Baxter’s Neuritis versus Plantar Fasciitis
A rare nerve entrapment that can explain some stubborn cases of “plantar fasciitis”
Baxter’s neuritis is one of several possible causes of plantar fasciitis… sort of. You could consider it a separate condition that mimics plantar fasciitis… or you could say that it’s just one of several possible causes of heel pain that can be tricky to tell apart.
Plantar fasciitis is a common overuse injury of the foot, notoriously stubborn, which plagues runners and people who have to stand on hard surfaces at work. It’s usually described as a kind of tendinitis of the arch, but that’s only one of several possible factors: like Baxter’s neuritis, heel spurs, calcaneal fatigue, and arch muscle trigger points. The name “plantar fasciitis” implies too much, and the condition should probably just be called plantar heel pain.1
Baxter’s neuritis, AKA distal tarsal tunnel syndrome, is entrapment of the first branch of the lateral plantar nerve. It’s rare, which is probably the best reason to regard it as its own condition, rather than a cause of plantar fasciitis. But when it occurs, it is often mistaken for plantar fasciitis.2 Podiatrist Dr. Patrick DeHeer:
Through my 23 years of practice, I often think of the old adage, “When you hear hoof beats, think horses, not zebras.” I consider myself a very good diagnostician. I base my diagnoses on comprehensive history and physical examination. However, there are times when the patient is not progressing as expected and those “hoof beats” are actually zebras. One such case is heel pain from Baxter’s neuritis, which is entrapment of the first branch of the lateral plantar nerve.
So although rare overall, it’s probably common enough among people with stubborn heel pain to be well worth considering.
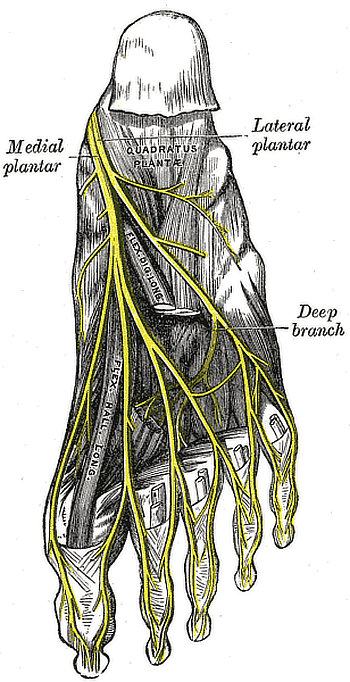
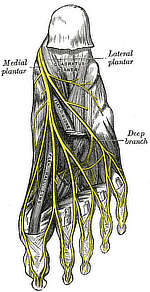
Gray’s Anatomy, Plate 833, nerves of the bottom of the foot
Nerve entrapment primer
Neuropathy is one of the three basic types of pain (with nociceptive and “other”). It seems obvious that pinching nerves will hurt, but in fact nerve trunks are surprisingly tolerant of physical stress. They have to be. As a general rule, concerns about “nerve pain” are overblown in our society, partly driven by advertisements for drugs to treat neuropathy.3
It takes more severe and persistent mechanical stress to piss off a nerve than most people realize. There are probably also subtle biological vulnerabilities that make us more prone to actually feeling a nerve pinch. For instance, a vitamin B12 deficiency might make an otherwise harmless entrapment into a real problem. There’s an excellent possibility that lots of people have lots of minor nerve entrapments all the time, but they are asymptomatic.
However, sometimes nerves get pinched harder, for longer, and/or the biological vulnerability is higher for some reason, and the result is peripheral neuropathy, which mostly causes pain, tingling, numbness, and weakness in the tissues supplied by the nerve. Some nerves are infamously more likely to get pinched than others, just because of their anatomical situation.
“Who thought it was a good idea to put this nerve here?!”
Baxter’s neuritis is probably a phenomenon because of the relatively vulnerable physical predicament of this nerve. As with everything else about plantar fasciitis, the main rehab challenge is that it’s so hard to reduce physical stresses in the foot without anti-gravity technology.
The lateral plantar nerve passes through the “tarsal tunnel,” which is similar the more famous carpal tunnel of the wrist, and Baxter’s neuritis could indeed be considered “the carpal tunnel syndrome” of the foot. The nerve then takes a sharp turn at the inside of the heel bone and travels diagonally across the arch towards the littlest piggy. It is the largest nerve that is more or less right in the arch of the foot. It’s the arch nerve.
When troubled, Baxter’s neuritis causes pain much like plantar fasciitis, but with some distinctive differences (which are all typical of neuropathy rather than tendinopathy):
- There’s minimal morning pain — a classic plantar fasciitis symptom. It tends to get worse as the day goes on instead.
- In addition to pain, there are also often weird sensations, numbness, and tingling, usually on the bottom-inside of the heel.
- And it hurts directly when touched, including the inside of the heel, where there is no plantar fascia.
Does any of that sound like you? If so, confirming or rejecting this diagnosis is a high priority: go see a neurologist.
Tarsal tunnel syndrome — a close cousin
Tarsal tunnel syndrome is closely related to Baxter’s neuritis, but involves the impingement of nerves just a little higher up, on the inside of the ankle, where they pass through the tarsal tunnel. Nerve entrapment at this location is more truly “the carpal tunnel syndrome of the foot” than Baxter’s.
Just like most cases of Baxter’s, TTS will be more obviously “nervy” than plantar fasciitis. But while Baxter’s affects just the arch, and thus is more easily mistaken for plantar fasciitis, TTS usually causes diffuse symptoms all over the bottom of the foot, making it much less likely to be mistaken for plantar fasciitis.
Also, there’s a very easy test for tarsal tunnel syndrome: firmly tap behind the inside ankle bone. If your symptoms flare right up, bingo! This is called the “tarsal tap” test, a quick and easy way to confirm or deny tarsal tunnel syndrome.
An entrapped nerve does not necessarily mean you need surgery
When an entrapped nerve is confirmed as the cause of a chronic pain problem, we all tend to assume that it needs to be cut free, like freeing a dolphin from a fishing net. And that certainly can work.
But it doesn’t always work, and it may not be necessary. The conservative approach to treating nerve entrapments, in broad strokes, goes like this:
- Give it a rest, of course. Tissues rarely calm down and heal without being given a bit of an opportunity. This can be a tall order with foot problems, but that’s life — it’s the body parts we need the most that get hurt the most. Read more about the art of resting for rehab.
- Reduce your vulnerability and sensitivity to nerve entrapment generally. That is, try to identify and eliminate all factors that could be contributing not to the trap itself, but how much the entrapment hurts. This boils down to a broad-spectrum effort to improve your health and fitness in every possible way, starting with the lowest-hanging fruit. “A rising tide lifts all boats.”
END OF FREE INTRODUCTION
This article is an excerpt of my popular plantar fasciitis tutorial, a 86,000-word e-book, regularly updated for over a decade, that reviews the nature of the beast in extreme detail, and every treatment option. Sales of e-books are how PainScience.com has been producing accessible, science-based advice for painful problems since the early mid-2000s. You can buy the whole book here, or read the free introduction first.

Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help
| company | PainScience.com |
|---|---|
| owner | Paul Ingraham |
| contact | 778-968-0930 |
| refunds | 100%, no time limit +Customers are welcome to ask for a refund months after purchase — I understand that it can take time to decide if information like this was worth the price for you. |
| more info | policies page ❐ |
| payments |
- What do you get, exactly? An online tutorial, book-length (68 chapters). Free updates forever, read on any device, and lend it out. E-book only! MORE
- Secure payment takes about 2 minutes. No password or login: when payment is confirmed, you are instantly granted full, permanent access to this page.MORE
- Collect them all. Get an “e-boxed” set of all 10 PainScience.com tutorials, ideal for pros … or patients with a lot of problems.MORE
Q. What am I buying? Is there an actual paper book?
A. Payment unlocks access to 61 more chapters of what is basically a huge webpage. There is no paper book — I only sell book-length online tutorials. This format is great for instant delivery, and many other benefits “traditional” e-books can’t offer, especially hassle-free lending and updates. You get free lifetime access to the always-current “live” web version (and offline reading is easy too).

Read on any device. Lend it out. New editions free forever.
Q. I just don’t like reading on the computer! Is there any way around that?
A. The design and technology of the book is ideal for reading on tablets and smart phones. You can also print the book on a home printer.
Q. Can I lend the tutorial out?
A. Yes! Feel free to lend your tutorial: I do not impose silly lending limits like with most other ebooks. No complicated policies or rules, just the honour system! You buy it, you can share it. You can also give it as a gift.
Q. Is it safe to use my credit card on your website?
A. Literally safer than a bank machine. Payments are powered by Stripe, which has an A+ Better Business Bureau rating. Card info never touches my servers. It’s easy to verify my identity and the legitimacy of my business: just Google me [new tab/window].
Q. I can really get a refund at any time?
A. Yes. All PainScience.com ebooks have a lifetime money-back guarantee.
Q. Why do you ask for contact information?
A. To prevent fraud and help with order lookups. You aren’t “subscribing” to anything: I never send email to customers except to confirm purchases.
Q. Can I buy this anywhere else? Amazon?
A. Not yet. Maybe someday.
See the “fine print page” for more about security, privacy, and refunds. No legalese, just plain English.
Save a bundle on a bundle
The e-boxed set is a bundle of all 10 book-length tutorials for sale on PainScience.com: 10 books about 10 different common injuries and pain problems. All ten topics are (all links open free intros in a new tab/window): muscle strain, muscle pain, back and neck pain, two kinds of runner’s knee (IT band syndrome and patellofemoral pain), shin splints, plantar fasciitis, and frozen shoulder. (Headache coming soon, fall of 2019.)
Most patients only need one book, because most patients have only one problem. But the set is ideal for professionals, and some keen patients do want all of them, for the education, and for lending to friends and family. And, of course, you do get a substantial discount for the bulk purchase. But no rush—complete the set later, minus the price of any books already bought. More information and purchase options.
Keep reading for free! The book page has a substantial free introduction, and there are some other related free articles on PainScience.com:
- EXCERPT Plantar Fasciitis Patients Have Thick Soles
- Is Running on Pavement Risky? — Hard-surface running might be a risk factor for running injuries like patellofemoral pain, IT band syndrome, shin splints, and plantar fasciitis
- Are Orthotics Worth It? — A consumer’s guide to the science and controversies of custom orthotics, orthopedic shoes, and other allegedly corrective foot devices
- Massage Therapy for Tired Feet (and Plantar Fasciitis!) — Perfect Spot No. 10, in the arch muscles of the foot
- Does barefoot running prevent injuries? — A dive into the science so far of barefoot or minimalist “natural” running
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
2020 — Added an article summary.
2019 — Publication.
Notes
- Riel H, Cotchett M, Delahunt E, et al. Is 'plantar heel pain' a more appropriate term than 'plantar fasciitis'? Time to move on. Br J Sports Med. 2017 Nov;51(22):1576–1577. PubMed 28219944 ❐
“We propose the term ‘plantar heel pain’ to describe the condition of pain under the heel when no differential diagnoses are indicated and until further research is undertaken to arrive at a clear understanding of the appropriate terminology and associated diagnostic criteria.”
The authors quite correctly point out that there are several possible causes of the condition that have nothing to do with the plantar fascia, and none of them correlate cleanly with symptoms. So an imprecise label is really the only honest one.
See also: one-minute video summary of this paper.
- Ferkel E, Davis WH, Ellington JK. Entrapment Neuropathies of the Foot and Ankle. Clin Sports Med. 2015 Oct;34(4):791–801. PubMed 26409596 ❐ “Distal tarsal tunnel syndrome results from entrapment of the first branch of the lateral plantar nerve and is often misdiagnosed initially as plantar fasciitis.”
- Ingraham. Neuropathies Are Overdiagnosed: Our cultural fear of neuropathy, and a story about nerve pain that wasn’t. PainScience.com. 2879 words.
There are 232 more footnotes in the full version of the book. I really like footnotes, and I try to have fun with them.
Jump back to:
The introduction
Paywall & purchase info
Table of contents
Top of the footnotes
Paying in your own (non-USD) currency is always cheaper! My prices are set slightly lower than current exchange rates, but most cards charge extra for conversion.
Example: as a Canadian, if I pay $19.95 USD, my credit card converts it at a high rate and charges me $26.58 CAD. But if I select Canadian dollars here, I pay only $24.95 CAD.
Why so different? If you pay in United States dollars (USD), your credit card will convert the USD price to your card’s native currency, but the card companies often charge too much for conversion — it’s a way for them to make a little extra money, of course. So I offer my customers prices converted at slightly better than the current rate.
refund at any time, in a week or a year
call 778-968-0930 for purchase help