Cervical myodural bridges: an obscure cause of neck pain?
Brace yourself for humility: this is a great example of how hard it is to be sure of anything in musculoskeletal medicine.
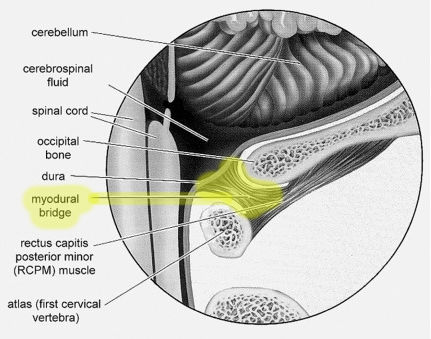
Cervical myodural bridges are an obscure anatomical feature of the neck that may cause pain (see Palomeque-Del-Cerro et al). They are variable soft tissue connections between the spinal cord wrapping (dura mater) and the muscles of the upper neck — basically some rogue gristle. Exactly what is connected and how tightly is unknown and is probably quite different from person to person, like all anatomy.
The clinical implications are unclear, but they surely exist (see Enix). Although I have vigorously denounced the overemphasis on structural and biomechanical causes of pain — and I stand by that — sometimes structure does matter. CMBs probably explain why some people can flex their upper neck more comfortably than others, and they probably cause headaches in some people. Indeed, they may be one sneaky way that cervicogenic (“from the neck”) headaches work.
Obviously there’s not much to be done about a CMB — surgery in that region is serious business, and could be worse than the disease in most cases. Don’t even think about it, especially because it’s nearly certain that some CMBs cause no trouble at all.
It’s also nearly certain that a few cases are a bigger deal. Consider the evidence that chronic intermittent spinal cord irritation is strongly associated with fibromyalgia. Regular tugging on the dura mater might really suck. Just sayin’.
You can at least get some sense of whether or not this might be a problem for you just by strongly flexing your upper neck (tuck your chin down firmly): if it’s uncomfortable, there’s a chance you have pesky myodermal bridges! Or …
Maybe it’s just trigger points in your suboccipital muscles? Trigger points are common sore spots in soft tissue of unknown and controversial nature. Which are also sensitive to stretch. So it’s probably impossible to tell the difference between a neck that is sore because of “trigger points” and one that is sore because of a CMB. Some people might get suboccipital trigger points because of the CMB, so “all of the above” is definitely a possibility — and a fine example of how we might be poking at our suboccipital muscles in vain, hoping to “release” trigger points that either aren’t there at all, or are effectively untreatable because a CMB is delivering an infinite source of minor irritation. How many massages have tried to rub away CMB discomfort?