Preventing arthritis and tendinitis is easier than you think (with patience)
One of the most deeply held beliefs in musculoskeletal medicine is that osteoarthritis is a “wear and tear” condition — that joints slowly crumble under the onslaught of gravity and use and abuse. This fundamentally mechanical view of arthritis directly suggests that the heavier we are, the more likely we are to have trouble in our load-bearing joints.
But that’s just not the case: osteoarthritis prevalence doubled in the 20th Century independent of age and weight (Wallace 2017).
So something else has to be going on. People got heavier on average, but not twice as heavy!
Or consider this: obese people get more osteoarthritis of the hand (Jiang 2016), but probably not because they are walking on their hands.
So … why?
This post weaves together the threads of several past posts about the biochemical foundations of seemingly “mechanical” problems, and you may recognize some pieces. But this is an all-new synthesis, anchored by some good science news you can use — practical and encouraging, which is a rare pleasure.
The root cause of “mechanical” degeneration of tissue
A new review by Lynskey et al. adds to the pile of evidence showing that seemingly mechanical conditions like arthritis and tendinopathy are much more about metabolic health than physical stresses. Physiology and biochemistry more than anatomy and biomechanics.
Take two people with the same physical stresses on the knee and it’ll probably be the borderline diabetic who gets the knee osteoarthritis first.
So what goes wrong with “metabolic health”? It’s a mash-up of what most people know as your risk of heart disease and diabetes — all familiar stuff. You know your metabolic health might be mangled when you are “out of shape” — high blood sugar, high blood pressure, lots of cholesterol in your blood and belly fat. You get out of breath taking a flight or two of stairs. All of this going on at once is known as “metabolic syndrome.”
With apologies to Indiana Jones, it’s not the years or the mileage — it’s the biological context!
Here's a nice mini-infographic on this topic:
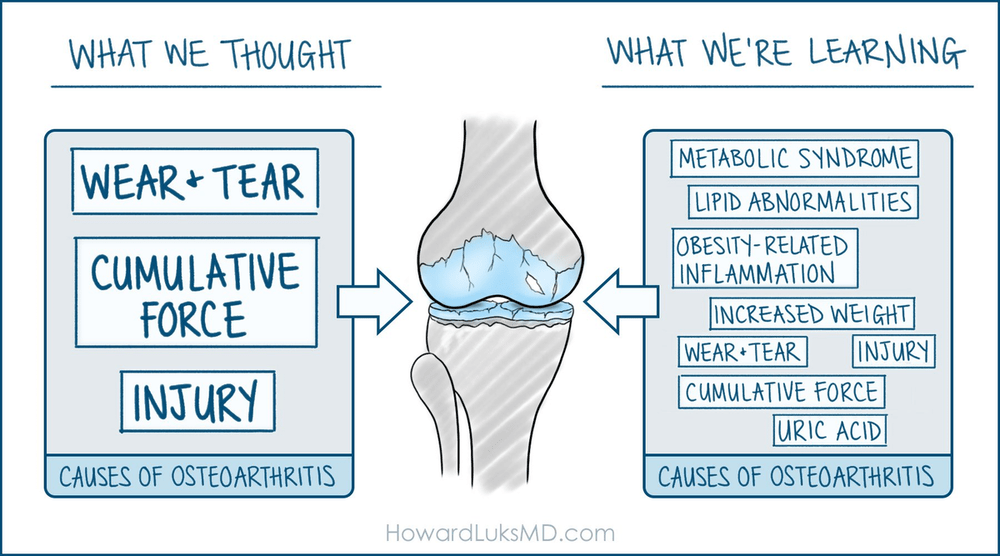
So what’s the link between being at risk for heart attacks and knee osteoarthritis?
Inflammation, of course. It’s all about the inflammation. That’s the common denominator.
Chronic systemic inflammation does all kinds of harm over time. It’s not just the trigger for the formation of arterial plaques (the key mechanism of heart disease). It also chips away at our musculoskeletal system.
I think of it kind of like slowly “rusting.”
It makes problems like arthritis, tendinitis, and stress fractures far more likely. It makes them actually worse (more damage) and also feel worse (neurological sensitization). And it makes them harder to bounce back from. And it makes our tissues harder to fortify with exercise to prevent the next injury.
No wonder aging is hard! Even if you stay in shape as best you can, aging eventually leads to metabolic syndrome … which is why aging and inflammation are so intertwined that we have the charming term “inflammaging.”
So it’s hard to stop the inflammation. But it is wise to try! I’ll conclude with some good news today.
Exercising for arthritis prevention is easy (but slow)
Exercise can probably modestly treat arthritis in the short term (Weng et al), but it’s not exactly spectacular, and it might not even work at all (see my posts about Bandak et al.). Prevention is a more realistic goal.
If you want to improve your metabolic health — and so your musculoskeletal health as well — you probably need to play the long game. And postponing death is, hopefully, the longest game of all! It’s well established that exercise reduces mortality, but how much do you need?
Probably less than you think! Hakuna Matata!
Ahmadi et al. studied how much regular vigorous physical activity we need to reduce our risk of death from heart disease, cancer, and more … and the results were quite encouraging. They found that relatively easy workouts for a year were effective at preventing deaths: “well under the current recommended 75 min/week of vigorous physical activity were associated with the lowest risk.”
This was of those morbid mortality studies, a big one cross-referencing deaths with fitness gadget data for tens of thousands of people. People died less if they did frequent small doses of vigorous exercise — less than 2-minute sessions, and only one or two per day. Intense and regular, but just little blasts of action. Micro workouts.
The benefits of that became measurable at 15-minutes per week, and continued to improve up to a total of an hour per week (distributed over 4 very small workouts per day). Still very manageable!
The reduced “all-cause mortality” studied by Ahmadi et al. definitely overlaps with the “reduced systemic inflammation” measured by Klasson et al., suggesting that taming inflammation was probably partly how mortality was reduced. In other words, although this study did not study the effect of exercise on arthritis… it’s a safe bet they would have found an effect if they did.
So how should we prevent or slow down the progression of arthritis and tendinitis?
Mainly with a modest exercise effort in the Goldilocks zone. Not only do you not have to be “hardcore,” you mostly shouldn’t be — because wear-and-tear is also still a factor! “Overdoing it” also causes (local) inflammation.
And remember last week’s post? “Weekend warriorism maybe not so bad,” because of science showing that we don’t need to exercise every day, or even every other day, to compensate for being lazy. That harmonizes very nicely with this. Put it all together for this bottom line advice:
To maintain metabolic and musculoskeletal health, do vigorous but relatively brief workouts — get out of breath, however you like — and allow adequate recovery.
And this is about a thousand times more important than, say, fussing over your posture.