Alternative Medicine’s Choice
What should alternative medicine be the alternative to? The alternative to cold and impersonal medicine? Or the alternative to science and reason?
Modern health care consumers are faced with a hair-raising dilemma: the hard choice between medical care that is often overconfident, cold, and tangled in red tape,1 versus the so-called “alternative” options that mostly do not work, but come with plenty of dangerous nonsense.2 It’s a poor choice — and often no choice at all, especially for patients with chronic pain, who mostly can’t get good help from either source.
Acupuncture is the ultimate in alternative medicine, allegedly proven by countless studies — most of which are poor quality and show only trivial benefits. See Does Acupuncture Work for Pain?
I quit! My own departure from alternative medicine
I am so concerned by some (not all) of what passes for health care in complementary and alternative medicine (CAM) that I gave up my credentials as a Registered Massage Therapist at the beginning of 2010,3 and I have moved on to greener pastures. I am an alt-med apostate — one of the very few.
I mainly quit because I wasn’t proud of being an “alternative” health care professional. I quit because there is no realistic hope of redefining alternative health care as simply the “warm and friendly” alternative to big and institutionalized medicine — it’s a lovely idea, but it’s never going to happen. I quit because the anti-scientific character of alternative medicine is well-established.4 The aggressive “integration” of alternative medicine into medical schools and hospitals is a hostile takeover.
However, for the record, alternative medicine didn’t have to turn out that way.
Alternative medicine could have grown-up to be something different and better than it is. And for individual ethical professionals, alt-med still doesn’t have to be that way. Being an alternative health professional can still be mainly about better bedside manners — spending more time with people, and offering a few of the more plausible and harmless treatment options, rather than pushing a bewildering array of dubious and unproven “miracle cures” on people.
Should we keep an open mind about astrology, perpetual motion, alchemy, alien abduction and sightings of Elvis Presley? No, and I am happy to confess that my mind has closed to homeopathy in the same way.
Mike Baum, The dangers of complementary therapy, Breast Cancer Res. 2007; 9(Suppl 2): S10
Mainstream medicine: impersonal and institutionalized
People love to hate “mainstream” medicine. Why? Simple: because it’s largely institutionalized. Indeed, what bothers people has much more to do with the institutionalization of care than with medicine itself, or medical science. Most large organizations, if they were people, would be assholes.
This isn’t just an abstract gripe! There are good reasons to suspect that dysfunctional healthcare organizations can actually directly make people unhealthier, with an inversion of the placebo effect: nocebo.5 That is, they can probably make people worse rather than better, much like a careless individual professional can.6
“An organization acting as a nocebo could create negative experiences along the patient’s care pathway, possibly exacerbating their symptoms and worsening their clinical condition.”
I’ve encountered many organizations that seemed likely to act like nocebos.
Like many alternative health care professionals, I was originally inspired to pursue my career by some poor care I received from doctors — or so I thought. I have since come to understand that most doctor bashing is deeply unfair, routinely rooted in patient’s fear and pain, and in ignorance of the high-stakes, no-win situations that doctors face every day. The training and clinical experience doctors obtain deserves respect, and — however unwise it may be — their infamous arrogance is justified in many ways. The good doctors I know are my role models.
Those professionals are the first to admit that health care systems are in trouble around the world. Consider the increasingly grim outlook for the National Health Service in the UK. Jonathon Tomlinson, a London GP, writes:
I believe that the corporatisation of healthcare is dehumanising. By this I mean that real, whole people living with their hopes and worries, ideas and expectations, are broken down by the process of corporatisation into biological parts not for diagnosis and treatment but so that they can be measured and converted into profits. We are far more than the sum of our biological parts; we also have relationships with our past and future, our family and friends, our work and environment, our country and our home. We are irrational and passionate as well as calculating and objective; we need kindness, affection and understanding as well as diagnoses and treatments. And healthcare is far more effective when this is taken into account.
Patients not Profits, by Jonathon Tomlinson
People are frightened to go the hospital. Many people have real horror stories about hospital experiences.7 Tragically, there’s more evidence every day that many surgeries — especially orthopedic surgeries — simply do not work and many more still have not been properly tested, exposing countless patients to serious unnecessary risks.8 Statistics about illness and surgical damage caused by doctors and hospitals seem like something from a third world country.910 Here in litigious North America, we have an epidemic of medical malpractice lawsuits.11 Even while our economy groans under the weight of common problems like back pain, a few doctors have proven that the majority are appallingly incompetent at treating musculoskeletal conditions,12 and cannot offer nutritional advice.13 And the litany of problems with universal health insurance here in Canada, or with for-profit medical institutions in America, is overwhelming. Pharmaceutical companies have perpetrated some of the largest health care frauds in medical history, and continue to do so.
The roots of all this evil are an impersonal, institutionalized approach to healthcare, and of course the profit motive.
Mainstream medicine: also hung up on the biomedical model
Success hides many sins. The triumphs of science and scientific medicine have a downside, and account for the common perception of medicine as “arrogant” or at least overconfident. Basically, it’s just gotten a bit out of hand. From the front cover of the July issue of The Lancet:15
“A radical shift of life sciences funding priorities, away from the biomedical bubble and towards the social, behavioural, and environmental determinants of health, is now needed.”
Some people have been calling for and working towards that radical shift for decades. Dr. Patch Adams comes to mind. In the same era, Dr. George Engel defined the biopsychosocial model of healthcare directly as an antidote to the rather cold and technical profession that medicine had become in the mid 20th Century.16
In 2018, Jacob Stegenga argued in his superb book Medical Nihilism that medicine has gotten a bit out of hand, and we should be more skeptical of it for the right reasons — not because we object to scientific medicine in principle, but because the science shows that too many common medical treatments do more harm than good.17 The biomedical model clearly isn’t all wrong, and indeed much about it is so right we should actually double-down on it (e.g. vaccination!). We definitely do not need a “radical shift” away from its strengths. Of course.
However,
No one needs that “radical shift” more than pain patients! But many others too. And when a pendulum needs to be swung, it’s often necessary to push away from where it’s been, to vigorously repudiate the past.
Tragically, alternative medicine could easily have inspired/shamed mainstream medicine into that important “radical shift”, but instead it’s done nothing but drive ever deeper into left field. It has only paid lip service to “social, behavioural, and environmental determinants of health,” while being much more truly defined by and deeply invested in snake oil and pseudoscience …
Alternative medicine: hung up on pseudoscience and anti-science
It was never a foregone conclusion that the “alternative” to medicine was going to be hostile to medicine, and anti-science. It was not inevitable that it would be all about homeopathy, Reiki, supplements and superfoods, detox quackery and toxic positivity, multi-level marketing, rejecting vaccines and denying germs, and generally never missing a chance to trash-talk doctors and anything “mainstream” or “allopathic.”
Such things did not have to be the “alternatives.” History didn’t have to go that way.
Alt-med could always have been, and should have been, just … slower, gentler, more personal care. We know that chronic pain patients benefit from that.18
It never had to be the alternative to what’s good in medicine. It could just have been an alternative to the hurried and cold bedside manner of many doctors. (“Not all doctors,” of course.19)
Despite efforts to rebrand alternative medicine as “complementary” and “integrative,” it has not turned out to have that character at all. CAM does not play well with others. A great many CAM practitioners are aggressively anti-scientific, picking fights with medicine and going for the jugular, treating it like a dangerous and contemptible enemy. And this is the main reason I got out. Sometimes CAM attacks doctors and medical care for some of the right reasons — they do exist, of course — but mostly for the wrong ones.
Naturopathic doctors in North America are trained well enough to know better,20 but still routinely sell products and services of dubious value, in league with a supplements and “natural” medicines industry that is almost as profitable and actually much more corrupt and dishonest than their “Big Pharma” counterpart.21 Homeopathic remedies in particular have been proven to be ineffective over and over again,22 and they have suffered serious public relations damage from exposés like the 2006 BBC story about dangerous anti-malarial substitutes.23 For the last twenty years, acupuncture has failed one fair scientific test after another,24 like the recent inability of acupuncturists to treat back pain in a particularly well-designed German study25 — yet acupuncture persists as a profession as if this research never happened. Doctors of traditional Chinese medicine, now popular in the west, continue to rely far too heavily on a variety of unproven folk remedies as if they were effective simply by virtue of being popular in China for a long time.26
In the physical therapies, the profession of chiropractic remains popular but the value of the profession’s services remain controversial. I avoid criticizing chiropractors directly on this website, due to legal concerns.27 Questioning chiropractic is better left to heavyweight experts and organizations.28 Training standards for massage therapy are all over the map; even here in BC, where massage therapists are trained quite rigorously,29 my own colleagues still routinely promote scientifically questionable ideas to patients (see sidebar). And a dizzying variety of superstitious sub-disciplines like craniosacral therapy, reflexology, and therapeutic touch and Reiki — fringe therapies that have failed to prove their efficacy despite many fair tests.30
In general, CAM practitioners are not the humble alternative to doctors — indeed, they generally seem to think much too highly of their training and abilities31 and suffer from “healer syndrome.”32 These practices and attitudes constitute a clear and present danger to the health of patients, and to their pocketbooks. Journalist and chronic pain patient Paula Kamen brilliantly exposes them for what they are in “Mind-Wallet Connection,” a chapter of her brilliant book, All in My Head, where she describes a tragicomic series of failed attempts to cure her nasty, chronic migraine with alternative therapies:
I was becoming turned off by what I saw as a lackadaisical attitude on the part of many healers. They had all the time in the world to follow “the mystical course of nature.” Just as no neurologist had ever admitted to me, “I don’t know,” none of them had said, “Well, you’ve given this enough of a try. You can stop these twice-weekly sixty-dollar visits.” If I didn’t stop these sessions, they would go on indefinitely, and we would grow old together.
All in My Head, by Paula Kamen, p. 191
Alternative medicine’s legal aggressiveness
Perhaps the most dire of alternative medicine’s faults is that it is so easy to hurt its feelings. Practitioners are notoriously intolerant of criticism. They are so thin-skinned that they are legally aggressive, and constantly equate legitimate criticism with slander and libel.
It’s childish. It’s small-minded bullshit. But it’s dangerous small-minded bullshit.
A savvy PainScience reader noticed a well-known manual therapy33 brand making blatantly extraordinary claims of healing prowess on their posh, slick website. He went looking for critique, and found nothing at all, not even here on PainScience.com — well-known for debunking and my alleged “negativity.” So he wrote to ask:
How do they get away with that? How can a significant brand in healthcare be so well-insulated from criticism?
Simple: because it’s legally dangerous to criticize brands in general, and even worse in this field, where bullshit abounds and skins are thin.
About half the serious anti-quackery activists I know have been sued at least once, and nearly all have been threatened or significantly harassed in some way. The danger is real. It doesn’t matter how right you are or how ridiculous the legal claim is: it’s expensive to fend off a determined SLAPP — strategic lawsuit against public participation — because that’s the whole point of them.34
The successful snake oil brands also excel at creating social media echo chambers, where the only people tuned in are the “true believers” and a discouraging word is never permitted, swarms of the faithful who will gleefully attack anyone who challenges their hive of dogma. I know several people who make a hobby of being voices of reason in such places, but usually all that comes of it is a quick block, their comments deleted. The idea is that such interventions are for the benefit of less militant observers — they witness someone disagreeing for reasonable reasons, and they might start to notice the problems with the brand.
Maybe. I applaud the effort, but I would rather stick my hand in a blender than be that kind of activist myself. I’ll stick to reviewing therapy claims in principle, rarely pointing at specific brands, or only quite strategically chosen ones (like ones that already have much more serious problems than critical bloggers). Most educated people already know the major examples anyway…and/or they can easily pick out the red flags themselves.
Have a look at John Oliver’s comedic reporting on SLAPP suits. It’s more fun than mine (obviously).
The shame of medical care
Like community policing or town meetings, house calls and humane, personal, socially interactive medical care has nearly disappeared from civil society. Such qualities are more likely to be found in places we consider “primitive” or “underdeveloped” because they lack adequate facilities — yet they may well be friendlier. The voice of Dr. Patch Adams, the most prominent medical spokesman for a “nicer” kind of medical care,35 has been completely drowned out. The failure to transcend bureaucracy and to be more about people than machines and money is the true shame of modern medicine.
Alternative health care, therefore, should be all about spending time with patients, listening to them, being personal with them. Alternative health care should be to mainstream medicine what small-scale organic farming is to industrialized farming.
But it isn’t. Instead, alternative health care has firmly established itself as the alternative to scientific health care. The message our industry sends out to the public is: “We’ll sell you whatever the doctors disapprove of. We’ll tell you what you want to hear. We’ll sell you ideas and potions that you’ll enjoy believing in, and we won’t spoil the experience with any boring, depressing science.”
But science is not the enemy. The enemy in medicine is institutionalization of care: red tape, chronically overwhelmed doctors and nurses, “factory” medicine. That is what alternative medicine should be the alternative to.
Science is good!
Science is not meant to cure us of mystery, but to reinvent and reinvigorate it.
Dr. Robert Sapolsky, from his classic book, Why Zebras Don't Get Ulcers
Science is a pretty good system for slowly but surely revealing all that is true in nature. However strange or difficult to understand, whatever actually is can sooner or later be understood as a part of the natural world — there is no such thing as “paranormal,” for, if it exists, it is normal.
Being anti-science is like being anti-honesty.
And science is not guilty by association with bad things that some people do with science.
I can appreciate the confusion, though, among alternative health care professionals and consumers alike. The “bad guys” try to use science all the time to defend ethically dubious practices. As long as tobacco companies and polluting industries continue to claim that “studies show” that they are innocent, it’s going to be hard to shake the impression that science is guilty by association. As long as technology continues to be used so disastrously to make war, it will be easy to think that scientists are the baddies.
And it’s not helping that politicians now reflexively refer to “the science” without ever actually understanding it or properly referencing it. In fact, science tends to get co-opted by practically anyone who wants to seem legit for the duration of a sound bite: even the flakiest of flakes will greedily cite a scientific study that seems to support their ideas,36 only to turn around and ignore and attack science the moment it clashes with their ideology.37 Talk about a fair weather friend!
In alternative medicine, hypotheses function more as fixed beliefs, and there is no study that can invalidate them. No matter how many times a hypothesis fails, the worst that happens is a call for more research.
Dr. Peter Lipson, for ScienceBasedMedicine.org
Just because science and poor medical care often seem to be mentioned in the same breath does not mean that they are actually the same thing, or that the shame of medical care is also the shame of science. On the contrary, just as alternative health care professionals have a lot to answer for in their rejection of science, doctors are also guilty of abusing and ignoring relevant scientific evidence.38 Many doctors do not “practice what they preach.” While this is defensible — doctors are human too, and should not have to paragons of virtue in order to practice medicine — it is a neglected issue.
My simple, unlikely prescription for complementary and alternative medicine
It will never happen, but … my prescription for alternative medicine is simply to embrace the science and embrace the client. Focus on spending time with patients discussing rational, science-based clinical options. Be more personal than most doctors have the opportunity to be. Be the alternative to institutionalized care. But also learn and promote the science of medicine!
In other words, be compassionate and attentive not only to your patients, but to your colleagues in mainstream medicine as well. In particular, don’t try to claim that alternative medicine has some kind of a monopoly on compassionate, attentive care — almost everyone in health care really wants to help, and is doing the best they can with the resources they have. Work with them.
The notion that only those who preach the gospel of integrated medicine are able to perform the art of medicine is as ridiculous as it is insulting to everyone in healthcare who does his/her best to meet the needs of their patients. The assumption that unproven or disproven treatments become acceptable simply because they are often administered in a kind and caring fashion is quite simply not true.
The “integrated medicine” straw-man, by Edzard Ernst
Did you find this article useful? Interesting? Maybe notice how there’s not much content like this on the Internet? That’s because it’s crazy hard to make it pay. Please support (very) independent science journalism with a donation. See the donation page for more information & options.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Related Reading
- Reviews of Pain Professions — An opinionated guide to the most popular sources of professional help for injuries and chronic pain
- Does Massage Therapy Work? — A review of the science of massage therapy … such as it is
- Pain Science Reading Guide for Skeptics — A tour of PainScience.com for readers who have doubts and concerns about the validity and efficacy of popular treatments for injuries and chronic pain
- Does Acupuncture Work for Pain? — A review of modern acupuncture evidence and myths, focused on treatment of back pain & other common chronic pains
- The demon-haunted world: science as a candle in the dark (book), by Carl Sagan and Ann Druyan. Amazon.com ❐ This treatise on critical thought is one of my all-time favourites, a book that makes ten others unnecessary, the kind of book that will change how you think forever.
- QuackWatch: Your Guide to Quackery, Health Fraud, and Intelligent Decisions (QuackWatch.org). Quackwatch fights health-related frauds, myths, fads, fallacies, and misconduct. Its primary focus is on health consumer information that is difficult or impossible to get elsewhere. Dr. Stephen Barrett, the founder of QuackWatch and author of most of the articles, is one of the great figures of anti-quackery activism. For many years now, I’ve been watching his work and the controversies and legal battles that swirl around QuackWatch, and I have been consistently impressed by Dr. Barrett’s integrity and intelligence — and unimpressed by the tactics and quality of his critics. He is also providing a vital service and a sorely neglected perspective on health care.
- Quackery Red Flags — Beware the 3 D’s of quackery: Dubious, Dangerous and Distracting treatments for aches and pains (or anything else)
- Most Pain Treatments Damned With Faint Praise — Most controversial and alternative therapies are fighting over scraps of “positive” scientific evidence that damn them with the faint praise of small effect sizes that cannot impress
- Why “Science”-Based Instead of “Evidence”-Based? — The rationale for making medicine based more on science and not just evidence… which is kinda weird
- Science versus Experience in Physical Medicine — The conflict between science and clinical experience and pragmatism in the management of aches, pains, and injuries
What’s new in this article?
Jul 16, 2025 — Added discussion of “medical nihilism,” as elucidated by Jacob Stegenga in his 2018 book.
2024 — Added a significant sidebar, “The epic double-standards for mainstream and alternative medicine.”
2024 — Improved a section I added a while back and forgot to log: “Alternative medicine: hung up on pseudoscience and anti-science.”
2024 — Science update. Added a couple citations about the harm that can be done by health care institutions and (closely related) physicians who lack empathy.
2020 — Added a section about the legal hazards of anti-quackery activism.
2018 — Cited and commented on The Lancet’s excellent editorial calling for “a radical shift of life sciences funding priorities, away from the biomedical bubble.”
2016 — Added citation to Louw 2016 about bogus surgeries, plus a couple minor edits. Added a picture.
2006 — Publication.
Notes
- More specific criticism of modern mainstream medicine will be provided below, with plenty of citations. However, for a sneak preview, on my favourite sources is Jacob Stegenga’s excellent book, Medical Nihilism, which criticizes medicine competently and credibly without being anti-scientific.
- Again, more specific evidence will be provided below. But for an excellent general source, see ScienceBasedMedicine.org.
- Sciencebasedmedicine.org [Internet]. Ingraham P. Why I Quit My Massage Therapy Career; 2019 February 22 [cited 19 Feb 23]. PainSci Bibliography 52363 ❐
In 2007, I was accused by my profession’s regulator of being an ‘unprofessional’ Registered Massage Therapist for criticizing pseudoscience in alternative medicine. I accepted an unusual public reprimand and made a few changes to my website, but my regulator pressed their case, effectively demanding that I quit writing altogether. I quit the profession instead.
- As Dr. Steven Novella has written: “Fifty years ago what passes today as CAM was snake oil, fraud, folk medicine, and quackery. The promoters of dubious health claims were charlatans, quacks, and con artists. Somehow they managed to pull off the greatest con of all — a culture change in which fraud became a legitimate alternative to scientific medicine, the line between science and pseudoscience was deliberate blurred, regulations designed to protect the public from quackery were weakened or eliminated, and it became politically incorrect to defend scientific standards in medicine.”
- Poulter D, Miciak M, Durham J, Palese A, Rossettini G. Don't be a nocebo! Why healthcare organizations should value patients' expectations. Frontiers in Psychology. 2024;15. PainSci Bibliography 51495 ❐
- Licciardone JC, Tran Y, Ngo K, et al. Physician Empathy and Chronic Pain Outcomes. JAMA Netw Open. 2024 Apr;7(4):e246026. PubMed 38602675 ❐ PainSci Bibliography 51466 ❐
This study of chronic low back pain patients reports that they did better with more empathic physicians. Quite a bit better! I’m not really surprised by the positive result, but I am surprised by how positive it was.
They divided physicians into two groups, “very” empathic and only “slightly” empathic (as determined by a survey, the “Consultation and Relational Empathy measure”). Various scores were much better for the lucky patients who got some empathy — disability and fatigue especially, but also actual pain intensity.
Clinically relevant caring!
If empathy can help, then its neglect is a harm. Needlessly forfeiting a medical benefit is indistinguishable from harm, so this citation is just as just as good for making the point that a lack of empathy is harmful to patients.
- Like my friend, after a motorcycle accident, who was refused a spinal X-ray by emergency room doctors at Royal Jubilee Hospital in Victoria, BC, only to discover the next day that his vertebrae were indeed broken. Like one of my own stories: a battle royale to prevent a determined nurse from dragging me off for a chest X-ray, even though my arm was in a sling because of the elbow injury that had brought me there. Or one told by a client, about having to advocate for himself while drugged, to convince a surgeon that he was in the hospital for a foot problem, and did not need abdominal surgery.
- Louw A, Diener I, Fernández-de-Las-Peñas C, Puentedura EJ. Sham Surgery in Orthopedics: A Systematic Review of the Literature. Pain Med. 2016 Jul. PubMed 27402957 ❐ PainSci Bibliography 53458 ❐
This review of a half dozen good quality tests of four popular orthopedic (“carpentry”) surgeries found that none of them were more effective than a placebo. It’s an eyebrow-raiser that Louw et al. could find only six good (controlled) trials of orthopedic surgeries at all — there should have been more — and all of them were bad news.
The surgeries that failed their tests were:
- vertebroplasty for osteoporotic compression fractures (stabilizing crushed verebtrae)
- intradiscal electrothermal therapy (burninating nerve fibres)
- arthroscopic debridement for osteoarthritis (“polishing” rough arthritic joint surfaces)
- open debridement of common extensor tendons for tennis elbow (scraping the tendon)
Surgeries have always been surprisingly based on tradition, authority, and educated guessing rather than good scientific trials; as they are tested properly, compared to a placebo (a sham surgery), many are failing. This review of the trend does a great job of explaining the problem. This is one of the best academic citations to support the claim that “sham surgery has shown to be just as effective as actual surgery in reducing pain and disability.” The need for placebo-controlled trials of surgeries (and the damning results) is explored in much greater detail — and very readably — in the excellent book, Surgery: The ultimate placebo, by Ian Harris.
- Quackometer.net [Internet]. Lewis A. Quack Word #20: ‘Iatrogenic’; 2007 Jul 3 [cited 16 Feb 11]. PainSci Bibliography 57019 ❐
“Iatrogenic illness,” or medically induced harm, covers the concept of harm having been done by the healer. In 2000, a presidential task force labelled medical errors a “national problem of epidemic proportions.” There are many technically correct and hair-raising stats about just how dangerous medicine can be — but the term and the stats are also often badly abused for ideological reasons. This article does a good job of putting it all in perspective.
- Perspective and context: people find stats about doctor-caused illness and injury to be shocking, but they almost never consider how many lethal, no-win situations doctors are faced with. You try running a hospital and get the error rate down to zero. Good luck with that! That’s not to say there aren’t serious systemic and institutional problems that need solving — there definitely are — but it’s because good health care is just inherently extremely challenging. People who point and blame without any sympathy or interest in those challenges are not helping. See Medical Errors in Perspective.
- MedicalNewsToday.com [Internet]. In Hospital Deaths from Medical Errors at 195,000 per Year USA; 2004 [cited 10 Nov 2]. PainSci Bibliography 56529 ❐
This article focusses on a major American study of medical error, summarizes the results of other similar studies, and paraphrases their conclusions: “medical errors caused up to 98,000 deaths annually and should be considered a national epidemic.”
Many doctors, especially general practitioners, lack the skills and knowledge to treat even common aches, pains, and injury problems, never mind the stubborn and puzzling cases. Some doctors are well aware of this, but many just have no idea, underestimate the complexity of pain care, and cannot even triage and refer appropriately. Even specialists tend to be too specialized, and many patients fall into the huge cracks between fields like rheumatology and neurology. Even pain specialists are often too specialized for many patients, their expertise invested in helping people with major and exotic disease pain — not relatively “minor” problems like back pain.
Medical researchers have done many studies showing that most doctors jut do not know much about pain, and don’t heed expert recommendations. For instance, family doctors frequently ignore guidelines for the care of low back pain (Williams et al.). Freedman et al. wrote: “It is ... reasonable to conclude that medical school preparation in musculoskeletal medicine is inadequate.” In 2005, Matzkin et al. concluded that “training in musculoskeletal medicine is inadequate in both medical school and non-orthopaedic residency training programs.” In 2006, Stockard et al. reported that 82% of medical graduates “failed to demonstrate basic competency in musculoskeletal medicine.” Orthopedic surgery is notorious for pushing bogus procedures like Knee Debridement is a Completely Ineffective Procedure. MRI is overwhelmingly abused as “medical theatre.” fibromyalgia patients are still referred for mental health care in droves. And so on and on ever since: the basics and well-established guidelines and best practices are widely neglected.
- See Matzkin, Freedman, and Stockard.
- Mijatović N, Šljivić J, Tošić N, et al. Big Suppla: Challenging the Common View of the Supplements and Herbs Industry Affects the Willingness to Try and Recommend Their Products. Studia Psychologica. 2022 Mar;64(1):91–103. PainSci Bibliography 51970 ❐
The term “Big Suppla” is a witty delivery mechanism for the truth bomb that debunks the underdog myth about the supplements industry. It’s quite clever. If Suppla is just as Big as Pharma… well, the whole point is that the implication is so clear that no further explanation is even required.
But does that reach people? Is it an effective debunking strategy? Mijatović et al. actually tested this, and the results were positive, huzzah! Minds were changed! This is a great relief for me to hear, because I started deploying “Big Suppla” in about 2006. Specifically, they tested the effect of this terminology by giving about 250 people three different kinds of information about the supplements industry:
- Neutral information was just the origins of the words “supplements” and “alternative.”
- Big Suppla information framed the industry as “powerful, profit-oriented, and unregulated.” Which it actually is.
- Baby Suppla information portrayed the supplements industry as a virtue-motivated underdog. Which it definitely is not.
The test results were better than science communicators could have hoped for. Not only did the “Big Suppla” framing change minds, but it even worked on some of the hardest targets: subjects who were prone to conspiratorial thinking. Those people were more likely to be keen on supplements to begin with, but they were still persuaded by “Big Suppla.” Perhaps it’s because this debunking method exploits the “follow the money” trope that practically defines conspiratorial thinking.
- The Lancet. UK life science research: time to burst the biomedical bubble. Lancet. 2018 Jul;392(10143):187. PubMed 30043738 ❐ PainSci Bibliography 53048 ❐
- Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977 Apr;196(4286):129–36. PubMed 847460 ❐
This paper is the origin of the now famous biopsychosocial model of healthcare, advocating for a kinder, more nuanced and artful medicine, as opposed to the rather cold, clinical, and technical profession it had become in the middle of the 20th Century thanks to its immense science-powered successes.
Engel argued that the dominant biomedical model inappropriately reduced too many complex health concerns to biology and pathology alone (reductionist), excessively separated body and mind (dualist), and left “no room within its framework for the social, psychological, and behavioral dimensions of illness.” In short, he believed medicine had become dehumanizing, excluding the patient and their “…attributes as a person, a human being.”
Engel proposed that the BPS model could provide a “…blueprint for research, a framework for teaching, and a design for action in the real world of health care.”
Ever since publication of this landmark paper, the BPS model has been extensively interpreted and misinterpreted, used and abused and co-opted and perverted. Cormack et al. describe many of the problems that emerged over the years, and I explored that topic in detail, see: BPS-ing badly! How the biopsychosocial model fails pain patients.
- Stegenga J. Medical nihilism. First edition ed. Oxford University Press; 2018.
How good is modern medicine? Almost everyone loves to hate it, but routinely for the wrong reasons. We are used to hearing criticism of medicine mostly from cranks and quacks, and about 90% of it is just in service of selling their bullshit “alternatives.” In the post-pandemic US, medicine and medical science are now also on the front lines of the American culture war on science and expertise.
Imagine criticizing medicine for the right reasons. What a surprisingly rare and refreshing idea! I’d like to strongly recommend this extremely skeptical, high-quality take on the state of art and science of medicine, from the podcast EconTalk, interviewing Jacob Stegenga.
Stegenga is harsh but absolutely fair, criticizing medicine without being anti-scientific. He gives credit to medicine where due, but only where due, and argues persuasively that we should have little confidence in the effectiveness of medical interventions, and a lot of caution about their harms. He proposes that we need a lot more “gentle medicine” that errs on the side of less intervention.
I think this is the kind of criticism medicine actually needs. There’s a fantastic book, and a short British Medical Journal editorial about it. Listening to Stegenga talk about it himself on a podcast is another good introduction to the book.
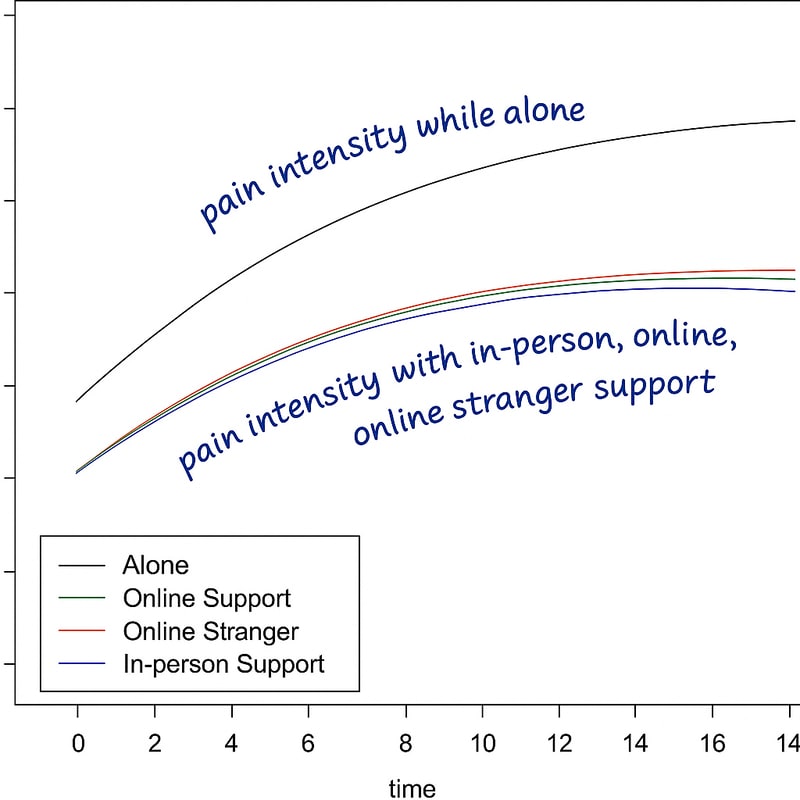
- Karos K, Meulders M, Courtois I, et al. The effect of online social support on experimental pain. The Journal of Pain. 2025 2025/04/17.
There there. 🤗 I hear you. I understand your pain (seriously). I’ve got your back.
And now I bet you’re feeling better already, less pain just from reading these empathetic words! You’re welcome!
A new study by Karos et al. concludes that even online social support can blunt pain. And from strangers, no less! If they’re nice. The active ingredient of empathy can be delivered through the internet’s tubes, perhaps.
Good to know, if true. There are disclaimers, of course — small study, acute pain, lab conditions, any number of possible confounders, et cetera — but it’s an interesting little experiment.
![Line graph showing pain intensity over time under different social conditions. The x-axis represents time and the y-axis represents pain intensity (not numerically labeled). Four lines are plotted: a black line for “Alone” showing the highest pain intensity; green for “Online Support,” red for “Online Stranger,” and blue for “In-person Support,” all showing lower and nearly identical pain intensities. Large curved text emphasizes the contrast: “pain intensity while alone” above the black line, and “pain intensity with in-person, online, online stranger support” below the other three lines.]()
Note that this result harmonizes nicely with a 2024 study by Licciardone that showed better outcomes for chronic low back pain patients working with empathic doctors.
- Even the best physicians will struggle to be personal and thorough because of the scale, institutionalization, economics, and harsh dilemmas of medicine. (For instance, neurologists can’t really be expected to take a lot of time for detailed troubleshooting and brainstorming about maybe-neurology problems, clinical puzzles that are often legitimately beyond their understanding, while they are appropriately preoccupied with (and indeed probably overwhelmed by) clinical challenges like strokes, multiple sclerosis, and amyotrophic lateral sclerosis.)
- That is, all the basic medical science classes are in the curriculum — anatomy, physiology, pathology, and so on.
- Being virtually unregulated (see Scott Gavura’s Supplement Regulation: Be Careful What You Wish For), they sell useless and contaminated products at markups that the average person would regard as egregious (see Scott Gavura’s Do the Natural Health Products Regulations Benefit Canadians?).
- ScienceBasedMedicine.org [Internet]. ScienceBasedMedicine.org. Science-Based Medicine Homeopathy Resource Page; 2010 [cited 12 Feb 19]. PainSci Bibliography 55804 ❐
- News.BBC.co.uk [Internet]. Jones M. Malaria advice ‘risks lives’: Some high street homeopaths claim they can prevent malaria, a Newsnight investigation has found; 2006 [cited 12 Feb 19]. PainSci Bibliography 56534 ❐
Secret filming revealed homeopaths were claiming their preparations could be used instead of anti-malarial drugs to protect travellers in high risk areas such as sub-saharan Africa.
- See my review of the evidence in Does Acupuncture Work for Pain?.
- See Haake and a detailed of discussion that paper in Does Acupuncture Work for Pain?.
- Hopefully it’s obvious that a billion Chinese can be wrong. They can be. They routinely are.
- The chiropractic profession has often responded to scientific criticism with legal threats. I have even received legal threats from chiropractors for saying that— oh, irony! The most famous example of chiropractic litigiousness was the (fortunately unsuccessful) attempt to sue science journalist Simon Singh, forcing him to spend vast sums of money to defend his right to express an opinion. It was like Hollywood suing a movie reviewer for criticizing a film.
- For more about this cautious approach to evaluating chiropractic, see The Chiropractic Controversies
- Massage therapy training in British Columbia, Canada, has been unusually rigorous compared to most places in the world. When I trained in the late 90s, the requirements included a 3000-hour training program, an internship, and some challenging certification exams. I believe it’s back down to 2000 hours, but it remains unusual by global standards.
- Many of my readers may find that last statement too harsh. Perhaps a clarification will help, however: I do not attack the reputation of such practices because I have any doubt that “The universe is not only queerer than we suppose, but queerer than we can suppose.” (Haldane), but rather because of it. I do not doubt that the universe is a fascinating and bizarre place and that there are many wonderful things yet to learn about it. What I do doubt is that my fellow alternative health care practitioners are able to comprehend it well enough, without benefit of rigorous study and insights into biology the likes of which no serious scientist enjoys, in order to offer patients therapeutic benefits by completely unproven methods. In other words, I question their competence. If they were ethical, they would be more honest and humble about the limitations of their knowledge and skill — a quality conspicuously lacking from a group of people so fond of referring to themselves as “healers” and “masters.”
Many alternative health care practitioners, especially chiropractors, claim that they are as well trained as physicians. This is false. Doctor’s academic training is routinely longer, and — more importantly — most of their serious learning occurs during extensive on-the-job training, where they are thrust into demanding clinical environments and supervised for years as they deal with a great variety of clinical situations and many extremely sick and hurt patients. That hands-on phase of their training is where all doctors will tell you that they became professionals — and there is nothing like it in any non-medical health care training.
- “Healer syndrome” is a common delusion of grandeur in alternative medicine, especially massage therapy, naturopathy, and chiropractic, where many afflicted professionals like to be known as “healers” with allegedly unusual curative powers, vaguely defined, pseudoscientific, or based on the exaggerated importance of a single idea. Such lack of humility is tragically common. Healer syndrome has reached its most extreme in some of the founders of methods of therapy, what I call “modality empires.” See Healer Syndrome: The problem with health care professionals, especially in alternative medicine, who want to be known as “healers”.
- “Manual therapy” refers mainly to massage, spinal adjustment, and other costly methods of using hands/tools to “fix” tissue, mainly treatments that are done to passive patients. Although mostly the domain of massage therapists and chiropractors, physical therapists also use many manual methods. Unfortunately, it is mostly a pseudoscientific dumpster fire based more on authority, tradition, and marketing than good research. And yet some practitioners are responsible, and the power of compassionate touch to comfort and inspire should never be underestimated. For more information, see Manual Therapy: What is it, and does it work? The science of "fixing" tissue with hands-on treatments like massage and spinal manipulation.
- There are anti-SLAPP laws in many places around the world now, so it’s getting better, but it’s still tricky and risky, especially because plaintiffs can often find a way to sue in a jurisdiction without anti-SLAPP laws (or ones with significant loopholes).
- Gesundheit! (http://www.patchadams.org)
- Flamm B. The Columbia University ‘Miracle’ Study: Flawed and fraud. Skeptical Inquirer. 2004 Sep/Oct;28(5):25. PainSci Bibliography 57193 ❐
A Columbia University paper published in a peer-reviewed scientific journal claimed clear evidence of the efficacy of remote prayer, and was reported with great enthusiasm by the American media in the aftermath of post-9/11, and continues to be widely cited routinely in support of similar claims. Yet the first-named author “doesn’t respond to inquires,” the “lead author said he didn’t learn of the study until months after it was completed,” and then the third author, “indicted by a federal grand jury, has pleaded guilty to conspiracy to commit fraud” — not with regards to the study, but several other charges of fraud.
- Ingraham. Ioannidis: Making Medical Science Look Bad Since 2005: A famous and excellent scientific paper … with an alarmingly misleading title. PainScience.com. 3272 words.
- For instance, the “soft” social sciences in particular, but also hard biochemistry, have produced reams of data about the medical importance of “subtleties” like the relationship between outcomes and time spent with patients, the effects of fear and anxiety, the need for better nutrition in hospital meals, the hazards of impersonal care, setting a good example in lifestyle habits, and so on and on and on.