Hydrocephalus and craniosacral therapy
“Hydrocephalus” is a brain squeeze from excess fluid, a serious thing. 😬 Can craniosacral therapy treat it? A reader asked me about this on behalf of his wife, because her implanted cerebrospinal fluid shunt isn’t working quite well enough for her, and they have a friend strongly recommending CST.
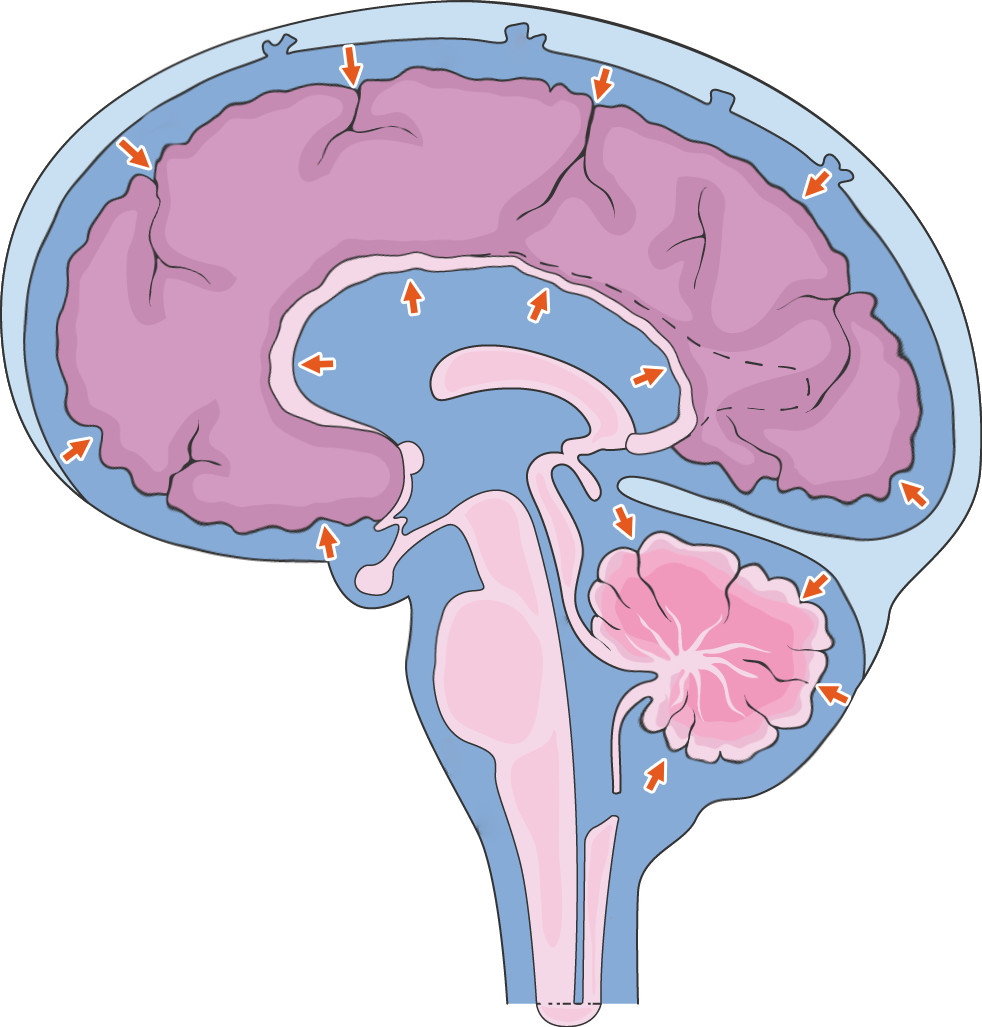
Hydrocephalus squeezes the brain. The skull cannot yield to a higher volume of increased cerebrospinal fluid, so the brain yields instead.
I answered in detail by email, and then in even more detail in a new section of my craniosacral therapy page, and here’s the much less detailed summary:
Craniosacral therapy is intended to tinker with cerebrospinal fluid circulation, so there is some reason to think it might be useful, if you give it the benefit of the doubt. But there’s not really much reason for us to give CST the benefit of the doubt — it really hasn't earned it over the decades — and whatever minor effects CST has on the brain’s watery cushion, if any, are probably just swamped by the forces involved in hydrocephalus.
Like trying to stop the tide with a bucket.
In short, CST has about as much chance of helping hydrocephalus as I have of getting into Hogwarts. The main harm would be the wasted money, and potentially the distraction from legitimate care.
Would you like some bad science with that?
While I was working on the hydrocephalus update, I also came across this delicious takedown of an impressively junky “review” of craniosacral therapy for pain by Jonathan Jarry of the McGill Office for Science and Society. The paper claims to have found “significant and robust effects of CST on pain and function,” based on the data from 10 studies. But the studies weren’t fit to line a birdcage. “If you don’t look up these individual trials,” Jonathan writes, “you won’t know just how bad they are.”
It’s easy to find fault in studies, maybe even a little too easy. It’s important to remember that even good studies have weaknesses, almost without exception, and that doesn’t make them worthless. I am painfully aware of the problem illustrated by this flowchart:
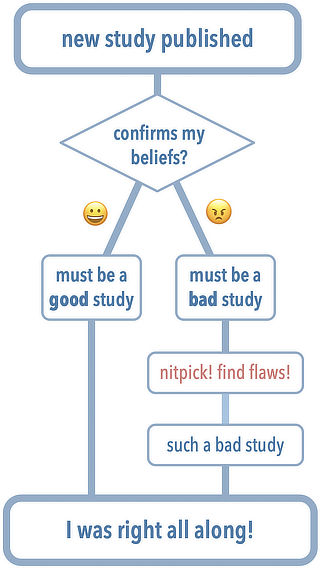
Excessively skeptical, knee-jerk dismissal of evidence does happen. But bad studies do exist! Lots of bad studies! It’s a far larger problem than overzealous skepticism, and they do need to be dismissed. We just have to do it well (like Jonathan did).
Bottom line: CST almost certainly does not do much to help people with pain, and scientific review papers are only as good as the studies they review.
Duty versus inspiration
It took me about four to six hours over three days to write and publish that update this week, and arguably it pulled me away from much more important updates. But the reader question was poignant, and I really wanted to answer it, and properly. So I decided to follow my inspiration rather than my overwhelming to-do lists — a choice I never seem to regret.