Spinal Fracture Bracing and Fixation
My wife’s terrible accident, and a whirlwind tour of the science and biomechanics of her spine brace
In early 2010, my wife’s back was temporarily held together with titanium, aluminum, and nylon straps. She’d suffered a major T12 burst fracture, along with a few other fractures in a car accident in Laos. This article focusses on treatment for her spinal injuries. For the full story, see “Injured Abroad: My wife’s nasty accident while travelling alone in Asia.”
This very serious injury was braced (“fixated”) by surgically implanted titanium — bracing on the inside. After we’d spent a few weeks in hospital in Laos, we flew her home encased in a wearable spine brace as well: an elaborate contraption of bars and straps and covered in an almost fashionable taupe leather. It consisted mostly of metal in the back, which was tied to her as tightly as she could stand around the shoulders and belly. For weeks, every time she got out of bed, we had to strap her into that thing to protect her spine — allegedly.
I wondered all along if it was really doing anything. Her experience was inherently interesting, and full of lessons relevant to low back pain. And I was already aware that bracing is of surprisingly limited value for other kinds of rehab, like after surgical repair of a ripped up shoulder.1 There are many signs that the very medical impulse to stop or limit movement may be misguided, clues that how we heal and why we hurt has more to do with biochemistry and use-it-or-lose-it than structural integrity and alignment. There are many lower-stakes examples, like orthotics, therapy taping, and soft-bracing.
Getting a little closer to home, lumbar fusion is a notoriously lousy treatment for chronic back pain — there is now very strong evidence against it.2
But with major fractures, especially spinal fractures? All those pesky doubts about the conventional wisdom scatter like cockroaches in the light. Iit seems necessary to immobilize such injuries — dangerous not to! But, as I learned, it really isn’t that straightforward. Nothing in the business of pain and rehab ever is.
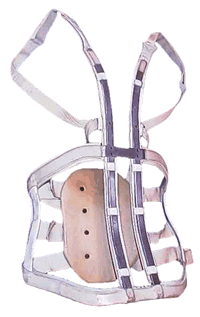
This is the kind of brace Kim wore: aluminum bars and straps, leather and canvas. A bit antiquated, this is what we were given in Thailand.
Breaking titanium!
One of the most interesting clues that my wife did not need spinal "scaffolding" installed was that hers broke. So they weren't doing much.
Ironically, her titanium fixations — we always just called them the bars, as in “How are the bars feeling today?” — actually fell apart during this period. I had been suspicious of this for some time. In certain positions, she even squeaked like a dry hinge — an unmistakable metal-on-metal sound! Muted by a little flesh.
This might have remained a permanent puzzle, until I personally confirmed the breakage studying MRI images. The radiologist had missed it!3 I am proud of making that discovery, even though it is not really as amazing as it sounds. Certainly it’s a minor embarrassment for the radiologist, but mostly his attention was properly on my wife’s bones and spinal canal, not so much her bars. The find was quickly confirmed by a surgeon, who was more amused than shocked (amused in a good, friendly way). “It’s rare. Less than 5% probably,” he explained. “But it does happen, and it’s really not that big a deal.” The bars are simply an internal brace, and are more or less useless dead weight once the bone has healed.
And maybe even long before.
My wife had the bars removed in early 2012. They had become bothersome — a constant, nagging, uncomfortable presence. The procedure and recovery went well. With the ordeal fully behind us, I decided it was time to write about the bracing question. It is not terribly relevant to most of my usual readers, who come here for good information about back pain, not back fractures.
But it is just interesting, and instructive about the nature of backs.
Spine bracing basics
Back braces are routinely recommended to patients during rehabilitation from back injuries and surgeries. In particular, braces are usually assumed to be necessary either as the primary treatment method for a minor spinal fracture, or as a key factor in rehabilitation after surgical repair of a more serious fracture. Aggressive immobilization with a brace probably is necessary to treat a serious fracture without surgery — however, even that is not completely clear cut. It’s not clear that any back brace is actually working as advertised. There is a lot of debate and controversy. There are “better safe than sorry” surgeons and physiatrists who insist on them, and others who think it’s useless.4
It’s not necessarily a bad idea to stabilize an injured spine. The trouble is that it may just not be possible. It has always been a bit unlikely that a back brace is really capable of stabilizing the spine significantly — the spine is powerful and squirmy, back braces are awkward and external — and there is plenty of evidence that clearly suggests that it cannot.
There is a near total lack of good evidence directly comparing bracing and not bracing (in any kind of spinal patient).5 All the scientific literature has really shown so far is that no one really knows whether bracing actually works or not. Not even the most expert of experts can provide an opinion any better than an educated guess. This is surprisingly typical of surgery, which is less science-based than most people assume. When surgeries are properly tested — compared to a placebo, or no treatment — the results are often disappointing, and this is especially true about orthopedic surgeries,6 including ones that seem more necessary, like stabilizing a burst fracture.7
But it doesn’t take a genius to see this: if a back brace is physically incapable of significantly limiting spinal movement or reducing the forces on vertebrae and metal implants, then logically it cannot possibly be very stabilizing or important.
The mechanics of spinal bracing and spinal stability
There are braces and there are braces!
Some braces are obviously better at immobilizing spines than others: custom-fitted “clamshell” braces that cinch your entire trunk into rigid plastic are certainly more likely to reduce spinal movement, especially bending and twisting. However, even the most aggressive braces can probably only do so much to resist the force of gravity. Why?
The ribs are quite flexible and mobile, and simply cannot provide firm enough resistance to prevent the weight of the upper torso settling onto the lower vertebrae. And any lesser brace simply stands no chance at all!
I suspect that even a remarkable amount of bending and twisting is still possible within any brace. It certainly seemed that way with Kim’s brace. Despite all the tight straps and clever bars, she could definitely still squirm around inside that thing.
All of this was shown quite clearly by German researchers in 1999.8 They used “telemeterized” implants — steel fixation rods with meters on them! so cyborgy! — to measure the effect of common external braces on spinal forces. This is a clever science experiment. If you have implants stabilizing your spine internally, measuring the stresses on them directly is a good way of checking to see if an external brace is doing anything.
They found that “none of the braces studied were able to markedly reduce the loads” on the implants. There was some reduction — just not “marked,” nothing to write home about.
More surprisingly, some of their measurements showed that bracing actually increased forces on the implants! That’s extremely interesting. I couldn’t have predicted it, but it does seem possible.
Another perspective: in a 2019 experiment, sacroiliac joint ligaments in cadavers were severed, roughly doubling the range of motion of the joint. Screwing it back together decreased the instability but did not eliminate it. Even after installing a more elaborate rig of screws and fixation rods, the stability of the intact joint was not fully restored.9
The spine is an extraordinarily dynamic structure. Somewhat like slouching into a comfortable chair, a brace may actually cause some sloppiness of spinal function, resulting in “resting” on the fixations, rather than using muscle to support and control the spine.
One of the most recent bracing trials compared bracing to no bracing in a fair number of patients with minor (stable) burst fractures, and simply found no difference at all, suggesting that such fractures are “inherently a very stable injury and may not require a brace.”10
Some bracing conclusions
Considering all factors, I think it’s a bit of a no-brainer that back bracing is probably pretty unimportant for the minor spinal fracture or surgery patient. As some doctors believe, it may simply do nothing at all except inconvenience the patient.
The more interesting question is whether or not it matters to more seriously injured patients. Should someone with a scarier low back fracture wear a brace, just in case? Kim was certainly such a patient — right on the brink of paralysis. It was a very close call.
But such a patient will almost always be fused surgically, as the evidence about that is quite clear: it works. And once an unstable fracture has been fixated it quickly becomes quite similar to a stable fracture as well. And if a brace made no difference at all to recovery from minor burst fractures, it’s doubtful that it would make any significant difference in more serious ones that have been repaired with steel implants. Especially since we already know that a typical brace can’t actually take the pressure off of the steel implants at all!
Back braces are notoriously frustrating for patients, and all the more so in cases where they are supposedly more necessary. Patient compliance is definitely a problem (I certainly saw that with my own eyes). Patients flat out ignore physician recommendations, and cheerfully push the limits.
And yet there’s clearly no epidemic of patients who have suffered serious complications from failing to use their brace properly.
Even though Kim’s fixations broke, there’s a good chance that they were sound enough for long enough that, by the time she was starting to get up and around, her vertebra had already healed enough that she needed neither the metal inside or the metal and straps outside. We’ll never know.
Did you find this article useful? Interesting? Maybe notice how there’s not much content like this on the Internet? That’s because it’s crazy hard to make it pay. Please support (very) independent science journalism with a donation. See the donation page for more information & options.
About Paul Ingraham

I am a science writer in Vancouver, Canada. I was a Registered Massage Therapist for a decade and the assistant editor of ScienceBasedMedicine.org for several years. I’ve had many injuries as a runner and ultimate player, and I’ve been a chronic pain patient myself since 2015. Full bio. See you on Facebook or Twitter., or subscribe:
What’s new in this article?
2023 — Revised the introduction and put the topic more in context, relating to it to other topics on the site. Eventually this is going to become part of a larger article about the “medical impulse to stop or limit movement”: bracing in general.
2017 — Added citation to Avilés about the similarity of outcomes from surgery versus conservative therapy for burst fractures.
2016 — Added citations to Louw and Harris about ineffective surgeries in general.
2012 — Publication.
Notes
- Kim YS, Chung SW, Kim JY, et al. Is early passive motion exercise necessary after arthroscopic rotator cuff repair? Am J Sports Med. 2012 Apr;40(4):815–21. PubMed 22287641 ❐
This was a test of two rehab strategies in 105 patients with surgically repaired rotator cuff tears (small to medium-sized tears of the shoulder muscles). Half were fully braced after surgery, while others performed mobilization exercises. Range of motion, pain, and function were the same across the board for both groups. “Early passive motion exercise after arthroscopic cuff repair did not guarantee early gain of ROM or pain relief but also did not negatively affect cuff healing.” So a bit fat nothing burger, but interesting that early movement was fine.
- Mannion AF, Brox JI, Fairbank JC. Consensus at last! Long-term results of all randomized controlled trials show that fusion is no better than non-operative care in improving pain and disability in chronic low back pain. Spine J. 2016 May;16(5):588–90. PubMed 27261844 ❐
Excellent and important commentary on Hedlund et al., which was an important long-term experiment comparing spinal fusion to physiotherapy over more than a decade. It seemed to produce a contradictory result that “prevents a strong conclusion.” But the waffling wasn’t necessary. That good-news-bad-news conclusion was a bit of an illusion. The authors cherry-picked the best possible sounding news from their own data, creating the appearance of uncertainty about spinal fusion where in fact there was none. Mannion, Brox, and Fairbank explain exactly why.
For full details, see Long term results of spinal fusion: good news and bad?
- I found it myself, staring at those magical black and white transverse slices of my wife’s back, which clearly revealed cross-sections of a screw (so unlike any anatomy!) floating in the wrong place, the end of one bar well out of its home bracket, and the other on the verge of coming loose as well.
- Connolly PJ, Grob D. Bracing of patients after fusion for degenerative problems of the lumbar spine—yes or no? Spine (Phila Pa 1976). 1998 Jun;23(12):1426–8. PubMed 9654635 ❐
This research is really just asking two experienced surgeons their opinion on the value of bracing after back surgery (for non-traumatic back problems). They disagree. “Dr. Connolly argues that an external orthosis is advisable in many cases; Dr. Grob feels that the rigidity of internal fixation should be adequate to obviate the need for external bracing.”
- Giele BM, Wiertsema SH, Beelen A, et al. No evidence for the effectiveness of bracing in patients with thoracolumbar fractures. Acta Orthop. 2009 Apr;80(2):226–32. PubMed 19404808 ❐
Researchers reviewed several studies that have attempted to determine if bracing works in patients with traumatic thoracolumbar fractures. The results? Inconclusive.
- Louw A, Diener I, Fernández-de-Las-Peñas C, Puentedura EJ. Sham Surgery in Orthopedics: A Systematic Review of the Literature. Pain Med. 2016 Jul. PubMed 27402957 ❐ PainSci Bibliography 53458 ❐
A review of a half dozen high quality tests of four popular orthopedic (“carpentry”) surgeries, all showing a lack of efficacy compared to placebos. This review is an excellent academic citation to support the claim that sham surgery has shown to be just as effective as actual surgery in reducing pain and disability. It’s also an eyebrow-raiser that Louw et al. could find only six good (controlled) trials of orthopedic surgeries, and all of them were bad news.
- Avilés C, Flores S, Molina M. Conservative versus operative treatment for thoracolumbar burst fractures without neurologic deficit. Medwave. 2016 Mar;16 Suppl 1:e6383. PubMed 27028069 ❐ We don’t actually even know if surgery for a burst fracture is better than conservative therapy — surgery might reduce the risk of developing neurological problems, but increase the risk of complications. Those pros and cons roughly cancel each other out, and surgery has no clear benefit over conservative rehab otherwise.
- Rohlmann A, Bergmann G, Graichen F, Neff G. Braces do not reduce loads on internal spinal fixation devices. Clin Biomech (Bristol, Avon). 1999 Feb;14(2):97–102. PubMed 10619096 ❐
- Dall BE, Eden SV, Cho W, et al. Biomechanical analysis of motion following sacroiliac joint fusion using lateral sacroiliac screws with or without lumbosacral instrumented fusion. Clin Biomech (Bristol, Avon). 2019 May;68:182–189. PubMed 31234032 ❐
- Bailey CS, Dvorak MF, Thomas KC, et al. Comparison of thoracolumbosacral orthosis and no orthosis for the treatment of thoracolumbar burst fractures: interim analysis of a multicenter randomized clinical equivalence trial. J Neurosurg Spine. 2009 Sep;11(3):295–303. PubMed 19769510 ❐ For a thorough and readable summary of this research, see Is a Back Brace Really Needed for a Burst Fracture of the Spine?