Thixotropy is Nifty, but It’s Not Therapy
A curious property of connective tissue is often claimed as a therapy
This article is about the idea that massage therapy works by softening connective tissues, specifically fascia, because of “thixotropic effect.” This claim is often made by massage therapists, and they are fond of calling it “melting” — which is misleading.
A quick look at the physiology of thixotropy shows that it’s extremely implausible that it would have anything important to do with massage therapy. The thixotropic effect is nifty physiology, but it’s not a therapeutic effect in itself, nor is it the mechanism for any benefit. It was never more than an idea that Ida Rolf had in the 1970s about how her therapy method (Rolfing) supposedly worked — and Ida’s idea was wrong.
This article is an abridged and simplified excerpt from a much longer article about fascia, with extensive footnotes and citations (dozens of them). If you want the more rigorous version, see: Does Fascia Matter? A detailed critical analysis of the clinical relevance of fascia science and fascia properties.
The basic biology of thixotropy
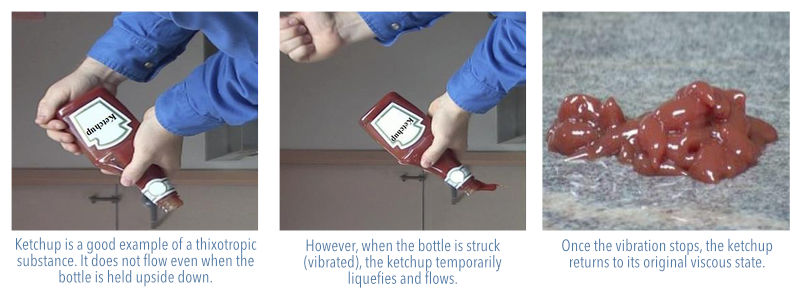
Thixotropic effect is an obscure physical property of certain slimy body fluids that get thinner when agitated or stressed. You can easily observe thixotropic effect in beach sand, near the water’s edge: stamp your feet in the sand, and it starts to liquify. Ta da, thixotropy!
Thixotropic fluids in the human body include synovial fluid in joints, mucus, semen, and the gelatinous and poorly-named goo called “ground substance” — the stuff that gristly connective tissue fibres are embedded in like bits of coconut in Jello. Ground substance is the most plentiful thixotropic substance in the body.
What makes these substances gooey and slimy? Why, a family of carbohydrate molecules, of course: the glycosaminoglycans. Also known as the snot molecule. Think of any movie monster with gobs of gross, ropey saliva — that’s glycosaminoglycans!
Thixotropy as therapy?
The therapy theory of thixotropy is that massage limbers you up by inducing thixotropic effect in your connective tissues. In particular, Ida Rolf used thixotropy to explain fascial “releases.” Robert Schleip is a researcher who is known for his focus on the properties of fascia:
Many of the current training schools which focus on myofascial treatment have been profoundly influenced by Rolf (1977). In her own work Rolf applied considerable manual or elbow pressure to fascial sheets in order to change their density and arrangement. Rolf’s own explanation was that connective tissue is a colloidal substance in which the ground substance can be influenced by the application of energy (heat or mechanical pressure) to change its aggregate form from a more dense ‘gel’ state to a more fluid ‘sol’ state.
Schleip, 2003, Journal of Bodywork & Movement Therapies
But thixotropy is minor and ephemeral … and fascia is too tough to change in general, probably just impossible in the context of manual therapy.
Fascial sheets are incredibly tough, and you can’t “change their density and arrangement” quickly or easily. And thixotropy just isn’t fast enough to explain the relatively speedy, dramatic effects on tissues that therapists claim to achieve. Dr. Schleip: “either much longer amounts of time or significantly more force are required for permanent deformation of dense connective tissues.” Thixotropy might make connective tissues more pliable, but not stretchier. The extensibility of tendons and ligaments is determined by the properties of the collagen fibres that give them their bulk and tensile strength, and they are (much) stronger than steel cable.
Even if it works in some small way, thixotropic effect is going to be temporary, fading within seconds or minutes after hands are removed. When the stimulation stops, so does the thixotropy — and a therapy is unlikely to be powered by such a transient effect, if tissue immediately reverts to its previous state. Dr. Schleip calls this the “reversibility problem” and “definitely not an attractive implication of this model for the practitioner.”
Last but not least, thixotropic effect is simply a minor effect. It’s occurring a little bit all the time, with or without massage. Massage surely does induce it a little, but just as surely much less than ordinary physical activity — like with circulation. Among many other things, massage therapists are also very fond of claiming that massage “increases circulation” … but the effect is much smaller than what exercise does! Perspective matters. For more information, see Does Massage Increase Circulation? Almost certainly not in a clinically important way, and definitely not as much as even a small amount of exercise
Another similar thought experiment: if sustained pressures or sheering could significantly change connective tissue, then working in a chair all day long — or any prolonged postural stress — would also deform your fascia.
But, most importantly, who cares? The whole idea that it’s therapeutic to have “looser” connective tissue is obviously simplistic nonsense, and always was. There are few therapeutic situations where you would actually want looser connective tissue, and even in those situations the problem could not be solved by thixotropy.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
Related Reading
Casual abuse of the concept of thixotropy is the tip of an iceberg of bad ideas about manual and massage therapy. There are many others, and more important ones.
The major myths about massage therapy are:
- Massage increases circulation. Probably not… and definitely not as much as a little exercise.
- “Tightness” matters. The three most common words in massage therapy — “you’re really tight” — are pointless.
- Massage detoxifies. It’s actually the opposite, if anything.
- Massage patients need to drink extra water to “flush” the toxins liberated by massage.
- Massage treats soreness after exercise. Studies have shown only slight effects.
- Massage reduces inflammation. An extremely popular belief based mainly on a single seriously flawed study.
- Fascia matters. The biggest fad in the history of the industry.
- Scars and adhesions can be scraped away. Often uncomfortable, sometimes dangerous, always expensive and ineffective.
- The psoas muscle is a big deal. The most overhyped single muscle.
- Massage stimulates endorphins (natural opioid) and reduces cortisol (stress hormone). They do not.
- “Trigger points” are evidence-based. Actually, the science is seriously half-baked.
- Massage therapists have spooky palpation skills. No, it’s just ordinary expertise… and misleading.
The complete list of dubious ideas in massage therapy is much larger. See my general massage science article. Or you can listen to me talk about it for an hour (interview).
And massage is still awesome! It’s important to understand the myths, but there’s more to massage. Are you an ethical, progressive, science-loving massage therapist? Is all this debunking causing a crisis of faith in your profession? This one’s for you: Reassurance for Massage Therapists: How ethical, progressive, science-respecting massage therapists can thrive in a profession badly polluted with nonsense.