An evidence-based guide to ME/CFS
Introduction: when is fatigue a syndrome?
There are many fatiguing illnesses. Fatigue can be caused by almost any health issue, from common and familiar problems like iron-deficiency, to depression, to pathology like long COVID. “Chronic fatigue syndrome” (CFS) is an informal term that describes any long-term struggle with unexplained fatigue, some of which are caused by surprisingly ordinary problems like anemia that simply haven’t been diagnosed yet; more severe cases with no other explanation are often called myalgic encephalomyelitis (ME), largely to distinguish it from a mere "fatigue" problem — and that word is often absurdly inadequate — but the labelling is controversial while the underlying pathology is a mess of overlapping possibilities that continues to defy diagnosis. Regardless, many cases of ME/CFS are clearly caused by some kind of unknown disease process that can ruin lives.
This is a thorough, readable exploration of the topic — small for a book, big for an article. I am a science journalist who has suffered from ME/CFS myself since 2015. I am particularly interested in the overlap between ME/CFS and pain (fibromyalgia).
Why is it always ME-slash-CFS? And where’s FM?! Myalgic encephalomyelitis vs chronic fatigue syndrome (vs fibromyalgia)
What is this two-for-one acronym with the slash: “ME/CFS”? Many people know that the CFS is for “chronic fatigue syndrome.” But only a few know that ME is for “myalgic encephalomyelitis,” fewer still can pronounce it, and hardly anyone can explain why their acronyms are always smushed together. Or why FM for fibromyalgia doesn’t get included.
In theory (and officially), ME and CFS are literally the same thing. In practice, not so much, because — right or wrong — the CFS label is used much more loosely, and applied to many people who would not meet the diagnostic criteria for ME/CFS, but are definitely sick in a CFS-y way.
And so, in practice…1
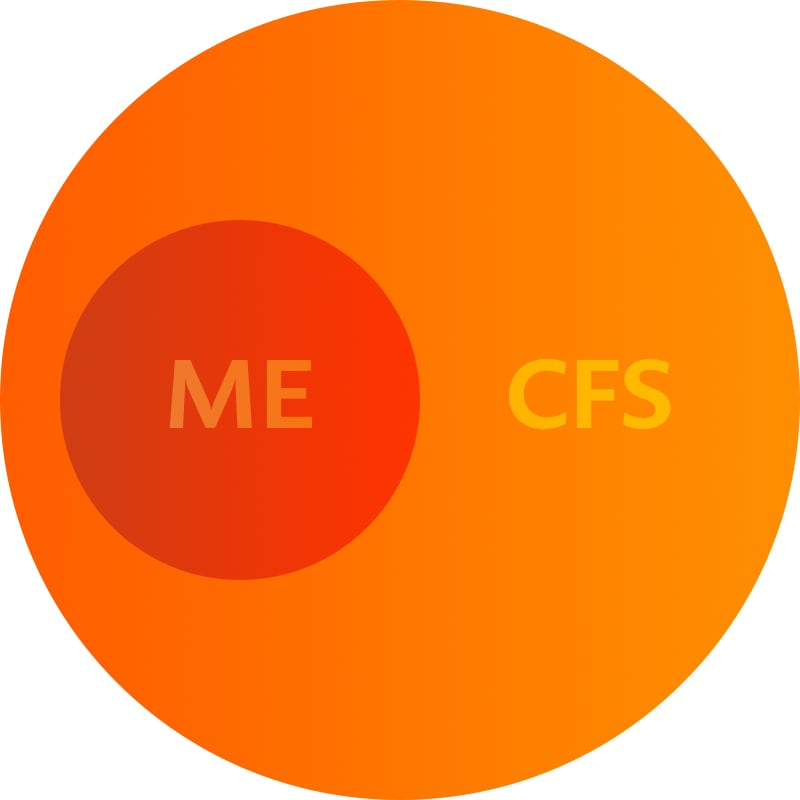
ME is the nastiest and most pathologically distinct member of the sprawling and dysfunctional CFS family, which includes all the things that ever get called CFS, rightly or wrongly (which is very controversial). ME and CFS always get mentioned in the same breath because they are too different to completely combine into one condition, and too similar to simply separate!
“Chronic fatigue syndrome” is not a diagnosis per se: it’s just a descriptive label for a pattern of symptoms dominated by fatigue, and with no obvious explanation but an incredible range of possibilities, including well understood fatiguing illnesses, as well as puzzling fatiguing illnesses that may never get a diagnosis more specific than CFS.
If CFS was a country — a crappy country you do not want to visit — then ME would be its capital city. It is much closer to being an actual diagnosis, with more severe and predictable symptoms and signs.
Importantly, ME patients can actually be identified by someone other than themselves: that is, they have objective signs of disease, and not just subjective symptoms. Unfortunately, those signs are exotic biomarkers that can only be detected in a research context; there are still no clinical tests, nothing patients can ask their doctor for.
Meanwhile, ME patients have notoriously “normal” looking results for all widely available medical tests — and anything that does crop up is probably coincidental and a red herring. Pure ME simply doesn’t show up on standard medical tests. The only abnormalities that can be readily confirmed are the signs of several common health problems that are common in these patients — “comorbidities” like postural orthostatic tachycardia syndrome and irritable bowel syndrome — but their involvement is erratic and not specific to ME. They are signs of a severely distressed system.
So if ME is so different from CFS, why constantly pair it with CFS?
Not everyone with chronically fatigue illness has the hallmarks (or biomarkers) of ME, not even close. All ME is CFS, but not all CFS is ME. CFS is a category, ME is the biggest and baddest thing in that category, the most extreme and well-defined member of that club — which includes lots of members whose membership status is uncertain. Patients with undiagnosed fatiguing illnesses who eventually get a diagnosis (like cancer) get kicked out of the CFS club.
But ME patients will always belong in the CFS club. Indeed, most will be lifetime members.
And so the routine labelling of ME and CFS as a pair persists because it’s really hard to break them up. Referring only to ME would rudely leave out far too many people who have quite similar problems. But referring only to CFS would ignore the most important kind of CFS! It’s actually “politically” vital to use ME, to help emphasize the fact that a lot of CFS is definitely a distinct pathology — that’s part of how it gets taken seriously by doctors and researchers.
And so… ME/CFS.
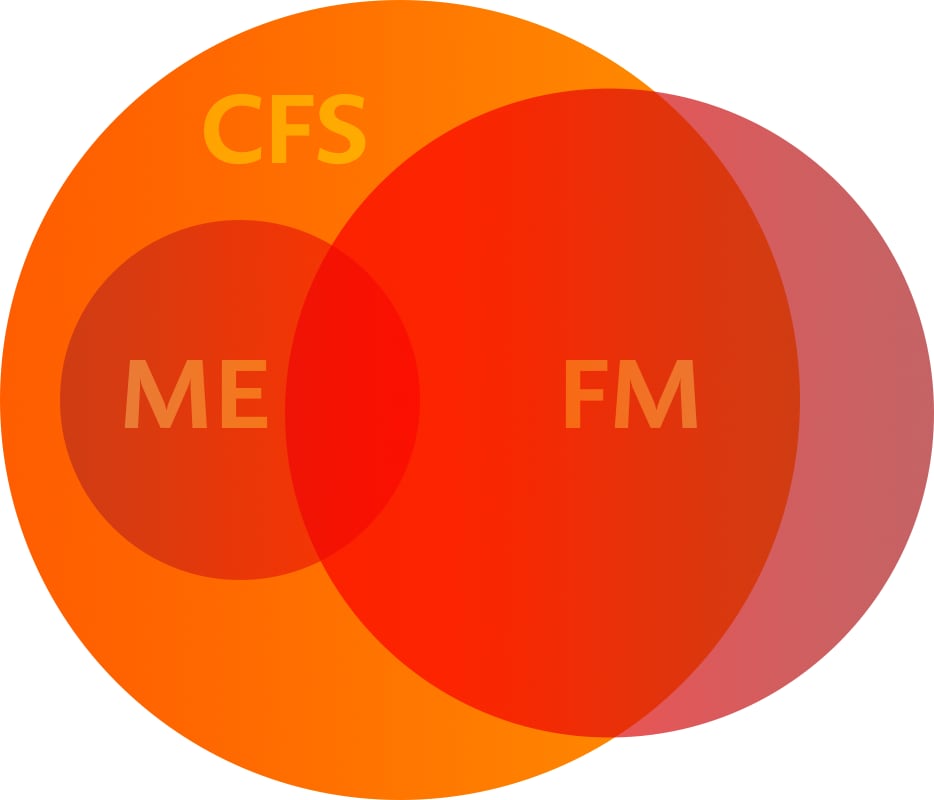
The ME/CFS “Death Star” Venn.
And why not ME/CFS/FM, hmmm? WHY?!
Fibromyalgia is no more of a “diagnosis” than CFS is. It’s a label for a similar pattern of symptoms … but one that’s dominated by pain rather than fatigue. So it’s really just “chronic pain syndrome,” but it got it’s own weird name for historical reasons, and that makes it sound more different than it is. Many cases are not very different.
Formal diagnostic criteria also seem to separate all of these conditions, but the messy clinical reality is that fibromyalgia is often extremely similar to ME/CFS with extra pain. And ME, CFS, and FM also clearly share many symptoms and common comorbidities. For instance, fibromyalgia can include mental fog and exercise intolerance … just like ME/CFS.
And vice versa: many patients with ME/CFS also have quite a lot of pain, and would probably be considered fibromyalgia patients if the pain wasn’t so overshadowed by even worse fatigue/malaise.
Although they can be quite different, they can also be very similar. And so fibromyalgia seems an awful lot like a sibling to ME/CFS — but you never see “ME/CFS/FM.” Whyever not? Because they do have distinct diagnostic criteria, officially. But the overlap is so substantial that I do always group them together in my head. I won’t catch on, but it’s always going to be “ME/CFS/FM” to me.
And then there's long COVID! Which is clearly relevant to ME, CFS, and FM. It’s not a twin, but the resemblance is striking. However, “ME/CFS/FM/LC” would be a bit ridiculous.
Mystery fatigue vs. merely “undiagnosed so far”: primary and secondary CFS
Some CFS is actually an exotic mystery, but most of it is probably just undiagnosed pathology — and it’s very important to eliminate that possibility. It occurs as a result of some other conditions that is knowable and diagnosable in principle, albeit not always in pratice (see next section). Such CFS is formally known as secondary CFS.
“Mystery CFS” has poorly understood or entirely mysterious causes, and/or just rather rare and exotic diseases. In these cases, the ME/CFS is primary: that is, it’s the main problem as far as we know. Obviously there is a cause, but it is either entirely unknown or very poorly understood. Post-viral syndrome is a great example: we know it exists, and that’s about it. Like cancer, it is probably not one thing.
Even secondary CFS often defies diagnosis
Celiac disease is a good example of a disease that causes fatigue and malaise, but often goes undiagnosed even though it never “should.” Many celiac patients feel gross and tired for many years before finally being diagnosed (if they ever are). They may believe that they have “CFS.” And they do… until they are finally diagnosed with celiac disease!
Sadly, secondary CFS is often much harder to diagnose — even when it wouldn’t be in a better world. Some of the pathologies that mainly cause fatigue as a symptom are easily detected by any reasonably thorough medical investigation. But, tragically, even these diagnoses can get missed for due to poor accessibibility of care and physician incompetence and knee-jerk prejudice against “difficult” patients with vague symptoms (which is in turn greatly exacerbated by other prejudices, especially sexism and racism). Some diseases are medically underestimated.
Other cases of secondary CFS are genuinely difficult to diagnose in practice, even with very competent care. One big category of candidates of this type are the diseases that can make people feel awful for months or even years (“prodromal” symptoms) without ever becoming clear or severe enough for diagnosis.
This was written by Lynn (@brickandbutton) on Apr 9, 2019 [original gone]. She added in a comment: “I’ve come to a point after 7 years where I’m still fighting (and waiting) but I expect to be this severely sick forever. Anything else will be a fun surprise.”
Nature of the beast: causes of primary ME/CFS
ME/CFS can be a disease in its own right, and not just the consequence of some known diagnosable condition. Long COVID has made this much clearer than it used to be (even though post-infection syndrome has always been a known phenomenon). Conveniently, Nature just published a long article about Long COVID,2 which is an excellent place to review the most prominent theories, which extensively overlap with ideas about ME/CFS. As of late 2023, we also now have two large long-term studies (in Nature and JAMA) giving us lots of insights we've been waiting for.
According to Davis, McCorkell, Moore, and Topol: “around half of individuals with long COVID are estimated to meet the criteria for ME/CFS.” And I strongly suspect that number would be much higher if you looked only at more severe cases of long COVID. (It’s likely that some Long Covid is essentially just a case of taking months to fully recover from a severe infection, and not actually an ongoing pathological process.) It’s very clear that long COVID and ME/CFS are similar, albeit not quite identical. Here are some highlights from the Nature paper:
- Much like CFS, long COVID is probably not one thing: “There are likely multiple, potentially overlapping, causes of long COVID.” In fact, this beast-with-many-heads problem may be the main reason it’s been such a difficult medical problem to solve.
- Several viral and bacterial infections were already known to cause postinfectious illnesses characterized by ME/CFS and/or dysautonomia and a list of other typical comorbidities, and COVID appears to be similar.
- The main explanatory theories:
- Blood clotting — This is might be unique to COVID, but not necessarily. “Microclots and hyperactivated platelets are found not only in individuals with long COVID but also in individuals with ME/CFS.”
- Viral persistence — The most obvious possible explanation for long COVID is simply that people continue to feel sick because they are still sick, simple as that: a chronic infection, subtle only relative to the acute phase. SARS-CoV-2 was found in long COVID patients long after there was none left in fully recovered patients.
- Immune dysregulation — There are many complicated disturbances to normal immune function in long COVID patients.
- Excessive cytokines — One major sign of dysregulation is excessive cytokines, a ubiquitous immune system signalling molecule. That is also a classic sign of ME/CFS, which slowly fades over 2-3 years, even as symptoms persist — but it hasn’t been long enough to know if Long COVID works the same way.
- Reactivated viruses — Both long COVID and ME/CFS could be explained by other common persistent viral infections, usually well controlled but surging back to activity when the immune system is weakened or “distracted” by other issues. It’s broadly plausible that human health involves a lot more long-term erratic wars with pathogens than we appreciate. We are still very actively learning major new things about the role of viruses in human health.
- Autoimmunity and immune priming — “Autoantibodies” are a class of molecule associated with autoimmune disease, and there’s ongoing controversy about whether they are linked to long COVID or ME/CFS (some studies say yes, others say no).
- Comorbidities — Several conditions are “comorbid” (occur at the same time) with both ME/CFS and long COVID. These can and do exist independently of ME/CFS, and yet they occur so commonly together that they can also be thought of as “symptoms” of both ME/CFS and long COVID. Each of these things has been independently blamed for ME/CFS in the past. But the fact that all of them often occur together strongly suggests that they are probably mostly the result of a common cause.
- Dysautonomia, especially POTS (postural orthostatic tachycardia syndrome).
- Mast cell activation syndrome (MCAS).
- Connective tissue disorders.
- Craniocervical junction disorders — Several conditions with the potential to irritate upper cervical spinal cord, brain stem, or cranial nerves.
- Endometriosis.
- Microbiota dysbiosis — This is common and substantial in long COVID, and has also long been linked to ME/CFS. The dysbiosis state may be either cause and/or consequence. Dysbiosis may occur for other pathological reasons, and the go on to become a mechanism that drives symptoms.
- Most long COVID does not resolve on its own, or only very slowly, which is consistent with what we've seen with much smaller populations of ME/CFS patients over much longer periods. The severity of complications following covid strongly correlates with infection severity (e.g. much worse in hospitalized), but it cannot be emphasized enough that even milder cases have an extraordinary list of complications. While the second year of long COVID is less harsh, it is still substantially disabling, with dozens of elevated risks.
Diagnosis is mostly about eliminating secondary CFS
Primary ME/CFS can only be diagnosed with high confidence by eliminating secondary CFS, which is quite difficult. The list of things that can cause prolonged or episodic fatigue/malaise is quite substantial. Here's a high-level overview:
- infections
- anemia
- various organ failures and dysfunctions
- some cancers
- nutrient deficiencies
- autoimmune diseases
There's plenty of low-hanging fruit on that list, stuff that's relatively easy to check, and obviously every patient with CFS should do try to do this. It is a very high priority in the early stages.
But then there's also a long tail of conditions that are much harder to decisively rule in or out — and it’s not so obvious that every CFS patient should go to those lengths, especially if there's good reason to suspect primary ME/CFS.
Eliminating causes of secondary CFS is a higher priority in the early stages … and a lower priority later on for people with a lot more experience. It is possible for secondary CFS to elude detection for many years, but it does get less likely as the years tick by, especially for any well-educated patient who has been paying attention to their signs and symptoms for a long time. It just get a lot less likely that there’s a sneaky explanation for those symptoms that hasn’t revealed itself in all these years. But for the newer patient, or the less well-informed, most of the list of possibilities is still fair game for quite a while.
The ME-CFS Clinician Coalition has a good quality guide to diagnosis — probably a bit overwhelming for patients, but a very useful tool to take to a trusted doctor.
Warning: it’s very difficult to prioritize a search for cause of chronic fatigue!
Wouldn’t it be great if I could provide a nice prioritized list of conditions to check? This is what every thoughtful patient realizes they want at some point.
Unfortunately, I think it’s nearly impossible to prioritize diagnostic investigations for the generic CFS patient. A single sign or symptom can completely re-sort the list! For instance, an absence of any obvious issues with digestion doesn’t eliminate GI tract disorders, but it does dramatically reduce the probability that such a diagnosis will eventually be found (and therefore the priority that should be placed on investigating those conditions). But for the CFS patient who is painfully aware that they are always feeling bloated or have clear symptom exacerbations after eating... that patient should definitely pull on that thread.
Judging the priority of any given diagnostic investigation is going to have huge “it depends” caveats. Properly prioritizing diagnosis actually requires detailed clinical consultation with a patient.
The problem of “lots of weird symptoms”
“Lots of weird symptoms” is a symptom in itself. That is, in addition to the typical symptoms of ME/CFS, there is a nearly universal meta-symptom: a collection of symptoms that are not just atypical, but downright unique. These highly idiosyncratic symptoms are a big part of what makes ME/CFS patients seem “difficult” to healthcare professionals, and I think are probably a combination of (at least) three things:
- Complex, unpredictable physiological consequences. Whatever’s wrong, it can clearly be quite serious and physiological fundamental, and it may have a lot of potential to wreak havoc in unpredictable ways. The most likely explanation for “lots of weird symptoms” is that there are “lots of things wrong.”
- Interoception is hard. “Interoception” is sensing things inside the body, and interpreting a lot of unusual sensations it’s like trying to do a jigsaw puzzle in the dark. To a significant degree, we just can’t. And so the stories people tell about strange internal sensations can go in wildly different directions …
- Now add fear and misery! Emotional distress likely amplifies and distorts perception that was already chaotic to begin with.
Combine all of these factors and it’s hardly surprising that most ME/CFS patients report some very weird symptoms indeed. And yet the result is often so “colourful” that I think this is the main reason that so many ME/CFS patients are dismissed as melodramatic hypochondriacs. It’s very hard for a healthy person to relate to an interoceptive catastrophe like this.
An example: Whitney Dafoe described his extreme case of ME/CFS for Healthcare (Basel), and it is dramatic in two distinct ways: his typical ME/CFS symptoms are severe, but then he also has particularly weird symptoms that I’ve never even heard of before.3 Much of what Mr. Dafoe reports is so bizarre that I’m not sure how useful it is to report it.4 But a kaleidoscopic array of symptoms seem to be prevalent in ME/CFS patients, and this is a good example of it. I suspect this is explained by an unholy blend of (a) complex pathology affecting many systems, and (b) the emotional chaos and hardship of serious unexplained illness.
Another example, from someone more articulate and perhaps level-headed: novelist Madeline Miller was struck with Covid and then long Covid early in the pandemic, still in the winter of 2020, a “first waver.”5 Her symptoms were “classic” and yet diverse:
“Looking at old photos, I was overwhelmed with grief and bitterness. I didn’t recognize myself. On my best days, I was 30 percent of that person. … everyone [with long Covid] had stories like mine: life-altering symptoms, demoralizing doctor visits, loss of jobs, loss of identity. The virus can produce a bewildering buffet of long-term conditions, including cognitive impairment and cardiac failure, tinnitus, loss of taste, immune dysfunction, migraines and stroke, any one of which could tank quality of life.”
Both patients and professionals should understand that it seems “normal” for ME/CFS patients to have a lot of strange symptoms. It’s normal for all of us to think “WTAF?” But let’s not then go on to think, “Must be crazy.” Instead, let’s embrace the likely reality that this disease is profoundly disorienting and disruptive, and it would be weird if it didn’t get weird.
Consider celiac disease [STUB]
As mentioned above, celiac disease is a classic example of a condition that can fly under the diagnostic radar for years, causing all kinds of chronic malaise. Many a celiac patient has a story about the revelatory experience of discovering WTAF is wrong with them.
It’s easy to informally test for celiac disease with a couple provocation and elimination tests: just avoid gluten for two weeks, and then have a day of quite starchy eating. Pasta party! Only a fun idea for non-celiacs! Anyone with celiac disease is going to feel better, and then a bunch worse. Repeat to be “sure.” If there’s an obvious fluctuation in symptoms, you immediately seek out a specialist to confirm. “Easy.”
But the priority of going through this process is much lower if there’s not already a known pattern of eating-associated symptoms!
Clinically diagnosing primary ME/CFS
Some patients are just very ME/CFS-y. Primary ME/CFS is easy enough to recognize clinically with moderate confidence, but it is very difficult to achieve high confidence. Primary ME/CFS is quite likely if you have …
- typical symptoms over a long period with no other obvious explanation
- one or two classic comorbidities
- a story that began after an infection (or other major physiological event)
Unfortunately, all none of those factors are exclusive to ME/CFS. Secondary CFS can do a fine job of mimicking primary CFS.
And there are no specific clinical tests for primary ME/CFS. A few tests can detect some signs that are common in these patients, and can help to substantiate the diagnosis, but no sign is unique to ME/CFS.
So moderate diagnostic confidence is in reach for many cases, but high confidence is very elusive.
Diagnosing ME/CFS at the lab
Unfortunately, this just isn't possible. There are well-established biomarkers for ME/CFS, but they are only useful in a research context. There are no widely available clinical tests for any of those biomarkers.
In other words, researchers have the ability to identify these signs in their experimental subjects in their labs lab, but physicians do not have any way to do the same thing with their patients. The lab in your community that processes tests ordered by doctors is a well-oiled machine that deals only with well-established standardized tests. They don’t do "weird" tests, period. At best, some hospitals or private clinics might have set up labs that can do almost any kind of test, with smart doctors using all kinds of tools, like on an episode of House MD — but that will be very rare and fabulously expensive (especially in America).
The comorbidities of ME/CFS: complications? causes? both? neither?
Many a CFS sufferer has at some point decided that their problem must be one of the following:
- dysautonomia & postural orthostatic tachycardia syndrome (POTS)
- mast cell activation syndrome
- connective tissue disorders causing hypermobility, including Ehlers–Danlos syndrome
- craniocervical junction (CCJ)-related conditions
- endometriosis
The problem with these “diagnoses” is that they are probably rarely the heart of the matter. Indeed, they may be more like symptoms than causes.
These conditions are all found more commonly in people ME/CFS — known as comorbidities, morbidities than tend to co-exist. But many have different ones, or none at all. It is clearly possible to have ME/CFS without any of these conditions. And it is also possible to have any of these conditions without ME/CFS! So while it is possible for some of them to be the root problem, those cases are probably the exception.
Those exceptions certainly exist. Jen Brea's famous case has largely proven to be a CCJ issue. Some of the "co" morbidities can indeed be the main problem.
But the comorbidities tend to crop up as The Diagnosis a lot more often than they should because they are relatively obvious — they can actually be diagnosed! They have objective signs that don’t exist in many "pure" cases of ME/CFS.
Most confusing of all, the comorbidities probably exist because they can all be both a symptom and a cause. That is, they can become part of a vicious cycle in which they are made worse by other factors, and then also make a bad situation worse.
Dysautonomia and POTS
Dysautonomia is dysfunction of the autonomic nervous system, which controls your organs and physiology. There are a lot of details, of course, but mainly the ANS regulates your blood pressure and breathing.
Dysautonomia has many possible symptoms, but the most obvious is postural orthostatic tachycardia syndrome (POTS), which mostly involves the heart racing and getting dizzy and woozy when you stand up — excessive “head rushes,” basically. There are other signs of dysautonomia, but POTS captures so much of it that dysautonomia and POTS are largely synonymous in practice.
Like ME/CFS, dysautonomia can be a disease in its own right — a failure of the ANS itself — or as fallout from some other disease (and there are many). When severe, dysautonomia/POTS could plausibly be the cause of ME/CFS. However, it is much more likely that dysautonomia is part of ME/CFS. That is, whatever is causing ME/CFS in the first place also causes dysautonomia… and dysautonomia is what powers many classic ME/CFS symptoms.
Dysautonomia is quite common in ME/CFS and long COVID patients, one of the most prominent comorbidities — but it is not required. Many have no POTS at all, or only mild.
POTS can be managed a bit, regardless of what causes it — mainly by raising blood pressure with increased fluid and salt intake (+5g/day), and sleeping with your head elevated. Most ME/CFS patients should try these things, because it’s cheap and safe, and they might reduce ME/CFS symptoms… and wouldn’t it be great if it was that easy? If this presumptive treatment works, it also largely confirms that POTS is a factor in your case.
Official diagnosis of POTS requires a tilt-table test, in which your vital signs are monitored as you get moved from horizontal to vertical and back again — like a fairground ride, but with medical machines. There are other ways to test for POTS, and in general POTS is fairly obvious. But only the definitive, “formal” diagnosis is via the tilting table.
But you can get the same information much more easily in the comfort of your own home…
POTS and the NASA lean test
Wouldn’t it be great if there was a self-serve alternative to the tilt table test? And there is, or I wouldn’t ask.
This test comes to us from … NASA? Yep, it’s an astronaut thing! Low and zero gravity involves a lot of weird effects on autonomic regulation of blood pressure, so they developed a relatively simple way to check for POTS. Basically you lie down and then stand up and lean against a wall, slightly off vertical, and if your blood pressure drops too much or you feel gross … that’s POTS.
This is an easily obtained objective diagnostic sign of ME/CFS or long COVID — the only one that there is!
It’s not a complicated test, but here is exactly how to do it:
- Lie down quietly for 3 minutes. Take your blood pressure and heart rate once or twice to get a relaxed baseline. (Note that this is not normally how blood pressure is taken, and it will probably be lower than what you’d see from a normal seated test with your arm at heart level, e.g. on an arm-rest. BP measuring is not an exact science, and changing any detail will get a different result. What we’re interested in here is the degree of change between lying down and standing.)
- After your peaceful lie down: get up and lean against wall with your heels 15 centimetres (6 inches) from that wall. In other words, you are a leaning on the wall.
- Now hang out there for a while, at least long enough to take three blood pressure and heart rate readings.
- Stop if you feel the need, if there are nasty symptoms: weakness, heart palpitations, chest pain, racing heart.
- The test is positive for POTS if your systolic blood pressure (the first, big number) drops by more than 20 points, and/or if your diastolic drops by more than 10, and/or if your heart rate surges more than 30 beats per minute. Symptoms not required! You will not necessarily feel it.
Not everyone with ME/CFS or long COVID has POTS, and not everyone with POTS has ME/CFS or long COVID. But they definitely tend to go together, and if you get a clear signal with the NASA lean test, that matters.
Treatment options for primary ME/CFS
The best hope for ME/CFS patients is the diagnostic discovery that their fatigue is caused by something else that can be treated (secondary CFS). Those treatment possibilities are very diverse and entirely contingent on the specific diagnosis.
But primary ME/CFS has no clearly understood cause to attack, and so there is no truly promising treatment of any kind to date. This isn’t surprising in the absence of a clearly understood mechanism. Even if we did understand the nature of the beast, we wouldn’t necessarily know how to tame it. For instance, if the problem is as conceptually straightforward as “it’s immune dysfunction” … unfortunately, there is no way to fix that.
But we’ll review the many dubious possibilities.
Fawzy et al. just published (Jan 2023) a very thorough review of recent or current trials of therapies for Long COVID — and therefore, to a great extent, primary ME/CFS as well.6 This is not a review of the latest and greatest, but just the “latest” — it is an undescriminating report, and absurdly inclusive. They identified over 300 treatment trials, and it is discouraging how few are based on new or more specific ideas. Most are just the same old usual suspects, anything and everything that has ever been tried for anything medical science doesn't know what to do with. There are lots of alternative therapies that are touted to be panaceas, now being speculatively applied to long COVID, and the majority. Some major categories on this list:
- Rank quackeries like homeopathy and photobiomodulation.
- Folk medicine and large categories like yoga, traditional Chinese medicine, Ayurveda, nutraceuticals, and — the vagueness of this one made me LOL — "electrical stimulation." These non-specific to point of silliness, entire treatment philosophies and cultural traditions, being "tested" as therapy for Long COVID.
- Trendy modern bullshit like platelet-rich plasma, ivermection, Vitamin D.
- Lots of coping and harm reduction strategies that I’m sure no one expects to cure anything … but it would certainly be valuable to have a proven method of helping people cope.
Some themes and context about treatment:
- For now, I have limited the scope of this document (for now) to hypothetical treatments, not “coping mechanisms” and “management” or “symptom relief” strategies (with the exception of a discussion of pacing and working around exercise intolerance). But obviously these are very important and certainly have a place in any complete discussion of ME/CFS.
- I have also mostly stayed away from most of the pharmacotherapies, commenting only a few I know something about. There are 76 of them on Fawzy et al.’s list, most of which are unfamiliar to me, and it is possible that some of them are more interesting and promising that others. But that is a big job! To be continued!
- Fibromyalgia hand-me-downs are a big theme. Many fibromyalgia treatments have been transplanted to CFS. In general, they are weak options for fibromyalgia (there are no strong ones), and they are weakened further by the leap from fibromyalgia. It is quite plausible that fibromyalgia and CFS are pathological siblings or cousins. But it is far from certain, and even if they are related they probably still have important differences. Any treatment for CFS that exists mainly because it is known as a fibromyalgia treatment is on very thin conceptual ice.
- Several CFS treatments have their roots in the long history of patronizing/sexist perceptions of the syndrome as malingering and/or laziness and/or depression. For instance, although the point of anti-depressants for CFS patients is putatively to improve sleep, its persistence and popularity is almost certainly powered by the ableist distortion field that categorizes most chronically ill people (especially women) as “maybe not quite right in the head.”
Immune modulation and suppression
This category of treatment options is based on a decent hypothesis… and very little data so far. It is probably the most promising category of options, but it’s also still very early days. Many cases of CFS may be caused by "immune dysfunction" (just as vague as it sounds), and therefore may respond to immunomodulators (like monoclonal antibodies, vaccines, and cytokines), or immunosuppresants (like methotrexate, sulfasalazine, hydroxychloroquine; or even the very potent steroids, like Prednisone— basically the drugs used to treat autoimmune disease). These are the major options:
- Vaccination. There's some modest corroboration from evidence that Long COVID is attenuated by vaccination for COVID, as summarized by this Nature.com article from late 2021.7 And so it could conceivably be valuable for ME/CFS.
- Low-dose naltrexone — There is no direct evidence of efficacy for LDN for CFS, and no clear idea about how it might work. It has been proposed as a CFS treatment mainly based on limited evidence for fibromyalgia and autoimmune disease,8 and the possibility that it is immunomodulatory.9 However, even for that indication LDN is currently overhyped: lots of clinical anecdotes, lots of belief, very little good evidence. It is quite safe and perhaps worth trying, but it’s a much less exciting a possibility than its reputation suggests.
- Embrel (etanercept) is a drug for autoimmune diseases that inhibits "tumor necrosis factor" (TNF), a soluble inflammatory cytokine. It has been hypothesized (in an academic opinion piece)10 that TNF is persistently over-produced in the aftermath of both infections and some brain injuries, and may explain persistent malaise in patients with surprisingly diverse clinical stories. No clinical trial evidence clearly supports this. It’s worth noting that Etanercept isn't even represented on the absurdly inclusive list of Long COVID treatments compiled by Fawzy et al.! Going even further out on a limb…
- Perispinal etanercept: Controversial injection of Etanercept into the fluid around the spinal cord has been sold to patients with brain injuries by a Florida and California clinic for many years now. The physician primarily responsible for this usage of etanercept, Edward Tobinick, is not a neurologist. His practices were seriously criticized and characterized as medical quackery by neurologist and prominent medical skeptic Steven Novella. Tobinick sued Novella, but despite great legal expenses for all involved, Tobinick's claims were ultimately dismissed as a nuisance (SLAPP) suit with major flaws.
- Over-the-counter anti-inflammatories, especially the NSAIDs (ibuprofen, aspirin, etc) — This idea for treating CFS makes only a little bit of sense. It’s like if someone needed to shovel snow from their driveway, you could tell them, "Well, how about a hair dryer? Heat can melt snow!" CFS symptoms may indeed be inflammatory in various senses, and so any anti-inflammatory medication that is anti-inflammatory has some very ham-handed potential. And these medications are highly accessible, and relatively safe (though definitely not entirely safe). But they are also very specific in their action, and they are only anti-inflammatory in "one" way: they inhibit the activity of a family of enzyme that are mostly involved in the making a class of proteins, the prostaglandins, which are in turn ubiquitous in physiology and certain key parts of inflammation. But not all inflammation! And NSAIDs are infamously erratic in their effects even on their primary intended target: inflammatory pain. So it’s really quite unlikely that they are going to help.
Anti-depressants for insomnia
Likely ineffective, based on evidence of absence11 and lack of plausible/relevant mechanism. The role of sleep in CFS is unknown, and could be a driver or just a symptom. Why is this even on the list? Because there's a definite link between fibromyalgia and sleep … but no one knows if there's also a CFS-insomnia link. This intervention has never been very promising, and doubt that it ever will be.
Anticonvulsants (gabapentin/pregabalin, AKA gabapentinoids, as in brands like Lyrica and Neurontin)
There’s just no data on using these drugs for CFS, and for good reason: it isn’t promising enough to have inspired any trials. This treatment is based solely on speculation about a neuropathic mechanism for CFS, which is highly speculative. We know from neuropathy evidence that these drugs undoubtedly do help some patients with neuropathic pain, and there may be some overlap between bog-standard neuropathy and weirder, undiagnosed chronic pain — but even that is speculative. It’s quite a leap to proposing that it might be relevant to CFS without pain. The only thing about CFS that has a neuropathy smell is that neuroinflammation is a likely mechanism. But you really have to be quite generous with the definition of “neuropathy” for it to include neuroinflammation.
Can viagra help ME/CFS? [STUB]
Maybe! The drug sildenafil (Viagra) was originally of medical interest because of its complex effects on blood pressure. The whole penis-pill thing was literally a side effect (an insanely profitable one). It is definitely plausible that this drug could also counteract the effects of dysautonomia/POTS, which may be a major symptom mechanism for CFS. So …not crazy. I give it a thumbs up as weirdly worthwhile: definitely potentially relevant, and not very risky to try. Probably the worst thing about it would be trying to talk a doctor into prescribing it to a woman.
I, on the other hand, would probably find it ridiculously easy to get that Rx. 🤣
Androgen replacement therapy [STUB]
Androgen replacement therapy (ART) is a weirdly appropriate non-crazy option for CFS patients to consider. It is better-known (but less accurately) as testosterone replacement therapy (TRT), and more broadly known as hormone replacement therapy (HRT). Androgens are male hormones, but they aren't just for men — women use them too!
Officially, ART is only for people who have a conspicuous lack of androgen. It’s like supplementing a vitamin: you should probably only do it if you are obviously deficient in that vitamin. And it’s not clear that all that many people actually need more androgens.
But people with CFS are in another category. It’s unlikely that a lack of androgens is actually The Problem… but extra androgens may do a good job of compensation for whatever is actually wrong.
It’s almost a no-brainer thing to try for an aging male with CFS. It is much less clear that it is appropriate for women without a clear and specific biological rationale, and it is certainly harder to get an prescription. Most doctors will probably balk at that, and it’s probably sane and reasonable for them to do so.
Infrared light therapy
Infrared light therapy has been proposed as a treatment for both COVID and long COVID, entirely by people who were over-excited about the medical powers of infrared light long before 2020. Photobiomodulation is out in medicine’s left field, rife with dubious claims and quackery and wild speculation about various forms of it might work, but precious little convincing evidence that it actually does work.12 It’s particularly bad in the sub-category of laser therapy, but infrared is probably a close runner-up.
The biological rationale for treating COVID with infrared light isn’t crazy, but it is entirely hypothetical, and I don’t care for the way it is basically all just a fancy riff on “sunshine is good for you.” While that broad claim is probably true in some ways for a variety reasons, I’m pretty damned sure that "sunshine is medicine for COVID" is a near perfect example of an "extraordinary" medical claim. It’s extremely implausible that infrared light (or sunshine) alone is impressively therapeutic for anything, let alone a disease like COVID. So it needs to be tested with a real experiment, not a thought experiment.
As of Spring 2023, PBM for COVID (not long COVID) has been tested in exactly one clinical trial — but I’m not sure it quite qualifies as a “real experiment.”13 It’s just one under-powered trial conducted by people who clearly already believed that PBM works … and they set out to prove what they believe. There are numerous obvious problems with the study design, and it is doomed to be dismissed as “poor quality” in a meta-analysis some day along with a few others like it. This doesn’t even rise to the level of “promising” evidence for ME/CFS patients. If you have ME/CFS, by all means get whatever sunshine you enjoy, because that has other benefits — but please don’t spend money on infrared therapy gadgets.
Avoidance of environmental triggers
Toxins and moulds are the two major hypothetical environmental causes or triggers for primary ME/CFS (although there are many others).
Mould avoidance — Plausible but unproven hypothesis, and basically zero evidence. I wouldn’t include this option if it hadn’t been taken so seriously by science journalist Julie Rehmeyer in her excellent book, Through the Shadowlands. The mould hypothesis is actually plausible, despite the lack of science and some of the crazy people who believe it and obsess about it. Unfortunately, the only way to personally test this idea effectively is to avoid mould, which basically means “move to a desert for a while” … and even that is problematic, as Julie explains in great detail. Consequently, the mould thing is more interesting than useful.
Toxin avoidance — Entirely unproven and extremely difficult to test, but broadly plausible. The hypothesis: CFS is caused by exposure and/or excessive sensitivity to diverse toxins. The (not unreasonable) fear of toxins has been spectacularly exploited by quacks. But even if we filter out that noise, it remains plausible that some chronic illness could be caused by environmental toxins, mostly based on extrapolation from compelling current and historical examples of underestimated threats like lead, traffic-related air pollution, surgical implants (especially meshes), the emerging microplastics threat, persistent organic pollutants (a large category of nasty chemicals including things like DDT and ), the even more persistent “forever chemicals” (per- and polyfluoroalkyls, or PFAS), and (maybe) a few good additives. I review all of these and more in detail in Chronic, Subtle, Systemic Inflammation: One possible sneaky cause of puzzling chronic pain.
However, there is no clear, specific scapegoat for CFS or any other chronic illness, and several of the candidates are worrisome precisely because they are so ubiquitous and bioaccumulative that they are truly impossible to escape. So as tempting and concerning as this hypothesis may be — even without hyperbole — it presents nearly impossible practical challenges in identifying or avoiding toxins. Realistically, if CFS cases caused by toxicity do exist, most will probably never be solved.
The great danger of these hypotheses about environmental factors is that they are unfalsifiable. No matter how hard you try to avoid them, it’s always possible that you could have seen a benefit if you had avoided them better — because they might more even more ubiquitous and subtle than you previously feared! As long as you’re still sick, you can never actually know if you’ve eliminated them. And so in practice these ideas tend to haunt patients without offering much benefit or even realistic hope, and they can be a powerful driver of medical anxiety.
Morris protocol: helping mitochondria and gut permeability [STUB]
Morris et al. argued in 2019 that mitochondrial dysfunction and reduced gut permeability are both major factors in ME/CFS.14 They propose a treatment “protocol,” a batch of treatment ideas with a strong theme: improving mitochondrial function and lowering gut permeability with: curcumin, N-acetylcysteine, coenzyme Q, melatonin, hydrogen-enriched water, and probiotics. Each of these treatment could be the focus of its own section (and I will do that in time). For the moment, I’m reviewing the paper and the treatment theme as a whole, and highlight some potential weaknesses, namely:
- Curcumin is notoriously difficult to absorb, and there’s no way to ever be sure that you’re actually getting it into your system effectively. Although curcumin is widely available, unfortunately it is poorly absorbed without other agents such as black pepper extract (e.g. piperine). Most bottles advertise one method or another of enhancing absorption, and some of them use it to justify a much higher price point, but it’s hard to know (maybe impossible) how well any of them actually work. Just be aware that straight curcumin may not be effective.
- Coenzyme Q makes me worry a little about the credibility of anyone recommending it. Not condemn! Just… worry. Because the evidence of CoQ is really not great, and in any case is mainly concerned with treating statin-associated myalgia — which is in turn a somewhat over-hyped problem, of genuine concern, but rarely severe.15 The rationale for using it treat ME/CFS is pretty thin.
- Prescribing any “probiotics” strikes me as virtually meaningless. There are major conceptual problems with recommending them to anyone for anything. I have a full discussion of this topic in my supplements article, but the gist is that the microbiome is far too complex to be manipulated with confidence simply by adding species of bacteria.
How do you stay in shape when you cannot tolerate exercise? Or barely?
People with ME/CFS are sick. They are so sick that they cannot exercise effectively any more than someone going through chemotherapy. It is extremely clear that most are not just lazy/deconditioned and can actually get quite a lot sicker when they exercise, a distinct phenomenon known as “exercise intolerance.” The notorious British PACE trial got all this spectacularly wrong, with serious consequences for a generation of ME/CFS sufferers.1617 Repeat after me:
- Exercise can actually harm ME/CFS patients!
- Exercise can actually harm ME/CFS patients!
- Exercise can actually harm ME/CFS patients!
Because they are not just de-conditioned!
This is clear in the case of ME/CFS, but it applies to most unexplained chronic illness. Exercise is only pushed on patients who have no objectively obvious disease.
I extoll the virtues of exercise-as-medicine extensively on PainScience.com. However, I no longer ever speak of exercise being “the next best thing to a miracle cure”18 without at least mentioning the phenomenon of exercise intolerance — because it such a potent, serious, and relatively unknown caveat for so many people with chronic illness and pain.
But the only thing worse than exercise intolerance is also being seriously de-conditioned. Knowing that you may be getting literally weaker, your condition ever more destructive, adds substantially to the frustration and depression. And so most ME/CFS patients certainly want to be as fit as possible… but they want to do it safely! They want a solution.
Given the legacy of PACE, it’s ironic that the solution is actually still “pacing” … just with a different goal, and slower and more careful.
Pacing isn’t a recovery tactic; it’s mostly a way of not getting worse, which makes its value harder to appreciate
Fatigue Can Shatter a Person, Ed Yong (in his last post for The Atlantic)19
How do you work within the limits imposed by exercise intolerance?
Some ideas…
- Many ME/CFS patients can maintain some degree of physical fitness, but some really just cannot — and it’s dangerous to even try. However, whatever capacity you do have, however little, it is wise to use it (or lose that too).
- The challenge is identical in principle to what healthier people face: everyone must find their Goldilocks zone. The difference is that the Goldilocks zone for ME/CFS patients is much smaller, so it require much more meticulous “load management.” You must pay much closer attention to activity levels and stressors, much like a diabetic has to pay way closer attention to diet and blood sugar than non-diabetics. Healthy people have a crapload more “leeway” than, and yet they still routinely overdo and underdo it … but mostly out of ignorance, carelessness. They haven’t been forced by experience to be super careful!
- It is often necessary to redefine “exercise,” and to consider and include quite easy activities that most people wouldn’t call “exercise.” For you, taking the dog out for a pee and climb three flights of stairs might not register as a workout for a healthy person, but it can be your workout!
- Most people with exercise intolerance have good days and bad days … and weeks, and even months. It’s important to learn to recognize them as best you can, to adapt to the changes in how much exercise can be tolerated. Periods of remission are precious. Pounce on those opportunities! But pounce gently, being careful not to overdo it and cause a relapse. Conversely, it’s important to skip the vulnerable days, or at least take it easier. The threshold for triggering exercise intolerance gets even lower when you're compromised by, say, sleep deprivation. Small doses of exercise that might be fine while well-rested could be a real problem on days when you’re not.
- Fitness is not just about exercise — it’s about protecting and optimizing your ability to exercise. Optimize every other possible thing, especially diet and sleep. Don’t sabotage fitness in other ways with preventable failures. The more days you have to skip due to sleep loss that might have been prevented, the more fitness it costs!
The scenario that every ME/CFS sufferer dreads: the Goldilocks zone shrinking down to almost nothing, such a small target that they can no longer hit it, no matter how careful they are. And there are people in that predicament. However, most ME/CFS patients can, with careful load management, probably keep themselves fitter than an couch potato.
If fatigue was an Olympic sport, I’d probably come in fourth so I didn’t have to walk up to the podium.
unknown
Can exercise intolerance be reduced by sneaking up on it?
Many people with exercise intolerance can probably preserve a lot of their physical fitness despite their illness. But what about actually getting better? What if we respected the limits of exercise intolerance but also still tried to progress beyond it?
In general, the PACE trial was terrible because it was based on the bogus assumption that the only problem was de-conditioning, and so it recommended exercise that was too much like an ordinary get-back-in-shape challenge, and that is doomed to collide with fundamental pathological limitations. Some causes of exercise intolerance are never going to be beaten by exercise, just impossible in principle, like trying to cure cancer with push-ups.
In some people, it might be possible in theory, but just too difficult in practice.
And maybe a few people can work through exercise intolerance, depending on what exactly is wrong. If they go slow enough. Maybe. The strategy would be just extremely slow progression, with great caution about never overdoing it. Very baby steps. Painfully slow. So slow that it seems almost ridiculous.
For instance, running just a single kilometre… and then, three days later, running 1.1 kilometres!
I have tried to defeat my own exercise intolerance problem this way, and I reported on my experience for my Project Try Everything newsletter (with somewhat inconclusive results as of that post).
References
Scientific papers and other sources that were particularly useful in preparing this document.
- “Long COVID: major findings, mechanisms and recommendations,” Davis et al., Nat Rev Microbiol, 2023.
- “Autonomic dysfunction and postural orthostatic tachycardia syndrome in post-acute COVID-19 syndrome,” Fedorowski et al., Nat Rev Cardiol, 2023.
- “A systematic review of trials currently investigating therapeutic modalities for post-acute COVID-19 syndrome and registered on WHO International Clinical Trials Platform,” Fawzy et al., Clin Microbiol Infect, 2023.
- “ME/CFS Clinician Coalition Resources,” MECFSClinicianCoalition.org.
- MEpedia (me-pedia.org).
ME/CFS Reading List
Julie Rehmeyer is a science journalist best known for her memoir, Through the Shadowlands: A science writer's odyssey into an illness science doesn't understand. It has a particular emphasis on the somewhat sketchy (but seductive!) mould hypothesis. All of her articles about CFS are also highly recommended, and they are listed here:
https://www.julierehmeyer.com/journalism#mecfs
- Getting It Wrong on Chronic Fatigue Syndrome In 2011, a Lancet study claimed that psychotherapy and gradually increasing exercise could cure chronic fatigue syndrome. But their data showed it couldn't. Patients worked for years to bring the problems with the trial to light, and it was an honor and a thrill to publish a piece in the New York Times (cowritten with David Tuller) bringing the fruit of their labors to light. (March 18, 2017)
- A Disease Doctors Refuse to See — The highly prestigious Institute of Medicine wrote that ME/CFS is a real, non-psychiatric disease, based on a review of the scientific literature, and it called for doctors to take it seriously. Many doctors responded by sneering. (February 25, 2015)
- Why Did It Take The CDC So Long to Reverse Course on Debunked Treatments for Chronic Fatigue Syndrome? — David Tuller and I congratulate the CDC on its recent move to stop recommending cognitive behavioral therapy and graded exercise therapy, and we exhort it to do far, far more to make up for recommending ineffective and often dangerous treatments, for decades. (September 25, 2017)
- Bad Science Misled Millions with Chronic Fatigue Syndrome. Here's How We Fought Back — I'm especially proud of this piece. Patients had just won access to the PACE trial data and published their initial reanalysis, which showed that the PACE investigators' claims of recovery were bogus. I told the story from my own, personal point of view. I think it's the story that best captures the drama of the situation. (September 21, 2016)
David Tuller is a science journalist who has focused on ME/CFS much as I have focused on pain, and he is one of the few sources that I consider to be really exceptional. Although he doesn't have a book, he has a book's worth of articles published on Virology Blog:
Jen Brea is an ME/CFS patient who had a very severe case of ME for many years, and then experienced a dramatic recovery with surgical repair of upper cervical instability. She is a good writer and speaker. I think she was a Harvard PhD student when her illness stopped her. Her TED talk is a great primer, and her blog has a good overview of her experience with links to the highlights:
Dr. Andrew Maxwell is a physician-scientist with a bunch of journal publications and a couple of dense, technical YouTube videos about the "pentad," five malfunctioning systems that seem to underlie ME/CFS. It’s aimed at professionals and it’s hard to watch and absorb, but even without understanding the details, the videos do a nice job of painting a picture of the complexity of the problem.
MEpedia is a wiki devoted to ME/CFS, and seems to be quite well-done, and is probably a good place to start looking for any particular answer. Their primer for patients is a good place to start:
Meghan O'Rourke is a science-friendly writer with ME/CFS who recently published a book, The Invisible Kingdom: Reimagining Chronic Illness. I haven't read it yet, but I have listened to a couple substantive interviews with her, and she seems like a great source.
Loose ends
Links to resources I haven't fully integrated into the document. Not necessarily good!
Notes
This is very tricky, so here’s some elaboration on why I’ve chosen to explain this the way that I have in this document. Basically, I’ve prioritized “practice” over “theory.”
ME and CFS are both used to describe the same patients, but there’s been a great deal of controversy over that, because of the trivializing focus on “fatigue” in “chronic fatigue syndrome.” And so officially there’s no difference between ME and CFS. And what’s official about it is that there are diagnostic criteria for ME/CFS, and there are no there are no special diagnostic criteria for ME as distinct from CFS. We just have diagnostic criteria for a disease that gets labelled with both names. Anyone who meets those criteria is perfectly welcome to identify as a person suffering from either ME or CFS, and they are not wrong. As I wrote, “All ME is CFS.”
But a great deal of CFS-ish illness — like my own, which is probably relevant here! — does not fit the diagnostic criteria for ME/CFS! Ruh roh.
Consequently, there is extremely widespread informal use of the term CFS to label people who do not meet the diagnostic criteria for ME/CFS — the infamous “wastebasket diagnosis,” applied to people with some other undiagnosed “fatiguing illnesses.” This category is extremely contentious and conceptually difficult and many people have argued very forcefully that it needs to go away. If only wishing (or pounding the table) could make it so! Language prescriptivism is largely futile, and CFS is too descriptive and generic to ever go away. It’s only a “wastebasket” diagnosis if it’s clinically abused (as it often is, but railing against the TERM is not going to fix that much larger problem).
So the defacto reality that I chose to describe is that ME means only one thing: a really nasty illness with well-established diagnostic criteria. But “CFS” means both that … aaaand a whole bunch of other stuff: it refers to people who do not meet the diagnostic criteria for ME, often because their symptoms are much milder, and their brains aren’t inflamed, etc.
This isn’t necessarily right. But it’s certainly not carelessly expressed. I am well aware of the controversies about the terminology. For instance, I know that some experts (perhaps most notably Jodi Bassett) have argued very forcefully that “CFS” should never be used to describe anyone ever again. I respect that opinion, but I do not agree with it.
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023 Mar;21(3):133–146. PubMed 36639608 ❐ PainSci Bibliography 51215 ❐
- Dafoe W. Extremely Severe ME/CFS—A Personal Account. Healthcare (Basel). 2021 Apr;9(5). PubMed 33925566 ❐ PainSci Bibliography 51629 ❐
- To make things a little more awkward, he seems to present many of his strange experiences as though they are intrinsic features of the disease. For instance, he treats his inability to tolerate the presence of people in his room is presented like it’s a kind of allergy to people and a primary symptom of ME/CFS… but it seems much more likely to me that it’s an idiosyncratic epiphenomenon, and not of much clinical interest beyond that.
- WashingtonPost.com [Internet]. Miller M. For millions like me with long covid, the pandemic isn’t over; 2023 Aug 9 [cited 24 Oct 22]. PainSci Bibliography 51628 ❐
Surprisingly, the number and quality of the comments on this article is exceptional. Ms. Miller has some excellent fans, I think!
- Fawzy NA, Abou Shaar B, Taha RM, et al. A systematic review of trials currently investigating therapeutic modalities for post-acute COVID-19 syndrome and registered on WHO International Clinical Trials Platform. Clin Microbiol Infect. 2023 Jan. PubMed 36642173 ❐ PainSci Bibliography 51212 ❐
- Nature.com [Internet]. Ledford H. Do vaccines protect against long COVID? What the data say; 2023 February 25 [cited 23 Mar 1]. PainSci Bibliography 51213 ❐
- Raknes G, Småbrekke L. Low dose naltrexone: Effects on medication in rheumatoid and seropositive arthritis. A nationwide register-based controlled quasi-experimental before-after study. PLoS One. 2019;14(2):e0212460. PubMed 30763385 ❐ PainSci Bibliography 51250 ❐
- Yi Z, Guo S, Hu X, et al. Functional modulation on macrophage by low dose naltrexone (LDN). Int Immunopharmacol. 2016 Oct;39:397–402. PubMed 27561742 ❐
- Clark IA. Chronic cerebral aspects of long COVID, post-stroke syndromes and similar states share their pathogenesis and perispinal etanercept treatment logic. Pharmacol Res Perspect. 2022 Apr;10(2):e00926. PubMed 35174650 ❐ PainSci Bibliography 51248 ❐
- Everitt H, Baldwin DS, Stuart B, et al. Antidepressants for insomnia in adults. Cochrane Database Syst Rev. 2018 May;5(5):CD010753. PubMed 29761479 ❐ PainSci Bibliography 51418 ❐
“Mechanism masturbation” is wishful thinking about why/how treatments might work, usually as a substitute for evidence that they actually do work. The term was coined by science journalist Jonathan Jarry). Musculoskeletal and pain research, alternative as well as more mainstream research, is particularly rotten with “mechanism masturbation.” There’s almost no good clinical trial data, so we get fanciful speculation instead — even in scientific publications, especially the lower quality ones. The field is surprisingly rotten with cart-before-horse speculation about how they how they could work, might work, should work, maybe work… when the clinical trials (if they exist at all) tend to show that they don’t actually work, or not very well. For more, see Speculation-Based Medicine or 15 Kinds of Bogus Citations.
- Pereira PC, de Lima CJ, Fernandes AB, Zângaro RA, Villaverde AB. Cardiopulmonary and hematological effects of infrared LED photobiomodulation in the treatment of SARS-COV2. J Photochem Photobiol B. 2023 Jan;238:112619. PubMed 36495670 ❐ PainSci Bibliography 51278 ❐
- Morris G, Puri BK, Walker AJ, et al. Myalgic encephalomyelitis/chronic fatigue syndrome: From pathophysiological insights to novel therapeutic opportunities. Pharmacol Res. 2019 Oct;148:104450. PubMed 31509764 ❐
- Cholesterol Treatment Trialists' Collaboration. Effect of statin therapy on muscle symptoms: an individual participant data meta-analysis of large-scale, randomised, double-blind trials. Lancet. 2022 Aug. PubMed 36049498 ❐
This is an enormous review of nineteen placebo controlled tests of the side effects of statins, following over 30,000 patients for about 4 years on average. A data set like that makes a typical little musculoskeletal medicine study look like a shack in the shadow of the Burj Khalifa.
There was no major difference in the rates of muscle pain and weakness in statins versus placebo. They saw a modest signal in the first year, and for more intensive statin therapy: slightly more myopathy with statins, and mostly mild. Only about 1 in 15 cases of allegedly statin-induced myopathy reported by patients were actually related to statins, according to this data, and those were pretty tame. The researchers concluded:
“Statin therapy caused a small excess of mostly mild muscle pain. Most (>90%) of all reports of muscle symptoms by participants allocated statin therapy were not due to the statin. The small risks of muscle symptoms are much lower than the known cardiovascular benefits.”
This statin evidence cuts both ways: it undermines the Legend of Statin Associated Myopathy, but it also confirms that there is indeed an unpleasant side effect. Even a 5% risk of very mild-but-chronic muscle pain might seem unacceptable to many people. One in twenty is not “rare,” and no amount of chronic pain is cool. So even as it fights excessive hype about SAM, it’s not particularly reassuring either.
Note that statins were directly caught on "camera" meddling in muscle cell metabolism (see Weninger). While not capable of explaining everything about statin myopathy, this significantly boosts the case for a genuine medical side effect.
For a more detailed report on this paper, see “Sign me up for mild muscle pain? The statins dilemma.”
- www.virology.ws [Internet]. Tuller D. Trial by Error: The Troubling Case of the PACE Chronic Fatigue Syndrome Study; 2017 August 17 [cited 21 Nov 18]. PainSci Bibliography 52991 ❐
- www.nytimes.com [Internet]. Rehmeyer J, Tuller D. Getting It Wrong on Chronic Fatigue Syndrome; 2021 November 18 [cited 23 Aug 30]. PainSci Bibliography 52219 ❐
The huge but notoriously flawed PACE trial seemed to support the idea that chronic fatigue syndrome patients are just de-conditioned and therefore need to suck it up and exercise, slowly building themselves back up again. This was evidence-based medicine at its very worst: one low quality but influential study drowning out both contradictory evidence and patient voices. It has become the most extreme example of telling sick people that their illness is “all in your head.” Julie Rehmeyer and David Tuller’s NYT piece is the canonical summary of the whole debacle.
- Academy of Medical Royal Colleges. Exercise: The miracle cure and the role of the doctor in promoting it. AOMRC.org.uk. 2015 Feb. PainSci Bibliography 53672 ❐
This citation is the primary authoritative source of the quote “exercise is the closest thing there is to a miracle cure” (although there are no doubt many variations on it from other sources over the years).
- www.theatlantic.com [Internet]. Yong E. Fatigue Can Shatter a Person: Everyday tiredness is nothing like the depleting symptom that people with long COVID and ME/CFS experience; 2023 August 3 [cited 23 Aug 3]. PainSci Bibliography 51284 ❐