Barefoot walking for plantar fasciitis: better than I thought? (Member Post)
“Barefoot walking” is not something I would ever have thought to prescribe for plantar fasciitis. In fact, I probably would have warned readers not to do that! But now a surprising new study suggests that I might need to change my tune.1 The results are of practical interest to anyone with persistent arch and/or heel pain.
Or… maybe it was just that all the walking was on treadmills? The same test of barefoot walking on concrete might have been a huge mistake!
For members only today, I will explore the paper and its implications for about 2000 words (5-10 minutes reading). I’ll explain why the study results seem so surprising… and then I’ll turn that around and explain why they probably aren’t so surprising after all … but for a surprising reason. I also dig into overuse versus dis-use, a digression relevant to many injuries.
This post is also a new chapter of my plantar fasciitis book ($20, large free intro).
“That’s a really good overview.”
Asaf Weisman, one of the authors of the paper (no really, he did say to that to me)

Three legs are better than two? I have yet to get much use out of any of the AI image generators — they have so many conspicuous glitches that I have mostly just given up in disgust. In this case, I was able to produce some useful images… but I decided to stick with this three-legged version just for giggles.
Most PainScience.com content is free and always will be, but there are members-only zones scattered around the site, delivering "deep dive" info for my most curious readers, both patients and pros.
- “Good” members get all premium posts for $3/month or $30/year, but only by email on publication (new sign-ups will receive the most recent post).
- “Better” and “awesome” members ($5 and $10/month) get much more: web access to all posts and the archives, podcast, full-text RSS feed, and lots of members-only areas in the main PainSci library. For details, see the membership page. ❐
Buy Good, Better, or Awesome PainSci Membership…

Change or cancel plans with ease. Payment data handled safely by Stripe.com. More about security & privacy. PainScience.com is a small publisher in Vancouver, Canada, since 2001. 🇨🇦
The salamander’s domain is for people who are serious about this subject matter. If you are serious — mostly professionals, of course, but many keen patients also sign-up — please support this kind of user-friendly, science-centric journalism.

Some background: the barefoot running fad
I have heaped skeptical scorn on barefoot running for many years as “the biggest fad in running since running itself,” a topic rife with bullshit, and plenty of evidence that it doesn’t actually prevent injury (the main reason people do it). Indeed, there is good evidence that it produces no important difference in injury rates, just the types of injuries.2
But I’d never even considered the possibility that more modest doses of “natural” running or walking might be therapeutic. Reinstein et al’s experiment encourages me to reconsider.

Vibram FiveFingers were so easy to make fun of!
{kind=link}
And some plantar fasciitis basics
Plantar fasciitis is foot arch tendinitis, an overuse injury — that’s an oversimplification, but good enough to start. Arch support is a relief to most people with plantar fasciitis, because it relieves strain on the inflamed, overworked connective tissue of the arch. Arch support is more of a Band-Aid than a cure for most people, but there’s no doubt it’s a relief to many patients because it’s taking load off the arch. For the record, I speak from personal as well as professional experience (as I often do). For some people, a little arch support and taking it easy for a while actually does the trick.
Barefoot walking seems like the opposite of giving the arch a rest. So why would it help plantar fasciitis? Especially in less than a month!
The new barefoot walking study
Reinstein et al. hypothesized that barefoot walking would reduce pain and improve function in people with plantar fasciitis. They compared the short-term effects of a 4-week barefoot walking program to walking in shoes.
| title | Barefoot walking is beneficial for individuals with persistent plantar heel pain: A single-blind randomized controlled trial |
|---|---|
| journal | Annals of Physical and Rehabilitation Medicine |
| Volume 67, Number 2, Mar 2024, 101786 | |
| authors | Miriam Reinstein, Asaf Weisman, and Youssef Masharawi |
| links | publisher • PubMed • PainSci bibliography |
They studied 52 people with plantar fasciitis, split evenly between two groups, one with shoes and one without. The shod group used their own comfortable sports shoes, while the barefoot group had truly naked feet: no shoes, no socks! This was all on a treadmill (a key detail, because treadmills are quite a lot springier than sidewalks). Everyone walked for 10 minutes for each of two weekly sessions at first (super easy!) ramping up to 30 minutes by the end (a fair bit for people with stubborn foot pain).
Everyone also got a dose of therapeutic ultrasound after each walk — a notoriously popular-but-ineffective therapy,3 and included in this experiment “to comply with ethical standards.” Apparently it’s unethical to withhold a useless treatment from patients with sore heels?
The main thing they were looking for was an effect on function, as measured by the “36-Item Short Form Health Survey,” a way to measure of changes in quality of life related to health issues. They also measured heel pain and tenderness specifically.
The promising results
Function improved for everyone, but the gains were greater for the barefooters. Heel tenderness and pain tolerance also improved, while not budging at all for the shod group. Reinstein et al.:
The current study demonstrates that adding a 4-week barefoot and shod walking program on a treadmill to standard care (therapeutic ultrasound) is beneficial for people with PPHP. The results also indicate that walking barefoot is associated with even greater improvements in pain levels and function than walking when wearing shoes.
Good news in research is often like an unjust “technicality” in a court of law,4 but in this case the barefooters’ win seems to be based on what we’d like to see: results anyone can feel, a meaningful improvement. This was not merely a “statistically significant” win (a low risk of a false positive, the p-value, a notoriously “hackable” and abused number). It was a good “effect size” (a Cohen’s d score of .89 for pain, which is considered “large”).
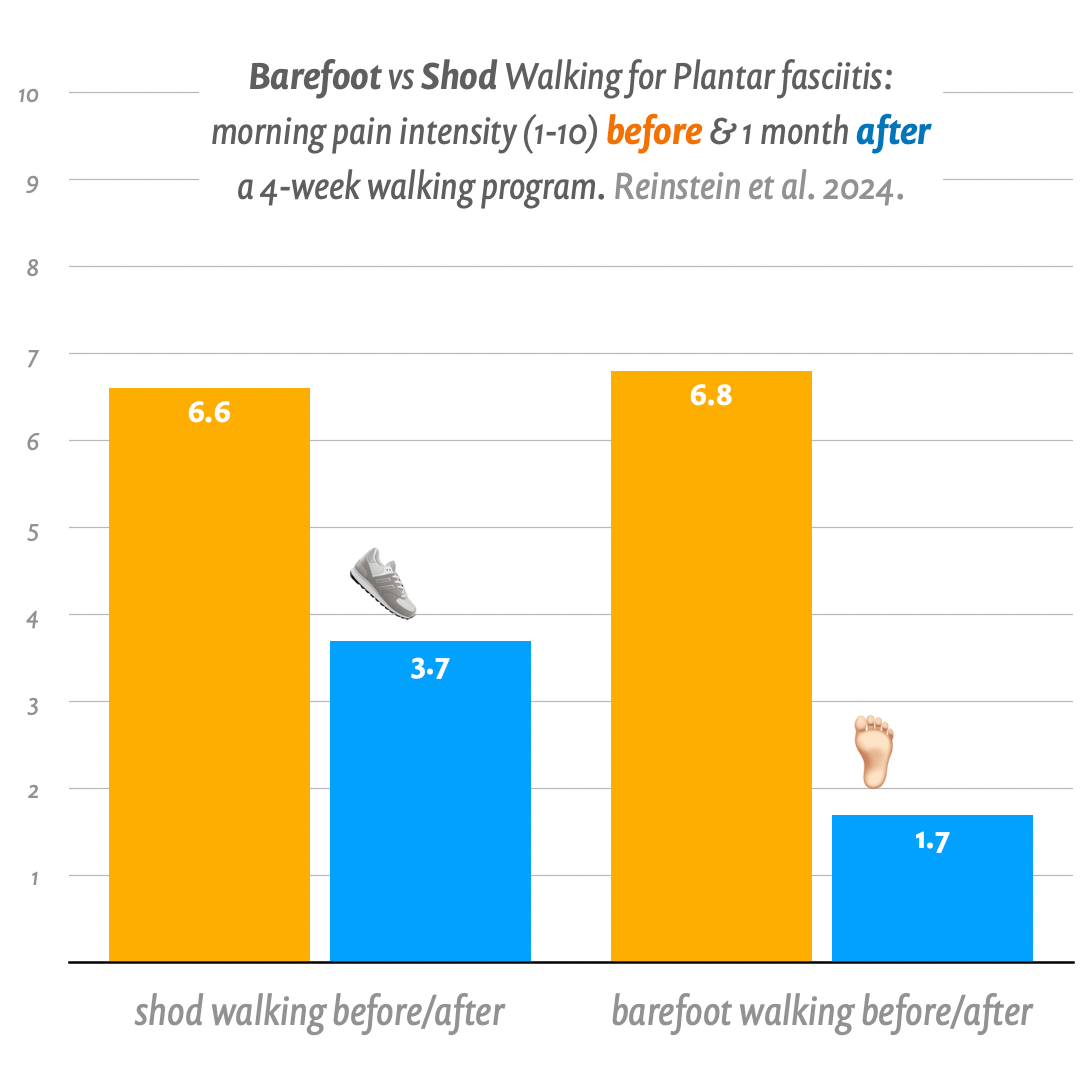
The barefooters’ pain dropped 5.1 points on a 10-scale, compared to just 2.9 for the shod (that’s using the numbers at follow-up one month after the end of the walking program). That 2.2-point difference is what counts here. It’s not huge, but who doesn’t want those two points? No one, that’s who.
And what number did they actually end up at? How much pain when the feet hit the floor in the morning, plantar fasciitis’s most classic symptom?5 The shoe-wearers got down to 3.7±2.6, and the barefooters 1.7±1.8.
Everyone still had some pain and limitation, but it was getting down to pretty minor levels for the barefooters. Wow. Cool.
Looks good. Next time I have plantar fasciitis, I want to experience a drop in pain like that.
Are the results really surprising? Many of you have been thinking, “well, duh”
The possible power of barefoot walking to treat plantar fasciitis does not seem like a surprise to a lot of people. Admit it, you thought, “Well, duh!”
But this is mostly because of a pro-barefoot bias, and the more general love of all things “natural” or “paleo,” of doing anything at all the way our ancestors did it. That’s belief catnip for a lot of people. This is why it’s a strong theme in so many health and fitness fads.
So people who already think very well of barefooting for any reason have been telling me “I’m not surprised,” because — they think — of course walking barefoot “makes your feet stronger” or “toughens them up” or “desensitizes them” or “squirts rainbows out your toes” or whatever. I’m not necessarily dismissing those explanations for the positive results of this study, but I am taking them with a grain of salt the size of a cinder block because I do not share the pro-barefoot bias.
My bias is against barefoot anything as a health practice (see above about barefoot running as a fad). Which doesn’t mean I think that nothing good can ever come of shucking your shoes; it just means that I lean away from thinking “naturally barefooting did well.” After twenty years of deconstructing health fads, and finding the naturalistic fallacy at the heart of so many of them, I’m pretty much done with assuming that something is good just because my Great Uncle Thag did it that way.
I also know, having read the study carefully, that “toughening up” the feet is not actually the most plausible explanation for the good results (more about that shortly).
So why was I surprised? Why was a barefoot skeptic surprised that barefoot walking seemed to help plantar fasciitis? Seems obvious when I put it that way, doesn’t it? But that’s just the reason that I’d never even considered the possibility that more modest doses of “natural” running or walking might be therapeutic.
The specific reason I was surprised by the results of this study is that barefoot walking seems like the opposite of giving the arch a rest. It’s giving a screaming, exhausted arch more to do. So why would that help plantar fasciitis? Especially in less than a month!
That is why I was surprised. Initially. Since you were well-duh wondering.
Maybe not as surprising as it seems at first (but for a surprising reason)
So the results were surprising for the simple (to me!) reason that it seems like barefoot walking would increase load on the arch of the foot — which is the last thing any overuse condition needs. Right?
But I suspect the explanation is that it actually did not increase load on the weakest link in this chain. Surprise! This was probably just a case of load management in disguise, and I like the authors’ educated guess:
"This may be explained by the fact that the biomechanics of barefoot walking transfers force absorption to the front of the foot and decreases pressure on the heels. Our 4-week walking program may have allowed the heel tissues sufficient time to recover and desensitize."
In other words, barefoot walking may have shifted much of the burden to the healthier tissues of the forefoot. Thus the overwhelmed tissues got only a little just-right stimulation — and even overused tissues still need some use, and almost certainly benefit from it if the dose is just right.
That’s better, DALL-E! This is officially the first time I have gotten more or less what I wanted out of one of the image generators relatively easily. This was produced “only” on the seventh try. Others were rejected for things such as bizarrely hairy men’s legs, a kooky foot deformity, facing sideways on the treadmill, and a cyberpunk treadmill!
Over-use vs. dis-use
So-called overuse injuries, AKA “repetitive strain” injuries, are not always just a matter of obviously overdoing anything. Overuse is always relative to what the tissue can handle. One person’s “overuse” can be completely fine for another person, for a host of reasons, including subtle genetic, metabolic, and pathological variables.
But the most common reason that a tissue might be fragile and vulnerable to overuse is … just not using it enough!
That isn’t quite the paradox it sounds like. Connective tissues weaken with neglect. Use it or lose it.
I strongly suspect that the relative-overuse of degenerated arch tissues is common with plantar fasciitis — because lots of people have cruddy, under-exercised arches — and so that might be why the results were so good here: because barefoot walking is a nice way of exercising the arch in the Goldilocks zone.
So am I going to start recommending barefoot walking as an evidence-based treatment method?
Nope! No study is perfect, and even a perfect study could be wrong by fluke. That barefoot group could have been polluted with several easier cases completely by chance — which wouldn't be anywhere near as rare as a 29-hand in crib. Such flukes happen in science surprisingly often, and it’s one of the main reasons that good news always needs replication.
This study was good — better than most — but it could have been larger, and would have been greatly improved by diagnostic imaging, a control group only receiving ultrasound therapy, and more control over confounding factors.
For instance, I think it’s all-too possible that the treadmills are a fly in this science ointment. We have good evidence that the springy structures in the lower limbs have less work to do when we are walking on a springy surface (a topic I discuss in detail in my plantar fasciitis book). That might be why the barefoot strategy succeeded. It’s plausible that barefoot — minimally shod, no arch suport — walking on pavement (sidewalks) would have been not just ineffective but risky. I’d really love the see the same test done without treadmills.
Still, it’s not like walking barefoot is going to be a disaster or anything. I won’t “recommend” it based on this evidence alone, but I’ll certainly start telling readers that barefoot walking might be useful — and it’s not foolish to consider trying it. I will definitely upgrade it from “just seems like a bad idea,” to “maybe worth trying … especially on a treadmill.”
Notes
- Reinstein M, Weisman A, Masharawi Y. Barefoot walking is beneficial for individuals with persistent plantar heel pain: A single-blind randomized controlled trial. Ann Phys Rehabil Med. 2024 Mar;67(2):101786. PubMed 38118297 ❐ PainSci Bibliography 51689 ❐
- Altman AR, Davis IS. Prospective comparison of running injuries between shod and barefoot runners. Br J Sports Med. 2016 Apr;50(8):476–80. PubMed 26130697 ❐
I waited a long time for this one: at last, the first prospective comparison of injury rates in shod versus barefoot running. All research on this topic until now has been unable by design (methodologically inadequate) to answer this question, and so for many years now we’ve endured tedious argument about injury rates based on the wrong kind of data. “Prospective” is what we needed the whole time: following a bunch of initially uninjured runners of both types to see what happens to them.
For this test, 200 experienced runners were studied over the course of a year: 94 wearing shoes, 107 with no shoes or (for about a quarter of their mileage) “true minimalist shoes.” The barefooters had been running that way for at least six months, and more than 18 on average, so they weren’t in that awkward transition phase where injury rates could well be higher.
The results are clear and unsurprising: there was no important difference in injury rates, just the types of injuries. Each is better in some ways, worse in others. Although the paper emphasizes “fewer overall injuries” for barefoot runners, injury rates are what matters — the number of injuries per 1,000 miles, say — and they were “not statistically different between groups due to significantly less mileage run in the barefoot group.”
But there’s an extremely important caveat, and it does not flatter barefoot running: the barefoot running volume was just 24 kilometres a week, while runners in shoes ran nearly twice as much — 41km — without an increase in injury rate. Although this is all made clear in the paper, it’s strange that it wasn’t more strongly emphasized. As Alex Hutchinson put it for Runner’s World, “The only way the comparison has any relevance is if they’re arguing that barefoot running reduces injuries by preventing you from running as much as you’d like.”
Naturally, a larger, longer study may have different results. But this is an excellent start, and we can now say with high confidence that barefoot running is not a panacea for running injuries.
- Ultrasound and shockwave therapy are used to treat injuries like tendinitis with sound and/or pressure waves that warm, vibrate, and even harm tissues a little to “kickstart” healing. Ultrasound has been popular for decades, and almost defines the experience of physical therapy for many patients, but it has been undermined or damned with faint praise by every scientific review for decades. Shockwave therapy is now supplanting ultrasound, but it’s over-hyped, unproven, more expensive, and often painful. See Does Ultrasound or Shockwave Therapy Work? They seem like mainstream physical therapies, but warming and vibrating tissues with sound/pressure waves has never been supported by good evidence.
- The word “significant” in scientific abstracts is routinely misleading. It does not mean that the results are large or meaningful, and in fact is used to hide precisely the opposite. When only “significance” is mentioned, it almost invariably refers to the notoriously problematic “p-value,” a technically-true distraction from the more meaningful truth of a tiny “effect size”: results that are not actually impressive. This practice has been considered bad form by experts for decades, but is still extremely common. See Statistical Significance Abuse: A lot of research makes scientific evidence seem much more “significant” than it is.
- Specifically they measured “VAS score (0−10) during first steps in the morning,” a very distinctive symptom of plantar fasciitis. This was one of the *secondary* outcomes of the study, but — I believe — the best overall indicator of how bad a case of plantar fasciitis is, and the number most people care about the most.