Don’t get caught in the corrective exercise trap
“Corrective exercise” is the idea that specific exercises can be prescribed to fix alleged performance deficiencies and injury risks. It’s often pretentious, because it implies that ordinary exercise and training isn’t good enough. And because it needs something to correct, it slips all to easily in pathologizing and nocebo (harm from negative expectations).

“The Corrective Exercise Trap” (plus bonus content), an article in Personal Training Quarterly, decisively but very gently and diplomatically tips over this most sacred cow of personal training and therapy. “The danger here” — the trap! — “is that many fitness professionals might end up making their training process more about a formalized evaluation procedure and less about good personal training.”
It is “really about the particular evaluation procedure—the performance standard used to drive exercise prescription decisions” and the belief that “properly applying good personal training practices is insufficient for finding a safe and individualized training direction.”
How are deficiencies and risks identified anyway? Can anyone actually do that, and — even if so — can precise exercise prescriptions actually solve anything?
In order to spot a physical flaw that needs to be corrected, one must begin by having a reliable measure of whether or not it is actually problematic in the first place.
Spoiler alert: there is no such reliable measure! Corrective exercise is built on wishful thinking. Screening for movement dysfunctions has been failing one fair scientific test after another. The importance of posture has been wildly exaggerated. The importance of anatomical variation has been virtually ignored.
Although it is often assumed that identified so-called “dysfunctions” in posture, movement quality, or body function are reliably predictive of potential injury and performance, the preponderance of the scientific evidence casts a great amount of doubt on any claims about the strength and reliability of such relationships. This is because natural variations in human posture, movement and mobility/flexibility make identifying strict ideas of what is “correct” difficult and possibly invalid in many cases. Humans naturally move in different ways to accomplish different tasks, and identifying small variations in that movement as a “dysfunction” may not be very useful or helpful.
The practical implications of this are that the fitness professional should not immediately qualify a movement pattern as a dysfunction just because it does not fit within certain standards of a given corrective exercise evaluation, and that fitness professionals can better appreciate that exercise in general is far more valuable from a therapeutic perspective than is often thought in corrective exercise belief circles.
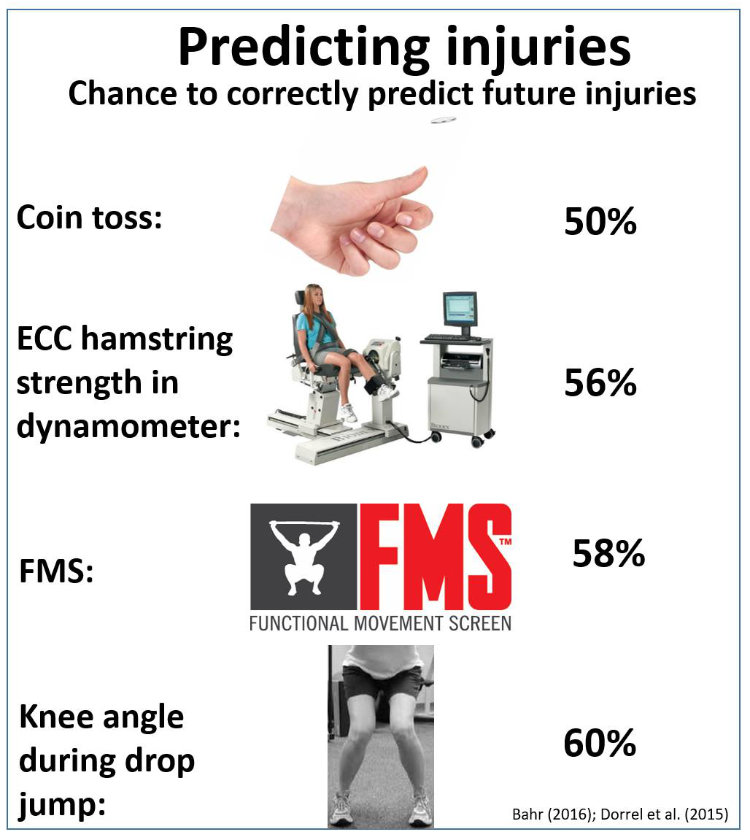
It’s 2017, and we still know very little about risk factors for common musculoskeletal injuries, and even less about identifying them in specific patients. In broad strokes, this is probably because the real risk factors are just invisible to the average personal trainer, physical therapist, or sports medicine specialist: psychological factors, social factors, genetic factors, pathological factors like chronic systemic inflammation that boost vulnerability, and so on. Thanks to Bas Van Hooren for the graphical interpretation of the evidence from Bahr and
Authors Nick Tumminello, Jason Silvernail, and Ben Cormack all have excellent credentials and top notch clinical reasoning skills. These are smart guys tackling several thorny sub-topics like postural dysfunction, movement dysfunction, core stability, and — most important of all, I think — the “nocebo concerns” with corrective exercise:
As the allied health fields understand more about pain and injury, allied health professionals appreciate the influence of patient/client beliefs on their risk of injury and pain and their likelihood of recovery. Specifically, patients/clients with beliefs about their body that center on fragility/risk of harm, the importance of appropriate posture, or the need to move in specific ways to avoid injury are more likely to have pain and less likely to recover from a future problem. That is the opposite of the kind of physical and psychological resiliency that personal training is designed to build. With this evidence in mind, allied health professionals also understand that when clients are told such things about themselves from an authority figure (as they might be during some corrective exercise evaluations), that this potentially makes one’s clients less resilient and more prone to injury and pain. The authors suggest that fitness professionals who choose to use corrective exercise evaluations to guide their exercise prescription decisions consider this concept carefully, and relay evaluations to clients with carefully chosen words that are less likely to make the client think their bodies are fragile and prone to injury if they do not lift, bend, move, sit, or stand the way that the corrective approach or program suggests is best.
Translation sans diplomacy: stop #%&^ telling patients they are fragile and weak!
All of this is the same kind of thing I’ve been writing on PainScience.com for years, primarily in my article on structuralism, but the key points about it come up everywhere (that article is cited by 48 others on the site). So it’s nice to have such credible backup.