What are the worst kinds of chronic pain?
No pain can be objectively “the worst,” of course. What makes a pain terrible is extremely personal.
I know a guy who had two equally intense chronic pain problems for over a year, plantar fasciitis and frozen shoulder, both notoriously disabling conditions — but he never mentioned his shoulder through months of chatting with him about his plantar fasciitis. When he finally did, I asked why he hadn’t brought it up sooner.
“Because it doesn’t stop me from walking! That’s all I really care about. I can’t live without my walks! Shoulder schmoulder, pfft.”
And I think he really meant that he couldn’t “live” without walks. The plantar fasciitis disability felt like life-or-death stakes to him. No walks, no life! For him, plantar fasciitis was a deadly disease, consigning him to a fate worse than death.
(Good news: he more or less recovered the ability to walk! And the shoulder? “Oh, that? Yeah, that’s fine now too.”)
That tale of two pains was all about pain-related suffering, the meaning and significance of the pain to the person who has it, rather than its intensity alone. It illustrates that intensity is not the only thing that matters. In fact, there are many things that matter: many factors affect how we rank the awfulness of pain.
In today’s post, I will explain how it’s seductive and misleading and ultimately impossible to rank pain by its awfulness … but then I will go right ahead and do it anyway, with a list of the worst possible kinds of chronic/recurrent pain. Good morbid fun!

Backwards-Hand Disease (BHD) is a notoriously painful and disabling condition. No wonder her Pain-O-Meter is in the red!
What makes pain worse?
Pain has many dimensions: intensity, duration, unpredictability! Fatigue, cognitive impact, emotional load! The effect on work, play, pride. And location, location, location: Central or peripheral? Is it embarrassing, secret? Is it shared or borne in isolation? Does it come with other distressing sensations, like itch? Or other awful symptoms, like vomiting?
And many more.
“Intensity” gets most of attention (and the rating), but “duration” is probably the most neglected secondary factor, the burden of intensity × time: no pain is “mild” if it never lets up, and some of the worst pain experiences are based on the simple multiplication of a moderately intense pain by every hour of the day.
A condition that peaks higher in one way may be far more endurable overall than another. Unpredictability can be more ruinous and disabling than intensity. Sleep loss, brain fog, and fear conditioning can be more corrosive and insufferable in the long-term than any dose of nociception. Pain is harder when it’s linked to cultural taboos, like pelvic pain, and especially purely sexual pain.
Ranking and comparison can distort care and credibility: they invite suffering “contests,” stigmatize and sideline people whose pain doesn’t “sound” dramatic, and reward conditions with more theatrical symptoms. Clinically and ethically, the scale that matters is impact on function and life — not just how far the pain pushes the needle of a hopelessly hypothetical pain-o-meter.
But here’s my list of the worst chronic pain problems anyway
There’s more to a pain than its sheer wattage … but the intensity still matters, and it matters a lot. Also, some conditions are predictably nasty in multiple ways. So I’m still going to do a list, because we can still say with confidence that cluster headaches tick a lot of pain-awfulness boxes. But notice that this is just a list, not a ranked list, not an ordered “top 10” — because any of these could be dialed up or down depending on the personal context.
This list is not about acute pain, even if it can occasionally turn chronic or recurrent. I’ve excluded pains that are mostly one bad experience, like a kidney stone or appendicitis. This list includes disorders that mainly cause continuous, long-term pain, or episodes that are severe/frequent/long enough to really mess with people’s lives.
An early Facebook share of this post quickly attracted many suggestions (“hockey puck to the groin”), some of which I’ve now integrated here (before sending it out to newsletter subscribers).
Continuous or near-continuous severe pain:
- Complex regional pain syndrome
- Central pain syndromes (post-stroke, spinal cord injury, multiple sclerosis)
- Small fiber neuropathy
- Trigeminal neuralgia (when frequent or refractory)
- Chronic pancreatitis
- Interstitial cystitis / bladder pain syndrome
- Fibromyalgia
- Advanced cancer pain syndromes
- Endometriosis
- Pudendal neuralgia
Chronic-episodic pain with extreme intensity:
- Cluster headache (people who’ve had both cluster headaches and other kinds of severe pain all seem to agree that cluster headaches are by far the worst, see graph from Burish et al below)
- Chronic migraine
- Hemicrania continua / SUNCT-type disorders
- Recurrent severe gout / chronic tophaceous gout
- Sickle-cell pain crises
- New daily persistent headache (a headache that starts one memorable bad day and just never stops)
- Recurrent renal colic (stone formers with frequent obstruction)
- Trigeminal autonomic cephalalgias (broader group)
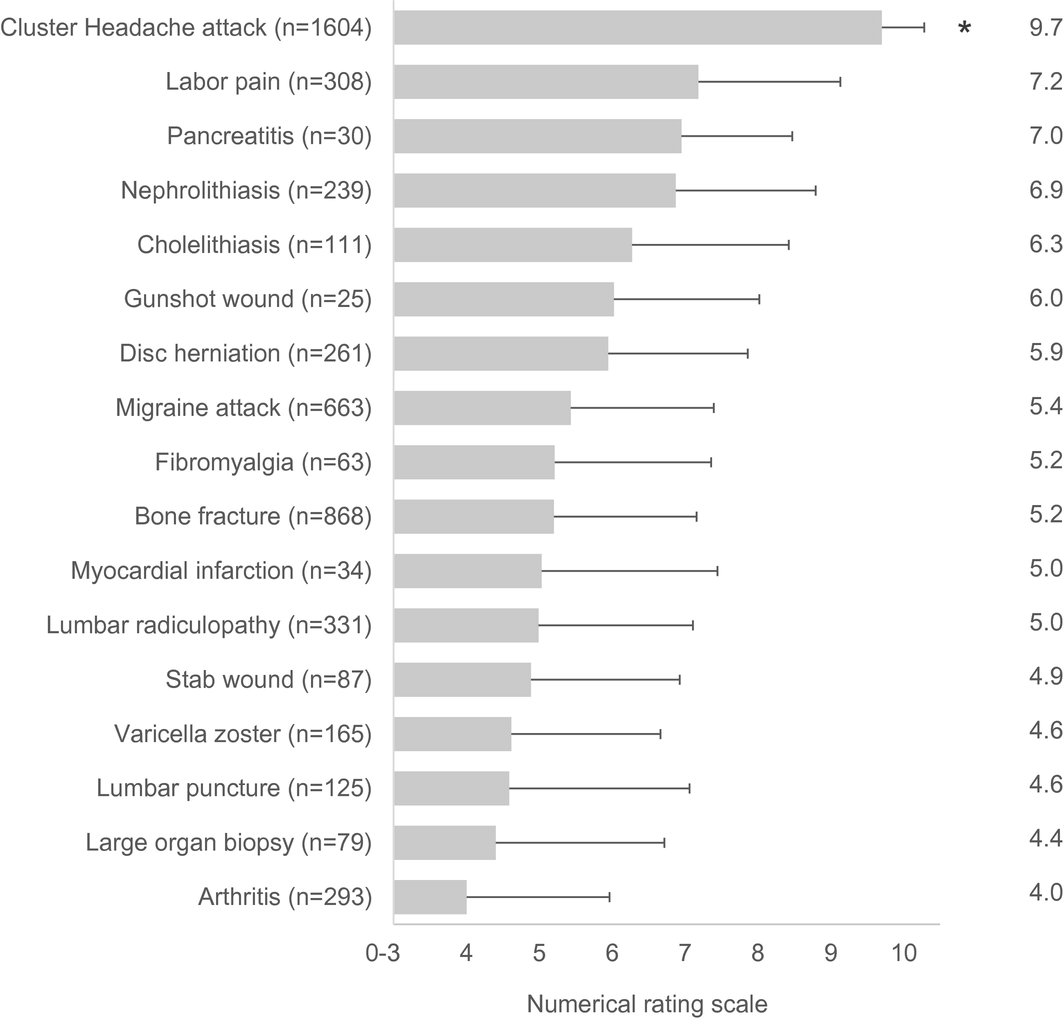
Cluster headache patients think cluster headaches are more painful than any of those other things — based on their own experience with both cluster headaches and those other conditions! 🤯 (Exploding head emoji unusually apt here!) Graph is from Burish et al., Headache, 2020.
Intermittent-but-progressive or relapsing neuropathic/inflammatory:
- Post-herpetic neuralgia (not shingles, but pain that persists after the shingles subsides)
- Severe rheumatoid arthritis or ankylosing spondylitis
- Ehlers-Danlos with chronic pain flares
- Diabetic neuropathy
Honourable mentions, conditions that aren’t so much known for their intensity but are “special” in some other way that makes them terrible:
- Eczema, thanks to the combination of pain with itching — extremely distressing.
- Vaginismus, vulvodynia and vestibulodynia, thanks to the intense stigma.
- Phantom limb syndrome, because it is so bizarre: very psychologically unsettling!
- I’ve already mentioned MS, but the “multiple sclerosis hug” deserves a callout: a painful, suffocating spasticity of the trunk muscles.
- Pubic symphysis diastasis, probably because it feels so “core.”
- Polymyalgia rheumatica: although treatable with steroids such that it’s only a temporary horror for most patients, it is notoriously savage … and not everyone gets diagnosed and treated.
I’m sure that’s not all, and more suggestions are welcome, of course, if you’re seeing this for the first time.
This list is also a to-do list
Curiously, PainScience.com offers content about almost none of these conditions (just the three links you see there), but that’s something I’d like to change. Listing the nastiest is a bit of a reminder to myself to start tackling the full range of painful conditions — not just what I’ve focused on historically, the “aches and pains” and relatively “minor” injuries … like fate-worse-than-death plantar fasciitis!