Extra, extra! Extra floating ribs are way more common than anyone knew (Member Post)
Coincidentally, an old friend has been suffering through a nasty example of the very painful problem I have been writing about for the last week: slipped rib syndrome. The lower ribs are unstable at the best of times, and they can slide under a neighbour and pinch an intercostal nerve (among other discomforts). As always, a physical predicament like this may or may not feel as bad as it sounds (depending on the metabolic context). But the result for my friend was a classic and severe blaze of intense pain around one side of his lower ribcage. It started suddenly with no apparent provocation a couple weeks ago, and it made his life hell for a few days:
“I was in so much pain I couldn’t sleep, couldn’t breathe properly, couldn’t lie down or sit, couldn’t really do anything.” So he just sweated and squirmed his way through. “It’s been backing off this week, but it’s still bad.”
This was a new experience for him, but he has a form of muscular dystrophy that has already given him a lot of back trouble, and it probably increases the risk of this rib nonsense (due to weakness of the trunk musculature). But there’s also a much more common risk factor that no doctor or physical therapist would have known about … because no one could have known about it without reading a recent study of the anatomy of the ribcage.
You’d think ribcage anatomy would be settled science, but nope! And that is what I was writing about: not only is the lower ribcage an anatomically chaotic area, but specifically there are far more floating ribs down there than we see in the textbooks … and they are slippery. It’s new anatomy that matters.
“The word ‘normal’ is probably an inappropriate word to apply to the human body.”
This is a members-only post, with an audio version. And it’s a big one, about 4000 words (15 minutes reading). It covers the surprising new anatomy, the problems it causes, and some treatment options (mostly self-treatment). Members paying $3/month have already received the full text in their inboxes (sign up on Aug 9) and you can get it too. $5+/month members get the audio and full web versions as well, plus the entire archives, and more.
This post will also soon be converted into a chapter of my low back pain book as well, so you can also get access to it with a one-time purchase of USD $20.
Buy Good, Better, or Awesome PainSci Membership…

Change or cancel plans with ease. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism.

It’s getting routine for scientists to personally tell me about their research, which is delightful. Dr. Evert Eriksson, Trauma Medical Director at the Medical University of South Carolina, read my article about anatomical variation — about all the ways that anatomy differs from one person to the next — and he thought, I should tell this guy about my rib study! Bet he’ll like that. And he did tell me, and I did like it. Very much.
One could hardly ask for a better example of an interesting and problematic body oddity. What Laswi et al. found, studying 8th, 9th, and 10th ribs in forty cadavers, was a lot more free 9th tips, and entire floating 10th ribs, than they were supposed to find:1
A whopping 59% of forty cadavers had three fully floating ribs — 10th, 11th, and 12th — rather than the officially standard pair.
And 86% of 9th ribs had a free tip, even though they were not otherwise true floating ribs. The 9th was always (100%) attached to the 8th by cartilage, but … messily, and most of their tips were free floating. So the 9th is kind of a hybrid (partly a “false” rib, partly a floater).
The general theme here is quite a lot more costal margin hypermobility and variability than expected. Even if their findings were exaggerated,2 they would still be important. The authors reasonably conclude that “the 9th and 10th ribs are not invariably attached to the costal margin as described in anatomy books.” Consistent with all that floating and messy looseness of the lower ribs, Laswi et al. also found plenty of subluxations and free and “upwardly hooked tips” — all potential sources of discomfort and pain, maybe downright likely sources. If free rib tips are more common than anyone realized? Well, then so are their problems.
The new normal: three floating ribs, not two
All of Laswi et al.’s findings may be anatomically significant, but the floating tenths is a bit of bombshell. The paper is respectably calm and professional about it. I can make more of a fuss about it here.
No one should be surprised that there are a few 10th ribs floating around out there — anatomical quirks are legion3 — but more than half? That’s the surprise. That’s not a “quirk”! If true, it clashes with the textbooks, and redefines “normal.”
Redefining normal is tight. (That’s a reference to a running gag on my favourite comedic movie review channel, “Pitch Meeting.”) It’s really neat when research challenges extremely long-term assumptions about anatomy!
Look at most model skeletons or anatomical diagrams and they will show just two floating ribs. I checked several standard sources, and they all described only an 11th and 12th floating rib, with the occasional mention of “rare” 10th floaters. Above the 10th, the 9th rib is always depicted as a nice tidy false rib, merging with the cartilage that links it to the sternum.4 Extra floating ribs are often said to be common in the Japanese, a claim mentioned all over the Internet, but supported with only one dubious old citation that I have not been able to find.56 Wikipedia’s rib cage page mentions floater variation, but only barely — 10th floaters occur “sometimes” in “several ethnic groups, most significantly the Japanese” — and citing just a textbook (not the Japanese study). But they do show the original, vintage version of Gray’s ribcage … which does include three floaters! Interesting.

Most anatomical diagrams of the ribcage show only two floating ribs — as is normal. There are probably exceptions, but this is the only one I know of: the original, vintage Gray’s Anatomy, plate 112. Notice how sharp they look! Eek!
But in all the modern renderings I checked, both the 9th and the 10th are tidy false ribs, with no free tips. The reality as reported by Laswi et al. is far messier and looser, with way more 9th and 10th rib tips roaming free than anyone has ever known.
I have to turn in my “freak” card
Bonus rib messiness (not covered by Laswi et al.): there’s sometimes even an extra floating rib: the 13th! (“Thirteen!” ~ Titus and Pullo, HBO’s Rome)
Several years ago, I discovered that I have both a floating 10th and a stubby little floating 13th. I marvelled at how I’d missed those oddities for so many years — but who counts their floating ribs?! Not even me, not even with a long history of weird rib pain and a keen interest in anatomy. It simply did not occur to me.
Based on conventional anatomy, I assumed that my floating 10th was relatively rare. But with the 60% incidence identified by Dr. Eriksson’s group, a floating 10th is not just a quirk … it’s actually how the spine models should be built! It’s what should be in the texts! 🤯 Even if another study found “just” 40%, it’s clear that this anatomical bug/feature is actually much more common than red hair, hazel eyes, or having a tongue long enough to touch the tip of your nose. There are clearly a lot of floating ribs out there — probably a lot more than most physical therapists ever imagined.
I guess I have to turn in my “freak” membership card, because a 10th floater is less exotic than having freckles.
But I have had many of the symptoms of “slipped rib syndrome” off and on for my entire life, gradually worsening over the years. Isn’t “normal” anatomy fun? It’s time to talk about pathology…
“59% of us float down here. You might float, too.”
Pennywise, AKA "It" (Stephen King)
What could possibly go wrong? More floaters = more pathology
Subluxations, slipped rib syndrome, and hooked tips, that’s what. ☹️ Slipped rib syndrome is the catch-all term for a variety of problems related to the looseness of the lower ribs and their stabby floating tips. (This is very similar to Tietze syndrome and costochondritis, but not quite the same thing.7)
These lower ribs aren’t exactly the most stable anatomy to begin with, and the floaters are especially wibbly-wobbly. The lower ribs are more chaotically and loosely attached to each other and the costal margin than conventional anatomy has ever suggested, probably even in healthy young people — and age no doubt makes it worse as their attachments to each other and to the costal margin loosen and break, the ribs sliding under and over each other, and the tips in particular making trouble by poking intercostal nerves.
The end result for many patients is back pain, flank pain, some abdominal, and occasionally even groin pain: “a complex pain response,” as Laswi et al. put it. Unsurprisingly, symptoms are triggered by practically any movement or position of the trunk. Almost any combination of consistency, chronicity, and severity seems to be possible, which makes diagnosis quite challenging. Some people experience dramatic episodes of severe pain, which may last minutes or hours or days, but they may be largely pain-free between episodes — or not! Others may live with milder and more erratic symptoms for many years, never knowing what’s going on.
The symptoms of slipped rib syndrome are as variable as the anatomy, because the pathogenesis equation is freakishly complex. There are at least four ways that these loose ribs can cause trouble:
- Subluxation (partial dislocation) is the most obvious and distinct thing that can go wrong. This is not joint subluxation we’re talking about, not a spinal issue,8 but displacement of the ribs themselves, which can cross over each other like fingers. Laswi et al. found this in 19% of 9th ribs (despite not being true floaters), and 33% of 10th ribs.9 That’s just as startling as the incidence of 10th floaters, and much more direct evidence that associated pathology is probably also more common.
- Intercostal neuropathy occurs when a rib subluxation pinches an intercostal nerve. This usually feels like a burning pain in a stripe around one side of the torso, but it’s not always that simple. For instance, the twelfth intercostal nerve is linked to the first lumbar nerve … which results in bonus neuropathy: pain in the lower abdomen and groin! And so we get a sub-type of slipped rib syndrome: twelfth rib syndrome.
- Inflammation around rib tips. A rib tip does not have to pinch a nerve to cause trouble. Any rib with a pointy end — paging Arya Stark — can irritate the tissue around it.
- Cramping, exhausted, and sensitive muscle is another likely factor — certainly as a complication, and possibly also a cause or perpetuating factor. The body probably tries to stabilize/immobilize painfully displaced ribs by tightening up the area, which might lead to fatigue and irritation as a consequence. The intercostal muscles in particular can become extremely sensitive. And muscle dysfunction (cramping and/or weakness) might also predispose someone to subluxation in the first place. How many ribs have been pulled out of place?
If there are more floating ribs than we thought, with more free tips… then all of these predicaments are probably also more common and more severe.
“Stick ’em with the pointy end.”
Arya Stark, Game of Thrones (George RR Martin)
Hooked tips on the tenths
Another interesting variation that Laswi et al. found was hooked tips on 10% of 10th ribs — quite common. One in ten people is plenty of people.
The hook is a cartilaginous extension to the 10th rib that curves upwards towards the 9th.10 This is actually nicely depicted in the Gray’s drawing above: that wicked-looking curved extension to the rib!
The hook is clearly just an incomplete cartilaginous connection to the costal margin: rather than merging with the rib or cartilage above, it falls short of it to some degree, making the 10th a floating rib rather than a false rib … but a floating rib with a barb of cartilage pointed directly at the underside of the 9th rib! And free to slip over or under it.
Indeed, over 60% of 10th ribs with hooks were also displaced. Do you know where the tip of your 10th rib is?
Are rib subluxations “a thing”? Skepticism about the skepticism
I have seen several knee-jerk skeptical takes about rib subluxations over the years, overconfidently declaring that they are “not a thing.” Scoffing at the unknown is not exactly skepticism putting its best foot forward. Like so many other things in musculoskeletal medicine, it simply hasn’t been studied much. As Laswi et al. have shown, we didn’t even have the basic anatomy!
The skepticism is mostly aimed at subluxations of the joints between the spine and the ribs, and tends to ignore displacement of rib bodies. I have certainly had my own suspicions about those kinds of rib subluxations, mainly because of their conceptual and anatomical proximity to intervertebral subluxations and some of the worst chiropractic nonsense that has come from that idea. But I carefully, consciously curbed my skepticism until I knew more … and I wish skeptics as a group would do more of that. It might help a bit to undo our strong reputation for throwing babies out with the bathwater.
Granted, there are probably far more chiropractors opportunistically exaggerating the importance of rib subluxation, and profitably overstating their ability to fix it, than there are skeptics cynically underestimating it and rolling their eyes.
But I’m now “fairly” sure that the truth is in the middle: clinically significant rib subluxations probably exist.11
Therapy for rib subluxations
I am not aware of any evidence-based conservative therapy for rib subluxation, but we can easily apply some sensible principles to the problem. Self-treatment may even be preferable to trying to get professional help — because professional help could easily be overkill, adding hassle and expense for very little additional gain (to say nothing of the perpetual risk of wasting money on all the silliness that pollutes all the physical therapy professions).
The same looseness that makes these joints prone to trouble might also mean that — for some lucky patients — it’s relatively easy for them to go back where they belong. There are at least four things that have the potential to normalize rib position:
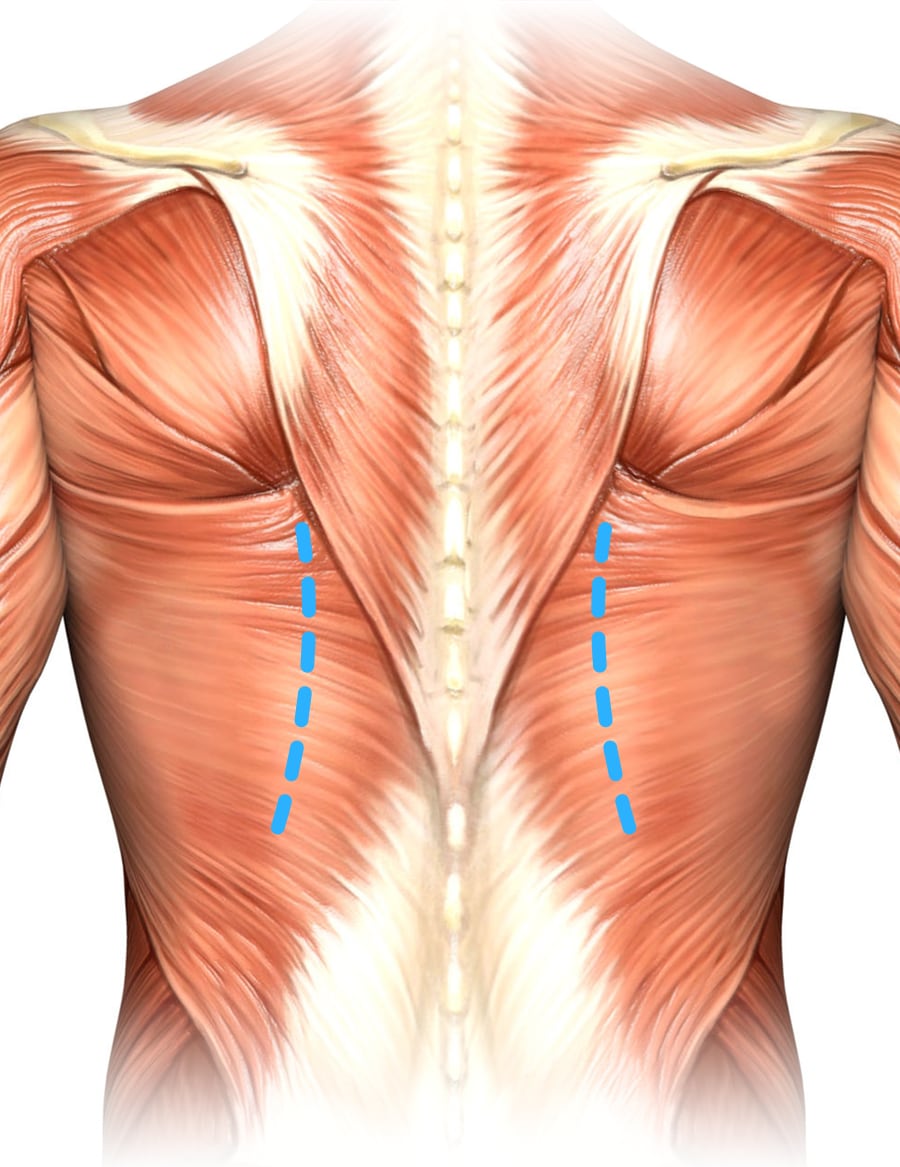
To mobilize the costovertebral joints (not the main focus of this article, but relevant), apply pressure along the spine, roughly 2–4 inches from the centre.
- Mobilizations, AKA dynamic joint mobility drills. Rhythmically twist, bend, flex, and stretch the lower back and abdomen.
- Use a foam roller or ball on the back to flex and push the rib joints around a bit, with pressure beside the spine. The posterior rib joints are not the focus of this article, but I think they are relevant: they are the fulcrum for rib movement.12
- Massage the intercostal muscles … as best you can yourself, or with professional help. It’s easy to get a thumb between the ribs on the front for self-massage. It gets more awkward the further around back you get, and the higher you get — and less relevant? But, again, I do think the posterior is relevant — the intercostals back there also have a significant influence on rib position.
- Hot soaking. Any relaxing heat might be helpful, but in this case actual immersion might be helpful, because of the supportive buoyancy. (Never use heat if it’s not appealing. It could harm rather than help, if something is sufficiently inflamed. However, I suspect that’s quite rare, and in most cases bath-heat will be fine or appealing.)
For bonus points, combine the last two — massage in a bath! Specifically, roll on a rubber ball beside the spine to flex those rib joints in that warm, safe-feeling, buoyant context. This is The Bath Trick for Trigger Point Release, which I wrote a whole article about many years ago.
These are all just ways of relaxing and wiggling the anatomy. If you can think of others, by all means go for it.

Allan Saltzman’s simple but particularly firm “spinal rollers” (YogaTools.com) are ideal for flexing the rib joints… but the softer common kind you can get just about anywhere now are also fine, and more comfortable for many people. But, for this purpose, I quite like my sturdy roller.
Notes
- Laswi M, Lesperance R, Kaye A, et al. Redefining the costal margin: A pilot study. J Trauma Acute Care Surg. 2022 Dec;93(6):762–766. PubMed 36121266 ❐
- There are two main ways that Laswi et al. may have found more hypermobility in the cadavers they studied than actually exists in living people, both of which they acknowledged. First, their subjects were quite old, an average age of 83 years at the time of death. Second, their dissection techniques could have actually created some of the hypermobility they observed. But none of that would affect their most amazing result: the extremely high incidence of floating tenths.
- Strange, wonderful, and problematic anatomical variations occur in humans all the time. The best anatomical diagrams depict average anatomy only, and sometimes they are even wrong about what’s average — which is what this post is all about. The line between “normal variation” and “defect” is very blurry. We often make a fuss over the visible anatomical variations — too much of a fuss in many cases (“structuralism”) — while neglecting more common invisible oddities that may well matter much more. Such cases often join the “X-files” of therapy, the unsolved clinical mysteries that every pro encounters. Floating ribs are an excellent candidate example of this. “For every visible, superficial oddity, there may be an invisible internal one… and only surgeons ever find out about them” (Dr. Sherwin Nuland). See You Might Just Be Weird.
- For instance, a modern edition of the classic textbook, Gray’s Anatomy, shows and definitively describes only two floaters in numerous diagrams, with no mention of variation at all. Same with Netter’s Atlas of Human Anatomy, which is next in line for “most famous anatomy text.” I have both of these texts in my library, and I dusted them off for this (literally).
- Shimaguchi S. Tenth rib is floating in Japanese. Anatomischer Anzeiger. 1974;135(1-2):72–82. PubMed 4416068 ❐
- Mysteriously, PubMed answered my search for floating rib data with just one other weird item, in addition to the Japanese study: “Insect succession on a decomposing piglet carcass placed in a man-made freshwater pond in Malaysia,” which chronicles the lives of insects on said floating carcass for, you guessed it, ten days. “The carcass along with the maggots sunk on day tenth [sic, and probably the reason for the weird result], leaving an oily layer on the water surface.” Search tech is tricky.
- Both Tietze and costochondritis affect the junction of the sternum with costal cartilage. Tietze tends to be worse: it’s associated with ominous causes like infection, autoimmune disease, cancer, and occurs mostly in the upper ribcage. Costochondritis is more like an arthritic flare-up: milder and more evenly distributed. Slipped rib syndrome is clearly a sibling condition, but it doesn't affect a connection between rib and sternum.
- The costovertebral joints in back may also get irritated, with or without subluxation — in the same way that I don’t have to dislocate a knuckle for it to ache with arthritis. But Laswi et al. only studied the costal margin.
- That was the number whether the rib was floating or not, and not all of those subluxations were internal subluxations. Not all subluxations displace the rib inward (which is the only way an intercostal nerve can get squeezed.)
- A more exact description by Laswi et al.: “In the experience of the authors caring for patients with slipped rib syndrome, many of these patients have a ‘hook’ tip of the 10th rib. A ‘hook’ tip on the 10th rib is a cartilaginous tapering to the rib that curves up towards the 9th rib at an acute angle compared with the normal curvature of the 10th rib.”
- A proper ontological audit would call for a whole ‘nother article, and I will probably write it someday. But today is not that day. For now, I will just say that I have seen enough evidence-based reasons to suspect that rib subluxations are a legit phenomenon … along with an awful lot of anecdotes that are hard to explain without rib subluxations. Including quite a few of my own experiences. I have much less faith that anyone can reliably put those joints back where they belong, but I’m now quite confident that the need is real.
Pressure directly beside the spine will mostly be wasted, because the joint is hidden behind thick muscle and the transverse process of the vertebrae. You have to press on the ribs a little further out, roughly 2-4 inches from the centre — roughly where you can first feel them as they emerge from behind the thick column of paraspinal musculature right beside the spine. You cannot actually press on the joint directly, so instead you push on the rib as close to it as you can get. This happens quite naturally and easily with a foam roller, because these ridges “stick out” and the roller naturally falls onto them.