Muscle Pain as an Injury Complication
The story of how I finally “miraculously” recovered from the pain of a serious shoulder injury, long after the injury itself had healed
In the summer of 2008, near the end of the years I spent working as a Registered Massage Therapist,1 I tore up my acromioclavicular joint, a shoulder sprain, a difficult injury to recover from. It became the eye of a storm of muscle pain in the area that lasted for months longer than the sprain alone would have caused pain. I had serious trouble for many (sleepless) months with my body’s reaction to that sprain — all much worse than the original injury. To this day, 18 years later, I still have flare ups of trouble in that area. Fortunately, I can always put out the fire with basic trigger point therapy tactics, especially self-massage.
This article uses the story of my injury as a good example of how injury rehabilitation might be worsened and prolonged by muscle pain, or even perniciously replaced by the original problem.
Two kinds of hurt
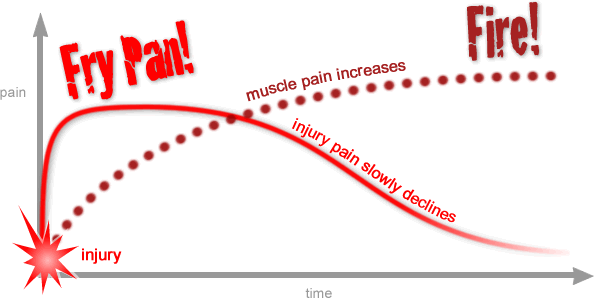
First the pain of an injury (the frying pan), and then the pain of seriously irritated muscle (the fire). A much more detailed version of this graph is presented at the end of the article.
The injury story
I got hurt when I tried to stop someone else from catching a Frisbee, playing goaltimate (a variation of the intense Frisbee sport, ultimate2). I leapt high in the air, tumbled clear over the other player who was catching the disc, and fell a couple of feet onto the tip of my shoulder. It should have been a collarbone cracker. My ligaments tore instead.
My acromioclavicular joint, on the shoulder-end of the collarbone, gave way with a wet rip. And over the last several months of healing, that injury gave me an opportunity to test and practice much of what I preach.3
Just to add insult to injury … the other guy caught the Frisbee. And scored. Winning the game. (Now that’s painful!)
Sprains: one of the most difficult injuries
A ligament tear is called a “sprain.” Joints are held together by both muscle and ligament. When ligaments tear, it causes severe pain, and takes a minimum of many weeks to heal. A serious sprain can leave a joint more or less permanently damaged — people often talk about never really recovering from their sprains. Sprained joints are never quite the same again.
Ligament is tough stuff, but once it is torn, it just does not heal particularly well.
I knew I was in trouble, because my joint was so damaged that it was loose — a sure sign of actual ripping. Yikes. I could feel the joint moving in a disturbing way, clunking and bulging and almost dislocating and causing vicious, sharp pain with every unwise attempt to use my arm.
I could barely drive home from the field. I probably shouldn’t have.
I couldn’t lift my arm more than a few degrees. I couldn’t sleep on that side … for months to come.
Muscle pain as a complication of injury
“Muscle pain” usually takes the form of acutely sensitive patches of muscle tissue associated with aching and stiffness, and sometimes a palpable lump or “trigger point.” Trigger points, colloquially known as muscle knots, are linked to a lot of world’s aches and pains, and can be amazingly fierce. Their nature is unclear, but the dominant idea is that they are basically “micro cramps.”4 This is a complex, fascinating, and controversial phenomenon; this article is partially excerpted from my advanced tutorial, The Complete Guide to Trigger Points & Myofascial Pain
Trigger points seem to be a routine complication of most injuries. In the aftermath of an injury, pain and stiffness in the area often increase significantly. At first, this isn’t surprising: inflammation and sensitization are normal features of wound healing. Spasm and fatigue of muscles around the injury may also play a role, but already we’re venturing out on a scientific limb here (more on this below).
This appears to be what happened to me. Before I continue the story, a little more about the phenomenon:
How does injury trigger trigger points?
It’s an article of faith among trigger point therapists and experts that injury can “activate” trigger points — a trigger point trigger — along with almost any other source of stress:
Trigger points are activated directly by acute overload, overwork fatigue, radiculopathy, and gross trauma. Trigger points are activated indirectly by other trigger points, visceral disease, arthritic joints, joint dysfunctions, and emotional distress.
Siegfried Mense, David G Simons, and IJ Russell, Muscle pain: understanding its nature, diagnosis and treatment, 2000 p. 213
Like the Dude said: “Yeah, well, that’s just, like, your opinion, man.” Unfortunately, it’s never clear what statements like that are actually based on. Probably because they aren’t based on much of anything.
There is not much direct evidence that trigger points are a complication of injury, let alone that they can be worse than the injury itself, as I have claimed. There is some weak/indirect evidence,56 but mostly I’m willing to endorse the dogma based on my own professional and personal observations. It may be largely unsupported dogma, but it is unsupported dogma that fits nicely with my own experience with this subject.
Here are a few possible explanations for why trigger points crop up around a healing injury:
- Muscular reaction to the injury may be exhausting and stressful, making muscles more vulnerable to TrP formation. But note that the idea of “protective spasm” (aka “muscle splinting”) is a bit simplistic and probably only one facet of very complex muscular response to trauma.7
- Inflammation in the region might contribute directly to TrP formation. Although trigger points don’t seem to be especially inflamed, per se, that doesn’t mean inflammation can’t be a trigger.
- When tissue is injured, we immediately develop protective sensitivity that powerfully discourages us from disturbing injured tissue. This sensitization is obvious in the short term with simple injuries, but it definitely can have more sinister chronic effects.8 Our pain threshold may be somewhat lower and funky for a long time after an injury, and that could simply lower the threshold at which trigger points cause discomfort, without actually changing how they work, like rocks exposed by an unusually low tide: they were always there, they just weren’t obvious before.
Whatever causes trigger points to form around injuries, we tend to underestimate their severity and their longevity. Never underestimate a trigger point! They can produce worse pain than most healing injuries, and for much longer. While some trigger points resolve spontaneously, or relatively easily with some treatment, they tend to last and last, especially around injuries — perhaps because even minor ongoing provocation from the original injury constantly “recharges” them. While most injury slowly but surely heals, trigger point pain often overstays its welcome.
Therapist, heal thyself
There is nothing quite like personal experience to really test a complex idea. It offers both much more and much less than scientific research. Nothing can be proven from personal experience alone, but the subjective data it supplies is rich: a torrent of sensory data to parse and correlate with my detailed knowledge of the subject. Many times per day I had the opportunity to compare my expectations with my experience.
It was almost worth being injured. 😜
I knew within days that I was growing a nice crop of trigger points around my injury. I also knew that there wasn’t much I could do about it, at first — even if I relieved the trigger points, the joint would still be very sensitive, and the trigger points would quickly come back. So I did some basic therapy for trigger points to try to keep the area healthy, but mostly I just waited for the joint to slowly calm down, which it seemed to be doing.
And then I re-injured it.
I had underestimated how messed up and fragile and vulnerable the joint was, and I tore it again, and worse, simply by reaching up for something too quickly. A Frisbee again, as it happens. Oops.
Things get ugly
After re-injury in late August, the bulk of the autumn of 2008 was a blur of pain. Every hour, every minute was coloured by shoulder misery. I couldn’t sleep on my right side at all, which disrupted my sleep significantly. I couldn’t pull things out of cupboards, couldn’t carry even a light bag, could not do my job without pain, pain and more pain.
Like most injured people, I was adaptable, and founds ways of getting by. I really had to work — my wife and I were still paying for an expensive flooding incident that occurred around the time of the initial injury. I just couldn’t work without pain. My muscles could hold my shoulder together, but they were becoming extremely tired and riddled with trigger points as a result.
I knew, of course, that things might be really bad. I knew I might need surgery to bolt my shoulder back together. I knew that, just possibly, it was never going to heal as long as I kept using my shoulder as a power tool in my work, day in and day out.
But the Great Recession of ’08 had officially started and there was debt to pay, so I opted to watch and wait and hope for signs of progress. If I could detect signs of healing under these circumstances, then they would probably continue, and I could suffer through.
My first attempt at trigger point therapy
In about late September, I took my first stab at serious trigger point therapy. I knew full well that many of my worst symptoms were probably now caused by trigger points. A deep pain had set in, a low rumble that never let up, with a toothachy epicentre that was much more acute, and yet too dull to be the injured joint itself — classic trigger point sensations.
But I was also still getting a lot of sharp stabbing joint pain with incautious shoulder movements. Clearly, the joint was still in a pickle. Would relieving the trigger points really do much? Could I relieve them? Trigger point therapy is experimental, unreliable at best,9 snake oil at worst.
It was worth a shot.
My first impression was really positive. Provocation of trigger points throughout the region felt crazy significant to me. It clearly reproduced not only pain in the shoulder, but associated pain throughout the region. For example, a trigger point in the infraspinatus muscle, way on the back of the shoulder blade was especially impressive: it radiated pain in a spike right into the acromioclavicular joint, almost as if it was causing the injury pain.10
And I got a small but distinct dose of relief. I almost started celebrating. I re-treated several times over the next few days. I threw everything I had at my trigger points.
But the relief was short-lived. I quickly hit bottom. I was still just too injured — there was a distinct limit to what trigger point therapy could do. It was like digging a hole in easy soil for a couple of feet … and then hitting bedrock. The worst of the trigger point pain could be dealt with, but there was that bedrock of ripped-ligament pain that was not budging.
Back to the drawing board.
Will this ever end?
There is a stage in every healing process when the patient begins to think, This is never going to end. I am going to hurt forever.
I had sunk into that state of despair quite quickly. It was only early November. Only two months had passed since the re-injury. That’s not really that long for ligament recovery, which can take months. But by early November, I was starting to fear the worst, and starting to plan for taking time off and pursuing surgery, perhaps because I saw no sign of improvement whatsoever. In fact, if anything, I was worse than ever.
But I was being fooled.
I was being fooled by trigger points. Even after years of teaching this stuff, I was being fooled by trigger points. Damn!
It ends!
In fact, my acromioclavicular joint was healing. In fact, it was healing surprisingly well. I just couldn’t tell. I had transitioned seamlessly from the frying pan of ligament injury to the fire of trigger-point pain … and I hadn’t noticed the difference. They were both really hot and unpleasant.
I did not suspect what had happened until the second week of November, when I decided it was time to “take the edge off” my pain again with a good dose of trigger point therapy … and virtually cured myself overnight.
This time my shovel didn’t hit bedrock. The joint pain wasn’t there to defy me anymore. As my trigger points eased, I simply felt better. A lot better. 90% better.
And it lasted. Because, of course, there was relatively little joint pain remaining to re-aggravate the trigger points.
Why couldn’t I tell the difference? How was I fooled? Don’t the two kinds of pain feel different? They do — but the switcheroo is gradual — by the time that trigger-point pain had replaced sprain pain, I had been feeling a little bit more of the former and less of the latter each day for several weeks.
There’s some interesting neurology that probably also explains it, especially the neurological phenomenon of “convergence.” The brain has difficulty isolating internal pain. The result is essentially a confusing mess of sensation that seems to be coming from several different places, like trying to figure out where a sound is coming from in an echoey room. The brain literally has trouble telling the difference between the trigger-point pain and the injury pain, and starts to treat them as essentially the same message — which makes sense in a way, doesn’t it? It’s basically the same problem. This is why the trigger point in the shoulder blade felt so much like the injury itself — that’s the phenomenon of “referred pain” at work. The brain detects a disturbance in adjacent tissue and it just can’t tell the difference any more.
Convergence and referred pain are really fascinating. For keen patients and physiology students, the full trigger point tutorial discusses convergence in detail, comparing several different prevalent theories about it.
Epilogue and a fun graph of pain
My surprise victory wasn’t transient. The relief was lasting.
I cancelled my plans to take time off work, and there were no more thoughts of surgery. The shoulder has never again been perfect, not by a long shot, and it has probably always been vulnerable to re-injury ever since. But the overall suffering is dropped down to only about 5% of what it had before, and has been that or better ever since.
My experience strongly validated the vital therapeutic principle that muscle pain can replace and supercede injury pain, and create a compelling illusion that the injury isn’t healing. Of course, as long as the trigger points carry on, in a sense it is not “healing” — but whereas the original injury was relatively untreatable and simply required adequate time for recovery, trigger points can almost always be at least partially relieved, and often banished from tissues, especially if they are in an area where there was no history of problems.
To wrap this up, I want to retell the story graphically.
I’ve saved this for last because it’s a complicated scenario and a complicated graph. It probably would not have made an awful lot of sense at the beginning of the article. But, hopefully, the interwoven tales of these two types of pain will now seem quite obvious …

Why this story matters
The crazy thing about muscle pain is that it often becomes worse than the original injury, and it lasts much longer. It’s more than a “complication” of injury — it’s a common consequence of physical traumas, sometimes serious and long-term.
Untreated trigger points can last forever. No one really knows why a trigger point would ever go away, or why it would stop once it’s started. Fortunately, they often do go away. But they often don’t! And they especially tend to be long-lived in the aftermath of injury. While the injury heals, trigger point pain overstays its welcome.
My shoulder story illuminates the relationship between injury and the strange phenomenon of trigger points. Understanding it is of great potential value to anyone with an injury that doesn’t seem to be recovering. This article may convince the injured of exactly why they need to know how to self-treat trigger points … but this tutorial will teach you how to do that:
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
2019 — Thoroughly edited and modernized.
2016 — Revised the introduction.
2015 — Added the example of tension headaches in post-concussion syndrome, and some miscellaneous minor editing.
2008 — Publication.
Related Reading
- Basic Self-Massage Tips for Myofascial Trigger Points — Learn how to massage your own trigger points (muscle knots)
- Mobilize! — Dynamic joint mobility drills are an alternative to stretching, a way to “massage with movement”
- Heat for Pain and Rehab — A detailed guide to using heat as therapy for acute and chronic pain and recovery from injury
Notes
- I was a Registered Massage Therapist with a busy practice in Vancouver, Canada, from 2000–2010. I quit the profession in disgust before I could be “fired” for being critical of pseudoscience and alternative medicine. I changed my professional focus to science journalism and anti-quackery activism, writing mostly about massage-adjacent topics in the early years, but then spreading out into anything relevant to any kind of chronic pain or injury rehab — an effectively infinite list of topics. Even fifteen years after my last hands-on work, I still think of myself as a massage therapist. That said, I don’t exactly feel like an “insider” either, and I’ve branched out a lot in that time. See my bio.
- Ultimate is a Frisbee team sport, co-ed and self-refereed, with soccer-like intensity and usually the mood of a good party. Players tend to be jock-nerd hybrids: lots of engineers and scientists. Hippies invented the sport, but have mostly been displaced. I’ve been playing since 1997.
- This isn’t the first time I’ve had the opportunity to “study” my own injuries, either — not hardly. I’ve had several other sports injuries. This is partly how I earn my credibility as a publisher on this subject.
The “expanded integrated hypothesis” was presented by Dommerholt, Gerwin, and Shah in 2004. It’s detailed and technical! When abridged and oversimplified, it closely resembles the integrated hypothesis (“a possible explanation”) put forward by Travell and Simons in the first edition of their famous textbook in 1981. The expanded integrated hypothesis basically says this:
Under some circumstances, muscular stresses can cause patches of poor circulation, which results in the pooling of noxious metabolic wastes and high acidity in small areas of the muscle. This is both directly uncomfortable, but also causes a section of the muscle to tighten up — a micro cramp — and perpetuate a vicious cycle. This predicament is often called an “energy crisis.” It constitutes a subtle lesion. TrPs research has largely been concerned with looking for evidence of a lesion like this.
- Zhang H, Lü JJ, Huang QM, et al. Histopathological nature of myofascial trigger points at different stages of recovery from injury in a rat model. Acupunct Med. 2017 Dec;35(6):445–451. PubMed 29109129 ❐ PainSci Bibliography 52259 ❐ An animal study showing more trigger points around injuries in rats than in healthy rats.
- Ettlin and Fernández-Pérez are both small observational studies basically showing that people with whiplash have more trigger points. Not convincing to a skeptic, but better than nothing.
Muscle has a large behavioural repertoire, reacting in many ways to many different situations. There are undoubtedly competing and confused reflexes: situations where the body isn’t quite sure how to respond, and handles it differently over time and as conditions change. The classic idea of a “protective spasm,” for example, would obviously be disastrous around a fragile bone fracture. Protective paralysis is more likely with some injuries, and a neurological ban on movement can be quite potent. For a discussion of other possibilities, see Cramps, Spasms, Tremors & Twitches.
For our purposes here, it’s enough to emphasize that muscular reactions to injury are complex and not well-understood, probably often stressful, fatiguing. Another possibility is the irritation of stagnancy. Injuries often constrain joints to strictly limited ranges of motion — like being stuck in an uncomfortable position for too long. All of the contortions that we learn when we are injured, all the limping and squirming and fidgeting and careful avoidance of certain movements, requires unfamiliar and often intense and precise muscle activity.
This stressful challenge is the most likely explanation for why trigger points tend to form around injuries.
- Pain itself often modifies the way the central nervous system works, so that a patient actually becomes more sensitive and gets more pain with less provocation. This is called “central sensitization.” (And there’s peripheral sensitization too.) Sensitized patients are not only more sensitive to things that should hurt, but also to ordinary touch and pressure as well. Their pain also “echoes,” fading more slowly than in other people. See Sensitization in Chronic Pain: Pain itself can change how pain works, resulting in more pain with less provocation.
- Trigger point massage has never been subjected to even one sufficiently rigorous clinical trial. There are only about a dozen studies worth knowing about, and all have serious flaws and were conducted by researchers with a high risk of bias. Most report only minor benefits, and a couple are blatantly negative despite positive-sounding conclusions (if you look at the actual data). Only one (Aguilera 2009) reports a more robust effect. Three of the less-bad studies are Hodgson 2006, Gemmell 2008, and Morikawa 2017. I’ve reviewed all the evidence thoroughly in my main trigger points tutorial, but the bottom line is clear: the evidence is promising if you’re a trigger point therapist, but damningly faint praise if you’re a skeptic, and just inconclusive if you don’t have a dog in the fight.
- The brain is somewhat inept at precisely locating internal pain and so sometimes we experience pain in a broad area around or near the cause, or even further afield. This is the same phenomenon as heart attack pain felt mainly in the arm: the brain just can’t figure out where the pain is coming from, and the arm pain is a bad “guess.” Patterns of referral from the musculoskeletal system are somewhat predictable, and most referred pain spreads away from the centre and the head (laterally, distally). By contrast, visceral referral is much more erratic.