The Phantom of Complex Compensatory Injuries
Are your old injuries the insidious cause of your new ones?
A “compensatory injury” in physical medicine is an injury to one part of the body caused by the stress and strain of an older injury or insult in another part of the body. There’s nothing controversial about straightforward examples — they are usually just called “complications,” and major injuries clearly can lead to distinct new aches, pains, and breakdowns, sometimes even many years later. But the relationship is usually relatively simple, clear, and rarely clinically interesting.
It’s the idea of much slower and weirder examples that’s controversial.

Compensatory injury ideas really do get quite silly.
What people are keen on — both clinicians and patients — are the more exotic causal links that might connect the dots between injuries and complications separated by much more time and anatomy, like blaming a shoulder pain in 2023 on a knee injury from 2005. As the number of dots increases, the more impressive it gets — and more speculative. Push this far enough and it gets absurd. But not too absurd to be popular! Subtle, sneaky, and almost spooky causal links really fascinate people. People seem to like to believe that their pain has deep roots, and they love it when professionals claim to have exposed them. Even when it’s extremely implausible.
This kind of “explanation” for pain and injury has become a bit of a cliché of physical medicine, and a major sub-type of “structuralism” — an excessive emphasis on elaborate and subtle biomechanical vulnerabilities.1
In practice, the idea of compensatory injury is dominated by more speculative and self-serving examples — pet theories about the cause of pain that make professionals sound diagnostically sophisticated, wise and insightful about the interconnectedness of the body. Compensatory injury claims are great for justifying and selling treatments.
The basics of basic compensatory injury (AKA ordinary “complications” of injury)
Let’s review the conventional wisdom before tackling its common abuse. Here’s how compensatory injury allegedly works, and almost certainly does work in simpler cases:
- Primary Injury: It all begins with an initial injury or dysfunction, which could be anything from a sprained ankle to an episode of sciatica to frozen shoulder, or even insult from a pathology: anything that has the potential to change how we use our bodies.
- Altered Movement: We adapt to the primary injury by moving differently. For example, if your left knee hurts, you might start putting more weight on your right leg. This is no big deal at first … or ever for most minor injuries, and even many major ones.
- Compensation and Overuse: In some cases, the body is not prepared for the extra load. This leads to overuse of vulnerable tissues and new pain or injuries or flare-ups of minor pre-existing problems.
- Sensitization: Overuse is always relative to load tolerance, and load tolerance is a function of complex biopsychosocial factors (e.g. it’s lowered by sleep deprivation). The primary injury may reduce load tolerance systemically or regionally through mechanisms like neurological sensitization, lowering the threshold at which a complication might flare up.
- Kinetic Chain Reaction: Compensatory injuries are injuries in their own right, and so they may themselves cause more compensatory injuries: a chain reaction up and down the “kinetic chain.” However, importantly, they also decline in severity with time and distance from the primary injury.
Here are some uncontroversial examples that all involve relatively short term and obvious causal effects in adjacent body parts (although even here one could question some of the assumptions):
- Back pain from limping: Limping due to a foot or ankle injury could lead to uneven loading of the spine. Over time, this might contribute to the development of chronic low back pain. Assuming back pain can even be caused by slightly uneven loading, which is far from a sure thing. (See what I mean about the assumptions?)
- Shoulder Overuse from Elbow Injury: Consider a tennis player with the predictable elbow injury (lateral epicondylalgia, “tennis elbow”): the pain might alter their technique, leading to increased load on the shoulder joint, and then a new injury like a rotator cuff tendinitis.
- Knee Pain Following Hip Injury: After a hip injury, such as a hip labral tear, a person might walk a bit funny to adapt to the reduced hip ROM, putting additional stress on the knee, potentially leading to new knee problem like patellofemoral pain — or exacerbating existing knee conditions, which are quite common and may well have already been simmering away when the hip trouble started.
These examples are all legit to some extent… but so what? Such spin-off injuries are not very clinically significant or actionable.2
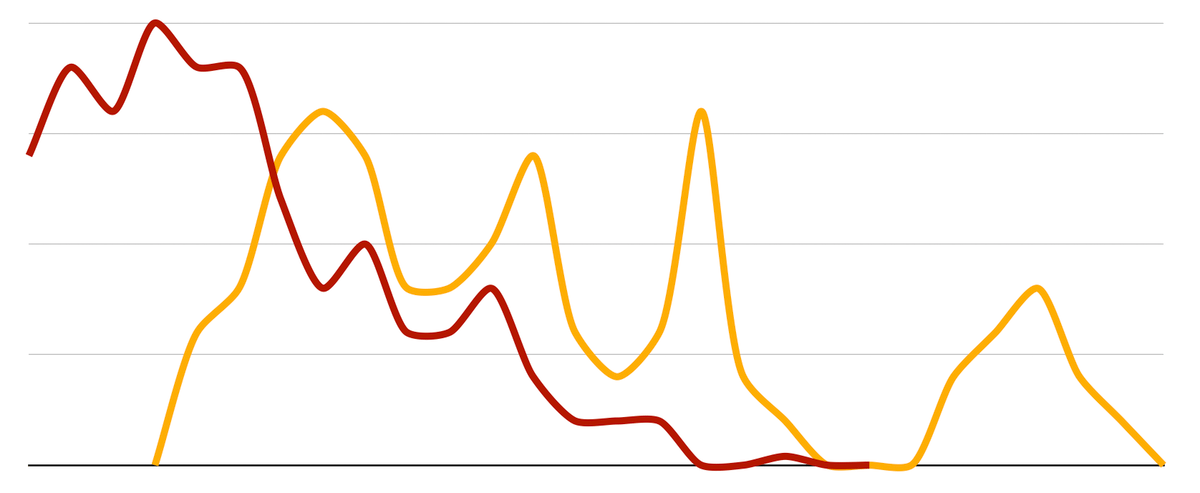
This graph shows how a simple (believable) compensatory injury (orange) tends to follow on the heels of a primary injury (red), but is still generally lesser and limited and more or less concurrent. In other words, compensatory injuries are mostly not major complications that come out of seemingly nowhere many months or years later.
Cooler compensatory injuries: connecting dots across the body and the years
“Do I have back pain because I blew a knee playing basketball twenty years ago?”
People ask questions like this all the time, and they have mostly learned to ask those questions from healthcare professionals who float theories like this. There are clinicians who take long-term, subtle compensatory injuries seriously — much too seriously in many cases. Here are some genuine examples from chats I’ve had with physical therapists on social media while I was writing this article (and I’ve seen countless variations in my inbox over the last twenty years):
- A toe stub in 2005 can cause hallux limitus in 2023.
- A sprained ankle in adolescence is the seed of frozen shoulder in middle age.
- Chronic abdominal pain is the root cause of carpal tunnel syndrome someday.
These are based on highly speculative causal links between old and new problems. I call these “complex” compensatory injuries, because the implied or specified chain of causality is always long and full of guesses. The biomechanical dots are connected from one end of the body to the other and across many months or years.
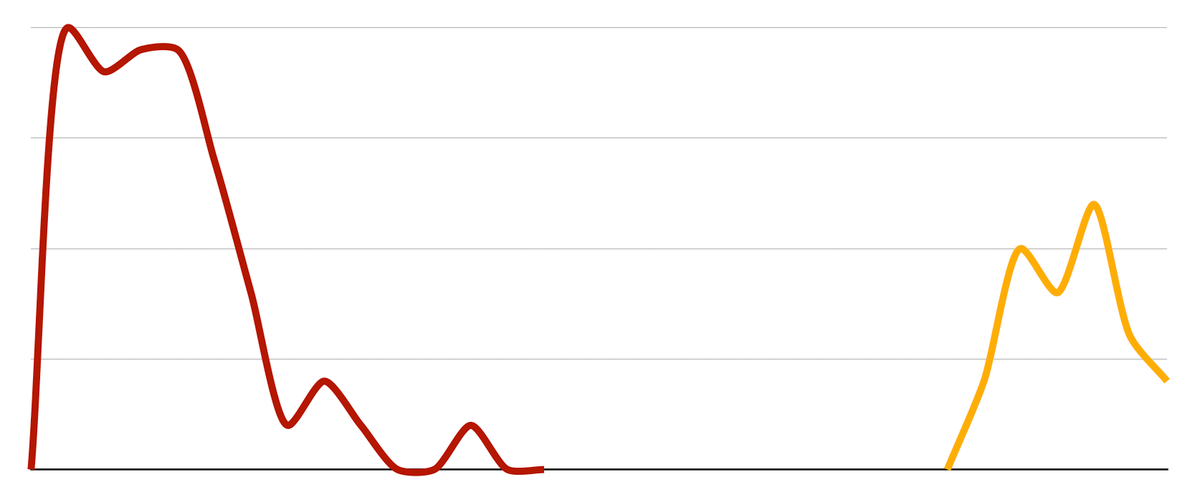
This graph tracks a hypothetical compensatory injury (orange) that is well seperated from the original injury (red) — in time at least, but of in a completely different part of the body as well.
In short, these kinds of compensatory injuries look much less like obvious complications of the primary injury, and much more like new injuries connected to the primary injury only by … a fishy story about causality that seems like diagnostic wizardry.
These are the kinds of compensatory injuries that people talk about. And the more dots are connected, the cooler it is. It’s like the conspiracy theorist’s wall of red string — but for knees and spines instead of shadowy cabals.
Charlie Day’s “Pepe Silvia conspiracy meme” from FX’s It’s Always Sunny in Philadelphia. This is probably the most familiar example of the “evidence board” trope, also known as a “conspiracy board” or “crazy wall”: a collage of media from different sources, pinned to a pinboard or stuck to a wall, interconnected with string to mark connections. it’s a disturbingly apt metaphor for a lot of poor quality reasoning in physical therapy!
Do complex compensatory injuries actually exist?
Probably a handful. But for every legitimate example, there are may be dozens that range from sketchy to properly bogus.
One weird example: we know that scoliosis can be triggered by trauma. Something about the dizzyingly complex physiology and kinesiology of the spine results in a slow-motion vicious cycle of dysfunction in the aftermath of some major spinal injuries. Whatever intricate feedback systems manage the curvature of the spine, they are derailed by the damage, and slowly but surely the spine (literally) spirals out of control. Sadly, my wife has this problem, ever since a serious vertebral “burst” fracture in a major car accident in 2010.
But such fates are the exceptions that prove the rule: the “cooler” the compensatory injury is, the less likely it gets. If a hypothetical causal link is subtle and complex and long-term and links remote anatomy, it’s implausible, if not just ridiculous. I suspect that “compensation” for old injuries as a major mechanism for new ones is quite rare — and also impossible to be sure of.
Of course severe injuries can cause obvious strain from trying to adapt to them. But people don’t feel a need to even ask about those. Obvious is (mostly) obvious! What people do wonder about is the possibility of a small-yet-corrosive force, something that they were barely even aware of, leading eventually to a surprisingly delayed and serious breakdown of some other tissues.
In broad strokes, this is the “slow loading” hypothesis. To make sense, the allegedly stressful adaptations have to be stressful enough to be a problem, to cause enough wear and tear to someday lead to tissue overload, degeneration, and new injuries … and yet they also can't be stressful enough to be an obvious problem along the way. If the stress was obvious, no expert insight would even be required.
Complex compensatory injuries always rely on a story about causality to link two problems. But causality is one of the hardest things to establish in medicine, because of the endless riot of variables and confounders: truly tricky scientific research is needed to “prove” causes, and it has hardly ever been done for much of anything at all, let alone anything in the relative backwater of physical medicine. Even seemingly obvious causal relationships often turn out to be wrong! There’s not even strong cross-sectional evidence (just identifying correlations) for major risk factors for common overuse injuries like iliotibial band syndrome or tennis elbow. We cannot clearly establish that biomechanical abnormalities, gait quirks, or posture are correlated with injuries and pain problems … let alone that they cause them … let alone that the relationship can spread across chasms of time and anatomy.
Compensatory injury as a deepity
What seems fascinating about compensatory injury is mostly an illusion. The coolest examples are the least likely to be true. Profound but false.
But more straightforward and plausible short-term complications of injury are boring, and not what most people are thinking about when they talk about compensatory injuries … because why would you? Yeah, duh, injuries can cause related flareups of strain and discomfort! True but trivial. The boring examples only get referenced to prop up the less plausible ones.
This is a classic deepity, a claim that is either profound but false or true but trivial. “Deepity” was coined by philosopher Daniel Dennett to describe anything that seems impressive at first glance, but the impressive part is nonsense, and the true part is ho-hum. In other words, profound claims are often made to seem more plausible by linking them to a seed of truth, and Dennett gave us a name for that gambit.
The world of musculoskeletal medicine and manual therapy is rife with deepities, and subtle compensatory injuries are one the great examples. The credibility of implausible causes of injury is boosted by linking them to the seed of truth of more ordinary injury complications.
Is there room for some truth in the middle? What about the medium compensatory injuries?
On the one hand, I’ve described simple compensatory injuries with obvious links to a primary injury. On the other, I’ve described complex, subtle compensatory injuries linked by highly speculative and vague mechanisms. What about a compromise between these extremes? Are there some compensatory injuries hanging out in the middle of that spectrum?
Perhaps, but we just have no way of knowing. Anatomical and kinesiological abnormalities aren’t clearly established causes of injury even when they are obvious (measurable), a major take-home message from decades of research showing that injuries do not correlate cleanly with seemingly obvious risk factors. The general implication is that there are major variables we don’t understand, probably a mess of bio (neuroimmunological) and psychosocial factors.
If you can’t reliably blame patellofemoral pain on poor patellar tracking — and you really can’t — then good luck nailing down a causal relationship between a five-year old hip injury and a new back problem (let alone anything more stretched out across time and anatomy).
That is how I’ve come to the conclusion that compensatory injuries that exist somewhere between simple and complex are not much more clinically interesting than the more polarized versions. It’s not that I think they don’t exist at all — there are probably a few — it’s just that it’s effectively impossible to nail down the cromulent ones.
Another way of putting it is that any link that isn’t extremely clear and simple is going to be a bit of a reach, regardless of whether they are way out on the speculative frontier or in the more reasonable gray zone. This is a major in practice problem even if moderately complex compensatory injuries are for real in theory. Which they might not be.
Stop blaming old injuries for new ones
No one should be enthusiastic about the identification and correction of ancient adaptions to address the “root cause” of new injuries or unexplained pain. Patients should be extremely wary of paying for help based on a tune like this.
To the extent that compensatory injuries are real, they are also not particularly interesting or important, and are rarely actually discussed. The more interesting claims of compensation are highly speculative “stories” about causality that cannot be proven and aren’t very plausible … but they do enhance the reputation of the clinician, and greatly help to justify and sell therapy! Predictably, it’s particularly prevalent in the “freelance” manual therapies, like massage and chiropractic, which are motivated to convince patients to pay substantial and ongoing fees of out of pocket (and evidence-based medicine is either neglected or rejected).
And yet, unfortunately, compensatory injury speculation surprisingly prevalent in physical therapy as well.
I believe the idea of compensatory injury is one of the greatest hits of structuralism, and it is dominated by lazy wishful thinking and self-serving speculation, and almost no science at all. It should mostly be ignored and left behind.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
Sep 20, 2025 — Substantive editing and revision, and an audio version. Ta da!
2025 — Revised and published for the first time on PainScience.com.
2024 — Originally published in the 2nd edition of MSKMag in early 2024.
Notes
- “Structuralism” is the excessive focus on crookedness and “mechanical” problems as causes of pain. It has been the dominant way of thinking about how pain works for decades, and yet it is a source of much bogus diagnosis. Structuralism has been criticized by several experts, and many studies confirmed there are no clear connections between biomechanical problems and pain. Many fit, symmetrical people have severe pain problems! And many crooked people have little pain. Certainly there are some structural factors in pain, but they are generally much less important than messy physiology, neurology, psychology. Structuralism remains dominant because it offers comforting, marketable simplicity. For instance, “alignment” is the dubious goal of many major therapy methods, especially chiropractic adjustment and Rolfing. See Your Back Is Not Out of Alignment: Debunking the obsession with alignment, posture, and other biomechanical bogeymen as major causes of pain.
- That is, they are still mainly overshadowed by the primary injury and mostly resolve in sync with it, usually on a scale of weeks or months … and there’s often not much to be done to prevent or treat them. It’s generally a fantasy that injury healing can be facilitated or sped up. The need for “treatment” of minor injuries is routinely exaggerated. I’m not saying there’s no point whatsoever in trying to help someone with a spin-off injury, just that it’s a relatively low priority. As long as it doesn’t turn out to be unusually stubborn, it’s mostly just a waiting game.