link, and quoted from it a bit.
2008–2016 — Many unlogged updates.
2008 — Publication.
Related Reading
- “Fibromyalgia Meets Craniosacral Therapy,” John Quintner, FMperplex.com. A detailed history and analysis of “craniosacral therapy,” especially as it relates to treating fibromyalgia.
- “Craniosacral therapy and professional responsibility,” Flynn et al., Journal of Orthopaedic & Sports Physical Therapy, 2006. A clear, concise summary (for professionals) of the poor state of the science of craniosacral therapy, calling for advocates to “prove that it works, or move on.” The authors do a good job of putting CST in context, comparing and contrasting with other treatment methods.
- Use the Force! The myth of healing energy in massage and bodywork — Reiki, therapeutic touch, and other “energy medicine” methods are culturally rich but scientifically bankrupt
- The Complete Guide to Chronic Tension Headaches — A detailed, science-based tour of stubborn headache diagnosis and treatment, for both patients and professionals
- Psoas, So What? — Massage therapy for the psoas major and iliacus (iliopsoas) muscles is not that big a deal
- Spinal Subluxation — Can your spine be out of alignment? Chiropractic’s big idea has been misleading patients for more than a century
- Even the Best Scientific Studies Can Lie: The Case of Craniosacral Therapy, Jonathan Jarry, McGill.ca.
The major myths about massage therapy are:
- Massage increases circulation. Probably not… and definitely not as much as a little exercise.
- “Tightness” matters. The three most common words in massage therapy — “you’re really tight” — are pointless.
- Massage detoxifies. It’s actually the opposite, if anything.
- Massage patients need to drink extra water to “flush” the toxins liberated by massage.
- Massage treats soreness after exercise. Studies have shown only slight effects.
- Massage reduces inflammation. An extremely popular belief based mainly on a single seriously flawed study.
- Fascia matters. The biggest fad in the history of the industry.
- Scars and adhesions can be scraped away. Often uncomfortable, sometimes dangerous, always expensive and ineffective.
- The psoas muscle is a big deal. The most overhyped single muscle.
- Massage stimulates endorphins (natural opioid) and reduces cortisol (stress hormone). They do not.
- “Trigger points” are evidence-based. Actually, the science is seriously half-baked.
- Massage therapists have spooky palpation skills. No, it’s just ordinary expertise… and misleading.
The complete list of dubious ideas in massage therapy is much larger. See my general massage science article. Or you can listen to me talk about it for an hour (interview).
And massage is still awesome! It’s important to understand the myths, but there’s more to massage. Are you an ethical, progressive, science-loving massage therapist? Is all this debunking causing a crisis of faith in your profession? This one’s for you: Reassurance for Massage Therapists: How ethical, progressive, science-respecting massage therapists can thrive in a profession badly polluted with nonsense.
Notes
- “Manual therapy” refers mainly to massage, spinal manipulation, acupuncture, and many other methods and techniques for assessing and treating common musculoskeletal problems and injuries with hands and/or tools. Most of this is done to/for patients, so it is also sometimes called passive therapy as opposed to active (mainly exercise therapy). It exemplifies the best that alternative medicine offers — the time, compassion, and touch that medicine lacks — but it is also a pseudoscientific dumpster fire fueled mostly by faith that tissue can be “fixed.” What little good research exists shows modest medical benefits at best. The time required for it is costly, and the intensity of some methods means that there are some risks. Although mostly the domain of massage therapists and chiropractors, physical therapists are also surprisingly invested in it, and notorious for their dubious methods (e.g. ultrasound). And yet! There probably is a signal somewhere in all that noise. Rational practitioners can ethically offer more plausible techniques; and the power of touch, compassion, and novel sensations to inspire and comfort should not be underestimated. See Manual Therapy: What is it, and does it work? The science of "fixing" tissue with hands-on treatments like massage and spinal manipulation.
- Osteopathy is a confusing profession with colourful history, extremely diverse training and certification standards, and not much to unite practitioners except their focus on musculoskeletal health. Some osteopaths have true medical degrees, but that’s mostly in the United States and England. Most are lesser-trained alternative medicine practitoners, indistinguishable from chiropractors as far as most patients are concerned. For more information, see Reviews of Pain Professions.
- CST can traces its roots back to 18th century philosopher and scientist Emanuel Swedenbourg (1688–1772), who was well ahead of his time, but also made many mistakes of course (this was very early in the history of medical science). In particular, he was aware of the phenomenon of the pulsation of the brain. Andrew Taylor Still actually founded osteopathic medicine. Much later, American osteopath William Sutherland (1873-1954) took this further, and proposed many of the specific features of modern CST, particularly the notion that the dura mater is anchored to both cranium and sacrum and can transmit forces between the two — hence we have “craniosacral” therapy. He was the first person to claim to feel rhythmic shape change in the bones of the cranium, the “Primary Respiration,” and he thought it was the Key To Everything in human health (because of course he did). Upledger’s primary contribution was a refinement to that big idea: he suggested the mechanism, that cerebrospinal fluid pressure fluctuates with a cycle of production and resorption.
- Which, incidentally, is great marketing: portmanteaus of anatomical terminology co-opt the dignity of Latin. They sound formal and serious. But there’s no good reason outside of this treatment concept to blend the terms “cranial” and “sacral” — they have no other relationship in biology or medical science. There is no “craniosacral system” according to anyone but craniosacral therapists. The terms simply refer to the top and bottom of the central nervous system: head-to-tail therapy, in other words.
Obviously CST practitioners themselves attribute all kinds of problems to CSF stagnancy, especially medically unexplained symptoms for which medicine has no explanation or solutions. But no one outside the world of CST is aware of any common concern about CSF circulation. Certainly things can go wrong that involve CSF — infection, leakage, hydrocephalu — but these are quite specific and/or serious medical problems, and none of them are remotely relevant to the CST goal of manipulating CSF circulation.
This complete lack of any problem for CST to solve is in stark contrast to, say, manual lymphatic drainage — which may or may not work, but is at least intended to help with a specific medical proble — lymphedema, swelling in a limb. CST has no similarly clear purpose!
- Haller H, Lauche R, Sundberg T, Dobos G, Cramer H. Craniosacral therapy for chronic pain: a systematic review and meta-analysis of randomized controlled trials. BMC Musculoskelet Disord. 2019 Dec;21(1):1. PubMed 31892357 ❐ PainSci Bibliography 51863 ❐
This is a pseudoscientific review of other pseudoscience, with a completely untrustworthy positive conclusion that “significant and robust effects of CST on pain and function.” They “reviewed” ten extremely low quality studies. Jonathan Jarry writes, “If you don’t look up these individual trials, you won’t know just how bad they are.” One was not even a trial of CST, or published; two were actually negative; five had such glaring design flaws that they never should have been considered; another superficially adequate trial was so underpowered that the results had “error bars so large you could drive an entire cohort of participants through them.” Only a single study of the ten had the outward appearance of a trial worth reviewing, but a serious design flaw is apparent with even a little digging.
It is easy to find faults in scientific papers. Even good ones have major limitations. But it’s a matter of degree, and this is one of the most dramatic examples of “garbage in, garbage out” I have ever seen. There isn’t enough data here to review in any way, let alone meaningful statistical pooling (meta-analysis). And while it isn’t technically “evidence of absence” — there’s almost no actual “evidence” involved at all — the complete failure to produce credible positive evidence, despite a dramatic bias in favour of CST, is a kind of conclusion in itself.
See Jarry’s more detailed analysis: Even the Best Scientific Studies Can Lie.
- Downey PA, Barbano T, Kapur-Wadhwa R, et al. Craniosacral therapy: the effects of cranial manipulation on intracranial pressure and cranial bone movement. J Orthop Sports Phys Ther. 2006 Nov;36(11):845–53. PubMed 17154138 ❐
This is a study of the effect of craniosacral therapy on rabbit skulls and their cerebrospinal fluid circulation. The researchers found that “low loads of force, similar to those used clinically when performing a craniosacral frontal lift technique, resulted in no significant changes in coronal suture movement or intracranial pressure in rabbits.”
If you can’t move rabbit skull bones or change their intracranial pressure, it’s safe to assume that you probably can’t do it to humans either — and without that mechanism in good working order, craniosacral therapy has no basis at all. The researchers concluded: “These results suggest that a different biological basis for craniosacral therapy should be explored.” But, of course, a “different biological basis” for craniosacral therapy has never even been suggested, let alone tested.
- Dreha-Kulaczewski S, Joseph AA, Merboldt KD, et al. Inspiration is the major regulator of human CSF flow. J Neurosci. 2015 Feb;35(6):2485–91. PubMed 25673843 ❐
There has never been any significant controversy over whether cerebrospinal fluid actually moves around (only whether or not it’s palpable or can be manipulated, with or without effect/benefit). This is an MRI study of how the fluid circulates, and it confidently concludes it’s pumped every time you take a breath in: “The present results unambiguously identify inspiration as the most important driving force for CSF flow in humans.”
This strongly suggests that the rhythm CST therapists claim to be able to feel is exactly in sync with respiration. Not so exotic! This is just one paper, and it isn’t necessarily the last word about the mechanism of CSF circulation, but it does strongly suggest that there is indeed a CSF circulation phenomenon to explain, and it’s powered in a straightforward way that probably can’t be significantly manipulated by any means other than holding your breath.
- Increased intracranial pressure gets serious with small increases in the fluid volume — only about a 100mL. There are well-described mechanisms that the body uses to try to compensate for increasing intracranial pressure: see the Monro-Kellie hypothesis. Expansion of the cranium is not one of the mechanisms that relieves pressure.
- Wirth-Pattullo V, Hayes KW. Interrater reliability of craniosacral rate measurements and their relationship with subjects' and examiners' heart and respiratory rate measurements. Phys Ther. 1994 Oct;74(10):908–16; discussion 917–20. PubMed 8090842 ❐
The first test of the claim that craniosacral therapists are able to palpate change in cyclical movements of the cranium. They concluded that “therapists were not able to measure it reliably,” and that “measurement error may be sufficiently large to render many clinical decisions potentially erroneous.” They also questioned the existence of craniosacral motion and suggested that CST practitioner might be imagining such motion. This prompted extensive and emphatic rebuttal from Upledger.
- Moran RW, Gibbons P. Intraexaminer and interexaminer reliability for palpation of the cranial rhythmic impulse at the head and sacrum. J Manipulative Physiol Ther. 2001 Mar-Apr;24(3):183–190. PubMed 11313614 ❐
“Palpation of a cranial rhythmic impulse (CRI) is a fundamental clinical skill used in diagnosis and treatment” in craniosacral therapy. So, researchers compared the diagnostic methods of “two registered osteopaths, both with postgraduate training in diagnosis and treatment, using cranial techniques, palpated 11 normal healthy subjects.” Unfortunately, they couldn’t agree on much: “interexaminer reliability for simultaneous palpation at the head and the sacrum was poor to nonexistent.” Emphasis mine.
- Haller H, Lauche R, Cramer H, et al. Craniosacral Therapy for the Treatment of Chronic Neck Pain: A Randomized Sham-controlled Trial. Clin J Pain. 2016 Sep;32(5):441–9. PubMed 26340656 ❐ PainSci Bibliography 54129 ❐
This study reports that craniosacral therapy is an effective treatment for chronic neck pain, compared to “light touch,” in a few dozen patients.
Before I comment on the scientific value of this paper, I’d like to point out that it’s poorly written. It’s a mess. Just sayin’.
And the scientific value is probably nil. It’s in that awkward grey zone between good science and overt pseudoscience. The abstract begins with a glaringly disingenuous exaggeration of the scientific context — there is no credible “growing evidence” that craniosacral therapy works! Making such a claim betrays a strong bias that is clear throughout the paper, numerous examples of highly motivated reasoning and ideological dedication to CST. This experiment was obviously conducted by researchers fishing for confirmation that CST works, the kind of research that finds what it’s looking for and that more objective researchers never seem to be able to replicate.
The results were technically positive and statistically significant, but also clinically unremarkable and attributable to many possible confounding factors rather than “because CST works.” Even if the results could be accepted at face value, it wouldn’t validate the mechanisms of CST, which are just as dubious as ever. And we know that statistical significance validity, poor at the best of times, is even worse when testing highly implausible claims (see Pandolfi 2014). Either CST only appeared to outperform a sham, thanks to bias-powered mistakes, or it outperformed it only because the CST treatment ritual had more robust nonspecific effects.
And yet even if the results could be trusted, they would be underwhelming, and the authors themselves concede that "the effect sizes are comparable to those of neck pain guideline treatments" and "they "found comparable effects in blinded patients with respect to sham." This is what we see with essentially all passive interventions: a modest and transient effect at best, likely attributable to a combination of p-hacking and non-specific effects common to virtually any pleasant therapeutic interaction.
The authors believe (because of course they do) that the effect they measured "more than likely cannot be explained exclusively by nonspecific treatment effects," and it’s largely based on the premise that the signal is legit in the first place … a benefit of the doubt I am not willing to extend to an obviously biased test of a highly implausible treatment.
This study will be undoubtedly be touted by CST practitioners as proof that CST works, but it is no such thing without replication that it will almost certainly never get. Remember, there are lots of “positive” studies of homeopathy and acupuncture too … and we know how much that means.
- Montagu A. Touching: the human significance of the skin. 3rd ed. Harper & Row; 1986.
An impressive and well-documented examination of the importance of touching to growth and development, health and well being. Although several other books have been written about the touch since, Montague’s is arguably still the best.
- Cascio CJ, Moore D, McGlone F. Social touch and human development. Dev Cogn Neurosci. 2019 02;35:5–11. PubMed 29731417 ❐ PainSci Bibliography 52553 ❐
The entire paper is relevant, but for an excellent overview of the effect of touch on growth and development in particular, see section 4, “Social touch over the human lifespan.”
- This is hypothetical but plausible. In any case, the claim isn’t required to make the point that ASMR is pleasurable and motivating by definition, and therefore likely more than “just” a feeling — it does have predictable effects on mood and physiology, and “may have therapeutic benefits for mental and physical health” (Poerio).
- Green C, Martin CW, Bassett K, Kazanjian A. A systematic review of craniosacral therapy: biological plausibility, assessment reliability and clinical effectiveness. Complement Ther Med. 1999;7(4):201–207.
From the abstract: “This systematic review and critical appraisal found insufficient evidence to support craniosacral therapy. Research methods that could conclusively evaluate effectiveness have not been applied to date.”
- Hartman SE. Cranial osteopathy: its fate seems clear. Chiropractic & Manual Therapies. 2006;14:10. PainSci Bibliography 56267 ❐ A short but clear, compelling, and strong critique of cranial osteopathy. As an osteopath himself, Dr. Hartman’s opinion carries considerable weight, and he writes well.
- Ingraham. Insurance Is Not Evidence: Debunking the idea that “it must be good if insurance companies pay for it”. PainScience.com. 1325 words.
- Ethics 101: making risks and limitations of therapy clear to the patient before they agree to it or pay for it is called “informed consent,” a well-defined necessity for the ethical delivery of any health care product or service.
- Flynn TW, Cleland JA, Schaible P. Craniosacral therapy and professional responsibility. J Orthop Sports Phys Ther. 2006 Nov;36(11):834–6. PubMed 17154136 ❐ “It is also imperative that physical therapy professionals who perform cranial techniques do not communicate to patients disproved concepts of moving cranial sutures or balancing cranial rhythms. This language is disingenuous and may lead to creating disability in our patients by providing the perception that there is some sort of structural deformity in their body and implying that they are ill.”
- Dreha-Kulaczewski 2015, op. cit. Again, these results “unambiguously identify inspiration as the most important driving force for CSF flow in humans.”
- “Official” insofar as the Upledger Institute has publicly stated it:
If the client’s hydrocephalus is not controlled by a shunt (a little tube placed in the ventricles to drain CSF in order to control CSF pressure), or if the shunt is not working properly, then CranioSacral Therapy is contraindicated. If the cause is unknown, it is better to take the safe route and not treat.
Declaring that a treatment method might be unsafe is a classic gambit in alternative medicine. It implies that it’s potent enough to be dangerous. Why emphasize the need for “responsibility” if there isn’t “great power”?
For instance, it’s routine for homeopaths to issue warnings about the misuse of their ridiculous nostrums, which is why skeptics have demonstrated the harmlessness of overdose. Another good example: there’s a common belief among massage therapists that stimulating an acupuncture point in the ankle can sabotage a pregnancy — such power! It’s nauseating when massage therapists try to communicate sophisticated diligence by highlighting their avoidance of this “risk.”