A test of lidocaine for neck pain
Lidocaine is an anaesthetic rather than an analgesic. That is, it doesn’t just relieve pain, it stops all sensation in affected tissue. That’s quite useful if you know specifically what tissue to apply it to.
And if there’s a practical way to get it there. Dentists make good use of it, because they can inject it right where it’s temporarily needed.
But it’s a poor candidate for “non-specific” pain. What exactly needs numbing? We often cannot know.
Not that the uncertainty stops people from trying! Lidocaine patches are the second most popular kind of topical pain medication, after NSAIDs like diclofenac, e.g. Voltaren.
Cohen et al. pitted lidocaine patches against placebo patches — a nice tidy test — in a few dozen people with unexplained chronic, moderate neck pain. Unfortunately (but unsurprisingly) lidocaine showed no sign of being useful:
“No significant differences were observed between the lidocaine and placebo patches.”
The study was based on the assumption that neck pain is often driven by muscle. However much controversy there is about the nature of “trigger points,” no one disputes that we do get poorly understood sore spots, so it’s certainly not crazy to try to numb them. But lidocaine only soaks in about a centimetre right under the patch, while the muscle tissue there is up to several centimetres deep. So unless that neck pain is coming mainly from a small patch of tissue right under the patch … good luck with that!
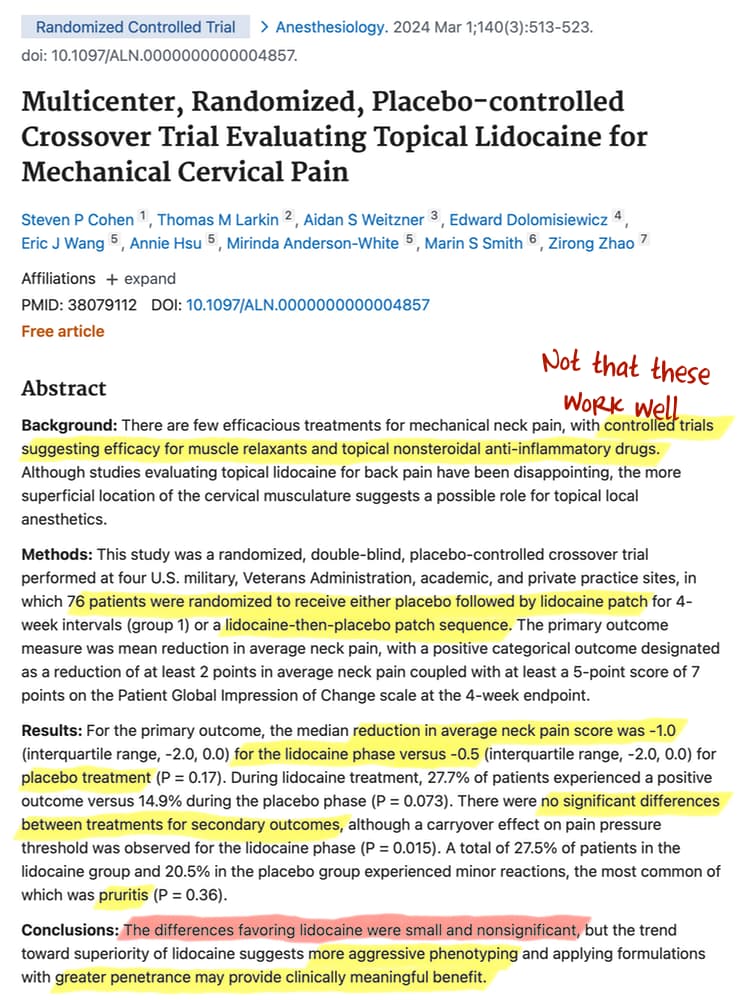
The authors point out that lidocaine was slightly superior to a placebo, albeit in a statistically trivial way. They speculate that lidocaine could work better with a better patch applied to more carefully selected patients (more likely to have neck pain attributable to cranky muscle). I agree it’s possible, but wake me up when someone has actually done that test and lidocaine has put in an impressive showing.
And what, pray tell, would be a “better patch”? That would be one with a “penetrant,” a solvent that carries the drug deeper into the tissue — like DMSO (dimethyl sulfoxide), which I coincidentally just wrote a lot about last week. And I gave it low marks for safety. It’s also touted as an analgesic in its own right, so it would complicate a test like this.